Embed Size (px)
Citation preview
2013/05/02
1
Reading Chest X-rays
HS Schaaf
Desmond Tutu TB Centre, Department of Paediatrics and Child
Health, Stellenbosch University
Chest X-ray
• Most frequently performed radiographic investigation in children
• Important to read correctly as diagnosis and treatment is often based on this
• Technical errors may influence interpretation
• Normal variations do occur
• Supine antero-posterior (AP) projection used in infants
• Erect AP projection in toddler
2013/05/02
2
Basic Conditions • A good viewing box makes it easier (or
digital system)
• AP and lateral radiographs must be done
• All previous chest radiographs must be
looked at and compared to current one
• Use a systematic approach every time
you evaluate a chest radiograph (e.g. rule
of 3’s)
Artifacts
• Skin folds
• Incubators
• Hair plaited or dressed with ornaments
• Clothes with metal objects
2013/05/02
3
Systematic approach
• Identity (3)– Name
– Date
– Type of CXR (projection AP, PA, lateral; erect or supine)
• Quality (3)– Rotation
– Penetration
– Inspiration
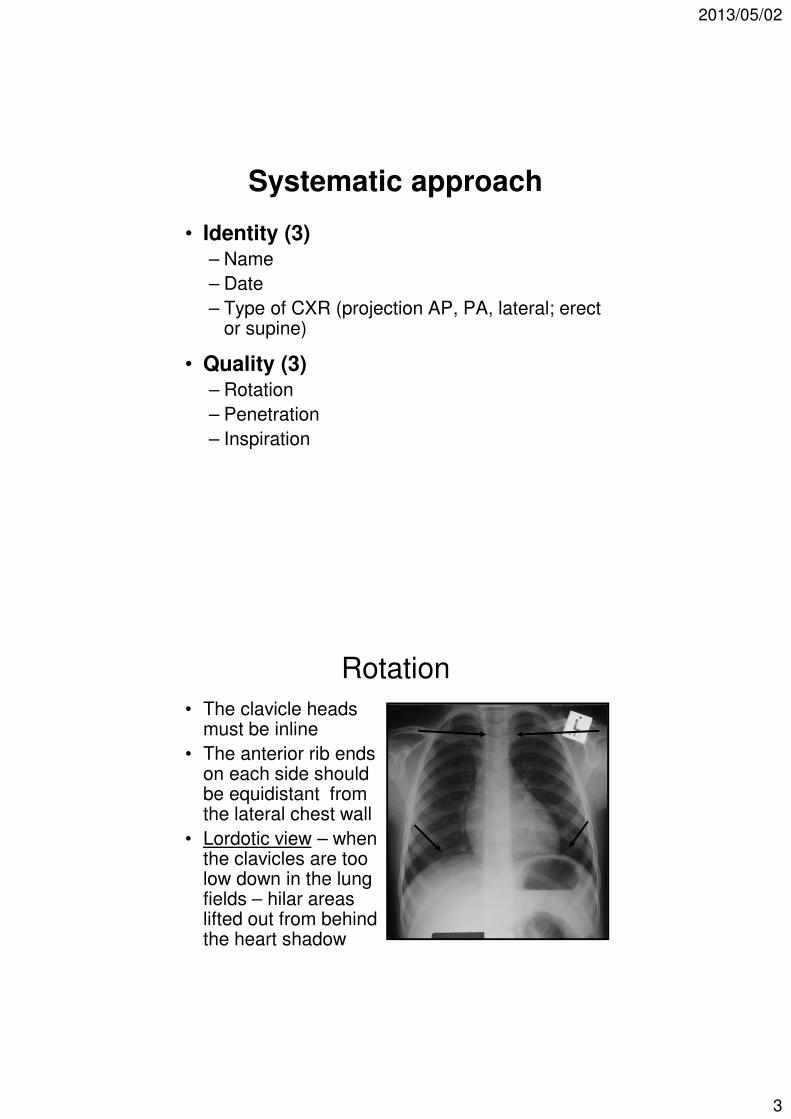
Rotation
• The clavicle heads must be inline
• The anterior rib ends on each side should be equidistant from the lateral chest wall
• Lordotic view – when the clavicles are too low down in the lung fields – hilar areas lifted out from behind the heart shadow
2013/05/02
4
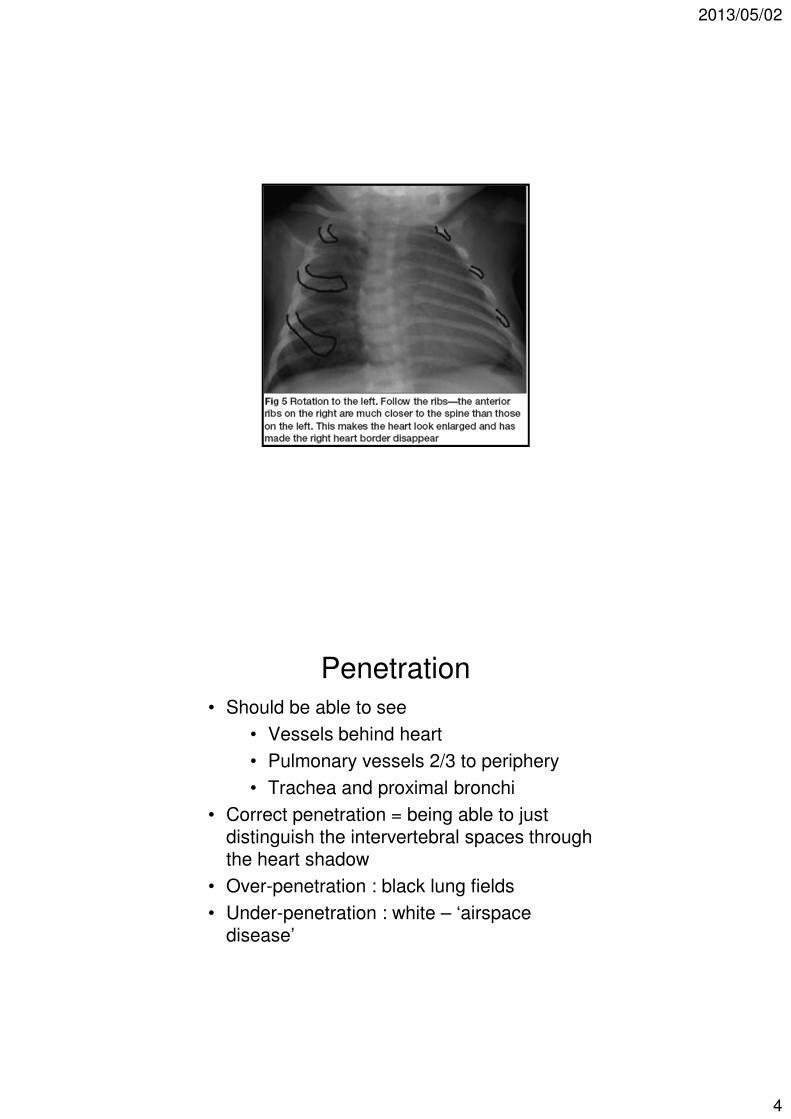
Penetration
• Should be able to see
• Vessels behind heart
• Pulmonary vessels 2/3 to periphery
• Trachea and proximal bronchi
• Correct penetration = being able to just distinguish the intervertebral spaces through the heart shadow
• Over-penetration : black lung fields
• Under-penetration : white – ‘airspace disease’
2013/05/02
5
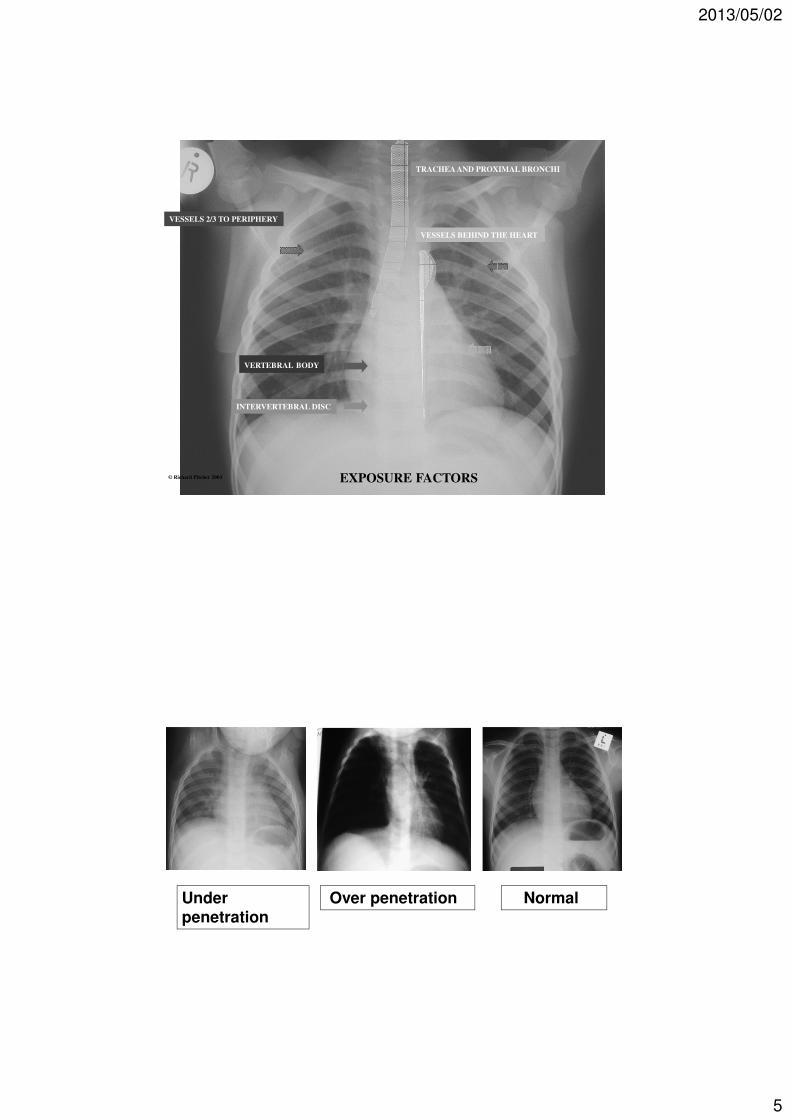
VERTEBRAL BODY
INTERVERTEBRAL DISC
VESSELS BEHIND THE HEART
VESSELS 2/3 TO PERIPHERY
TRACHEA AND PROXIMAL BRONCHI
EXPOSURE FACTORS © Richard Pitcher 2003
Under penetration
Over penetration Normal
2013/05/02
6
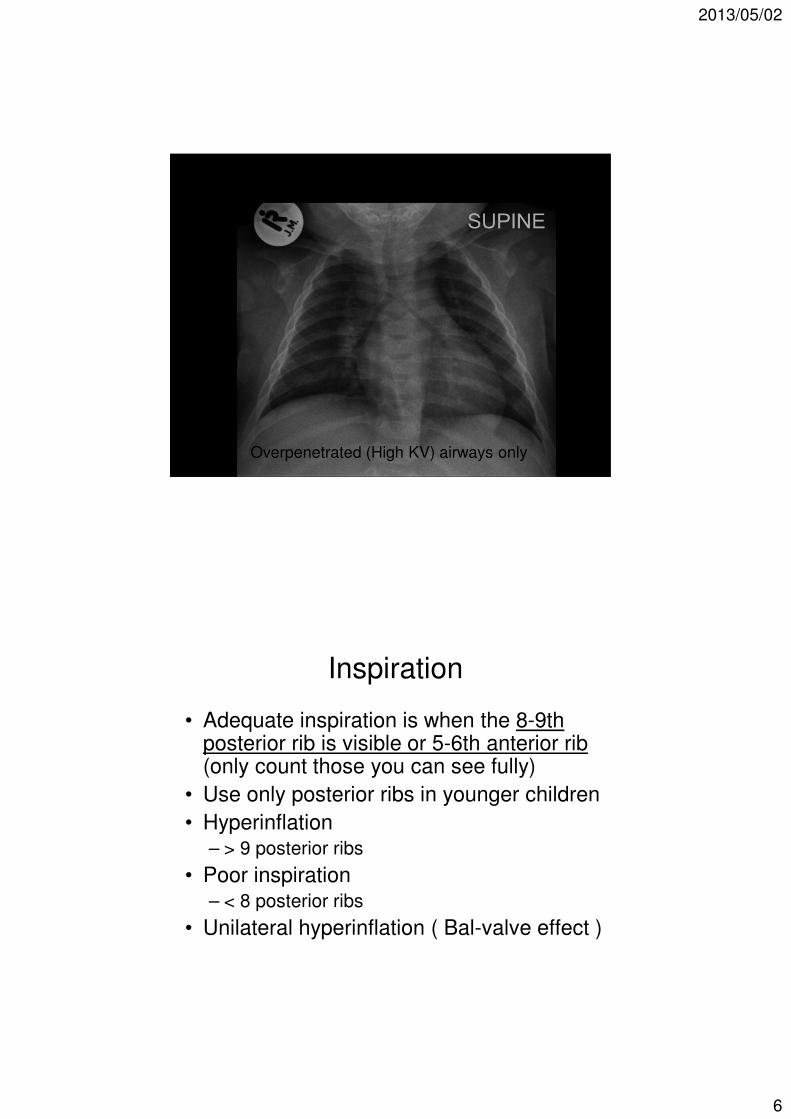
Overpenetrated (High KV) airways only
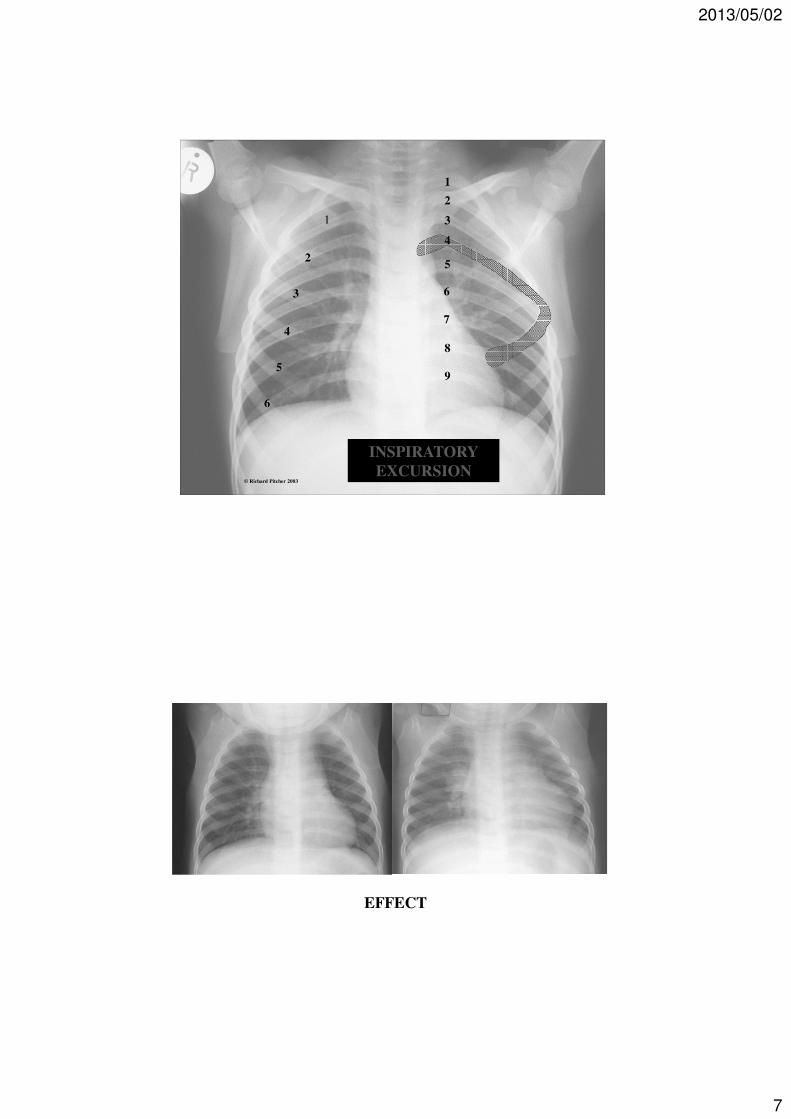
Inspiration
• Adequate inspiration is when the 8-9th posterior rib is visible or 5-6th anterior rib (only count those you can see fully)
• Use only posterior ribs in younger children
• Hyperinflation– > 9 posterior ribs
• Poor inspiration– < 8 posterior ribs
• Unilateral hyperinflation ( Bal-valve effect )
2013/05/02
7
INSPIRATORY
EXCURSION
1
2
3
4
5
6
7
8
9
1
2
3
4
5
6
© Richard Pitcher 2003
EFFECT
2013/05/02
8
1
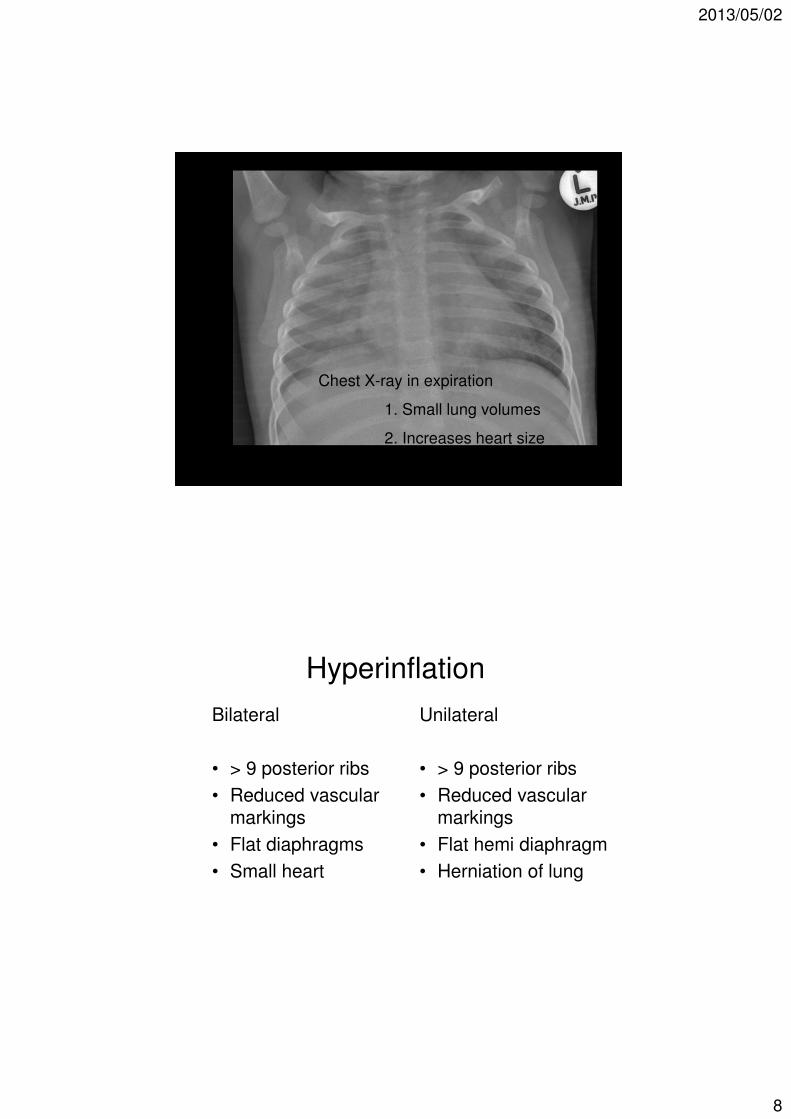
Chest X-ray in expiration
1. Small lung volumes
2. Increases heart size
3. Airways difficult to see
Hyperinflation
Bilateral
• > 9 posterior ribs
• Reduced vascular markings
• Flat diaphragms
• Small heart
Unilateral
• > 9 posterior ribs
• Reduced vascular markings
• Flat hemi diaphragm
• Herniation of lung
2013/05/02
9
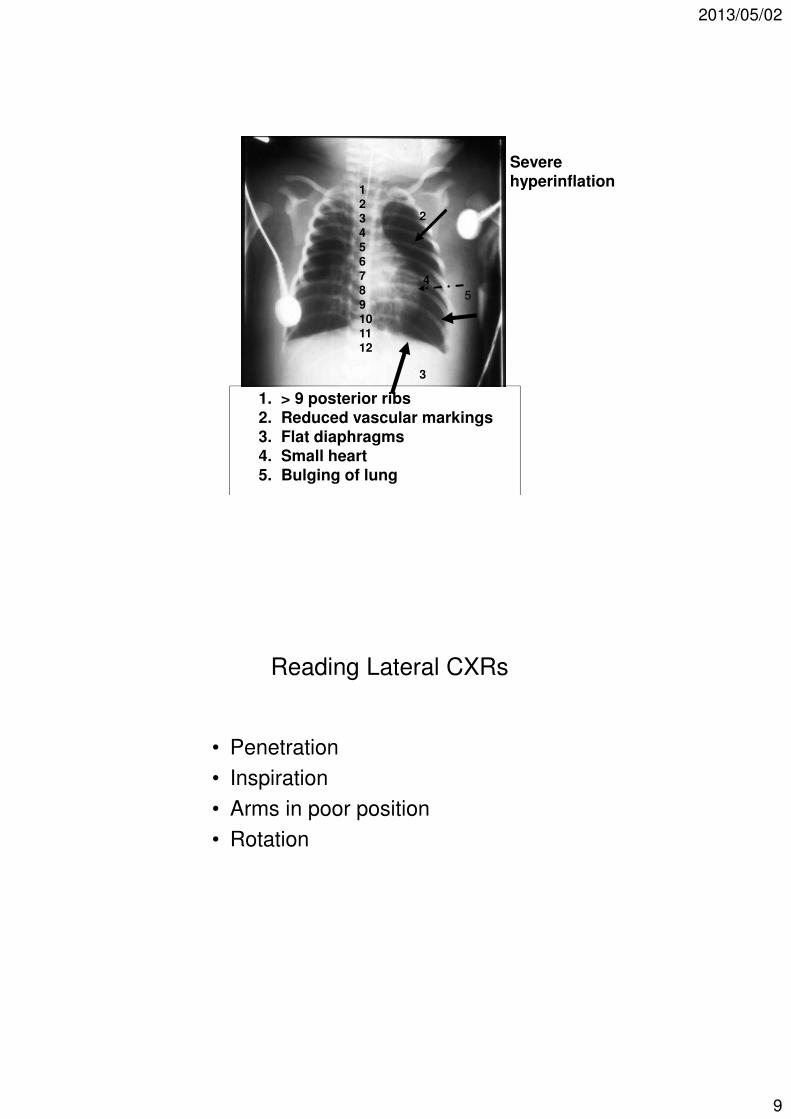
123456789101112
1. > 9 posterior ribs
2. Reduced vascular markings3. Flat diaphragms4. Small heart5. Bulging of lung
2
3
4
5
Severe
hyperinflation
Reading Lateral CXRs
• Penetration
• Inspiration
• Arms in poor position
• Rotation
2013/05/02
10
1
2
4
6
5 7
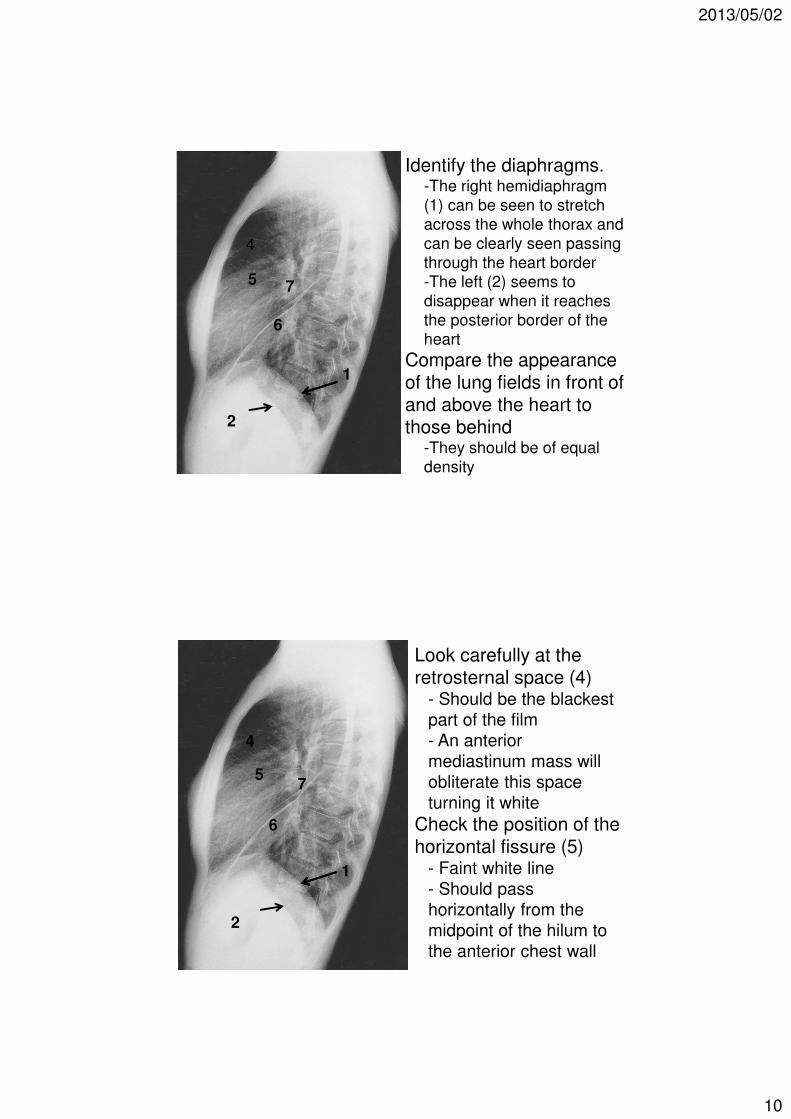
Identify the diaphragms.-The right hemidiaphragm
(1) can be seen to stretch
across the whole thorax and
can be clearly seen passing
through the heart border
-The left (2) seems to
disappear when it reaches
the posterior border of the
heart
Compare the appearanceof the lung fields in front ofand above the heart tothose behind
-They should be of equal
density
1
2
4
6
57
Look carefully at the retrosternal space (4)
- Should be the blackest
part of the film
- An anterior
mediastinum mass will
obliterate this space
turning it white
Check the position of thehorizontal fissure (5)
- Faint white line
- Should pass
horizontally from the
midpoint of the hilum to
the anterior chest wall
2013/05/02
11
1
2
4
6
5 7
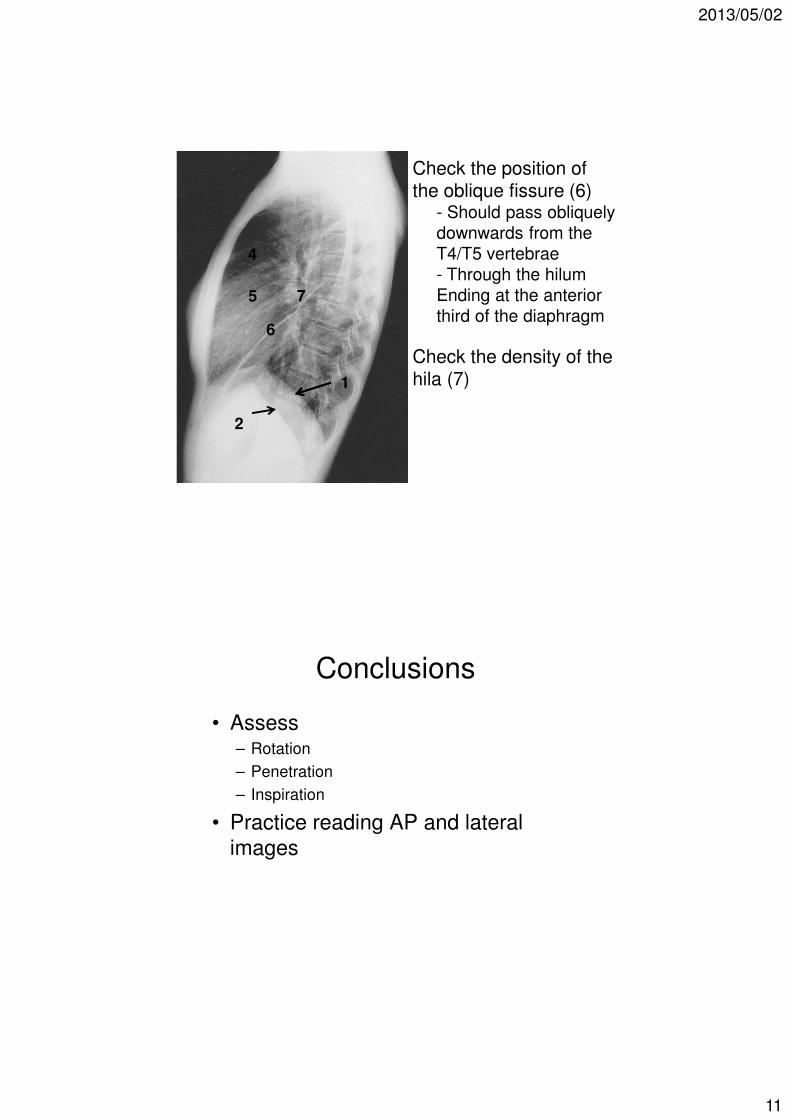
Check the position of the oblique fissure (6)
- Should pass obliquely
downwards from the
T4/T5 vertebrae
- Through the hilum
Ending at the anterior
third of the diaphragm
Check the density of the hila (7)
Conclusions
• Assess– Rotation
– Penetration
– Inspiration
• Practice reading AP and lateral
images
2013/05/02
12
Systematic approach
• White things (3)
– Mediastinum
– Heart shadow
– Bones / soft tissue (remember the spine in TB)
• Black things (3)
– Stomach bell
– Airways
– Lung fields
2013/05/02
13
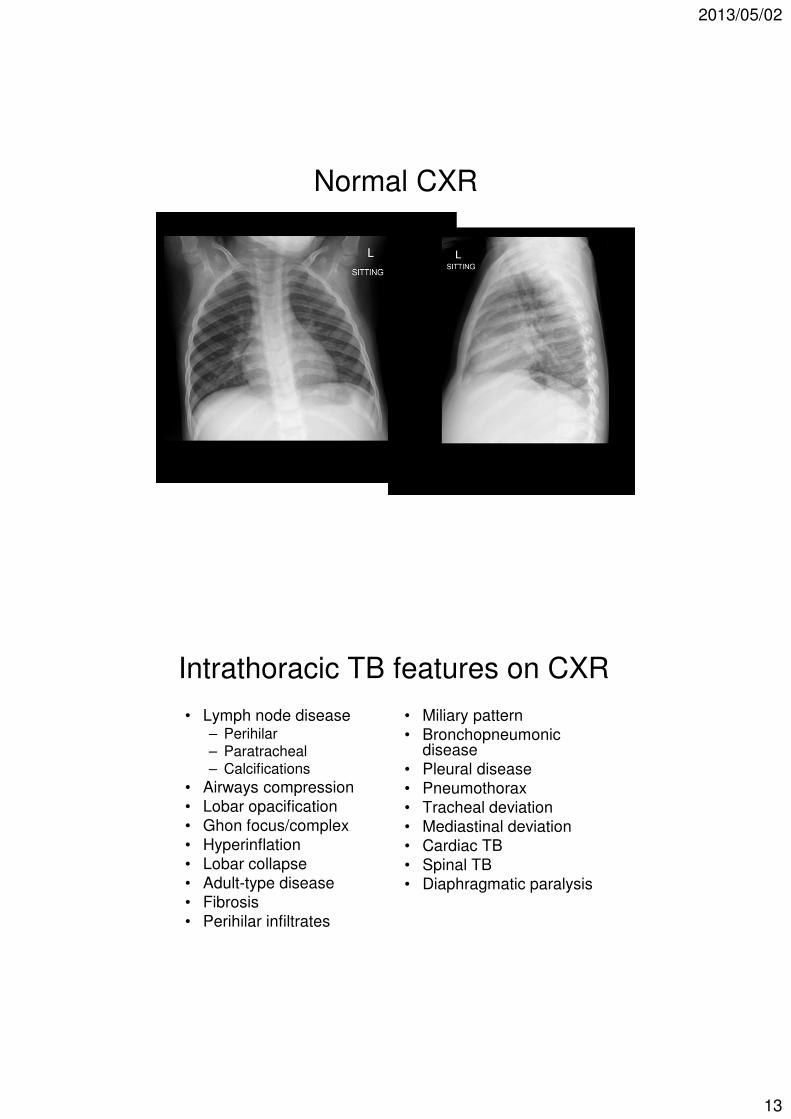
Normal CXR
Intrathoracic TB features on CXR
• Lymph node disease– Perihilar– Paratracheal– Calcifications
• Airways compression
• Lobar opacification
• Ghon focus/complex
• Hyperinflation
• Lobar collapse
• Adult-type disease
• Fibrosis
• Perihilar infiltrates
• Miliary pattern
• Bronchopneumonicdisease
• Pleural disease
• Pneumothorax
• Tracheal deviation
• Mediastinal deviation
• Cardiac TB
• Spinal TB
• Diaphragmatic paralysis