Embed Size (px)
Citation preview

Solitary Pulmonary Nodule
Military Medicine Radiology Corner, May 2010
Radiology Corner
Solitary Pulmonary Nodule Guarantor: LT Rebecca Johnson, MC, USN1 Contributors: LT Rebecca Johnson, MC, USN; COL Les Folio, USAF, MC, SFS 2
Note: This is the full text version of the radiology corner question published in the April 2010 issue, with the abbreviated answer in the May 2010 issue. 1
Over 150,000 solitary pulmonary nodules are found each year on chest imaging.1 The major concern of the patient is whether or not the nodule is cancerous. This can typically be difficult to distinguish from a benign cause on imaging studies alone. Characteristics of the mass seen on imaging studies can help to determine the likelihood that a mass is benign or malignant. These include size, border, density, growth over time, and calcifications. Patient characteristics such as age, smoking history, and history of cancer are also important and need to be taken into account. Through combination of both patient and mass characteristics, it is possible to determine if a mass is likely benign or malignant.
Introduction
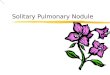
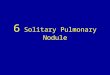
A 63 year old female presents to the ED in Augusta, GA while on vacation with a cough that has been worsening over the past two weeks. Seen previously by her primary care physician and treated with a cough suppressant. Her medical history is significant for left breast cancer treated by mastectomy. This patient has no history of tobacco use. A chest radiograph (Fig. 1) and CT (Fig. 2) were performed.
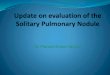
Summary of Imaging Findings A nodule is visible in the upper left upper lobe on the chest radiograph (Fig. 1). On CT, a nodule is seen in the left upper lobe measuring 2.93 cm x 2.34 cm with scalloped borders and no calcifications (Fig. 2).
1 School of Medicine, Uniformed Services University, Bethesda, Maryland
20814-4799 2 Department of Radiology and Radiological Sciences; Uniformed Services
University, Bethesda, Maryland 20814-4799 Reprint & Copyright © by Association of Military Surgeons of U.S., 2010.
Fig. 1a Chest radiograph demonstrating a left upper lobe pulmonary nodule.
Patient discussion:
Differentiating between a benign and malignant pulmonary nodule by imaging can be very difficult. Below are five imaging characteristics of a pulmonary nodule or mass that can be used to aid in differentiating the likelihood that a lesion is either benign or malignant. Patient and nodule characteristics can also be use to aid in determining the likelihood that a nodule or mass is benign or malignant shown in the chart below.

Report Documentation Page Form ApprovedOMB No. 0704-0188
Public reporting burden for the collection of information is estimated to average 1 hour per response, including the time for reviewing instructions, searching existing data sources, gathering andmaintaining the data needed, and completing and reviewing the collection of information. Send comments regarding this burden estimate or any other aspect of this collection of information,including suggestions for reducing this burden, to Washington Headquarters Services, Directorate for Information Operations and Reports, 1215 Jefferson Davis Highway, Suite 1204, ArlingtonVA 22202-4302. Respondents should be aware that notwithstanding any other provision of law, no person shall be subject to a penalty for failing to comply with a collection of information if itdoes not display a currently valid OMB control number.
1. REPORT DATE MAY 2010 2. REPORT TYPE
3. DATES COVERED 00-00-2010 to 00-00-2010
4. TITLE AND SUBTITLE Solitary Pulmonary Nodule
5a. CONTRACT NUMBER
5b. GRANT NUMBER
5c. PROGRAM ELEMENT NUMBER
6. AUTHOR(S) 5d. PROJECT NUMBER
5e. TASK NUMBER
5f. WORK UNIT NUMBER
7. PERFORMING ORGANIZATION NAME(S) AND ADDRESS(ES) Uniformed Services University of the Health Sciences,Department ofRadiology and Radiological Sciences,4301 Jones Bridge Road,Bethesda,MD,20814
8. PERFORMING ORGANIZATIONREPORT NUMBER
9. SPONSORING/MONITORING AGENCY NAME(S) AND ADDRESS(ES) 10. SPONSOR/MONITOR’S ACRONYM(S)
11. SPONSOR/MONITOR’S REPORT NUMBER(S)
12. DISTRIBUTION/AVAILABILITY STATEMENT Approved for public release; distribution unlimited
13. SUPPLEMENTARY NOTES
14. ABSTRACT
15. SUBJECT TERMS
16. SECURITY CLASSIFICATION OF: 17. LIMITATION OF ABSTRACT Same as
Report (SAR)
18. NUMBEROF PAGES
3
19a. NAME OFRESPONSIBLE PERSON
a. REPORT unclassified
b. ABSTRACT unclassified
c. THIS PAGE unclassified
Standard Form 298 (Rev. 8-98) Prescribed by ANSI Std Z39-18

Solitary Pulmonary Nodule
Military Medicine Radiology Corner, May 2010
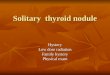
Fig. 1b Lateral chest radiograph demonstrating a left upper lobe pulmonary nodule.
Fig. 2 Chest CT demonstrates a solitary pulmonary nodule within the left upper lobe with scalloped borders without calcifications. Note breast implant on left.
Low Intermediate High1
Once the likelihood of benignity or malignancy for the nodule or mass in question has been determined, this can be used to aid in the differential diagnosis.
Benign nodules generally fall into two categories making up 90% of all benign lesions. These are infectious granulomas incorporating 80% of benign nodules and hamartomas comprising 10% of the remainder. Infectious granulomas are generally caused by fungi endemic to the environment or mycobacteria. Hamartomas will have areas of fat, muscle, myxomatous tissue, and fibroblastic tissue that may be able to be seen on imaging studies. It also classically has “popcorn” calcifications.1 Another benign albeit rarer diagnosis that can be considered in patients from the southern, southeastern and eastern coastal states is Dirofilariasis. This is more commonly Benign Malignant
known as the dog heart worm. Humans are infected through the bite of mosquitoes but as this is not the intended host subsequently die. The dead larvae embolize to the lungs and can form a non-calcified pleural based nodule.4
Diameter of nodule
<1.5 cm 1.5-2.2 cm >2.3cm
Age <45 45-60 >60
Smoking Status
Never Current (<20cig/d)
Current (>20cig/d)
Smoking Cessation
Quit >7 yr ago Quit <7 yr ago Never quit
Border Smooth Scalloped Corona radiata or spiculated
Size 80% of nodules <2cm
80% of nodules >3cm2 (ie. Mass)
Border 80% of nodules with smooth, discrete border
60% with scalloped border 90% with spiculated border 95% with corona radiata3
Calcifications Diffuse homogenous Central Laminated “Popcorn”
Any other pattern
Density *seldom used as different >164 HU
scanners vary at institutions <147 HU2
Growth Slow growing Doubling time of 20-400 d = 30% inc in diameter

Solitary Pulmonary Nodule
Military Medicine Radiology Corner, May 2010
In this patient, the nodule has a higher likelihood of malignancy due to its size, borders, and the age of the patient. Malignancies generally fall into three categories including primary lung cancer, carcinoid, and metastases. The location of a nodule or mass can be useful in developing a differential diagnosis as well. Primary lung cancers include the peripherally based adenocarcinoma and large cell carcinoma and the centrally based small cell and squamous cell carcinomas. Carcinoid is a well circumscribed mass generally centrally located although 20% can occur peripherally. Metastatic disease has a 25% probability of being the diagnosis when the patient has a history of extrathoracic malignancy as in this patient. The cancers most likely to metastasize to the lung include melanoma, sarcoma, and colon, breast, renal, and testicular carcinoma.5
Approach to Diagnosis
One area of imaging that is becoming more commonly used
to help determine if a mass is malignant or benign is positron-emission tomography (PET). This measures the glucose metabolism of tissues with malignancy generally having a higher rate of metabolism than a benign process. The sensitivity for identifying a malignant process is 96.8 percent with a specificity of 77.8 percent.6 This may also provide staging information and identify a primary malignancy in the case of a metastasis to the lung. While PET scans are expensive, this is generally a cost effective strategy since it has been shown to reduce the number of patients requiring surgery by up to 15 percent.1 If the likelihood of malignancy is much greater than the probability that the lung nodule is benign as in this patient, then tissue needs to be obtained for evaluation to determine what type of malignancy and thus what treatment options are available to the patient. The location of the lung nodule or mass plays a large role in determining which method is to be used for retrieving of a tissue sample. Bronchoscopy is one method for retrieving tissue non-surgically. The sensitivity is variable from 20-80 percent for detecting a malignant process depending upon the size and location of the lesion. When a bronchus leads to the mass, the sensitivity increases to 70 percent. Transthoracic fine-needle aspiration biopsy can also determine if a mass is malignant. It has an 80-95 percent sensitivity for malignant lesions. Even with small lesions of less than 2 cm, it has a 60 percent sensitivity for detecting a malignancy. Complication rates are higher with this procedure than
bronchoscopy with an incidence of pnuemothorax around 30 percent.
Determining the probability of cancer in a solitary
pulmonary lung nodule still remains inexact. Thus the characteristics of both the mass and the patient are a good starting point. Note: Follow this link for Category 1 CME or CNE in the case
of the week in the MedPix™ digital teaching file.
http://rad.usuhs.mil/medpix/medpix.html?mode=single&recnum=6969&th=-1#top
References
1 Ost, D, Fein, AM, Feinsilver, SH: Clinical practice. The solitary pulmonary nodule, N Engl J Med 2003; 248:2535. 2 Steele, JD: The solitary pulmonary nodule: report of a cooperative study of resected asymptomatic solitary pulmonary nodules in males. J Thorac, Cardiovasc Surg 1963; 46:21. 3 Rigler, LG: An overview of cancer of the lung, Semin Roentgenol 1977; 12:161. 4 Nicholson, CP, Allen, MS, Tastek, VF, et al: Dirofilariasis immitis: A rare, increasing cause of pulmonary nodules, Mayo Clin Proc 1992; 67:646. 5 Seo, JB, Im, JG, Goo, JM, et al: Atypical pulmonary metastases: spectrum of radiologic findings, Radiographics 2001; 21:403. 6 Gould MK, Maclean CC, Kuschner WG, Rydzak CE, Owens DK: Accuracy of positron emission tomography for diagnosis of pulmonary nodules and mass lesions: a meta-analysis, JAMA 2001;285:914-924