Embed Size (px)
Citation preview

ORIG I NALRESEARCH
PAPER
Relationships between objectivephysical characteristics and the use ofweight control methods inadolescence: A mediating role foreating attitudes?
E. Peñas Lledó*, L. Sancho*, and G. Waller*** Department of Pharmacology and Psychiatry and Department of Physiology, Medical School, University ofExtremadura, Badajoz, Extremadura, Spain, and ** Department of General Psychiatry, St. George’s HospitalMedical School, University of London, London, UK
ABSTRACT. This study of non-clinical adolescent males and females examined associationsof objectively measured physical characteristics with greater use of methods of weight con-trol and considered whether the relationships between these variables might be explained bya mediating effect of a subjective characteristic - unhealthy eating attitudes. Non-clinical maleand female adolescents completed measures of weight control and eating attitudes, and theirphysical characteristics were measured using a range of standardized anthropometry tech-niques. Regression analyses were used to test the role of eating attitudes as mediators in therelationship between physical characteristics and the use of weight control methods. Thedata were compatible with a partial mediator model, where physical characteristics influenceeating attitudes, and those where attitudes drive the use of methods to control weight.However, not all of the relationship was explained by this mediator. In addition, there weredifferent patterns of association for men and women, consistent with different patterns ofbodily focus between the genders. These findings stress the importance of understandingobjective physical characteristics as well as subjective eating attitudes to find out why peopleuse different levels of weight control behaviours. Limitations, further research and potentialimplications for clinical and preventative programmes are discussed.(Eating Weight Disord. 6: 148-156, 2001). ©2001, Editrice Kurtis
INTRODUCTION
Dieting is an important risk factor for thedevelopment of an eating disorder (1-3),especially since it usually precedes bothanorexia and bulimia nervosa (4-6). Thisbehaviour is generally seen as primarily aconsequence of dissatisfaction with one’sperceived body weight and shape, particu-larly in a social context such as social com-parison or teasing (7-9). Many studies haveshown that non-clinical women dissatisfiedwith their bodies use a range of methods toreduce their weight (10-12). However, it isimportant to remember that perceived bodycharacteristics will have some form ofgrounding in objective body characteristics,though the association of the subjective andthe objective is often less than perfect.
In studies where objective physical mea-sures have been used, it is clear that actualbody size and shape have an influence oneating attitudes. However, this literature hasthree drawbacks. First, it has focused almostexclusively on the role played by a limited setof objective indicators of body size, such asbody mass index (BMI) and waist/hip size (7,8, 13-15), whereas the literature on anthro-pomorphic measurement (16) suggests that awider range of physical characteristicsshould be used to understand body composi-tion (17). Second, the conclusions are drawnfrom large samples of non-clinical females.The little research on males (14, 18-21) hasmainly focused on the role of BMI as a pre-dictor of unhealthy eating attitudes.
However, it cannot simply be assumedthat the same physical characteristics will
Key words:Anthropometry, eatingattitudes, weight control,adolescence, males, females.Correspondence to:Eva Peñas Lledó,Department ofPharmacology andPsychiatry, Medical School,University of Extremadura,Avenue of Elvas s/n,06071 Badajoz,Extremadura, Spain.Received: June 12, 2000Accepted: January 31, 2001
148

have the same impact across genders. Thethird major deficiency is that there havebeen few attempts to build a model encom-passing the links between body size/shape,eating attitudes and the actual use ofweight control methods. In one such study(22), the authors have demonstrated thatfalse feedback about actual weight (tellingwomen that they weighed more than theyactually did) has a disinhibiting effect onsubsequent eating, but only amongrestrained eaters. Such studies suggest thatit will be important to develop models thataccount for the complex relationshipsbetween actual body shape/size, eating atti-tudes and eating behaviours, rather thansimply considering the bivariate linksbetween these phenomena.
A model of this kind would need to con-sider whether subjective eating attitudesand objective body size have additiveeffects upon the use of methods to controlweight, or whether a more complex causalmodel is necessary. It is proposed here thatthe impact of actual body size and shapeupon the use of weight control methodswill be mediated by subjective eating atti-tudes. Therefore, the aim of the presentstudy was to determine whether objectivephysical characteristics are associated withthe use of methods to control weight, andwhether this relationship is mediated bythe development of restrictive and bulimicattitudes, and body dissatisfaction.
METHOD
ParticipantsThe participants were a non-clinical
group of 157 female and 174 male adoles-cent students in their pre-university year.
Their mean age was 18.2 (SD=1.39) forthe women and 18.4 (SD=1.38) for the men.They were screened to exclude reportedcases of present or past treatment for anypsychological disturbance and none hadany known history of psychological prob-lems.
This sample was derived from an initialsample of ten government and three pri-vate high schools selected within a singleregion of Spain (Extremadura - 1,100,000inhabitants) which had a population of11,951 students in this age group duringthe academic year 1997-1998. Thirty stu-dents were randomly selected from the
final year of each school. Of the 390 stu-dents selected in this way, 331 took partfully. The remainder were absent duringthe assessment, declined to participate ordid not complete the questionnaires prop-erly.
Participants were tested in classes sepa-rately during one school lesson (50 min-utes). All of the final group gave their con-sent to participate, and parental consentwas obtained for those under 18 at the timeof testing.
Measures and procedureThe participants completed two question-
naires, and had a number of anthropomor-phic measures taken in the order givenbelow. They then completed demographicmeasures and were asked about any previ-ous history of eating disorders or otherpsychological problems (see above).
Eating Disorders Inventory (EDI). The EDI(23) is a well-validated measure of eatingand related psychopathology, whichincludes three scales that measure eatingattitudes (Drive for thinness; Bulimia; Bodydissatisfaction). The Spanish translationused has been demonstrated to have ade-quate psychometric properties (24).
The first edition of the EDI (eight scales)was used because the Spanish translation(25) of the more recent and expanded sec-ond edition (26) was not available.
Weight control practices. Each partici-pant completed a checklist of seven meth-ods used to control weight in the past yearand/or at present: diet prescribed by spe-cialist; diet from a magazine; skippingmeals; cutting out foods; reducing thequantity of energy intake meals; excessivephysical activity with the aim of burningcalories (at least 4 times a week for anhour); and others (laxatives, diuretics, dietpills or vomiting). The use of each methodscored one, giving a potential score rangeof 0-7.
Anthropomorphic measures. The follow-ing objective anthropometric data werecollected: BMI [weight(kg)/height(m2)] hipand waist circumference (cm); mean armcircumference (cm); triceps skinfold thick-ness (g/mm2 - reflecting fat content of thebody); and arm muscle area (cm2). Eachperson was measured (in private if desired,and never in the presence of a member ofthe other gender) in light clothing andwithout shoes. Replicability (16) was
Weight control in adolescence
149

E. Peñas Lledó, L. Sancho and G. Waller
assured by measuring under the followingconditions. Height was measured to thenearest 0.5 cm a Harpenden™ stadiometer,and weight to the nearest 0.2 kg on a stan-dard, calibrated platform scale. Waist andhip circumference (narrowest and widestpoints respectively) were measured to thenearest mm using a metal tape, with girlsstanding, arms at their side and feet togeth-er. Waist to hip ratio was calculated fromthe formula waist circumference/hip cir-cumference. The mean arm circumferencein cm was measured at the midpoint of theright upper arm. Triceps skinfold thicknesswas also measured here on a standardHoltain™ calliper, using the acromion andolecranon as landmarks with the arm bentat 90° (27). The measurement was madewith the arm fully extended at the subject’sside, with the skinfold parallel to the longi-tudinal axis of the upper arm. Arm musclearea was calculated from arm circumfer-ence and triceps skinfold thickness (27).The averages of three hip and waist cir-cumference and subcutaneous triceps skin-fold thickness measurements were used inthe data analysis.
Data analysisInitially, males’ and females’ scores on the
measures were compared using t tests (two-tailed). Second, correlations (two-tailedPearson’s r) were carried out (for males andfemales separately) to determine the associ-ation of the use of weight control measureswith subjective eating attitudes and objec-tive measures of physical characteristics.An alpha level of p<0.01 was adopted forthese t tests and correlations to reduce therisk of Type 1 errors. Lastly, Baron et al’smethod of staged multiple regression analy-sis (28) was used separately for men andwomen to find out whether the associationswere mediated by the hypothesis of a medi-ating role for subjective eating attitudes inthe relationship between objective physicalcharacteristics and the use of several meth-ods of weight control. To determinewhether the relationship between physicalcharacteristics and methods to controlweight is mediated by EDI eating attitudes,a significant relationship must first beestablished between the anthropometricscores measures and the number of weightcontrol methods. In the final step, whensubjective eating attitudes are included inthe regression equation, the remaining rela-
tionship between objective physical charac-teristics and use of practices to reduceweight should either be no longer signifi-cant or be weakened substantially (28). Ifthe relationship is no longer significant, eat-ing attitudes are said to be a perfect media-tor. If it is merely weakened, eating atti-tudes are said to be a partial mediator (28).
RESULTS
Group characteristicsTable 1 shows the mean male and female
scores for the number of weight controlmethods, eating attitudes (EDI eatingscales) and physical characteristics (anthro-pometric measures), together with the t testresults. There were the expected differ-ences in levels of restrictive behaviour (EDIDrive for thinness), body dissatisfaction,BMI and other physical characteristics,with women having less healthy eating atti-tudes and men having generally largerbodies. In addition, the women used signif-icantly more weight control methods.
Bivariate associations of methods used forweight control with eating attitudes andphysical characteristicsCorrelations (Pearson’s r) were used todetermine which eating attitudes and phys-ical characteristics were associated withthe greater use of weight control methods.
These analyses were conducted separate-ly for men and women. The findings (Table2) showed that the number of weight con-trol methods was greater among individu-als with less healthy eating attitudes andthose who were heavier/less slim. Therewere only minor differences in this patternbetween men and women.
Testing the mediatorThe following analyses (conducted sepa-
rately for men and women) use Baron etal’s method (28) to determine whether thedata are compatible with a model whereunhealthy eating attitudes mediate the rela-tionship between physical characteristicsand the number of weight control methods.
Given the results of the correlations(above), only certain physical characteris-tics were used in the mediator analysis.
Weight was not used for either group,due to its high collinearity with BMI.
Male participants. For men, BMI, triceps
150
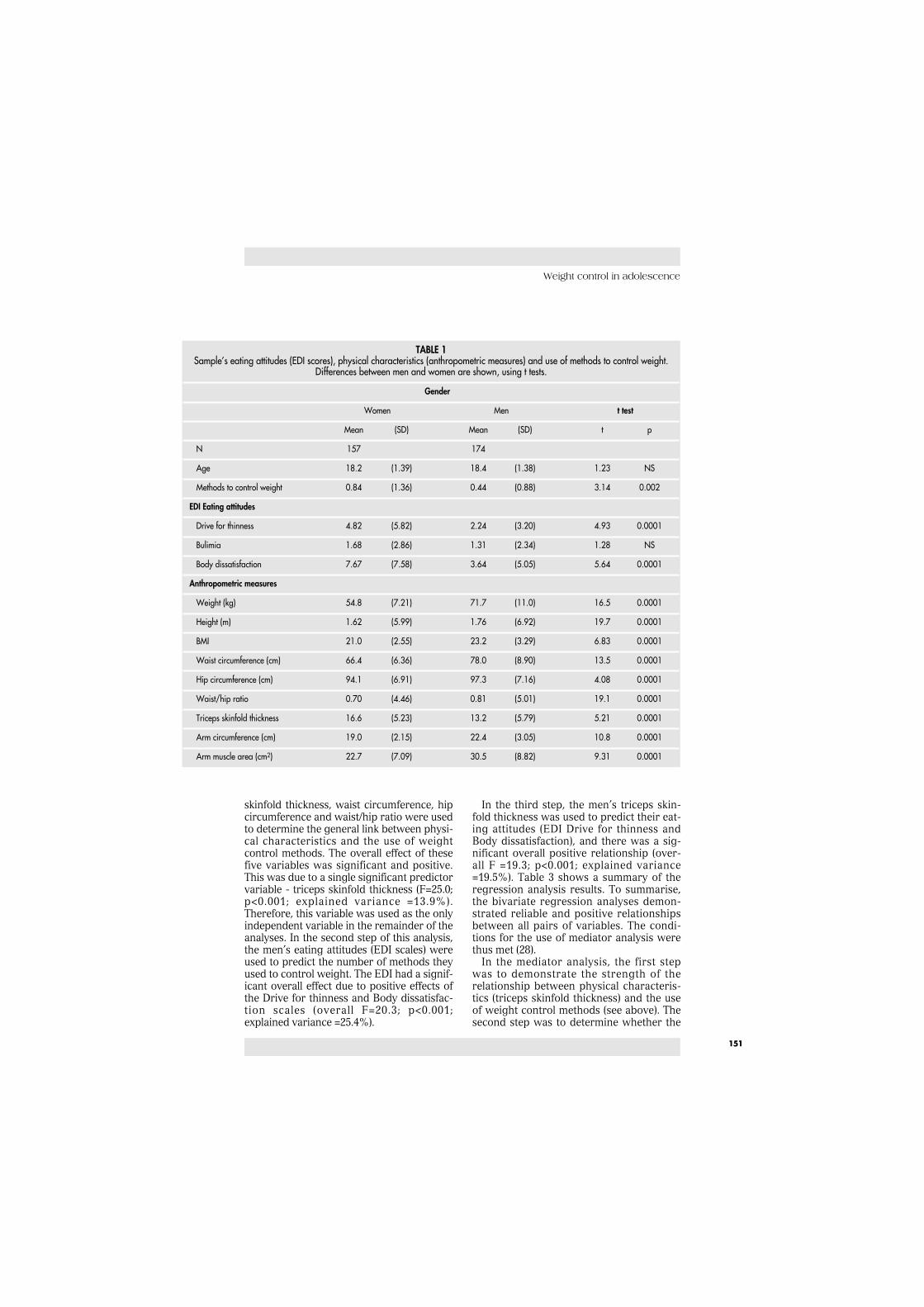
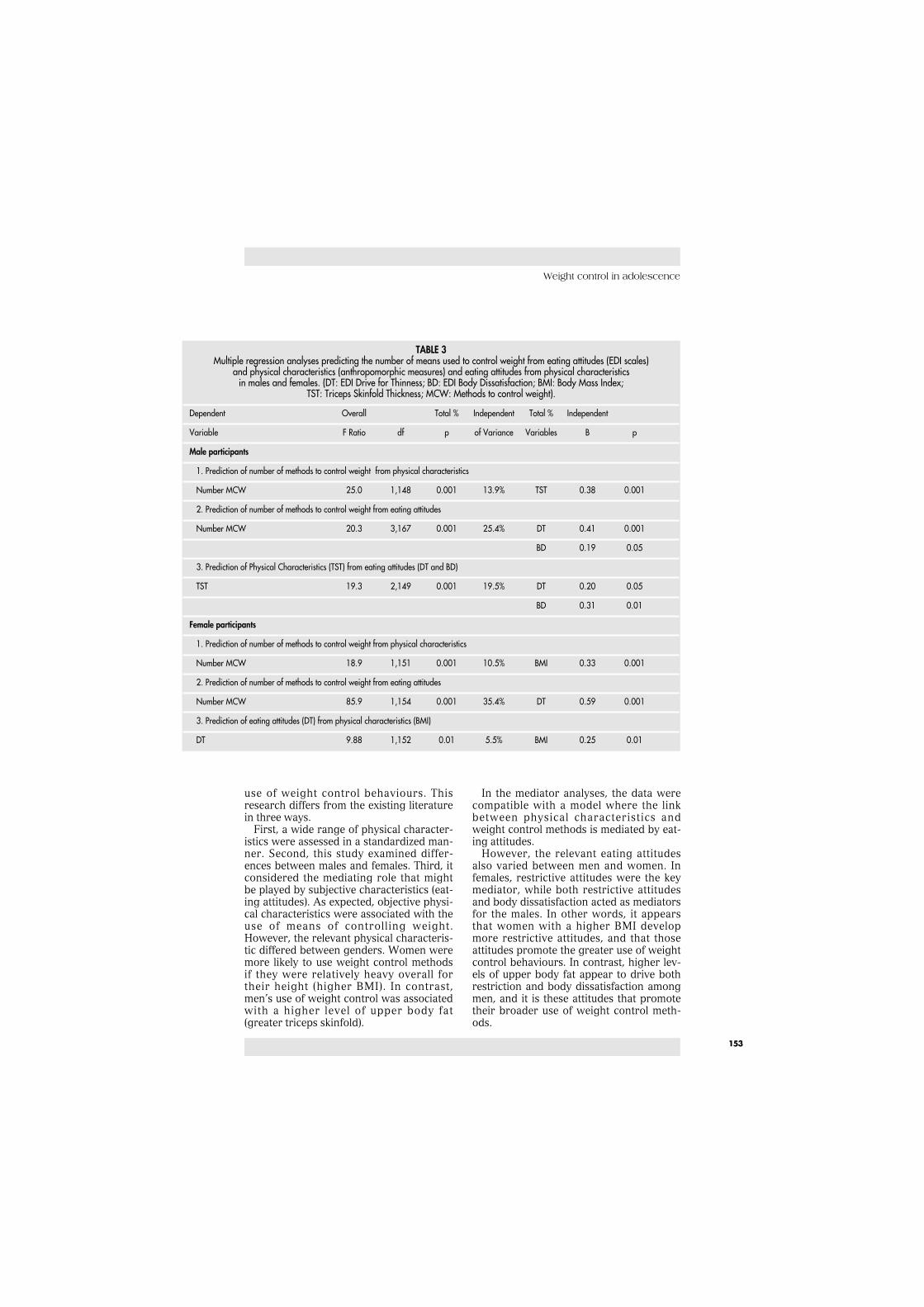
skinfold thickness, waist circumference, hipcircumference and waist/hip ratio were usedto determine the general link between physi-cal characteristics and the use of weightcontrol methods. The overall effect of thesefive variables was significant and positive.This was due to a single significant predictorvariable - triceps skinfold thickness (F=25.0;p<0.001; explained variance =13.9%).Therefore, this variable was used as the onlyindependent variable in the remainder of theanalyses. In the second step of this analysis,the men’s eating attitudes (EDI scales) wereused to predict the number of methods theyused to control weight. The EDI had a signif-icant overall effect due to positive effects ofthe Drive for thinness and Body dissatisfac-tion scales (overall F=20.3; p<0.001;explained variance =25.4%).
In the third step, the men’s triceps skin-fold thickness was used to predict their eat-ing attitudes (EDI Drive for thinness andBody dissatisfaction), and there was a sig-nificant overall positive relationship (over-all F =19.3; p<0.001; explained variance=19.5%). Table 3 shows a summary of theregression analysis results. To summarise,the bivariate regression analyses demon-strated reliable and positive relationshipsbetween all pairs of variables. The condi-tions for the use of mediator analysis werethus met (28).
In the mediator analysis, the first stepwas to demonstrate the strength of therelationship between physical characteris-tics (triceps skinfold thickness) and the useof weight control methods (see above). Thesecond step was to determine whether the
Weight control in adolescence
151
TABLE 1Sample’s eating attitudes (EDI scores), physical characteristics (anthropometric measures) and use of methods to control weight.
Differences between men and women are shown, using t tests.
Gender
Women Men t test
Mean (SD) Mean (SD) t p
N 157 174
Age 18.2 (1.39) 18.4 (1.38) 1.23 NS
Methods to control weight 0.84 (1.36) 0.44 (0.88) 3.14 0.002
EDI Eating attitudes
Drive for thinness 4.82 (5.82) 2.24 (3.20) 4.93 0.0001
Bulimia 1.68 (2.86) 1.31 (2.34) 1.28 NS
Body dissatisfaction 7.67 (7.58) 3.64 (5.05) 5.64 0.0001
Anthropometric measures
Weight (kg) 54.8 (7.21) 71.7 (11.0) 16.5 0.0001
Height (m) 1.62 (5.99) 1.76 (6.92) 19.7 0.0001
BMI 21.0 (2.55) 23.2 (3.29) 6.83 0.0001
Waist circumference (cm) 66.4 (6.36) 78.0 (8.90) 13.5 0.0001
Hip circumference (cm) 94.1 (6.91) 97.3 (7.16) 4.08 0.0001
Waist/hip ratio 0.70 (4.46) 0.81 (5.01) 19.1 0.0001
Triceps skinfold thickness 16.6 (5.23) 13.2 (5.79) 5.21 0.0001
Arm circumference (cm) 19.0 (2.15) 22.4 (3.05) 10.8 0.0001
Arm muscle area (cm2) 22.7 (7.09) 30.5 (8.82) 9.31 0.0001

E. Peñas Lledó, L. Sancho and G. Waller
strength of that relationship was reducedby taking into account the effect of eatingattitudes (mediator) prior to assessing theimpact of the physical characteristics (inde-pendent variable) upon weight control(dependent variable). In this case, the sig-nificant effect of eating attitudes on the useof weight control (see above) substantiallyreduced the relationship between the inde-pendent and dependent variables, althoughthat difference remained significant (overallF =5.52; p<0.02).
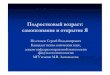
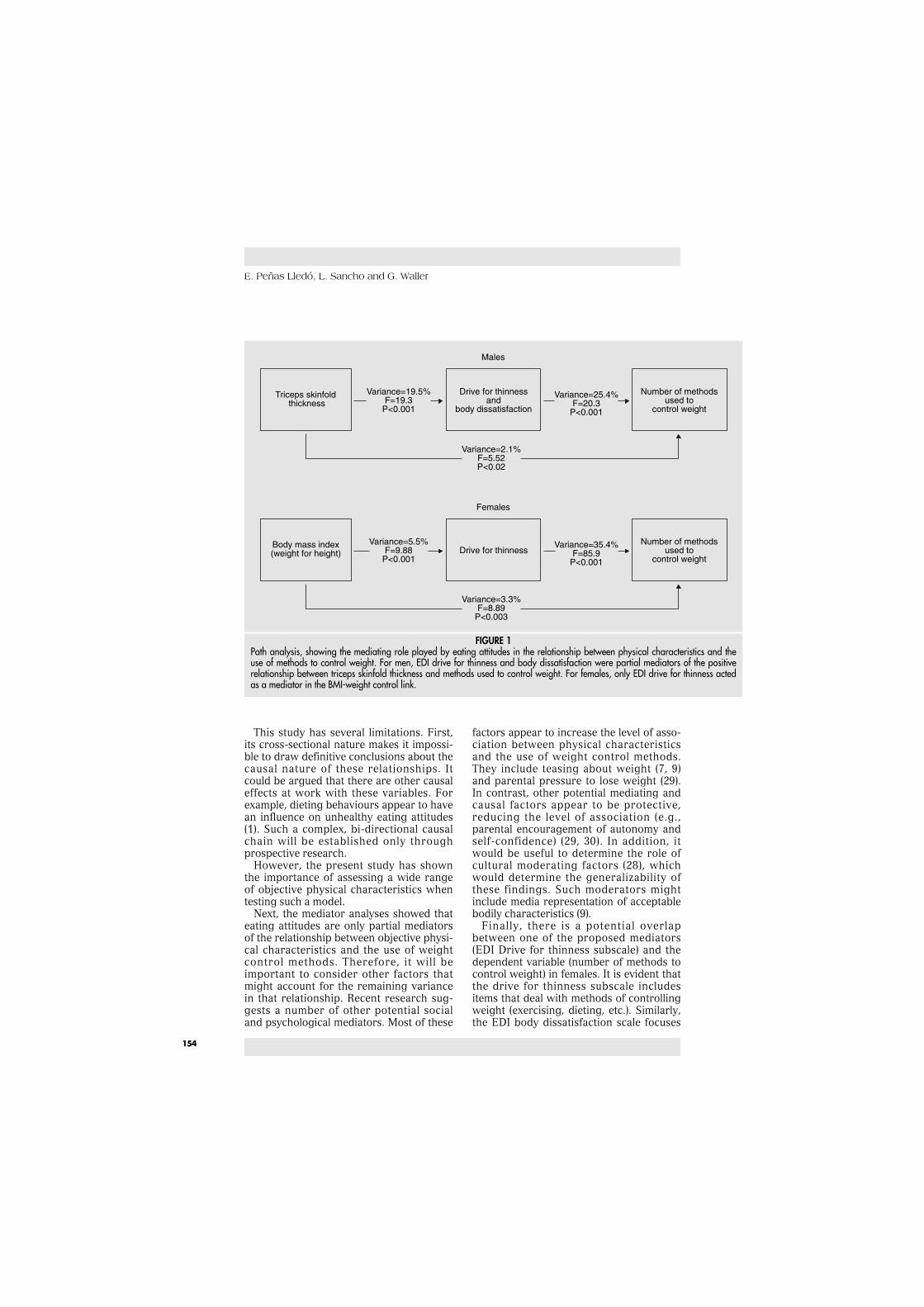
The explained variance fell from 13.9 to2.1%. The standardized regression coeffi-cient also fell substantially (from Beta =0.38to Beta =0.18). Therefore, these findings arecompatible with a model where men’s eatingattitudes (Drive for thinness; Body dissatis-faction) act as partial mediators of the posi-tive relationship between their upper bodyfat levels (triceps skinfold thickness) andtheir use of more methods to control weight.This relationship is illustrated in Figure 1.
Female participants. For women, BMI, tri-ceps skinfold thickness and waist and hipcircumferences were used to determine thegeneral link between physical characteris-tics and the use of weight control methods.The overall effect of these four variableswas significant and positive. This effect wasdue to a single predictor variable - BMI(F=18.9; p<0.001; explained variance=10.5%). Thus, BMI was used as the onlyindependent variable in the rest of theanalyses. In the second step, the women’seating attitudes were used to predict thenumber of methods they used to controlweight. The EDI scales had a significantoverall effect, due to Drive for thinness(F=85.9; p<0.001; explained variance=35.4%). In the third step, women’s BMIwas used to predict their EDI Drive for thin-ness scores.
Again there was a significant and posi-tive relationship (F=9.88; p< 0.01; explainedvariance =5.5%). Table 3 shows a summaryof the regression analysis results demon-strating significant and reliable relation-ships between the individual variables andallowing the use of mediator analysis (28).
Having established the significant rela-tionship between BMI and the use ofweight control behaviours (see above), thesecond stage is to determine whether Drivefor thinness (mediator) reduces the impactof BMI (independent variable) upon weightcontrol (dependent variable). The signifi-
cant effect of Drive for thinness on thepractice of weight control behavioursreduced the association between BMI andweight control behaviours, although itremained significant (F =8.89; p<0.01). Theexplained variance fell from 10.5% to 3.3%,and the standardised regression coefficient(Beta) fell from 0.33 to 0.19. To summarise,these findings are compatible with a modelwhere women’s restrictive eating attitudes(Drive for thinness) act as a partial media-tor of the positive relationship betweentheir BMI and their use of more weightcontrol methods. This relationship is illus-trated in Figure 1.
DISCUSSION
This study of non-clinical adolescentsaimed to determine the role of objectivephysical characteristics in determining the
152
TABLE 2Associations (Pearson’s r correlations) of physical characteristics
(anthropometric measures) and eating attitudes(EDI scales) with the number of methods used to control weight.
Methods to control weight
Women Men
EDI
Drive for thinness 0.60* 0.49*
Bulimia 0.29* 0.07
Body dissatisfaction 0.46* 0.41*
Anthropometric measures
Weight 0.35* 0.29*
Height 0.09 -0.08
BMI 0.33* 0.35*
Waist circumference 0.27* 0.28*
Hip circumference 0.25* 0.24*
Waist/hip ratio 0.15 0.23*
Triceps skinfold thickness 0.25* 0.38*
Arm mean circumference 0.07 0.04
Arm muscle area 0.05 0.02
* p<0.000
use of weight control behaviours. Thisresearch differs from the existing literaturein three ways.
First, a wide range of physical character-istics were assessed in a standardized man-ner. Second, this study examined differ-ences between males and females. Third, itconsidered the mediating role that mightbe played by subjective characteristics (eat-ing attitudes). As expected, objective physi-cal characteristics were associated with theuse of means of controlling weight.However, the relevant physical characteris-tic differed between genders. Women weremore likely to use weight control methodsif they were relatively heavy overall fortheir height (higher BMI). In contrast,men’s use of weight control was associatedwith a higher level of upper body fat(greater triceps skinfold).
In the mediator analyses, the data werecompatible with a model where the linkbetween physical characteristics andweight control methods is mediated by eat-ing attitudes.
However, the relevant eating attitudesalso varied between men and women. Infemales, restrictive attitudes were the keymediator, while both restrictive attitudesand body dissatisfaction acted as mediatorsfor the males. In other words, it appearsthat women with a higher BMI developmore restrictive attitudes, and that thoseattitudes promote the greater use of weightcontrol behaviours. In contrast, higher lev-els of upper body fat appear to drive bothrestriction and body dissatisfaction amongmen, and it is these attitudes that promotetheir broader use of weight control meth-ods.
Weight control in adolescence
153
TABLE 3Multiple regression analyses predicting the number of means used to control weight from eating attitudes (EDI scales)
and physical characteristics (anthropomorphic measures) and eating attitudes from physical characteristicsin males and females. (DT: EDI Drive for Thinness; BD: EDI Body Dissatisfaction; BMI: Body Mass Index;
TST: Triceps Skinfold Thickness; MCW: Methods to control weight).
Dependent Overall Total % Independent Total % Independent
Variable F Ratio df p of Variance Variables B p
Male participants
1. Prediction of number of methods to control weight from physical characteristics
Number MCW 25.0 1,148 0.001 13.9% TST 0.38 0.001
2. Prediction of number of methods to control weight from eating attitudes
Number MCW 20.3 3,167 0.001 25.4% DT 0.41 0.001
BD 0.19 0.05
3. Prediction of Physical Characteristics (TST) from eating attitudes (DT and BD)
TST 19.3 2,149 0.001 19.5% DT 0.20 0.05
BD 0.31 0.01
Female participants
1. Prediction of number of methods to control weight from physical characteristics
Number MCW 18.9 1,151 0.001 10.5% BMI 0.33 0.001
2. Prediction of number of methods to control weight from eating attitudes
Number MCW 85.9 1,154 0.001 35.4% DT 0.59 0.001
3. Prediction of eating attitudes (DT) from physical characteristics (BMI)
DT 9.88 1,152 0.01 5.5% BMI 0.25 0.01
E. Peñas Lledó, L. Sancho and G. Waller
This study has several limitations. First,its cross-sectional nature makes it impossi-ble to draw definitive conclusions about thecausal nature of these relationships. Itcould be argued that there are other causaleffects at work with these variables. Forexample, dieting behaviours appear to havean influence on unhealthy eating attitudes(1). Such a complex, bi-directional causalchain will be established only throughprospective research.
However, the present study has shownthe importance of assessing a wide rangeof objective physical characteristics whentesting such a model.
Next, the mediator analyses showed thateating attitudes are only partial mediatorsof the relationship between objective physi-cal characteristics and the use of weightcontrol methods. Therefore, it will beimportant to consider other factors thatmight account for the remaining variancein that relationship. Recent research sug-gests a number of other potential socialand psychological mediators. Most of these
factors appear to increase the level of asso-ciation between physical characteristicsand the use of weight control methods.They include teasing about weight (7, 9)and parental pressure to lose weight (29).In contrast, other potential mediating andcausal factors appear to be protective,reducing the level of association (e.g.,parental encouragement of autonomy andself-confidence) (29, 30). In addition, itwould be useful to determine the role ofcultural moderating factors (28), whichwould determine the generalizability ofthese findings. Such moderators mightinclude media representation of acceptablebodily characteristics (9).
Finally, there is a potential overlapbetween one of the proposed mediators(EDI Drive for thinness subscale) and thedependent variable (number of methods tocontrol weight) in females. It is evident thatthe drive for thinness subscale includesitems that deal with methods of controllingweight (exercising, dieting, etc.). Similarly,the EDI body dissatisfaction scale focuses
154
Variance=3.3%F=8.89
P<0.003
Variance=35.4%F=85.9
P<0.001
Variance=5.5%F=9.88
P<0.001
Variance=2.1%F=5.52P<0.02
Variance=25.4%F=20.3
P<0.001
Number of methodsused to
control weight
Triceps skinfold thickness
Drive for thinnessand
body dissatisfaction
Males
Number of methodsused to
control weight
Body mass index(weight for height) Drive for thinness
Females
Variance=19.5%F=19.3
P<0.001
FIGURE 1Path analysis, showing the mediating role played by eating attitudes in the relationship between physical characteristics and theuse of methods to control weight. For men, EDI drive for thinness and body dissatisfaction were partial mediators of the positiverelationship between triceps skinfold thickness and methods used to control weight. For females, only EDI drive for thinness actedas a mediator in the BMI-weight control link.

on body aspects to which women are par-ticularly sensitive (such as thighs, hips andabdomen), and not on areas that might becentral to men´s body dissatisfaction (e.g.,poor upper body strength or poor muscu-lature). This overlap was only partial, sincethe correlation coefficients (Table 2) sug-gest that the maximum level of shared vari-ance between the constructs was approxi-mately 36%. Thus, the EDI scores are notsimply reflective of the use of weight con-trol methods. However, future studiesmight use measures that address eatingattitudes in isolation from weight controlbehaviours and are applicable to bothmales and females [e.g., Stroop tasks withbody shape and food words; the ThreeFactor Eating Questionnaire (31)].
While similar research needs to be car-ried out with clinical populations, the pre-sent results suggest that treatment pro-grammes to reduce the use of weight con-trol methods might benefit from address-ing the eating attitudes (and other factors)that mediate the relationship between actu-al physical characteristics and restrictiveeating. These findings might also bear onthe development of primary preventionprogrammes, suggesting that the optimumtargets for change will be eating attitudes,rather than the physical characteristicsthemselves. However, the attitudes thatwould require targeting are likely to be dif-ferent between males and females.
ACKNOWLEDGEMENTS
The authors would like to acknowledge the assis-tance of the schools that allowed access to theparticipants. The research was supported by aresearch grant from the Junta de Extremadura.This research was also assisted by the advice ofcolleagues in the Department of Pharmacologyand Psychiatry, Medical School, University ofExtremadura. Thanks are also due to Professor J.E. Campillo,Department of Physiology, University ofExtremadura.
REFERENCES
1. Patton C.J., Selzer R., Coffey C., Carlin J.B.,Wolfe R.: Onset of adolescent eating disor-ders: population based cohort study over 3years. Br. Med. J., 318, 765-768, 1999.
2. Santonastaso P., Friederici S., Favaro A.: Full
and partial syndromes in eating disorders: Aone-year prospective study of risk factorsamong female students. Psychopathology, 32,50-56, 1999.
3. Striegel-Moore R.H., Silberstein L.R., RodinJ.: Towards an understanding of risk factorsfor bulimia. Am. Psychol., 41, 246-263, 1986.
4. Fairburn C.G., Welch S.L., Doll H.A., DaviesB.A., O´Connor M.E.: Risk factors for bulim-ia nervosa. A community based case-controlstudy. Arch. Gen. Psychiatry, 54, 509-517,1997.
5. Fairburn C.G., Cooper Z., Doll H.A., WelchS.L.: Risk factors for anorexia nervosa: threeintegrated case-control comparisons. Arch.Gen. Psychiatry, 56, 468-476, 1999.
6. Polivy J., Herman C.P.: Dieting and binge-ing: a causal analysis. Am. Psychol., 40, 193-201, 1985.
7. Thompson J.K., Coovert M.D., Richards K.J., Johnson S., Cattarin J.: Development ofbody image, eating disturbance, and generalpsychological functioning in female adoles-cents: covariance structure modeling andlongitudinal investigations. Int. J. Eat.Disord., 3, 221-236, 1995.
8. Shisslak C.M., Crago M., McKnight K.M.,Estes L.S., Gray N., Parnaby O.G.: Potentialrisks factors associated with weight controlbehaviors in elementary and middle school-girls. J. Psychosom. Res., 44, 301-313, 1998.
9. Taylor C.B., Sharpe T., Shisslack C., BrysonS., Estes L.S., Gray N., McKnight K.M., CragoM., Kraemer H.C., Killen J.D.: Factors associ-ated with weight concerns in adolescentgirls. Int. J. Eat. Disord., 24, 31-42, 1998.
10. Grigg M., Bowman J., Redman S.: Disorderedeating and unhealthy weight reduction prac-tices among adolescent females. Prev. Med.,25, 748-756, 1996.
11. Patton G.C., Johnson-Sabine E., Wood K.,Mann A.H., Wakeling A.: Abnormal eatingattitudes in London schoolgirls: outcome attwelve-month follow-up. Psychol. Med., 20,383-394, 1990.
12. Paxton S.J., Wertheim E.H., Gibbons K.,Szmuckler G.I., Hillier L., Petrovich J.L.:Body image satisfaction, dieting beliefs, andweight loss behaviours in adolescent girlsand boys. Journal of Youth and Adolescence,14, 191-206, 1991.
13. Bailey S., Goldberg J., Swap W.C., ChomitzV.R., Houser R.F.: Relationships betweenbody dissatisfaction and physical measure-ments. Int. J. Eat. Disord., 9, 457-461, 1990.
14. Hoffman J., Brownell K.D.: Sex differencesin the relationship of body fat distributionwith psychosocial variables. Int. J. Eat.Disord., 22, 139-147, 1997.
Weight control in adolescence
155

E. Peñas Lledó, L. Sancho and G. Waller
15. Radke-Sharpe N., Whitney-Saltiel D., RodinJ.: Fat distribution as a risk factor for weightand eating concerns. Int. J. Eat. Disord., 9,27-36, 1990.
16. Mahan K., Escott-Stump S.: Krause’s Food,Nutrition & Diet Therapy. McGraw-Hill,Mexico, 1998.
17. Killen J.D., Hayward C., Wilson D.M., TaylorC.B., Hammer L.D., Litt I., Simmonds B.,Haydel F.: Factors associated with eatingdisorder symptoms in a community sampleof 6th and 7th grade girls. Int. J. Eat. Disord.,4, 357-367, 1994.
18. Buddeberg-Fisher B., Bernet R., Sieber M.,Schmid J., Buddeberg C.: Epidemiology ofeating behaviour and weight distribution in14 to 19-year-old Swiss students. ActaPsychiatr. Scand., 93, 296-304, 1996.
19. Neumark-Sztainer D., Story M., Falkner N.H. Beuhring T., Resnick M.D.: Sociode-mographic and personal characteristics ofadolescents engaged in weight loss andweight/muscle gain behaviors: who is doingwhat?. Prev. Med., 28, 40-50, 1999.
20. Toro J., Castro J., García M., Pérez P., CuestaL.: Eating attitudes, sociodemographic factorsand body shape evaluation in adolescence. Br.J. Med. Psychol., 62, 61-70, 1989.
21. Whitaker A., Davies M., Shaffer D., Johnson J.,Abrams S., Walsh B.T., Kalikov K.: The strug-gle to be thin: a survey of anorexic and bulimicsymptoms in a non-referred adolescent popu-lation. Psychol. Med., 19, 143-163, 1989.
22. McFarlane T., Polivy J., Herman C.P.: Effectsof false weight feedback on mood, self-eval-uation, and food intake in restrained andunrestrained eaters. J. Abnorm. Psychol., 2,312-318, 1998.
23. Garner D.M., Olmstead M.A., Polivy J.:Development of a multidimensional EatingDisorder Inventory for anorexia nervosaand bulimia. Int. J. Eat. Disord., 2, 15-34,1983.
24. Guimerá Querol E., Torrubia Beltri R.:Adaptación española del “Eating DisorderInventory” (EDI) en una muestra depacientes anoréxicas. Anales de Psiquiatría,3, 185-190, 1987.
25. Corral S., Gonzalez M., Pereña J., SeisdedosN.: EDI-2, Inventario de trastornos de la con-ducta alimentaria. Madrid, TEA Ediciones,S.A., 1998.
26. Garner D.: Eating Disorder Inventory - 2.Professional Manual. Odessa, PsychologicalAssessment Resources, 1991.
27. Alastrué A.: Antropometría y obesidad.Medicina Clínica de Barcelona, 102, 16-19,1994.
28. Baron R.M., Kenny D.A.: The moderator-mediator variable distinction in social psy-chological research: Conceptual, strategicand statistical considerations. J. Pers. Soc.Psychol., 51, 1173-1182, 1986.
29. Strong K.G., Huon G.F.: An evaluation of astructural model for studies of the initiationof dieting among adolescent girls. J.Psychosom. Res., 44, 315-326, 1998.
30. Huon G.F., Hayne A., Gunewardene A.,Strong K., Lunn N., Piira T., Lim J.:Accounting for differences in dieting status:Steps in the refinement of a model. Int. J.Eat. Disord., 26, 420-433, 1999.
31. Stunkard A., Messick S.: Three-FactorEating Questionnaire to measure dietaryrestraint, disinhibition and hunger. J.Psychosom. Res., 29, 71-83, 1985.
156