Embed Size (px)
Citation preview
The LaryngoscopeVC 2009 The American Laryngological,Rhinological and Otological Society, Inc.
Relocation Pharyngoplasty for ObstructiveSleep Apnea
Hsueh-Yu Li, MD, FACS; Li-Ang Lee, MD
Objectives/Hypothesis: To investigate the effi-cacy of relocation pharyngoplasty as a surgical tech-nique both to enlarge pharyngeal airspace and todecrease pharyngeal collapse in the treatment of ob-structive sleep apnea (OSA).
Study Design: Prospective comparative studyperformed in a tertiary referred sleep center.
Methods: Ten adult male OSA patients (medianage of 38 years, median apnea-hypopnea index [AHI]of 41.6 events/hour, and median body mass index of25.8 kg/m2) with favorable oropharyngeal structurewere enrolled. Principal procedures of the relocationpharyngoplasty include tonsillectomy, removal ofsupratonsillar mucosa and adipose tissue, splintingthe lateral pharyngeal wall by suturing the placatingsuperior pharyngeal constrictor muscle to the ante-rior pillar, and advancing the soft palate by suturingthe posterior pillar flap cephalad laterally to thesupratonsillar fossa.
Results: No patients experienced swallowingdisturbance or change of voice after 3 months postop-eratively. The median time for patients to return tonormal nourishment was 15 days. Six months afterthe operation, there were statistically significantimprovements in snoring (P ¼ .005) and daytimesleepiness (P ¼ .008). Repeated polysomnographyrevealed significant improvement in AHI (P ¼ .005)and rapid eye movement period (P ¼ .037). Further-more, reduction in AHI following relocation pharyngo-plasty was found in all patients.
Conclusions: In selected patients, relocationpharyngoplasty by advancing the soft palate andsplinting the lateral pharyngeal wall obtains signifi-cant improvement in subjective snoring and daytimesleepiness, as well as objective adverse sleep respira-tory events and sleep architecture, while retainingnormal pharyngeal function.
Key Words: Obstructive sleep apnea, relocationpharyngoplasty, snoring, daytime sleepiness, apnea-hypopnea index.
Laryngoscope, 119:2472–2477, 2009
INTRODUCTIONIt is crucial to establish whether obstructive sleep
apnea (OSA) is an anatomic disease or neurological dis-order, as the direction of treatment could differaccordingly: whether to enlarge airspace from an ana-tomic viewpoint or to avoid collapse from a neurologicalbase.1 Clinically, abnormal anatomy in the upper airwayis obvious in some OSA patients; however, no significantnarrowing of the upper airway is found in others. It isplausible to presume that both anatomy and neurologymay play a role in contributing to OSA with differentproportions in different individuals. Consequently, sur-gery in treating OSA may need to correct both anatomicobstruction and pharyngeal collapse.
Surgical treatments for OSA aim primarily toreduce pharyngeal narrowing by either removing thepharyngeal soft tissue or moving forward the maxillofa-cial bone to enlarge the pharyngeal lumen. However,there is no difference in pharyngeal cross-sectional areasbetween OSA patients and the weight-matched nonap-neic control.2 Additionally, image studies were unable toshow strong correlations between the severity of OSAand pharyngeal dimension.3,4 Further, the enlarged pha-ryngeal lumen was not associated with improvedpolysomnographic parameters.5,6 These results appear tosupport that OSA cannot fully be attributed to structuralnarrowing of pharyngeal lumen, and enlargement of thepharyngeal airway does not necessarily improve OSA.
The lateral pharyngeal wall (LPW) is a complexstructure composed of numerous pharyngeal musclegroups, in addition to lymphoid tissue (palatine tonsils).The role of the LPW in the pathogenesis of OSA hasbeen demonstrated by Swab et al.7 The LPW is thickerand more collapsible in sleep disordered breathingpatients than in normal subjects when under pressurefrom airflow during awake respiration.8 The narrowingof the LPW appears to be the sole independent risk fac-tor in oropharyngeal findings for male OSA patientswhen controlling for body mass index (BMI) and neckcircumference.9 Through progressive increase of positive
From the Department of Otolaryngology, Sleep Center, Chang GungMemorial Hospital, Taipei, Taiwan (H.-Y.L., L.-A.L.); the Department ofOtolaryngology, School of Medicine, Chang Gung University, Taoyuan,Taiwan (H.-Y.L., L.-A.L.); and the Department of Sleep Medicine, RoyalInfirmary Edinburgh, Edinburgh, United Kingdom (H.-Y.L.).
Editor’s Note: This Manuscript was accepted for publication onJune 16, 2009.
Send correspondence to Hsueh-Yu Li, MD, Department of Otolar-yngology, Chang Gung Memorial Hospital, 5, Fu-Shin Street, Kweishan,Taoyuan 333, Taiwan. E-mail: [email protected]
DOI: 10.1002/lary.20634
Laryngoscope 119: December 2009 Li and Lee: Relocation Pharyngoplasty for OSA
2472
pressure in a normal subject, the enlargement of airwaylumen appears mainly in its lateral dimensions withreduction of thickness of the LPW, and with minimalchanges in the soft palate and tongue.10 Surgical proce-dures to alter the LPW can be approached by indirecttensioning of the LPW through repositioning the sur-rounding bone by maxillomandibular advancement11 ordirect splinting of the LPW by sewing the superior pha-ryngeal constrictor (SPC) muscle.12
The purpose of this article is to present the authors’preliminary results in the treatment of OSA patientsusing our technique, known as relocation pharyngo-plasty, which involves advancement of the soft palateand splinting of the LPW to fulfill both increase of pha-ryngeal airspace and decrease of pharyngeal collapse.
MATERIALS AND METHODS
Patient SelectionInclusion criteria. Candidates for relocation pharyngo-
plasty must have experienced significant clinical symptoms ofsnoring and/or daytime sleepiness with apnea-hypopnea index(AHI) >5 events/hour. All patients failed to respond to conserva-tive measures, such as changes in sleep position and sleephygiene, and were either intolerant of or unwilling to submit tocontinuous positive airway pressure therapy before beingselected of surgical intervention.
Specific criteria of relocation pharyngoplasty included: 1)webbing, thin, and pliable posterior pillars in physical examina-tion (Fig. 1); and 2) sagittal collapse of retropalatal space of50% or more in Muller’s maneuver during fiberopticlaryngoscopy.
Severity of OSA is not the major concern in patient selec-tion of relocation pharyngoplasty. Patients with severe OSAwith favorable anatomic conditions were enrolled in this study.
Exclusionary criteria. Elderliness (age >60 years), mor-bid obesity (BMI >35 kg/m2), gross maxillary and mandibulardeformities (mainly retrognathia), macroglossia, and presence ofhypopharyngeal obstruction during Muller’s maneuver in fiber-optic laryngoscopy are the exclusion criteria of relocationpharyngoplasty.
Surgical ProcedureAll the procedures were performed while the patient was
under general anesthesia with orally endotracheal intubation.Patients had their heads extended and a mouth gag (Naga-shima Medical Instrument Co., Tokyo, Japan) was used toadequately expose the oropharynx. The operation was initiatedwith a bilateral tonsillectomy. The palatoglossus, palatopharyn-geus, and SPC muscles were easily identified following the
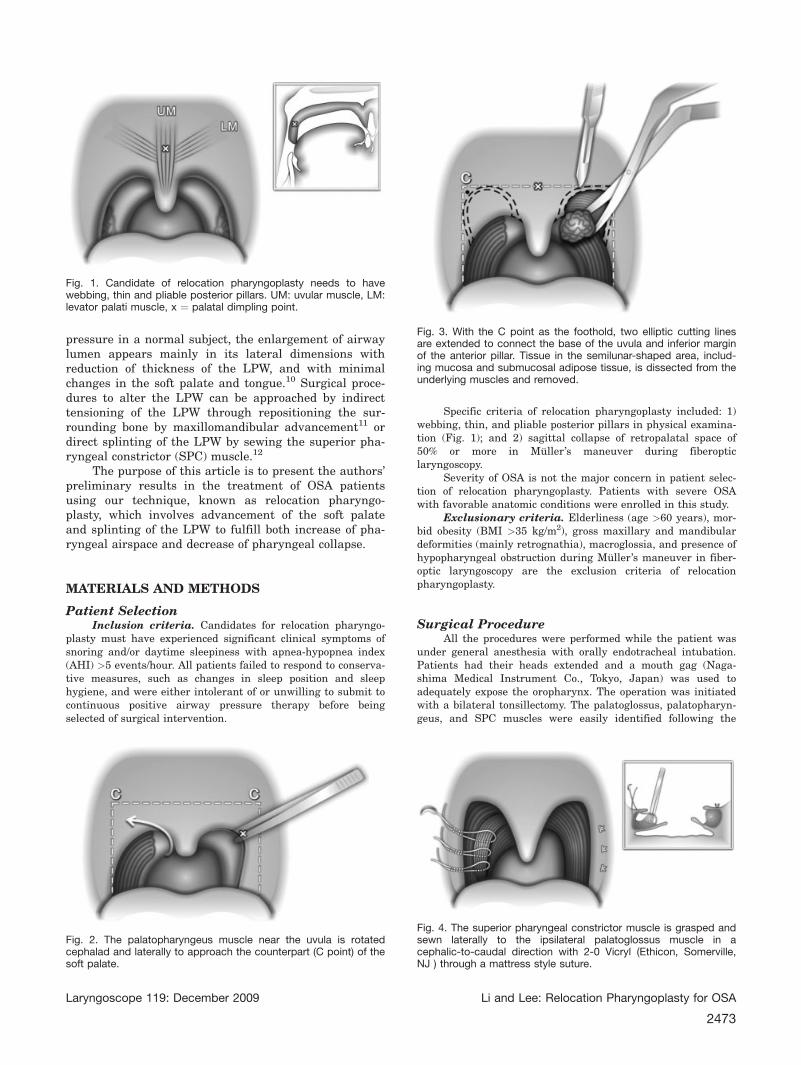
Fig. 1. Candidate of relocation pharyngoplasty needs to havewebbing, thin and pliable posterior pillars. UM: uvular muscle, LM:levator palati muscle, x ¼ palatal dimpling point.
Fig. 2. The palatopharyngeus muscle near the uvula is rotatedcephalad and laterally to approach the counterpart (C point) of thesoft palate.
Fig. 3. With the C point as the foothold, two elliptic cutting linesare extended to connect the base of the uvula and inferior marginof the anterior pillar. Tissue in the semilunar-shaped area, includ-ing mucosa and submucosal adipose tissue, is dissected from theunderlying muscles and removed.
Fig. 4. The superior pharyngeal constrictor muscle is grasped andsewn laterally to the ipsilateral palatoglossus muscle in acephalic-to-caudal direction with 2-0 Vicryl (Ethicon, Somerville,NJ ) through a mattress style suture.
Laryngoscope 119: December 2009 Li and Lee: Relocation Pharyngoplasty for OSA
2473
tonsillectomy. The palatopharyngeus muscle near the uvula wasrotated cephalad and laterally to approach the counterpart ofthe soft palate (C point in Fig. 2). With the C point as a foot-hold, two elliptic cutting lines were extended to connect thebase of the uvula and inferior margin of the anterior pillar. Tis-sue in the semilunar-shaped area including mucosa andsubmucosal adipose tissue was dissected from the underlyingmuscles and removed (Fig. 3).
The SPC muscle was grasped and sewn laterally to the ip-silateral palatoglossus muscle in a cephalic-to-caudal directionwith 2-0 Vicryl (Ethicon, Somerville, NJ) through a mattressstyle (Fig. 4) suture. The suture usually requires three to fourseparated stitches to splint the SPC muscle in one tonsillarfossa. The palatopharyngeal muscle was divided from the SPCmuscle to facilitate tension-free approximation. The posteriorpillar flap was then erected from a horizontal to vertical planeand sewn onto the residual palatoglossus muscle (Fig. 5). Thesame procedure was repeated on the opposite side and, finally,the distal (nonmuscular) part of the uvula was resected (Fig. 6).
Outcome MeasurementChange in AHI 6 months following the relocation pharyn-
goplasty was the primary measure of outcome. Other outcomesincluded changes in polysomnographic indices (e.g., minimal ox-ygen saturation and sleep architecture) and OSA-relatedsymptoms. The institutional review board of the Chang GungMemorial Hospital approved the study.
Statistical AnalysisStatistical analyses were performed using the SPSS ver-
sion 11.0 for Windows (SPSS Inc., Chicago, IL). Changes inOSA-related symptoms and polysomnographic parametersbefore and after relocation pharyngoplasty were compared usingthe Wilcoxon signed rank test. Data are expressed as mean andmedian. A 2-tailed P value of <.05 was considered significant.
RESULTSTen adult male OSA patients with a median age of
38 years, a median AHI of 41.6 events/hour, and a me-dian BMI of 25.8 kg/m2 were enrolled for surgicalintervention using relocation pharyngoplasty (Table I).Extubation in the operation theater resulted in no com-promise of the airway. The patients reportedpostoperative pain at a mean value of 6 on the 10-pointvisual analog scale. The mean time for patients to returnto a normal diet was 15.2 days. We did not observe anypostoperative wound bleeding in this study population.Additionally, there was no nasal regurgitation, alterna-tions in speech, or taste loss observed 3 monthspostoperatively. It is noteworthy that only one patient
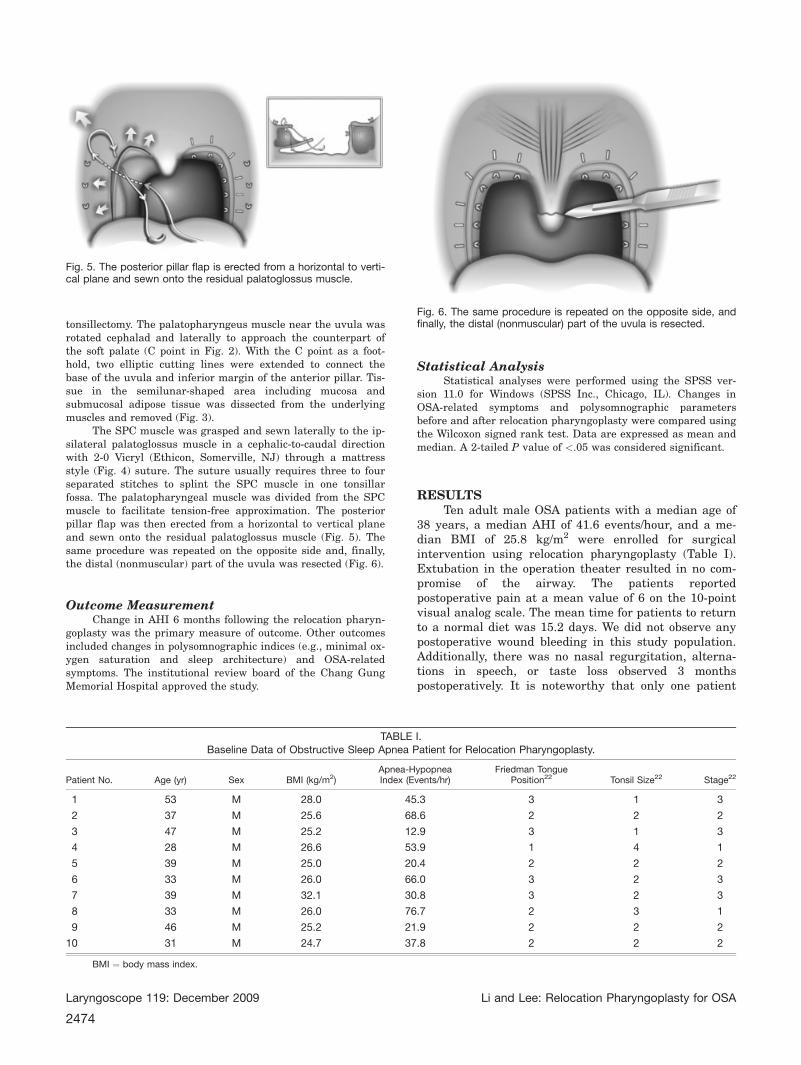
Fig. 5. The posterior pillar flap is erected from a horizontal to verti-cal plane and sewn onto the residual palatoglossus muscle.
Fig. 6. The same procedure is repeated on the opposite side, andfinally, the distal (nonmuscular) part of the uvula is resected.
TABLE I.Baseline Data of Obstructive Sleep Apnea Patient for Relocation Pharyngoplasty.
Patient No. Age (yr) Sex BMI (kg/m2)Apnea-HypopneaIndex (Events/hr)
Friedman TonguePosition22 Tonsil Size22 Stage22
1 53 M 28.0 45.3 3 1 3
2 37 M 25.6 68.6 2 2 2
3 47 M 25.2 12.9 3 1 3
4 28 M 26.6 53.9 1 4 1
5 39 M 25.0 20.4 2 2 2
6 33 M 26.0 66.0 3 2 3
7 39 M 32.1 30.8 3 2 3
8 33 M 26.0 76.7 2 3 1
9 46 M 25.2 21.9 2 2 2
10 31 M 24.7 37.8 2 2 2
BMI ¼ body mass index.
Laryngoscope 119: December 2009 Li and Lee: Relocation Pharyngoplasty for OSA
2474
experienced wound dehiscence in the inferior pole of theright tonsillar fossa.
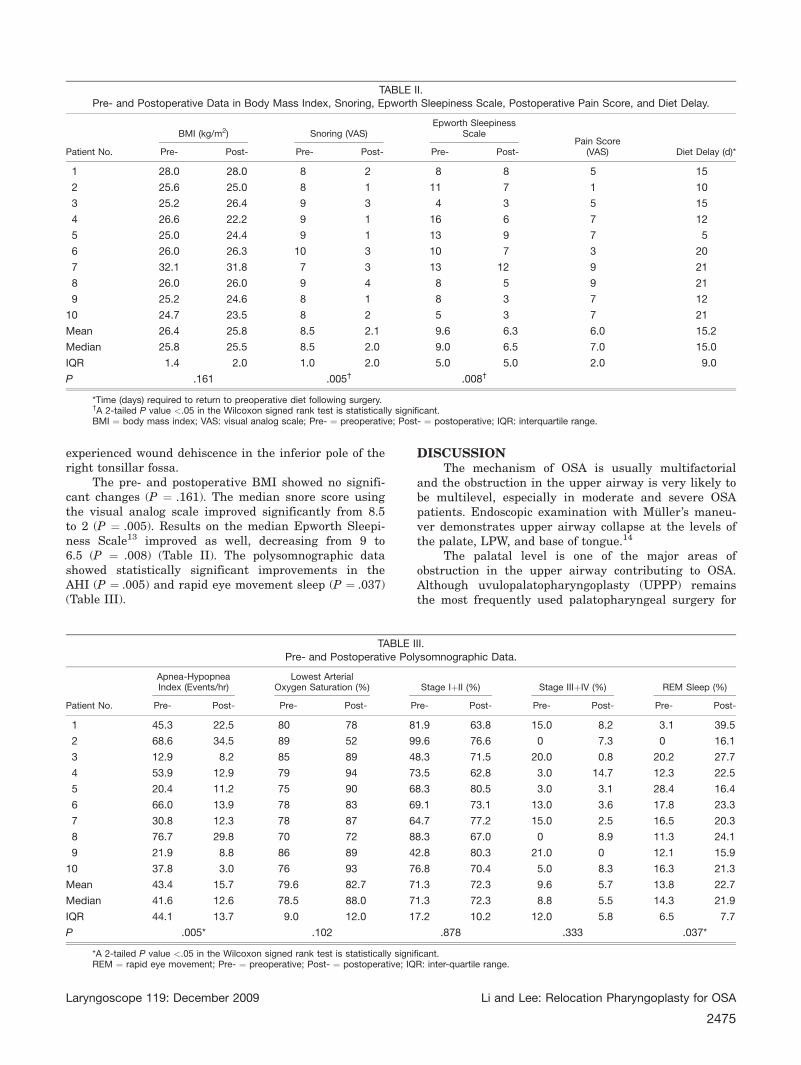
The pre- and postoperative BMI showed no signifi-cant changes (P ¼ .161). The median snore score usingthe visual analog scale improved significantly from 8.5to 2 (P ¼ .005). Results on the median Epworth Sleepi-ness Scale13 improved as well, decreasing from 9 to6.5 (P ¼ .008) (Table II). The polysomnographic datashowed statistically significant improvements in theAHI (P ¼ .005) and rapid eye movement sleep (P ¼ .037)(Table III).
DISCUSSIONThe mechanism of OSA is usually multifactorial
and the obstruction in the upper airway is very likely tobe multilevel, especially in moderate and severe OSApatients. Endoscopic examination with Muller’s maneu-ver demonstrates upper airway collapse at the levels ofthe palate, LPW, and base of tongue.14
The palatal level is one of the major areas ofobstruction in the upper airway contributing to OSA.Although uvulopalatopharyngoplasty (UPPP) remainsthe most frequently used palatopharyngeal surgery for
TABLE II.Pre- and Postoperative Data in Body Mass Index, Snoring, Epworth Sleepiness Scale, Postoperative Pain Score, and Diet Delay.
Patient No.
BMI (kg/m2) Snoring (VAS)Epworth Sleepiness
ScalePain Score
(VAS) Diet Delay (d)*Pre- Post- Pre- Post- Pre- Post-
1 28.0 28.0 8 2 8 8 5 15
2 25.6 25.0 8 1 11 7 1 10
3 25.2 26.4 9 3 4 3 5 15
4 26.6 22.2 9 1 16 6 7 12
5 25.0 24.4 9 1 13 9 7 5
6 26.0 26.3 10 3 10 7 3 20
7 32.1 31.8 7 3 13 12 9 21
8 26.0 26.0 9 4 8 5 9 21
9 25.2 24.6 8 1 8 3 7 12
10 24.7 23.5 8 2 5 3 7 21
Mean 26.4 25.8 8.5 2.1 9.6 6.3 6.0 15.2
Median 25.8 25.5 8.5 2.0 9.0 6.5 7.0 15.0
IQR 1.4 2.0 1.0 2.0 5.0 5.0 2.0 9.0
P .161 .005† .008†
*Time (days) required to return to preoperative diet following surgery.†A 2-tailed P value <.05 in the Wilcoxon signed rank test is statistically significant.BMI ¼ body mass index; VAS: visual analog scale; Pre- ¼ preoperative; Post- ¼ postoperative; IQR: interquartile range.
TABLE III.
Pre- and Postoperative Polysomnographic Data.
Patient No.
Apnea-HypopneaIndex (Events/hr)
Lowest ArterialOxygen Saturation (%) Stage IþII (%) Stage IIIþIV (%) REM Sleep (%)
Pre- Post- Pre- Post- Pre- Post- Pre- Post- Pre- Post-
1 45.3 22.5 80 78 81.9 63.8 15.0 8.2 3.1 39.5
2 68.6 34.5 89 52 99.6 76.6 0 7.3 0 16.1
3 12.9 8.2 85 89 48.3 71.5 20.0 0.8 20.2 27.7
4 53.9 12.9 79 94 73.5 62.8 3.0 14.7 12.3 22.5
5 20.4 11.2 75 90 68.3 80.5 3.0 3.1 28.4 16.4
6 66.0 13.9 78 83 69.1 73.1 13.0 3.6 17.8 23.3
7 30.8 12.3 78 87 64.7 77.2 15.0 2.5 16.5 20.3
8 76.7 29.8 70 72 88.3 67.0 0 8.9 11.3 24.1
9 21.9 8.8 86 89 42.8 80.3 21.0 0 12.1 15.9
10 37.8 3.0 76 93 76.8 70.4 5.0 8.3 16.3 21.3
Mean 43.4 15.7 79.6 82.7 71.3 72.3 9.6 5.7 13.8 22.7
Median 41.6 12.6 78.5 88.0 71.3 72.3 8.8 5.5 14.3 21.9
IQR 44.1 13.7 9.0 12.0 17.2 10.2 12.0 5.8 6.5 7.7
P .005* .102 .878 .333 .037*
*A 2-tailed P value <.05 in the Wilcoxon signed rank test is statistically significant.REM ¼ rapid eye movement; Pre- ¼ preoperative; Post- ¼ postoperative; IQR: inter-quartile range.
Laryngoscope 119: December 2009 Li and Lee: Relocation Pharyngoplasty for OSA
2475

OSA, its low success rate and sequent morbidities limitthe procedure’s clinical use. Many modifications ofUPPP have been proposed to contend with anatomicalvariations of the pharynx and minimize morbidities.15–18
Advancing the palate forward was advocated by Wood-son and Toohill,19 who excised the hard palate, created apalatal flap, and pulled forward the flap, a procedurethat the authors called transpalatal advancement pha-ryngoplasty. The advancement of the soft palate inrelocation pharyngoplasty is achieved by removingsupratonsillar mucosa and submucosal adipose tissue tocreate a space for the reconstruction of the velopharynx.The rotation of the posterior pillar flap in a cephalad-lat-eral direction toward the third molar turns the posteriorpillars from a horizontal plane to a vertical plane, andconsequently moves the soft palate in a forward direc-tion, thus enlarging the retropalatal space. (Fig. 7). It isworth noting that the magnitude of forward movementof the soft palate is dependent on the amplitude of trac-tion of the posterior pillar flap, which is closer to theroot of uvula as the traction point leads further forwardof the soft palate (Fig. 8). The relocation pharyngoplastyby advancement instead of excision of the soft palate notonly enlarges the retropalatal space to relieve obstruc-tion for snoring, but also preserves palatal muscles andglands for normal swallowing, speech, and pharyngealfunction. In the study, significant improvements in snor-
ing (P ¼ .005) and daytime sleepiness (P ¼ .008) werenoted. Further, no patients experienced nasal regurgita-tion, voice change, and/or pharyngeal dryness by the3rd-month follow-up. The preliminary results supportthat relocation pharyngoplasty leads to favorableresponse in the treatment of OSA and maintains pha-ryngeal function. To further investigate the impact ofrelocation pharyngoplasty on swallowing and phonation,a study to compare pre- and postoperative changes innasalance, nasality, voice, and articulation has beenundertaken.
The technique of splinting the LPW to decreasepharyngeal collapse in OSA patients was introduced byCahali,12 who dissected the SPC muscle into medial andlateral flaps, and sutured the lateral flap to palatoglos-sus muscle, which the author called lateralpharyngoplasty. The preliminary results in a group of 10patients showed significant improvement of AHI from41.2 to 9.5 events/hour (P ¼ .009). The present studyrevealed similar results with significant reduction ofAHI from 41.6 to 12.6 events/hour (P ¼ .005). These con-sistent data suggest that a direct approach to LPW byrelocating the SPC muscle may splint the collapsiblepharynx and produce appreciable benefits for OSApatients.
Although the similar core value in splinting theLPW properly, there are some obvious differences intechnique between relocation pharyngoplasty and lateralpharyngoplasty.
First, the relocation pharyngoplasty does not under-mine the SPC muscle. Without violating the SPC muscleand exposing the parapharyngeal space, relocation pha-ryngoplasty essentially avoids the possibility ofdamaging major neurovascular structures herein. Eventhough Cahali12 reported no major complications in thelateral pharyngoplasty, patients did experience signifi-cant dysphagia following surgery, which eventuallyresolved. In the study, no serious dysphagia occurredand all patients returned to normal nourishment within2 to 3 weeks postoperatively. In addition to safety con-cerns, the disuse of microscopic dissecting of the SPCmuscle makes relocation pharyngoplasty simpler andless time-consuming.
Second, instead of suturing the lateral flap of theSPC muscle in lateral pharyngoplasty, relocation pha-ryngoplasty sutures the plicate SPC muscle. Theplicateness of the SPC muscle can rebuild tonsillar fossa
Fig. 7. The rotation of the posterior pillar flap in a cephalad-lateraldirection moves the soft palate in a forward direction, thus enlarg-ing the retropalatal space.
Fig. 8. Endoscopic view demonstrates that the magnitude of theforward movement of the soft palate is dependent on the ampli-tude of traction of the posterior pillar flap, closer to the root ofuvula as the traction point leads further forward of the soft palate.
Laryngoscope 119: December 2009 Li and Lee: Relocation Pharyngoplasty for OSA
2476
and avoid the cicatricial effect from tonsillar woundsthat pull the tongue backward, decrease the distancebetween tongue base and posterior pharyngeal wall, andconsequently narrow the retroglossal airspace. In ourprevious study,6 three-dimensional computed tomogra-phy was used to assess the changes of the upper airwaydimension following extended uvulopalatal flap surgery,which included primary closure of the tonsillar fossa.The results showed a decrease of the retroglossal spacefrom 171.0 � 110.8 mm2 to 149.0 � 92.4 mm2 despitesignificant enlargement at the retropalatal space from38.2 � 40.3 mm2 to 71.2 � 45.8 mm2 (P < .001). Shepardand Thawley20 also reported the paradoxical changes(enlarged retropalatal space with narrowed retroglossalspace following UPPP). We presume that the decreasedretroglossal space from scarring contraction of the tonsil-lar wound may play a confounding factor in theunpredictable UPPP outcomes. Further study thatincludes measuring the retroglossal space following relo-cation pharyngoplasty is warranted to confirm thishypothesis.
It is well known that weight reduction has a sub-stantial ameliorative effect on OSA.21 In our patients wedid not observe a significant reduction of BMI 6 monthsafter surgery (25.8 kg/m2 vs. 25.4 kg/m2; P ¼ .161). Con-sequently, the bias of weight change following surgerycan be excluded from surgical outcomes for OSA in thisstudy. Anatomic consideration is crucial to the analysisof surgical outcomes for OSA. In the Friedman stagingsystem,22 OSA patients with stage III are least likely tobenefit from UPPP, with only an 8% rate of success(defined by an AHI reduction of 50% and postoperativeAHI <20 events/hour). In this study, the success rate instage III patients was 50% (2/4). We theorize that splint-ing the SPC muscle in relocation pharyngoplastydecreases the LPW collapse and consequently stabilizesthe retroglossal space that contributes to overcomingunfavorable tongue position.
CONCLUSIONThe study provides a surgical technique to rebuild
the narrow pharynx by advancing the soft palate andsplinting the LPW in an attempt to enlarge airwaylumen and lessen pharyngeal collapse. In appropriatelyselected patients, the relocation pharyngoplasty pro-duces promising results while retaining normalpharyngeal functions that offer a favorable alternativeto traditional UPPP in OSA patients.
BIBLIOGRAPHY1. Schwab RJ, Strohl KP. Sleep apnea is (not) an anatomic dis-
order. Am J Respir Crit Care Med 2003;168:270–273.2. Stauffer JL, Zwillich CW, Cadieux RJ, et al. Pharyngeal
size and resistance in obstructive sleep apnea. Am RevRespir Dis 1987;136:623–627.
3. Bhattacharyya N, Blake SP, Fried MP. Assessment of theairway in obstructive sleep apnea syndrome with 3-
dimensional airway computed tomography. OtolaryngolHead Neck Surg 2000;123:444–449.
4. Li HY, Chen NH, Wang CJ, Shu YH, Wang PC. Use of 3-dimensional computed tomography scan to evaluateupper airway patency for patients undergoing sleep-disor-dered breathing surgery. Otolaryngol Head Neck Surg2003;129:336–342.
5. Ryan CF, Lowe AA, Li D, Fleetham JA. Three-dimensionalupper airway computed tomography in obstructive sleepapnea: a prospective study in patients treated by uvulopa-latopharyngoplasty. Am Rev Respir Dis 1991;144:428–432.
6. Li HY, Li KK, Chen NH, Wang CJ, Liao YF, Wang PC. Three-dimensional computed tomography and polysomnographyfindings after extended uvulopalatal flap surgery for ob-structive sleep apnea. Am J Otolaryngol 2005;26:7–11.
7. Schwab RJ, Gefter WB, Hoffman EA, et al. Dynamic upperairway imaging during awake respiration in normal sub-jects and patients with sleep-disordered breathing. AmRev Respir Dis 1993;148:1385–1400.
8. Schwab RJ, Gupta KB, Gefter WB, et al. Upper airway andsoft tissue anatomy in normal subjects and patients withsleep-disordered breathing: significance of the lateralpharyngeal walls. Am J Respir Crit Care Med 1995;152:1673–1689.
9. Schellenberg JB, Maislin G, Schwab RJ. Physical findingsand the risk for obstructive sleep apnea: the importanceof oropharyngeal structures. Am J Respir Crit Care Med2000;162:740–748.
10. Schwab RJ, Pack A, Gupta HB, et al. Upper airway andsoft tissue structural changes induced by CPAP in normalsubjects. Am J Respir Crit Care Med 1996;154:1106–1116.
11. Riley RW, Powell NB, Li KK, et al. Surgery and obstructivesleep apnea: long-term clinical outcomes. OtolaryngolHead Neck Surg 2000;122:415–421.
12. Cahali MB. Lateral pharyngoplassty: a new treatment forobstructive sleep apnea hypopnea syndrome. Laryngo-scope 2003;113:1961–1968.
13. Johns MW. A new method for measuring daytime sleepi-ness: the Epworth Sleepiness Scale. Sleep 1991;14:540–545.
14. Terris DJ. Hanasono MM, Liu YC. Reliability of the Mullermaneuver and its association with sleep-disorderedbreathing. Laryngoscope 2000;110:1818–1823.
15. Fairbanks DNF. Uvulopalatopharyngoplasty complicationsand avoidance strategies. Otolaryngol Head Neck Surg1990;102:239–245.
16. Powell N, Riley R, Guilleminault C, et al. A reversible uvu-lopalatal flap for snoring and sleep apnea syndrome.Sleep 1996;19:593–599.
17. Friedman M, Ibrahim HZ, Vidvasagar R, Pomeranz J. Z-palatoplasty (ZPP): a technique for patients without ton-sils. Otolaryngol Head Neck Surg 2004;131:89–100.
18. Li HY, Li KK, Chen NH, Wang PC. Modified uvulopalato-pharyngoplasty: the extended uvulopalatal flap. Am JOtolaryngol 2003;24:311–316.
19. Woodson BT, Toohill RJ. Transpalatal advancement pharyn-goplasty for obstructive sleep apnea. Laryngoscope 1993;103:169–176.
20. Shepard JW, Thawley SE. Evaluation of the upper airwayby computerized tomography in patients undergoing uvu-lopalatopharyngoplasty for obstructive sleep apnea. AmRev Respir Dis 1989;140:711–716.
21. Schwartz AR, Gold AR, Schubert N, et al. Effect of weightloss on upper airway collapsibility in obstructive sleepapnea. Am Rev Respir Dis 1991;144:494–498.
22. Friedman M, Ibrahim H, Joseph NJ. Staging of obstructivesleep apnea/hypopnea syndrome: a guide to appropriatetreatment. Laryngoscope 2004;114:454–459.
Laryngoscope 119: December 2009 Li and Lee: Relocation Pharyngoplasty for OSA
2477