Embed Size (px)
Citation preview

REMARKS ON THIRTY-THREE CASES OF SUBDURALEFFUSION IN INFANCY
BY
E. HERZBERGER, Y. ROTEM and J. BRAHAMFrom the Departments of Neurosurgery, Paediatrics and Neurology, Tel-Hashomer Government Hospital,
Tel-Aviv, Israel
(RECEIVED FOR PUBLICATION SEPTEMBER 20, 1955)
Following the pioneer work of Ingraham andMatson (1954), the diagnostic possibility of subduraleffusion in infancy has excited the interest ofpaediatricians and neurosurgeons. Guthkelch(1953) remarks that the condition may be regardedas one of the most frequent neurosurgical disordersin infancy, a striking observation when it is con-sidered that up to 10 years ago the diagnosis wasrarely made. The absence of a clear history oftrauma in many cases, together with the discoverythat effusions may follow meningitis, has led manypaediatricians to perform subdural taps in a widerange of clinical conditions. Although otherwiseunsuspected effusions may be revealed in this wayone may be left with an uneasy feeling that thecondition is being over-diagnosed, the more so asrecognition of the condition carries with it in manycases a firm recommendation to craniotomy.The purpose of this paper is to present our
personal experience of 33 cases treated in the Tel-Hashomer Hospital between 1953 and 1955, andour views regarding various aspects of the problem.The babies were of an age varying from 1 day to
24 months and in the main were from new immigrantfamilies living in poor conditions. Eighteen wereadmitted from other institutions with an establisheddiagnosis of subdural effusion.
AetiologyIn 15 cases there was an antecedent purulent
meningitis; the causative organisms were Haemo-philus influenzae, pneumococci or meningococci.In three cases a reasonably certain history of birthinjury was obtained, and in one a history of a fall.One case was of Torula histolytica encephalitis.
In 13 cases no certain history of trauma could beobtained. It must be emphasized that cooperationwith the parents was in many instances not satis-factory and in the kind of homes from which thechildren came there was ample opportunity forunrecognized trauma.
44
The pathogenesis of the effusion has already beenadequately discussed (Guthkelch, 1953). It shouldbe added that the role of the tap itself is not entirelyunsuspect, and it is not always possible to denythat needling may indeed be the cause of localeffusion, particularly where it is repeated wheninitially unproductive. That this is at any rate notalways the case was demonstrated in 32 cases of thepresent series where the first tap did, in fact, revealfluid. Biochemical examinations of the fluid con-firmed the naked-eye impression that it was notidentical with cerebrospinal fluid; protein values ofthe order of 180 to 3,400 mg. % were consistentlyobtained, whereas in the C.S.F. the average laybetween 20 and 180 mg. %.
PathologyOpportunities for observation of meningeal and
cerebral changes were provided by burr holes(22 cases) and post-mortem examination (sevencases). In three of the latter, burr holes hadbeen made previously, and it was possible to confirmthe conclusion that they permitted a reliable impres-sion to be obtained of the state of the underlyingstructures.
In this way clear evidence of brain damage(excluding simple reversible compression) was seenin 16 out of 22 operated cases. The changesincluded (a) atrophy, microgyria, scarring-varyingin degree from moderate to most severe; (b) oedema,greyish-red discoloration, purulent cortical softening,milky opacity of the pia and pial congestion-theselatter occurring chiefly in post-meningitic patients.Of the seven cases examined at necropsy, one
(Case 3) was a baby dying on the day of birth with alarge right-sided subdural haematoma (undiag-nosed). One died following purulent meningitisand was found to have a thalamic abscess. In fourinfants the effusion developed during the course ofan illness characterized otherwise by gastro-enteritis, malnutrition, bronchopneumonia and a
copyright. on 21 July 2018 by guest. P
rotected byhttp://adc.bm
j.com/
Arch D
is Child: first published as 10.1136/adc.31.155.44 on 1 F
ebruary 1956. Dow
nloaded from
SUBDURAL EFFUSION IN INFANCY
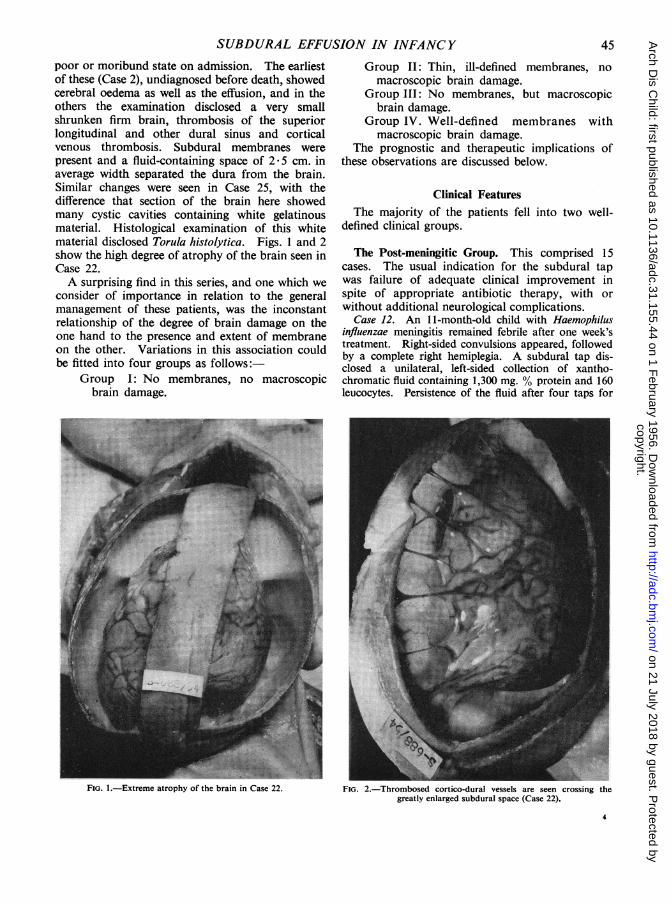
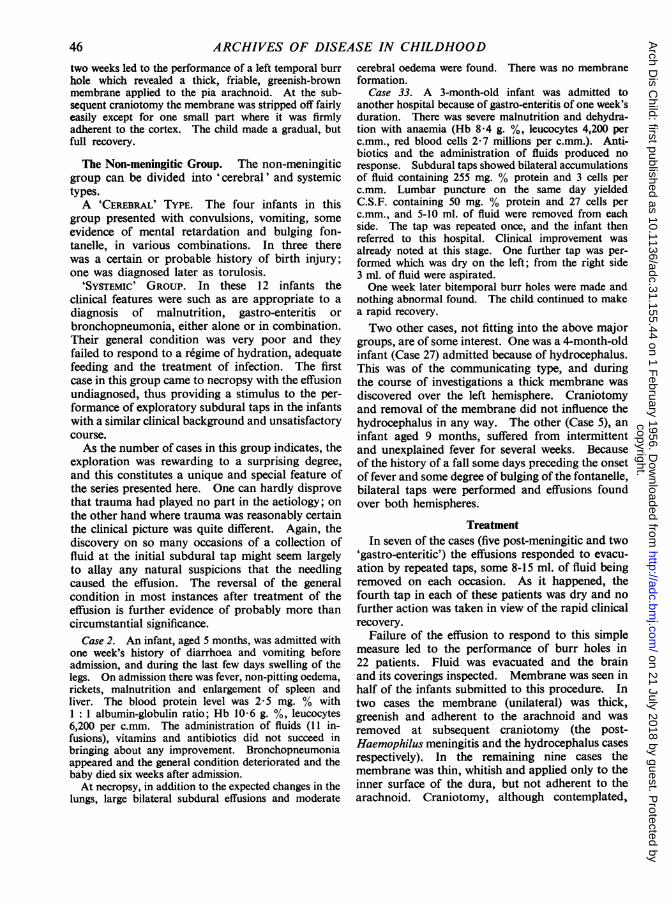
poor or moribund state on admission. The earliestof these (Case 2), undiagnosed before death, showedcerebral oedema as well as the effusion, and in theothers the examination disclosed a very smallshrunken firm brain, thrombosis of the superiorlongitudinal and other dural sinus and corticalvenous thrombosis. Subdural membranes werepresent and a fluid-containing space of 2 5 cm. inaverage width separated the dura from the brain.Similar changes were seen in Case 25, with thedifference that section of the brain here showedmany cystic cavities containing white gelatinousmaterial. Histological examination of this whitematerial disclosed Torula histolytica. Figs. 1 and 2show the high degree of atrophy of the brain seen inCase 22.A surprising find in this series, and one which we
consider of importance in relation to the generalmanagement of these patients, was the inconstantrelationship of the degree of brain damage on theone hand to the presence and extent of membraneon the other. Variations in this association couldbe fitted into four groups as follows:-
Group I: No membranes, no macroscopicbrain damage.
FIG. 1.-Extreme atrophy of the brain in Case 22.
Group II: Thin, ill-defined membranes, nomacroscopic brain damage.
Group III: No membranes, but macroscopicbrain damage.
Group IV. Well-defined membranes withmacroscopic brain damage.
The prognostic and therapeutic implications ofthese observations are discussed below.
Clinical FeaturesThe majority of the patients fell into two well-
defined clinical groups.
The Post-meningitic Group. This comprised 15cases. The usual indication for the subdural tapwas failure of adequate clinical improvement inspite of appropriate antibiotic therapy, with orwithout additional neurological complications.
Case 12. An 11-month-old child with Haemophilusinfluenzae meningitis remained febrile after one week'streatment. Right-sided convulsions appeared, followedby a complete right hemiplegia. A subdural tap dis-closed a unilateral, left-sided collection of xantho-chromatic fluid containing 1,300 mg. % protein and 160leucocytes. Persistence of the fluid after four taps for
FiG. 2.-Thrombosed cortico-dural vessels are seen crossing thegreatly enlarged subdural space (Case 22).
45copyright.
on 21 July 2018 by guest. Protected by
http://adc.bmj.com
/A
rch Dis C
hild: first published as 10.1136/adc.31.155.44 on 1 February 1956. D
ownloaded from
ARCHIVES OF DISEASE IN CHILDHOODtwo weeks led to the performance of a left temporal burrhole which revealed a thick, friable, greenish-brownmembrane applied to the pia arachnoid. At the sub-sequent craniotomy the membrane was stripped off fairlyeasily except for one small part where it was firmlyadherent to the cortex. The child made a gradual, butfull recovery.
The Non-meningitic Group. The non-meningiticgroup can be divided into 'cerebral' and systemictypes.A 'CEREBRAL' TYPE. The four infants in this
group presented with convulsions, vomiting, someevidence of mental retardation and bulging fon-tanelle, in various combinations. In three therewas a certain or probable history of birth injury;one was diagnosed later as torulosis.
'SYSTEMIC' GROUP. In these 12 infants theclinical features were such as are appropriate to adiagnosis of malnutrition, gastro-enteritis orbronchopneumonia, either alone or in combination.Their general condition was very poor and theyfailed to respond to a regime of hydration, adequatefeeding and the treatment of infection. The firstcase in this group came to necropsy with the effusionundiagnosed, thus providing a stimulus to the per-formance of exploratory subdural taps in the infantswith a similar clinical background and unsatisfactorycourse.As the number of cases in this group indicates, the
exploration was rewarding to a surprising degree,and this constitutes a unique and special feature ofthe series presented here. One can hardly disprovethat trauma had played no part in the aetiology; onthe other hand where trauma was reasonably certainthe clinical picture was quite different. Again, thediscovery on so many occasions of a collection offluid at the initial subdural tap might seem largelyto allay any natural suspicions that the needlingcaused the effusion. The reversal of the generalcondition in most instances after treatment of theeffusion is further evidence of probably more thancircumstantial significance.
Case 2. An infant, aged 5 months, was admitted withone week's history of diarrhoea and vomiting beforeadmission, and during the last few days swelling of thelegs. On admission there was fever, non-pitting oedema,rickets, malnutrition and enlargement of spleen andliver. The blood protein level was 2*5 mg. % with1 :1 albumin-globulin ratio; Hb 10-6 g. %, leucocytes6,200 per c.mm. The administration of fluids (11 in-fusions), vitamins and antibiotics did not succeed inbringing about any improvement. Bronchopneumoniaappeared and the general condition deteriorated and thebaby died six weeks after admission.At necropsy, in addition to the expected changes in the
lungs, large bilateral subdural effusions and moderate
cerebral oedema were found. There was no membraneformation.
Case 33. A 3-month-old infant was admitted toanother hospital because of gastro-enteritis of one week'sduration. There was severe malnutrition and dehydra-tion with anaemia (Hb 8-4 g. %, leucocytes 4,200 perc.mm., red blood cells 2-7 millions per c.mm.). Anti-biotics and the administration of fluids produced noresponse. Subdural taps showed bilateral accumulationsof fluid containing 255 mg. % protein and 3 cells perc.mm. Lumbar puncture on the same day yieldedC.S.F. containing 50 mg. % protein and 27 cells perc.mm., and 5-10 ml. of fluid were removed from eachside. The tap was repeated once, and the infant thenreferred to this hospital. Clinical improvement wasalready noted at this stage. One further tap was per-formed which was dry on the left; from the right side3 ml. of fluid were aspirated.One week later bitemporal burr holes were made and
nothing abnormal found. The child continued to makea rapid recovery.Two other cases, not fitting into the above major
groups, are of some interest. One was a 4-month-oldinfant (Case 27) admitted because of hydrocephalus.This was of the communicating type, and duringthe course of investigations a thick membrane wasdiscovered over the left hemisphere. Craniotomyand removal of the membrane did not influence thehydrocephalus in any way. The other (Case 5), aninfant aged 9 months, suffered from intermittentand unexplained fever for several weeks. Becauseof the history of a fall some days preceding the onsetof fever and some degree of bulging of the fontanelle,bilateral taps were performed and effusions foundover both hemispheres.
TreatmentIn seven of the cases (five post-meningitic and two
'gastro-enteritic') the effusions responded to evacu-ation by repeated taps, some 8-15 ml. of fluid beingremoved on each occasion. As it happened, thefourth tap in each of these patients was dry and nofurther action was taken in view of the rapid clinicalrecovery.
Failure of the effusion to respond to this simplemeasure led to the performance of burr holes in22 patients. Fluid was evacuated and the brainand its coverings inspected. Membrane was seen inhalf of the infants submitted to this procedure. Intwo cases the membrane (unilateral) was thick,greenish and adherent to the arachnoid and wasremoved at subsequent craniotomy (the post-Haemophilus meningitis and the hydrocephalus casesrespectively). In the remaining nine cases themembrane was thin, whitish and applied only to theinner surface of the dura, but not adherent to thearachnoid. Craniotomy, although contemplated,
46copyright.
on 21 July 2018 by guest. Protected by
http://adc.bmj.com
/A
rch Dis C
hild: first published as 10.1136/adc.31.155.44 on 1 February 1956. D
ownloaded from
SUBDURAL EFFUSION IN INFANCY
was not carried out in the first place because of thevery poor general condition of these infants. How-ever, when it was seen that this minor procedure wasfollowed by a considerable change for the better,the more formidable intervention of craniotomy wasdeliberately withheld in subsequent cases where thiskind of poorly-developed membrane was found.In others visible brain damage seemed to preclude thenecessity for craniotomy for removal of membranewhich, not being applied to the brain, could pre-sumably not be causing such damage.
ResultsRepeated taps, from two to four in number,
sufficed to bring about apparent cure in fivemeningitis cases and in two enteritis-malnutritioncases. All six of the 22 submitted to burr holes,in whom no brain damage was seen (Group I and II
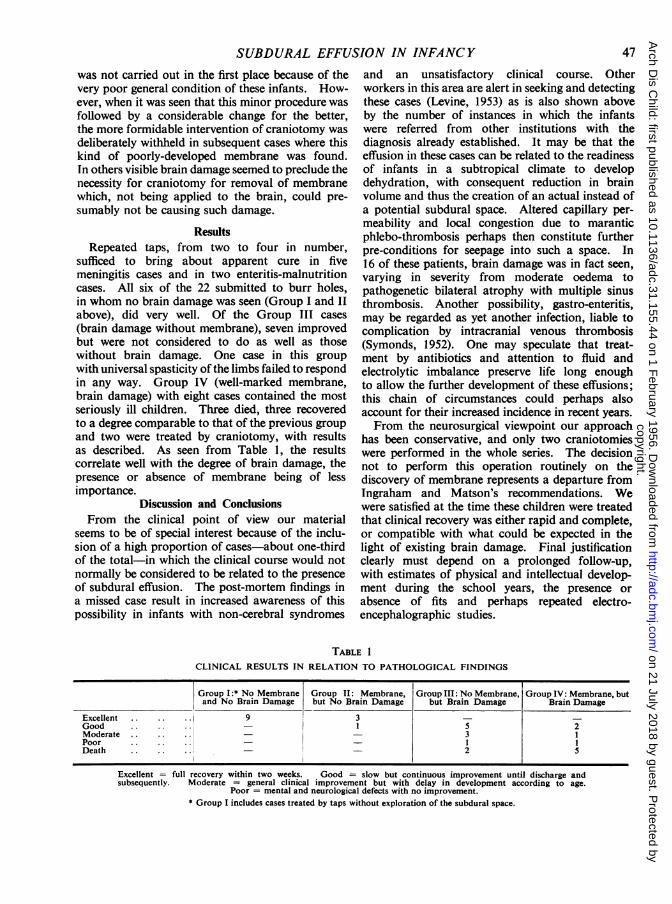
above), did very well. Of the Group III cases(brain damage without membrane), seven improvedbut were not considered to do as well as thosewithout brain damage. One case in this groupwith universal spasticity of the limbs failed to respondin any way. Group IV (well-marked membrane,brain damage) with eight cases contained the mostseriously ill children. Three died, three recoveredto a degree comparable to that of the previous groupand two were treated by craniotomy, with resultsas described. As seen from Table 1, the resultscorrelate well with the degree of brain damage, thepresence or absence of membrane being of lessimportance.
Discussion and ConclusionsFrom the clinical point of view our material
seems to be of special interest because of the inclu-sion of a high proportion of cases-about one-thirdof the total-in which the clinical course would notnormally be considered to be related to the presenceof subdural effusion. The post-mortem findings ina missed case result in increased awareness of thispossibility in infants with non-cerebral syndromes
and an unsatisfactory clinical course. Otherworkers in this area are alert in seeking and detectingthese cases (Levine, 1953) as is also shown aboveby the number of instances in which the infantswere referred from other institutions with thediagnosis already established. It may be that theeffusion in these cases can be related to the readinessof infants in a subtropical climate to developdehydration, with consequent reduction in brainvolume and thus the creation of an actual instead ofa potential subdural space. Altered capillary per-meability and local congestion due to maranticphlebo-thrombosis perhaps then constitute furtherpre-conditions for seepage into such a space. In16 of these patients, brain damage was in fact seen,varying in severity from moderate oedema topathogenetic bilateral atrophy with multiple sinusthrombosis. Another possibility, gastro-enteritis,may be regarded as yet another infection, liable tocomplication by intracranial venous thrombosis(Symonds, 1952). One may speculate that treat-ment by antibiotics and attention to fluid andelectrolytic imbalance preserve life long enoughto allow the further development of these effusions;this chain of circumstances could perhaps alsoaccount for their increased incidence in recent years.From the neurosurgical viewpoint our approach
has been conservative, and only two craniotomieswere performed in the whole series. The decisionnot to perform this operation routinely on thediscovery of membrane represents a departure fromIngraham and Matson's recommendations. Wewere satisfied at the time these children were treatedthat clinical recovery was either rapid and complete,or compatible with what could be expected in thelight of existing brain damage. Final justificationclearly must depend on a prolonged follow-up,with estimates of physical and intellectual develop-ment during the school years, the presence orabsence of fits and perhaps repeated electro-encephalographic studies.
LE 1
CLINICAL RESULTS IN RELATION TO PATHOLOGICAL FINDINGS
Group I:* No Membrane Group II: Membrane, Group III: No Membrane, Group IV: Membrane, butand No Brain Damage but No Brain Damage but Brain Damage Brain Damage
Excellent .i 9 3 _Good 1 5 2Moderate 3 1Poor .1Death 2 5
Excellent full recovery within two weeks. Good = slow but continuous improvement until discharge andsubsequently. Moderate = general clinical improvement but with delay in development according to age.
Poor = mental and neurological defects with no improvement.* Group I includes cases treated by taps without exploration of the subdural space.
47
copyright. on 21 July 2018 by guest. P
rotected byhttp://adc.bm
j.com/
Arch D
is Child: first published as 10.1136/adc.31.155.44 on 1 F
ebruary 1956. Dow
nloaded from
TABLE
SUMMARY OF T
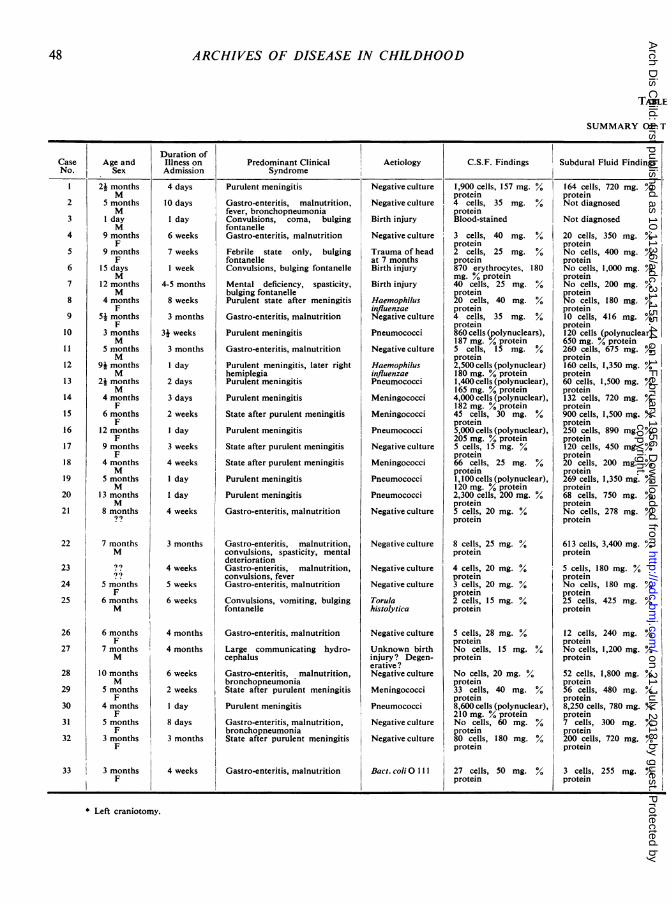
Duration ofCase Age and Illness on Predominant Clinical Aetiology C.S.F. Findings Subdural Fluid FindingsNo. Sex Admission Syndrome
Purulent meningitis
Gastro-enteritis, malnutrition,fever, bronchopneumoniaConvulsions, coma, bulgingfontanelleGastro-enteritis, malnutrition
Febrile state only, bulgingfontanelleConvulsions, bulging fontanelle
Mental deficiency, spasticity,bulging fontanellePurulent state after meningitis
Gastro-enteritis, malnutrition
Purulent meningitis
Gastro-enteritis, malnutrition
Purulent meningitis, later righthemiplegiaPurulent meningitis
Purulent meningitis
State after purulent meningitis
Purulent meningitis
State after purulent meningitis
State after purulent meningitis
Purulent meningitis
Purulent meningitis
Gastro-enteritis, malnutrition
Gastro-enteritis, malnutrition,convulsions, spasticity, mentaldeteriorationGastro-enteritis, malnutrition,convulsions, feverGastro-enteritis, malnutrition
Convulsions, vomiting, bulgingfontanelle
Gastro-enteritis, malnutrition
Large communicating hydro-cephalus
Gastro-enteritis, malnutrition,bronchopneumoniaState after purulent meningitis
Purulent meningitis
Gastro-enteritis, malnutrition,bronchopneumoniaState after purulent meningitis
Gastro-enteritis, malnutrition
Negative culture
Negative culture
Birth injury
Negative culture
Trauma of headat 7 monthsBirth injury
Birth injury
HaemophilusinfluenzaeNegative culture
Pneumococci
Negative culture
HaemophilusinfluenzaePneumococci
Meningococci
Meningococci
Pneumococci
Negative culture
Meningococci
Pneumococci
Pneumococci
Negative culture
Negative culture
Negative culture
Negative culture
Torulahistolytica
Negative culture
Unknown birthinjury? Degen-erative ?Negative culture
Meningococci
Pneumococci
Negative culture
Negative culture
Bact. coliO 111
1,900 cells, 157 mg. %protein4 cells, 35 mg.proteinBlood-stained
3 cells, 40 mg. %protein2 cells, 25 mg. %protein870 erythrocytes, 180mg. % protein40 cells, 25 mg. %protein20 cells, 40 mg. %protein4 cells, 35 mg. %protein860 cells (polynuclears),187 mg. % protein5 cells, 15 mg. %protein2,500 cells (polynuclear)180 mg. °0 protein1,400 cells (polynuclear),165 mg. % protein4,000 cells (polynuclear),182 mg. % protein45 cells, 30 mg. %protein5,000 cells (polynuclear),205 mg. °0 protein5 cells, 15 mg. %protein66 cells, 25 mg. %protein1,100 cells (polynuclear),120 mg. °0 protein2,300 cells, 200 mg. %protein5 cells, 20 mg. %protein
8 cells, 25 mg. %protein
4 cells, 20 mg. %protein3 cells, 20 mg. %protein2 cells, 15 mg.protein
5 cells, 28 mg. %proteinNo cells, 15 mg. %protein
No cells, 20 mg. %protein33 cells, 40 mg. %protein8,600 cells (polynuclear),210 mg. % proteinNo cells, 60 mg. %protein80 cells, 180 mg. %protein
27 cells, 50 mg. %protein
164 cells, 720 mg. %/oproteinNot diagnosed
Not diagnosed
20 cells, 350 mg. %proteinNo cells, 400 mg. %proteinNo cells, 1,000 mg. %proteinNo cells, 200 mg. %proteinNo cells, 180 mg. %protein10 cells, 416 mg. %protein120 cells (polynuclear)650 mg. % protein260 cells, 675 mg. %protein160 cells, 1,350 mg. %protein60 cells, 1,500 mg. %protein132 cells, 720 mg. %protein900 cells, 1,500 mg. %protein250 cells, 890 mg. %protein120 cells, 450 mg. %
protein20 cells, 200 mg. %protein269 cells, 1,350 mg. %protein68 cells, 750 mg. %proteinNo cells, 278 mg. %protein
613 cells, 3,400 mg. %protein
5 cells, 180 mg. %proteinNo cells, 180 mg. %protein25 cells, 425 mg. %protein
12 cells, 240 mg. %proteinNo cells, 1,200 mg. %protein
52 cells, 1,800 mg. %protein56 cells, 480 mg. %protein8,250 cells, 780 mg. %protein7 cells, 300 mg. %protein200 cells, 720 mg. %protein
3 cells, 255 mg. %protein
* Left craniotomy.
48 ARCHIVES OF DISEASE IN CHILDHOOD
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
24 monthsM
5 monthsM
1 dayM
9 monthsF
9 monthsF
15 daysM
12 monthsM
4 monthsF
5 monthsF
3 monthsM
5 monthsM
94 monthsM
24 monthsM
4 monthsF
6 monthsF
12 monthsF
9 monthsF
4 monthsM
5 monthsM
13 monthsM
8 months.99
7 monthsM99
5 monthsF
6 monthsM
6 monthsF
7 monthsM
10 monthsM
5 monthsF
4 monthsF
5 monthsF
3 monthsF
3 monthsF
4 days
10 days
I day
6 weeks
7 weeks
1 week
4-5 months
8 weeks
3 months
34 weeks
3 months
I day
2 days
3 days
2 weeks
I day
3 weeks
4 weeks
I day
I day
4 weeks
3 months
4 weeks
5 weeks
6 weeks
4 months
4 months
6 weeks
2 weeks
I day
8 days
3 months
4 weeks
copyright. on 21 July 2018 by guest. P
rotected byhttp://adc.bm
j.com/
Arch D
is Child: first published as 10.1136/adc.31.155.44 on 1 F
ebruary 1956. Dow
nloaded from
49SUBDURAL EFFUSION IN INFANCY
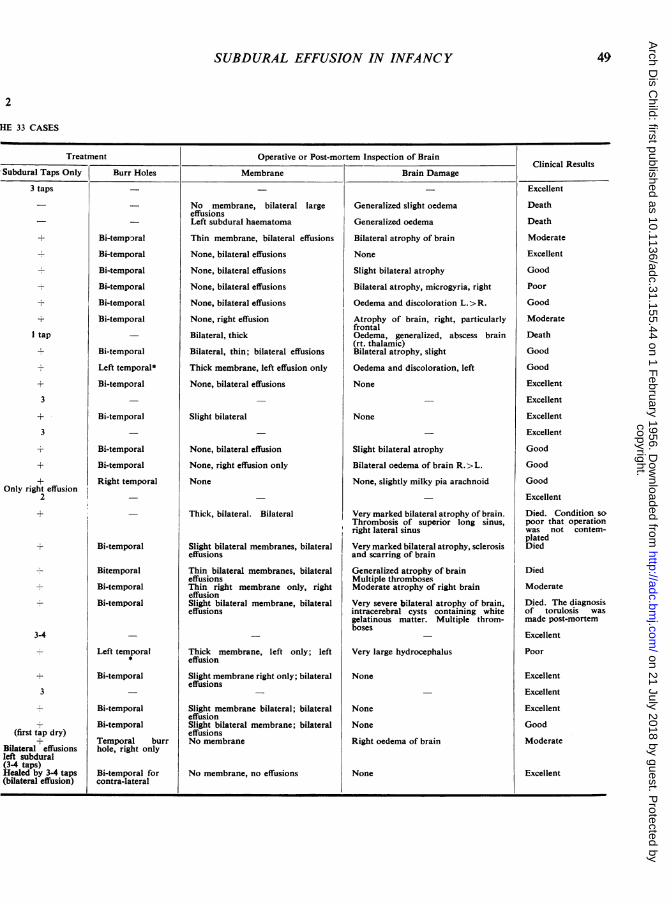
HE 33 CASES
Treatment Operative or Post-mortem Inspection of Brain__Subdural_Taps_Only BurrClinical ResultsSubdural Taps Only Burr Holes Membrane Brain Damage
3 taps
I tap
3
Only right effusion2
+
3-4
3
(first tap dry)
Bilateral effusionsleft subdural(34 taps)Healed by 34 taps(bilateral effusion)
Bi-temparal
Bi-temporal
Bi-temporal
Bi-temporal
Bi-temporal
Bi-temporal
Bi-temporal
Left temporal*
Bi-temporal
Bi-temporal
Bi-temporal
Bi-temporal
Right temporal
Bi-temporal
Bitemporal
Bi-temporal
Bi-temporal
Left temporal
Bi-temporal
Bi-temporal
Bi-temporal
Temporal burrhole, right only
Bi-temporal forcontra-lateral
No membrane, bilateral largeeffusionsLeft subdural haematoma
Thin membrane, bilateral effusions
None, bilateral effusions
None, bilateral effusions
None, bilateral effusions
None, bilateral effusions
None, right effusion
Bilateral, thick
Bilateral, thin; bilateral effusions
Thick membrane, left effusion only
None, bilateral effusions
Slight bilateral
None, bilateral effusion
None, right effusion only
None
Thick, bilateral. Bilateral
Slight bilateral membranes, bilateraleffusions
Thin bilateral membranes, bilateraleffusionsThin right membrane only, righteffusionSlight bilateral membrane, bilateraleffusions
Thick membrane, left only; lefteffusion
Slight membrane right only; bilateraleffusions
Slight membrane bilateral; bilateraleffusionSlight bilateral membrane; bilateraleffusionsNo membrane
Generalized slight oedema
Generalized oedema
Bilateral atrophy of brain
None
Slight bilateral atrophyBilateral atrophy, microgyria, right
Oedema and discoloration L.>R.
Atrophy of brain, right, particularlyfrontalOedema, generalized, abscess brain(rt. thalamic)Bilateral atrophy, slight
Oedema and discoloration, left
None
None
Slight bilateral atrophy
Bilateral oedema of brain R. >L.
None, slightly milky pia arachnoid
Very marked bilateral atrophy of brain.Thrombosis of superior long sinus,right lateral sinus
Very marked bilateral atrophy, sclerosisand scarring of brain
Generalized atrophy of brainMultiple thrombosesModerate atrophy of right brain
Very severe bilateral atrophy of brain,intracerebral cysts containing whitegelatinous matter. Multiple throm-boses
Very large hydrocephalus
None
None
None
Right oedema of brain
Excellent
Death
Death
Moderate
Excellent
Good
Poor
Good
Moderate
Death
Good
Good
Excellent
Excellent
Excellent
Excellent
Good
Good
Good
Excellent
Died. Condition sopoor that operationwas not contem-platedDied
Died
Moderate
Died. The diagnosisof torulosis wasmade post-mortem
Excellent
Poor
Excellent
Excellent
Excellent
Good
Moderate
No membrane, no effusions None Excellent
copyright. on 21 July 2018 by guest. P
rotected byhttp://adc.bm
j.com/
Arch D
is Child: first published as 10.1136/adc.31.155.44 on 1 F
ebruary 1956. Dow
nloaded from

50 ARCHIVES OF DISEASE IN CHILDHOOD
Summary
A series of 33 cases of subdural effusion in infancyis presented. In four only was there a reasonablecertainty of a traumatic aetiology; 15 followedpurulent meningitis and in 12 the effusion appearedin the course of a general illness with gastro-enteritis, malnutrition and bronchopneumonia.
Neurosurgical intervention was limited to burrholes in 22 cases; craniotomy for removal of themembrane was performed on two occasions only.The immediate results of such conservative
management were considered to justify withholding
major surgery, though final opinion must wait upona long follow-up.
It is a pleasure to acknowledge the cooperation of thepaediatricians of the 'A' and 'B' Paediatric Departmentsof the Tel-Hashomer Hospital.We are also much indebted to the physicians in charge
of the Paediatric Departments of the Assaf Harofe(Sarafand), Zahalon (Jaffa), Rambam (Haifa), Schweitzer(Tiberias) and Hadassah (Tel-Aviv) Hospitals whoreferred many of the cases.
REFERENCESGuthkelch, A. N. (1953). Brit. med. J., 1, 233.Ingraham, F. D. and Matson, D. D. (1954). Neurosurgery of
Infancy and Childhood, 456 pp. Springfield, Illinois.Levine, S. (1953). Personal communication.Symonds, C. P. (1952). Ann. roy. Coll. Surg. EngI., 10, 347. Quoted
by Guthkelch.
copyright. on 21 July 2018 by guest. P
rotected byhttp://adc.bm
j.com/
Arch D
is Child: first published as 10.1136/adc.31.155.44 on 1 F
ebruary 1956. Dow
nloaded from








![Management of subdural effusion and hydrocephalus ......hydrocephalus in patients with DC for TBI is 10 to 40% [10, 12, 13, 19]. SDE is defined as cerebrospinal fluid (CSF) accumula-tion](https://img.pdfslide.net/doc/110x75/60f77946a97a3c60fd2cc41f/management-of-subdural-effusion-and-hydrocephalus-hydrocephalus-in-patients.jpg)




















