Embed Size (px)
Citation preview

Vol. 107 No. 5 May 2009
CLINICOPATHOLOGIC CONFERENCE Editor: Paul C. Edwards
Rapidly progressing soft tissue mass of the anterior mandibularregionVenkatesh G. Naikmasur, MDS,a Kruthika S. Guttal, MDS,b Sushma Kaveriappa,c andK. S. Datta, MD, DPB, FICPath, FIAMS,d Dharwad and Navanagar, IndiaSHRI DHARMASTHALA MANJUNATHESHWARA COLLEGE OF DENTAL SCIENCES AND HOSPITAL ANDKARNATAK CANCER HOSPITAL AND RESEARCH INSTITUTE (Oral Surg Oral Med Oral Pathol Oral
Radiol Endod 2009;107:607-611)CLINICAL PRESENTATIONA 28-year-old woman reported to the Department of
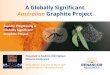
Oral Medicine with a swelling in the anterior mandib-ular region of one month duration. The swelling hadrapidly increased in size, causing severe pain and ele-vation of the tongue, forcing the patient to maintain afluid diet. Physical examination revealed a 10 � 8 cmsolitary growth involving the anterior mandible, ex-tending from the region of the left mandibular canine tothe right mandibular first molar and obscuring the man-dibular anterior teeth. The lobulated mass involved thelabial and lingual gingiva and floor of the mouth. Areasof ulceration were observed on the surface of the lesion(Figs. 1 and 2). On palpation, the lesion was tender, softto firm in consistency and nonfluctuant. There was noparesthesia associated with the swelling.
aProfessor and Head, Department of Oral Medicine and Radiology,Shri Dharmasthala Manjunatheshwara College of Dental Sciencesand Hospital.bAssistant Professor, Department of Oral Medicine and Radiology,Shri Dharmasthala Manjunatheshwara College of Dental Sciencesand Hospital.cPostgraduate Student, Department of Oral Medicine and Radiology,Shri Dharmasthala Manjunatheshwara College of Dental Sciencesand Hospital.dChief Pathologist, Department of Pathology, Karnatak Cancer Hos-pital and Research Institute.Received for publication Aug 30, 2007; returned for revision Nov 3,2008; accepted for publication Nov 19, 2008.1079-2104/$ - see front matter© 2009 Published by Mosby, Inc.
doi:10.1016/j.tripleo.2008.11.025Occlusal (Fig. 3) and panoramic (Fig. 4) radiographsdemonstrated an ill-defined osteolytic zone extendingfrom the region of the left mandibular canine to theright mandibular first molar, accompanied by alveolarbone destruction and displacement of teeth.
Computerized tomographic imaging (Fig. 5) re-vealed destruction of the buccal and lingual corticalplates. Post-contrast imaging showed a large soft tissuecomponent of the tumor involving the buccal and lin-gual aspects with irregular enhancement. Laboratory
Fig. 1. Swelling involving the mandibular symphysis.
investigations ruled out immunodeficiency (HIV).
607

OOOOE608 Naikmasur et al. May 2009
Differential diagnosisIt was not evident from the clinical appearance
whether the tumor was of peripheral or central origin. Apathologic process beginning within bone and second-arily extending into soft tissues typically follows theinside–out principle, where the soft tissue mass issmaller than the degree of bone destruction.1 In thepresent case, the degree of bone destruction was sig-
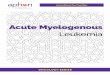
Fig. 2. Extensive tumor mass involving the labial and lingualvestibule, obscuring the teeth in the anterior mandibular re-gion with surface ulcerations.
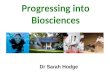
Fig. 3. Mandibular occlusal radiograph showing permeativepattern of destruction of the medullary as well as corticalbone.
nificantly smaller compared with the soft tissue mass,
suggesting an origin from the peripheral tissue. There-fore, our differential diagnosis focused on malignantprocesses of peripheral origin, including squamous cellcarcinoma, carcinoma of the minor salivary glands,sarcomas of nonodontogenic origin, and non-Hodgkinlymphoma.
The probability that this lesion represented a squa-mous cell carcinoma was considered unlikely, owing tothe clinical and radiographic presentation. Furthermore,the patient denied any history of tobacco use, which is
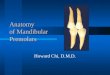
Fig. 4. Panoramic radiograph showing the extension of thebone destruction from the region of left mandibular canine tothe right mandibular first molar.
Fig. 5. Axial computerized tomography sections (bone win-dow) showing destruction of the medullary bone, buccal, andlingual cortices.
a strong predilection factor in Indian subpopulations.

OOOOEVolume 107, Number 5 Naikmasur et al. 609
Malignant tumors of minor salivary gland origincomprise the second most common type of primaryintraoral cancer,2 with mucoepidermoid carcinomabeing the most common.2 It is more common infemales and occurs in the third to fifth decades oflife.3 Frequent sites of occurrence include the palate,buccal mucosa, lips, floor of the mouth, and retro-molar pad.3 High-grade mucoepidermoid carcinomasare most common among children and adolescents,3
typically manifesting as a rapidly growing mass withulceration of the overlying mucosa. These lesions arenot encapsulated and tend to infiltrate into deeperstructures.3 The present case had similar clinicalmanifestations, demonstrating infiltration into the an-terior mandibular region.
Other salivary gland carcinomas that commonlyinvolve the minor salivary glands include adenoidcystic carcinoma and polymorphous low-grade ade-nocarcinoma.2 These lesions were considered lesslikely, because they are very slow growing and theduration of symptoms is quite long, in contrast to therapid growth rate reported in the present case.
Among sarcomas of the oral cavity, fibrosarcomawas considered to be high on our differential diagnosis,because 2%-20% of cases are known to involve thehead and neck region.4
Fibrosarcoma can occur de novo or subsequent toprevious radiation therapy. It commonly presents as apainful swelling with ulceration of the overlying mu-cosa. Its origin can be in soft tissues or bone. Paresthe-sia and tooth mobility are commonly observed. Radio-graphically, fibrosarcoma involving bone presents as anosteolytic lesion with ill-defined borders.5
Malignant fibrous histiocytoma (MFH) is frequentlyassociated with pain and swelling. MFH arises predom-inantly from the soft tissues, and can occur at any agedespite its peak incidence of occurrence between thefifth and seventh decades of life.6 The nasal cavity andthe paranasal sinuses are the most commonly affectedsites in the head and neck region.6 In the jaws, MFHtends to be very aggressive with a high rate of localrecurrence. Radiographic findings include a moth-eatenappearance, cortical erosion, irregular bone destruction,pathologic fracture, and root resorption. However,these radiographic findings are not specific to MFH.6
Leiomyosarcoma (LMS), a malignant tumor ofsmooth muscle origin, was also considered in the dif-ferential diagnosis. Typically, LMS manifests as a pain-ful, lobulated, and fixed mass involving the submucosaltissues. It typically occurs in middle-aged and olderindividuals. Favored sites in the head and neck regioninclude the floor of the mouth and cheek.7 LMS is aslow growing tumor, with secondary ulceration of the
mucosal surface noted in many cases. LMS has beenpostulated to arise from smooth muscle cells of theblood vessel wall and from undifferentiated mesenchy-mal cells.7 The clinical appearance in our case and theage range were compatible with LMS.
Non-Hodgkin lymphoma (NHL) was also consideredin the differential diagnosis. Commonly involved ex-tranodal sites in the oral cavity include the palate, floorof the mouth, gingiva, buccal mucosa, and tongue.8
One of the more common presentations of NHL in thejaws is a mass or a swelling with or without toothmobility. Other common presentations include ulcer-ation, discoloration, pain, paresthesia, or anesthesia.Some cases of NHL may even mimic inflammatoryconditions such as periodontitis.8 Patients in the sixthand seventh decades of life are at highest risk, NHL canaffect individuals of any age. The high-grade lympho-blastic and small noncleaved cell types are more com-mon in children and young adults.8
Synovial sarcoma (SS) was also considered in thedifferential diagnosis. Contrary to its name, SS rarelyarises from the synovial membranes (only 10% involvethe joints).4 The mean age for patients with SS of thehead and neck region varies from 25 to 30 years. Sitesof predilection vary and include the superior aspect ofthe neck (beneath the mandible), the anterior region ofthe neck, and orofacial and laryngeal sites. Synovialsarcoma usually presents as a painless mass, thoughpain may be observed in 20% of the cases.4
The Ewing sarcoma family of tumors that can occurin the head and neck region comprise osseous andextraosseus Ewing sarcoma (EES) and peripheral prim-itive neuroectodermal tumor (pPNET).9 Several casesof pPNET have been reported in the head and neckregion involving the mandible, cerebellopontine angle,and the skull base.9 Presently, pPNET is considered tobe a neoplasm of nonneural soft tissues that primarilyaffects children and adolescents; with 90% of patients�30 years of age.4 It commonly presents as a largepainful mass of recent onset. EES, a rare subset ofEwing sarcoma arising in the soft tissues, commonlyaffects individuals in the 19–26-year-old age group.4 Inthe head and neck region, the soft tissues of the neckare most commonly affected. EES is usually observedin the deeper tissues, but may also arise from superficialcutaneous or subcutaneous tissues.4 A common mani-festation of EES is an extensive tumor mass that growsrapidly with or without pain, as in the present case.
Diagnosis and managementHistologic evaluation of the biopsy specimen under
light microscopy showed a highly cellular neoplastictissue composed of large compactly arranged spindle-and fusiform-shaped cells (Fig. 6). The presence of
interlacing bundles of cells was a prominent feature.
OOOOE610 Naikmasur et al. May 2009
The nuclei of the spindle-shaped cells were elongatedand wavy, whereas fusiform cells contained round tocomma-shaped distinct nuclei with eosinophilic andscanty cytoplasm. Foci of pleomorphism were notedwith the spindle cells as well as in mononucleated andmultinucleated tumor giant cells. Occasional fieldsshowed nuclear palisading and a fibrillar arrangementof cells resembling Schwann cells. A few areas re-vealed typical fascicle formation resulting from themerger of pleomorphic cells with adjacent less cellular,myxomatous areas. Scattered pleomorphic cells withmitotic figures and nuclear anaplasia were frequentlynoted in the hypercellular areas. Occasional areasshowed tumor cells arranged in a whorled pattern (Fig.7). Areas of necrosis and hemorrhage were rarely seen,and vascular channels appeared normal. Occasionalfields showed cells resembling Schwann cells. The tu-mor was focally reactive to S-100 (Fig. 8).
The final diagnosis was malignant peripheral nervesheath tumor (MPNST).
The severity as well as the overall prognosis wasexplained to the patient. Radical surgery was planned.However, the patient failed to report back for furthertreatment and succumbed to death within 1 month ofher initial assessment.
DISCUSSIONMalignant peripheral nerve sheath tumor is the pre-
ferred terminology for most spindle cell sarcomas arisingfrom the nerve or showing nerve sheath differentiation, asadopted by the World Health Organization committee forclassification of soft tissue tumors. MPNST replaces theearlier terms malignant schwannoma, neurofibrosarcoma,neurogenic sarcoma, neurilemmosarcoma, and malignant
Fig. 6. Streaming spindle cells arranged in fascicles, withmarked pleomorphism and hyperchromatism (hematoxylinand eosin, �100).
neurofibroma.10
MPNST is a highly aggressive tumor that may arisede novo or from a preexisting schwannoma or neuro-fibroma and represents about 5%-10% of soft tissuesarcomas.11 MPNST is uncommon in the head and neckregion, those regions representing 8%-16% of cases.11
The mandible and the labial and buccal mucosa are themost favored sites within the oral cavity.12 When thelesion arises from the soft tissues, it usually has indis-tinct margins with an ulcerated surface and symptomsranging from pain to paresthesia.11
Malignant peripheral nerve sheath tumor in head andneck region typically involves the third, fourth, fifth,seventh, and eighth cranial nerves,13 with the trigemi-nal nerve being most commonly involved. The size ofthe tumor mass in the present case was quite extensive,making it impossible to identify a nerve or nerve branchfrom which the lesion arose. We hypothesize that thelesion may have originated from the terminal nervebranches in the soft tissues of the labial vestibule or the
Fig. 7. Tumor cells arranged in whorled pattern (hematoxylinand eosin, �100).
Fig. 8. Neoplastic cells focally positive for S-100 (Envisiontechnique, �100).
floor of the mouth.

OOOOEVolume 107, Number 5 Naikmasur et al. 611
Approximately 40%-50% of MPNSTs are associatedwith a family history of neurofibromatosis type 1 (NF-1), although most of these cases are extragnathic.14 Ourpatient had no family history of NF-1
Histologically, 95% of MPNSTs are of the spindlecell type, with the remaining 5% being of the epithe-lioid variant.15 MPNSTs are composed of irregularlyshaped cells exhibiting significant variability in thedegree of cellularity, ranging from hypocellular myxoidareas to areas with prominent cellularity. Other helpfulhistologic features include the presence of spindle cellswith comma-shaped nuclei with lightly staining indis-tinct cytoplasm, nuclear palisading, hyaline bands, andcurlicue or whorled arrangement of spindle cells.10,16
The last feature suggests rudimentary tactoid differen-tiation but is not as well developed as the pacinianbodies of benign neurofibroma.10 The presence of tu-mor cells in a whorled pattern is a characteristic featureof MPNST,4 although characteristic schwannoma-likedifferentiation is noted only in 10% of cases.10 Immu-nohistochemistry is useful in confirming neural differ-entiation.10 S-100 immunoreactivity is seen in 50%-90% of MPNSTs.10 Leu-7 and myelin basic proteinpositivity are noted in 50% and 40% of cases, respec-tively.10
The prognosis for patients with MPNST, whetherassociated with NF-1 or not, depends mainly on tumorpresentation, whether the lesion represents a primarytumor or recurrent disease, the size of the tumor, andthe site of origin. Patients with tumors of the extremi-ties typically have a more favorable outcome comparedwith those with tumors occurring in the trunk or headand neck region. Surgical removal remains the main-stay of treatment. Adjuvant radiation therapy may im-prove local control.17
The authors acknowledge Dr. C. Bhasker Rao, Principal,SDM College of Dental Sciences, Dharwad, for hissupport and encouragement, Dr. A. C. Deka, MedicalSuperintendent, Karnatak Cancer Hospital, Navnagar, andDr. Lakshmi Rao, Consultant Pathologist, KMC Hospital,Manipal, for their assistance in the immunohistochemicalstudy, and Dr. Sudhindra Prabhu, Assistant Professor,Department of Oral and Maxillofacial Pathology, andMr. Madhu Kadam, Department of Photography, SDMCollege of Dental Sciences, Dharwad, for their assistancein procuring photomicrographs.
REFERENCES1. Rowe LJ, Yochum TR, editors. Principles of radiologic interpre-
tation. In: Essentials of skeletal radiology. 3rd ed. Philadelphia:Lippincott Williams and Wilkins; 2005. p. 710.
2. Torske KR. Malignant lesions of the oral cavity. In: Werning JW,
editor. Oral cancer diagnosis, management and rehabilitation.New York: Thieme; 2007. p. 23.
3. Eveson JW. Salivary gland tumors. In: Barnes L, Eveson JW,Reichart P, Sidransky D, editors. Pathology and genetics of headand neck tumors. Lyon: IARC Press; 2005. p. 190.
4. El-Mofty SK, Kyriakos M. Soft tissue and bone lesions. In:Gnepp DR, editor. Diagnostic surgical pathology of the head andneck. Philadelphia: Saunders; 2001. p. 505-39.
5. Soares AB, Lins LH, Mazedo AP, Pereira-Neto JS, Vargas PA.Fibrosarcoma originating in the mandible. Med Oral Patol OralCir Bucal 2006;11:E243-6.
6. Senel FC, Bektas D, Caylan R, Onder E, Gunhan O. Malignantfibrous histiocytoma of the mandible. Dentomaxillofac Radiol2006;35:125-8.
7. Rajendran R. Benign and malignant tumors of the oral cavity. In:Rajendran R, Sivapathasundharam B, editors. Shafer’s text bookof oral pathology. New Delhi: Elsevier; 2007. p. 271.
8. Chan ACL, Chan JKC. Haematolymphoid tumors. In: Barnes L,Eveson JW, Reichart P, Sidransky D, editors. Pathology andgenetics of head and neck Tumors. Lyon: IARC Press; 2005. p.199.
9. Alrawi SJ, Tan D, Sullivan M, Winston J, Loree T, Hicks W, etal. Peripheral primitive neuroectodermal tumor of the mandiblewith cytogenetic and molecular biology aberrations. J Oral Max-illofac Surg 2005;63:1216-21.
10. Enzinger FM, Weiss SW, editors. Malignant tumors of the pe-ripheral nerves. In: Soft tissue tumors. 3rd ed. St. Louis: Mosby;1995. p. 889-928.
11. Fernandes AM, Johann AC, da Silveira-Junior JB, Aguiar MC,do Carmo MA, Mesquita RA. Malignant peripheral nerve sheathtumor of the tongue. Oral Oncol Extra 2006;42:210-2.
12. DiCerbo M, Sciubba JJ, Sordill WC, DeLuke DM. Malignantschwannoma of the palate: a case report and review of theliterature. J Oral Maxillofac Surg 1992:50:1217-21.
13. Hemalatha AL, Karthikeyan TM, Bharatnur SS, Anil Kumar S.Malignant peripheral nerve sheath tumor in oral cavity—a raresite. Indian J Pathol Microbiol 2006;49:397-9.
14. Kenali MS, Bridger PG, Baldwin M, Smee R. Malignant periph-eral nerve sheath tumor of the tongue. Aust N Z J Surg1999;69:243-6.
15. Thompson LDR, Fanburg-Smith JC. Malignant soft tissue tu-mors. In: Barnes L, Eveson JW, Reichart P, Sidransky D, editors.Pathology and genetics of head and neck tumors. Lyon: IARCPress; 2005. p. 41-2.
16. Bagan JV, Sanchis JM, Jiménez Y, Murillo J, Poveda R, DiazJM. Malignant peripheral nerve sheath tumor of the maxilla. OralOncology Extra 2005;41:70-3.
17. Anghileri M, Miceli R, Fiore M, Mariani L, Ferrari A, Mussi C,et al. Malignant peripheral nerve sheath tumors prognostic fac-tors and survival in a series of patients treated at a singleinstitution. Cancer 2006;107:1065-74.
Reprint requests:
Dr. Venkatesh G. NaikmasurProfessor and HeadDepartment of Oral Medicine and RadiologySDM College of Dental Sciences and HospitalDharwad 580 009KarnatakaIndia
[email protected]