Embed Size (px)
DESCRIPTION
about takayasu arteritis
Citation preview

Radioisotope Lung Scanning inTakayasu's Arteritis1
Yutaka Suzuki, M.D., Kaoru Konishi, M.D.,and Kinichi Hisada, M.D.
ABSTRACT-Of 15 patients with Takayasu's arteritis studied by 131l-macroaggregated albumin lung scanning, 12 showed perfusion abnormalities. Thelung scan proved very useful in detecting the pulmonary artery disorders associated with Takayasu's arteritis. The pathogenesis of this disease and clinicalusefulness of this study are discussed.
INDEX TERMS: Lungs, radionuclide studies • Pulmonary Arteries • PulselessDisease
Radiology 109: 133-136, October 1973
NuclearMedicine
ALTHOUGH Takayasu's arteritis is a diseaserl. characterized by stenotic lesions of theaorta and its major branches due to unknown etiology, there are several articles which have reported pulmonary arterial involvement in thissyndrome (3, 6, 8).
Radioisotope lung scanning is a very simpleand safe technique for evaluating pulmonary bloodflow. We have done lung scanning in 15 patientswith Takayasu's arteritis. It is the purpose ofthis paper to describe findings at lung scanningwith 131I-macroaggregated albumin (13II-MAA)and discuss their clinical usefulness.
MATERIALS AND METHODS
A total of 15 patients with Takayasu's arteritis
who had been admitted to the Kanazawa University Hospitals were studied with lung scanning.All were women and the age at the time of theadmission ranged from 16 to 49, with an averageof 24 years (TABLE I). The diagnosis of Takayasu's arteritis was made on the basis of clinicalevidence and arteriography.
Two hundred microcuries of 1311_MAA wasinjected intravenously while patients were lyingsupine and a lung scan was done with the isosensitive rectilinear scanner (MUCH).
The lung scans were interpreted by one of theauthors without knowledge of the other clinicaldata. The lung scan was divided into six areasi.e., upper, middle and lower in both lungs andeach area classified into three grades according
TABLE I: SUMMARY OF CLINICAL, ROENTGENOLOGICAL AND SCANNING DATA OF 15 PATIENTS WITH TAKAYASU'S ARTERITIS
Case Age-No. Sex
Chest X-Ray Findings------Lung Scanning Findings*------
.-----Right Lung-.----, .------Left Lung----,Upper Middle Lower Upper Middle Lower
1 16F Essentially normal (-) (- ) (- ) (+ ) (- ) (- )2 25F Essentially normal (+ ) (- ) (- ) (- ) (+ ) (- )3 17F Pleural reaction in the lower left lung (- ) (- ) (++) (- ) (- ) (- )4 44F Essentially normal (- ) (- ) (- ) (- ) (+ ) (++)5 21F Tortuous and dilated descending aorta (++) (++) r- ) (+ ) (++) (++)6 18F Essentially normal (- ) (- ) (- ) (- ) (- ) (- )7 38F Essentially normal (+ ) (- ) (- ) (- ) (- ) (- )8 36F Essentially normal (++) (- ) (- ) (- ) (- ) (- )9 41F Dilated and tortuous aorta; notching in the
left 6th rib (- ) (+) . (- ) (++) (- ) (- )10 49F Essentially normal (- ) (- ) (++) (- ) (- ) (- )11 32F Slight bulge of the middle arch of the left heart
border (- ) (++) (++) -) (+) (- )12 42F Essentially normal (- ) (- ) (++) -) (- ) (- )13 18F Essentially normal (- ) (- ) (- ) -) (- ) (- )14 38F Essentially normal (- ) (- ) (- ) -) (- ) (- )15 32F . Diffuse patchy shadows in the right upper and
middle lung field (++) (- ) (- ) (- ) (- ) (- )abnormal 5 3 4 3 4 2perfusion cases cases cases cases cases cases
* ( + + )Absence of perfusion; ( + ) decreased perfusion; (-) normal perfusion.
1 From the Department of Nuclear Medicine, School of Medicine, Kanazawa University, Takara-machi 13-1, Kanazawa-shi, Japan.Accepted for publication in May 1973. shan
133

134 Y. SUZUKI, K. KONISHI AND K. HISADA October 1973
-.0 l'
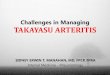
Fig. 1. CASE 2. A. Postero-anterior chest radiograph is essentially normal.
B. Lung scan demonstrates absence of perfusion in the right apexand decreased perfusion in the lower left lung.
C. Pulmonary arteriogram showing decreased vascularity in theupper right and lower left lung.
to the degree of perfusion abnormality: absence ofperfusion, decreased perfusion, and normal. Noattempt was made to reinterpret the chest x-rayfilms, and the original report sent at the time ofthe study was taken from the chart.
RESULTS
Twelve of 15 patients (80%) showed some abnormalities in the lung scan, but the chest filmsof all patients except one were interpreted asnormal in the lung field. The abnormal perfusionwas more common in the right lung but there wasno certain area of the lung which had specialtendency to be affected. There were 4 patientswho had abnormal perfusion in both lungs andone of these patients showed abnormal perfusionin the entire left lung (TABLE I).
There was no correlation between the incidenceof abnormal lung scans and age of the patients.
Only 2 patients had subjective symptoms in thechest.
CASE REPORTS
CASE 2. A. H., a 25-year-old woman was admitted to theKanazawa University Hospitals because of headache, generalmalaise and dull pain in the left arm. On physical examination, bruit was heard in the left neck, upper abdomen andleft inguinal region and the pulse was not palpable in theleft carotid artery and left radial arteries. Blood pressurewas 160/72 mm Hg in the right arm. The pulsations in thelower extremities were normal. The erythrocyte sedimentation rate was 111 mm in an hour. A serological test for syphylis was negative and a C-reactive protein (CRP) test waspositive.
The chest film was interpreted as essentially normal (Fig.1, A). Lung scanning revealed absence of perfusion in theright apex and markedly decreased perfusion in the leftlower lung (Fig. 1, B). Pulmonary arteriography showeddecreased vascularity in the right upper and left lower lung(Fig. 1, C). Aortography demonstrated complete obstruction in the left subclavian artery and narrowness in the left

Vol. 109 RADIOISOTOPE LUNG SCANNING IN TAKAYASU'S ARTERITIS
Nuclear135 Medicine
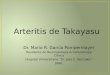
Fig. 2. CASE 11. A. Postero-anterior chest filmshowinga slightbulge of the middle arch of the left heart border. The lung field isessentially normal.
B. Lung scan demonstrates absence of perfusion in the lower rightlung and slightly decreased perfusion in the middle left lung.
C. Pulmonary arteriogram demonstrating occlusion of the rightpulmonary descending and the lingular segmental branches.
common carotid artery, radial artery, thoracic aorta, abdominal aorta, both renal arteries and femoral arteries.
CASE 11. M. A., a 32-year-old woman was admitted tothe Kanazawa University Hospitals with complaints of dizzyspells, fever,and dull pain in the left upper extremity. Sherecalled that doctors had difficulty in feeling her radial pulsefor about four years. On examination, bruit was heard overthe left carotid artery and the left radial pulse was diminished. Blood pressure was 150/76 rnrn Hg in the right armand 104/72 mm Hg in the left. Serological examination forsyphilis was negative and the CRP test was negative. Theerythrocyte sedimentation rate was 50 mm in an hour.
On the chest film, a slight bulge of the middle arch of theleft heart border was seen (Fig. 2, A). Lung scanning showedabsence of perfusion in the right lower lung and slightly decreased perfusion in the left middle lung (Fig. 2, B). Pulmonary arteriography demonstrated occlusion of the rightpulmonary descending branch and the lingular segmentalartery (Fig. 2, C). Aortography revealed partial occlusionin the left subclavian artery and tortuosity in the abdominalaorta.
DISCUSSION
Takayasu's arteritis is more common in Japanand the Orient but is not so infrequent in theUnited States and European countries as oncebelieved (1, 3, 4). It most commonly affectsyoung women and its incidence among thein is 5 r-..J
10 times higher than among males (6, 7, 10).Its etiology is still unknown, but it might be
classified among the autoimmune diseases (10).In this disorder, all three layers of the arterial wallmay be involved but the inflammatory process ismost intense in the media, so this disease couldessentially be called mesoarteritis (7). Initially,attention was focused on the circulatory disturbances of the upper extremities and the brain.Shimizu and Sano (9) defined the process as"chronic obliterative brachiocephalic arteries"and proposed the term' 'pulseless disease." How-

136 Y. SUZUKI, K. KONISHI AND K. HISADA October 1973
ever, it soon became clear that it could spreadfurther to the entire aorta and any of its branches(3, 5, 7).
A lesion in the pulmonary artery was firstdescribedin 1940 by Oota (8) and several articlesabout this entity have been published since thattime (3, 5-8). The lesion was often found. at thetrunk or main branches of the pulmonary artery(7). Kozuka et al. (6) reported that the lesionwas more likely to affect the upper part of theright lung. In our study, we also noted a slightlyhigher incidence in the right lung, but no particular part of the lung had a special tendency to beaffected.
Chest x ray may show decreased or sparseareas of lung vascularity in Takayasu's arteritis but it may often be difficult to detect suchsubtle changes in the lung field. In our study,all chest x-ray reports except one did not mentionany abnormal :findings in the lung field and nochange could be found retrospectively either.Without doubt, the chest film is very importantin the diagnosis of Takayasu's arteritis, but oneshould also .rcmember that chest x-ray alone isnot a sufficient screening test for the pulmonarylesion of Takayasu's arteritis.
Lung scanning is a nonspecific examination andany kind of lung disease may cause an abnormalityin the scan. Most lung diseases, however, couldbe ruled out by the chest radiograph taken at thetime of scanning. The abnormal lung scan inTakayasu's arteritis is similar to that in pulmonaryembolism, which shows decreased or absent perfusion corresponding to specific blood vessels, i.e.,subsegrnental, segmental, and lobar arteries, because the lesions are mainly in the pulmonaryarteries. Although it could be difficult to differentiate Takayasu's arteritis from pulmonaryembolism without clinical findings, there are somedifferences in the lung scans between these twodiseases. In pulmonary embolism, perfusiondefects often resolve, particularly in youngerpatients (2). On the other hand, perfusion de-
fects in Takayasu's arteritis do not change for along time. These findings might be useful inruling out pulmonary embolism.
Although pulmonary angiography should bedone to confirm pulmonary artery disorders inTakayasu's arteritis, the technique is not simple.Moreover, pulmonary angiography might not detect the lesion involving arteries smaller than 2 mmin diameter (2). Lung scanning is quite sensitivein the evaluation of pulmonary blood flow and thetechnique is simple and safe.
Our results have shown the high incidence ofpulmonary artery disorders in Takayasu's arteritis, so it seems reasonable to Screen these patientsby means of lung scanning. In the appropriateclinical setting, the abnormal lung scan with clearlungs on the chest radiograph makes the diagnosis of pulmonary artery disorders in Takayasu'sarteritis highly probable and pulmonary angiography should be done in these cases.
Department of Nuclear MedicineKanazawa University School of MedicineTakara-machi 13-1, Kanazawa-shiJapan
REFERENCES
1. Ask-Vpmark E: On the "pulseless disease" outside ofJapan. Acta Med Scandinav 149:161-178,1954
2. Deland FH, 'Wagner HN Jr: Atlas of Nuclear Medicine.Vol 2, Lung and Heart. Philadelphia, W. B. Saunders, 1st ed,1970, pp 54-55
3. Gotsman MS, Beck W, Schrire V: Selective angiography in arteritis of the aorta and its major branches. Radiology 88:232-248, Feb 1967
4. Grollman JH, Hanafee W: The roentgen diagnosis ofTakayasu's arteritis. Radiology 83:387-395, Sep 1964
5. Hachiya J: Current concepts of Takayasu's arteritis.Semin Roentgen 52:245-259, Jul1970
6. Kozuka T, Nosaki T, Sato K, et alr; Aortitis syndromewith special reference to pulmonary vascular changes. ActaRadiol [Diag] 7:25-32, Jan 1968
7. Nasu T: Pathology of pulseless disease. A systematicstudy and critical review of twenty-one autopsy cases reportedin Japan. Angiology 14:225-242, May 1963
8. Oota K: Ein seltener Fall von beiderseitegern CarotisSubclaviaverschluss. Trans Soc Path Tap 30:680-690, 1940
9. Shimizu K, Sano K: Pulseless disease. J NeuropathClin Neuroll:37-47, Jan 1951
10. Veda H, Morooka S, Ito I, et al: Clinical observationof 52 cases of aortitis syndrome. Jap Heart J 10:277-288, Jul1969