Embed Size (px)
Citation preview

Radiographic techniques Radiographic techniques
R.Hemalatha1st year
Dept. Of Pedodontcs and Preventive Dentistry

Contents…Contents…1. Introduction2. Parts of X-ray tube3. Projection Geometry• Principles of projection geometry• Terms• Focal spot• Magnification• Distortion• Heel effect3. Intra oral radiographs• Periapical radiography
1. Paralleling technique2. Bisecting angle technique
• Bite wing radiography• Occlusal radiography

• Placement of the film in children and its management
• Full mouth radiography• Object localisation technique• Radiographic faults4. Extraoral techniques• Lateral cephalometric projections• Submentovertex projections • Waters• Posteroanterior cephalometric• Reverse-towne projections5. Digital radiography and advanced
imaging techiques6.Effects of dental radiographs in oral cavity7.Radiation protection8. Conclusion 9.Refrences
Contents…

IntroductionIntroduction
• Radiograph is a 2D image of a 3D object.• A good radiograph is required for use as a
good diagnostic aid.• Principles of projection geometry teach us
how to reach perfection during radiography.
• The intraoral radiograph, when correlated with the case history and clinical examination, is one of the most important diagnostic aids to the dental practitioner.

Parts of X-Ray Parts of X-Ray
An X-ray tube is a vacuum tube that produces X-rays. They are used in X ray machines. X-rays are part of the electromagnetic spectrum, an ionizing radiation with wavelengths shorter than ultraviolet light.

• As with any vacuum tube, there is a cathode, which emits electrons into the vacuum and an anode to collect the electrons, thus establishing a flow of electrical current, known as the beam, through the tube.
• A high voltage power source is connected across cathode and anode to accelerate the electrons.
• The X-Ray spectrum depends on the anode material and the accelerating voltage.
• Electrons from the cathode collide with the anode material, usually tungsten, molybdenum or copper, and accelerate other electrons, ions and nuclei within the anode material.
• About 1% of the energy generated is emitted/radiated, perpendicular, rest of the energy is released as heat.

• tungsten will be deposited from the target onto the interior surface of the tube, including the glass surface.
• The arc will jump from the cathode to the tungsten deposit, and then to the anode. This arcing causes an effect called "crazing" on the interior glass of the X-ray window, tube becomes unstable even at lower voltages, and must be replaced.
• The X-ray photon-generating effect is generally called the Bremsstrahlung effect.
• emitted X-ray photons, or dose, are adjusted by controlling the current flow and exposure time (high voltage controls X-ray penetration, and thus the contrast of the image and tube current and exposure time affect the dose and darkness of the image.
• Aluminum filters are installed in the path of the X-ray beam to remove "soft" (non-penetrating) radiation.

• Fundamentals of radiography are-
Central beam should pass through the area to be examined.
The x-ray film should be placed in position so as to record the image with the least amount of image distortion

Principles of Projection Geometry…
Principles of Projection Geometry…
Object and Film should be in contact or as close together as possible.
Object and film should be parallel to one another.
X-ray tube head should be positioned that, beam meets both the object and film at right angles.

“Terms and conditions apply”
“Terms and conditions apply”
• Image sharpness-The ability of a radiograph to reveal the boundary between two areas of different radiodensity; or to define an edge precisely.
• Image spatial resolution-Ability of a radiograph to reveal small objects that are close together.Line pairs per mm.
OPG- 5line pairs/mm.IOPAR- 20line pairs/mm.


• Image size distortion-It is the increase in size of the image on the radiograph compared with the actual size of the object.

• Image shape distortion-It is the unequal magnification of different parts of the same object on a single radiograph.

For a good radiograph…For a good radiograph…

Focal spotFocal spot
• Actual focal spot size= 1x3mm.• Effective focal spot size= 1x1mm.
• Size of the EFS- Angulation of the anode target to the long axis of the incident electron beam from the cathode.
• Ideal angle= 10-20o
• Smaller effective focal spot size, increased image sharpness and resolution.

• Dec. heat production
• Inc. X-ray tube life
• Dec. sharpness and resolution
• Dec. clarity• Inc.
“geometric unsharpness”
• Inc. heat production
• Dec. X-ray tube life
• Inc. sharpness and resolution
• Inc. clarity

Umbra and PenumbraUmbra and Penumbra
Fuzzy edge- Geometric Unsharpness
To have sharp edge of image:• Longer
“a”• Reduced
“b”• Smaller
EFS
BLURRING


MagnificationMagnification
• Formula= Size of the image = Focal spot to film distance Size of the object Focal spot to object distance
• When an image is magnified, the shape is maintained because every dimension of the object is magnified to the same extent, provided the object is placed parallel to the film.

Use large FS to object distance
Use small object to film distance

DistortionDistortion• Results from unequal
magnification of different parts of the same object.
• When not all the parts of the object are at the same FS to object distance.
Position the film parallel to the object.
Orient the central ray perpendicular to the film and the object.

ForeshorteningRay perpendicular to the film but not the object
ElongationRay perpendicular to the object but not the film

Heel effectHeel effect• Intensity of x-rays are not uniform over the area irradiated.• Due to the electrons having to travel more through the anode, less energy and intensity beam is seen towards the anode than towards the cathode , photons get absorbed by the target anode it self..
Biobrain article

Increases with increas
e in anode angle steepn
ess
Increases with increase in
roughness of the anode
Decreases with increase in focal
spot to film distance
Decreases with
decrease in film sizeHeel Effect

INTRA ORAL
RADIOGRAPHS
Periapical radiograp
hs
Bite wing radiograp
hs
Occlusal radiograp
hs

Intra Oral Periapical Radiography…
Intra Oral Periapical Radiography…
• Includes the teeth and the tissues around the apices.
• Uses- • Detection of apical infection/
inflammation.• Assessment of periodontal status• Assessment of an unerupted tooth• Assessment of root morphology• Evaluate position and prognosis of
implants

• Ideal positioning requirements-• Tooth and film should be as close to each
other as possible.• Tooth and film should be parallel to each
other.• The film is positioned with its long axis
vertical for anterior teeth and horizontal for posterior teeth.
• Beam must be directed at 90o to both the teeth and the film.
• Positioning must be reproducible.

Placement of the film…Placement of the film…
• The white side of the film always faces the teeth.
• Anterior films are always placed vertically.
• Posterior films are always placed horizontally.
• The identification dot on the film is always made to face the operator and on the occlusal end of the radiograph.
• The film is always centred over the areas to be examined.
• Ideally 2mm of the alveolar bone must be seen periapically.

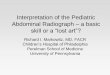
Landmarks used…Landmarks used…
Inner canthusPupil
Outer canthus
Occlusal Plane

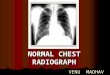
Paralleling TechniqueParalleling Technique• C. Edmund Kells in 1896 • developed by Gordon M.
Fitzgerald in 1947.• Used by Franklin W.
McCormack in practical dental radiography.
• It was so named because the object (tooth), receptor (film packet), and end of the position indicating device (PID) are all kept on parallel planes.

• Long axis of the tooth is parallel to long axis of the film• Central ray at 90o to both.• Film holder and x-ray tube head positions can be reproduced.• Film placed at same distance away from the tooth.• Long open ended aiming cylinder
Long con techRight Angled tech
PRINCIPLEThe image sharpness is primarily affected by the distance from the focal spot within the tube head and the film, object-film distance, motion, and the effective focal spot size of the x-ray tube.
Dentomaxillofacial Radiology (2011) 40, 385-389The British Institute of Rdiology


• Projection method-• Maxillary projections, superior border
of the film placed at the height of the palatal vault.
• Mandibular projections, inferior border of the film placed on the floor of the mouth.
• Vertical angulation- 90o
• Horizontal angulation- 0o
Now more commonly used method

• Film holders- • Rinn XCP, Rinn stabe film holders,
Precision film holders, EEZEE grip film holders.
• Most preferred is Rinn XCP film holder• Parts- Plastic ring and plastic bite block,
metal indicator arms, addable ring collimators.

DIS
AD
VA
NTA
GES
AD
VA
NTA
GES-Accuracy,
minimal distortion-Simplicity-Duplication is possible due to standardisation-Periodontal bone levels are well depicted.-Angulations and positions are reproducible.-The technique reduces the risk of cone cuts.
-Film placement in children or small mouths or shallow palate is difficult.-Discomfort-Apices of the teeth may appear close to the edge of the film.-Film holder needs autoclaving.

• Developed by Weston Price in 1904.
Bisecting Angle Technique
PRINCIPLE- When the rule of isometry is used, the length of the tooth is equal to the length of the image on the radiograph.

Ciezynski’s rule of isometry
Multirooted teeth- Angled differently for each root

• Projection method-• For maxillary projections- Patient’s head
must be upright, with the sagittal plane vertical and the occlusal plane horizontal.
• For mandibular projections- Head is tilted back slightly.

+400 +450
+300
+200

-150 -200
-100
-50

• Size of Intraoral films• Size 0 (22x35mm) used for bitewing and
periapical radiographs of small children• Size 1 (24x40mm) used for radiographing anterior
teeth in adults.• Size 2 (31x41mm) used for anterior occlusal
radiograph,periapical radiograph and bitewing survey in mixed and permanent dentition.
• Occlusal films have a size of 57x76 mm and are taken for viewing entire maxillary and mandibular arches

DIS
AD
VA
NTA
GES
AD
VA
NTA
GES- Can be used
without a film holder.- Decreased exposure time.- Positioning of the film is relatively more comfortable to the patient in all areas of the mouth.
- Image distortion.- Angulation problems.- Unnecessary
exposure.- Shadow of
the zygomatic bone is frequently seen over the apex of the maxillary molars.
- Difficulty in angulation.
- Not reproducible.

Comparison of Parelleling technique and bisecting angle
technique
Comparison of Parelleling technique and bisecting angle
technique

Bite wing radiographs…Bite wing radiographs…• Also called as the INTERPROXIMAL
TECHNIQUE.• Developed by Howard Riley Raper in 1925.• Shows crowns of maxillary and mandibular
teeth, interproximal areas, and areas of crestal bone on the same radiograph.
• Name originated as the patient bites on the wing to stabilize the film.

• Uses-• Checking the
interproximal areas of teeth
• Checking the alveolar bone on the radiograph.
• Caries in deciduous and transitional dentiton phase
AAAPD guideline for prescribing dental radiographs,2012

• Vertical angulation- recommended angulation of +10o. Used to
compensate for slight bend of the upper portion of the film and tilt
of maxillary teeth.• Horizontal angulation- central ray
is directed perpendicular to the curvature of the arch and through the contact areas.
• Vertical bite wings are used to visualise the level of the alveolar bone, normally used as post treatment films after periodontal treatment.

Occlusal radiograph…Occlusal radiograph…
• Occlusal radiography is defined as those intraoral radiographic techniques taken using a dental X-ray set where the film packet (5.7 x 7.6 cm) or a small intraoral cassette is placed in the occlusal plane.
USESI. To precisely locate roots, supernumerary,
unerupted & impacted teeth.II. To localize foreign bodies in the jaw & stones in the
duct of sublingual & submandibular gland duct.
III. Another use-- To demonstrate & evaluate the integrity of anterior, medial & lateral outlines of maxillary sinus.
IV. To obtain information about location, nature, extent & displacement of fractures of mandible & maxilla.
v Patients with reduced mouth openingvi. Cleft palate cases

i. Topographic projectionsShows anterior part of maxilla or mandible and the anterior teeth.The cone is placed between the eye brows on the bridge of the nose.
Maxillary and Mandibular Occlusal Projections

i. Topographic projectionsShows anterior part of maxilla or mandible and the anterior teeth.
Mandibular Occlusal Projections

• ii. Vertex projectionShows the entire teeth present in the arch.

ii. Vertex Mandibular projection ( cross sectional projection)
ii. Vertex Mandibular projection ( cross sectional projection)

iii. Posterior Lateral projectionShows the posterior part of the maxilla and the upper posterior teeth on one side.
iv. Pediatric projectionShows the anterior part of the maxilla, used in children of 5years age or younger.

• iii. Posterior Oblique Mandibular Occlusal projection

• Positioning the Radiograph• Positioning the radiograph vertically in the mouth for
both periapical and bitewing radiographs reduces the distal extension of the radiograph and may result in greater tolerance by patients, especially those with a mild gag reflex.
• The vertical bitewing radiograph provides greater detail of the periapical area.

Primary dentition (3 to 6 years)Primary dentition (3 to 6 years)
Maxillary anterior occlusal projection• Place no. 2 film with its long axis perpendicular to the
sagittal plane and the pebbled surface towards maxillary teeth.
• Direct the central ray at a vertical angulation of +60 degrees through the tip of the nose towards the center of the film
Mandibular anterior occlusal projection • Seat the child with the head tipped back so that the
occlusal plane is about 25 degrees above the plane of the floor.
• Place a no. 2 film with the long axis perpendicular to the sagital plane and the pebbled surface towards the mandibular teeth.
• Orient the central ray at -30 degrees vertical angulation and through the tip of the chin towards the film.

Bitewing projection• Use no. 0 film with paper loop holder.• Place the film in the child’s mouth as in the adult
premolar bitewing projection.• The image field should include the distal half
ofthe canine and the deciduous molars.• Positive vertical angulation of +5 to +10 degrees.
Decidious maxillary molar periapical projection• Use no. 0 film , Position the film in the midline of
the palate with anterior border extending to the maxillary primary canine.
• The image field should include the distal half of the primary canine and both primary molars

• Deciduous mandibular molar projectionProjection a no. 0 filmThe exposed radiograph should show the distal half of the mandibular primary canine and the primary molar teeth.
• Mixed dentition(7 to 12 years) Maxillary anterior periapical projection Center a no.1 film on the embrasure between the
central incisors in the mouth behind the maxillary central
and lateral incisors.Center the film on the midline.

• Mandibular anterior periapcal projectionPosition no.1 film behind the mandibular central and lateral incisors
• Canine periapical projection Position no. 1 film behind each of the canines. Decidious and permanent molar periapical projection Position no.1 or no. 2 film with anterior edge behind the canine
• Posterior bitewing projection Use no.1 or no. 2 films as previously describedExpose four bitewings projections when the second permanent molars have erupted

• Probable Technical Errors1. Improper placements of films.2. Cone cutting3. Incorrect horizontal angulations4. Incorrect vertical angulations5. Over exposure due to defective devices.6. A high exposure of the patient to radiation
because of repetition of taking X-rays due to an uncooperative child.

Radiation hygiene measures
Radiation hygiene measures
• Proper registration and maintenance of radiographic units.
• Training of personnel who are associated with radiography
• Dosage monitoring• Radiation protection of the child patients by using lead
apron with thyroid collar.• Use of long lead-lined cylinder and cone positioning
devices• Use of electronically controlled exposure timer• Use of high speed films• Use of automatic processing machines that give good
consistent result• Employing proper technique to avoid the chances of
repeating exposure

• The Snap-A-Ray is also useful for those patients that have a fear of swallowing the radiograph.
• By biting on the large positioning device and watching in a mirror they are assured they will not swallow the radiograph
A self sticking sponge tab may also reduce impingement ofthe radiograph on the intraoral soft tissue.For patients frightened of the procedure itself,desensitization techniques may be necessary to gain the patient cooperation

Desensitization Techniques
Desensitization Techniques
• Desensitization is defined as gradually exposing the child to new stimuli or experiences of increasing intensity.
• An example of this is introducing the patient to x-rays by initially taking an anterior radiograph which is easier to tolerate than a posterior radiograph.
“Lollipop Radiograph Technique.”The child is given a lollipop to lick (preferably sugarless).
• After a few licks, the lollipop is taken from the child and a radiograph is attached to the lollipop using an orthodontic rubber band.
• The lollipop with the attached film is returnedto the child, who is told to lick the lollipop again.
• After a few licks, the child is told to hold the lollipop in his mouth while we take a tooth picture.The exposure is made

Procuring Posterior RadiographsProcuring Posterior Radiographs
• Procuring posterior radiographs can be made more pleasant by associating it with a pleasurable taste….bubble gum.
• Before placing the radiograph in the patient’s mouth apply bubble gum flavored toothpaste to the film.
• The child will be more accepting of the radiograph

Gag reflex Gag reflex • Some patients, young and old, have an
exaggerated gag reflex.• The etiology of an exaggerated gag reflex had
been attributed to psychological and physical factors.
• The easiest is through diversion and positive suggestion.
• The operator suggests to the patient the gag reflex can be reduced by concentrating on something other than the procedure.
• The patient’s palate can be sprayed with a topical anesthetic to reduce the sensation of the radiograph on the palate and tongue.
• An alternative is the use of nitrous oxide analgesia

• Another alternative is to place the radiograph in such a manner to not come in contact with the palate or tongue.
• This is accomplished by either extraoral placement of the film or placing the film between the cheek and the tooth and exposing the film from the opposite jaw.
• The film side of the packet (the solid color side) is facing the buccal surface of the tooth
• The x-ray head is placed at the opposing side, and the coneis positioned under the angle of the ramus on the opposite side.
• As the x-ray beam is traveling a longer distance to the film than in the typical positioning, it is necessary to double the exposure time.
• It is imperative that after mounting radiographs are Reversed.
• Incorrect mounting and labeling of the reverse radiograph can result in misdiagnosis and treatment of the wrong tooth
Newman and Friedman Extraoral Radiographic Technique
Newman M, Friedman, S. Extraoral Radiographic Technique: An Alternative Approach. Journal Of Endodontics 2003;29:419-421


• Eshagali Saberi, Ladan Hafezi, Narges Farhadmolashahi, Manoochehr Mokhtari
Modified Newman and Friedman Extraoral Radiographic Technique
The patient sitting upright and the Frankfort plane being
horizontal to the floor and when the head was tilted 10 degrees
toward the side being examined.
For the upper posterior teeth the center of the image
receptor was placed on the intersection of the ala-tragus
and a parasagittal line while the upper border of receptor was parallel to the canthomeatal
line.
The cone was positioned a negative 25 degrees from the
horizontal plane.

Modified Newman and Friedman Extraoral Radiographic Technique
The central beam was directed from midway between
maxillary and mandibular
premolars and molars of the
opposite side..
For the lower posterior teeth, the receptor was placed against the cheek
on the side of interest and its
lower border was parallel and 2 cm above the inferior
border of the mandible
The cone was angled -20 degrees from the horizontal
plane while the central beam was directed towards the mandibular molar-premolar
region.
Saberi1, Hafezi L, Farhadmolashahi1 N, Mokhtari M. Modified Newman And Friedman Extraoral Radiographic Technique


Type of encounter Child with primary dentition (prior erruption of 1st molar)
Child withTransitional Dentition(after eruption of firstpermanent tooth)
Adolescent withPermanent Dentition(prior to eruption ofthird molars)
New patient* being evaluated for dental diseases and dental development
Individualizedradiographic examconsisting of selectedperiapical/occlusalviews and/or posteriorbitewings if proximalsurfaces cannot bevisualized or probed.Patients withoutevidence of disease andwith open proximalcontacts may notrequire a radiographicexam at this time.
Individualizedradiographic examconsisting of posteriorbitewings withpanoramic exam orposterior bitewings andselected periapicalimages.
Individualized radiographic exam consisting of
posterior bitewings with panoramic exam orposterior bitewings and selected periapical images. A full mouth intraoral radiographic exam ispreferred when the patient has clinical evidence of generalized dental disease or a history of extensive dental treatment.
Recall patient* with clinical caries or at increased risk for caries**
Posterior bitewing exam at 6-12 month intervals if proximal surfaces cannot be examined visually or with a probe..
Recall patient* with no clinical caries and not at increased risk for caries
Posterior bitewing exam at 12-24 month intervalsif proximal surfaces cannot be examined visuallyor with a probe
Posterior bitewingexam at 18-36 monthintervals.
Recall patient* with periodontal disease
Clinical judgment as to the need for and type of radiographic images for the evaluation of periodontal disease. Imaging may consist of, but is not limited to, selected bitewing and/or periapical images of areas where periodontal disease (other than nonspecific gingivitis) can be identified clinically.

Type of Encounter Child with PrimaryDentition (prior to eruption of first permanent tooth)
Child withTransitional Dentition(after eruption of firstpermanent tooth
Adolescent withPermanent Dentition(prior to eruption ofthird molar
Patient for monitoring of growth and development
Clinical judgment as to need for and type ofradiographic images for evaluation and/ormonitoring of dentofacial growth and development.
Clinical judgment as toneed for and type ofradiographic images for evaluation and/ormonitoring ofdentofacial growth and development.Panoramic or periapicalexam to assessdeveloping third molars
Patient with other circumstances including, but not limited to, proposed or existing implants, pathology, restorative/endodontic needs, treated periodontal disease and caries
Clinical judgment as to need for and type of radiographic images for evaluation and/or monitoring in these circumstances

• Large or deep restorations• Malposed or clinically
impacted teeth• Mobilty of teeth• Sinus tract/ fistula• Clinically suspected sinus
pathology• Oral involvement in known
or suspected systemic disease
• Unxplained bleeding, sensistivity of tooth,
• Unusual erruption,spacing or migration of teeth, tooth morphology, calcification or colour, absence of teeth
• Clinical erosion• High level fo caries
experience• h/o of reccurent caries• High titre of cariogenic
titre• Exsisting restoration of
poor quality
AMERICAN ACADEMY OF PEDIATRIC DENTISTRY-2012
• Poor oral hygiene• Inadequate fluoride exposureft in
diet• Poor family dental health• developmentrequentl high sucrose
content• Prolonged nursing bottle or breast
feeding• developmental or acquired enamel
defects• Developmental or acquired
disability• Xerostomia• Genetic abnormality of teeth• Many multisurface restorations• Chemo/radiation therapy• Eating disorders• Drug/alcohol abuse• Irregular dental care
Indications for pediatric radiographs

Radiographic SurveysRadiographic Surveys
• The three most common series of radiographs taken in the dental office are
• Bitewing Surveys- consist of a premolar view and a molar view for each side of the mouth taken in occlusion (2 or 4 films) taken to examine the contact areas of the premolar and molar regions, and periapicals for the other teeth and edentulous areas.
• Full Mouth Surveys - series of x-rays that properly represent every tooth in the patient's mouth (with 3 to 4 millimeters of surrounding bone) and all other tooth bearing areas of the mouth even if edentulous
• panoramic film.

Full Mouth RadiographsFull Mouth Radiographs
Permanent Dentition
22 total=18 IOPA + 4 Bite wings

Mixed Dentition12= 10 IOPA+2 bite wings

Deciduous Dentition
8 film= 6 IOPA + 2 Bitewings

Object localisation techniques…
Object localisation techniques…
• To determine the location of a foreign object or an impacted tooth in the jaw.
• Two methods are used for localizing the object;
• Perpendicular technique-• Used to localize an object in or about the maxilla
or mandible in three dimensions.• In clinical practice the position of an object on
each radiograph is noted relative to anatomic landmarks.
• The right angle or cross section technique is best in mandible
• An IOPAR and an occlusal radiograph are used.

B. Tube shift technique (SLOB Method)This method is also known as “buccal object rule”
or “Clark’s rule”(1910)Rationale for this technique derives from the
manner in which the relative positions of radiographic images of two separate objects change when projection angle at which the images are made is change.
Two radiographs are taken with different horizontal angulations.

Radiographic Faults…Radiographic Faults…

Quality Assessment…Quality Assessment…• Depends on-• X-Ray equipment• Focusing• Image processing• Patient• Operator and radiographic technique.
• If radiograph quality is poor, diagnostic information is lost.

i. Light radiographsi. Light radiographsUnderexposure-• Insufficient
milliamperage• Insufficient peak
kilovoltage• Insufficient exposure
time• FS- Film distance to
much• Film packet reversed
Processing errors-• Underdevelopment
(Low temp, short time)
• Depleted developer solution
• Diluted or contaminated developer
• Excessive fixation

ii. Dark radiographsii. Dark radiographsOverexposure-• Excessive
milliamperage• Excessive peak
kilovoltage• Excessive exposure
time• FS- Film distance to
short
Processing errors-• Overdevelopment
(high temp, long time)
• Developer concentration high
• Inadequate fixation• Improper safe
lighting• Accidental exposure
to light

iii. Insufficient contrastiii. Insufficient contrast
• Underdevelopment
• Underexposure• Excessive peak
kilovoltage• Excessive film
fogiv. Film Fog• Improper safe
lighting• Light leaks• Over development• Contaminated
solutions• Deteriorated films

Light fog
Radiation fog
Chemical fog
Deterioration of the film
• Light leaks• Turning on the
overhead white light too soon
• Improper storage
• Insufficient protection• Developer
temperature too high
• Overdevelopment
• Temperature of storage area too high
• Too high humidity

v. Dark spots or linev. Dark spots or line
• Finger print contamination
• Black wrapping paper sticking to the film
• Film in contact with tank or another film during fixing
• Film contaminated with developer before developing
• Excessive bending• Static charge to film
before processing• Excessive roller
pressure or dirty rollers

vii. Light spotsvii. Light spots
• Film contaminated with fixer before processing
• Film in contact with tank or another film during development
• Excessive bending of the film

viii. Yellow or Brown stainsviii. Yellow or Brown stains
• Depleted developer
• Depleted fixer
• Insufficient washing
• Contaminated solutions

ix. Herring bone or tire track appearence
ix. Herring bone or tire track appearence
• Placement of the film backwards, with the lead foil facing the x-ray tube.

x. Blurringx. Blurring
Head restShort exposure time
Motion blurring
Slow speed filmsFiner grain sizeClose contact between film and screen
Image receptor blurring
Wet film viewing avoidedIntensifying screens
Geometric blurring
Parallax
Double exposure

xi. Partial imagesxi. Partial images
• Top of the film not immersed in the developing solution
• Misalignment of the x-ray tube head (Cone cut).

x. Emulsion peelx. Emulsion peel
Incorrect positioning of the x-ray tube head
Incorrect placement of the film packet
Foreshortening Reverse placement
Elongation Double exposure
Overlapping
Cone cut
• Abrasion of the film during processing.
• Excessive time in wash water.
• Improper handling of the film.
xi. Typical positioning faults

Overlapping crown regions due to faulty horizontal angulation of the tube head.
Double exposure of the same film.

EXTRA ORAL TECHNIQUESEXTRA ORAL TECHNIQUES

• Extraoral radiograph are examination made of
the head and facial region using films located
outside the mouth.
• They are taken when large areas of the skull or
jaw must be examined or when patients are
unable to open their mouths for film placement
and areas not fully covered by IOPA.• Images are not as defined or sharp as intraoral
films.

Extraoral radiographs can be used alone or in conjunction with intra oral radiographs.
Except for the panoramic radiographs, extraoral radiographs are not frequently used by General
practitioners.
Major users are orthodontistic, prosthodontic and oral surgeries

Purpose and use of extraoral radiographs
Purpose and use of extraoral radiographs
Examine large areas of the jaws
and Skull.
Cervical spine for diseases
Detect fractures and evaluate
trauma
Study growth and development of bone and teeth
Detect pathological lesions and
Diseases of the jaws.
Detect and evaluate
impacted teeth.
Evaluate TMJ Disorders.

Many film positions and techniques require …..special equipment's and …a sound knowledge of the anatomical
structures through which the radiation beam is directed.
…produced with conventional dental x-ray machines, certain models
of panoramic machines or higher capacity medical x-ray units.
TECHNIQUE
Cassette, Films, Intensifying Screens . grids

Image receptor
• Cephalometric and skull views - 20x25cm (8x10 inch) image receptor.
• Lateral oblique projections of the mandible - 13x18cm (5x7 inch) image receptor.
• Panoramic views - 12.7x30.5cm (5x12 inch) or 15x30cm (6x12 inch)image receptor.

It is critical to correctly and clearly label the right and left sides of the image.
It is done by placing a metal marker of R or L on the outside
of the cassette in a corner in which the marker does not obstruct diagnostic information.
The proper exposure parameters depend on the patient’s size, anatomy and head orientation,image receptor speeds,x-ray source to receptor distance and the use of grids.
3 to 4 sec
65 Kvp
10 mA

The main anatomical landmark used in
patient positioning is the
CANTHOMEATAL LINE.
The canthomeatal line forms approximately a 10-degree angle with
the FRANKFORT PLANE.
REFERENCE PLANES

Lateral cephalometric projection of the
sagittal or median plane.
Submentovertex projection of the
transverse or horizontal plane.
Water’s of the coronal or frontal plane.
Posteroanterior cephalometric
projection of the coronal or frontal
plane.
Reverse-Towne projection of the coronal or frontal
plane.
Lateral oblique projection of the
mandibular body and ramus.
Temperomandibular joint projections
Newman and Friedman Technique
Orthopantomography
VARIOUS EXTRA ORAL RADIOGRAPHIC TECHNIQUES ARE:

Frontal (Posteroanterior)
Lateral skull projections.
Cephalometric means measurements of the head.
Either conventional x-ray machines modified for Cephalometric work or special units are needed
Cephalometric Radiographs

It shows the entire
skull from the side
INDICATIONS
LATERAL SKULL PROJECTION
(LATERAL CEPHALOMETRIC PROJECTION)
•Measure and compare changes in Growth and development of
bone and the teeth through pre & progress and post treatment
records.
Facial soft tissue profile of the face
1. The contour of the lips and the face.
2. The relation ship of the teeth before removal, this will helps to construct prosthetic appliances that look natural.
•Evaluate trauma.•To determine the location and extent of fractures.•Malignancies.•injuries to TMJ

Image receptor and patient placement
The image receptor is positioned parallel to the
patient’s midsagittal plane
The site of interest is placed towards
the image receptors to minimize distortion
The patient is placed with the left
side towards the image receptor
A wedge filter at the tube head is
positioned over the anterior aspect of
the beam to absorb some of the
radiation and to allow visualization of soft tissues of the
face.
LATERAL SKULL PROJECTION (LATERAL CEPHALOMETRIC PROJECTION)

Position of the central x-ray beam
The central beam is perpendicular to the midsagittal plane of the patient and
the plane of the image receptor and is central over the external auditory
meatus

Cephalostats have ear rods that stabilizes the patient’s head parallel to the film and at right angle to the direction of the beam
The Cephalometer allows the exposure to be taken several times for the same patient in the same head position

5 feet
X-ray source
Cephalostat
Film
• For cephalometric applications the distance should be 152.4 cm (60 inches) between the x-ray source and the midcoronal plane.
• This increased distance provides an resultant image with a broader gray scale of the patient.

Resultant image Exact
superimposition of
right and left sides
is impossible
because
structures on the
side near the
image receptor
are magnified less
than the same
structure on the
side far from the
image receptor.
Bilateral structures close to the
midsagittal plane demonstrate
less discrepancy in size
compared with bilateral
structures farther away from the
midsagittal plane.
Structures close to
the midsagittal
plane (e.g., the
clinoid processes
and inferior
turbinate's) should
be nearly
superimposed.

USES
• Asymmetry• Trauma• Developmental
abnormalities• Fractures of skull
vault• Investigation of
frontal sinus• Conditions
affecting cranium( Paget's disease, multiple myeloma, hyperparathyroidism.)
• Intracranial calcification
Posteroanterior (PA) cephalometric projection
Shows the entire skull in a Posteroanterior plane.
The beam passes through the skull in a posterior to anterior direction.

• The image receptor is placed in front of the patient, perpendicular to the midsagittal plane and parallel to the coronal plane.
• The patient is positioned so that the canthomeatal line forms a 10-degree angle with the horizontal plane and the frankfort plane is perpendicular to the image receptor.

The central beam is perpendicular to the image receptor, directed from the posterior to the anterior (hence the name postero-anterior) parallel to patient’s midsagittal plane and is centred at the level of the bridge of the nose

The midsagittal plane should divide the skull into two symmetric halves.
The superior border of the petrous ridge should lie in the lower third of the orbit.
Resultant image

To Evaluate the maxillary, frontal and
ethmoid sinuses..
Detecting the lefort’s fractures, zygomatic-
complex, naso-ethmoidal fractures, orbital blow out
fractures.
Water’s view projection
Also known as sinus projection.
It’s similar to the postero-anterior projection except that the center of interest is focused on the middle third of the face.

The image receptor is placed in front of the
patient and perpendicular to the midsagittal plane..
The patient’s head is tilted upwards so that the canthomeatal line forms a 37-degree angle with the
image receptor.
If the patient’s mouth is open, the sphenoid sinus
will be seen superimposed over the
palate.
The central beam is perpendicular to the image receptor and centered in the
area of the maxillary sinuses.
technique

The midsagittal plane should divide the skull image in to two symmetrical halves.
The petrous ridge of the temporal bone should be projected below the floor of the maxillary sinus
Resultant image

To examine fractures of the condylar neck of the mandible.
Intracapsular fractures of the TMJ.
Condylar hyperplasia or hypoplasia.
Reverse –towne (open mouth) projection
Purpose:

The image receptor is placed in front of the patient, perpendicular to the
midsagittal and parallel to the coronal plane.
The patient’s head is tilted downward so that the
canthomeatal line forms a 25 to 30-degree angle with the
image receptor.
To improve the visualization of the condyles, the patient’s mouth is opened so that the condylar heads are located
inferior to the articular eminence.
The central beam is perpendicular to the image
receptor and parallel to patient’s midsagittal plane and it is centered at the level of the
condyles.
technique

Resultant image
The midsagittal plane (imaginary line extending from the middle of the foramen magnum and the posterior arch of the atlas through the middle of the bridge of the nose and the nasal septum) should divide the skull image into two symmetric halves.
The petrous ridge of the temporal bone should be superimposed at the inferior part of the occipital bone and the condylar heads should be projected inferior to the articular eminence.

the base of the skull.
Sphenoid sinus
The position and orientation of the condyles
Fractures of the Zygomatic arch.
Submentovertex (base) projection
Purpose: Used to show

The image receptor is positioned parallel to patient’s
transverse plane and perpendicular to the midsagittal
and coronal plane.
To achieve this, the patient’s neck is extended as far
backward as possible with the canthomeatal line forming a 10-
degree angle with the image receptor.
The central beam is perpendicular to the image receptor, directed from below the mandible towards the
vertex of the skull (hence the name) and centred about 2cm anterior to a
line connecting the right and left condyles.
technique

The buccal and lingual cortical plates of the mandible should be projected as uniform opaque lines.
An underexposed view is required for the evaluation of the zygomatic arches because they will be over exposed or “burned out” on radiography obtained with normal exposure factors.
Resultant image
The midsagittal plane should divide the skull image into two symmetrical halves.

Mandibular body
projection.
Mandibular ramus
projection
Lateral jaw (lateral oblique) projection
It has been largely replacead by panoramic radiographs but still taken when image details is needed.
Two types

To Examine the posterior region of
the mandible.
Valuable in children, or Senile patients
who can’t withstand intraoral films.
Patients who have fractures or
swelling.
It evaluate the condition of the
bone and to locate impacted teeth or
large lesions.
Indications

Cassette is positioned flat against the cheek and centered in the
molar- premolar area.
The lower border of the cassette is parallel
and at least 2 cm below the inferior
border of the mandible
Head position is tilted about 10 to 20 degree toward the side to be
examined and the chin is protruded.
Mandibular body projection –Film placement and head position

The central ray is directed toward the molar-premolar region of the mandible from a point 2cm below the angle of
the opposite side of the mandible

Resultant image
A clear image of the teeth, the alveolar ridge and the body of the mandible should be obtained.
If significant distortion is present, the head was tilted excessively.
If the contra-lateral side of the mandible is superimposed over the area of interest, the head was not tilted sufficiently.

Image receptor is placed over the ramus and far enough posteriorly to include the condyle.
The lower border of the cassette is parallel and at
least 2cm below the inferior border of the
mandible.
The head is tilted toward the side being examined so that the condyle
of the area of interest and the contra-lateral angle of the mandible form a
horizontal line. The mandible is protruded.
The central beam is directed the center of the imaged
ramus, from 2cm below the inferior border of the opposite side of the
mandible at the area of the first molar.
Mandibular ramus projection

• A clear image of the third molar-retro molar area, angle of the mandible, ramus and condylar head should be obtained.
• If significant distortion – head was tilted excessively
• If contralateral side of the mandible is superimposed over the area of interest – head was not tilted sufficiently
Resultant image

• It provides a sagittal view of the lateral aspects of condyle and temporal component.
Used for
Trans cranial
Identifying gross osseous
changes on the lateral aspect of
the joint
Displaced condylar fractures
Range of motion

• It provides a sagittal view of the medial pole of the condyle.
• Used for visualizing erosive changes of the condyle
Trans pharyngeal ( Parma) projection
-5 degree though the sigmoid notch of the opposite side

Trans orbitalIt is similar to trans maxillary projection in that both provide an anterior view of the TMJ, perpendicular to trans cranial and trans pharyngeal.
Uses: To detect condylar neck fractures

• Extra oral images should first be evaluated for overall quality
• Interpreting poor quality images can lead to diagnostic errors and subsequent treatment errors.
A thorough knowledge of normal radiographic anatomy and the
appearance of normal variants is critical for the identification of
pathology
Abnormalities cause disruption of normal anatomy
Detecting the altered anatomy precedes classifying the type of
change and developing a DD
Evaluation of the image

Extra-oral Near Parallel TechniqueExtra-oral Near Parallel Technique
This technique is an alternative to the bisecting angle technique, for the maxillary molars. It is of particular use in cats, where the zygomatic arch superimposes over standard intra-oral bisecting angle views.
The patient is in lateral recumbency
The long axis of the target teeth is as near parallel to the film as possible and the beam is angled at approximately 70 degrees to the film and the target.
The mouth is opened, with a prop, to direct the beam onto the film without superimposing the maxillary teeth on the mandibular teeth

Accuracy is dependent on the ability
to keep teeth as near parallel to film as
possible and to prevent superimposing the
maxillary teeth on the mandibular teeth.

ORTHOPANTOMOGRAM
PANORAMIC IMAGING.
OPG

Orthopantomography
iIt is a technique for producing single tomographic image of facial structures that includes both maxillary and mandibular dental arches & their supporting structures.
• Ortho – correct/straight
• Panorama-“an unobstructed view of a region in every direction”
• Tomography- “X-ray technique of making radiographs of layer of tissue depth, without interference of tissues above and below it.”

Historical milestones for digital panoramic systems :
1985-1991-The first dental digital panoramic systems
were designed by McDavid et al.
1995-DXIS, the first dental digital panoramic x-rays system available in the
market, was introduced by Signet of France.
1997-SIDEXIS, of siemens (currently sirona dental
systems, germany) offered a digital option for ortophos
plus panoramic unit.
Digipan of trophy radiology (France) offered a digital
option for the OP 100 panoramic made by
instrumentarium (Finland).
1998-2004- Many panoramic manufacturers offered their
own digital systems.
2006- SCAN300FP, of ‘Ajat’ (Finland) is the latest
innovation offered

Patero working independently, Numata were the first to describe the principles of panoramic radiography.
Dr. NUMATA 1934Dr.PAATERO 1934
Father of Panoramic Radiography

To interpret OPG competently one must have a thorough understanding of the following :
1. Principles of Panoramic image formation.
2. Techniques for Patient positioning with head alignment 3. and their rationale.4. Radiographic appearance of normal anatomic structures.

Principles of Panoramic image formation

rotation center
filmtube head angled upward

ROTATION CENTERis the pivotal point, or
axis, around which
the cassette carrier
and x-ray tube head
rotate.
* Depending on the
manufacturer, the
number and location
of the rotational
center differ:
ROTATION CENTER
Split image
Single-center rotation
Double-center rotationTriple-center rotation
Moving center rotation – Ellipso
pantomography

Double-Center rotation

Triple-center rotation

Parts of the machine
X-ray tube head
Cassette and
carriage
assembly
Patient
positioning
device
Exposure control

ProMax (PLANMECA)
Panoramic machine.
Scanora multimodality Panoramic machine.
Orthopantomography op 100 panoramic machine.

Three-dimensional curved zone or image layer in which structures are reasonably well defined
Focal Trough, focal corridor
Depends upon :
1. Arch path
2. velocity of receptor and Tube head
3. Cassette size

The occlusal plane is aligned so that it is lower anteriorly, angled 20 to 30 degrees below the horizontal plane.

149
The four Diagnost
ic regions in OPG
The four Diagnost
ic regions in OPG
Dentoalveolar region
Maxillary region
Mandibular region
TMJ including retro maxillary and cervical region

150
Maxillary region

151
Mandibular regionMandibular region

152
Dentoalveolar region
Dentoalveolar region
• Shape and angulation of roots.• Alveolar bone and periodontium• Shows gentle curve of occlusal plane

153
Soft tissue images

154
Air spaces
Air spaces

Broad coverage of the facial bones and teeth. Low patient radiation dose.
Convenience of the examination for the
patient.
Ability to be used in patients unable to open
their mouths.
Patient's readily understand of panoramic
films, making them a useful visual aid in patient
education and case presentation.
Short time required - 3 to 4 minutes
Easy to store, compared to the large set of intra oral x-
rays which are typically used Principle advantages of
panoramic Images:

DISADVANTAGES
DISADVANTAGES
Magnification, Geometric
distortion and overlapped
images.
Resolution of fine anatomic details of
peri-apical area and periodontal
structures is less.
Poor image is obtained when
sharp inclination of anterior teeth
towards labial or lingual side.
The spinal cord superimpose on anterior region.
Common to have overlapped teeth
images, particularly in premolar area.
Artefacts are common and may
easily be misinterpreted.
Expensive

USES
• First examination of new patients (patients with multiple deep carious
lesions, with orthodontic and periodontal problems)
• Early diagnosis of dental anomalies (recommended especially at ages of
10, 15 and 20 years), to check dentition and to provide a timely diagnosis
of the odontogenic tumors or cysts
• Establishing the exact cause of missing teeth
• Radiographic examination of the teeth with endodontic treatment
• Odontogenic sinus disease suspicion
• Disorders of TMJ caused by malocclusion (in such cases, the
Orthopantomogram should be performed with the patient in habitual
occlusion)
• Facial and maxillary asymmetry
• Painful or asymptomatic swelling

• Multiple dental extractions, with suspected osteomyelitis
• Examination of non-odontogenic cysts, tumors and tumor-like lesions of
bone tumors
• Suspicion of invasive bone tumors or bone metastases
• Neural tumors
• Unusual sensitivity of teeth, unusual eruption, spacing or migration of
teeth
• Radiographic examination of the oromaxillo-facial area in systemic
diseases and syndromes
• Maxillo-facial fractures and suspected post-traumatic fractures
• Before and after surgery in the oromaxillo-facial surgery.

Panoramic Technique Errors

Ghost image:- A ghost image looks like the real object except that it appears on the opposite side of the film.

Shadow of vertebral column, usually from patient not standing straight

Lead apron shadow

Anterior teeth narrower and blurred

Anterior teeth wider and blurred
Teeth too posterior

Structures smaller on the side to which head is turned; larger on opposite side.

Mandibular incisors shortened, V-shaped mandible
HEAD TIPPED DOWN

HEAD TIPPED UP
Squared-off mandible, palate superimposed over maxillary teeth

REVERSE OPG:
The chin rest was removed so that the patient can be positioned posteriorly such that the condylar region is moved closer to the
lateral centre of rotation within a fixed distance between the X ray source and the cassette.
The technique is simple to perform with the patient in the reverse position in an Orthopantomogram
Reverse panoramic radiography is a radiographic technique to view the lateral aspect of the condylar head and its neighboring
structures more clearly and with less distortion.


Advances in radiogrpahic techniques

• Sustantial amount of bone loss is required in conventional radiograph to be detected in radiograph.
• Enables use of computerized images, can be stored, manipulated and corrected.
• Image is constructed using pixels• These pixels are arranged in grids and rows on
the sensor
Digital Radiogrpahy

Image acquisitionTwo systems are thereDirectIndirect
Direct digiital radiogrpahy• Uses (CCD) sensor linked with a fiber optic to the computer system• Real time imaging radiography
Disadvantages• Limited sensor area depics one or two teeth• Sensor rigidity

Direct Digital radiographyDirect Digital radiography• nondestructive test (NDT)• image is produced electronically, rather than on film, • very little lag time occurs between the item being
exposed to radiation and the resulting image. • the electronic image that is viewed results from the
radiation passing through the object being inspected and interacting with a screen of material that fluoresces or gives off light when the interaction occurs.
• Fluorescent elements of the screen form the image much as the grains of silver form the image in film radiography.

• Commercial digora system
• Uses phosphor luminescence flexible film like radiation sensor placed
• Intraorally and exposed to x ray tubes\
• A laser scanner reads exposed plates offline and reveals digital image data.
Indirect Digital radiography

Advantages • Dose reduction• Image manipulation• Measurements• 3-D reconstruction can be done• Storage• Environmental friendly
• contrast, density
• magnification of area of interest
• edge enhancement
• color renderingDisadvantages
• Expensive • Sensor cannot be sterlized, barriers can be used but if contamined they have to be discared• Medicolegal purposes- images can be manipulated, there are concerns about their use

• The image formed is a "positive image" since brighter areas on the image indicate where higher levels of transmitted radiation reached the screen.
• This image is the opposite of the negative image produced in film radiography.
• The lighter, brighter areas represent thinner sections or less dense sections of the test object.

Radio-visographyRadio-visography
• X rays takes using sensor that transmit images directly onto computer monitor
• Helps patient understand the doctors explanation more easily
• Enables the doctor to zoom in on a digitizes specific area of tooth
• digitizes ionizing radiation• Provides an instantaneous image on video
monitor• Reduces exposure by 90%• Equipment has fiber optic intra oral sensor (with
selenium coated plate)

Radio-visiographyRadio-visiographyParts • The radio- hypersenitve intra oral sensor and
conventional X-ray unit.• The visio-> video moniter and display processing
u• The graphy>high resolution video printer that
instantly provides a hard copy of screen images using same video signal.

• Advantages• Elimination of xray film• Significant reduction in exposure
time• Instantaneous image display• RVG System appears to be
promising for the future of dentistry.Disadvantages
• Resolution is slightly lower than convenional films
• Exposure above .15s at 75Kp reults in pixels saturation that results in shortening in saturation of the length of the intrument

Digital Substraction Radiography
Digital Substraction Radiography
• Image enhancement method• Area under focus being clearly
displayed against a neutral gray black background or it is superimposed on the radiographic itself.
• Relies on conversion of serial radiogrpahs into digital images
• Quantitative changes can be accompalished by eans of a computer (Computer Assisted Substraction Radiography

• Advantages• reduced radiation up to 80% • faster imaging without X-ray film and developing
images • digital intraoral sensor is used instead of X-ray film• immediate imaging on the computer screen • high quality of the digital image that can be analyzed
and processed• saving images in the patient's file• children friendly for reduced radiation, if imaging is
necessary• Evaluation of success of treatment• Changes in alveolar bone levels• Progress of an incipient carious lesion to DEJ• Assessing healing or expansion of periapical lesion after
RCT
Disadvantages • Need to be close to identical porjection alignment
during the exposure of sequential radiographs• Makes this method very impractical in a clinical
setting.

• Recently , new image substraction methods DIAGNOSTIC SUBSTRACTION RADIOGRAPHY (DSR) have been introduced combining use of a positioning device during film exposure with a specialized software.

Computed TomographyComputed Tomography• powerful nondestructive evaluation (NDE) technique
for producing 2-D and 3-D cross-sectional images of an object from flat X-ray images.
• Characteristics of the internal structure of an object such as dimensions, shape, internal defects, and density are readily available from CT images.

• The test component is placed on a turntable stage that is between a radiation source and an imaging system.
• The turntable and the imaging system are connected to a computer
• 2-dimensional shadowgraph image of the specimen just like a film radiograph.
• Specialized computer software produces cross-sectional images of the test component as if it was being sliced.

IndicationsIndications• Investigation of intracranial disease including tumours,
haemorrhage & infarcts.• Suspected intra cranial, spinal cord damage.• Fractures-In the orbit, naso- ethmoid complex. - Cranial base. -Odontoid peg - Cervical spine
• Cyst-Site, size & extent.• Disease within para nasal air sinuses.-• Tumor staging- site, size, extent of affecting different
regions. • Tumour and tumour like discreet swellings both
intrinsic and extrinsic to salivary glands.• Investigation of osteomyelitis.• Investigation of TMJ.• Preoperative assessment of maxillary and mandibular
alveolar bone height.•

Advantages Disadvantages
Very small amounts and differences in x-ray thus detailed imaging of intra cranial lesions, imaging of hard and soft tissues both hard and soft tissues.
Axial tomographic sections are obtainable.
Reconstructed images can be obtained from information obtained I the axial plane.
Images an be enhanced by the use of IV contrast media to delineate blood vessels.
• Equipment is very expensive.
• Very thin contiguous or overlapping slices result in very high dose investigation.
• Metallic objects produce marked streak or artifacts.
• Inherent risks associated with IV contrast agents.

• Also known as digital volume tomography/(CBCT) are a variation of traditional CTsystems.
• used by dental professionals • rotate around the patient, capturing data using a cone-
shaped X-ray beam. • reconstruct a three-dimensional (3D) image of the
following regions of the patient’s anatomy: dental (teeth); oral and maxillofacial region (mouth, jaw, and neck); and ears, nose, and throat.
• One an is 20-40secs, and in one scan image I cylindrical in volume described as field of view.
• Field of view of 15cm diameter is used for scanning maxillofacial skeleton
CONE BEAM CT

CT CBCT
200-300 conventional radiographs.
2-8 conventional panoramic radiographs
.When compared with ortho pantamogram
3D accuitomo images a small cylinder of information thus enabling high resolution images of specific teeth to be obtained.Voxel size is 0.125mm x 0.125 mm x 0.125mm.Dose of this very low when compared to 3-4 peri apical radiographs.

IndicationsIndications• Investigation of all conditions affecting the mandible
or maxilla including cysts, tumours, giant cells and osseous dysplasia.
• Cleft palate assesment• Investigation of maxillary antra• Investigation of TMJ.• Implant assessment .• Orthodontic assessment.• Localisation of unerupted tooth/ odontomes.• Assessment of lower 3rd molars .• Investigation of fractures of mandible or middle 1/3rd
of facial skeleton.• For multi planar imaging of a single tooth in terms of
peri apical & periodontal tissue with high resolution scanners.

Advantage Disadvantage
• Multi planar imaging and manipulation.
• Low radiation dose• Very fast scanning
time.• Inexpensive and
affordable.• Used mainly for
implant and cephalometric planning
• Soft tissue detailing is not possible.
• Computer derived panoramic image I not comparable with conventional panoramic radiographs- particular are is needed for interpretation.
• Metallic fillings/objects produce streaks and star artefacts like CT.
J of canadian dental association 2006

MRIMRIPrincipleRadio frequency signal emitted by excited hydrogen atoms in the body (present in any tissue containing water molecules) using energy from an oscillating magnetic field applied at the appropriate resonant frequency. The orientation of the image is controlled by varying the main magnetic field using gradient coils. coils are rapidly switched on and off they create the characteristic repetitive noises of an MRI scan. The contrast between different tissues is determined by rate at which excited atoms return to the equilibrium state, Exogenous contrast agents may be given intravenously, orally or intrarticulary.[
Current science , VOL 67 , No 12, 25 dec 1994

IndicationsIndications• three-dimensional hard- and soft-tissue imaging of
teeth without the use of ionizing radiation. • potential to image minute dental structures within
clinically relevant scanning times. • Endodontists-potential method to longitudinally
evaluate teeth where pulp and root structures have been regenerated.
• Distinguish between various soft tissues and localisation of soft tissue lesions.
• Stray field microscope- modification of MRI – can detect canals in tooh for endodontic purposes
• Differentiate aglossia from hypoglossia• TMJ displacements and related problems
J.endod 2011 Jun;37(6):745-52.

contraindicationscontraindications• Ferromagnestic substance s like
pacemaker,shrpnels,etc could be disloged causing complications.
• Chromic alloy arch wires, stainless steel crowns. Banda and bonded metals cause artifacts

Ultra soundUltra sound
• Non-invasive investigation which use a very high frequency (7.5-20MHz) pulsed ultrasound beam rather than ionizing radiation.
• Produces high resolution images of more superficial structures.
Oral surg oral med oral pathol oral radiol 203 june

Ultrasound travels to the
skin
Some waves are reflected back by tissues to
produce echoes.
Which is picked up by the
transducer and converted into electrical signal
then into real time black , white and
grey images

• sectional image which represents topographical map of depth of tissue interfaces.
• thickness is determined by width of ultra sound beam thus different density in the black /white echo picture is described as hypo echoic(dark) or hyper echoic(light).
• A change in the frequency of sound reflected from a moving source allows the detection of arterial and venous blood flow - Doppler effect.
Oral surg oral med oral pathol oral raiol 203 june

1. caries detection, 2. dental fractures3. soft tissue and periapical lesions4. maxillofacial fractures 5. periodontal bony defects6. gingival and muscle thickness7. Temporomandibular disorders8. Implant dentistry.9. Evaluation of the swellings of the neck ,those
involving thyroid, cervical lymph nodes, major salivary glands thus to detect solid and cystic soft tissue masses.
10. Detection of salivary gland and duct calculi.11. Determination of vascularity and vascular
structures.12. Assessment of vascularity of carotids and carotid
tumors.13. Sialolithotripter –to break salivary calculi into 2mm
fragments thus avoiding major surgery.14. Ultra sound guided FNA biopsy.
Indications :-Indications :-

Advantage Disadvantage
• Non ionizing radiation.• No known harmful
effects• Good differentiation
between soft and hard tissues.
• Widely available and relatively in expensive.
• Bone absorbs ultrasound thus is not detected.
• Real time imaging.• Technique sensitive• Difficult to interpret
for inexperienced operator.
Oral surg oral med oral pathol oral raiol 203 june

Contrast studiesContrast studies
Radiopaque substances alter the density of different
parts of patient.
Alters the subject contrast.
Thus certain organs , structures, tissues, invisible by conventional means
be seen.

Different contrast studiesDifferent contrast studiesSialography –Salivary
glands.
Arthrography
Angiography
Lymphography- Lymph nodes and
vessels
Urography
Barium meal, swallow and enema-GI tract.
Computed tomography-general
enhancement.

IndicationsIndications
To show vascular anatomy and feeder vessels associated with haemangiomas.
To show vascular anatomy of arterio venous formation
Investigation of suspected sub-arachnoid haemorrhage resulting from an aneurysm in
the circle of willis.
Investigation of transient ischaemic attacks due to emboli from atheromatous plaques.

ComplicationsComplications• Mild. Eg:-Headache, nausea, warmth/pain,
flushing, sneezing, constipation.• Moderate. Eg :-Vomiting , bronchopasm,
urticaria and hypotension. • Severe. Eg:-Cardiac arrhythmias, cardiac
arrest, convulsions, anaphylactic shock and pulmonary edema.
• Fatal.

Patients at riskPatients at risk
1. Very young patients2. Patients with a history of allergy to
contrast media3. Diabetes, patients suffering from cardiac
failure, renal failure, severe pulmonary disorders including asthma
Cause of complications• Allergy• Chemotoxicity• Osmolality• Anxiety

Hazards of dental x-rays in oral cavity
Hazards of dental x-rays in oral cavity
• da Silva et al have demonstrated that panoramic radiography increases the number of nuclear anomalies (except micronuclei), with significant statistically differences in exfoliated cells from the lateral border of the tongue,
• were exposed to a repeat radiograph it induces a genotoxic effect on epithelial gingival cells that increases the frequency of chromosomal damage and nuclear alterations indicative of apoptosis.
• The comparison of nuclear changes before and after radiation exposure revealed a statistically higher number of broken eggs, buds, karyorrhexis and binucleate cells 10 days after exposure.
.Dentomaxillofac Radiol. 2012 March; 41(3): 181–184

• X-ray increased other nuclear alterations closely related to cytotoxicity, such as karyorrhexis, pyknosis and karyolysis.
• Digital lateral radiography (cephalometric radiography) obtained on a panoramic radiographic machine showed similar results when compared with conventional radiography in oral mucosa cells.
• Yoon et al18 revealed high expression levels of pChk2 and γ-H2AX in oral cells after radiation exposure.-indicators of low-dose radiation exposure.
Dentomaxillofac Radiol. 2012 March; 41(3): 181–184

• When the effect of dental X-ray exposure in children was investigated, no statistically significant differences were found between micronucleated oral mucosa cells before and after radiation exposure.
• radiation did lead to other nuclear alterations closely related to cytotoxicity, including karyorrhexis, pyknosis and karyolysis: there were significant statistically.
• CBCT in clinical practice evaluated DNA damage (micronucleus) and cellular death (pyknosis, karyolysis and karyorrhexis) in exfoliated buccal mucosa cells from adults. The effective dose was 12 μSv.
Dentomaxillofac Radiol. 2012 March; 41(3): 181–184

RADIATION PROTECTIONRADIATION PROTECTION
• Radiation is energy in the form of waves or moving subatomic particles.

TYPES OF RADIATIONTYPES OF RADIATION
• NON-IONIZING RADIATION
• IONIZING RADIATION• capable for producing ions
when interact with matter. PARTICULATE (alpha, beta,
neutrons) ELECTROMAGNETIC (X-Rays,
Gamma Rays)

PATIENT EXPOSURE & DOSE
PATIENT EXPOSURE & DOSE
• Patient dose from dental radiography is usually reported as the amount of radiation received by a target organ.
• Most common measurements is skin or surface exposure.
• Other target organs - Mean active bone marrow, thyroid & gonads.

• The International Commission on Radiological Protection (ICRP) devised a system of dose limitation.
Based on following general principles:• No practice shall be adopted unless its
introduction produces a positive net benefit.• All exposures shall be kept as low as
reasonably achievable (ALARA), taking economic & social factors in account.
• The dose equivalent to individuals shall not exceed the limits recommended by the commission.

What is ALARAWhat is ALARA• ALARA is an acronym for As Low As
reasonably Achievable. This is a radiation safety principle for
minimizing radiation doses and releases of radioactive materials by employing all reasonable methods.
• regulatory requirement for all radiation safety programs
• Current radiation safety philosophy is based on the assumption that radiation dose and its
• biological effects on living tissues are modeled by a relationship known as the “Linear Hypothesis

Mitigation of External Radiation Exposures The three (3) major principles to assist with
maintaining doses ALARA are : 1) TIME – minimizing the time of exposure
directly reduces radiation dose. 2) DISTANCE – doubling the distance between
your body and the radiation source will divide the radiation exposure by a factor of 4. 3) SHIELDING - using absorber materials such
as Plexiglas for beta particles and lead for X-rays
and gamma rays is an effective way to reduce
radiation exposures

Mitigation of Internal Radiation Exposures 1) Good hygiene techniques that prohibit the consumption of food and drink in the lab and the control of personal gestures that involve “hand-to- mouth” contacts. 2) Frequent swipe surveys and lab area monitoring of
work areas, refrigerators, hoods, sinks, phones and computer keyboards, etc.
3) Control contamination with absorbent paper and spill trays, properly labeled waste containers, equipment, etc. and prompt decontamination of any detected contamination.
4) Use fume hoods for materials which could become airborne (e.g., vapors, dust, aerosols, etc.) and present an inhalation hazard to workers.
5) Use proper protective equipment (PPE) such as disposable gloves, safety glasses, lab coats, etc. to
reduce the possibility of ingestion or absorption of radioactive materials

Maximum Annual Occupational Dose Limits
Maximum Annual Occupational Dose Limits
Whole Body …………………… 5000 millirem Extremities ……………………. 50000 millirem Lens of the Eye ……………….. 15000 millirem Fetus ……………………………… 500 millirem* Individuals in the General Public …100 millirem * 500 millirem for the fetus is during the gestation periodThe ALARA concept imposes lower operational dose limits that are even more restrictive than the maximum legal dose limits in the table above.If a radiation worker’s dose for any calendar quarter (3 months) or calendar year (12 month period) exceeds these values, an investigation is conducted by
the RSO to determine if there are reasonable ways to reduce
the dose levels and discuss with the worker methods for limiting the potential dose

ICRP divided the population into 3 groups:
• PATIENTS• RADIATION WORKERS• GENERAL PUBLIC

PATIENTSPATIENTS
• Examination directly associated with illness.
• Systemic examinations (periodic health checks)
• Examination for occupational, medico-legal insurance purposes.
• Medical research.

RADIATION WORKERSRADIATION WORKERS
• Exposed to radiation during the course of their work.
• Divided into 2 subgroups depending on the level of occupational exposure:CLASSIFIED WORKERSNON-CLASSIFIED WORKERS

CLASSIFIED WORKERSCLASSIFIED WORKERS• Receive high levels of radiation
exposure to radiation at work (nuclear power industry)
• Require compulsory personal monitoring.
• Require compulsory annual health checks.

NON-CLASSIFIED WORKERSNON-CLASSIFIED WORKERS• Receive low levels of exposure to
radiation at work.• The annual dose limits are 3/10 of
the classified worker’s limit.• Personal monitoring is not
compulsory.• Annual health checks are not
required.

GENERAL PUBLICGENERAL PUBLIC• Originally set annual dose limits - 5
mSv.• Current recommendation - 1 mSv.

SOURCES OF RADIATION IN DENTAL RADIOLOGY
SOURCES OF RADIATION IN DENTAL RADIOLOGY
• PRIMARY BEAM• SECONDARY RADIATION• STRAY RADIATION• SCATTERED RADIATION

CONDUCT OF EXAMINATIONCONDUCT OF EXAMINATION
• CHOICE OF EQUIPMENT• CHOICE OF TECHNIQUE• OPERATION OF THE EQUIPMENT• PROCESSING OF THE RADIOGRAPH• INTERPRETATION OF THE RADIOGRAPH

CHOICE OF THE EQUIPMENT
CHOICE OF THE EQUIPMENT
• IMAGE RECEPTER• FOCAL SPOT TO FILM DISTANCE• COLLIMATION• FILTERATION• POSITION INDICATING DEVICE• FILM HOLDING DEVICE• LEADED APRONS AND COLLARS

INTRAORAL IMAGE RECEPTOR
INTRAORAL IMAGE RECEPTOR
• In 1920, regular dental X-ray film – EASTMAN KODAK COMPANY.
• Intraoral dental X-ray film – D & E speed.• Speed of E-speed film – 2 times of D-speed
film & 50 times of regular dental X-ray film.• E-speed film (Ektaspeed film, Eastman
Kodak Company) - 1981.

• Patient dose reductions :– 60% compared with E-speed film.– 77% compared with D-speed film.
• Digital Imaging – 50 to 95% reduction in patient exposure.

EXTRAORAL FILMS/INTENSIFYING
SCREENS
EXTRAORAL FILMS/INTENSIFYING
SCREENS
• Calcium tungstate – emits blue light.• Rare earth elements Gadolinium &
Lanthanum – emits green light.• Rare earth screens -
– 8 times more sensitive to X-rays.– 55% reduction in patient
exposure.

FOCAL SPOT TO FILM DISTANCEFOCAL SPOT TO FILM DISTANCE
• 2 standard FSFDs: – 8 inches (20 cm) – 16 inches (41 cm)
• Federation Regulation – Minimum X-ray source-skin distance: – 7 inches (18 cm) X-ray tube operating
above 50 kVp.– 4 inches (10 cm) X-ray tube operating
below 50 kVp.


• COMPARISION OF 16 INCHES AND 8 INCHES FOCAL SPOT:– 38% decrease in thyroid dose with 90
kVp X-rays.– 45% decrease in thyroid dose with 70
kVp X-rays.
• Longer FSFD – 32% reduction in exposed tissue volume.

COLLIMATIONCOLLIMATION• Helps to control the size & shape of X-
ray beam.• Recommended beam size – 23/4 inches.

• Decreases radiation exposure.• Minimizes scattered radiation Decreases fogging of film
Sharper image & better contrast


• Collimation is done with lead diaphragm within the tube head or at the end of lead-lined cylinder.
• 2 types : Round & Rectangular.

DENSPLY/RINN RECTANGULAR COLLIMATOR

MARSEL PRECISION INSTRUMENT

• Round collimator – 3 times the area necessary to expose the film.
• Rectangular collimator reduces patient dose approx 55%.

FILTERATIONFILTERATION
• Filteration removes the low energy X-ray photons selectively from the X-ray beam.
• Filteration is stated in mm of Al.

TYPES OF FILTERATIONTYPES OF FILTERATION• INHERENT FILTERATION – 0.5 to 1.0 mm
of Al.• ADDED FILTERATION – 0.5 mm of Al.• TOTAL FILTERATION – Inherent + Added
filteration

• X-ray beam filtered with 3 mm of Al – surface exposure reduces by 20%.

• Al + rare earth materials like Samariun, Erbium, Yttrium, Niobium, Gadolinium, etc
• Selective filteration of low & high energy photons ( X-ray energies most effective in producing image: 35 keV to 55 keV)
• Reduces patient exposure by 20% to 80%

POSITION INDICATING DEVICE (PID)
POSITION INDICATING DEVICE (PID)
• PID - an extension of X-ray tubehead.• Direct the X-ray tube.• Minimize the volume of tissue
irradiated.• 3 basic types :
– Conical– Rectangular– Round

CONICAL PID

POSITION INDICATING DEVICE (PID)

• PIDs are commonly available in 3 lengths :– 8 inches– 12 inches– 16 inches
• Long PID is preferred.

FILM HOLDING DEVICEFILM HOLDING DEVICE• Helps to stabilize the film position in the
mouth.

OFFER PROTECTION TO THE PATIENT :• Reduces frequency of retakes.• External guide to indicate the film
position.• Possibility of misalignment of the X-ray
tube. • Collimate the beam to the size of film
being used.• Reduction in the exposure to patient’s
fingers.

PROTECTIVE BARRIERSPROTECTIVE BARRIERS• LEAD APRONS• THYROID COLLARS

LEAD APRONSLEAD APRONS• A flexible shield of lead placed over the
patient chest & lap.• To protect reproductive organs & bone
marrow.• Recommended for all intraoral &
extraoral radiography. • Protective equivalent – 1/4 mm of Pb.

• Attenuate 98% of scatter radiation to the gonads.
• LEADED TORSO (BODY) aprons

THYROID COLLARTHYROID COLLAR• Flexible lead shield placed securly
around the patient’s neck.• Protect thyroid gland.• Recommended for intraoral radiographs.• Reduce the thyroid gland exposure by
92%.


CHOICE OF INTRAORAL TECHNIQUE
CHOICE OF INTRAORAL TECHNIQUE
• Bisecting angle technique• Paralleling long cone technique• Rinn XCP instrument / Precision
instrument.

OPERATION OF THE EQUIPMENT
OPERATION OF THE EQUIPMENT
• KILOVOLTAGE (kV)• MILLIAMPERAGE (mA)• TIME SETTINGS

KILOVOTAGE (kVp)KILOVOTAGE (kVp)• X-ray machine : 70 – 90 kVp.• Produce fewer low-energy X-rays.• Gibbs etal (1988) reported that effective
dose reduces to 23% - increasing kVp from 70 to 90 kVp.
• Constant potential X-ray machine – reduces patient exposure by 20%.

• Higher kVp – periodontal diagnosis.• Low kVp – caries or soft tissue
calcification.

MILLLIAMPERE-SCONDS (mAs)
MILLLIAMPERE-SCONDS (mAs)
• X-ray machine : 8-10 mA.• IMAGE DENSITY – milliamperage &
exposure time.• Exposure time – most crucial factor
influencing diagnostic quality of radiographs.

TIMERTIMER• Timer on the X-ray machine should be
electronic.• “dead-end” control.• Calibrated in 60th of sec.

PROCESSING OF THE RADIOGRAPHS
PROCESSING OF THE RADIOGRAPHS
• DARKROOM LIGHTING• FULL DEVELOPMENT PROCESSING• PROCESSING SOLUTIONS

DARKROOM LIGHTINGDARKROOM LIGHTING• Kept free from light leaks.• Safelight filter – Kodak GBX-2 (red light)• 15 watt bulb.• Safelight lamps – min of 4 ft from
working area.

FULL DEVELOPMENT PROCESSING
FULL DEVELOPMENT PROCESSING
• Time-temperature processing• Radiation exposure may be decreased
by 25%.
TEMPERATURE (in OF) DEVELOPMENT TIME (in min)
68 5
70 41/2
72 4
76 3
80 21/2

PROCESSING SOLUTIONSPROCESSING SOLUTIONS• Changed regularly• Stirred thoroughly twice each day• Kept covered to prevent oxidation• Not subjected to excessively high
temperatures.• Weekly quality control checks.• Chemicals should be replenished
according to manufacturer’s instructions.

INTERPRETATION OF RADIOGRAPHS
INTERPRETATION OF RADIOGRAPHS
• Viewed in a dimly lit room with a properly functioning illuminator (view-box).
• Illuminator with variable intensity.

3 basic methods to reduce occupational exposure:3 basic methods to reduce occupational exposure:
• POSITION• DISTANCE• SHIELDING
OPERATOR RADIATION PROTECTION
OPERATOR RADIATION PROTECTION

DISTANCE RECOMMENDATIONS
DISTANCE RECOMMENDATIONS
• 6 feet away from X-ray tubehead during exposure.
• When distance is not possible – Protective lead barrier

POSITION RECOMMENDATIONS
POSITION RECOMMENDATIONS
• 90o to 135o angle to the primary beam.• Never hold a film in place for a patient• Never hold or stabilize the tubehead ………during radiation exposure.

Dystrophic nail changes Squamous cell carcinoma

POSITION DISTANCE RULE“The operator should stand at least 6 feet
away from the patient in a safe quadrant at an angle of 90o to 135o to
the central ray of X-ray beam.”

SHIELDING RECOMMENDATIONS
SHIELDING RECOMMENDATIONS

ROLLING RADIATION PROTECTION SHIELDROLLING RADIATION PROTECTION SHIELD
• Offers 0.5 mm lead protection.
• Measures 24 X 231/2.
• Adjusts 36”-56” above the floor.

PROTECTION OF THE ENVIRONMENT
PROTECTION OF THE ENVIRONMENT
• Surrounding environment must be protected from radiation to avoid the exposure of persons in the environment.
• Primary beam should never be directed at any one other than the patient.
• X-ray beam is aimed at the wall of the room and not through door.

QUALITY ASSURANCEQUALITY ASSURANCE “Any systemic action to ensure that a
dental office will produce consistently high-quality images with minimal
exposure to patients & personnel.”
“Currently some state require dental offices to establish written guidelines
for quality assurance & maintain written records of quality assurance test.”

Quality assurance
X ray unit
Leakage radiation
Stability of tube
housing
CollimationTimer accuracy
Ancillary instrument maintenanc
e
Dark room maintenance


VARIOUS RADIATION MONITORING DEVICES
AVAILABLE:
VARIOUS RADIATION MONITORING DEVICES
AVAILABLE:• ELECTRICAL
– Ionization chamber– Thimble chamber– Geiger counter
• CHEMICAL– Film– Chemical dosimeter
• LIGHT– Scintillation counter– Gerenkov counter
• THERMOLUMINESCENCE– Thermoluminescent dosimeter
• HEAT– Calorimeter

PERSONAL MONITORING DEVICES
PERSONAL MONITORING DEVICES
• POCKET DOSIMETER• FILM BADGE• THERMOLUMINESCENT DOSIMETER
(TLD)• ELECTRONIC DOSIMETER

• Modified version of badge

THERMOLUMINESCENCE DOSIMETER (TLD)
THERMOLUMINESCENCE DOSIMETER (TLD)
• Most common personal monitoring device.
• Used for measurements of the actual dose received by the operator.

ELECTRONIC DOSIMETERELECTRONIC DOSIMETER• 5 to 200 times more sensitive than TLD.• With an audible alarm system.

Unique Considerations for Radiation Exposure in Children in
CT scans
Unique Considerations for Radiation Exposure in Children in
CT scans
• There are three unique considerations in children.• Children are considerably more sensitive to radiation
than adults, as demonstrated in epidemiologic studies of exposed populations.
• longer life expectancy than adults- larger window of opportunity for expressing radiation damage.
• The risk for developing a radiation-related cancer can be several times higher for a young child.
• The use of more than one scan further increase the radiation dose.
• Majority of cases, a single scan should be sufficient during pediatric CT.
University of Michigan Children hospital site

Radiation reductionRadiation reductionPerform only necessary CT examinations-• When appropriate, other modalities such as ultrasound MRI,
which do not use ionizing radiation, should be considered.Adjust exposure parameters for pediatric CT based on
– Child size: guidelines based on individual size / weight parameters should be used.
– Region scanned: the region of the body scanned should be limited to the smallest necessary area.
– Organ systems scanned: lower mA and/or kVp settings should be considered for skeletal, lung imaging, and some CT angiographic and follow up examinations.
• Scan resolution: the highest quality images are not always required to make diagnoses. many cases, lower-resolution scans are diagnostic.
• Providers should be familiar with the multiphase examinations. These result in a considerable increase in dose and are rarely necessary, especially in body (chest and abdomen) imaging.
University of Michigan Children hospital site

“value of a diagnostic procedure depends upon the amount of information that can be derived from it”
Although these radiographic techniques are essential in arriving at a diagnosis, appropriate usage of the right technique in the right time to an apt condition becomes vital to the clinician in guiding to arrive at a conclusion for diagnosis and there by treatment planning
CONCLUSION

ReferencesReferences
Principles and Interpretations of Oral Radiology, 5th Edition By Stuart C.WHITE and MICHAEL J.Pharoah.
Essentials of Dental Radiography, 3rd Edition by Haring . Text Book of dental and maxillofacial Radiology By Frenry
R. Karjodkar.. Essentials of Dental radiology and radiology,3rd edition,
Eric whites Text book of Pedodontics (Mc Donald & Avery) Oral radiology- principles and interpretation; Paul W.
Goaz, Stuart C. White Web Page – Radiographic techniques for pediatric patients
(steven Schwartz) dentalcare.com Intra-Oral Radio Graphs for the Pediatric Dental
Patient Pedo- fourth molar web page