-
8/8/2019 Report Empyema
1/32
-
8/8/2019 Report Empyema
2/32
Empyema
An accumulation of thick,
purulent fluid within thepleural space, often with
fibrin development & aloculated (walled-off) area
where infection is located
-
8/8/2019 Report Empyema
3/32
Causes/Risk Factors:
Presence of bacterial pneumonia orlung abscess
Penetrating chest trauma
Hematogenous infection of thepleural space
Nonbacterial infections
Iatrogenic causes (after thoracic
surgery or thoracentesis)
-
8/8/2019 Report Empyema
4/32
Assessments with
PE & NHHSigns & Symptoms:
FeverNight
sweatsPleural pain
CoughDyspnea
AnorexiaWeight loss
-
8/8/2019 Report Empyema
5/32
Assessments with
PE & NHHPhysical Exams:
r or absent breathsounds over affected area
dullness on chestpercussionr
fremitus
-
8/8/2019 Report Empyema
6/32
Diagnostic & Lab Studies
Computed Tomography(CT) scan reveals largeempyema collection
with
atelectic lobe andconsolidation
-
8/8/2019 Report Empyema
7/32
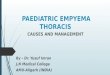
CT scan of chest showing empyemanecessitans (long arrow), a
chronic
untreated empyema that has eroded
through the thoracic cage and formed a
subcutaneous abscess (short arrow)
-
8/8/2019 Report Empyema
8/32
CT scan showing empyema with split pleura
sign (enhancement of the thickened inner
visceral and outer parietal pleura separated by
a collection of pleural fluid)
-
8/8/2019 Report Empyema
9/32
Diagnostic & Lab Studies
Diagnostic Thoracentesis,under ultrasound guidance
extraction of a cloudy orfrankly purulent fluid; little
or no offense odor (aerobicpus); foul smelling
(anaerobic pus)
-
8/8/2019 Report Empyema
10/32
Diagnostic & Lab Studies
Diagnostic Thoracentesis,under ultrasound guidance
fluid analysispH < 7.2Glucose 1000
IU/ml
Total protein >3g/ml
WBC > 15,000cells/mm3
-
8/8/2019 Report Empyema
11/32
Diagnostic
Thoracentesis
-
8/8/2019 Report Empyema
12/32
Presence ofParapneumonic Effusion
Release of inflammatory
mediators
Pathophysiology
-
8/8/2019 Report Empyema
13/32
permeability of thecapilliaries
Attracts WBCs to the site
Escape of albumin & otherprotein from the capillaries
-
8/8/2019 Report Empyema
14/32
Pleural fluid
Presence of free-flowing,protein rich pleural fluid
(Stage I)
-
8/8/2019 Report Empyema
15/32
-
8/8/2019 Report Empyema
16/32
Extensive purulentexudate production
Initiation of fibroblastic
activity(Stage II)
-
8/8/2019 Report Empyema
17/32
Adherence of the two
pleural membranes(Stage III)
Formation of a peel
-
8/8/2019 Report Empyema
18/32
Nursing Diagnosis
Impaired Gas Exchange r/tcompressed lung
Acute Pain r/t infection ofthe pleura
Risk for Activity Intolerancer/t hypoxia secondary to
empyema
-
8/8/2019 Report Empyema
19/32
Principles of Management
Help the patient cope withthe condition
Instruct patient in lung-expanding breathing exercises
to restore normal respiratoryfunction
-
8/8/2019 Report Empyema
20/32
-
8/8/2019 Report Empyema
21/32
Pharmacology
Antibiotic, cephalosporin (secondgeneration) for
bacterialinfections;
Cefuroxime (Zinacef) forstaphylococcal & streptococcal
organisms; most often selectedinitial antibiotic (Adult:
750-1500mg IV q8h; Pedia:
150mg/kg/d IV divided q8h)
-
8/8/2019 Report Empyema
22/32
Pharmacology
Antibiotics, anaerobic infections an aspiration or likely
anaerobicinfection is the cause of the
pneumoniaClindamycin (Cleocin) for gram-
positive organisms & anaerobes(Adult: 600-1200mg/d
IV/IMdivided q6-8h; Pedia: 25-
40mg/kg/d IV divided q6-8h)
-
8/8/2019 Report Empyema
23/32
Pharmacology
Antibiotic, Miscellaneous whenmethicillin-resistant S.aureus
issuspected.
Vancomycin (Vancocin, Vancoled) a glycopeptide agent for
gram-
positive (Adult: 500mg IV q6h or1g IV q12h- not to exceed
infusionrate of 10mg/min; Pedia:
40mg/kg/d IV divided tid/qid)
-
8/8/2019 Report Empyema
24/32
Pharmacology
Thrombolytic Agents convertplasminogen to plasmin, leading
toclot lysis.
Alteplase (Activase) binds tofibrin in a thrombus &
converts
the entrapped plasminogen toplasmin, initiating
localfibrinolysis. (administered
intrapleural via chest tube)
-
8/8/2019 Report Empyema
25/32
Surgery/Special Procedures
Antibiotic Therapy prescribedin large doses based on the
causative organismThoracentesis for small fluid
volume w/c is not too purulentor thick
-
8/8/2019 Report Empyema
26/32
Surgery/Special Procedures
Tube Thoracostomy forloculated or complicated
pleuraleffusions
Open Chest Drainage viaThoracotomy, including potential
rib resection for thickenedpleura & removal of the
underlyingdiseased pulmonary tissue
-
8/8/2019 Report Empyema
27/32
-
8/8/2019 Report Empyema
28/32
-
8/8/2019 Report Empyema
29/32
BioEthics
Is open thoracotomy
still a good treatmentoption for the
management ofempyema in children?
-
8/8/2019 Report Empyema
30/32
Open thoracotomy remains an
excellent option for managementof stage IIIII empyema
inchildren. When openthoracotomy is performed in atimely manner
there is low
morbidity and it provides rapidresolution of symptoms with
ashort hospital stay.
-
8/8/2019 Report Empyema
31/32
However, delayed referrals mayresult in advanced pulmonarysepsis
and a protracted clinicalcourse. The late results are
encouraging. Use of thoracoscopyor fibrinolysis should
beconsidered on the basis of theirown merit, not on the
assumptionof probable adverse outcomes
after thoracotomy.
-
8/8/2019 Report Empyema
32/32
THATS ALL,
THANK
YOU!!!