Embed Size (px)
Citation preview
Randomized trial
Randomized clinical trials to determine the role of topicalglyceryl trinitrate in peripheral intravenous nutrition
B. M. Dobbins, J. A. Catton, M. J. Tighe, G. V. Miller, I. G. Martin and M. J. McMahonAcademic Unit of Surgery, The General Infirmary at Leeds, Leeds, UKCorrespondence to: Mr B. M. Dobbins, Calderdale and Huddersfield NHS Trust, Acre Street, Lindley, Huddersfield HD3 3HE, UK(e-mail: [email protected])
Background: The contribution of glyceryl trinitrate (GTN) to prevention of peripheral veinthrombophlebitis (PVT) during peripheral intravenous nutrition delivered by fine-bore midlineintravenous catheter is unclear. The aim of this study was to establish its role.Methods: Two consecutive randomized clinical trials were conducted. In trial 1 patients were randomizedto receive standard peripheral intravenous nutrition containing heparin and hydrocortisone with orwithout the placement of a topical GTN patch (triple therapy or dual therapy). In trial 2 patients wererandomized to receive standard peripheral intravenous nutrition with either dual therapy or topical GTNalone (monotherapy).Results: Dual therapy was as effective as triple therapy in preventing PVT (incidence 10 of 37 versus 11of 39 patients respectively). Dual therapy reduced the incidence and increased the time to onset of PVTcompared with monotherapy (14 of 41 versus 22 of 35 patients respectively, P = 0·012; median 17·3 (95per cent confidence interval (c.i.) 13·4 to 21·1) versus 8·9 (95 per cent c.i. 6·7 to 11·0) days, P = 0·007).Conclusion: Use of a topical GTN patch confers no benefit when peripheral intravenous nutrition isdelivered via a fine-bore midline intravenous catheter.
Paper accepted 8 March 2003Published online in Wiley InterScience (www.bjs.co.uk). DOI: 10.1002/bjs.4205
Introduction
Intravenous nutrition (IVN) is an invaluable technique forthe administration of daily nutritional requirements whenthe enteral route cannot be used. IVN is usually adminis-tered via a central venous catheter. Despite improvementsin catheter design and administration devices, as well asimproved training and catheter care, complications associ-ated with central venous catheters still occur1.
Infusion of IVN via a peripheral vein avoids many of thepotential complications of central venous catheterization,but peripheral vein thrombophlebitis (PVT) is a majorproblem even with infusion of electrolytes2,3. The onsetof PVT is influenced by various factors, including catheterand cannula design4–6, and feed characteristics such asosmolality7, pH8 and lipid content9. Use of topicalglyceryl trinitrate (GTN) patches10, non-steroidal anti-inflammatory preparations11, and the addition of heparinand hydrocortisone12–14 to the intravenous feed have allbeen shown to be effective in preventing PVT14.
A combination of therapies (topical GTN patch and theaddition of heparin and hydrocortisone to the feed – tripletherapy) used with a fine-bore polyurethane midlinecatheter has been shown significantly to reduce theincidence and to delay the onset of PVT15, even withthe use of high-osmolarity feeds that provide full IVN.The extent to which each of these therapies contributesto this antiphlebitic effect is unknown. Vasoconstrictionis thought to be one of the events that trigger thedevelopment of PVT16. Topical GTN patches are believedto have a vasodilatory effect when used as prophylaxisduring delivery of peripheral IVN10. There is evidenceto support this theory when short polytetrafluoroethylene(PTFE) cannulas are used for peripheral IVN, but notfor fine-bore polyurethane midline catheters. Recentultrasonographic studies have suggested that topical GTNdoes not have a vasodilatory effect on upper arm veins17
commonly used for the insertion of fine-bore midlinecatheters, nor does the delivery of IVN through thesecatheters appear to induce vasoconstriction18. The vein
Copyright 2003 British Journal of Surgery Society Ltd British Journal of Surgery 2003; 90: 804–810Published by John Wiley & Sons Ltd
B. M. Dobbins, J. A. Catton, M. J. Tighe et al. ž Glyceryl trinitrate during intravenous nutrition 805
used for cannulation may also have a significant effect onthe development of PVT when this type of catheter isemployed19.
This study was designed to assess the role of topicalGTN in preventing PVT. Two consecutive randomizedclinical trials were used to compare dual therapy(heparin and hydrocortisone) with triple therapy (heparin,hydrocortisone and topical GTN), and dual therapy withmonotherapy (topical GTN alone).
Patients and methods
The studies were carried out between January 1997 and July1998 among patients who were referred to the NutritionalSupport Service at the General Infirmary in Leeds. Localresearch ethics committee approval for each clinical trialwas granted and informed consent was obtained fromeach participating patient. Eligibility criteria for entry intothe study were the presence of an adequate peripheralvein in the antecubital fossa and the expectation thatnutritional support would be required for more than 7 days.A suitable vein was defined as a palpable, patent vein ineither proximal forearm or antecubital fossa, large enoughto permit cannulation with the fine-bore polyurethanemidline catheter. Patients were excluded if the decision tofeed centrally or by the peripheral route had been made
before starting the feed or if placement of the midlinecatheter was unsuccessful.
A fine-bore polyurethane midline catheter (22G, SecalonHydrocathTM; Ohmeda, Swindon, UK) was inserted intothe chosen vein using a strict aseptic protocol, by anexperienced practitioner. The catheter was inserted for alength of 15 cm into the vein, ensuring that the tip laywithin the arm and proximal to the axillary vein. Localanaesthetic was used and the catheter was secured inplace with fine silk sutures and a transparent occlusivedressing (TegadermTM; 3M Medical Surgical Division, StPaul, Minnesota, USA). Normal saline was infused slowlythrough the catheter to maintain patency before startingthe intravenous feed. A standard feed, as used routinely viathe central venous route, was administered to all patients.The feed provided 1800 kcal of non-protein energy perday, consisting of 800 kcal from glucose (Fresenius HealthCare Group, Basingstoke, UK), and 1000 kcal in the formof 20 per cent lipid (Soyacal 20%; Alpha Therapeutics,Thetford, Norfolk, UK). The feed also contained 13 gnitrogen as amino acids (Freamine III; McGaw, Irving,Texas, USA) and supplied 130 mmol sodium and 80 mmolpotassium in a total volume of 2500 ml. The osmolality ofthe feed was 1190 mOsm/kg. The stability of heparin andhydrocortisone in the standard feed was confirmed beforethe start of the study.
Table 1 Patient demographics
Trial 1 Trial 2
Triple therapy(n = 39)
Dual therapy(n = 37)
Dual therapy(n = 41)
Monotherapy(n = 35)
Age (years)* 60 (51–76) 65 (49–77) 63 (40–71) 64 (48–74)Sex ratio (M : F) 24 : 15 24 : 13 25 : 16 23 : 12Vein inserted
Basilic — — 29 24Cephalic — — 12 11
Total period of feeding (days)* 9·9 (7·7–12·2) 9·8 (8·3–11·2) 8·5 (6·9–10·1) 6·7 (5·5–8·0)
*Values are median (interquartile range).
Table 2 Indications for intravenous nutritional support
Trial 1 Trial 2
Triple therapy(n = 39)
Dual therapy(n = 37)
Dual therapy(n = 41)
Monotherapy(n = 35)
Upper gastrointestinal malignancy 18 15 10 12Colorectal malignancy 4 4 8 2Pancreatitis 9 4 7 3Inflammatory bowel disease 2 7 7 6Vascular disease 1 1 3 6Other 5 6 6 6
Copyright 2003 British Journal of Surgery Society Ltd www.bjs.co.uk British Journal of Surgery 2003; 90: 804–810Published by John Wiley & Sons Ltd
806 Glyceryl trinitrate during intravenous nutrition ž B. M. Dobbins, J. A. Catton, M. J. Tighe et al.
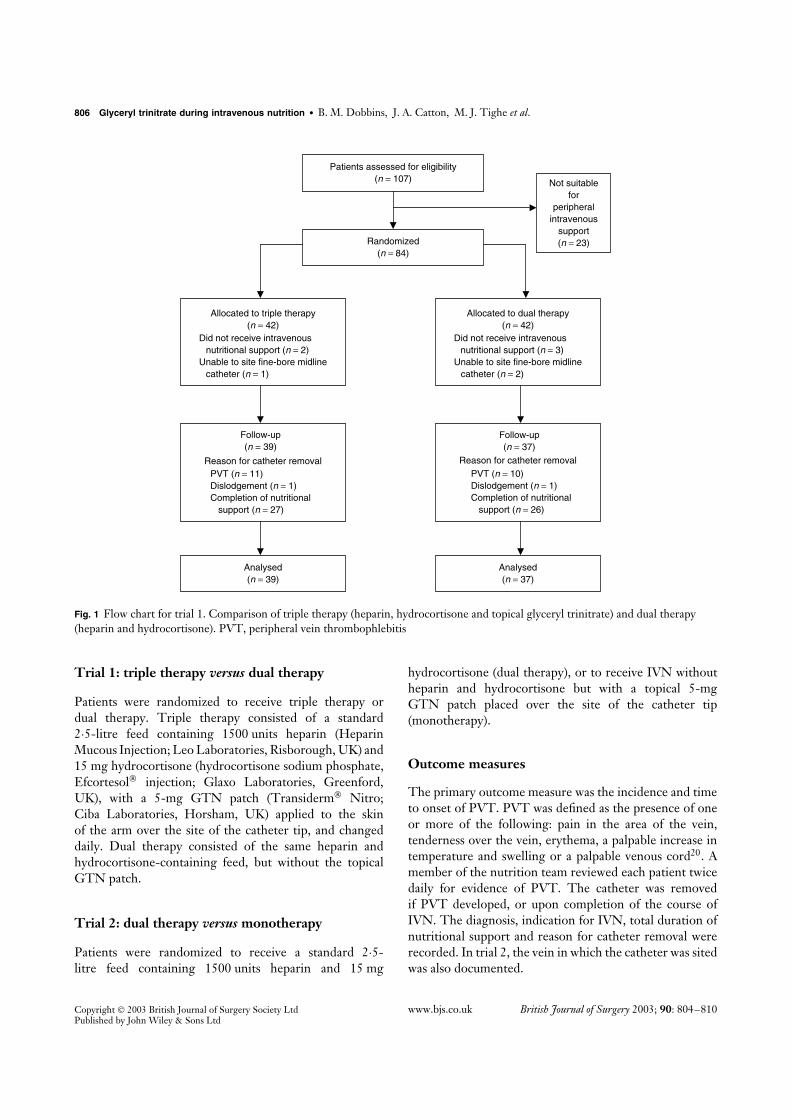
Patients assessed for eligibility(n = 107)
Randomized(n = 84)
Allocated to triple therapy(n = 42)
Did not receive intravenous nutritional support (n = 2)Unable to site fine-bore midline catheter (n = 1)
Analysed(n = 39)
Allocated to dual therapy(n = 42)
Did not receive intravenous nutritional support (n = 3)Unable to site fine-bore midline catheter (n = 2)
Analysed(n = 37)
Not suitablefor
peripheralintravenous
support(n = 23)
Reason for catheter removal
Follow-up(n = 37)
PVT (n = 10)Dislodgement (n = 1)Completion of nutritional support (n = 26)
Follow-up(n = 39)
Reason for catheter removalPVT (n = 11)Dislodgement (n = 1)Completion of nutritional support (n = 27)
Fig. 1 Flow chart for trial 1. Comparison of triple therapy (heparin, hydrocortisone and topical glyceryl trinitrate) and dual therapy(heparin and hydrocortisone). PVT, peripheral vein thrombophlebitis
Trial 1: triple therapy versus dual therapy
Patients were randomized to receive triple therapy ordual therapy. Triple therapy consisted of a standard2·5-litre feed containing 1500 units heparin (HeparinMucous Injection; Leo Laboratories, Risborough, UK) and15 mg hydrocortisone (hydrocortisone sodium phosphate,Efcortesol injection; Glaxo Laboratories, Greenford,UK), with a 5-mg GTN patch (Transiderm Nitro;Ciba Laboratories, Horsham, UK) applied to the skinof the arm over the site of the catheter tip, and changeddaily. Dual therapy consisted of the same heparin andhydrocortisone-containing feed, but without the topicalGTN patch.
Trial 2: dual therapy versus monotherapy
Patients were randomized to receive a standard 2·5-litre feed containing 1500 units heparin and 15 mg
hydrocortisone (dual therapy), or to receive IVN withoutheparin and hydrocortisone but with a topical 5-mgGTN patch placed over the site of the catheter tip(monotherapy).
Outcome measures
The primary outcome measure was the incidence and timeto onset of PVT. PVT was defined as the presence of oneor more of the following: pain in the area of the vein,tenderness over the vein, erythema, a palpable increase intemperature and swelling or a palpable venous cord20. Amember of the nutrition team reviewed each patient twicedaily for evidence of PVT. The catheter was removedif PVT developed, or upon completion of the course ofIVN. The diagnosis, indication for IVN, total duration ofnutritional support and reason for catheter removal wererecorded. In trial 2, the vein in which the catheter was sitedwas also documented.
Copyright 2003 British Journal of Surgery Society Ltd www.bjs.co.uk British Journal of Surgery 2003; 90: 804–810Published by John Wiley & Sons Ltd
B. M. Dobbins, J. A. Catton, M. J. Tighe et al. ž Glyceryl trinitrate during intravenous nutrition 807
Patients assessed for eligibility(n = 111)
Randomized(n = 84)
Allocated todual therapy
(n = 42)Did not receive intravenous
nutritional support (n = 0)Unable to site fine-bore midline
catheter (n = 1)
Analysed(n = 41)
Analysed(n = 35)
Not suitablefor
peripheralintravenous
support(n = 27)
Allocated tomonotherapy
(n = 42)Did not receive intravenous
nutritional support (n = 4)Unable to site fine-bore midline
catheter (n = 3)
Follow-up(n = 41)
Reason for catheter removalPVT (n = 14)Dislodgement (n = 3)Occlusion (n = 1)Completion of nutritional
support (n = 23)
Follow-up(n = 35)
Reason for catheter removalPVT (n = 22)Dislodgement (n = 3)Completion of nutritional
support (n = 10)
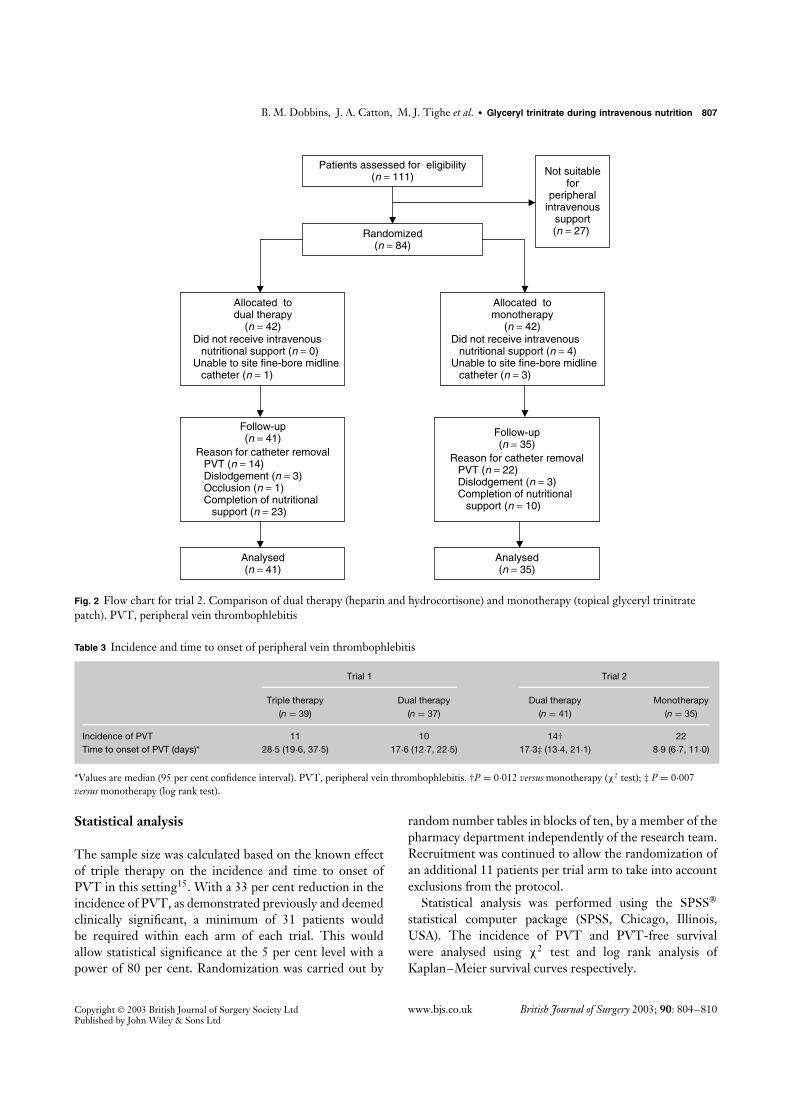
Fig. 2 Flow chart for trial 2. Comparison of dual therapy (heparin and hydrocortisone) and monotherapy (topical glyceryl trinitratepatch). PVT, peripheral vein thrombophlebitis
Table 3 Incidence and time to onset of peripheral vein thrombophlebitis
Trial 1 Trial 2
Triple therapy(n = 39)
Dual therapy(n = 37)
Dual therapy(n = 41)
Monotherapy(n = 35)
Incidence of PVT 11 10 14† 22Time to onset of PVT (days)* 28·5 (19·6, 37·5) 17·6 (12·7, 22·5) 17·3‡ (13·4, 21·1) 8·9 (6·7, 11·0)
*Values are median (95 per cent confidence interval). PVT, peripheral vein thrombophlebitis. †P = 0·012 versus monotherapy (χ2 test); ‡ P = 0·007versus monotherapy (log rank test).
Statistical analysis
The sample size was calculated based on the known effectof triple therapy on the incidence and time to onset ofPVT in this setting15. With a 33 per cent reduction in theincidence of PVT, as demonstrated previously and deemedclinically significant, a minimum of 31 patients wouldbe required within each arm of each trial. This wouldallow statistical significance at the 5 per cent level with apower of 80 per cent. Randomization was carried out by
random number tables in blocks of ten, by a member of thepharmacy department independently of the research team.Recruitment was continued to allow the randomization ofan additional 11 patients per trial arm to take into accountexclusions from the protocol.
Statistical analysis was performed using the SPSS
statistical computer package (SPSS, Chicago, Illinois,USA). The incidence of PVT and PVT-free survivalwere analysed using χ2 test and log rank analysis ofKaplan–Meier survival curves respectively.
Copyright 2003 British Journal of Surgery Society Ltd www.bjs.co.uk British Journal of Surgery 2003; 90: 804–810Published by John Wiley & Sons Ltd
808 Glyceryl trinitrate during intravenous nutrition ž B. M. Dobbins, J. A. Catton, M. J. Tighe et al.
Time from onset of feeding (days)
151050
Pro
babi
lity
of r
emai
ning
PV
T fr
ee
1·0
0·9
0·8
0·7
0·6
0·5
0·4
0·3
0·2
0·1
Triple therapy
Dual therapy
39
37
35
35
14
18
16
3
Triple therapy
Dual therapy
No. at risk
Fig. 3 Probability of a fine-bore polyurethane midline catheterremaining free from peripheral vein thrombophlebitis (PVT)with the use of triple therapy (heparin, hydrocortisone andtopical glyceryl trinitrate patch) or dual therapy (heparin andhydrocortisone). P = 0·946 (log rank test)
Time from onset of feeding (days)
151050
Pro
babi
lity
of r
emai
ning
PV
T fr
ee
1·0
0·9
0·8
0·7
0·6
0·5
0·4
0·3
0·2
0·1
Dual therapy
Monotherapy
Dual therapy 41
35Monotherapy
34
24
13
75
1
No. at risk
Fig. 4 Probability of a fine-bore polyurethane midline catheterremaining free from peripheral vein thrombophlebitis (PVT)with the use of dual therapy (heparin and hydrocortisone) ormonotherapy (topical glyceryl trinitrate patch). P = 0·012 (logrank test)
Results
There were no significant differences in age, sex (Table 1)and indication for feeding (Table 2) between patients in thetwo arms of either trial. Flow diagrams for each trial aregiven in Figs 1 and 2.
Trial 1: triple therapy versus dual therapy
Seventy-six patients completed the trial and were included
Time from onset of feeding (days)
151050
Pro
babi
lity
of r
emai
ning
PV
T fr
ee
1·0
0·9
0·8
0·7
0·6
0·5
0·4
0·3
0·2
0·1
Basilic vein
Cephalic vein
No. at riskBasilic vein 53 43 18 6Cephalic vein 23 15 2 0
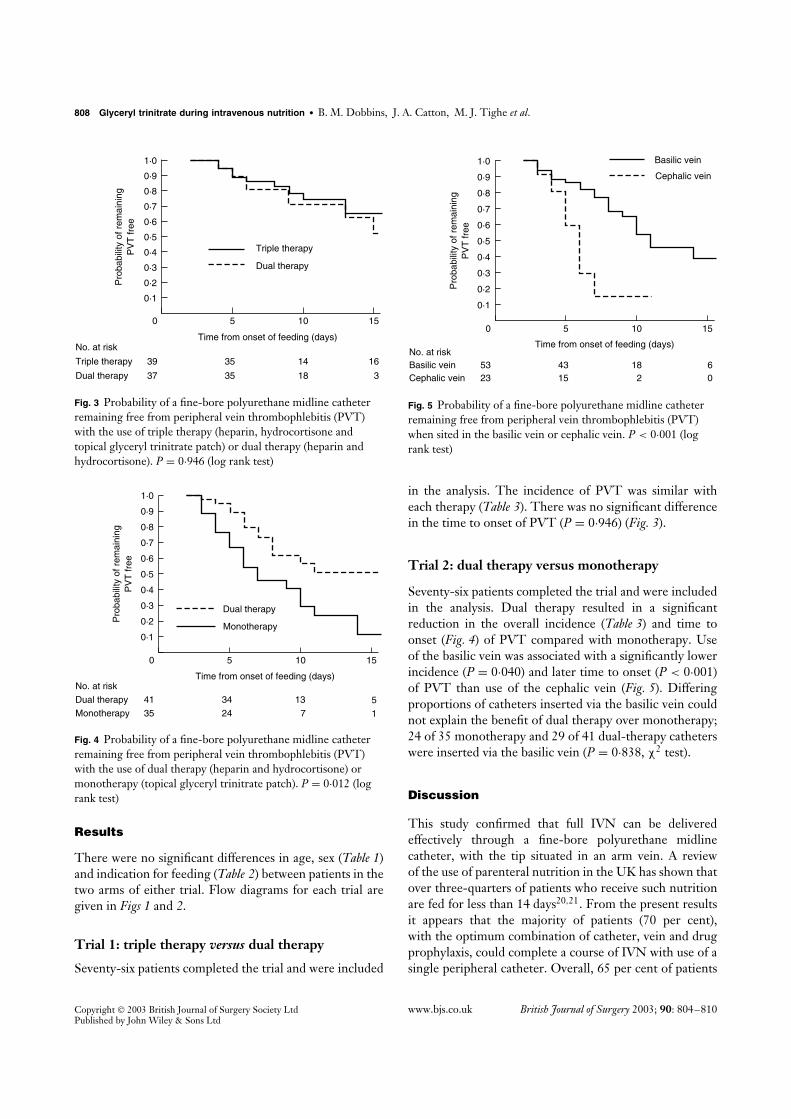
Fig. 5 Probability of a fine-bore polyurethane midline catheterremaining free from peripheral vein thrombophlebitis (PVT)when sited in the basilic vein or cephalic vein. P < 0·001 (logrank test)
in the analysis. The incidence of PVT was similar witheach therapy (Table 3). There was no significant differencein the time to onset of PVT (P = 0·946) (Fig. 3).
Trial 2: dual therapy versus monotherapy
Seventy-six patients completed the trial and were includedin the analysis. Dual therapy resulted in a significantreduction in the overall incidence (Table 3) and time toonset (Fig. 4) of PVT compared with monotherapy. Useof the basilic vein was associated with a significantly lowerincidence (P = 0·040) and later time to onset (P < 0·001)of PVT than use of the cephalic vein (Fig. 5). Differingproportions of catheters inserted via the basilic vein couldnot explain the benefit of dual therapy over monotherapy;24 of 35 monotherapy and 29 of 41 dual-therapy catheterswere inserted via the basilic vein (P = 0·838, χ2 test).
Discussion
This study confirmed that full IVN can be deliveredeffectively through a fine-bore polyurethane midlinecatheter, with the tip situated in an arm vein. A reviewof the use of parenteral nutrition in the UK has shown thatover three-quarters of patients who receive such nutritionare fed for less than 14 days20,21. From the present resultsit appears that the majority of patients (70 per cent),with the optimum combination of catheter, vein and drugprophylaxis, could complete a course of IVN with use of asingle peripheral catheter. Overall, 65 per cent of patients
Copyright 2003 British Journal of Surgery Society Ltd www.bjs.co.uk British Journal of Surgery 2003; 90: 804–810Published by John Wiley & Sons Ltd

B. M. Dobbins, J. A. Catton, M. J. Tighe et al. ž Glyceryl trinitrate during intravenous nutrition 809
in the dual- and triple-therapy groups completed a courseof IVN using a single fine-bore midline catheter.
The use of a topical GTN patch conferred no additionalbenefit, and used alone was less effective than low-doseheparin and hydrocortisone in preventing PVT. Thisresult differs from the findings of studies that employedshort cannulas, in which a topical GTN patch appeared tobe effective in preventing PVT13,22 One interpretationof this difference is that vasoconstriction may occurmore readily around short cannulas. Alternatively, a shortcannula may occlude the vein more easily than a fine-boremidline catheter, making venodilatation more importantto maintain blood flow and prevent PVT.
The results of the present study suggest that dualtherapy with the addition of heparin and hydrocortisone,in the doses stated, is effective for the prevention of PVT.Further work is needed to establish the individual effectsand optimal dosage of heparin and hydrocortisone. Thelow doses of heparin and hydrocortisone used suggesta local rather than systemic effect in prevention ofthrombophlebitis in the catheterized vein. The effect ofGTN on the smooth muscle of the veins is also thoughtto be more pronounced locally23,24, although its systemiceffects are clearly seen in patients who experience GTN-induced headache.
The placement of the GTN patches directly over thecatheter tip of a fine-bore midline catheter would appearto be less predictable than over a short cannula. However,placement of GTN patches close to the vein, rather thandirectly over the vein itself, has been shown not to influencethe local effects of GTN22. The basilic and cephalic veinsare relatively constant in their anatomical position, andplacement of the patches on the medial or lateral aspect ofthe upper arm, 15 cm from the catheter insertion site, islikely to provide a similar local GTN effect to that of otherstudies in which short cannulas have been used.
The stability of heparin and hydrocortisone in the feedused was established in this study (on the proviso thatinfusion took place within 24 h of addition), but concernsabout stability with respect to the potential of heparin toform heparin–lipid complexes have been raised25. Lowmolecular weight heparins are believed to offer greaterstability in lipid admixtures26 but their benefit in preventingPVT during peripheral intravenous nutritional support isunknown. Further studies will be required to establish theirrole and the appropriate dose.
The finding of a lower incidence of PVT when thecatheter lay in the basilic vein rather than the cephalicvein confirmed previous observations with the use offine-bore midline catheters27. The basilic vein, unlike thecephalic, is not subcutaneous and is therefore less prone
to fluctuations in ambient temperature. Vasoconstrictionin response to a decrease in ambient temperature in thesubcutaneously positioned cephalic vein may alter the flowrate, predisposing to the development of thrombophlebitis.The ability of the fine-bore midline catheter to ‘float’ in thelumen of the vein, without traumatizing the endothelium,may also be increased in the larger basilic vein19. Thediameter of the cephalic vein is significantly smaller in theupper arm than in the antecubital fossa. The basilic veindiameter appears to increase as it ascends the arm17, andthis will allow a greater flow rate and more rapid dilutionof the hypertonic IVN solution.
The role that infection plays in the pathogenesis of PVTwith fine-bore peripheral catheters is unclear. Although‘septic’ thrombophlebitis is encountered occasionally,infection of peripheral feeding catheters has largely beenignored. Catheter-related bloodstream infection associatedwith central venous catheters is a major source ofmorbidity28, and the incidence increases with dwell time29.The prolonged life of peripheral catheters, as seen inthis study, may therefore increase the potential risk ofcatheter-related bloodstream infection.
Some authors have advocated 24-h rotation of cannulasfor peripheral IVN to prevent PVT9,30. A similarpolicy with fine-bore midline catheters may reduce thecomplications of PVT further. The median duration ofIVN via fine-bore midline catheters is 9 days in this unitand so the majority of patients may be fed using only twoperipheral catheters, with a rotational system of between 5and 7 days.
In most published reports of peripheral IVN, theosmolality of the feed was significantly reduced to preventPVT. The present authors have used standard feedsthat offer full nutritional support, and the results clearlydemonstrate that prolonged peripheral feeding does notrequire compromise of optimal protein and calorificprovision31.
The use of topical GTN patches when full IVNcontaining heparin and hydrocortisone is delivered viaa fine-bore midline catheter can no longer be advocated.The choice of vein is also important in the delivery ofperipheral IVN, as the basilic vein was associated with alower incidence and longer time to onset of PVT.
References
1 Mughal MM. Complications of intravenous feedingcatheters. Br J Surg 1989; 76: 15–21.
2 Collin J, Collin C, Constable FL, Johnston ID. Infusionthrombophlebitis and infection with various cannulas. Lancet1975; ii: 150–153.
Copyright 2003 British Journal of Surgery Society Ltd www.bjs.co.uk British Journal of Surgery 2003; 90: 804–810Published by John Wiley & Sons Ltd

810 Glyceryl trinitrate during intravenous nutrition ž B. M. Dobbins, J. A. Catton, M. J. Tighe et al.
3 Tanner WA, Delaney PV, Hennessy TP. The influence ofheparin on intravenous infusions: a prospective study. Br JSurg 1980; 67: 311–312.
4 Madan M, Alexander DJ, McMahon MJ. Influence ofcatheter type on occurrence of thrombophlebitis duringperipheral intravenous nutrition. Lancet 1992; 339: 101–103.
5 May J, Murchan P, MacFie J, Sedman P, Donat R, Palmer Det al. Prospective study of the aetiology of infusion phlebitisand line failure during peripheral parenteral nutrition. Br JSurg 1996; 83: 1091–1094.
6 Reynolds JV, Walsh K, Ruigrok J, Hyland JM. Randomisedcomparison of silicone versus Teflon cannulas for peripheralintravenous nutrition. Ann R Coll Surg Engl 1995; 77:447–449.
7 Bayer-Berger M, Chiolero R, Freeman J, Hirschi B.Incidence of phlebitis in peripheral parenteral nutrition:effect of different nutrient solutions. Clin Nutr 1989; 8:181–186.
8 Fonkalsrud EW, Carpenter K, Masuda JY, Beckerman JH.Prophylaxis against postinfusion phlebitis. Surg Gynecol Obstet1971; 133: 253–256.
9 Nordenstrom J, Jeppsson B, Loven L, Larsson J. Peripheralparenteral nutrition: effect of a standardized compoundedmixture on infusion phlebitis. Br J Surg 1991; 78:1391–1394.
10 Khawaja HT, Williams JD, Weaver PC. Transdermalglyceryl trinitrate to allow peripheral total parenteralnutrition: a double-blind placebo controlled feasibility study.J R Soc Med 1991; 84: 69–72.
11 Payne-James JJ, Bray MJ, Kapadia S, Rana SK,McSwiggan D, Silk DB. Topical nonsteroidalanti-inflammatory gel for the prevention of peripheral veinthrombophlebitis. A double-blind, randomised,placebo-controlled trial in normal subjects. Anaesthesia 1992;47: 324–326.
12 Madan M, Alexander DJ, Mellor E, Cooke J, McMahon MJ.A randomised study of the effects of osmolarity and heparinwith hydrocortisone on thrombophlebitis in peripheralintravenous nutrition. Clin Nutr 1991; 10: 309–314.
13 Messing B, Leverve X, Riguard D, Krummel Y, Botta D,Laterget J et al. Peripheral venous complications of ahyperosmolar (960mOsm) nutritive mixture. A multicenterdouble-blinded random study in 98 patients. Clin Nutr 1986;5: 57–61.
14 Reid I, Keane FBV, Monson JRT, Tanner WA.Thrombophlebitis following peripherally infused parenteralnutrition: a randomised clinical study of the effects ofadditives. Surg Res Commun 1990; 9: 69–77.
15 Tighe MJ, Wong C, Martin IG, McMahon MJ. Do heparin,hydrocortisone, and glyceryl trinitrate influencethrombophlebitis during full intravenous nutrition via aperipheral vein? JPEN J Parenter Enteral Nutr 1995; 19:507–509.
16 Woodhouse CR. Infusion thrombophlebitis: the histologicaland clinical features. Ann R Coll Surg Engl 1980; 62: 364–368.
17 Everitt NJ. Ultrasonic investigation of the effect of topicalglyceryl trinitrate on peripheral arm vein diameter:implications for intravenous nutrition. JPEN J ParenterEnteral Nutr 1999; 23: 360–362.
18 Everitt NJ. Effect of prolonged infusion on vein calibre: aprospective study. Ann R Coll Surg Engl 1999; 81: 109–112.
19 Everitt NJ, Madan M, Alexander DJ, McMahon MJ. Finebore silicone rubber and polyurethane catheters for thedelivery of complete intravenous nutrition via a peripheralvein. Clin Nutr 1993; 12: 261–265.
20 Maddox RR, Rush DR, Rapp RP, Foster TS, Mazella V,McKean HE. Double-blind study to investigate methods toprevent cephalothin-induced phlebitis. Am J Hosp Pharm1977; 34: 29–34.
21 Payne-James JJ, De Gara CJ, Grimble GK, Bray MJ,Rana SK, Kapadia S et al. Artificial nutrition support inhospitals in the United Kingdom – 1991: second nationalsurvey. Clin Nutr 1991; 11: 187–192.
22 Wright A, Hecker JF, Lewis GB. Use of transdermal glyceryltrinitrate to reduce failure of intravenous infusion due tophlebitis and extravasation. Lancet 1985; ii: 1148–1150.
23 Franks AG Jr. Topical glyceryl trinitrate as adjunctivetreatment in Raynaud’s disease. Lancet 1982; i: 76–77.
24 Hecker JF, Lewis GB, Stanley H. Nitroglycerine ointment asan aid to venepuncture. Lancet 1983; i: 332–333.
25 Rattenbury JM, Timmins JG, Cawthorne EA, Ganapathy S,Taylor CJ. Identification of the cause of separation(creaming) of lipid emulsions in intravenous infusion.J Pediatr Gastroenterol Nutr 1989; 8: 491–495.
26 Durand M-C, Barnett M. Heparin in parenteral feeding:effect of heparin and low molecular weight heparin on lipidemulsions and all-in-one admixtures. Br J Intensive Care1992; 2: 10–20.
27 Everitt NJ, McMahon MJ. Influence of fine-bore catheterlength on infusion thrombophlebitis in peripheralintravenous nutrition: a randomised controlled trial. Ann RColl Surg Engl 1997; 79: 221–224.
28 Fletcher SJ. Central venous catheter related infection.Anaesth Intensive Care 1999; 27: 425.
29 Darouiche RO, Raad II, Heard SO, Thornby JI,Wenker OC, Gabrielli A et al. A comparison of twoantimicrobial-impregnated central venous catheters.Catheter Study Group. N Engl J Med 1999; 340: 1–8.
30 Palmer D, MacFie J, Bradford IM, Murchan PM, Harrison J,Mitchell CJ. Administration of peripheral parenteral nutri-tion: a prospective study comparing rotation of venous accesssites with ultrafine cannulas. Clin Nutr 1996; 15:311–315.
31 Williams N, Wales S, Irving MH. Prolonged peripheralparenteral nutrition with an ultrafine cannula andlow-osmolality feed. Br J Surg 1996; 83: 114–116.
Copyright 2003 British Journal of Surgery Society Ltd www.bjs.co.uk British Journal of Surgery 2003; 90: 804–810Published by John Wiley & Sons Ltd