Embed Size (px)
Citation preview

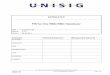
RBC ENZYMOPATHIES(Congenital Haemolytic Anaemia)

Glucose Glucose 6-
phosphate
2 ATP
GLYCOLYSIS PATHWAY
HEXOSE MONOPHOSP
HATE PATHWAY
G6PD
6-phosphogluconate
Phosphoenolpyruvate
Pyruvate
Pyruvate Kinase
(Embden Meyerhof Pathway)
NADP+
NADPH
GSSG(Oxidised Glutathione)
GSH(Reduced Glutathione)Oxidati
ve Stress

RBC ENZYMOPATHIES
Defects in the hexose monophosphate shunt pathway result in periodic haemolysis induced by oxidative stress.
Defects in the Embden-Meyerhof pathway result in shortened RBC survival and chronic haemolysis.

G6PD DEFICIENCY
Glucose 6-phosphate dehydrogenase is pivotal in the HMS pathway.
G6PD deficiencies result in the most common human enzymopathy.
Affects 10% of the population.
Geographical distribution parallels the malaria belt.

Prevalence of G6PD Deficeciency

Prevalence of Malaria

G6PD DEFICIENCY
Genetics: The enzyme is made of subunits that are encoded by
a gene on the X-chromosome.
The deficiency affects males and homozygote females.
Carrier females are affected in: The neonatal period. The presence of extreme lyonisation.

G6PD DEFICIENCY
Genetics: There are over 400 variants described, classified into 5
classes
Different biochemical forms of the enzyme are exhibited; distinguished by different electrophoretic mobility and kinetic properties.
Majority of the variants result from a single point-mutation, resulting in amino acid substitution in gene encoding for G6PD located at the Xq28 region on the tip of the long arm of the X- chromosome.

G6PD DEFICIENCY
Genetics:
Variants with normally active but unstable G6PD:
B+ enzyme, present in Caucasians and 70% of Afro-Caribbeans.
A+ enzyme, present in 20% of Afro-Caribbeans.
Variants with less active, stable G6PD: A- enzyme, present in 10% of Afro-Caribbeans. B- (Mediterranean) enzyme, present in Caucasians.

G6PD DEFICIENCY
Clinical Features:
Acute haemolysis in response to precipitating factors
Chronic compensated haemolysis (in severe disease, class I)
Infection or acute illness (absent leucocyte G6PD levels)
Neonatal jaundice; may be a feature of B- enzyme
Favism, i.e. acute haemolysis after ingestion of broad beans, usually seen in B- variant. The offending agent is divicine.

G6PD DEFICIENCY
Factors precipitating acute haemolysis: Drugs: Analgesics: Aspirin, Phenacetin Antimalarials: Primaquine, Quinine, Chloroquine,
Pyrimethamine Antibiotics: Sulphonamides, Nitrofurantoins, Ciprofloxacin Miscellaneous: Quinidine, Probenecid, Vitamin K, Dapsone
Infections
Diabetic Ketoacidosis
Henna; causes haemolytic crisis in G6PD deficient infants

G6PD DEFICIENCY
Laboratory Findings: During a haemolytic episode: Bite cells Blister cells Irregularly shaped small cells Polychromasia, reflecting the reticulocytosis Denatured haemoglobin visible as Heinz bodies
within the RBC cytoplasm



G6PD DEFICIENCY
Laboratory Findings: G6PD level (Screening tests): Screening test for G-6-PD enzyme depends on the
presence of NADPH. Quantitative G-6-PD assay by spectrophotometer. Cyanide-Ascorbate test. Genetic studies: PCR, especially for heterozygotes.

G6PD DEFICIENCY
Management: Stop any precipitant drugs and treat
underlying infections Maintenance of good urine output during the
haemolytic episode. Folic acid Exchange transfusion in the newborn Acute transfusion support may be life-saving

PYRUVATE KINASE DEFICIENCY
The second most common RBC enzyme defect.
Inherited as an autosomal recessive trait.

PYRUVATE KINASE DEFICIENCY
Results in ATP deficiency and chronic haemolytic anaemia.
Enzyme activity is only 5-20% of normal.
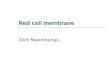
Causes non-spherocytic haemolytic anaemia
Blood film shows characteristic ‘prickle cells’.

PRICKLE
CELLS

PYRUVATE KINASE DEFICIENCY
Management:
Folic acid supplements.
Splenectomy.

PYRIMIDINE 5’ NUCLEOTIDASE DEFICIENCY
Pyrimidine 5’ nucleotidase catalyses dephosphorylation of nucleoside monophosphate.
Important during the degradation of RNA in reticulocytes.
The deficiency is inherited as autosomal recessive trait.
Coarse basophilic stippling. Feature of lead poisoning.