Embed Size (px)
Citation preview

RS
Rtifttdmqb
ptiesilstpbt
D
A
1d
enal Biopsy of Dogs and Catshelly L. Vaden, DVM, PhD, Diplomate ACVIM
Renal diseases are common in dogs and cats. Renal biopsy may be required during theevaluation of the patient to establish a definitive diagnosis, determine the severity of thelesion and formulate an optimal treatment plan. Renal biopsy specimens can be collectedvia several methods. Percutaneous techniques are performed with ultrasound guidance inboth dogs and cats or blindly in cats. If ultrasound guidance is not available, the keyholetechnique can be used in dogs. Biopsy can also be performed using laparoscopy orsurgery. While complications can arise with any of these techniques, complications areless frequent when an experienced operator uses proper technique. Renal biopsy speci-mens must be processed and evaluated appropriately if consistent and accurate diagnosesare to be rendered. The article summarizes patient selection and evaluation, renal biopsytechniques, expected complications of renal biopsy, and appropriate processing and eval-uation of the renal biopsy specimen.Clin Tech Small Anim Pract 20:11-22 © 2005 Elsevier Inc. All rights reserved.
KEYWORDS renal biopsy, kidney biopsy, percutaneous kidney biopsy, laparoscopic kidneybiopsy, surgical kidney biopsy, complications of renal biopsy, light microscopy, electronmicroscopy
dspurt
PRadmbnteitl
dellendf
enal diseases are common in dogs and cats. Historicalinformation, physical examination and clinical labora-
ory data often allow for the differentiation of renal diseasesnto the general categories of acute renal failure, chronic renalailure, and glomerular disease. However, renal biopsy is of-en required to establish a definitive diagnosis and determinehe severity of the lesion. A precise and accurate histologiciagnosis may also be needed to formulate an optimal treat-ent plan. Accurate assessment of response to therapy re-
uires knowledge of both the type and severity of the diseaseeing treated.1-4
There is often reluctance on the part of the practitioner toursue renal biopsy in the clinical evaluation of their pa-ients. Many concerns probably contribute to this reluctance,ncluding the potential complications of renal biopsy, thexpenses associated with procurement of the renal biopsypecimen, and adequate evaluation of the renal biopsy spec-men as well as the belief that the rendered diagnoses mayack consistency. Studies have shown that the frequency ofevere complications from renal biopsy is relatively low andhat renal biopsy minimally affects renal function whenroper technique is employed.1,2,5-11 The expense of the renaliopsy procedure can be minimized by correct patient selec-ion and the use of proper technique. Consistent and accurate
epartment of Clinical Sciences, College of Veterinary Medicine, NorthCarolina State University, Raleigh, North Carolina.
ddress reprint requests to Dr. Shelly L. Vaden, Professor, Internal Medi-cine, Department of Clinical Sciences, College of Veterinary Medicine,North Carolina State University, 4700 Hillsborough St., Raleigh, NC
a27606. E-mail: [email protected]
096-2867/05/$-see front matter © 2005 Elsevier Inc. All rights reserved.oi:10.1053/j.ctsap.2004.12.003
iagnoses are more likely to be obtained when renal biopsypecimens are appropriately processed and evaluated. Theurpose of this article is to discuss patient selection and eval-ation, renal biopsy techniques, expected complications ofenal biopsy, and appropriate processing and evaluation ofhe renal biopsy specimen.
atient Selectionenal biopsy is indicated only when the results are likely tolter patient management by providing an accurate histologiciagnosis or by facilitating prognostication. Patients whoseanagement is most likely to be altered by results of a renal
iopsy include those with glomerular disease (protein losingephropathy) or acute renal failure (Table 1). Client factorshat also need to be considered include the ability to incur thexpense of the procedure and proper evaluation of the spec-men as well as their desire to pursue additional treatment ofheir dog or cat, as may be indicated once an accurate histo-ogic diagnosis is rendered.
Renal biopsy provides a definitive diagnosis of glomerularisease but may not be needed if a potential underlying dis-ase is identified and treatment of this disease leads to reso-ution of proteinuria. Likewise, a definitive diagnosis is un-ikely to be of benefit to the patient with glomerular disease ifnd stage renal disease is already present. In patients that doot have end stage renal disease, clinical decisions regardingiagnosis, therapy, and prognosis can be made from the in-ormation obtained through renal biopsy. In fact, obtaining
n accurate histologic diagnosis may be one of the more11

iwtmc
romotftwmtret
owrmocp
CBBpticctucosleihpp
tHa
wdorsd�trdicowabwprcn
tpsdoSbwiccaivifytksrcIr
PRR
T
P
Aterior
12 S.L. Vaden
mportant factors in successful management of the dog or catith glomerular disease. In most cases, appropriate evalua-
ion of a renal biopsy specimen from a dog or cat with glo-erular disease includes light, electron and immunofluores-
ent microscopy.Renal biopsy is indicated in the dog or cat that has acute
enal failure that is either persistently severe (ie, persistentliguria or uremia) or has deteriorated despite appropriateedical management. In these patients, determining an eti-
logic diagnosis may lead to additional therapeutic measureshat are specific for the primary disease. Renal biopsy can alsoacilitate prognostication in patients with acute renal failurehrough assessment of the overall appearance of the tissue asell as determination of the integrity of the tubular basementembrane. Light microscopy may be all that is required in
he evaluation of a biopsy specimen from a patient with acuteenal failure but renal tissue should also be collected forlectron and immunofluorescent microscopy in the eventhat a glomerular disease is causing the acute renal failure.
Renal biopsy is unlikely to alter the prognosis, therapy orutcome of a patient with chronic renal failure. For patientsith end stage renal disease, it is unlikely that the cause of the
enal disease will be determined by renal biopsy. Further-ore, studies in people undergoing renal biopsy have dem-
nstrated an increased risk of complication in patients withhronic renal failure.12 For these reasons, renal biopsy ofatients with chronic renal failure is generally not indicated.
onsiderationsefore Renal Biopsy
efore renal biopsy, it is generally recommended that theatient be thoroughly evaluated by obtaining a current his-ory, performing a complete physical examination, measur-ng systemic blood pressure, and analyzing results of a bio-hemical profile, complete blood count, urinalysis, andoagulation profile. These are performed not only to assesshe current state of health and suitability of the patient tondergo renal biopsy but also to verify that there are noontraindications to biopsy. Contraindications to renal bi-psy include the presence of an uncorrectable coagulopathy,evere anemia, hydronephrosis, uncontrolled hypertension,arge or multiple renal cysts, perirenal abscess, extensive py-lonephritis, and end stage renal disease. Some authors havencluded a solitary kidney as a contraindication to biopsy;owever, biopsy of a solitary kidney may be performed ifroper technique is used and other contraindications are notresent.To identify patients with bleeding tendencies, a coagula-
ion profile is generally recommended before renal biopsy.owever, studies in people have demonstrated that preoper-
able 1 Indications for Renal Biopsy
rotein losing nephropathy Identify and treat potentialLow yield in patients with eAppropriate evaluation may
cute renal failure Consider in patients with pConsider in patients that de
tive coagulation profiles are not only unnecessary in patients n
ithout an obvious tendency to bleed but abnormal resultso not correlate with bleeding after percutaneous liver biopsyr general surgery.13,14 Contrary to these findings, a recenteport demonstrated that dogs and cats with moderate toevere thrombocytopenia (platelet counts �80,000/uL),ogs with prolonged one-stage prothrombin time (OSPT1.5� normal) and cats with prolonged activated partial
hromboplastin time (APTT �1.5� normal) had a greaterisk of hemorrhage from ultrasound-guided biopsy proce-ures.15 Other patient factors that may be associated with an
ncreased risk of hemorrhage include severe azotemia (serumreatinine �5 mg/dL), uncontrolled systemic hypertensionr administration of a nonsteroidal anti-inflammatory drugsithin the previous 5 days.12,16-18 However, these patient
bnormalities may not be absolute contraindications to renaliopsy. Rather, when renal biopsy is planned for patientsith identified bleeding tendencies, the clinician should berepared to monitor the patient for severe perirenal hemor-hage postbiopsy and have suitable blood products from aompatible donor available to administer to the patient ifeeded.Abdominal ultrasound is generally performed as part of
he initial evaluation in patients with acute renal failure orrotein losing nephropathy. In addition to assessing the size,hape, contour, and internal architecture of the kidney, ab-ominal ultrasound also allows for the identification of manyf the previously listed contraindications to renal biopsy.evere hydronephrosis is a contraindication to renal biopsyecause of concern of penetrating the distended renal pelvishich is likely to be under increased pressure as well as the
ncreased risk of transecting the larger arteries located in theorticomedullary junction and the medulla. Rupture of renalysts and release of their contents into perirenal tissues isssociated with pain in people. Although the risk of inducingnfection through renal biopsy is low, cyst infections may beery difficult to treat because of poor antibiotic penetrationnto the cyst fluid. Concern over inducing renal pain or in-ection via biopsy of renal cysts and the limited diagnosticield of a biopsy specimen which contains large cysts has ledo the recommendation that renal biopsy not be performed inidneys that contain large or multiple cysts. Perirenal absces-ation and extensive pyelonephritis are contraindications toenal biopsy because of the possibility that the abdomenould become seeded with bacteria or other infectious agents.deally, urinary tract infections should be eliminated beforeenal biopsy.
rocurement of theenal Biopsy Specimen
enal biopsies can be obtained using one of several tech-
ying diseases before biopsy.ge renal disease.
re light and electron microscopy and immunology staining.ntly severe uremia or oliguria.ate during appropriate medical management.
underlnd starequi
ersiste
iques (Table 2). Regardless of the method selected, only

cmsmsBistswtrcdmidifi
PPFtatoip
biab
NAbctrtnrl
nPdacDiwtttf
lMo
Fuu
T
P
S
oing la
F
Renal biopsy of dogs and cats 13
ortical tissue should be obtained. Most diagnoses can beade through evaluation of cortical tissue alone. The risk of
erious hemorrhage may increase as the kidney is penetratedore deeply because renal vessels progressively increase in
ize from the surface of the kidney toward the renal pelvis.iopsy of the renal medulla may also be associated with an
ncreased risk of creating large areas of infarction and fibro-is.19,20 Whenever possible, the biopsy is taken from eitherhe cranial or caudal pole of the kidney because it is easier totay in cortical tissue over a larger portion of the kidneyithin the poles. In the dog with generalized renal disease,
he right kidney is often preferred over the left kidney forenal biopsy. The right kidney is more stable because theaudate lobe of the liver provides resistance to movementuring the biopsy procedure. Conversely, the left kidney isore movable during the biopsy procedure but can be found
n a more caudal position, providing easier access in someeep chested dogs. Feline kidneys are located more caudally
n the abdomen when compared with canine kidneys. Botheline kidneys can be easily localized and immobilized mak-ng both equally suitable for renal biopsy.
atient Sedation or Anesthesiaroper biopsy technique requires patient immobilization.ailure to immobilize the patient may increase the likelihoodhat serious complications will develop after renal biopsy. Inddition, providing general anesthesia to the patient duringhe biopsy procedure has been associated with procurementf a quality biopsy specimen.17 Although general anesthesias most likely to produce complete immobilization of theatient, some patients who are very ill may be immobilized
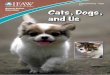
igure 1 Disposable spring-loaded biopsy instrument that can besed for renal biopsy (E-Z Core Single Action Biopsy Devise, Prod-
able 2 Methods used to Obtain Renal Biopsy Specimens
ercutaneousBlind or palpation technique Better suited for catLaparoscopic biopsy Requires specializedKeyhole technique Used in dogs if ultraUltrasound guidance Preferred method fo
urgicalWedge biopsy Preferred method fo
or animals underg
cts group International, Inc., Lyons, CO). u
y sedatives alone. Incomplete anesthesia of the peritoneums a disadvantage of using only sedation and local anesthesiand can result in sudden abdominal movement during theiopsy procedure.5
eedle Selectionvariety of needles are available for percutaneous kidney
iopsy. The Tru-cut biopsy needle was once the needle ofhoice, largely because other options were limited. However,hese needles can be difficult to use. Improper technique canesult in poor quality biopsy specimens and inadvertentrauma to the kidney. With the availability of spring-loadedeedles and biopsy guns, the Tru-cut cannot be routinelyecommended. Likewise, the Vim-Silverman needle is noonger routinely used for renal biopsy.
We prefer disposable spring-loaded biopsy needles for re-al biopsy (Fig. 1) (E-Z Core Single Action Biopsy Devise,roducts group International, Inc., Lyons, CO). These nee-les can easily be operated using only 1 hand and are avail-ble in 14, 16, 18, and 20 gauge with lengths of 6, 9, or 15m. An advantage of this needle lies in the throw mechanism.uring biopsy, the spring-loaded stylet is advanced first and
s visible by ultrasound. The cutting cannula is activatedhen the operator fully depresses the plunger with their
humb. The biopsy instrument does not move deeper into theissue during activation of the cannula. The biopsy needle canhen be removed from the animal and the specimen retrievedrom the specimen notch.
Alternatively, some institutions use automatic spring-oaded biopsy guns (Fig. 2) (eg, Bard Biopty, C. R. Bard, Inc.,
urray Hill, NJ) that can be loaded with disposable needlesf appropriate gauges and lengths that are available from a
dogsment and expertiseguidance not available>5 kg and all cats
<5 kg, animals with isolated areas of the kidney to avoid,parotomy for another reason.
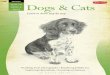
igure 2 Automatic spring-loaded biopsy gun and needle that can be
s thanequip
soundr dogs
r dogs
sed for renal biopsy (Bard Biopty, C. R. Bard, Inc., Murray Hill, NJ).

vscagoobytmn
fns
dntt
PuPbltssrbfprlisn
tessnpnaatiWfsofRta
psoma
KTgrscpbltlila
Forpe
F
14 S.L. Vaden
ariety of manufacturers. We have found that the weight andize of the gun can render the use of these more difficult whenompared with the spring-loaded biopsy needles. The oper-tor needs to have large and strong hands to easily use theun single handedly. These guns may be less suitable forbtaining kidney biopsies when compared with biopsy ofther organs because of the limited control of the depth ofiopsy. Activation of the needle causes the throw to go be-ond where the tip of the needle is placed at the beginning ofhe procedure. This is a potential source of operator error anday be associated with an increased risk of penetration of theeedle into the medulla.We use either a 16 or 18 gauge needle that is 9 cm in length
or our kidney biopsies. In 1 study, use of a 14-gauge biopsyeedle was associated with a greater likelihood that biopsypecimens contained medulla.17
Obtaining a good quality biopsy specimen with limitedamage to the kidney requires the use of a sharp biopsyeedle. Because needles become dull after several biopsies areaken and the needles are relatively inexpensive, reuse ofhese disposable needles is not generally recommended.
ercutaneous Biopsysing Ultrasound Guidanceercutaneous renal biopsy using ultrasound guidance hasecome the renal biopsy method of choice for dogs that are
arger than 5 kg and for all cats that do not have other con-raindications for renal biopsy.7 With this technique, ultra-ound is used to identify and examine the kidneys and sub-equently guide correct placement of the needle. The normalenal cortex can easily be differentiated from the medullaecause of the relative hyperechogenicity of the cortex; dif-erentiation may be more difficult in diseased kidneys. Theatient is placed in left lateral recumbency for biopsy of theight kidney or in right lateral recumbency for biopsy of theeft kidney. The hair over the biopsy site is removed, the skins aseptically prepared and sterile coupling gel is applied. Aterile sleeve is placed over the ultrasound probe. The kid-
igure 3 Schematic demonstrating the correct and incorrect methodf directing the renal biopsy needle. Note that the needle shouldemain in the renal cortex, preferably in either the cranial or caudalole. The needle should not cross the corticomedulary junction nornter either the renal medulla or pelvis.
eys are scanned for general examination of the renal archi- p
ectures and for selection of the biopsy site. Once the site ofntry for the biopsy needle is determined, a small stab inci-ion is made through the skin, allowing for the needle to stayharp as it easily passes through the skin. The tip of theeedle is guided to the renal capsule with 1 hand while therobe is held with the other (Figs. 3 and 4). The tip of theeedle should be placed through the renal capsule beforectivation to prevent sliding of the needle along the capsulend avoid tearing the capsule. The biopsy is then taken usinghe method that is appropriate for the selected needle, mak-ng sure that the needles remains in the renal cortex (Fig. 5).
hen using a percutaneous method to obtain a renal biopsyrom a patient with glomerular disease, at least 2 qualityamples of renal cortex should be obtained using either a 16r 18 g needle; 1 cortical biopsy may be all that is requiredrom a patient with acute renal failure (see Evaluation theenal Biopsy Specimen). Digital pressure should be applied
o the kidney transabdominally for approximately 5 minutesfter biopsy to minimize hemorrhage.
Although needle guides are available for the ultrasoundrobe, we do not generally use these. The guides are probepecific and are not available for all probes. The requirementf specific computer software for operation of the guidesakes their usage rather expensive. In addition, some oper-
tors find that the guides are confining.
eyhole Techniquehe keyhole technique can be used in dogs if ultrasounduidance is not available.21,22 The dog is placed in left lateralecumbency for biopsy of the right kidney. The dog’s backhould be facing the surgeon. The hair in the lumbar fossa islipped and the skin is aseptically prepared. An oblique,aralumbar 7.5 to 10 cm skin incision is made on a line thatisects the angle between the last rib and the edge of the
umbar musculature (Fig. 6). It may be impossible to palpatehe kidney if the incision is made too far caudal or ventral. Aarge, vascular muscle mass will need to be dissected if thencision is made too far dorsal. Too cranial of an incision mayead to puncture of the intercostal artery. The muscle fibersre separated along muscle planes and the peritoneum is
igure 4 Ultrasound guided renal biopsy in a dog. Note that the
robe is held in 1 hand while the needle is held in the other hand.
ilcaisttmttannqbt
cttp
eHqn
BPdkiqmlbctkt
lTishiksmtnbtiar
LLut
Fi
Foo
Fm(
Renal biopsy of dogs and cats 15
ncised. The peritoneal incision must be large enough to al-ow for easy insertion of the surgeon’s index finger over theaudal pole of the kidney. The index finger holds the kidneygainst the edge of the lumbar musculature. The other handnserts the biopsy needle through a separate small stab inci-ion in the lateral body wall. The biopsy needle is guided intohe peritoneal cavity and the tip of the needle is positioned athe surface of the kidney or stabbed just through the capsuleaking sure the angle is such that the needle will pass only
hrough renal cortex. Care should be taken not to penetrateoo deeply beyond the renal capsule as this will reduce themount of renal cortex in the biopsy specimen. Activate theeedle cutting mechanism as appropriate for the selectedeedle. Additional biopsy specimens can be obtained, as re-uired. After the needle is withdrawn, digital pressure shoulde placed for at least 5 minutes where the needle penetratedhe kidney to minimize hemorrhage.
Use of the keyhole technique has been associated with thereation of artifact in the biopsy sample, possibly because ofhe frequent need to displace the kidney a considerable dis-ance before biopsy. Such artifact includes congestion of theeritubular and glomerular capillaries and extravasation of
igure 5 The ultrasonographic image of the dog in Fig. 4. This images used to guide the needle to the kidney and through the cortex.
igure 6 Making the incision for insertion of a finger for percutane-us renal biopsy in the dog using the keyhole technique. (Courtesy
nf J. A. Barsanti, Athens, GA.)
rythrocytes into the tubular lumina and Bowman’s space.owever, in 1 study there were no differences in specimenuality between samples obtained with the keyhole tech-ique compared with those obtained by laparoscopy.10
lind or Palpation Techniqueerforming renal biopsy with guidance by palpation is rarelyone in dogs because of the more cranial location of theidneys and the fact that canine kidneys can be difficult to
mmobilize by palpation. However, blind biopsy is more fre-uently performed in feline kidneys, which are relativelyore caudal in position and can be more readily immobi-
ized. Nonetheless, we prefer ultrasound guidance for renaliopsies in cats because ultrasound affords the ability to con-urrently assess the renal architecture and establish that con-raindications to renal biopsy are not present (eg, polycysticidney disease) as well as guide the biopsy needle throughhe cortex.
Blind renal biopsy in cats is performed with the cat inateral recumbency. Either kidney is localized by palpation.he hair is clipped from the area over the kidney and the skin
s aseptically prepared. A small stab incision is made in thekin with a scalpel blade. The kidney is immobilized with 1and. The other hand advances the needle through the stab
ncision and directs it toward the cranial or caudal pole of theidney (Fig. 7). The tip of the needle is positioned at theurface of the kidney or stabbed just through the capsuleaking sure the angle is such that the needle will pass only
hrough renal cortex. Penetrating too deeply beyond the re-al capsule will reduce the amount of renal cortex in theiopsy specimen. The cutting mechanism of the needle ishen activated. Additional biopsy specimens can be obtained,f needed. Digital pressure should be applied to the kidney forpproximately 5 minutes after biopsy to minimize hemor-hage.
aparoscopic Biopsyaparoscopy is an endoscopic procedure that is performednder sterile conditions and allows for visual examination ofhe peritoneal cavity after establishment of a pneumoperito-
igure 7 Percutaneous kidney biopsy in the cat. The kidney is im-obilized by 1 hand while the other manipulates the biopsy needle.
Courtesy of J. A. Barsanti, Athens, GA.)
eum.1,23 Laparoscopy offers an advantage over the percuta-

nteihpnpaoneostacoteioEtodtt3t
liacnVfs
tasmo
SSstbrmsovasqb1atbltattpfitwi9wms
PIsdorkb2bficht
CAR
FTbft1
16 S.L. Vaden
eous biopsy techniques in that it allows for direct visualiza-ion and inspection of the kidneys through insertion of a rigidndoscope and permits visual control of the biopsy. Visual-zation of the kidneys before biopsy leads to a higher likeli-ood that diagnostic tissue will be obtained during biopsy,articularly if focal lesions are present. Because the abdomi-al incision is small, laparoscopy is less invasive and can beerformed more quickly than surgery, allowing for compar-tively less patient morbidity. Like surgery, other abdominalrgans can be inspected and biopsy specimens collected, ifecessary, during laparoscopy although complete abdominalxploration is not possible. As with surgery, postbiopsy hem-rrhage can be monitored during laparoscopy; direct pres-ure can be applied with the laparoscope or laparoscopicools if needed. Laparoscopy requires appropriate equipmentnd operator expertise. Contraindications to laparoscopy in-lude peritonitis, extensive abdominal adhesions, hernias,besity, coagulopathies, and operator inexperience.23 Poten-ial complications of laparoscopy include the creation of airmboli, pneumothorax, or subcutaneous emphysema, thentroduction of gas into a hollow viscus, damage to internalrgans with the Verres needle or trocar, and cardiac arrest.vacuation of the urinary bladder and colon before penetra-
ion into the abdomen will minimize the chance that thesergans are punctured. Operator experience and attention toetail, as well as the use of a surgically placed port instead ofhe Verres needle, may reduce the likelihood of complica-ions.23 In a study of laparoscopic renal biopsy performed in7 dogs and 1 cat, none of these complications were encoun-ered.
Laparoscopy can be performed through a right lateral, leftateral, or midline incision. The right kidney is readily visiblen dogs in left lateral recumbency (Fig. 8).1 To separate thebdominal wall from the organs, a pneumoperitoneum isreated via injection of carbon dioxide through the Verreseedle or a surgically placed trocar and cannula unit. If theerres needle technique is used, the trocar and cannula units
or the laparoscope are then inserted through a small (1 cm)
igure 8 Close-up laparoscopic view of the right kidney in a dog.he tip of a biopsy needle is in the field-of-view. Note that theiopsy needle is directed at a shallow angle to the capsule and awayrom the renal pelvis. From Grauer G, Laparoscopy of the urinaryract, in Tams TR (ed): Small Animal Endoscopy. St. Louis, Mosby,999, p 430.
kin incision. Once the assembly is in the abdomen, the r
rocar is removed from the cannula and replaced by the lap-roscope. The abdominal organs can be systematically in-pected. A biopsy needle can then be introduced into abdo-en through a separate site. The renal biopsy is taken while
bserving the procedure through the laparoscope.
urgical Biopsyurgical biopsy may be the preferred method in dogs that aremall (�5 kg) or in animals that either have isolated areas inhe kidney (eg, large cysts) that need to be avoided during theiopsy procedure or are undergoing laparotomy for anothereason. Likewise, surgical biopsy may be safer in some ani-als that have other listed contraindications to biopsy. A
urgical wedge biopsy is preferred over a surgical needle bi-psy. One has more control over the depth of biopsy and theolume of tissue collected when a wedge biopsy is obtaineds compared with a needle biopsy. It is not surprising thaturgical wedge biopsy were 5 times more likely to be of gooduality than were surgical needle biopsies.17 The surgicaliopsy can be obtained through a paracostal incision, if onlykidney is to be examined and biopsied, or a cranial midline
bdominal incision if other intra-abdominal procedures areo be performed or both kidneys need to be examined beforeiopsy.21 The paracostal incision is made with the patient in
ateral recumbency.24 The incision is parallel and 2 cm caudalo the last rib. The oblique muscles are divided between fibersnd retracted. The kidney is located after separating theransverse abdominal muscle. The kidney can be elevatedhrough the incision by placing umbilical tape around botholes. In obese animals, exposure of the kidney may be dif-cult through the paracostal incision. Following exposurehrough either type of incision, the kidney is immobilizedith thumb and forefinger before biopsy. A wedge shaped
ncision is made through the capsule and into the cortex (Fig.). Tissue forceps are used to gently lift the biopsy wedgehile the scalpel blade is used to sever any remaining attach-ents. Monofilament, absorbable suture material (4-0) in a
imple continuous pattern is used to close the renal capsule.
ostbiopsy Care of the Patientsotonic fluids should be given liberally intravenously foreveral hours after renal biopsy in amounts needed to pro-uce a diuresis. In theory, this will reduce the likelihood thatbstructing clots will form in the renal pelvis or ureter. Toeduce the risk of serious hemorrhage, the patient should beept relatively quiet and in the hospital for 24 hours afteriopsy. The patient’s packed cell volume should be evaluated4 hours after biopsy or sooner if a concern arises that majorleeding is occurring. Dogs should be walked only on a leashor 72 hours after biopsy. The color of urine should be mon-tored for several days after renal biopsy. Gross hematuria isommon after renal biopsy and usually resolves within 24ours. Persistent gross hematuria warrants re-evaluation ofhe kidneys and biopsy site.
omplicationsssociated with Renal Biopsy
esults of clinical studies indicate that complications after
enal biopsy are limited but vary in frequency from between
1rpfdpAdiari
bcstda
asc9lpiisubi
wapaa
FTtscapsTfiPfsl
Renal biopsy of dogs and cats 17
and 18% (Table 3).1,2,5-10,17 This variation in complicationate is almost certainly because of biopsy technique as well asatient status at the time of biopsy. In 1 retrospective study,
actors associated with the development of complications inogs included patient age �4 years, body weight �5 kg, andresence of severe azotemia (serum creatinine �5 mg/dL).17
hospital factor that appeared to be associated with theevelopment of complications was having a radiologist or
nternist perform the biopsy. This association may have beenresult of the use of percutaneous methods to collect the
enal biopsy or the use of sedation or injectable anesthesianstead of general anesthesia.
Microscopic hematuria is an expected finding after renaliopsy, developing in approximately 20 to 70% dogs andats.2,17 Microscopic hematuria is self-limiting, generally re-olving within 48 to 72 hours of biopsy. Macroscopic hema-uria is less common, developing in approximately 1 to 4% ofogs and cats after renal biopsy. Small perirenal hematomas
igure 9 Surgical kidney biopsy. (A)he kidney is immobilized between
humb and forefinger. A wedgehaped incision is made through theapsule and cortex. (B) Tissue forcepsre used to gently lift the biopsy sam-le. Any remaining attachments areevered with the scalpel blade. (C)he capsule is closed with 4-0 mono-lament absorbable suture material.ressure is applied with thumb andorefinger to appose the edges duringuturing. (Courtesy of E. A. Stone, Ra-eigh, NC).
re also common following renal biopsy if the kidney is ex- d
mined carefully by ultrasound. Severe hemorrhage, oftenevere enough to require blood transfusion, was the mostommon reported complication in 1 study, occurring in.9% of dogs and 16.9% of cats.17 In addition to the coagu-
ation abnormalities previously discussed, uncontrolled hy-ertension, uremia, the administration of nonsteroidal anti-
nflammatory drugs and the use of improper technique mayncrease the risk of serious hemorrhage.9,16,20 Hydronephro-is developing secondary to obstruction of the renal pelvis orreter by a blood clot is an uncommon complication of renaliopsy. Death is also an uncommon complication, occurring
n 3% or less of dogs and cats undergoing renal biopsy.9,17
Histologic changes in renal tissue after biopsy have beenell documented. Linear infarcts representing needle tracts
ssociated with varying amounts of atrophy and fibrosis ap-ear to be common after renal biopsy.25 Retention cysts canlso be found in association with the needle tract and prob-bly form secondary to tubular obstruction.25 Studies have
emonstrated correlations between severe renal parenchy-
mbttij
mierdoc
PRAumdepptsapspfbct(nimao
poi
stgHaHpatusaosbebtptrftruhImemnth
ERWtbafeealrucaclHhg
T
AB
CDH
HIIS
18 S.L. Vaden
al changes of hemorrhage, thrombosis, infarction, and fi-rosis and the presence of major renal vessels or medulla inhe biopsy specimen.19,20 These findings emphasize the needo direct the biopsy needle only through cortical tissue dur-ng the biopsy procedure, avoiding the corticomedullaryunction and medulla.
Despite histologic changes, renal biopsy appears to haveinimal effect on renal function.9,11 However, one could
magine that inflicting renal damage to an animal with pre-xisting renal disease could contribute to progressive loss ofenal function. Obtaining multiple biopsies of the kidneyoes not appear to produce more damage than biopsy withnly a single pass providing the biopsy needle remains inortical tissue.26
rocessing theenal Biopsy Specimen
n adequate sample of cortex has a minimum of 5 glomer-li when examined by light microscopy, although 1 glo-erulus may be all that is needed to make a definitive
iagnosis in generalized glomerular diseases. Microscopicxamination of each specimen using 10-fold magnificationrovides immediate verification that adequate biopsy sam-les have been obtained. Ideally this is performed with aransilluminating microscope but a standard light micro-cope can also be used. When 2 samples are obtained frompatient with glomerular disease, 1 sample should be
laced in formalin and the other should be divided into 2maller pieces containing glomeruli. One of the pieces isut into a fixative suitable for electron microscopy (eg, 4%
ormalin plus 1% glutaraldehyde in sodium phosphateuffer) and the other piece is frozen for immunofluores-ent microscopy. An alternative to freezing is to immersehe tissue in ammonium sulfate-N-ethylmaleimide fixativeie, Michel’s solution), which preserves tissue-fixed immu-oglobulins. Wedge biopsies should be divided in a sim-
lar fashion; tissue for electron microscopy should beinced appropriately. Although formalin fixation may be
ll that is required for adequate histopathologic evaluation
able 3 Reported Complications of Renal Biopsy
rteriovenous fistula formationiopsy of non-renal tissue (eg, liver, adrenal gland, fat,
muscle, connective tissue, spleen)yst formationeathemorrhageMicroscopic hematuriaMacroscopic hematuriaPerirenal hematomaIntrarenal hematomaLacerated renal artery or veinIntra-abdominal hemorrhage because of laceration of
other organ or vesselydronephrosis
nfarction and thrombosisnfectioncar formation and fibrosis
f specimens from patients with acute renal failure, sam- t
les should also be collected for electron and immunoflu-rescent microscopy in the event that a glomerular diseases causing the acute renal failure.
Thin sections (2-4 �m) of paraffin-embedded tissuehould be used for light microscopy because standard sec-ions of 5 to 6 �m are too thick for adequate assessment oflomerular cellularity and capillary loop thickness.27,28
ematoxylin and Eosin staining can be used for initialssessment of the general appearance of the specimen.owever, periodic acid-Schiff (PAS), which stains glyco-roteins, is the preferred stain of many nephropathologistsnd is particularly useful in the demonstration of intersti-ial and glomerular scarring and assessment of the glomer-lar basement membrane. Methenamine silver specificallytains the basement membrane of the tubules, glomerulind Bowman’s capsule. Trichrome is useful for evaluationf the mesangium and is also the best light microscopictain for visualization of immunoglobulins. Congo red cane used to demonstrate the presence of amyloid. Althoughlectron microscopy of renal biopsy specimens has noteen used frequently enough in dogs and cats to determinehe diagnostic merit in groups of patients with varyingresentations, it appears to be most helpful in the evalua-ion of people with renal hematuria, a familial history ofenal disease, or proteinuria with normal renal excretoryunction. However, a sample should be collected for elec-ron microscopy in nearly all dogs and cats undergoingenal biopsy because the exact diagnosis is most likelynknown. Immunofluorescent microscopy or immuno-istochemistry should include at a minimum stains forgM, IgG, IgA, and C3. Immunologic studies are becomingore readily available at a variety of laboratories. How-
ver, the requirement that samples from patients with glo-erular disease be evaluated by electron microscopy mayecessitate that samples from such patients be submittedo, and perhaps even collected at, a veterinary teachingospital.
valuating theenal Biopsy Specimenhenever possible, specimens should be evaluated by a pa-
hologist with expertise in nephropathology. Although renaliopsy specimens from dogs with acute renal failure may bedequately evaluated by light microscopy alone, specimensrom proteinuric dogs and cats should be evaluated by light,lectron, and immunofluorescent microscopy. Limiting thevaluation in these patients to light microscopy alone oftenllows for only a subjective interpretation of the glomerularesion with too much room for error. While there are manyeports describing glomerular lesions in dogs and cats, these of different nomenclature and different morphologicalriteria among pathologists sometimes makes interpretationsnd comparisons of the data difficult at best. A standardlassification system for the characterization of glomerularesions in dogs and cats needs to be embraced. The Worldealth Organization (WHO) criteria for the classification ofuman glomerulopathies have proven to be applicable tolomerular diseases in dogs.4 General acceptance of this sys-
em would lead to a better understanding of the natural his-
tg
ESTstogtsppbTTacc
epgatatlv
mmlsmM
warogumcTctptbwnpfbamcmjcFpfuAae(u
FN
Fads(p
Renal biopsy of dogs and cats 19
ory, pathogenesis, and response to treatment of the variouslomerular diseases in dogs and cats.
valuation of the Renal Biopsypecimen by Light Microscopyhe normal kidney is composed of glomeruli, tubules, inter-titium, and vasculature. The normal glomerulus contains 4o 8 lobules; each lobule is composed of capillaries supportedn a centrilobular core of mesangial matrix (Fig. 10).27,28 Thelomerular basement membrane is thin, delicate, PAS-posi-ive and argyrophilic (ie, capable of being impregnated withilver). The glomerular capillary lumen is normally widelyatent and lined with eosinophilic endothelial cell cyto-lasm. In any section, the glomeruli can appear of any sizeecause the glomeruli have been cut in different planes.here should only be 1 to 2 nuclei per mesangial cell region.he tubules normally have a thick basement membrane andre separated from each other by a fine interstitial stroma thatontains capillaries. The normal interstitium is relatively in-onspicuous.
The entire section should be evaluated under low power toxclude focal space occupying lesions (eg, granuloma, neo-lasia) and to evaluate the distribution of other lesions. Whenlomerular lesions are present and nearly all glomeruli areffected, the disorder is generalized. If less than one-half ofhe glomeruli are affected, the disorder is focal. When evalu-ting individual glomeruli, the pattern is diffuse or global ifhe entire glomerulus is affected. The lesion is segmental orocal if only a few lobules within affected glomeruli are in-olved.
In membranous glomerulopathy, the glomerular base-ent membrane appears uniformly thickened and appearsore rigid than normal (Fig. 11). Because the subepithe-
ial immune deposits do not become impregnated withilver, spikes may be identified on the outside of the glo-erular basement membrane when a silver stain is used.
igure 10 Normal glomerulus from a dog. Note the capillary lumensre widely patent and the capillary loops are thin, often appearingiscontinuous. Hypercellularity is not present. Used with permis-ion from Vaden SL, Glomerular disease, in Ettinger SJ, Feldman ECeds): Textbook of Veterinary Internal Medicine (ed 6). Philadel-hia, WB Saunders, 2005. © 2005 Elsevier Inc.
embranoproliferative glomerulonephritis is diagnosed h
hen there is a thickened glomerular basement membranend mesangial hypercellularity (�3 nuclei per mesangialegion) (Fig. 12). The glomerulus may become segmentedr lobular in appearance. Type I membranoproliferativelomerulonephritis, also called mesangiocapillary glomer-lonephritis, can have a “railroad” appearance to the glo-erular basement membrane when evaluated by light mi-
roscopy, and is often induced by infectious diseases.ype II membranoproliferative glomerulonephritis is alsoalled dense deposit disease and can be differentiated fromype I via electron microscopy. In people, the dense de-osits of type II membranoproliferative glomerulonephri-is are not believed to be immune deposits; type II mem-ranoproliferative glomerulonephritis is not associatedith infectious diseases. Mesangioproliferative glomerulo-ephritis may have several subcategories (eg, IgA ne-hropathy) and is characterized by focal segmental to dif-use global mesangial cell hyperplasia. Lupus nephritis cane associated with any glomerular abnormality and, whenctive, often has an interstitial infiltrate of mixed inflam-atory cells and acute damage to the tubules. Crescents
an loosely be defined as 2 or more layers of cells in Bow-an’s space and are suggestive of severe pathological in-
ury. Crescentic glomerulonephritis is diagnosed whenrescents are present in 50% or more of the glomeruli.ocal segmental glomerulosclerosis is diagnosed when theatient has proteinuria and glomerulosclerosis of only aew lobules within affected glomeruli and another glomer-lar lesion is not present to explain the sclerosis (Fig. 13).myloidosis is easy to diagnose by expansion of the mes-ngium and glomerular basement membrane by acellular,osinophilic staining material that stains red by Congo redFig. 14). Amyloid deposits are birefringent when viewednder polarized light.Tubular atrophy appears as irregular tubular basement
igure 11 Glomerulus from a dog with membranous nephropathy.ote the thickened, rigid appearing capillary loops and the lack of
ypercellularity (Courtesy of JL Robertson).
mgtfibcwpaeEr
ESPcarspralslemm9o
cpretrotmivdWfbl
FslamV2
FsapmP
Ftp
20 S.L. Vaden
embrane thickening and luminal collapse and may sug-est long-standing disease or a normal aging process. Theubules may be more widely separated than normal withbrous tissue and lymphocytes present between the tu-ules. Hyaline droplets or protein reabsorption dropletsan sometimes be seen in the renal tubular cells of patientsith proteinuria. The tubules should be examined forresence of casts, and foci of degeneration, regeneration,nd necrosis. The interstitium should be examined fordema, fibrosis, inflammation, or combinations of these.xpansion of the interstitium may occur with tubular at-ophy, edema, inflammatory infiltration, or fibrosis.
igure 12 Glomerulus from a dog with membranoproliferative (me-angiocapillary) glomerulonephritis. Note the thickened capillaryoops and the mesangial hypercellularity resulting in the segmentednd lobular appearance. Used with permission from Vaden SL, Glo-erular disease, in Ettinger SJ, Feldman EC (eds): Textbook ofeterinary Internal Medicine (ed 6). Philadelphia, WB Saunders,005. © 2005 Elsevier Inc.
igure 13 A glomerulus from a dog with a lesion resembling focalegmental glomerulosclerosis. Note the relatively normal appear-nce of the glomerular sections that are not sclerotic. Used withermission from Vaden SL, Glomerular disease, in Ettinger SJ, Feld-an EC (eds): Textbook of Veterinary Internal Medicine (ed 6).
mhiladelphia, WB Saunders, 2005. © 2005 Elsevier Inc.
valuation of the Renal Biopsypecimen by Electron Microscopyarietal epithelial cells, visceral epithelial cells, endothelialells, and mesangial cells comprise the normal glomerulusnd can easily be identified by electron microscopy. The pa-ietal epithelial cells are flattened cells that line the innerurface of Bowman’s capsule. The visceral epithelial cells, orodocytes, line the outer surface of the capillary loops andest on the glomerular basement membrane. The podocytesre characterized by foot processes and form the outermostayer of the capillary wall. The endothelial cells line the innerurface of the capillary loops with the nuclei disposed centri-obularly, toward the mesangium. The fenestrations of thendothelial cell cytoplasm can be visualized easily. The nor-al glomerular basement membrane should be approxi-ately the same thickness as the base of a foot process turned
0°. The mesangial matrix contains an interwoven networkf microfilaments.Minimal change disease is diagnosed when minimal
hanges are visualized via light microscopy (ie, slight hy-ercellularity as evident by 3-4 nuclei in the mesangialegion) and marked foot process effacement is noted vialectron microscopy (Fig. 15). Membranous glomerulopa-hy has 4 ultrastructural stages that correlate with tempo-al evolution of the disease and may predict therapeuticutcome; electron microscopy can be used to stage pa-ients with membranous nephropathy (Fig. 16). Electronicroscopy can also be used to identify the dense deposits
n type II membranoproliferative glomerulonephritis anderify the presence of electron dense, presumably immuneeposits in other patients with glomerulonephritis.hereas veterinarians have classically been taught to look
or these deposits within the glomerular basement mem-rane, in dogs with glomerulonephritis these deposits are
ocated more frequently within the mesangium. The glo-
igure 14 A glomerulus from a dog with segmental amyloid deposi-ion. Note the homogenously staining, acellular material that is ex-anding the mesangium.
erular basement membrane varies in thickness and is

sn
EbTosetlopgteo
FdpetElsevier Inc.
Fpp
Renal biopsy of dogs and cats 21
plit into a number of layers in patients with hereditaryephritis.27
valuation of the Renal Biopsy Specimeny Immunofluorescent Microscopyhe normal kidney should not have positive immunoflu-rescent or immunohistochemical staining. However,taining is positive in animals with immune-mediated dis-ase where there is either in situ immune complex forma-ion, as is believed to occur with membranous glomeru-opathy, or deposition of circulating complexes, as mayccur with type I membranoproliferative glomerulone-hritis. Because true antiglomerular basement membranelomerulonephritis has not been documented in the dog,he expected staining pattern is discontinuous occurringither in the capillary loops, giving a circular appearance,r in the mesangium.
igure 15 Electron micrograph of a glomerular capillary loop in aog with minimal change disease. There is effacement of the footrocesses. Used with permission from Vaden SL, Glomerular dis-ase, in Ettinger SJ, Feldman EC (eds): Textbook of Veterinary In-ernal Medicine (ed 6). Philadelphia, WB Saunders, 2005. © 2005
igure 16 Ultrastructural stages in therogression of membranous ne-hropathy. (Courtesy of JC Jennette).

SRdRettdidmlqli
ATfV
R
1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
2
2
2
22 S.L. Vaden
ummaryenal biopsy most often is indicated in the management ofogs and cats with glomerular disease or acute renal failure.enal biopsy can readily be performed in dogs and cats viaither percutaneous or surgical methods. Care should beaken to ensure that proper technique is used. When properechnique is employed and patient factors are properly ad-ressed, renal biopsy is a relatively safe procedure that min-
mally affects renal function. Patients should be monitoreduring the postbiopsy period for severe hemorrhage, theost common complication. Accurate diagnosis of glomeru-
ar disease, and therefore accurate treatment planning, re-uires that the biopsy specimens not only be evaluated by
ight microscopy using special stains but also by electron andmmunofluorescent microscopy.
cknowledgmenthis manuscript was reproduced in part with permission
rom Vaden SL: Renal biopsy: Methods and interpretation.et Clin North Am (Small Anim Pract) 34:887-908, 2004.
eferences1. Grauer GF, Twedt DC, Mero KN: Evaluation of laparoscopy for obtain-
ing renal biopsy specimens from dogs and cats. J Am Vet Med Assoc183:677-679, 1983
2. Minkus G, Reusch C, Hörauf A, et al: Evaluation of renal biopsies in catsand dogs–histopathology in comparison with clinical data. J SmallAnim Pract 35:465-472, 1994
3. Richards NT, Darby S, Howie AJ, et al: Knowledge of renal histologyalters patient management in over 40% of cases. Nephrol Dial Trans-plant 9:1255-1259, 1994
4. Vilafranca M, Wohlsein P, Trautwein G, et al: Histological and immu-nohistological classification of canine glomerular disease. ZentralblVeterinarmed A 41:599-610, 1994
5. Jeraj K, Osborne CA, Stevens JB: Evaluation of renal biopsy in 197 dogsand cats. J Am Vet Med Assoc 181:367-369, 1982
6. Léveillé R, Partington BP, Biller DS, et al: Complications after ultra-sound-guided biopsy of abdominal structures in dogs and cats: 246cases (1984-1991). J Am Vet Med Assoc 203:413-415, 1993
7. Hager DA, Nyland T, Fisher P: Ultrasound-guided biopsy of the canineliver, kidney and prostate. Vet Radiology 26:82-88, 1985
8. Groman RP, Bahr A, Berridge BR, et al: Effect of serial ultrasound-guided renal biopsy on kidneys of healthy adolescent dogs. Vet RadUltrasound 451:62-69, 2004
9. Osborne CA: Clinical evaluation of needle biopsy of the kidney and itscomplications in the dog and cat. J Am Vet Med Assoc 158:1213-1228,
19710. Wise LA, Allen TA, Cartwright M: Comparison of renal biopsy tech-niques in dogs. J Am Vet Med Assoc 195:935-939, 1989
1. Drost WT, Henry GA, Meinkoth JH, et al: The effects of a unilateralultrasound-guided renal biopsy on renal function in healthy sedatedcats. Vet Radiol Ultrasound 41:57-62, 2000
2. Parrish AE: Complications of percutaneous renal biopsy: A review of 37years’ experience. Clin Nephrol 38:135-141, 1992
3. McGill DB, Rakela J, Zinsmeister AR, et al: A 21-year experience withmajor hemorrhage after percutaneous liver biopsy. Gastroenterology99:1396-1400, 1990
4. McVay PA, Toy PTCY: Lack of increased bleeding after liver biopsy inpatients with mild hemostatic abnormalities. Am J Clin Pathol 94:747-753, 1990
5. Bigge LA, Brown DJ, Pennick DG: Correlation between coagulationprofile findings and bleeding complications after ultrasound-guidedbiopsies: 434 cases (1993-1996). J Am Anim Hosp Assoc 37:228-233,2001
6. Mezzano D, Tagle R, Pais E, et al: Endothelial cell markers in chronicuremia: Relationship with hemostatic defects and severity of renal fail-ure. Thromb Res 88:465-472, 1997
7. Vaden SL: Renal biopsy. How and Why, in 2000 Scientific Proceedings,18th Annual Veterinary Medical Forum, Seattle, WA, American Collegeof Veterinary Internal Medicine, 2000, pp 675-676
8. Larrain C, Langdell TD: The hemostatic defect of uremia. II. Investiga-tion of dogs with experimentally produced acute urinary retention.Blood 11:1067-1072, 1956
9. Osborne CA, Low DG, Jessen CR: Renal parenchymal response to nee-dle biopsy. Invest Urol 9:463-469, 1972
0. Nash AS, Boyd JS, Minto W, et al: Renal biopsy in the normal cat: Anexamination of the effects of a single biopsy. Res Vet Sci 34:347-356,1983
1. Stone EA, Barsanti JA: Diagnostic tests, in Stone EA, Barsanti JA (eds):Urologic Surgery of the Dog and Cat. Philadelphia, PA, Lea & Febiger,1992, pp 37-52
2. Osborne CA, Bartges JW, Polzin DJ, et al: Percutaneous needle biopsyof the kidney. Indications, applications, technique and complications.Vet Clinics North Am 26:1461-1504, 1996
3. Patterson JM: Laparoscopy in small animal medicine, in Kirk RW (ed):Current Veterinary Therapy VII Small Animal Practice. Philadelphia,PA, WB Saunders, 1980, pp 969-973
4. Stone EA, Barsanti JA: General surgical approaches, in Stone EA, Bar-santi JA (eds): Urologic Surgery of the Dog and Cat. Philadelphia, PA,Lea & Febiger, 1992, pp 100-106
5. Sweet EI, Davidson AJ, Hayslett JP: Complications of needle biopsy ofthe kidney in the dog. Radiology 92:849-854, 1969
6. Nash AS, Boyd JS, Minto AW, et al: Renal biopsy in the normal cat: Anexamination of the effects of repeated needle biopsy. Res Vet Sci 40:112-117, 1986
7. Jennette JC, Olson JL, Schwartz MM, et al (eds): Heptinstall’s Pathology ofthe Kidney (ed 5). Philadelphia, PA, Lippincott-Raven Publishers, 1998
8. Greenberg A, Cheung AK, Coffman TM, et al: Primer on Kidney Dis-
eases (ed 3). San Diego, CA, Academic Press, 2001