Embed Size (px)
Citation preview

An agency of the European Union
Regulatory requirements for early clinical testing of novel HCV antiviral drugs – the EU perspective
Filip Josephson M.D., Ph.D. Clinical Assessor Swedish Medical Products Agency
Presented at the 6th International Workshop on Clinical Pharmacology of Hepatitis Therapy, 22-23 June 2011, Cambridge, USA

Presented at the 6th International Workshop on Clinical Pharmacology of Hepatitis Therapy, 22-23 June 2011, Cambridge, USA
The European Regulatory System (1)
• The European Medicines Agency (EMA) is a decentralised regulatory agency of the European Union, located in London
• Each European Union member state retains a national competent authority
• The EMA Committee for Medicinal Products for Human Use (CHMP) is the decision-making body concerning drug approved through the “centralised procedure” for use in the European Union
• If the CHMP concludes that the risk-benefit of the medicinal product is sufficiently proven and positive, it adopts a positive opinion. This is sent to the European Commission to be transformed into a marketing authorisation valid for the whole of the EU.
The European Medicines Agency 2

Presented at the 6th International Workshop on Clinical Pharmacology of Hepatitis Therapy, 22-23 June 2011, Cambridge, USA
The European Regulatory System (2)
• All antivirals are approved through the “centralised procedure”
• The applicant’s dossier is primarily assessed by assigned national authorities (rapporteur/co-rapporteur), reviewed by all member state national agencies, and approved through the EMA/CHMP
• However, decisions on the approval of clinical trial protocols are taken by local ethics committees and National regulatory authorities
• EMA/CHMP guidelines for drug development de facto serve both externally as guidance for sponsors and internally as consensus documents
The European Medicines Agency 3

Presented at the 6th International Workshop on Clinical Pharmacology of Hepatitis Therapy, 22-23 June 2011, Cambridge, USA
The European Medicines Agency 4
Insert draft GL front page
Provides guidance on the clinical development of compounds for the treatment of Chronic Hepatitis C (CHC), including directly acting antivirals (DAAs) as well as host targeting antivirals (HTA).

Presented at the 6th International Workshop on Clinical Pharmacology of Hepatitis Therapy, 22-23 June 2011, Cambridge, USA
The approval procedures for Victrelis
(Boceprevir) and Incivo (telaprevir)
• Dossier assessments have provided further information and understanding since the adoption of the draft guidance
• The approval of the first generation NS3/4A inhibitors is changing the treatment paradigm with consequences for clinical trial design (e.g., control regimens)
The European Medicines Agency 5

Presented at the 6th International Workshop on Clinical Pharmacology of Hepatitis Therapy, 22-23 June 2011, Cambridge, USA
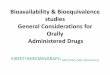
BMS-790052 + BMS-650032 ± PegIFN/RBV
for 24 Wks in GT1 Null Responders
In dual therapy arm, 2/2 GT1b vs
2/9 GT1a patients reached SVR12
and SVR24
No viral breakthrough with
quadruple therapy
Lok A, et al. EASL 2011. Abstract 1356.
BMS-790052 60 mg QD + BMS-650032 600 mg BID
(n = 11) Phase IIa study: GT1 null responders*
with HCV RNA ≥ 105 IU/mL
(N = 21)
Follow-up 48 wks BMS-790052 60 mg QD +
BMS-650032 600 mg BID + PegIFN/RBV
(n = 10)
Week 24 Stratified by HCV subtype
(1a vs 1b)
*< 2 log10 IU/mL decline in HCV RNA with ≥ 12 wks of pegIFN/RBV.
†1 patient not achieving SVR24 had HCV RNA < 25 IU/mL at EOT and undetectable on retesting at Day 35 of follow-up.
Undetectable HCV RNA, % (n)
BMS-790052 +
BMS-650032 (n = 11)
BMS-790052 + BMS-650032 +
PR (n = 10)
RVR 64 (7) 60 (6)
SVR12 36 (4) 100 (10)
SVR24 36 (4) 90† (9)
6

Presented at the 6th International Workshop on Clinical Pharmacology of Hepatitis Therapy, 22-23 June 2011, Cambridge, USA
EMA/CHMP expectations on preclinical virology assessment
• Cell-free functional assays (such as polymerase or protease assays) and cell-based assays such as the HCV replicon system are generally used in the study of anti-HCV activity in vitro, to define genotype/subtype specific antiviral activity, including the assessment of phenotypic resistance
• The risk of selection of drug resistant variants, their in vitro susceptibility and associated genotypic substitutions, and the potential for cross-resistance with other agents should be evaluated. In vitro studies of resistance are expected also for HTAs.
• The in vitro antiviral activity of a new agent should be investigated in combination with interferon, ribavirin and other potential agents for use in combination, as relevant.
The European Medicines Agency 7

Presented at the 6th International Workshop on Clinical Pharmacology of Hepatitis Therapy, 22-23 June 2011, Cambridge, USA
It is anticipated that PK and initial safety data in most
cases be generated in healthy volonteers prior to
conducting trials in patients
The European Medicines Agency 8
• The general principles for the preclinical investigation prior to studies in humans apply, as described in the relevant ICH/CHMP guidance

Presented at the 6th International Workshop on Clinical Pharmacology of Hepatitis Therapy, 22-23 June 2011, Cambridge, USA
Virological considerations prior to dose finding
monotherapy studies in patients with hepatitis
C virus infection
• An adequate range of doses should be studied, based on (protein binding-adjusted) IC50 values in vitro and on available PK data
• IC50 values of both wild-type virus and viruses with resistance mutations (single and in combination) derived during drug pressure in vitro should be taken into account, so that selected doses for combination studies could provide sufficient exposure for activity also against variants with reduced sensitivity, if this is feasible
• An understanding of the resistance profile (barrier to resistance) is needed to inform the conduct of the monotherapy study (e.g. the relevant duration)
The European Medicines Agency 9

Presented at the 6th International Workshop on Clinical Pharmacology of Hepatitis Therapy, 22-23 June 2011, Cambridge, USA
Dose finding monotherapy studies (1)
• Currently, 3 days of monotherapy, covering the first phase of viral decay, is considered sufficient in the general case
• Due to the risk of selection of drug resistant variants, it is expected that monotherapy studies would initially be performed in treatment naïve patients without advanced fibrosis
The European Medicines Agency: Overview and structure 10

Presented at the 6th International Workshop on Clinical Pharmacology of Hepatitis Therapy, 22-23 June 2011, Cambridge, USA
Dose finding monotherapy studies (2)
• There have been instances where differential effects between doses are seen in the second phase of viral decay but not in the first, and there may be a differential risk of early viral breakthrough between doses; thus a longer period of monotherapy may in fact be informative
• A longer period of monotherapy may increase the risk of acquired drug resistance.
• If there is a strong scientific rationale to prolong this period of monotherapy, longer duration studies could be warranted. In such a decision, the anticipated barrier to resistance of the compound should be taken into account.
The European Medicines Agency 11

Presented at the 6th International Workshop on Clinical Pharmacology of Hepatitis Therapy, 22-23 June 2011, Cambridge, USA
Further dose finding studies (phase 2a)
• Further dose-ranging studies are expected to be performed in combination with other agents.
• For studies of regimens including pegIFN + ribavirin viral response at 4 weeks, supported by efficacy and safety data at week 12 have generally been used to select doses for phase 2b trials aiming at estimating SVR rates
• Hitherto pegIFN+ribavirin has been used as reference treatment in the control group of phase 2a studies, and continued therapy with pegIFN+ribavirin has often been offered to all participants after the end of study
• How does a new standard of care affect the latter considerations? The European Medicines Agency: Overview and structure 12

Presented at the 6th International Workshop on Clinical Pharmacology of Hepatitis Therapy, 22-23 June 2011, Cambridge, USA
Host IL28B genotype
• Categorisation of patients with GT1 infection on the basis of a favourable or non-favourable genotype (e.g., rs12979860 C/C vs C/T, T/T) is of putative importance at several levels of drug development.
• When dose-ranging a DAA or HTA in a combination including pegIFN, it is recommended to stratify by IL28B genotype, as this not only reduces variability, but the optimal dose of the investigational agent may vary depending on genotype.
• Since IL28B genotype may also determine the optimal duration of therapy, and the incremental benefit of a new regimen may vary depending on IL28B genotype, similar stratification is valuable also later in drug development, including confirmatory trials.
The European Medicines Agency: Overview and structure 13

Presented at the 6th International Workshop on Clinical Pharmacology of Hepatitis Therapy, 22-23 June 2011, Cambridge, USA
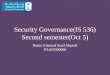
Implications of IL28B genotype for dose-ranging trials including pegIFN
From Thompson et al, Gastroenterology 2010

Presented at the 6th International Workshop on Clinical Pharmacology of Hepatitis Therapy, 22-23 June 2011, Cambridge, USA
Aspects of the virological rational for DAA/HTA combination studies
• Are there additive/synergistic effects in vitro?
• Is the likely sufficient sum “barrier to resistance” sufficient for each relevant genotype/subtype?
The European Medicines Agency 15

Presented at the 6th International Workshop on Clinical Pharmacology of Hepatitis Therapy, 22-23 June 2011, Cambridge, USA
Requirements for combination toxicology
studies for DAA/HTA combinations
• General guidelines for preclinical toxicology studies including the SWP guideline on combination toxicology (EMEA/CHMP/SWP/258498/2005) and ICH M3(R2) should be followed
• However, combination toxicology studies are not required “by default”
• Combination toxicology studies may be required if there are specific concerns about additive or synergistic toxicity. In case of unexpected toxicities with the combination in clinical trials, further preclinical studies may be warranted to elucidate the mechanism of toxicity
The European Medicines Agency: Overview and structure 16

Presented at the 6th International Workshop on Clinical Pharmacology of Hepatitis Therapy, 22-23 June 2011, Cambridge, USA
DDI studies prior to DAA/HTA combo trials
• The general principles of EMA/CHMP guidelines on the investigation of DDI are relevant
• Depending on available data on the pharmacokinetic interaction potential of the drugs to be combined, formal DDI studies in healthy volonteers may be needed prior to clinical combination trials, but such are not demanded by default
• PK is recommended to be investigated within early combination trials
• The possibility of transporter interactions should be kept in mind
The European Medicines Agency 17

Presented at the 6th International Workshop on Clinical Pharmacology of Hepatitis Therapy, 22-23 June 2011, Cambridge, USA
Studies of 2 or more DAA/HTA without pegIFN (1)
• Prior to combination therapy, each agent should be dose ranged in monotherapy studies, and results from drug interaction studies, if needed, should be at hand
• Investigating a least one of the agents along with pegIFN+ribavirin(e.g., 4-12 weeks study) is likely helpful in understanding the safety issues seen when DAA/HTAs are used in combination
• If neither agent has been studied without the other apart from very short term monotherapy, disentangling the safety profile of each agent per se may be difficult.
• Alternative approaches?
The European Medicines Agency 18

Presented at the 6th International Workshop on Clinical Pharmacology of Hepatitis Therapy, 22-23 June 2011, Cambridge, USA
Studies of 2 or more DAA/HTA without pegIFN (2)
• Due to the risk of selecting for drug resistance with still not fully investigated consequences for re-treatment, the first dose ranging studies of novel drug combinations should be performed in patient populations that can readily be salvaged with licensed therapeutic options in case of failure
• It is recommended that studies aiming at proof-of-concept for regimens without pegIFN include at least one treatment arm with ribavirin added to the experimental combination
The European Medicines Agency 19

Presented at the 6th International Workshop on Clinical Pharmacology of Hepatitis Therapy, 22-23 June 2011, Cambridge, USA
Studies of 2 or more DAA/HTA without pegIFN (3)
• The initial duration of such studies may be short (2-4 weeks) and the patients offered to continue with a licensed treatment alternative
• However, it may be that a longer duration of therapy may be appropriate already in early trials, to estimate the risk of viral breakthrough (available data indicate that viral breakthrough post week 4 may be relevant for the evaluation of a regimen)
• Initial trials with protocols up to, e.g., 12 weeks of duration may be considered, provided that there is intense real-time monitoring.
• Patients with end-of-treatment response could undergo viral monitoring after the end of therapy, with the follow-up regimen only being started if virus again becomes detectable when previously undetectable. This would allow for the detection of a putative SVR within the first trial The European Medicines Agency 20

Presented at the 6th International Workshop on Clinical Pharmacology of Hepatitis Therapy, 22-23 June 2011, Cambridge, USA
Alternative populations in proof-of-concept (of SVR) studies of pegIFN sparing experimental combination regimens
1. A population that might readily be salvaged with licensed therapeutic options
Or, provided that there are promising initial studies in patients with HCV and less advanced liver disease, as well as relevant PK data:
2. Patients with an immediate medical need that are deemed not to tolerate existing treatment options (i.e patients with very advanced cirrhosis and some signs of decompensation); this requires that the patients be fully informed about the lack of proof-of-concept
Patients on a transplantation waiting list might provide a bridging population to the general decompensated group
The European Medicines Agency: Overview and structure 21

Presented at the 6th International Workshop on Clinical Pharmacology of Hepatitis Therapy, 22-23 June 2011, Cambridge, USA
Populations not to include in proof-of-concept studies of pegIFN sparing combination regimens
• A population that should not be subjected to experimental regimens prior to obtaining proof-of-concept, and where drug resistance in case of failure is a risk, are patients that may not respond to licensed therapeutic options, but are not considered in immediate need of therapy (e.g., pegIFN null responders without advanced fibrosis)
The European Medicines Agency: Overview and structure 22