Embed Size (px)
Citation preview

Relationships Between Environmentand Quality of Life of Older Adults
with Physical Disabilities
Mélanie Levasseur, OT(C), MScJohanne Desrosiers, OT(C), PhD
Luc Noreau, PhD
ABSTRACT. This exploratory study used a convenience sample (n =46) to verify the relationships between self-perceived environment (Mea-sure of the Quality of the Environment) and subjective quality of life(Quality of Life Index) of community-dwelling older adults with physi-cal disabilities. Global scores for environment and quality of life werenot statistically related. However, the “Social support and attitudes” cat-egory of the environment was statistically related to quality of life. Also,the “Socioeconomic” quality of life was statistically associated with theenvironment. These exploratory findings might suggest that the social
Mélanie Levasseur is affiliated with the Research Centre on Aging, Sherbrooke Ge-riatric University Institute, Québec, Canada and Sherbrooke CLSC, Québec, Canada.
Johanne Desrosiers is affiliated with the Research Centre on Aging, SherbrookeGeriatric University Institute, Québec, Canada and the Family Medicine Department,Faculty of Medicine, Université de Sherbrooke, Québec, Canada.
Luc Noreau is affiliated with the Centre for Interdisciplinary Research in Rehabili-tation and Social Integration, Québec, Canada and the Rehabilitation Department, Fac-ulty of Medicine, Université Laval, Québec, Canada.
Address correspondence to: Mélanie Levasseur, OT(C), MSc, Research Centre onAging, Sherbrooke Geriatric University Institute, 1036 Belvédère South, Sherbrooke,Québec, Canada J1H 4C4 (E-mail: [email protected]).
The authors were supported by fellowships from the Fonds de la recherche en santédu Québec (FRSQ) and the Canadian Institutes of Health Research (CIHR).
Physical & Occupational Therapy in Geriatrics, Vol. 22(3) 2004http://www.haworthpress.com/web/POTG
2004 by The Haworth Press, Inc. All rights reserved.Digital Object Identifier: 10.1300/J148v22n03_03 37
Phys
Occ
up T
her
Ger
iatr
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f N
orth
Dak
ota
on 1
0/29
/14
For
pers
onal
use
onl
y.

environment is more important than the physical environment in regardsto the quality of life of this population. [Article copies available for a feefrom The Haworth Document Delivery Service: 1-800-HAWORTH. E-mail ad-dress: <[email protected]> Website: <http://www.HaworthPress.com> © 2004 by The Haworth Press, Inc. All rights reserved.]
KEYWORDS. Environment, quality of life, physical disabilities, olderadults
Limited health care resources and an aging population have raisedconcerns about community-dwelling older adults with physical disabil-ities. The physical and social environment, which is defined as externalcontexts and situations that individuals respond to (Law, 1991), shouldhelp these people meet their needs and appears to be one of the most im-portant factors for maintaining them in the community. It is recognizedthat an adaptive environment is important for people with physical dis-abilities (Richards et al., 1999), especially those who have moderate tosevere physical disabilities. Consequently, the quality of the environ-ment might have an impact on their quality of life (QOL).
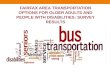
To address this issue, it is necessary to have a proper conceptualiza-tion of the disablement process which explains the various conse-quences of disease, trauma or aging. One of the existing models, theDisability Creation Process (DCP) conceptual model (Figure 1; Fougey-rollas et al., 1998), can be used to illustrate the potential contribution ofthe environment to a person’s social participation (daily activities andsocial roles). This model was developed through the revision process ofthe World Health Organization (WHO) International Classification ofImpairments, Disabilities and Handicaps (ICIDH; WHO, 1980; 1993;1997) which was updated recently (WHO, 2001). DCP is characterizedby the interactions between personal factors (age, gender, socioculturalidentity, impairments and disabilities), environmental factors, and par-ticipation in daily activities and social roles (life habits). Participation isconsidered a situational result that is strongly influenced by the qualityof the person’s environment. Environmental factors include physicaland social dimensions and are characterized as facilitators or obstacles.A “facilitator” environment helps people in their daily activities and so-cial roles, while an “obstacle” environment limits them. The environ-ment of a person who lives with disabilities has to compensate forpersonal deficits to allow optimal social participation and reduce or pre-vent the development of handicap situations (Fougeyrollas, 1994).
38 PHYSICAL & OCCUPATIONAL THERAPY IN GERIATRICS
Phys
Occ
up T
her
Ger
iatr
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f N
orth
Dak
ota
on 1
0/29
/14
For
pers
onal
use
onl
y.

Quality of life is the ultimate goal of physical and occupational ther-apy interventions (Day & Jankey, 1996). However, this concept is vague,varies over time and is unique to each person, and there is no consensusin the literature regarding its definition. Consequently, there is no goldstandard to measure or even estimate it. Some QOL measures are objec-tive while others are subjective. Objective QOL is usually estimatedwith health-related questionnaires such as the Medical Outcomes Study36-item Short-Form Health Survey (SF-36) (McHorney, Ware, Lu &Sherbourne, 1994). According to Dijkers (1997a), subjective QOL shouldtake into consideration the person’s cognitive and emotional percep-tions. It may be defined as the temporal perspective of the gap between aperson’s expectations and his/her achievements (Calman, 1984). Thecongruence between what a person feels or thinks about how life shouldbe and what he/she actually has, owns, or controls, produces a cognitiveor emotional reaction such as satisfaction or dissatisfaction, happinessor depression. A concept analysis in the context of older adults withphysical disabilities (Levasseur, St-Cyr Tribble & Desrosiers, submit-ted) defined QOL as a subjective evaluation of an individual’s life cir-cumstances according to his/her values. It demonstrates the importanceof physical, psychological, social and spiritual well-being, satisfaction
Levasseur, Desrosiers, and Noreau 39
Risk factors
Cause
Personal factors
OrganicSystems
Capabilities
Environmentalfactors
Facilitator ObstacleIntegrity Impairment Abilitiy Disability
Life habits
Interaction
Social participation Handicap situations
FIGURE 1. Disability Creation Process (Fougeyrollas et al., 1998)
Phys
Occ
up T
her
Ger
iatr
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f N
orth
Dak
ota
on 1
0/29
/14
For
pers
onal
use
onl
y.

with life and accomplishment of fulfilling occupations. The presence ofa satisfying functional status and adapted behaviors as well as a feelingof control over one’s life were also found to be essential components.Personal experience of living with physical disabilities is important inthe definition of self, vision of world, social context and relationships.QOL of people with physical disabilities is further defined in terms ofthe person’s ability to create and maintain balance between body, mindand spirit (Albrecht & Devlieger, 1999). It also depends on the creationand maintenance of harmonious relationships with the environment.
This study explored the relationships between self-perceived qualityof the environment and subjective QOL of community-dwelling olderadults with different levels of physical disabilities. Two research hy-potheses were formulated: (1) the environment is positively and signifi-cantly associated with QOL of older adults with physical disabilities,and (2) the relationship between environment and QOL is stronger forolder adults with moderate to severe physical disabilities than for thosewith minor physical disabilities.
METHODS
Participants. A convenience sample of community-dwelling adultsaged 60 and over was recruited from people receiving geriatric day hos-pital services and home care services from a local community servicecentre (CLSC). Eligibility criteria were: (1) preserved cognitive func-tions [Mini-Mental State Examination (MMSE) score above or equal tothe 25th percentile according to age and schooling (Bravo & Hébert,1997)]; (2) a level of functional autonomy indicating physical disabili-ties [Functional Autonomy Measurement System (SMAF; Hébert, Car-rier & Bilodeau, 1988) score above or equal to 5]; and (3) adequateunderstanding of French or English. People were excluded if they wereterminally ill or had moderate to severe language deficits.
Data Collection Procedures. This study used a cross-sectional de-sign and was approved by a Research Ethics Committee. All partici-pants signed an informed consent and were evaluated in their home bythe same occupational therapist. The evaluation began with the collec-tion of sociodemographic and clinical data: age, gender, residential sta-tus, living situation, socioeconomic status, medical diagnosis, durationof physical disabilities, self-perceived health, level of functional auton-omy and cognitive functions. The participants’ data on the main vari-
40 PHYSICAL & OCCUPATIONAL THERAPY IN GERIATRICS
Phys
Occ
up T
her
Ger
iatr
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f N
orth
Dak
ota
on 1
0/29
/14
For
pers
onal
use
onl
y.

ables were then collected, beginning with QOL and followed by qualityof the environment. To estimate refusal bias, sociodemographic andclinical data were also collected for those who refused to participate.
Measurement Instruments. Subjective QOL was estimated with theQuality of Life Index (QLI; Ferrans & Powers, 1985) that was devel-oped from Ferrans’ conceptual model of QOL. This instrument includes32 items related to four life domains (number of items): health and func-tioning (11), socioeconomic (10), psychological/spiritual (7), and fam-ily (4). Since the rank of values differs from person to person, each itemis evaluated in terms of satisfaction and importance. The satisfaction re-sponses are then adjusted according to importance in order to weighteach item. The total score therefore reflects not only satisfaction butalso how much the individual values each of the four domains. Re-sponses to each item are given by the participant on two 6-point Likertscales ranging from ‘very dissatisfied’ (1) to ‘very satisfied’ (6) or ‘notimportant’ (1) to ‘very important’ (6). The scale ranges from 0 to 30 foreach domain and the total score. Psychometric studies, carried out withhealthy subjects, graduate students and dialysis patients, showed ade-quate concurrent validity with a general satisfaction with life question (r =0.65 to 0.75), good test-retest reliability (r = 0.81 to 0.87) and highCronbach alphas of 0.90 to 0.93 (Ferrans & Powers, 1985).
Self-perceived environment was assessed using the Measure of theQuality of the Environment (MQE; Fougeyrollas, Noreau, St-Michel &Boschen, 1999) version 2.0. This questionnaire evaluates the influenceof the physical and social environment on a person when performinghis/her daily activities and social roles. The MQE comprises 109 itemsdivided into six categories which cover most aspects of the environment(number of items): social support and attitudes (14), income, labor andincome security (15), government and public services (27), equal op-portunities and political orientations (10), physical environment and ac-cessibility (38), and technology (5). In general, the first four categoriesrefer mainly to the social environment while the other two represent thephysical environment. The person’s perception is rated on a 7-pointLikert scale ranging from “major obstacle” (�3) to “major facilitator”(3). Two continuous scores, global (including the six categories) or bycategory, are calculated: an “obstacle” score and a “facilitator” score. Atest-retest reliability study carried out with adults with cerebral palsyshowed moderate to high kappas for 57% of the items (Boschen, Nor-eau & Fougeyrollas, 1998).
Statistical Analysis. Sociodemographic and clinical data were de-scribed by means and standard deviations or frequencies and percent-
Levasseur, Desrosiers, and Noreau 41
Phys
Occ
up T
her
Ger
iatr
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f N
orth
Dak
ota
on 1
0/29
/14
For
pers
onal
use
onl
y.

ages according to the type of variable (continuous or categorical, res-pectively). The Mann-Whitney test and Fisher’s exact test were used tocompare the sociodemographic characteristics of people who refused toparticipate with those who agreed. The presence of relationships be-tween the environment and QOL (global and category scores) were ver-ified with Spearman’s correlation coefficient (hypothesis 1). The equal-ity of correlation test (Fisher transformation) verified if the relationshipbetween the environment and QOL was stronger for older adults withmoderate to severe physical disabilities than those with minor physicaldisabilities (hypothesis 2). Estimation of the sample size was based onthe first hypothesis. Forty-six participants were necessary to detect cor-relations equal to or above 0.40, as significantly different from zero,based on a Type I error of 0.05 and a power of 80% (Machin, Campbell,Fayers & Pinol, 1997). Given the exploratory nature of this study and inorder to limit the likelihood of a Type II error, correlations with a signif-icance level under 0.15 were considered of interest.
RESULTS
Fifty-seven people were contacted in order to obtain the predeter-mined sample size since 11 of them refused. The remaining participants(n = 46) were interviewed during November or December 2000. Char-acteristics of the participants and refusals are presented in Table 1. Theywere equivalent with the exception of the “self-perceived health” vari-able, where those who refused to participate perceived themselves to bein better health than those who agreed. The participants, equally distrib-uted by gender, were aged between 60 and 90 years old. The majorityhad less than 11 years of education, lived at home with a spouse orother(s), and perceived themselves to be in fair or better health thanother people their age. In addition, for the most part, they had had dis-abilities for more than six months. These disabilities were mainly re-lated to orthopedic problems (e.g., hip fracture, amputation), followedby stroke and other medical conditions (e.g., arthritis). The functionalautonomy measurement scores indicated minor to severe physical dis-abilities.
Environment and QOL scores are shown in Table 2. The facilitatorand obstacle scores of the MQE clearly indicate that the environment isgenerally perceived as being more of a facilitator than an obstacle. A cu-mulative mean of 127 points indicates that the environment makes apositive contribution to the participants’ daily activities and social roles,
42 PHYSICAL & OCCUPATIONAL THERAPY IN GERIATRICS
Phys
Occ
up T
her
Ger
iatr
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f N
orth
Dak
ota
on 1
0/29
/14
For
pers
onal
use
onl
y.

Levasseur, Desrosiers, and Noreau 43
TABLE 1. Characteristics of participants (n = 46) and refusals (n = 11)
Continuous variablesI Participants Refusals p valueAge (years) 77.0 (6.9)* 76.0 (6.6) 0.58Functional autonomy (SMAF; /87) 19.6 (10.8) 19.5 (10.4) 0.57Cognitive functions (2MS; /30) 28.1 (1.2) 27.9 (1.4) 0.90Categorical variablesII
Gender:-Women 23 (50)** 6 (54.5) 1.00-Men 23 (50) 5 (45.5)
Residential status:- Owner 16 (34.8) 5 (45.5) 0.80-Tenant 19 (41.3) 3 (27.3)-Sheltered 8 (17.4) 3 (27.3)-Religious community 3 (6.5) 0
Living situation:- Alone 14 (30.4) 1 (9.1) 0.40- With spouse 19 (41.3) 7 (63.6)- With family members 3 (6.5) 0- Other 10 (21.7) 3 (27.3)
Income:
- < 10,000 2 (4.3) 0 0.09- 10,001-15,000 16 (34.8) 0- 15,001-20,000 7 (15.2) 1 (9.1)- 20,001-25,000 6 (13.0) 3 (27.3)- 25,001-40,000 8 (17.4) 4 (36.4)- > 40,001 5 (10.9) 0- Missing data 2 (4.3) 3 (27.3)
Medical diagnosis:- Orthopedic 26 (56.5) 9 (81.8) 0.38- Neurological 14 (30.4) 1 (9.1)- Medical 6 (13.0) 1 (9.1)
Duration of physical disabilities:- < 6 months 10 (21.7) 3 (27.3) 0.38- 6 months to 1 year 12 (26.1) 2 (18.2)- 1 year to 3 years 11 (23.9) 1 (9.1)- > 3 years 13 (28.3) 0- Missing data 1 (9.1)
Self-perceived health:- Excellent 1 (2.2) 1 (9.1) 0.03- Good 16 (34.8) 7 (63.6)- Fair 25 (54.3) 1 (9.1)- Poor 4 (8.7) 1 (9.1)- Missing data 1 (9.1)
IMann-Whitney test
IIFisher’s exact test
* Mean (standard deviation) ** Frequency (percentage)
Phys
Occ
up T
her
Ger
iatr
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f N
orth
Dak
ota
on 1
0/29
/14
For
pers
onal
use
onl
y.

while 22 points indicates a negative contribution. The “Technology”category included the most facilitators, closely followed by the “Physi-cal environment and accessibility” and “Government and public ser-vices” categories. The “Physical environment and accessibility” categorywas also the one perceived as having the most obstacles. Globally, theQLI scores indicate that the QOL of the participants varied between“slightly satisfied” and “satisfied.” The mean score for the “Health andfunctioning” domain of the QLI was the lowest while the “Family” do-main was the highest. However, the wide range of the “Family” domainscores indicates that some participants had a very low QOL in this do-main.
The first hypothesis is rejected: no statistically significant relation-ship was found between the global scores on the MQE and QLI (Table3). However, despite a lack of significant associations between theglobal scores, significant associations exist between some categories ofthe MQE and specific QLI domains. A general trend is that QOL is as-sociated more with the social than the physical environment. Specifi-cally, associations between the “Social support and attitudes” categoryof the MQE and most QLI domains are the highest reported (up to 0.40).These are associated, for the most part, with both facilitator and obstacleenvironments. As well, the “Socioeconomic” category of the QLI is themost related to the MQE. The “Health and functioning” domain of theQLI was not related to the MQE. Despite the fact that “Physical envi-ronment and accessibility” is the environmental category that has themost obstacles, only one weak relationship was found with the “Socio-economic” domain of the QLI. The “Income, labor and income secu-rity,” “Government and public services” and “Technology” categoriesof the environment were not related to the QLI.
For the second hypothesis, no statistically significant differenceswere found between correlations of environment and QOL according tothe two levels of disabilities (Table 4). One tendency, however, doesemerge: QOL is more associated with environmental items perceived asfacilitators for people with minor physical disabilities (SMAF � 19)than for those with moderate to severe physical disabilities (SMAF> 19) whereas QOL is more associated with environmental items per-ceived as obstacles for people with moderate to severe physical disabili-ties than for those with minor physical disabilities. Further descriptivestatistics of the two groups showed they had very similar QLI (20.8 and20.1) and MQE (facilitator: 128 and 126; obstacle: 23 and 22) scores.
44 PHYSICAL & OCCUPATIONAL THERAPY IN GERIATRICS
Phys
Occ
up T
her
Ger
iatr
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f N
orth
Dak
ota
on 1
0/29
/14
For
pers
onal
use
onl
y.

DISCUSSION
Results from this exploratory study with our older adults with physi-cal disabilities suggest that they have relatively good QOL. The studyfailed to observe any significant relationships between perceived influ-ence of the environment and their subjective QOL as a whole. However,the “Social support and attitudes” category of the environment wasfound to be associated with the QLI. The “Socioeconomic” domain ofthe QLI was the most related to the MQE. Finally, no statistical differ-ence was found in the correlations between environment and QOL ac-cording to the two levels of physical disabilities.
In this study, the lack of association between environment and QOLmay be partly explained by the deeper meaning of QOL which takesinto consideration the person’s cognitive and emotional perceptions.
Levasseur, Desrosiers, and Noreau 45
TABLE 2. Environment and quality of life scores (n = 46)
Continuous variables Mean (standard deviation) Range
1. Environment: Measure of the Quality of the Environment
• “Facilitator” 126.8 (20.4) 93-185
Social support and attitudes 20.7 (4.8) 10-30
Income, labor and income security 12.4 (3.4) 5-19
Government and public services 26.7 (6.1) 17-42
Physical environment and accessibility 27.1 (8.5) 14-44
Technology 28.6 (5.0) 16-39
Equal opportunities and political orientations 11.4 (5.0) 3-23
• “Obstacle” 22.4 (10.0) 4-48
Social support and attitudes 0.9 (2.1) 0-10
Income, labor and income security 0.5 (1.5) 0-9
Government and public services 0.4 (1.1) 0-6
Physical environment and accessibility 15.8 (8.4) 0-35
Technology 3.2 (2.1) 0-9
Equal opportunities and political orientations 1.7 (2.4) 0-9
2. Quality of life
• Quality of Life Index (score /30) 20.4 (2.6) 14.3-25.4
Health and functioning (score /30) 17.8 (3.5) 10-24
Socioeconomic (score /30) 21.1 (2.9) 13.9-26.5
Psychological/spiritual (score /30) 22.0 (3.4) 13.6-28.4
Family (score /30) 23.3 (4.4) 3-30
Phys
Occ
up T
her
Ger
iatr
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f N
orth
Dak
ota
on 1
0/29
/14
For
pers
onal
use
onl
y.

QOL is a holistic concept which is complex and difficult to measure orestimate. The QLI seems to cover individual QOL well but, accordingto an analysis of this concept by Levasseur and colleagues (submitted),the tool may have considered only certain aspects of QOL and over-looked others despite the weighting of each item. For example, the QLIdid not consider the accomplishment of fulfilling occupations or the
46 PHYSICAL & OCCUPATIONAL THERAPY IN GERIATRICS
TABLE 3. Correlations between environment and quality of life scores (n = 46)
QLIMQE Health and
functioningSocio-
economicPsychological/
spiritualFamily Global
scoreSocial categories
Social support and attitudes
- Facilitator – 0.40*** 0.25* – 0.25*
- Obstacle – �0.36*** �0.22* �0.33** �0.28*
Income, labor and income security
- Facilitator – – – – –
- Obstacle – – – – –
Government and public services
- Facilitator – – – – –
- Obstacle – – – – –
Equal opportunities and political orientations
- Facilitator – – – – –
- Obstacle – – – 0.27* –Physical categories
Physical environment and accessibility
- Facilitator – 0.28* – – –
- Obstacle – – – – –
Technology
- Facilitator – – – – –
- Obstacle – – – – –Global scores
- Facilitator – 0.34** – – –
- Obstacle – – – – –
– Correlations with a p value higher than 0.15 are not displayed* .05 < p value � .15** .01 < p value � .05***p value � .01QLI: Quality of Life IndexMQE: Measure of the Quality of the Environment
Phys
Occ
up T
her
Ger
iatr
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f N
orth
Dak
ota
on 1
0/29
/14
For
pers
onal
use
onl
y.

feeling of control over one’s life. In this study, the relatively high QLIscores may indicate a real stability of the QOL data over time despite theonset of physical disabilities or the difficulty older people may have inexpressing dissatisfaction. Also, the fact that the participants receivedservices from the Day Hospital or CLSC during the study period mayhave contributed to a higher QOL.
The MQE was chosen for this study since it is based on the DisabilityCreation Process conceptual model and considers the perception of theperson regarding his/her environment. It appears more important to re-late the subjective (self-perceived) approach to a concept such as QOL.The results would probably have been different if an objective QOL in-strument had been used. In addition, the MQE considers the environ-ment in a global way, including the social as well as the physical dimen-sion. However, one of the instrument’s limitations is the ambiguity ofsome questions, for example: “What influence do government orienta-tions have on your daily life?” in the “Government and public services”category.
Contrary to our study, Vlek and colleagues (1998) demonstrated thatthe physical environment is an important element of QOL. We found,however, that most obstacles were reported in the “Physical environ-ment and accessibility” category. Many previous studies have sup-ported an association between QOL and physical environment (Albre-cht & Devlieger, 1999; Chapman & Beaudet, 1983; Kirchman, 1986;Lau et al., 1998; Lawton et al., 1978; 1984; Lawton & Cohen, 1974; Pearl-man & Uhlmann, 1988; Richards et al., 1999; Takemasa, 1998; Vlek,Skolnik & Gatersleben, 1998).
Levasseur, Desrosiers, and Noreau 47
TABLE 4. Comparison of relationships between environment and quality of lifefor two different levels of functional autonomy
Correlations Comparison ofcorrelations
Groups SMAF 19(n = 24)
SMAF > 19(n = 22)
QLI and MQE facilitator 0.32 (0.13)* 0.06 (0.81) 0.39I
QLI and MQE obstacle �0.05 (0.81) �0.26 (0.24) 0.50
*Spearman’s Rho (p value)Ip value associated with equality correlation test according to level of functional autonomySMAF: Functional Autonomy Measurement SystemQLI: Quality of Life IndexMQE: Measure of the Quality of the Environment
Phys
Occ
up T
her
Ger
iatr
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f N
orth
Dak
ota
on 1
0/29
/14
For
pers
onal
use
onl
y.

Contrary to our results, Lawton and colleagues (1978) suggested thatQOL is more related to the physical than the social dimensions of theenvironment. Association of the social environment with QOL is con-firmed by many other studies (Abbey & Andrews, 1985; Albrecht &Devlieger, 1999; Blixen & Kippes, 1999; Dijkers, 1997b; Lau et al., 1998;Pearlman & Uhlmann, 1988; Prince et al., 1997; Takemasa, 1998). Ac-cording to Lau and colleagues (1998) and Flanagan (1982), housing isone of the factors that contribute to QOL. Richards and colleagues(1999) found that access to the environment is related to satisfactionwith life, and Pearlman and Uhlmann (1988) showed that QOL of olderadults with chronic diseases was influenced by their physical environ-ment. However, the latter were not able to reproduce these results (Pearl-man & Uhlmann, 1991).
Some hypotheses may be suggested to explain these different results.First, previous studies often defined the environment objectively, orconsidered only some aspects of it, and rarely evaluated it with a spe-cific instrument. Also, the QOL instruments used were often very dif-ferent. Many researchers used in-house instruments, which sometimesincluded only one QOL item for which few or no validity studies werecarried out. Previous studies were conducted with different populationsand often a larger sample size. Finally, total scores can hide specific as-sociations since some relationships might cancel out others. Environ-ment and QOL are both very large constructs, which reduces the likeli-hood of observing relationships and increases the probability of a TypeII error.
Furthermore, some aspects of the environment are inherited and dif-ficult to modify, which may influence how the environment is per-ceived. The weather, for example, is a part of the environment that is notmodifiable. With few points of reference, it may be difficult for a personto be objective about his/her environment. Limited knowledge of one’spower to modify the environment may also give the impression thatnothing can be done and force the person to accept his/her environmentas is. This might affect the perception of the quality of the environment.Moreover, moving might be especially laborious for older adults withphysical disabilities. As mentioned by Kahanna (1982), because of re-duced income, health problems, loss of social roles and few housing al-ternatives, older adults are often faced with a limited choice in regard tokeeping or finding a residential environment that meets their needs andpreferences.
The “Social support and attitudes” category of the MQE is mainlyassociated with most domains of the QLI and, for the most part, with
48 PHYSICAL & OCCUPATIONAL THERAPY IN GERIATRICS
Phys
Occ
up T
her
Ger
iatr
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f N
orth
Dak
ota
on 1
0/29
/14
For
pers
onal
use
onl
y.

both facilitator and obstacle environments. Participants had higher QOLwhen they perceived their social network as having more facilitatorsand fewer obstacles. Since globally our participants had good QOLscores, it is possible that help provided by the social network dimin-ished the potential negative influence of physical disabilities on QOL.This is in agreement with Blixen and Kippes (1999), who found that thesocial network had a significant impact on QOL of older adults withosteoarthritis by decreasing the stress caused by, among other things,physical disabilities.
The correlation found between the “Equal opportunities and politi-cal orientations” category of the MQE and “Family” domain of the QLIis difficult to understand. It is hard to believe that good QOL related tothe family may be associated with an environment perceived as an ob-stacle. This relationship may be the result of chance or for some peopleit may reflect the small impact that “Equal opportunities and politicalorientations” have on QOL. It is possible that, for some people, politicalorientations diminish the quality of their environment but are not suffi-cient to affect QOL.
The lack of statistically significant differences in the correlations be-tween environment and QOL according to the two levels of physicaldisabilities may be attributable to the statistical power of the analysis,which was reduced to 46% by dividing the sample. Despite the absenceof statistically significant results, the associations show some interest-ing tendencies. For example, participants with minor physical disabili-ties had higher QOL when more items in their environment wereperceived as facilitators while those with moderate to severe physicaldisabilities had higher QOL when fewer items in their environmentwere perceived as obstacles. Since the two groups had very similar QLIand MQE scores, these tendencies do not seem to be caused by the factthat people with minor physical disabilities perceived more facilitatorsand fewer obstacles in their environment and that people with moderateto severe physical disabilities perceived fewer facilitators and more ob-stacles in their environment. Why do only environmental facilitators ap-pear to contribute to QOL of people with minor physical disabilitieswhereas only environmental obstacles seem to contribute to QOL ofpeople with moderate to severe physical disabilities? The impact of en-vironmental facilitators might be enough to overcome physical disabili-ties when they are minor but not when they are moderate to severe. Onthe other hand, the impact of environmental obstacles might not be suf-ficient to affect QOL of people with only minor physical disabilities butmight affect QOL of people with moderate to severe disabilities.
Levasseur, Desrosiers, and Noreau 49
Phys
Occ
up T
her
Ger
iatr
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f N
orth
Dak
ota
on 1
0/29
/14
For
pers
onal
use
onl
y.

This study had some limitations. First, it was carried out with a con-venience sample of people receiving day hospital services or home careservices from a CLSC and might not be representative of community-dwelling older adults with physical disabilities. For example, the partic-ipants perceived themselves in worse health than those who refused.The sample size is another weakness of the study, making only explor-atory comparisons between older adults with moderate to severe physi-cal disabilities and those with minor disabilities (objective 2). Also,since many statistical analyses were done between categories of instru-ments, there is a risk of a Type I error and the correlations might be theresult of chance. A larger study and the addition of people without phys-ical disabilities are thus needed to confirm these results. The cross-sec-tional design of the present study is also a limitation since the parti-cipants were interviewed only once, making it impossible to look atvariations over time. Finally, because an interviewer collected the par-ticipants’ answers, there was the risk of a social desirability bias, eventhough the participants were assured of confidentiality and told therewere no right or wrong answers.
Despite these limitations, the findings of this study provide interest-ing leads for physical and occupational therapy interventions. First, thedefinition of QOL emphasizes the importance of considering the sub-jective evaluation of an individual’s life circumstances according to his/her values. Therapists must be careful and not take for granted that envi-ronmental interventions will improve the QOL of all clients.
According to this study, some environmental aspects, especially thesocial dimension, may significantly contribute to enhancing QOL ofcommunity-dwelling older adults with physical disabilities. By recom-mending environmental modifications based on an individual evalua-tion of the client, for example assistance with bathing, the therapist mightenhance his/her client’s quality of life. Also, in order to increase QOLfor people with minor physical disabilities, therapists might want to putmore emphasis on environmental aspects perceived as facilitators, where-as to increase QOL for people with moderate to severe physical disabili-ties, it might be better to address environmental aspects perceived as ob-stacles.
CONCLUSION
This study only partially supports the importance of the environmentin regard to the QOL of community-dwelling older adults with physical
50 PHYSICAL & OCCUPATIONAL THERAPY IN GERIATRICS
Phys
Occ
up T
her
Ger
iatr
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f N
orth
Dak
ota
on 1
0/29
/14
For
pers
onal
use
onl
y.

disabilities. These findings provide interesting leads that some environ-mental aspects, especially the social dimension, may significantly con-tribute to enhancing QOL of community-dwelling older adults with phy-sical disabilities. Consequently, help provided by the social networkmay diminish the potential negative impact of physical disabilities onQOL. Other studies are needed to clarify how environment influencesquality of life in this population.
REFERENCES
Abbey, A. & Andrews, F.M. (1985). Modeling the psychological determinants of lifequality. Social Indicators Research, 16, 1-34.
Albrecht, G.L. & Devlieger, P.J. (1999). The disability paradox: High quality of lifeagainst all odds. Social Science & Medicine, 48(8), 977-988.
Blixen, C.E. & Kippes, C. (1999). Depression, social support, and quality of life inolder adults with osteoarthritis. Image: Journal of Nursing Scholarship, 31(1),221-226.
Boschen, K., Noreau, L. & Fougeyrollas, P. (1998). Reliability studies of the Measureof the Quality of the Environment (MQE). 1er congrès du Réseau Provincial de re-cherche en adaptation-réadaptation. Québec. June 4-6, 1998. Canadian Journal ofRehabilitation, 11(4): 184-185.
Bravo, G. & Hébert, R. (1997). Age- and education-specific references values for theMini-Mental and Modified Mini-Mental State Examinations derived from a non-demented elderly population. International Journal of Geriatric Psychiatry, 12,1008-1018.
Calman, K.C. (1984). Quality of life in cancer patients–an hypothesis. Journal of Med-ical Ethics, 10, 124-127.
Chapman, N.J. & Beaudet, M. (1983). Environmental predictors of well-being forat-risk older adults in a mid-sized city. Journal of Gerontology, 38(2), 237-244.
Day, H. & Jankey, S.G. (1996). Lessons from the literature: Toward a holistic model ofquality of life. In Renwick, R., Brown, I. & Nagler, M. (Eds.), Quality of life inhealth promotion and rehabilitation (pp. 39-62). Thousand Oaks, CA: Sage.
Dijkers, M. (1997a). Measuring Quality of Life. In Fuhrer, M.J. (Ed.), Assessing Medi-cal Rehabilitation Practices: The Promise of Outcomes Research (pp. 153-179).Baltimore, MD: Paul H. Brookes Publishing Co.
Dijkers, M. (1997b). Quality of life after spinal cord injury: A meta analysis of the ef-fects of disablement components. Spinal Cord, 35, 829-840.
Ferrans, C.E. & Powers, M.J. (1985). Quality of life index: Development and psycho-metric properties. Advances in Nursing Sciences, 8(1), 15-24.
Flanagan, J.C. (1982). Measurement of quality of life: Current state of the art. Archivesof Physical Medicine and Rehabilitation, 63, 56-9.
Fougeyrollas, P. (1994). Les applications du concept de handicaps (désavantages) de laCIDIH (CIH) et de sa nomenclature. Réseau international CIDIH et facteursenvironnementaux, 25-51.
Levasseur, Desrosiers, and Noreau 51
Phys
Occ
up T
her
Ger
iatr
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f N
orth
Dak
ota
on 1
0/29
/14
For
pers
onal
use
onl
y.

Fougeyrollas, P., Noreau, L., Bergeron, H., Cloutier, R., Dion, S-A & St-Michel, G.(1998). Social consequences of long term impairment and disabilities: Conceptualapproach and assessment of handicap. International Journal of Rehabilitation Re-search, 21, 127-141.
Fougeyrollas, P., Noreau, L., St-Michel, G. & Boschen, K. (1999). Measure of thequality of the environment, Version 2.0. International Network of the DisabilityCreation Process. Lac St-Charles, Québec.
Hébert, R., Carrier, R. & Bilodeau, A. (1988). The functional autonomy measurementsystem (SMAF): Description and validation of an instrument for the measurementof handicaps. Age Ageing, 17, 293-302.
Kahanna, E. (1982). A congruence Model of Person-Environment Interaction. InLawton, M.P., Windley, P.G. & Byerts, T.O. (Eds.). Aging and the environment:Theoretical Approaches. New York: Springer Publishing Company.
Kirchman, M. (1986). Measuring the quality of life. Occupational Therapy Journal ofResearch, 6(1), 21-32.
Lau, A., Chi, I. & McKenna, K. (1998). Self-perceived quality of life of Chinese el-derly people in Hong Kong. Occupational Therapy International, 5(2), 118-139.
Law, M. (1991). The environment: A focus for occupational therapy. Canadian Jour-nal of Occupational Therapy, 58, 171-179.
Lawton, M.P., Brody, E.M. & Turner-Massey, P. (1978). The relationship of environ-mental factors to changes in well-being. Gerontologist, 18, 133-137.
Lawton, M.P. & Cohen, J. (1974). The generality of housing impact on the well-beingof older people. Journal of Gerontology, 29(2), 194-204.
Lawton, M.P., Kleban, M.H. & diCarlo, E. (1984). Psychological well-being in theaged. Factorial and conceptual dimensions. Research on Aging, 6(1), 67-97.
Levasseur, M., St-Cyr Tribble, D. & Desrosiers, J. (submitted). Préoccupations enversla qualité de vie des personnes âgées en perte d’autonomie fonctionnelle. CanadianJournal of Occupational Therapy.
Machin, D., Campbell, M.J., Fayers, P.M. & Pinol, A.P.Y. (1997). Sample Size Tablesfor Clinical Studies. Berlin, Germany: Blakewell Sciences Ltd.
McHorney, C.A., Ware, J.E., Lu, J.F.R. & Sherbourne, C.D. (1994). The MOS 36-itemShort-Form Health Survey (SF-36): III Test of data quality, scaling assumptions,and reliability across diverse patients groups. Medical Care, 32, 40-66.
Pearlman, R.A. & Uhlmann, R.F. (1988). Quality of Life in Chronic Diseases: Percep-tions of Elderly Patients. Journal of Gerontology, 43(2), M25-30.
Pearlman, R.A. & Uhlmann, R.F. (1991). Quality of Life in Elderly, Chronically IllOutpatients. Journal of Gerontology, 46(2), M31-8.
Prince, M.J., Harwood, R.H., Blizard, R.A., Thomas, A. & Mann, A.H. (1997). Socialsupport deficits, loneliness and life events as risk factors for depression in old age.The Gospel Oak Project VI. Psychological Medicine, 27(2), 323-332.
Richards, J.S., Bombardier, C.H., Tate, D., Dijkers, M., Gordon, W., Shewchuk, R. &DeVivo, M.J. (1999). Access to the Environment and Life Satisfaction after SpinalCord Injury. Archives of Physical Medicine and Rehabilitation, 80, 1501-1506.
Takemasa, S. (1998). Factors affecting QOL of the home-bound elderly disabled. KobeJournal of Medical Sciences, 44(3), 99-114.
52 PHYSICAL & OCCUPATIONAL THERAPY IN GERIATRICS
Phys
Occ
up T
her
Ger
iatr
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f N
orth
Dak
ota
on 1
0/29
/14
For
pers
onal
use
onl
y.

Vlek, C., Skolnik, M. & Gatersleben, B. (1998). Sustainable development and qualityof life: Prospective changes in economic and environmental conditions. Zeitschriftfur Experimentelle Psychologie, 45(4), 319-333.
World Health Organization (1980; 1993; 1997). International Classification of Func-tioning, Disability and Health (ICIDH). WHO: Geneva.
World Health Organization (2001). International Classification of Functioning, Dis-ability and Health-2 (ICIDH-2). WHO: Geneva.
Levasseur, Desrosiers, and Noreau 53
Phys
Occ
up T
her
Ger
iatr
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f N
orth
Dak
ota
on 1
0/29
/14
For
pers
onal
use
onl
y.