Embed Size (px)
Citation preview

CASE REPORT
Recurrent fever after a holiday in TurkeyAdrian Egli resident 1, Nina Khanna senior consultant 1, Thomas Schmid resident 2, Sonja Rudintechnician 3, Reno Frei head of division 3, Annette Blaich consultant 3
1Division of Infectious Diseases and Hospital Epidemiology, University Hospital Basel, CH-4031 Basel, Switzerland ; 2Department of Internal Medicine,University Hospital Basel; 3Division of Clinical Microbiology, University Hospital Basel
In early October 2010, a 64 year old man presented to ourhospital with chest pain, fever, and night sweats, which hadbeen present since his return to Switzerland three weeks earlier.He had been on holiday in Turkey from July to mid-September.On further questioning he reported an episode of diarrhoea andsickness associated with fever shortly after returning home toSwitzerland. During his stay in Turkey he had eaten fresh food,including meat and dairy products. Furthermore, he hadexperienced a myocardial infarction and had undergoneangiography and insertion of a bare metal stent on 4 Septemberwhile in Turkey.Previously he had been treated with a calcium channel blockerand an angiotensin II receptor antagonist because of high bloodpressure. On admission, aspartate aminotransferase at 79 U/L(reference range 11-36), alanine aminotransferase at 86 U/L(10-37), γ glutamyltransferase at 192 U/L (11-66), alkalinephosphatase at 238 U/L (0-129), and C reactive protein (CRP)at 25.4 mg/L (0-10) were all slightly raised. Stenosis of the rightcoronary artery was seen on angiography and another stent wasinserted. Over the next seven days he developed recurrent fevers,which were accompanied by chills and temperatures as high as39.5°C. Ten of 13 aerobic blood cultures taken at three to 10days after presentation grew very small Gram negative rods twoand a half to three days after incubation. Bloods taken duringthis time showed a normal white cell count and slightlydecreased haemoglobin of 130 g/L (140-180). An abdominalultrasound showed an enlarged spleen and mild hepatosteatosis.Computed tomography of the chest and abdomen andtransoesophageal echocardiography were performed to look fora source of infection, but all were uninformative.
Questions1 What bacterial infection do you suspect?2 What further tests might help to confirm the suspecteddiagnosis?3 How is this condition transmitted?
4 What are the most common signs and symptoms of thiscondition?5 How would you treat this patient?
Answers1 What bacterial infection do you suspect?Short answerBrucellosis.
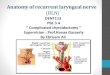
Long answerBrucellosis is the most likely cause of this man’s symptomsbecause of his travel history and the solely aerobic growth ofvery small Gram negative rods in blood cultures (fig 1) after amedian time to positivity of 61 hours in the automated bloodculture system (BacT/ALERT; bioMérieux). The time topositivity is defined as the period between the start of incubationof a blood culture and the detection of bacterial growth, and themedian time to positivity is the median of the time to positivityof all positive cultures. The median time to positivity ofbrucellosis has been previously described as 62.4 hours in theBacT/ALERT system.1 Fastidious bacteria such asHaemophilusinfluenzae andAggregatibacter aphrophilus are also small Gramnegative rods that resemble Brucella spp. However, Hinfluenzae, the most common isolated species, grows faster thanBrucella, with a median time to positivity of 25 hours, makingthis a less likely cause. Furthermore, Haemophilus spp andAggregatibacter spp grow under aerobic and anaerobicconditions (facultative anaerobes), in contrast toBrucella, whichis an obligate aerobe.
Correspondence to: A Blaich [email protected]
For personal use only: See rights and reprints http://www.bmj.com/permissions Subscribe: http://www.bmj.com/subscribe
BMJ 2011;343:d7832 doi: 10.1136/bmj.d7832 (Published 16 December 2011) Page 1 of 3
Endgames
ENDGAMES

Fig 1 Gram stain (original magnification, ×1000) of theblood cultures showing very small coccoid Gram negativerods in clusters (black arrow). The black patches are coalparticles that are found in the culture medium
The standard incubation time for blood cultures is five to sevendays, but Brucella spp are slow growing organisms, so if thediagnosis is suspected cultures should be incubated for at leastfour weeks.2 It is important to inform the laboratory of asuspected diagnosis of brucellosis to ensure that cultures arekept for the appropriate time. Laboratory staff also need to beaware of the suspected diagnosis, so that they can enforce strictersafety precautions when handling the specimens, becauseBrucella is highly contagious and the most commonly reportedlaboratory acquired infection.1 3
2What further testsmight help to confirm thesuspected diagnosis?Short answerIdentification of the bacterium with biochemical and molecularmethods; serological assays.
Long answerThe best way to diagnose brucellosis is by isolating thebacterium from blood, bone marrow, or tissue samples.2Preliminary identification at the genus level for Brucella sppcan be performed by using a biochemical identification system(such as Vitek 2; bioMérieux) and testing for severalbiochemical reactions (production of hydrogen sulphide,oxidase, and urease).2 Molecular methods (DNA sequencing,polymerase chain reaction) can be used to identify Brucella atthe genus and species levels.4 If Brucella cannot be isolated,serum agglutination to detect antibodies against the organismcan be useful for confirming the infection. A single titre of 1:160or more, or a fourfold increase in titre in paired serum samples(two or more weeks apart), confirms brucellosis.2 3 Positivetitres are seen in 94.9% of people with acute brucellosis.5 Thetitres remain high for a long time so they cannot be used tomonitor the success of antimicrobial treatment,2 and they maybemisleading in people who come from endemic regions, wheremany people are repeatedly exposed to Brucella.4 5 Therefore,the diagnosis of brucellosis should rely on the patient’s history,the clinical signs and symptoms, and the isolation of theorganism.2 4 5
3 How is this condition transmitted?Short answerTransmission is via consumption of unpasteurised dairyproducts.
Long answerIn endemic regions, such as the Mediterranean basin (forexample, Turkey), Brucella is usually transmitted byconsumption of unpasteurised dairy products, especially milk,cream, ice cream, butter, and soft cheese.2 6 In non-endemiccountries, infection is seen mostly in travellers to endemic areasor immigrants from these areas; it is also rarely caused byoccupational exposure (by inhalation of aerosolisedorganisms).2 3 5 6 Abattoir workers, veterinarians, and farmersmay be exposed to contagious aerosols that come from thesecretions and meat of infected animals.3 Brucella melitensis isthe most common causative species of brucellosis—so calledMalta fever.2 In Europe there are endemic, non-endemic (forexample, northern France), and brucellosis-free regions (forexample, the United Kingdom).6
4 What are the most common signs andsymptoms of this condition?Short answerFever, arthralgia, fatigue, sweating, chills, hepatomegaly,splenomegaly, anaemia, and raised C reactive protein.
Long answerThe onset of symptoms may be acute or creeping, but theyusually begin within two to four weeks of exposure.2 7
Brucellosis may present with a wide spectrum of symptomsbecause it can affect any tissue in the human body.2 4 5 7 Feveris the most common feature, followed by arthralgia andsymptoms such as fatigue, sweating, lack of appetite, chills, andweight loss.2 4 5 Fever may be undulant but also protracted, andmalodorous perspiration is almost a pathognomonic sign.2 7
Hepatomegaly and splenomegaly may be seen.2 Commonunspecific laboratory findings are anaemia and raised C reactiveprotein and transaminases.5 Endocarditis is rare but is the mostserious complication, with high mortality.2 4 5No defined criteriaare available to grade the disease in an acute, subacute, orchronic form—the classification is arbitrary.2 7 Relapses arecommon and usually not caused by antibiotic resistance.4 7
5 How would you treat this patient?Short answerTreatment is with a combination of antibiotics that are effectiveon bacteria that live inside phagocytic cells.
Long answerBrucella has the capacity to survive and replicate insidephagocytic cells, such as macrophages and dentritic cells.2 4 8
Therefore, treatment is based on antibiotics that kill intracellularmicro-organisms in infected cells. Doxycycline and rifampicincan both penetrate cell membranes,9 10 but aminoglycosides suchas gentamicin are poor at crossing this barrier.11 However, theaddition of gentamicin or streptomycin to treatment withdoxycycline lowers the relapse rate.4 12 Because of the highrelapse rate associated with monotherapy, brucellosis is usuallytreated with a combination of antibiotics.2 12 The World HealthOrganization recommends a doxycycline based regimen for atleast six weeks plus streptomycin for the first two to three weeksor rifampicin for six weeks; triple therapy can be used in severecases.4 Streptomycin may be replaced by gentamicin.12
For personal use only: See rights and reprints http://www.bmj.com/permissions Subscribe: http://www.bmj.com/subscribe
BMJ 2011;343:d7832 doi: 10.1136/bmj.d7832 (Published 16 December 2011) Page 2 of 3
ENDGAMES

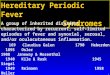
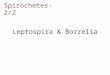
Patient outcomeTransfer of liquid from the positive blood cultures on to solidagar (subculturing) yielded very small transparent colonies afteraerobic incubation overnight; the colonies had a whitish colourafter three days and were white after seven days (figs 2 and 3).Brucella melitensiswas identified. If the first febrile episode inmid-September was taken to be the beginning of the illness,diagnosis and antimicrobial treatment was established fourweeks later and the fever resolved permanently after four anda half weeks (day 11). The treatment was intended for threemonths because of the prolonged bacteraemia; a brucellarendocarditis could not completely be ruled out despite aninconspicuous transoesophageal echocardiography. During the19 days that the patient was in hospital, aspartateaminotransferase, alanine aminotransferase, and C reactiveprotein normalised; γ glutamyltransferase and alkalinephosphatase dropped to 108 U/L and 138 U/L, respectively;and the serum agglutination test remained at a titre of 1:5120.Nine weeks later, at the last follow-up, the titre had dropped to1:640 and the patient was in good health.
Fig 2 Growth on blood agar after three days
Fig 3 Growth on blood agar after seven days
Thanks to Alex Schwank who provided some of the patient’s informationbefore his admission to hospital.
Competing interests: All authors have completed the ICMJE uniformdisclosure form at www.icmje.org/coi_disclosure.pdf (available onrequest from the corresponding author) and declare: no support fromany organisation for the submitted work; no financial relationships withany organisations that might have an interest in the submitted work inthe previous three years; no other relationships or activities that couldappear to have influenced the submitted work.Provenance and peer review: Not commissioned; externally peerreviewed.Patient consent obtained.
1 Baysallar M, Aydogan H, Kilic A, Kucukkaraaslan A, Senses Z, Doganci L. Evaluation ofthe BacT/ALERT and BACTEC 9240 automated blood culture systems for growth timeof Brucella species in a Turkish tertiary hospital. Med Sci Monit 2006;12:BR235-38.
2 Pappas G, Akritidis N, Bosilkovski M, Tsianos E. Brucellosis. N Engl J Med2005;352:2325-36.
3 Centers for Disease Control and Prevention. Brucellosis. 2007. www.cdc.gov/ncidod/dbmd/diseaseinfo/Brucellosis_g.htm.
4 Franco MP, Mulder M, Gilman RH, Smits HL. Human brucellosis. Lancet Infect Dis2007;7:775-86.
5 Buzgan T, Karahocagil MK, Irmak H, Baran AI, Karsen H, Evirgen O, et al. Clinicalmanifestations and complications in 1028 cases of brucellosis: a retrospective evaluationand review of the literature. Int J Infect Dis 2010;14:e469-78.
6 Pappas G, Papadimitriou P, Akritidis N, Christou L, Tsianos EV. The new global map ofhuman brucellosis. Lancet Infect Dis 2006;6:91-9.
7 Young EJ. Brucella species. In: Mandell GL, Bennett JE, Dolin R, eds. Principles andpractice of infectious diseases. 7th ed. Churchill Livingstone, 2010:2921-5.
8 Roop RM II, Gaines JM, Anderson ES, Caswell CC, Martin DW. Survival of the fittest:how Brucella strains adapt to their intracellular niche in the host. Med Microbiol Immunol2009;198:221-38.
9 Sabundayo BP, Standiford HC. Tetracyclines and analogues. In: Yu VL, Edwards G,McKinnon PS, Peloquin C, Morse GD, eds. Antimicrobial therapy and vaccines. Vol II:antimicrobial agents. 2nd ed. ESun Technologies, 2005:461-76.
10 Peloquin CA, Vernon AA. Rifamycins for mycobacterial infections. In: Yu VL, Edwards G,McKinnon PS, Peloquin C, Morse GD, eds. Antimicrobial therapy and vaccines. Vol II:antimicrobial agents. 2nd ed. ESun Technologies, 2005:383-401.
11 Lecároz C, Blanco-Prieto MJ, Burrell MA, Gamazo C. Intracellular killing of Brucellamelitensis in humanmacrophages withmicrosphere-encapsulated gentamicin. J AntimicrobChemother 2006;58:549-56.
12 Ariza J, Bosilkovski M, Cascio A, Colmenero JD, Corbel MJ, Falagas ME, et al.Perspectives for the treatment of brucellosis in the 21st century: the Ioanninarecommendations. PLoS Med 2007;4:1872-78.
Cite this as: BMJ 2011;343:d7832© BMJ Publishing Group Ltd 2011
For personal use only: See rights and reprints http://www.bmj.com/permissions Subscribe: http://www.bmj.com/subscribe
BMJ 2011;343:d7832 doi: 10.1136/bmj.d7832 (Published 16 December 2011) Page 3 of 3
ENDGAMES