Embed Size (px)
Citation preview
INTERNATIONAL JOURNAL OF HEALTH PLANNING AND MANAGEMENT, VOL. 6,273-286 (1991)
QUALITY OF CARE ASSESSMENT OF PUBLIC AND PRIVATE OUTPATIENT CLINICS IN
METRO CEBU, THE PHILIPPINES
DAVID H. PETERS’ AND STAN BECKER’ ’ Department of International Health, Johns Hopkins University, School of Hygiene and
Public Health, 615 North Wove St, Baltimore, MD, USA 21205 ’Department of Population Dynamics, Johns Hopkins University, School of Hygiene and
Public Health, Baltimore, MD, USA
SUMMARY Despite large investments in primary health care in developing countries, evaluation of the quality of services has been neglected. Managers need information on service quality to identify specific ways to improve health-care delivery, and to determine how health programs can achieve their desired effects.
We tested several quality-assessment methods in 48 public and private outpatient clinics in Metro Cebu, The Philippines. Structured observations of immunization ses- sions and clinic logistics highlighted functional problems at particular clinics that contri- buted to shortages of vaccines, sterilized needles and oral rehydration salts (ORS). Quality assessment of medical records for the treatment of diarrhea revealed a wide variation in the recorded quality of services. Clinical case histories were presented to public and private providers, who advised different approaches for case management, highlighting areas where improvement is needed. For example, public providers were more likely to use ORS to treat dehydration; private providers were more likely to enquire about symptoms of dysentery. Private providers were more likely to treat a mild respiratory infection with antibiotics, but few providers were likely to prescribe antibiotics for a child with signs suggestive of severe pneumonia. Advice to mothers was insufficient in most areas. These quality-assessment methods can be used by managers to develop training curricula and solve problems in the delivery of primary health-care services.
KEY WORDS: Quality assurance; Primary health care; Philippines
INTRODUCTION
Evaluations of primary health care (PHC) programs in developing countries have focused on health outcomes and cost-effectiveness. While such evaluations are useful for policy-makers and researchers, managers are often left without relevant information on the quality of services (Van Norren et al., 1989). Know- ledge of the quality of care is particularly vital to program managers, because it is within their power to modify how care is delivered. However, few studies have been published on quality assessment in developing countries, and metho- dologies are poorly developed for these settings. In an environment where
0749-615319 11040273-14$07.00 0 1991 by John Wiley & Sons, Ltd.
274 D. H. PETERS AND S. BECKER
many health systems are concentrating on PHC, simple and efficient assessment tools are urgently needed to optimize health services.
A theoretical framework for assessing the quality of medical care has been described in seminal works by Donabedian (1966, 1969). Inferences about qua- lity are made under three categories: structure, process and outcome. Structure refers to the attributes of the settings in which care occurs, including the material resources (such as equipment and facilities), human resources (such as the number and qualifications of the staff), and organizational structure (such as methods of staff organization and supervision). Process denotes what is actually done in giving and receiving care, while outcome refers to the effects of care on the health status of patients and populations, often described by morbidity and mortality levels.
Garner et al. (1990) presented a method for structural assessment of health facilities in rural Papua New Guinea, using a checklist primarily based on the presence of certain equipment and medicines. However, this method does not provide key information about how well facilities are performing. Process methods involve the direct examination of the functional components of deliver- ing and receiving services, but there are few examples of this in developing countries. In one case, Walker et al. (1988) developed explicit criteria for assess- ing the adequacy of inpatient management of infantile gastroenteritis by survey- ing local physicians in Jamaica. They then reviewed medical records and demonstrated that the survival of infants admitted with diarrhea was better at hospitals that practised good case management by their criteria.
This study uses several methods to evaluate the provision of key child survival activities at both public and private outpatient clinics. The main activities included immunizations and case management of diarrhea and acute lower respiratory infections (ALRI). Structural aspects were first examined by assess- ing clinic logistics, emphasizing the functional ability of the clinic to deliver services, rather than the mere presence of equipment. We also developed process indicators and systematically observed immunization delivery, audited clinic records for diarrhea therapy, and interviewed providers about clinical manage- ment of patients.
ORGANIZATION OF PRIMARY HEALTH SERVICES IN METRO CEBU
Metro Cebu, located on Cebu Island in the central Philippines, has a population of one million persons living in both urban and rural areas (Department of Health, 1988). Child health services are provided at both public and private outpatient facilities. Responsibility for the management of public facilities is divided between the Regional Department of Health, which largely serves rural areas, and three city administrations. The outpatient facilities are similar in the different jurisdictions, and are basically of three types: barangay health stations (BHS; barangays are the local administrative units), main health centers (some are called rural health units) and hospitals. Barangay health stations
QUALITY OF CARE ASSESSMENT OF PUBLIC AND PRIVATE OUTPATIENT CLINICS 275
are the smallest peripheral health units. They are usually staffed by trained midwives and community volunteers, though physicians hold clinics on some days. Main health centers are larger and better equipped, staffed by a nurse and/or a physician, and provide services to a larger population in addition to giving backup support to the BHS. Patients can also be referred to local hospitals which have more sophisticated outpatient services.
Immunizations are provided at all public facilities. They are usually given on scheduled days, on a weekly to monthly basis. For diarrhea treatment, all public facilities provide free ORESOL, the locally packaged oral rehydration salts (ORS). Health workers are trained to recognize and treat dehydration, in addition to promoting the use of home fluids and breastfeeding. There is presently no programme for the case management of ALRI at the public clinics, although one is now being planned. Nevertheless, public facilities are expected to provide simple curative care for patients with respiratory infections, and some facilities carry antibiotics for treatment. All treatments, including drugs, are free of charge at public clinics.
Private physicians offer services similar to those in the public clinics, but charge a fee for their services. They generally work in individual or group practices, or in an outpatient department of a private hospital. Private clinics do not usually have immunization days, and earlier work suggests that they provide less than 10 per cent of the immunizations to children in the region (Becker and Peters, 1991). In the urban areas, private practitioners provide most of the outpatient care for diarrhea and respiratory conditions in young children. They are not supplied with ORESOL from the government program, but do prescribe or distribute ORS and other therapies for diarrhea. There are many traditional healers who also are not supplied with ORESOL. Although they treat childhood illnesses, they were not included in this study.
METHODS
This study was part of a larger investigation of the effects of ORS and immuniza- tions on child morbidity and mortality, which involved over 8300 mothers and their children living in a random sample of 33 barangays (Becker and Peters, 1991). A baseline survey of mothers provided descriptive information on patterns of health-care utilization that was used in the selection of a represen- tative sample of 27 public clinics, including all public facilities located in the sample barangays. For barangays which did not have a public facility, the public facility in an adjacent barangay that was used most frequently for child- hood immunizations was chosen. For the selection of private providers, the provider most frequently seen for childhood diarrhea and respiratory symptoms in each barangay was chosen, yielding a total of 21 private physicians.
Data collection was conducted from February to March, 1990. A pre-tested, structured survey was administered by nurses trained and supervised for this study. Using the Primary Health Care Thesaurus (Shaikh, 1988), a checklist

216 D. H. PETERS AND S. BECKER
was designed to observe and record logistical functions of the clinics. The checklist covered items regarding storage and record-keeping for vaccines, ORESOL and antibiotics, and was supplemented by questions about methods of ordering supplies, and the length of time, if any, that the clinic was without certain supplies.
To assess the records of diarrhea therapy, we used procedures for lot quality- assurance sampling (Wolff and Black, 1989). Standards for acceptable diagnosis and treatment were defined with local public health officials, following the WHO guidelines for case management of diarrhea (WHO, 1989). The basic criteria for ‘acceptable’ management included an assessment of dehydration and an appropriate therapy. Only clinics that maintained records on patients treated for diarrhea in 1989 were considered. The audit of medical records was limited to diarrhea cases at public clinics, because most public clinics did not maintain records that could be used to assess the treatment of conditions other than diarrhea, and records at private clinics contained too little infor- mation to analyse.
Because of the relative infrequency of attendance at the clinics by children with ALRI and diarrhea, it was not practical to observe providers treating these conditions. Instead, the usual provider at each clinic was presented with oral summaries of clinical cases and asked to say how helshe would manage the case. The case summaries covered history taking, therapy and advice for diarrhea and respiratory infection, along with several cases about immunization. Interviewers were trained to probe for multiple answers without suggesting specific responses. To compare statistically the frequency of responses between public and private providers, Fisher’s exact test was used (Fleiss, 1981).
Structured observations were conducted at immunization sessions in each public facility. After the earliest possible start in the day, a child was selected every 30 min during registration until four were chosen. The child was followed from the point of registration until departure from the clinic. The key items examined were correct or incorrect dose and administration of the vaccine, record-keeping, and advice to the mother about the next dose of vaccine. The handling of vaccines and equipment for the session was also observed, and the duration that vaccine vials were left open was timed. When calculating the time that a vial was left open, all open vials were included, with the time truncated at the end of the clinic.
RESULTS
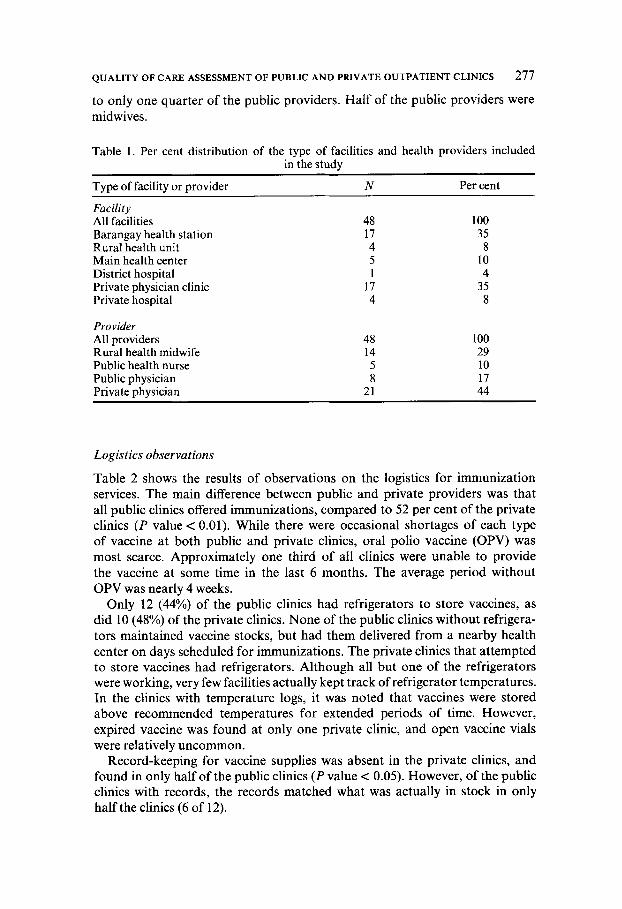
Assessments were completed at all 27 public and 21 private facilities (Table 1). Barangay health stations were the most frequent type of public clinic, while the private facilities were largely private doctors’ clinics and some hospital outpatient departments. A11 the private providers were physicians, compared
QUALITY OF CARE ASSESSMENT OF PUBLIC AND PRIVATE OUTPATIENT CLINICS 277
to only one quarter of the public providers. Half of the public providers were midwives.
Table 1. Per cent distribution of the type of facilities and health providers included in the study
Type of facility or provider N Per cent
Facility All facilities 48 100 Barangay health station 17 35 Rural health unit 4 8 Main health center 5 10 District hospital 1 4 Private physician clinic 17 35 Private hospital 4 8
Provider
Rural health midwife 14 29 Public health nurse 5 10 Public physician 8 17
All providers 48 100
Private physician 21 44
Logistics observations
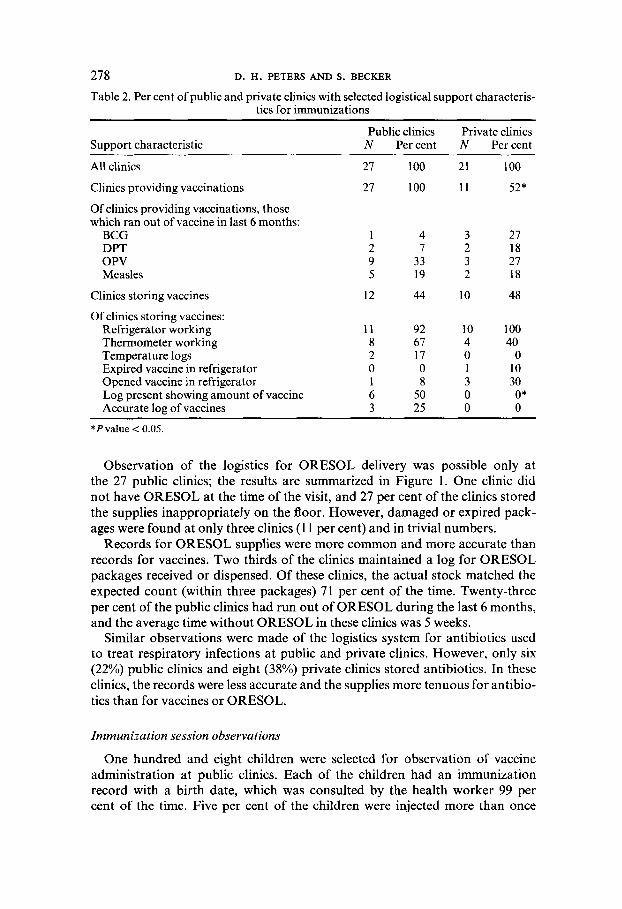
Table 2 shows the results of observations on the logistics for immunization services. The main difference between public and private providers was that all public clinics offered immunizations, compared to 52 per cent of the private clinics (P value < 0.01). While there were occasional shortages of each type of vaccine at both public and private clinics, oral polio vaccine (OPV) was most scarce. Approximately one third of all clinics were unable to provide the vaccine at some time in the last 6 months. The average period without OPV was nearly 4 weeks.
Only 12 (44%) of the public clinics had refrigerators to store vaccines, as did 10 (48%) of the private clinics. None of the public clinics without refrigera- tors maintained vaccine stocks, but had them delivered from a nearby health center on days scheduled for immunizations. The private clinics that attempted to store vaccines had refrigerators. Although all but one of the refrigerators were working, very few facilities actually kept track of refrigerator temperatures. In the clinics with temperature logs, it was noted that vaccines were stored above recommended temperatures for extended periods of time. However, expired vaccine was found at only one private clinic, and open vaccine vials were relatively uncommon.
Record-keeping for vaccine supplies was absent in the private clinics, and found in only half of the public clinics (P value < 0.05). However, of the public clinics with records, the records matched what was actually in stock in only half the clinics (6 of 12).
278 D. H . PETERS AND S. BECKER
Table 2. Per cent of public and private clinics with selected logistical support characteris- tics for immunizations
Support characteristic Public clinics Private clinics
N Percent N Percent
All clinics Clinics providing vaccinations Of clinics providing vaccinations, those which ran out of vaccine in last 6 months:
BCG DPT OPV Measles
Clinics storing vaccines Of clinics storing vaccines:
Refrigerator working Thermometer working Temperature logs Expired vaccine in refrigerator Opened vaccine in refrigerator Log present showing amount of vaccine Accurate log of vaccines
27 100
27 100
1 4 2 7 9 33 5 19
12 44
11 92 8 67 2 17 0 0 1 8 6 50 3 25
21 100 11 52*
3 27 2 18 3 21 2 18
10 48
10 100 4 40 0 0 1 10 3 30 0 O* 0 0
*Pvalue < 0.05.
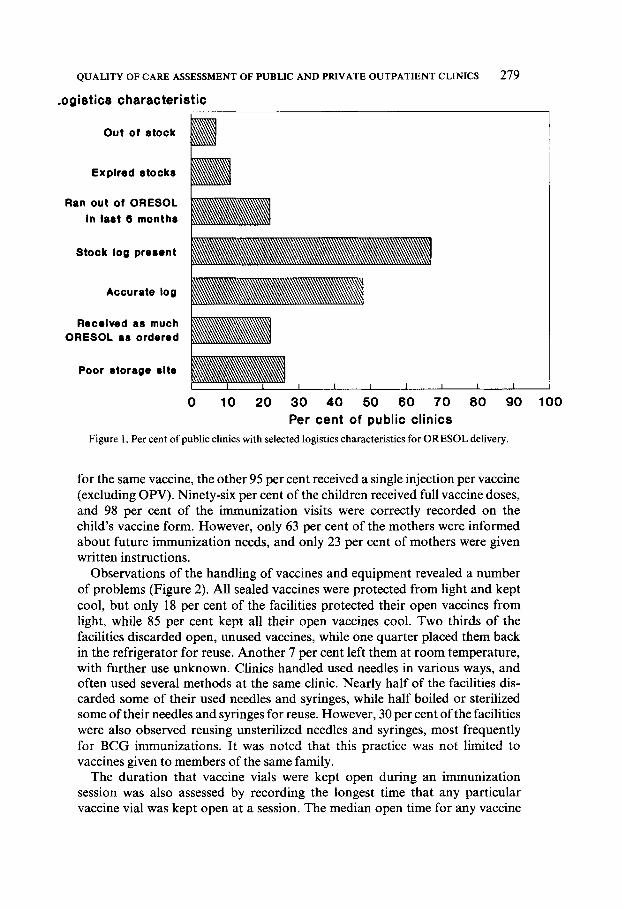
Observation of the logistics for ORESOL delivery was possible only at the 27 public clinics; the results are summarized in Figure 1. One clinic did not have ORESOL at the time of the visit, and 27 per cent of the clinics stored the supplies inappropriately on the floor. However, damaged or expired pack- ages were found at only three clinics (1 1 per cent) and in trivial numbers.
Records for ORESOL supplies were more common and more accurate than records for vaccines. Two thirds of the clinics maintained a log for ORESOL packages received or dispensed. Of these clinics, the actual stock matched the expected count (within three packages) 71 per cent of the time. Twenty-three per cent of the public clinics had run out of ORESOL during the last 6 months, and the average time without ORESOL in these clinics was 5 weeks.
Similar observations were made of the logistics system for antibiotics used to treat respiratory infections at public and private clinics. However, only six (22%) public clinics and eight (38%) private clinics stored antibiotics. In these clinics, the records were less accurate and the supplies more tenuous for antibio- tics than for vaccines or ORESOL.
Immunization session observations
One hundred and eight children were selected for observation of vaccine administration at public clinics. Each of the children had an immunization record with a birth date, which was consulted by the health worker 99 per cent of the time. Five per cent of the children were injected more than once
QUALITY OF CARE ASSESSMENT OF PUBLIC AND PRIVATE OUTPATIENT CLINICS 279
.ogistics characteristic
~
Out of stock
Explred stocks
Ran out 01 ORESOL in last 6 months
~
~
Stock log present
Accurate log
Recelved a8 much ORESOL as ordered
Poor storage slte I I I I I I 1
0 10 20 30 40 50 60 7 0 80 90 100 Per cent of public clinics
Figure 1. Per cent of public clinics with selected logistics characteristics for ORESOL delivery.
for the same vaccine, the other 95 per cent received a single injection per vaccine (excluding OPV). Ninety-six per cent of the children received full vaccine doses, and 98 per cent of the immunization visits were correctly recorded on the child’s vaccine form. However, only 63 per cent of the mothers were informed about future immunization needs, and only 23 per cent of mothers were given written instructions.
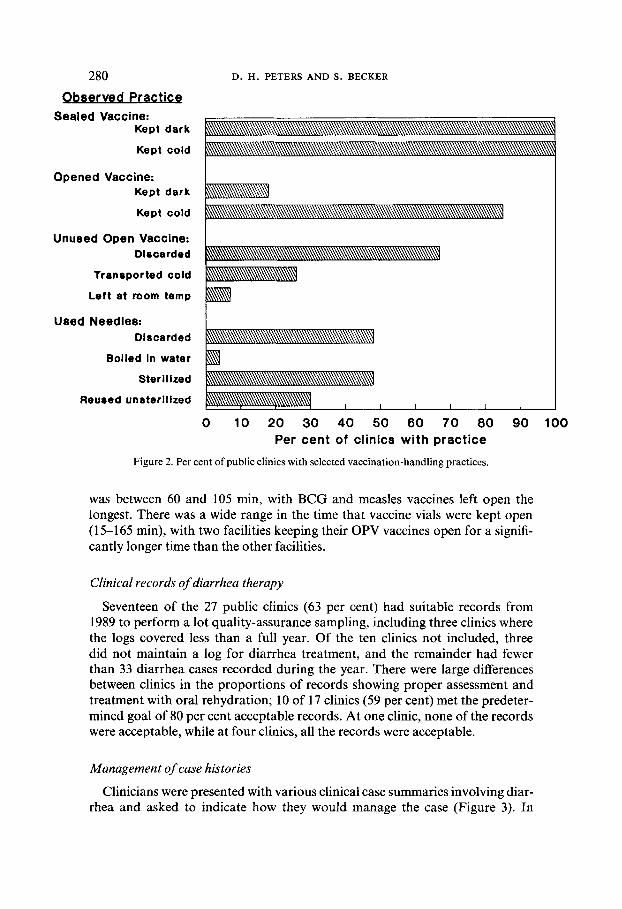
Observations of the handling of vaccines and equipment revealed a number of problems (Figure 2). All sealed vaccines were protected from light and kept cool, but only 18 per cent of the facilities protected their open vaccines from light, while 85 per cent kept all their open vaccines cool. Two thirds of the facilities discarded open, unused vaccines, while one quarter placed them back in the refrigerator for reuse. Another 7 per cent left them at room temperature, with further use unknown. Clinics handled used needles in various ways, and often used several methods at the same clinic. Nearly half of the facilities dis- carded some of their used needles and syringes, while half boiled or sterilized some of their needles and syringes for reuse. However, 30 per cent of the facilities were also observed reusing unsterilized needles and syringes, most frequently for BCG immunizations. It was noted that this practice was not limited to vaccines given to members of the same family.
The duration that vaccine vials were kept open during an immunization session was also assessed by recording the longest time that any particular vaccine vial was kept open at a session. The median open time for any vaccine
280
Observed Practice Sealed Vaccine:
Kept dark
Kept cold
Opened Vaccine: Kept dark
Kept cold
Unused Open Vaccine: Dlacarded
Tranrported cold
Left at room temp
Used Needles: Discarded
Boiled In water
Sterilized
Reu8ed unsterlllzed
D. H. PETERS AND S. BECKER
0 10 20 30 40 50 60 7 0 80 90 100 Per cent of clinics with practice
Figure 2. Per cent of public clinics with selected vaccination-handling practices.
was between 60 and 105 min, with BCG and measles vaccines left open the longest. There was a wide range in the time that vaccine vials were kept open (15-165 min), with two facilities keeping their OPV vaccines open for a signifi- cantly longer time than the other facilities.
Clinical records of diarrhea therapy
Seventeen of the 27 public clinics (63 per cent) had suitable records from 1989 to perform a lot quality-assurance sampling, including three clinics where the logs covered less than a full year. Of the ten clinics not included, three did not maintain a log for diarrhea treatment, and the remainder had fewer than 33 diarrhea cases recorded during the year. There were large differences between clinics in the proportions of records showing proper assessment and treatment with oral rehydration; 10 of 17 clinics (59 per cent) met the predeter- mined goal of 80 per cent acceptable records. At one clinic, none of the records were acceptable, while at four clinics, all the records were acceptable.
Management of case histories
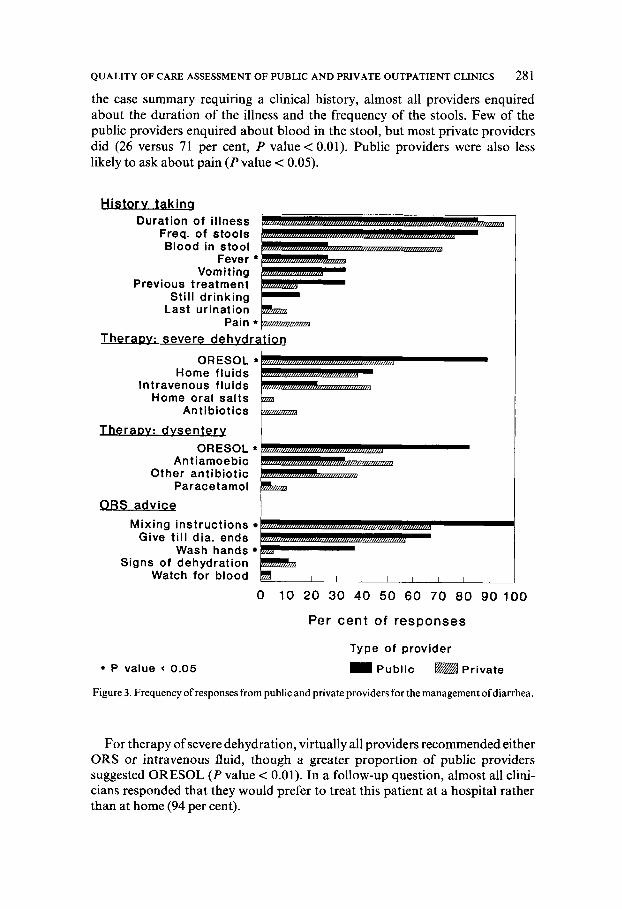
Clinicians were presented with various clinical case summaries involving diar- rhea and asked to indicate how they would manage the case (Figure 3). In
QUALITY OF CARE ASSESSMENT OF PUBLIC AND PRIVATE OUTPATIENT CLINICS 281
the case summary requiring a clinical history, almost all providers enquired about the duration of the illness and the frequency of the stools. Few of the public providers enquired about blood in the stool, but most private providers did (26 versus 71 per cent, P value < 0.01). Public providers were also less likely to ask about pain (P value < 0.05).
Historv tak ing Duration of illness
Freq. of stools Blood in stool
Previous treatment
Last urination
Home fluids Intravenous fluids
Home oral sal ts
T h e r a w : dvsenterv
Antiamoebic Other ant ib iot ic
Paracetamol
ORS advice Mixing instructions
Give till dia. ends Wash hands
Signs of dehydration Watch for blood
P value 0.05
0 10 20 30 40 50 60 70 80 90 100
Per cent of responses
Type of provider = Public @$&! Private
Figure 3. Frequency of responses from public and private providers for the management ofdiarrhea.
For therapy of severe dehydration, virtually all providers recommended either ORS or intravenous fluid, though a greater proportion of public providers suggested ORESOL ( P value < 0.01). In a follow-up question, almost all clini- cians responded that they would prefer to treat this patient at a hospital rather than at home (94 per cent).

282 D. H. PETERS AND S . BECKER
The case presentation of presumptive dysentery evoked diverse responses. Public providers were more likely to provide ORESOL (P value < 0.05), even though no information was given about the state of hydration. An antiamoebic drug was recommended by 42 per cent of all providers, while an antibacterial drug was recommended by 29 per cent of the providers, with no statistically significant difference between public and private providers.
The last case summary inquired about advice to give mothers when providing ORS. All of the public providers responded with instructions for mixing ORS, compared to 62 per cent of the private physicians (P value < 0.001). The duration of oral treatment was also usually mentioned (63 per cent). Thirty seven per cent of public providers also gave advice about personal hygiene, compared to only 5 per cent of private physicians ( P value < 0.01). Advice regarding the need to look for signs of dehydration or dysentery and then to return to the clinic was rarely given.
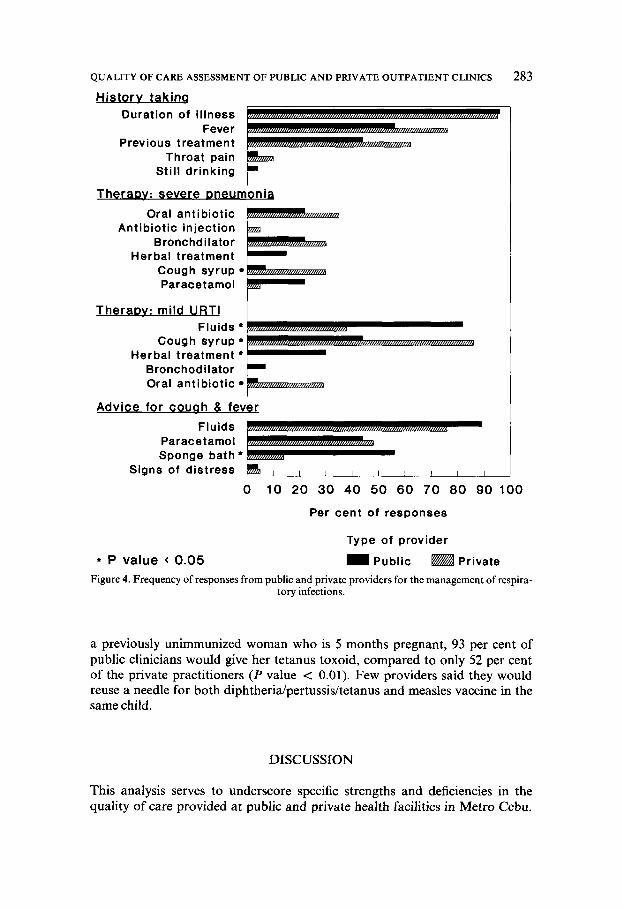
Clinical case summaries involving respiratory disease were also presented and responses elicited (Figure 4). The first case sought questions to ask about a 2-year-old girl who presents with a cough. Nearly all providers asked about the duration of the illness, but only 65 per cent enquired about fever. There was no significant difference found between public and private providers, and other relevant questions were asked less frequently.
Providers were asked to recommend therapy for an infant with signs of severe pneumonia. Remarkably, injectable antibiotics were infrequently sug- gested (< 5 per cent), as were oral antibiotics (31 per cent). Bronchodilators were suggested by 25 per cent of all practitioners. The only difference between public and private providers was that private providers suggested cough syrup more frequently (P value < 0.05). In response to a subsequent question, 88 per cent of all providers stated that they would prefer that this patient be treated in a hospital rather than at home.
For treatment of a child with a mild upper respiratory tract infection, public providers more commonly recommended increased fluids (P value < O.Ol), while private physicians more frequently suggested cough syrup ( P value < 0.01). Only 4 per cent of the public providers suggested an antibiotic, com- pared with 29 per cent of the private providers ( P value < 0.05). Thirty per cent of the public providers suggested a herbal remedy, compared with none of the private doctors (P value < 0.05). All but one public provider suggested that they would prefer to treat this patient at home rather than in a hospital.
For a child with cough and fever, the treatment most frequently recommended to mothers by both types of providers was to give fluids (83 per cent). Paraceta- mol was recommended by almost half of both providers, while sponge baths were commonly mentioned by public providers (56 per cent versus 14 per cent of private providers). Advice about signs of respiratory distress and the need for a revisit was rarely given.
Other differences between public and private clinicians are shown in their clinical decisions about immunizations; 96 per cent of public clinicians would immunize an eligible child with a mild respiratory infection, compared to only 60 per cent of private practitioners (P value < 0.01). When presented with
QUALITY OF CARE ASSESSMENT OF PUBLIC AND PRIVATE OUTPATIENT CLINICS
Historv takinq Duration of illness
Previous treatment
Still drinking
Oral antibiotic Anti biotic injection
Bronchd ilator Herbal treatment
Cough syrup Paracetamol
TheraDv: mild URTl
Cough syrup * Herbal treatment *
Bronchodilator Oral antibiotic
Paracetamol Sponge bath *
Signs of distress
283
0 10 20 30 40 50 60 70 80 90100
Per cent of resDonses
Type of provider
* P value < 0.05 Public ~ Private Figure 4. Frequency of responses from public and private providers for the management of respira-
tory infections.
a previously unimmunized woman who is 5 months pregnant, 93 per cent of public clinicians would give her tetanus toxoid, compared to only 52 per cent of the private practitioners (P value < 0.01). Few providers said they would reuse a needle for both diphtheria/pertussis/tetanus and measles vaccine in the same child.
DISCUSSION
This analysis serves to underscore specific strengths and deficiencies in the quality of care provided at public and private health facilities in Metro Cebu.
284 D. H . PETERS AND S. BECKER
While several general areas of program weakness were known before, the meth- ods used in this study were able to identify specific defects.
For example, managers and providers believed that the interruption of vac- cine supplies and vaccine failures were important problems. Serious flaws in the cold chain were discovered. These problems could be corrected by routine temperature checks, maintenance logs, and directions for backup storage if temperatures cannot be maintained. This is particularly important at the clinics where periodic vaccine shortages have been documented. Observation showed that shortages of needles and syringes resulted in unsafe immunization practices at several clinics, a problem which had previously gone unnoticed. Even if new supplies cannot be obtained, sterilization during the session could be poss- ible, or more reusable, sterilized needles could be brought to the session, and returned later for sterilization.
This study did not identify reasons why particular clinics had vaccine short- ages. At public clinics, supply interruptions occurred at both remote and central facilities. The methods of vaccine ordering and book-keeping at the clinics were not found to be related to shortages of vaccines; the logistics breakdowns occurred at a more central level. However, clinic record-keeping for vaccine stocks was usually absent or inaccurate. Clinics could potentially improve vac- cine supply by replicating the procedures of the few clinics that kept accurate records.
Despite these administrative problems, we found that the vaccinators carried out most tasks for immunizing children very well. The important exceptions were that unsterilized needles were occasionally used, and few mothers were given adequate advice about side-effects and the time for follow-up vaccinations.
The case histories provide useful information about the type of care that is likely to be given by public and private providers. This method is relatively untested, and it is not certain that providers who make good clinical decisions in response to case histories actually deliver better quality of care. Nevertheless, there were large differences in the responses, which probably reflect true differ- ences in clinical knowledge and practice, and suggest specific areas where further training would be useful. Public providers in their responses generally followed government policies about immunizing pregnant women or children with mild respiratory infections, while private physicians were more hesitant. This sug- gests that the training for immunization has produced more consistent results among public providers. On the other hand, private doctors were more likely to inquire about dysentery than the public providers, although both groups of providers commonly used inappropriate antiamoebic therapy instead of anti- bacterial treatment. Public providers more commonly used ORS for diarrhea or dysentery. This is consistent with results from the community survey, which showed that mothers who consulted public providers were more likely to use ORS, and less likely to use ‘liquid’ or ‘tablet’ medicine for diarrhea treatment than mothers who consulted private practitioners (Becker et al., 1991). Future training of public providers should place more emphasis on the diagnosis and treatment of dysentery, while private providers could particularly benefit from information about dispensing oral rehydration therapy.

QUALITY OF CARE ASSESSMENT OF PUBLIC AND PRIVATE OUTPATIENT CLINICS 285
One area of weakness in all the clinics was communication with mothers. Public providers were better at providing health education than private pro- viders: they were more likely to give instructions for mixing oral salts and on hygienic handling of food and excreta. However, few providers informed mothers of the danger signs for dehydration or respiratory distress, and when a child should return to the clinic. Advice about the treatment of fevers and prevention of diarrhea was also inadequate.
The treatment of severe pneumonia is another area where more training is needed. Only a minority of providers suggested an injectable or oral antibiotic for a 1-month-old child with signs of severe pneumonia, although most would appropriately refer the child to a hospital. The low response may be partly explained by the fact that few clinics actually had injectable antibiotics.
This type of survey identifies facilities whose performance deviates from others, thus providing information that is immediately useful to program managers for decision-making based on management by exception (Reinke, 1988). SimilarIy, medical organizations can use the information in assessing the needs for continuing education among their members. When problems are identified, solutions become more readily apparent. For example, those clinics which demonstrated poor diarrhea therapy could receive extra training and supervision in this area. To improve the cold chain, thermometers and tempera- ture logs could be used in clinics that need them. Clinics which are well-run could be used as models for other sites.
The observational methods were simple and produced useful information at the immunization sessions where there were frequent patient interactions. The observers may have influenced the performance of workers at the immuniza- tion sessions, and several authors have suggested that such methods are likely to overestimate quality (Peterson et al., 1956; Donabedian, 1966). However, this was not an important drawback because problems were identified. The observation checklists were easily administered, and could be adapted for use as a routine supervisory tool, though they are not always relevant at the smaller private clinics.
There are limitations to the methods used in this study. The clinical records at private clinics were inadequate for quality assessment, as has been noted in other settings (Peterson et al., 1956). Even in the public clinics, diarrhea was the only diagnostic category where record audits were possible. Although deficiencies were found at some public clinics, it is not easy to separate poor record-keeping from actual problems in the quality of care. However, in a classic study using hospital records, Rosenfeld (1957) showed that poor record- ing was also related to substantive shortfalls in quality of care. At public clinics, workers can be trained and supervised to keep standardized records for diarrhea and respiratory infection treatment, making a record audit more productive.
Quality-assessment methods such as those used in this study can be applied to many primary health-care programs. The methods need to be adapted and tested in a variety of settings. The information derived from such studies can provide efficient means for managers of health services to assess quality of care in order to make meaningful improvements in health services.
286 D. n. PETERS AND s. BECKER
ACKNOWLEDGEMENTS
We thank Fr. Wilhelm Flieger, Josephine Avilla, and the staff of the Office of Population Studies, University of San Carlos, whose enthusiasm and hard work made this study possible. The cooperation of the Philippines Region VII Department of Health, the Cebu Medical Society, and the Philippine Acad- emy of Family Practitioners is also appreciated. Robert Black and Ronald Gray provided valuable advice during all aspects of the research. The work was supported by a grant from the United States Agency for International Development.
REFERENCES
Becker, S., Peters, D.H. (1991). Evaluation of Key Child Survival Activities in Metro Cebu, The Philippines: Results of a Baseline Survey. Baltimore: The Johns Hopkins University Institute for International Programs (JHU/IIP) Occasional Paper Series, No. 13.
Becker, S., Peters, D.H., Logarta, J., Gray, R.H., Black, R.E. (1991). Estimates of availability and use of oral rehydration salts for the treatment of diarrhea in Cebu, The Philippines. To be presented at IUSSP seminar, Cairo, Egypt.
Department of Health. (1988). Annual Report 1988. Regional Health Office No. 7, Department of Health, Republic of the Philippines.
Donabedian, A. (1966). Evaluating the quality of medical care. Milbank Memorial Fund Quarterly, 44 (2), 166203.
Donabedian, A. (1969). A Guide to Medical Care Administratiorr, vol. 2: Medical Care Appraisal-Quality and Utilization. New York: American Public Health Association.
Fleiss, J.L. (1981). Statistical Methods for Rates and Proportions. New York: John Wiley and Sons.
Garner, P., Thomason, J., Donaldson, D. (1990). Quality assessment of health facilities in rural Papua New Guinea. Health Policy and Planning, 5,49-5 1.
Peterson, O.L., Andrews, L.P., et al. (1956). An analytical study of North Carolina general practice 1953-1954. Journal of Medical Education 31 (2), 1-165.
Reinke, W.A. (1988). Health Planning for Effective Management. New York: Oxford University Press, pp. 41-53.
Rosenfeld, L.S. (1957). Quality of medical care in hospitals. American Journal of Public Health, 47,856865.
Shaikh, J. (Ed.) (1988). Primary Health Care Thesaurus: A List of Service and Support Indicators (volume 2) . Bethesda: Center for Human Services, Primary Health Care Operations Research.
Van Norren, B., Boerma, J.T., Sempebwa, E.K.N. (1989). Simplifying the evaluation of primary health care programmes. Social Science and Medicine 28, 1091-1097.
Walker, G.J.A., Ashley, D.E.C., Hayes, R.J. (1988). The quality of care is related to death rates: Hospital inpatient management of infants with acute gastroenteritis in Jamaica. American Journal of Public Health 78, 149-152.
Wolff, M.C., Black, R.E. (1989). Manual for Conducting Lot Quality Assessments in Oral Rehydration Therapy Clinics. Baltimore: The Johns Hopkins University Institute for International Programs (JHU/IIP) Occasional Paper Series, No. 9.
World Health Organization. (1989). The Treatment and Prevention of Acute Diarrhoea: Practical Guidelines. Geneva: World Health Organization.








![Merdeka Generation Benefit #3 [English] - Gov.sg 3_eng.pdf · care through 3 Healthcare Touchpoints – CHAS GP and dental clinics, polyclinics, and public Specialist Outpatient Clinics](https://img.pdfslide.net/doc/110x75/60e4cbc3f1a7e21a7d0a8593/merdeka-generation-benefit-3-english-govsg-3engpdf-care-through-3-healthcare.jpg)



















