Embed Size (px)
Citation preview

Ftdperimfp(
FaN
2
Journal of the American College of Cardiology Vol. 50, No. 8, 2007© 2007 by the American College of Cardiology Foundation ISSN 0735-1097/07/$32.00P
Cardiac Imaging
Reliable High-Speed CoronaryComputed Tomography in Symptomatic Patients
Annick C. Weustink, MD,*† Willem B. Meijboom, MD,*† Nico R. Mollet, MD, PHD,*†Masato Otsuka, MD,* Fransesca Pugliese, MD,*† Carlos van Mieghem, MD,*† Roberto Malago, MD,†Niels van Pelt, MD,*† Marcel L. Dijkshoorn, BSC,† Filippo Cademartiri, MD, PHD,*†Gabriel P. Krestin, MD, PHD,† Pim J. de Feyter, MD, PHD*†
Rotterdam, the Netherlands
Objectives Our objective was to prospectively evaluate the diagnostic performance of the high-speed dual-source computedtomography scanner (DSCT), with an increased temporal resolution (83 ms), for the detection of significant coro-nary lesions (�50% lumen diameter reduction) in a clinically wide range of patients.
Background Cardiac motion artifacts may decrease coronary image quality with use of earlier computed tomography scan-ners that have a limited temporal resolution.
Methods We prospectively studied 100 symptomatic patients (79 men, 21 women, mean age 61 � 11 years) with atypi-cal (18%) or typical (55%) angina pectoris, or unstable coronary artery disease (27%) scheduled for conventionalcoronary angiography. Mean scan time was 8.58 � 1.52 s. Mean heart rate was 68 � 11 beats/min. Quantita-tive coronary angiography was used as the standard of reference. Irrespective of image quality or vessel size, allsegments were included for analysis.
Results Invasive coronary angiography demonstrated no significant disease in 23%, single-vessel disease in 31%, andmultivessel disease in 46% of patients; 1,489 coronary segments, containing 220 significant (14.8%) stenoses,were available for analysis. Sensitivity, specificity, and positive and negative predictive values of DSCT coronaryangiography for the detection of significant lesions on a segment-by-segment analysis were 95% (95% confi-dence interval [CI] 90 to 97), 95% (95% CI 93 to 96), 75% (95% CI 69 to 80), 99% (95% CI 98 to 99), respec-tively, and on a patient-based analysis 99% (95% CI 92 to 100), 87% (95% CI 65 to 97), 96% (95% CI 89 to 99),and 95% (95% CI 74 to 100), respectively.
Conclusions Noninvasive DSCT coronary angiography is highly sensitive to detect and to reliably rule out the presence of asignificant coronary stenosis in patients presenting with atypical or typical angina pectoris, or unstable coronaryartery disease. (J Am Coll Cardiol 2007;50:786–94) © 2007 by the American College of Cardiology Foundation
ublished by Elsevier Inc. doi:10.1016/j.jacc.2007.04.068
(8sbstpDcic
M
Sd
or almost 50 years, invasive coronary angiography has beenhe standard of reference for diagnosing coronary arteryisease. However, noninvasive coronary imaging with com-uted tomography (CT) has rapidly emerged, and initialxperience with 4-, 16-, and 64-slice CT coronary angiog-aphy has been reported (1–13). Despite technical advancesn CT technology, a substantial number of coronary seg-
ents remain unevaluable due to presence of motion arti-acts and a limited image resolution, which seriously ham-ered clinical implementation of CT coronary angiography4,14).
rom the *Department of Cardiology, Thoraxcenter, Rotterdam, the Netherlands;nd the †Department of Radiology, Erasmus Medical Center, Rotterdam, theetherlands.
qManuscript received December 28, 2006; revised manuscript received April 18,
007, accepted April 24, 2007.
A newly introduced dual-source computed tomographyDSCT) system, with an improved temporal resolution of3 ms independent of patient’s heart rate, allows forcanning of the coronaries without the use of prescaneta-blockers. The pitch is adapted to the heart rate, andcan times are reduced at higher heart rates. Shorter scanimes allow for reduction of radiation exposure to theatient. We now report the diagnostic performance ofSCT coronary angiography to detect or rule out signifi-
ant coronary stenoses in the clinically relevant coronary treen 100 patients with a wide spectrum of symptomaticoronary artery disease.
ethods
tudy population. After an initial 3-week test perioduring which scan protocols were optimized, we subse-
uently included during a 10-week period 111 symptomatic
pcsvthcEcc�((8sPbSwmcdaDnr
afiiCrs
8gdgmo
szwPbtc
msastic
simktmt
ubXXpwwstRdswdrpadeso
evUQenucie
tiswsuMDaAV
lo
787JACC Vol. 50, No. 8, 2007 Weustink et al.August 21, 2007:786–94 Noninvasive Coronary Imaging With Dual-Source CT
atients with atypical angina, typical angina, and unstableoronary artery disease (unstable angina or non–ST-egment elevation myocardial infarction) scheduled for con-entional coronary angiography (CCA). All CT examina-ions were performed before CCA. Only patients in sinuseart rhythm without previous history of percutaneousoronary intervention or bypass surgery were included.xcluded were 11 patients with known allergy to iodinated
ontrast material (n � 1), impaired renal function (serumreatinine �120 �mol/l) (n � 5), persistent arrhythmias (n
3), or logistic inability to perform a CT scan before CCAn � 2). Thus, the study population comprised 100 patients79 men, 21 women, mean age 61 � 10.9 years; range 28 to7 years). The institutional review board approved thetudy, and all patients gave informed consent.atient preparation. No oral or intravenous prescan beta-lockers were administered before the scan.can protocol and image reconstruction. All patientsere scanned using a DSCT (Somatom Definition, Sie-ens Medical Solutions, Forcheim, Germany). The system
ombines 2 arrays each consisting of an X-ray tube plusetector (64 slices) mounted on a single gantry with anngular offset of 90° and a gantry rotation time of 330 ms.ual source computed tomography permits spiral CT scan-
ing of the coronary arteries with an improved temporalesolution of 83 ms using single-segment reconstruction (15).
In DSCT, radiation exposure has been reduced by thepplication of an additional cardiac bowtie filter, a smallereld of vision of the second detector, and an increased pitch
n higher heart rates. All patients underwent a nonenhancedT scan for calcium scoring before DSCT coronary angiog-
aphy. All patients received nitroglycerin (0.4 mg/dose)ublingually just before scanning.
Calcium scoring scan parameters were a tube current of4 mAs/rot (maximum), and full X-ray tube current wasiven during 50% to 70% of the RR interval. A singleataset was reconstructed using electrocardiogram (ECG)ating with a slice thickness of 3 mm and increment of 1.5m using a medium convolution kernel (B35f) during 60%
f the RR interval.Dual source computed tomography scanner angiographic
can parameters were number of slices/rotation 32 � 2 with-flying focal spot for each detector, individual detectoridth 0.6 mm, rotation time 330 ms, tube voltage 120 kV.itch values were adapted to heart rate after an estimationased on the last 10 heartbeats preceding the scan. Eachube provided 412 mAs/rot (maximum), and full X-ray tubeurrent was given during 25% to 70% of the RR interval.
The volume of iodinated contrast material (Ultravist 370gl/ml, Schering AG, Berlin, Germany) was adapted to the
can time. A contrast bolus (60 to 90 mgl) was injected in anntecubital vein at a flow rate of 5.5 ml/s followed by aaline chaser of 40 ml at 5.5 ml/s. A bolus trackingechnique was applied to synchronize the arrival of contrastn the coronary arteries and the start of the scan. All CT
oronary angiography datasets were reconstructed with a mlice thickness of 0.75 mm andncrement of 0.4 mm usingedium-to-smooth convolution
ernel (B26f), resulting in a spa-ial resolution of 0.6 mm to 0.7
m in-plane and 0.5 mmhrough-plane (15).
The reconstruction algorithmses data from a single hearteat, obtained during a quarter-ray tube rotation by 2 separate-ray tubes, resulting in a tem-oral resolution of 83 ms. Imagesere reconstructed after a step-ise pattern depending on patient’s heart rate during
canning. Initially, a single dataset was reconstructed duringhe mid- to end-diastolic phase (350 ms before the next-wave) in patients with low heart rates (�60 beats/min),uring both the mid- to end-diastolic phase and end-ystolic phase (275 ms after the next R-wave) in patientsith intermediate heart rates (60 to 80 beats/min), anduring the end-systolic phase in patients with high heartates (�80 beats/min). Image quality was assessed on aer-segment level. In case of persistent coronary motionrtifacts in patients with low and high heart rates, additionalatasets were reconstructed in end-systolic and mid- tond-diastolic phase, respectively. If necessary, multiple data-ets of a single patient were used separately in order to obtainptimal image quality of all available coronary segments.
The effective dose for DSCT coronary angiography wasstimated based on Monte Carlo calculations (ImPACT,ersion 0.99x, St. George’s Hospital, Tooting, London,nited Kingdom).uantitative coronary angiography (QCA). One experi-
nced cardiologist, unaware of the results of DSCT coro-ary angiography, identified all available coronary segmentssing a 17-segment modified American Heart Associationlassification (16). All segments, irrespective of size, werencluded for comparison with DSCT coronary angiography,xcept for segments distal to a total occlusion.
Segments were classified as normal (smooth parallel orapering borders), as having nonsignificant disease (luminalrregularities or �50% diameter stenosis), or as havingignificant stenoses (�50% diameter stenosis). Stenosesere evaluated in 2 orthogonal views, and classified as
ignificant if the mean lumen diameter reduction was �50%sing a validated QCA algorithm (CAAS, Pie Medical,aastricht, the Netherlands).SCT image evaluation. One experienced observer, un-
ware of the results of CCA, calculated total calcium scores asgatston scores, using validated software (Syngo MMWPE20A, Siemens, Forcheim, Germany).One observer evaluated image quality on a per-segment
evel and classified as good image quality (defined as absencer presence of any image-degrading artifacts related to
Abbreviationsand Acronyms
CCA � conventionalcoronary angiography
CI � confidence interval
CT � computedtomography
DSCT � dual-sourcecomputed tomographyscanner
QCA � quantitativecoronary angiography
otion, calcification, or noise, but e
valuations possible with
gdcsc
CAirswSciivnccsssarttcvd
R
Pirwb
ctrTw(mcw1bhpow
wpp
1RaotDTsd1PawwhddaltmVaccoa
P
Ce
788 Weustink et al. JACC Vol. 50, No. 8, 2007Noninvasive Coronary Imaging With Dual-Source CT August 21, 2007:786–94
ood-to-moderate confidence), or poor (presence of image-egrading artifacts and evaluation only possible with lowonfidence). Irrespective of image quality, all available coronaryegments (including poor image quality) were included foromparison of DSCT with CCA.
Two experienced observers, unaware of the results ofCA, scored all DSCT coronary angiography datasets.xial views and maximum intensity projections were used to
dentify coronary lesions. In addition, (curved) multiplanareconstructions were used to classify coronary lesions intoignificantly diseased or not. Interobserver disagreementsere resolved by consensus in a joint session.tatistical analysis. The diagnostic performance of DSCToronary angiography for the detection of significant lesionsn coronary arteries with QCA as the standard of references presented as sensitivity, specificity, positive predictivealue and negative predictive values, and positive andegative likelihood ratios with the corresponding 95%onfidence intervals (CIs). Comparison between DSCToronary angiography and QCA was performed on 3 levels:egment-by-segment, vessel-by-vessel (no or any significanttenosis per vessel), and patient-by-patient (no or anyignificant stenosis per patient). An additional sensitivitynalysis to detect significant stenoses was performed afterandom selection of a single segment per patient to explorehe effect of nesting. Inter- and intraobserver variability forhe detection of significant coronary artery stenosis wasalculated using � statistics. To determine the intraobserverariability, 1 observer evaluated 30 (33%, 30 of 100) CTatasets twice with a time interval of 3 weeks.
esults
atient demographics are shown in Table 1. The meannterval between conventional and DSCT coronary angiog-aphy was 4.0 � 4.8 days (range 0 to 17 days). All scansere performed without the use of oral or intravenouseta-blockers.Mean scan range was 11.9 � 1.1 cm (range 9.3 to 13.8
m). Mean CT acquisition time was 8.6 � 1.5 s (range 5.7o 12.7 s). Pitch varied between 0.20 and 0.53. Mean heartate was 68 � 11 beats/min (range 44 to 107 beats/min).he overall radiation exposure for CT coronary angiographyas estimated as 11.1 to 14.4 (men to women) mSv; 71
71%, 71 of 100) patients had long-term beta-blockeredication. The estimated radiation exposure of DSCT
oronary angiography was 13.5 to 16.9 mSv (men toomen) in low heart rates (mean 56 beats/min), 10.7 to3.8 mSv (men to women) in moderate heart rates (mean 68eats/min), and 8.3 to 9.6 mSv (men to women) in higheart rates (mean 81 beats/min). In 5% (5 of 100) ofatients with a ventricular extrasystole and in 3% (3 of 100)f patients with a premature atrial complex, ECG editing
as successful. tA single dataset for the assessment of significant stenosesas used in 81%, 2 datasets in 16%, and 3 datasets in 3% ofatients in order to obtain optimal image quality on aer-segment level.Image quality was classified as good in 94% (1,400 of
,489) and poor in 6% (89 of 1,489) on a per-segment level.easons for poor image quality were breathing motion
rtifacts (33%, 29 of 89), cardiac motion artifacts (14%, 12f 89), severe calcifications (46%, 41 of 89), or low contrast-o-noise (8%, 7 of 89).
iagnostic performance of DSCT coronary angiography.he diagnostic accuracy of DSCT to detect significant
tenoses on a patient-, segment-, and vessel-based analysis isetailed in Table 2. Typical examples are shown in Figuresand 2.atient-by-patient analysis. Sixteen patients with eithern angiographically normal coronary angiogram (n � 16) orith nonsignificant disease (n � 4) were correctly identifiedith DSCT. Three patients were incorrectly classified asaving single-vessel disease. One patient with significantisease was incorrectly classified as having nonsignificantisease with DSCT. Agreement between DSCT coronaryngiography and QCA on a per-patient (no or any disease)evel was good (� value 0.89). Agreement between bothechniques for classifying patients as having no, single-, orultivessel disease was very good (� value 0.85).essel-by-vessel analysis. One significantly diseased left
nterior descending artery and 2 significantly diseased rightoronary arteries were incorrectly classified as nonsignifi-antly diseased on the CT scan. Sensitivity for the detectionf significantly diseased left anterior descending coronaryrteries was 98%, for the right coronary arteries 96%, and for
atient Demographics (n � 100)
Table 1 Patient Demographics (n � 100)
Age, yrs (range) 61 � 11 (28–87)
Men, % 79
Women, % 21
Clinical presentation
Atypical angina, % 18
Typical angina, % 55
Unstable CAD, % 27
Risk factors
Hypertension, % 58
Hypercholesterolemia, % 55
Smoker, % 63
Diabetic mellitus, % 19
Family history of CAD, % 38
Obese (body mass index �30 kg/m2), % 65
Invasive coronary angiography
Absence of CAD, % 16
Nonsignificant disease, % 7
Single-vessel disease, % 31
Multivessel disease, % 46
AD � coronary artery disease; Unstable CAD � patients with unstable angina or non–ST-segmentlevation myocardial infarction.
he left main and circumflex coronary arteries 100%. Agree-

mpStwwcwcaswspmrl
o
d0
sic
hit
odanidpa2(ipp
tad
tcwvp
gnos
tic
Per
form
ance
and
Pre
dict
ive
Val
ueof
DS
CT
Cor
onar
yA
ngio
grap
hyfo
rth
eD
etec
tion
ofSig
nific
ant
(>50%
)Ste
nose
s
able
2D
iagn
osti
cP
erfo
rman
cean
dP
redi
ctiv
eV
alue
ofD
SC
TC
oron
ary
Ang
iogr
aphy
for
the
Det
ecti
onof
Sig
nific
ant
(>50%
)Ste
nose
s
Pre
vale
nce
ofD
isea
se(%
)n
TPTN
FPFN
�Sen
siti
vity
(%)
Spe
cific
ity
(%)
PP
V(%
)N
PV
(%)
AC
C(%
)�
LR�
LR
atie
nt-b
ased
anal
ysis
All
patie
nts
77
10
07
62
03
10
.88
99
(92
–10
0)
87
(65
–97
)9
6(8
9–9
9)
95
(74
–10
0)
96
(92
–10
0)
7.6
0.0
1
egm
ent-b
ased
anal
ysis
All
segm
ents
15
1,4
89
20
81
,20
06
91
20
.81
95
(90
–97
)9
5(9
3–9
6)
75
(69
–80
)9
9(9
8–9
9)
95
(93
–96
)1
7.4
0.0
6
Pro
xim
alse
gmen
ts1
34
49
53
36
82
53
0.7
69
5(8
4–9
7)
94
(91
–96
)6
8(5
6–7
8)
99
(97
–10
0)
94
(92
–96
)1
4.9
0.0
6
Mid
segm
ents
26
28
97
11
92
23
30
.79
96
(88
–99
)8
9(8
4–9
3)
76
(65
–84
)9
8(9
5–1
00
)9
1(8
8–9
4)
90
.05
Dis
tals
egm
ents
13
30
53
72
58
73
0.8
69
3(7
9–9
3)
97
(94
–99
)8
4(6
9–9
3)
99
(96
–10
0)
97
(95
–99
)3
5.0
0.0
8
Sid
ebr
anch
es1
14
46
47
38
21
43
0.8
39
4(8
2–9
8)
97
(94
–98
)7
7(6
4–8
7)
99
(98
–10
0)
96
(94
–98
)2
6.6
0.0
6
esse
l-bas
edan
alys
is
All
vess
els
38
40
01
48
22
32
63
0.8
59
8(9
6–9
9)
90
(85
–93
)8
5(7
9–9
0)
99
(96
–10
0)
93
(90
–95
)9
.40
.02
LM7
10
07
92
10
0.9
31
00
(10
0)
99
(93
–10
0)
88
(47
–99
)1
00
(95
–10
0)
99
(97
–10
0)
93
0
LAD
51
10
05
03
51
41
0.7
09
8(9
5–1
00
)7
1(5
7–8
3)
78
(66
–87
)9
7(8
4–1
00
)8
5(7
8–9
1)
3.4
0.0
3
CX
47
10
04
74
67
00
.86
10
0(1
00
)8
7(7
4–9
4)
87
(74
–94
)1
00
(90
–10
0)
93
(88
–98
)7
.60
RCA
46
10
04
45
04
20
.88
96
(92
–10
0)
93
(81
–98
)9
2(7
9–9
7)
96
(86
–99
)9
4(8
9–9
9)
12
.90
.05
rdin
gto
the
17
-seg
men
tmod
ified
Am
eric
anH
eart
Ass
ocia
tion
clas
sific
atio
n,1
,48
9se
gmen
tsan
d4
00
vess
els
visu
aliz
edw
ithco
nven
tiona
lang
iogr
amw
ere
incl
uded
forse
gmen
tand
vess
elan
alys
is,r
espe
ctiv
ely.
Forpa
tient
-bas
edan
alys
is,1
00
patie
nts
wer
ein
clud
ed.
esin
pare
nthe
ses
repr
esen
tup
per
and
low
erbo
und
for
95
%co
nfide
nce
inte
rval
.CC
�ac
cura
cy;C
X�
circ
umfle
xco
rona
ryar
tery
;DSCT
�du
al-s
ourc
eco
mpu
ted
tom
ogra
phy
scan
ner;
FN�
fals
ene
gativ
e;FP
�fa
lse
posi
tive;
LAD
�le
ftan
terior
desc
endi
ngco
rona
ryar
tery
;LM
�le
ftm
ain
coro
nary
arte
ry;N
PV
�ne
gativ
epr
edic
tive
valu
e;P
PV
�po
sitiv
eic
tive
valu
e;R
CA
�righ
tco
rona
ryar
tery
;TN
�tr
uene
gativ
e;TP
�tr
uepo
sitiv
e;�
LR�
posi
tive
likel
ihoo
dra
tio;�
LR�
nega
tive
likel
ihoo
dra
tio.
789JACC Vol. 50, No. 8, 2007 Weustink et al.August 21, 2007:786–94 Noninvasive Coronary Imaging With Dual-Source CT
ent between CT coronary angiography and QCA on aer-vessel level was very good (� value 0.85).egment-by-segment analysis. A total of 1,489 segments
hat were visualized with invasive coronary angiographyere analyzed with DSCT coronary angiography. Thereere 12 (5.5%, 12 of 220) segments, which were incorrectly
lassified as having nonsignificant stenosis by DSCT, ofhich 3 segments demonstrated poor image quality due to
ardiac motion artifacts in 2 segments (mean heart rates 65nd 78 beats/min) and due to severe calcifications in 1egment. There were 69 (5.4%, 69 of 1,269) segments,hich were incorrectly classified as having a significant
tenosis by DSCT, of which 19 segments demonstratedoor image quality due to severe calcifications in 16 seg-ents, a cardiac motion artifact in 1 segment (mean heart
ate 68 beats/min), a breathing artifact in 1 segment, andow contrast-to-noise in 1 segment.
Agreement between CT coronary angiography and QCAn a per-segment level was very good (� value 0.81).The � value of inter- and intraobserver variability for the
etection of a significant stenosis per segment was 0.83 and.85, respectively.Table 3 shows the diagnostic accuracy of DSCT to detect
ignificant coronary stenoses in patients with low (17 � 27),ntermediate (198 � 96), and high (927 � 727) Agatstonalcium scores based on per-segment–based analysis.
Patients were divided into 3 groups based on the meaneart rate during DSCT. There was no significant difference
n diagnostic accuracy on a segment-based analysis betweenhese groups (Table 4).
In patients with low heart rates (mean 56.1 beats/min),ptimal datasets reconstructed during the mid- to end-iastolic phase were selected in 94% (31 of 33) of patients,nd additional datasets during the end-systolic phase wereeeded in 6% (2 of 33) of patients. In patients with
ntermediate heart rates (mean 67.9 beats/min), optimalatasets reconstructed during the mid- to end-diastolichase were selected in 74% (25 of 34) of patients, anddditional datasets in the end-systolic phase were needed in6% (9 of 34) of patients. In patients with high heart ratesmean 80.7 beats/min), optimal datasets reconstructed dur-ng the end-systolic phase were selected in 91% (30 of 33) ofatients, and additional datasets in the mid- to end-diastolichase were needed in 9% (3 of 33) of patients.Table 5 demonstrates the diagnostic accuracy of DSCT
o detect significant coronary stenoses in patients withtypical and typical angina, and unstable coronary arteryisease based on a segment-based analysis.A sensitivity analysis was performed after random selec-
ion of a single segment per patient. The sensitivity wasalculated as 92% (12 of 13, 95% CI 87 to 96); specificityas 94% (82 of 87, 95% CI 90 to 99); positive predictivealue was 71% (12 of 17, 95% CI 62 to 80); and negative
redictive value was 99% (82 of 83, 95% CI 97 to 100). Dia T P S VAcc
oVa
lu Apr
ed

D
Emlt2ap
sCouh
ssitupvb
Fqmamgca
cqpoihh
alQcc(risr
790 Weustink et al. JACC Vol. 50, No. 8, 2007Noninvasive Coronary Imaging With Dual-Source CT August 21, 2007:786–94
iscussion
arlier studies using 4- and 16-slice CT scanners reportedoderate-to-good diagnostic accuracy to detect significant
esions (1–8,14), but the technique was seriously limited byhe presence of unevaluable segments that were, on average,2% and 9% for the 4- and 16-slice CT, respectively (14). Inrecent multicenter study using 16-slice CT scanners, the
ercentage of unevaluable coronary segments was 29% (4).The development of 64-slice CT scanners involved a
ignificant improvement in image quality and robustness ofT coronary angiography; however, on average, 5% and inne report even 12% of segments were reported to benevaluable, and diagnostic accuracy was reduced at highereart rates (9,10,17,18).The introduction of DSCT is another step forward. This
canner is equipped with 2 X-ray tubes (dual source) therebyignificantly reducing the temporal resolution to 83 msndependent of heart rate, using single-segment reconstruc-ion. In non-DSCT systems, multisegment algorithms aresed to improve temporal resolution. However, this ap-roach is very dependent on a regular heart rate. Minorariation in the time interval between consecutive heart
Figure 1 A Significant Lesion in the LAD
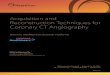
Volume-rendered dual source computed tomography scanner image (coloredimage) and corresponding conventional angiography image of the right coro-nary artery (RCA), left anterior descending artery (LAD), circumflex artery (CX),intermediate branch (IM), diagonal branches (D1, D2) in a 57-year-old man withstable angina and an equivocal bicycle test. Mean heart rate during scanningwas 78 beats/min. A significant lesion was found in the midpart of the LAD(arrow) with detailed color inlay, curved multiplanar reconstruction (bottomleft), and maximum intensity projections image (bottom right). The proximalpart of the CX showed an occlusion (arrowhead).
eats can result in interpolation artifacts and image blurring.
urthermore, multisegment reconstruction algorithms re-uire a lower pitch thus longer scan times, more contrastaterial, and a higher radiation exposure. Multisegment
pproaches can also be applied in DSCT, resulting in aean temporal resolution of up to 40 to 60 ms at 0.33 s
antry rotation time. This approach is not recommended fororonary angiography examinations, but may be useful fordvanced functional evaluation (15).
With the DSCT scanner we were able to evaluate alloronary segments irrespective of heart rate and imageuality. Despite the use of the high-speed DSCT scanner,oor image quality due to cardiac motion artifacts wasbserved in 14% of the coronary segments. However, thencidence of poor image quality occurred independent ofeart rate, and good image quality could also be obtained inigh heart rates.We demonstrated that DSCT coronary angiography hadhigh diagnostic accuracy to detect significant coronary
esions on a per-segment-based level as compared withCA. We selected a �50% diameter stenosis as the cutoff
riterion for significant coronary artery disease to allowomparison with the majority of previous published reports19). A segmental analysis is clinically useful in patientseferred for coronary angiography to assess location (prox-mal, mid, distal, right coronary artery, left anterior de-cending artery, circumflex artery); severity (luminal nar-owing �50%); and extent (1-, 2-, or 3-vessel disease) of
Figure 2 A High-Grade Stenosis in the Midpart of the RCA
Conventional angiography image and corresponding volume-rendered dualsource computed tomography scanner image (colored image) in a 68-year-oldman presenting with unstable coronary artery disease. Mean heart rate duringscanning was 66 beats/min. The arrow indicates a high-grade stenosis in themidpart of the right coronary artery (RCA). The arrowheads in the curved multi-planar reconstruction image (bottom) indicate cross sections proximal, within,and distal from the occlusion.

csTast5a
(nslsitpbpubrps
amtrfmgriaecXnSspeaac
hbsplbDee
uenc
eof
Aga
tsto
nS
core
onD
iagn
osti
cA
ccur
acy
ofD
SC
TC
oron
ary
Ang
iogr
aphy
(aSeg
men
t-B
ased
Ana
lysi
s)
able
3In
fluen
ceof
Aga
tsto
nS
core
onD
iagn
osti
cA
ccur
acy
ofD
SC
TC
oron
ary
Ang
iogr
aphy
(aSeg
men
t-B
ased
Ana
lysi
s)
roup
Mea
nA
gats
ton
Sco
reP
reva
lenc
eof
Dis
ease
(%)
n(S
egm
ents
)TP
TNFP
FN�
Sen
siti
vity
(%)
Spe
cific
ity
(%)
PP
V(%
)N
PV
(%)
AC
C(%
)�
LR�
LR
11
7�
27
85
20
39
47
16
40
.88
91
(77
–97
)9
9(9
7–9
9)
86
(73
–94
)9
9(9
8–1
00
)9
8(9
7–9
9)
72
.40
.10
21
98
�9
61
74
77
76
37
62
05
0.8
39
4(8
6–9
8)
95
(92
–97
)7
9(6
9–8
7)
99
(97
–10
0)
95
(93
–97
)1
8.7
0.0
7
39
27
�7
27
20
49
29
33
53
43
30
.74
97
(90
–99
)8
9(8
6–9
2)
68
(60
–76
)9
9(9
7–1
00
)9
1(8
8–9
3)
8.9
0.0
4
esin
pare
nthe
ses
repr
esen
tup
per
and
low
erbo
und
for
95
%co
nfide
nce
inte
rval
.bb
revi
atio
nsas
inTa
ble
2.
791JACC Vol. 50, No. 8, 2007 Weustink et al.August 21, 2007:786–94 Noninvasive Coronary Imaging With Dual-Source CT
oronary artery disease, which determines the value of CTcanning as an alternative to invasive coronary angiography.he patient-based diagnostic accuracy was high (96%), andnegative DSCT scan reliably ruled out the presence of a
ignificant coronary stenosis in patients with atypical andypical angina, and unstable coronary artery disease (Table). These findings indicate that DSCT scanning is reliables a gatekeeper of invasive coronary angiography.
In patients with a positive CT scan showing a severe�70% diameter stenosis) lesion or a totally occluded vessel,o further evaluation is necessary. However, a positive CTcan with an estimated lesion severity of around 50% hasimited value since it poorly discriminates functionallyignificant lesions from the ones that are not hemodynam-cally important (20). In this situation an additional func-ional imaging test such as myocardial perfusion scintigra-hy or stress echocardiography would be a logical stepefore referring the patient for an invasive angiogram andossible revascularization. In patients deemed necessary tondergo revascularization, direct referral to the cathlab maye more logical with invasive assessment of the functionalelevance of a lesion using fractional flow reserve anderformance of percutaneous coronary intervention in theame session.
Lastly, new developments in CT coronary angiographyre desirable for further improvement in clinical perfor-ance. Increased gantry rotation speed can further improve
emporal resolution, but structural modifications will beequired to account for a substantial increase in mechanicalorces on the gantry. An alternative concept is the use ofultiple (�2) X-ray sources and detectors within a single
antry, thereby obviating the need for an increased gantryotation speed to improve temporal resolution. Furthermproved spatial resolution of less than 0.6 mm can bechieved by the use of smaller detector rows. However, anqual contrast-to-noise ratio requires an exponential in-rease in X-ray power, which will result in an excessive-ray radiation exposure. Thus, new detector technology iseeded to further improve spatial resolution.tudy limitations. Dual source computed tomographycanner coronary angiography should not be performed inatients with significant renal dysfunction or contrast intol-rance. This further restricts the use of CT coronaryngiography to selected patients, which should be taken intoccount when the technique is going to be applied in generallinical practice.
One advantage of DSCT is that patients with highereart rates do not require premedication with beta-blockersecause necessary treatment with beta-blockers before CTcanning hampers the CT throughput. The majority ofatients (73%) in our study population already received
ong-term beta-blocker treatment and, therefore, did notenefit from an increased workflow. However, the use ofSCT in low or intermediate risk patient groups with
xpected lower use of chronic beta-blockers could be more
fficient in terms of diagnostic throughput. Infl T GValu A

adtp2eh(csenD
stdstwtdwsbt
Dwcrsvahe
ocstcchr(
sctcppe
Influ
ence
ofH
eart
Rat
eon
the
Dia
gnos
tic
Acc
urac
yof
DS
CT
Cor
onar
yA
ngio
grap
hy(a
Seg
men
t-B
ased
Ana
lysi
s)
able
4In
fluen
ceof
Hea
rtR
ate
onth
eD
iagn
osti
cA
ccur
acy
ofD
SC
TC
oron
ary
Ang
iogr
aphy
(aSeg
men
t-B
ased
Ana
lysi
s)
ean
Hea
rtR
ate
(s)
n(S
egm
ents
)P
reva
lenc
eof
Dis
ease
(%)
TPTN
FPFN
�Sen
siti
vity
(%)
Spe
cific
ity
(%)
PP
V(%
)N
PV
(%)
AC
C(%
)�
LR�
LREf
f.D
ose
(mS
v)
6.1
�4
.24
80
20
93
35
82
63
0.8
39
7(9
0–9
9)
93
(90
–95
)7
8(6
9–8
5)
99
(97
–10
0)
94
(92
–96
)1
4.3
0.0
71
3.5
–16
.9
7.9
�3
.84
90
12
54
41
81
53
0.8
39
5(8
5–9
9)
97
(94
–98
)7
9(6
6–8
7)
99
(98
–10
0)
96
(95
–98
)2
7.4
0.0
51
0.7
–13
.8
0.7
�8
.55
19
13
61
42
42
86
0.7
49
1(8
1–9
6)
94
(91
–96
)6
8(5
8–7
8)
99
(97
–99
)9
3(9
1–9
6)
14
.70
.10
8.3
–9.6
esin
pare
nthe
ses
repr
esen
tup
per
and
low
erbo
und
for
95
%co
nfide
nce
inte
rval
.f.
Dos
e�
effe
ctiv
edo
se(m
en–w
omen
);ot
her
abbr
evia
tions
asin
Tabl
e2
.
792 Weustink et al. JACC Vol. 50, No. 8, 2007Noninvasive Coronary Imaging With Dual-Source CT August 21, 2007:786–94
The rather high radiation exposure with CT coronaryngiography is of concern. In our study, the overall effectiveose for DSCT coronary angiography was estimated as 11.1o 14.4 mSv (men/women), which is lower than the re-orted effective dose in 64-slice CT angiography (15.2 to1.4 mSv men/women) (21). The significant reduction offfective radiation dose (8.3 to 9.6 mSv men/women) inigh (�80 beats/min) heart rates as compared with low�60 beats/min) heart rates (13.5 to 16.9 mSv men/women)an mainly be ascribed to an increased pitch and, therefore,horter scan times in patients with high heart rates. How-ver, compared with the effective dose in diagnostic coro-ary angiography (3 to 10 mSv) (22), the effective dose inSCT coronary angiography still remains relatively high.In this initial experience with the DSCT scanner, we
elected a relatively wide pulsing window (25% to 70% ofhe RR interval), which allows for reconstruction of datasetsuring both the mid- to end-diastolic phase and end-ystolic phase to obtain optimal image quality. However,here is a delicate balance between the width of the pulsingindow and radiation exposure to the patient. Earlier
echnical feasibility studies demonstrated a significant re-uction of the effective radiation dose by using a smalleridth of the pulsing window (15). Further clinical studies
hould establish which pulsing window provides the optimalalance between radiation exposure and image quality, andhe effect of a small pulsing window on diagnostic accuracy.
Persistent arrhythmias preclude accurate assessment withSCT. For the purpose of this study, we excluded patientsith persistent arrhythmias, which was also an exclusion
riteria in studies using 64-slice scanners. However, ouresults demonstrate that DSCT technology enables us tocan patients with minor heart rate irregularities, such as aentricular extrasystole or a premature atrial complex byutomatically switching off ECG pulsing during irregulareartbeats. This enables the operator to perform ECGditing to correct for minor heart rate irregularities.
Severe calcifications remain problematic. Calcificationsbscure the underlying lumen and preclude judgment oforonary lumen integrity resulting in overestimation of theeverity of a coronary stenosis. This explains the observationhat in 84% (16 of 19) of segments, which were incorrectlylassified as having a significant stenosis by DSCT, severealcifications resulted in poor image quality. In patients withigh (mean 927 � 727) Agatston scores, diagnostic accu-acy was lower (91%) as compared with patient with lowmean 17 � 27) Agatston scores (98%) (Table 4).
Our study was performed in a selected population con-isting of symptomatic patients who were referred foronventional coronary angiography. This was evidenced byhe fact that our study population had a high prevalence oforonary disease (77%, 77 of 100), and that a fairly largeopulation had multivessel disease (46%, 46 of 100). In thisopulation, DSCT coronary angiography performed well toxcellent, but it remains to be demonstrated that such a high
diagnostic accuracy will be achieved in a symptomaticT M 5 6 8
Valu Ef

pd
C
Owcsnsstiiop
RDBl
R
1
1
1
1
Dia
gnos
tic
Per
form
ance
and
Pre
dict
ive
Val
ueof
DS
CT
Cor
onar
yA
ngio
grap
hyfo
rth
eD
etec
tion
ofSig
nific
ant
(>5
0%
)Ste
nose
sin
Pat
ient
sW
ith
Aty
pica
lA
ngin
a,Ty
pica
lA
ngin
a,or
Uns
tabl
eC
AD
able
5D
iagn
osti
cP
erfo
rman
cean
dP
redi
ctiv
eV
alue
ofD
SC
TC
oron
ary
Ang
iogr
aphy
for
the
Det
ecti
onof
Sig
nific
ant
(>5
0%
)S
teno
ses
inP
atie
nts
Wit
hA
typi
calA
ngin
a,Ty
pica
lA
ngin
a,or
Uns
tabl
eC
AD
Pre
vale
nce
ofD
isea
se(%
)N
TPTN
FPFN
�Sen
siti
vity
(%)
Spe
cific
ity
(%)
PP
V(%
)N
PV
(%)
AC
C(%
)�
LR�
LR
atie
nt-b
ased
anal
ysis
Aty
pica
lang
ina
39
18
71
10
01
.00
10
0(5
6–1
00
)1
00
(68
–10
0)
10
0(5
6–1
00
)1
00
(68
–10
0)
10
0—
0
Typi
cala
ngin
a8
95
54
94
20
0.7
81
00
(91
–10
0)
67
(24
–94
)9
6(8
5–9
9)
10
01
00
(91
–10
0)
30
Uns
tabl
eCA
D7
82
72
05
11
0.7
99
5(7
4–1
00
)1
00
(52
–10
0)
10
0(4
0–1
00
)8
6(7
3–9
9)
96
(83
–10
0)
—0
.05
egm
ent-b
ased
anal
ysis
Aty
pica
lang
ina
62
81
17
26
04
00
.89
10
0(7
7–1
00
)9
9(9
6–1
00
)8
1(5
7–9
4)
10
0(9
8–1
00
)9
9(9
7–1
00
)6
6.0
0
Typi
cala
ngin
a1
78
09
12
56
33
42
90
.79
93
(87
–97
)9
4(9
2–9
5)
75
(67
–81
)9
9(9
7–9
9)
94
(92
–95
)1
5.0
0.0
7
Uns
tabl
eCA
D1
73
99
66
30
72
33
0.8
09
6(8
7–9
9)
93
(90
–95
)7
4(6
4–8
3)
99
(97
–99
)9
3(9
1–9
6)
13
.70
.05
revi
atio
nsas
inTa
bles
1an
d2
.
793JACC Vol. 50, No. 8, 2007 Weustink et al.August 21, 2007:786–94 Noninvasive Coronary Imaging With Dual-Source CT
atient population with a low-to-intermediate prevalence ofisease or in a nonchest-pain population.
onclusions
ur study was performed in a high-risk population with aide range of symptoms who were referred for conventional
oronary angiography. Dual source computed tomographycanner coronary angiography demonstrated a high diag-ostic accuracy for the detection or exclusion of significanttenoses in patients with various heart rates without exclu-ion of unevaluable segments. These results indicate that theechnique may now be tested in a cohort with a low-to-ntermediate pretest probability of coronary artery disease orn patients with nonanginal chest pain to establish the rolef DSCT coronary angiography in the management ofatients with suspected coronary artery disease.
eprint requests and correspondence: Dr. Pim J. de Feyterepartment of Cardiology and Radiology, Thoraxcenter, Rooma 589, ’s Gravendijkwal 230, 3000 CA Rotterdam, the Nether-
ands. E-mail: [email protected].
EFERENCES
1. Nieman K, Oudkerk M, Rensing BJ, et al. Coronary angiography withmulti-slice computed tomography. Lancet 2001;357:599–603.
2. Knez A, Becker CR, Leber A, et al. Usefulness of multislice spiralcomputed tomography angiography for determination of coronaryartery stenoses. Am J Cardiol 2001;88:1191–4.
3. Achenbach S, Ropers D, Pohle FK, et al. Detection of coronary arterystenoses using multi-detector CT with 16 � 0.75 collimation and 375ms rotation. Eur Heart J 2005;26:1978–86.
4. Garcia MJ, Lessick J, Hoffmann MH. Accuracy of 16-row multide-tector computed tomography for the assessment of coronary arterystenosis. JAMA 2006;296:403–11.
5. Heuschmid M, Kuettner A, Schroeder S, et al. ECG-gated 16-MDCT of the coronary arteries: assessment of image quality andaccuracy in detecting stenoses. AJR Am J Roentgenol 2005;184:1413–9.
6. Kuettner A, Beck T, Drosch T, et al. Diagnostic accuracy ofnoninvasive coronary imaging using 16-detector slice spiral computedtomography with 188 ms temporal resolution. J Am Coll Cardiol2005;45:123–7.
7. Ropers D, Baum U, Pohle K, et al. Detection of coronary arterystenoses with thin-slice multi-detector row spiral computed tomogra-phy and multiplanar reconstruction. Circulation 2003;107:664–6.
8. Mollet NR, Cademartiri F, Nieman K, et al. Multislice spiralcomputed tomography coronary angiography in patients with stableangina pectoris. J Am Coll Cardiol 2004;43:2265–70.
9. Leschka S, Alkadhi H, Plass A, et al. Accuracy of MSCT coronaryangiography with 64-slice technology: first experience. Eur Heart J2005;26:1482–7.
0. Raff GL, Gallagher MJ, O’Neill WW, Goldstein JA. Diagnosticaccuracy of noninvasive coronary angiography using 64-slice spiralcomputed tomography. J Am Coll Cardiol 2005;46:552–7.
1. Gallagher MJ, Ross MA, Raff GL, Goldstein JA, O’Neill WW,O’Neil B. The diagnostic accuracy of 64-slice computed tomographycoronary angiography compared with stress nuclear imaging in emer-gency department low-risk chest pain patients. Ann Emerg Med2007;49:125–36.
2. Stein PD, Hoffmann U, Beemath A, Moselewski F. Noninvasiveimaging of the coronary arteries. Minerva Cardioangiol 2006;54:619–31.
3. Nikolaou K, Knez A, Rist C, et al. Accuracy of 64-MDCT in the
diagnosis of ischemic heart disease. AJR Am J Roentgenol 2006;187:111–7.T P S
Abb

1
1
1
1
1
1
2
2
2
794 Weustink et al. JACC Vol. 50, No. 8, 2007Noninvasive Coronary Imaging With Dual-Source CT August 21, 2007:786–94
4. Stein PD, Beemath A, Kayali F, Skaf E, Sanchez J, Olson RE.Multidetector computed tomography for the diagnosis of coronaryartery disease: a systematic review. Am J Med 2006;119:203–16.
5. Flohr TG, McCollough CH, Bruder H, et al. First performanceevaluation of a dual-source CT (DSCT) system. Eur Radiol 2006;16:256–68.
6. Austen WG, Edwards JE, Frye RL, et al. A reporting system onpatients evaluated for coronary artery disease. Report of the Ad HocCommittee for Grading of Coronary Artery Disease, Council onCardiovascular Surgery, American Heart Association. Circulation1975;51:5–40.
7. Leber AW, Knez A, von Ziegler F, et al. Quantification of obstructiveand nonobstructive coronary lesions by 64-slice computed tomogra-phy: a comparative study with quantitative coronary angiography andintravascular ultrasound. J Am Coll Cardiol 2005;46:147–54.
8. Ropers D, Rixe J, Anders K, et al. Usefulness of multidetector row
spiral computed tomography with 64- � 0.6-mm collimation and330-ms rotation for the noninvasive detection of significant coronaryartery stenoses. Am J Cardiol 2006;97:343–8.
9. Hamon M, Biondi-Zoccai GG, Malagutti P, Agostoni P, Morello R,Valgimigli M. Diagnostic performance of multislice spiral computedtomography of coronary arteries as compared with conventionalinvasive coronary angiography: a meta-analysis. J Am Coll Cardiol2006;48:1896–910.
0. Schuijf JD, Wijns W, Jukema JW, et al. Relationship betweennoninvasive coronary angiography with multi-slice computed tomog-raphy and myocardial perfusion imaging. J Am Coll Cardiol 2006;48:2508–14.
1. Mollet NR, Cademartiri F, van Mieghem CA, et al. High-resolutionspiral computed tomography coronary angiography in patients referredfor diagnostic conventional coronary angiography. Circulation 2005;112:2318–23.
2. Morin RL, Gerber TC, McCollough CH. Radiation dose in com-
puted tomography of the heart. Circulation 2003;107:917–22.