Embed Size (px)
Citation preview

Vol. 109 No. 3 March 2010
CLINICOPATHOLOGIC CONFERENCE Editor: Paul C. Edwards
Rapidly progressing mass of anterior mandible following adental extractionA. Fasanmade, BDS, MBBS, FDSRCS, MRCS, FRCS,a M. Pring, BDS, FDSRCS, FRCPath,b
J. Pawade, MBBS, FRCPath,b P. Guest, BDS, MBBS, FDSRCS, FRCS,a andC. Bell, BDS, MSc, FDSRCS,a Bristol, United KingdomUNITED BRISTOL NATIONAL HEALTH SERVICE FOUNDATION TRUST
(Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2010;109:330-334)CLINICAL PRESENTATIONA 75-year-old woman was referred to the department
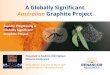
of oral and maxillofacial surgery for extraction of alone standing symptomatic mandibular right caninetooth. Clinically, the tooth was mobile (grade II). Theassociated free gingiva demonstrated erythema and gin-gival recession. There was no discharging sinus, mass,or other clinically evident soft tissue pathology noted.A periapical radiograph (Fig. 1) showed no secondarycaries of this restored tooth, although there was evidenceof mesial and distal bone loss with an intact dental lamina,consistent with chronic periodontal bone loss.
The patient’s previous clinical history included ade-nocarcinoma of the left breast 4 years before, for whichshe underwent radical left mastectomy and axillaryclearance for metastatic disease. Disease recurrence 3years later was successfully treated with systemic che-motherapy but was complicated by the development ofthrombocytopenia as a result of direct myelosuppres-sion. In addition, there was an associated abnormalityin the megakaryocytic lineage suggestive of a myelo-proliferative disorder (myelofibrosis). She had re-mained under the care of hematology specialists. Lab-oratory studies demonstrated low hemoglobin (10.1g/dL; normal 12-16 g/dL) and platelet counts (18 �109/L; normal 140-440 � 109/L) with a normal white
aDepartment of Oral and Maxillofacial Surgery.bDepartment of Pathology.Received for publication Oct 16, 2007; returned for revision Oct 2,2009; accepted for publication Oct 28, 2009.1079-2104/$ - see front matter© 2010 Mosby, Inc. All rights reserved.
doi:10.1016/j.tripleo.2009.10.051330
cell count (6.81 � 109/L; normal 4-11 � 109/L). Anuneventful dental extraction was performed after thepatient was prophylactically administered 2 units ofplatelets by our hematology colleagues. A biopsy wasnot obtained at that time, because there was no mass,sinus, or ulceration at initial presentation.
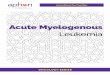
The patient presented 8 days after surgery complain-ing of intermittent bleeding from the extraction site. Onexamination, there was a 2 � 1.5 cm exophytic ulcer-ated granular mass arising from the extraction socket.The margins of the ulcerated surface had a brown togreenish hue (Fig. 2).
DIFFERENTIAL DIAGNOSISOur diagnostic consideration for this rapidly growing
exophytic soft tissue mass included pyogenic granu-loma (epulis granulomatosum), metastatic breast carci-noma, a preexisting primary gingival squamous cellcarcinoma, non-Hodgkin lymphoma including plasma-blastic lymphoma, and bacillary angiomatosis.
Pyogenic granuloma (PG) featured high on our dif-ferential diagnosis. PG is a common benign inflamma-tory hyperplasia seen in the oral cavity and on the skin.It arises in response to various stimuli, including localirritation, trauma, and hormonal changes. Seventy-fivepercent of all cases of oral PG occur on the gingiva,where they are thought to be associated with calculusdeposits within the gingival crevice.1 The term epulisgranulomatosum refers to a PG emanating post-surgi-cally from a dental extraction socket.2 PG presents as acompressible lobulated exophytic mass which may besessile or pedunculated with small erythematous pap-
ules present on its surface. It rarely exceeds 2.5 cm in
OOOOEVolume 109, Number 3 Fasanmade et al. 331
size. Its development is typically slow, asymptomatic,and painless but may grow rapidly, reaching its fullextent in weeks,1 mimicking some of the clinical fea-tures in the present case. Although the lesion in thiscase closely resembled a PG, it was important to ex-clude other causes, especially in view of the patient’smedical history.
Intraoral metastatic disease is a rare phenomena,representing �1% of all oral tumors. The mandible ismore frequently involved than the maxilla.3 Signs andsymptoms of metastatic jaw lesions include bone pain,swelling, mobile teeth, pathologic fracture, and numb-ness involving the inferior dental nerve. Carcinomas ofthe breast, kidney, lung, gastrointestinal tract, thyroid,and prostate may metastasize to the jaws.4 Metastaticbreast adenocarcinoma to the jaw was given seriousconsideration in view of our patient’s prior history ofbreast adenocarcinoma.
Non-Hodgkin lymphoma (NHL) occurs more com-monly within lymph nodes but may present as extran-odal disease, involving the oral cavity. Intraoral lym-phomas may involve either bone or soft tissue. NHLcan involve soft tissue of any region of the mouth,although it more commonly presents as an enlargementor swelling of the gingivae.5 NHL involving the jawmore frequently affects the mandible. These usuallypresent with pain and swelling, although alveolar bone
Fig. 1. Periapical radiograph of mandibular right canine be-fore extraction, showing localized alveolar bone loss.
enlargement may be the only initial presenting sign.
Loosening of teeth is also a common feature. Radio-logic signs may include a poorly defined irregular ra-diolucency, displacement of associated teeth and rootresorption may be noted. Acquired immune deficiencysyndrome (AIDS)–related NHL often manifests as ex-tranodal lesions in the oral mucosa.6 Plasmablasticlymphoma (PBL) is a subtype of diffuse large B-celllymphoma occurring almost exclusively in individualsinfected with the human immunodeficiency virus (HIV)and tends to arise in the oral cavity and jaws.5 It ofteninvolves the gingiva, with minimal erosion of underly-ing bone. PBL has been reported in individuals withoutHIV infection, but this is rare.7 NHL was considered inour differential diagnosis but was deemed to be un-likely based on the clinical presentation.
Bacillary angiomatosis (BA) is an atypical subcuta-neous vascular proliferative lesion that was first de-scribed in 1983 by Stoler et al.8 BA was initiallyreferred to as epithelioid angioma based on its histo-logic features. It is associated with HIV/AIDS andcaused by gram-negative bacilli of the group Bartonella(Rochalimae). There have since been reported cases inother forms of immune compromise as well as in im-munocompetent individuals.9,10 BA can affect virtuallyany organ system but more commonly involves skinand subcutaneous tissues. There are reports of intraoralinvolvement.11,12 BA has a clinical resemblance to thepresent case. However, multiple cutaneous nodular le-sions together with fever, chills, malaise, anorexia,headaches, and vomiting are common clinical featuresof BA, none of which were present in this case.
Squamous cell carcinoma (SCC) of the gingiva pre-senting as localized periodontal disease was also con-sidered. Gingival SCC accounts for �10% of all in-traoral SCC.13 The majority (70%) of gingival SCCs
Fig. 2. Exophytic ulcerated mass (2 � 1.5 cm) arising fromthe dental extraction socket, 8 days after dental extraction.
occur in relation to the mandible and may be insidious

OOOOE332 Fasanmade et al. March 2010
in onset and progression, thereby mimicking periodon-tal disease.14 Although a diagnosis of a preexistingprimary gingival SCC was deemed to be possible, noulceration or gingival swelling was noted before thedental extraction. However, SCC may present as aninconspicuous lesion mimicking a localized endoperi-odontic lesion, exhibiting rapid growth following adental extraction.15
Our final working diagnosis was gingival SCC.
DIAGNOSIS AND MANAGEMENTUnder local anesthesia, an incisional biopsy of the
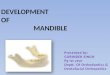
mass was carried out after preoperative platelet trans-fusion. Microscopic examination of the biopsy speci-men (Fig. 3) showed hyperplastic surface epitheliumoverlying edematous connective tissue containing clusters
Fig. 3. A, Photomicrograph demonstrating immature hema-topoietic cells within a background of capillary proliferation(hematoxylin and eosin stain, low magnification). B, Pho-tomicrograph demonstrating megakaryocyte (MGC) and im-mature myeloid precursor cells (MPC) (hematoxylin and eo-sin stain, high magnification).
of hematopoietic cells including atypical megakaryocytes,
erythroid colonies, and numerous myelocytes, predom-inantly of eosinophilic lineage. Erythroid colonies werealso present along with a small number of mononuclearmyeloid blasts. These erythroid colonies were immu-noreactive for glycophorin (Fig. 4a), which was used todefine normoblasts.16 Immunophenotyping demonstratedstrong diffuse immunoreactivity for the granulocytic pre-cursor marker CD68 (Fig. 4b), with blasts showing reac-tivity for CD34 and CD117 (c-kit). Megakaryocytes ex-pressed CD61 immunoreactivity (Fig. 4c).
The clinical, histologic, and immunohistochemicalfeatures were consistent with a diagnosis of extramed-ullary myeloid sarcoma (EMS).
EMS is typically a manifestation of systemic dis-ease.17 An urgent referral to the hematology departmentfor investigation of a possible blastic transformation ofpreviously diagnosed myelofibrosis was made. Subse-quent bone marrow biopsies did not show any evidenceof leukemic infiltrate. Further hematologic evaluationand bone marrow biopsies were consistent with theexisting diagnosis of myelofibrosis. After a multidisci-plinary team discussion, focal radiotherapy was se-lected as the treatment of choice.
DISCUSSIONExtramedullary myeloid sarcoma is a rare extramedul-
lary neoplasm of hematopoietic tissue incorporating myelo-blasts or immature granulocytic precursors, megakaryocytes,and erythroid precursors occurring outside of the bone mar-row. This entity, originally described by Burns18 in 1811,was referred to as “chloroma” by King17 in 1853 owingto the green color sometimes seen in the tissue. Thismacroscopic discoloration is due to the presence ofmyeloperoxidase. In 1967, Rappaport19 proposed thename granulocytic sarcoma, but more currently theWorld Health Organization refers to this entity as ex-tramedullary myeloid sarcoma.20
Presentation of extramedullary myeloid tumors out-side of the spleen and liver in myeloproliferative dis-orders is rare and signifies substantial bone marrowfibrosis as well as disease progression.21 It is oftenassociated with increasing blast counts, low plateletcount, and splenomegaly.
The most common area of involvement is the skin.Oral presentation is rare, with only 16% occurring inthe head and neck region. Lesions occurring in the jawsare uncommon,22,23 with only 33 previously reportedcases of oral myeloid sarcoma in the English-languageliterature between 1970 and July 2007.24
EMS classically precedes, coexists with, or follows apresentation of acute myeloid leukaemia.25 Develop-
ment of acute leukemia is nearly universal in the short
OOOOEVolume 109, Number 3 Fasanmade et al. 333
term, with mean survival times reported as rangingfrom 2.5 to 22 months. Less commonly, EMS can arise
Fig. 4. A, Glycophorin staining identifies the erythroid compo-nent. B, Photomicrograph demonstrating strong immunoreactivityto the granulocytic precursor marker CD68, which is highly ex-pressed on human monocytes and tissue macrophages. C, Photomi-crograph demonstrating numerous megakaryocytes (immunohisto-chemical staining with antimegakaryocytic marker CD61).
as a blastic transformation of an underlying chronic my-
eloproliferative disorder. EMS developing in a back-ground of myelodysplasia or myeloproliferative disease isgenerally considered to be equivalent to blast transforma-tion.26 This occurrence is typically an ominous sign withimminent deterioration in clinical course.
There are 3 major variants of EMS, depending on thepredominant cell type and the degree of maturation:blastic, immature, and mature variants. The blastic vari-ant has a predominance of myeloblasts, may be mis-taken for high-grade NHL, and is associated with apoorer prognosis.27 The immature variant displays amix of myeloblasts and promyelocytes, while the vari-ant presents with promyelocytes and more mature gran-ulocytes. Immunophenotyping is critical to confirm thepresence of abnormal megakaryocytes and erythroidand myeloid precursors. The most useful immunohis-tochemical markers include CD68, CD34, and CD61.Myeloperoxidase within immature myeloid cells is animportant marker of myeloid cell lines. The presence ofmyeloperoxidase can be confirmed by peroxidase, su-dan black, or diaminobenzidine reactions.
Treatment involves chemotherapy and, rarely, radio-therapy and local resection.28 Chemotherapy was deemedto be unsuitable in the present patient’s case because, inour opinion, further use of this modality in a backgroundof myelofibrosis was contraindicated.
There have been a number of differing reports con-cerning prognosis. In a study by Imrie et al.,21 themedian time to development of leukemia was 9 monthsafter a diagnosis of EMS, with a median survival of 22months. Fifty-four percent of patients in that studybegan chemotherapy upon the diagnosis of EMS. Ofthose, 41% went on to develop leukemia, comparedwith 71% in the nontreatment group.
At the time of writing, the present patient had re-mained free of systemic or local recurrence 9 monthsafter completion of treatment. She was continuing toattend regular follow-up.
REFERENCES1. Jafarzadeh H, Sanatkhani M, Mohtasham N. Oral pyogenic gran-
uloma: a review. J Oral Sci 2006;48:167-75.2. Leong R, Seng GF. Epulis granulomatosa: extraction sequelae.
Gen Dent 1998;46:252-5.3. Yagan R, Bellon EM, Radivoyevitch M. Breast carcinoma met-
astatic to mandible mimicking ameloblastoma. Oral Surg OralMed Oral Pathol Oral Radiol Endod 1984;57:189-94.
4. Bork K, Hoede N, Korting GW, Burgdorf WH, Young SK.Malignant tumours. In: Diseases of the oral mucosa and the lips.2nd ed. Philadelphia: Saunders; 1993; pp 324-42.
5. Delecluse HJ, Anagnostopoulos I, Dallenbach F, Hummel M,Marafioti T, Schneider U, et al. Plasmablastic lymphomas of theoral cavity: a new entity associated with the human immunode-ficiency virus infection. Blood 1997;89:1413-20.
6. Sapp PJ, Eversole LR, Wysocki GP. Diseases of blood. In: Con-temporary oral and maxillofacial pathology. 2nd ed. St. Louis: Mosby;
2004; pp 393-420.
OOOOE334 Fasanmade et al. March 2010
7. Lin F, Zhang K, Quiery AT, Prichard J, Schuerch C. Plasma-blastic lymphoma of the cervical lymph nodes in a humanimmunodeficiency virus-negative patient: a case report and re-view of the literature. Arch Pathol Lab Med 2004;128:581-4.
8. Stoler MH, Bonfiglio TA, Steigbigel RT, Pereira M. An atypicalsubcutaneous infection associated with acquired immune defi-ciency syndrome. Am J Clin Pathol 1983;80:714-8.
9. Schwartz RA, Gallardo MA, Kapila R, Gascón P, Herscu J,Siegel I, et al. Bacillary angiomatosis in an HIV seronegativepatient on systemic steroid therapy. Br J Dermatol 1996;135:982-7.
10. Gangopadhyay AK, Sharma PK. Bacillary angiomatosis in animmune competent patient. Indian J Dermatol Venereol Leprol2001;67:37-8.
11. Tucci E, Della Rocca C, Santilli F. Localised bacillary angioma-tosis in the oral cavity: observation about a neoplasm withatypical behaviour. Description of a case and review of literature.Minerva Stomatol 2006;55:67-75.
12. Lopez de Blanc S, Sambuelli R, Femopase F, Luna N, GravottaM, David D, et al. Bacillary angiomatosis affecting the oralcavity. Report of two cases and review. J Oral Pathol Med2000;29:91-6.
13. Yoon TY, Bhattacharyya I, Katz J, Towle HJ, Islam MN. Squa-mous cell carcinoma of the gingiva presenting as localized peri-odontal disease. Quintessence Int 2007;38:97-102.
14. Shah JP, Johnson NW, Batsakis JG. Oral cancer. London: MartinDunitz; 2003.
15. Levi PA Jr, Kim DM, Harsfield SL, Jacobson ER. Squamous cellcarcinoma presenting as an endodontic-periodontic lesion. J Peri-odontol 2005;76:1798-804.
16. Pileri SA, Ascani S, Cox MC, Campidelli C, Bacci F, Piccioli M,et al. Myeloid sarcoma: clinicopathologic, phenotypic and cyto-genetic analysis of 92 adult patients. Leukemia 2007;21:340-50.
17. King A. A case of chloroma. Monthly J Med 1853;17:97.18. Burns A. Observations of surgical anatomy. In: Head and Neck.
London: Thomas Royce and Co.; 1811. p. 364-6.19. Rappaport H. Tumors of the hematopoietic system. In: Atlas of
tumor pathology, section III, fascicle 8. Washington (DC):
Armed Forces Institute of Pathology, 1967:241-7.20. World Health Organization. Morphology code of the Interna-tional Classification of Diseases (ICD-O). 3rd ed. Geneva: WorldHealth Organization; 2000.
21. Imrie KR, Kovacs MJ, Selby D, Lipton J, Patterson BJ, Panta-lony D, et al. Isolated chloroma: the effect of early antileukemictherapy. Ann Intern Med 1995;123:351-3.
22. Ferri E, Minotto C, Ianniello F, Cavaleri S, Armato E, CapuzzoP. Maxillo-ethmoidal chloroma in acute myeloid leukaemia: casereport. Acta Otorhinolaryngol Ital 2005;25:195-9.
23. Adler CP, Schaefer HE. Eosinophilic chloroma (eosinophilicgranulocytic sarcoma). Histopathogy 2001;39:544-6.
24. Xie Z, Zhang F, Song E, Ge W, Zhu F, Hu J. Intraoral granu-locytic sarcoma presenting as multiple maxillary and mandibularmasses: a case report and literature review. Oral Surg Oral MedOral Pathol Oral Radiol Endod 2007;103:e44-8.
25. Dock G. Chloroma and its relation to leukemia. Am J Med Sci1893;106:152-7.
26. Brunning RD, Bennett J, Matutes E, et al. Acute myeloid leuke-mia not otherwise categorized. In: Jaffe ES, Harris NL, Stein H,Vardiman JW, editors. Pathology and genetics of tumours ofhaematopoietic and lymphoid tissues. World Health Organiza-tion classification of tumors, vol. 3. Lyon, France: IARC Press;2001. p. 104-5.
27. Paydas S, Zorludemir S, Ergin M. Granulocytic sarcoma: 32cases and review of the literature. Leuk Lymphoma 2006;47:2527-41.
28. Levine RL, Pardanani A, Tefferi A, Gilliland DG. Role of JAK2 in the pathogenesis and therapy of myeloproliferative disor-ders. Nat Rev Cancer 2007;7:673-83.
Reprint requests:
Adekunmi FasanmadeDepartment of Oral and Maxillofacial SurgeryBristol Dental HospitalLower Maudlin StreetBristol, BS1 2LYUnited Kingdom
[email protected]