Embed Size (px)
Citation preview

Biology of Human Tumors
Reproducible, Quantitative, and FlexibleMolecular Subtyping of Clinical DLBCL SamplesUsing the NanoString nCounter SystemMargaret H. Veldman-Jones1, Zhongwu Lai2, Mark Wappett1, Chris G. Harbron3,J. Carl Barrett2, Elizabeth A. Harrington1, and Kenneth S. Thress2
Abstract
Purpose: Diffuse large B-cell lymphoma (DLBCL) is a hetero-geneous disease with distinct molecular subtypes. The mostestablished subtyping approach, the "Cell of Origin" (COO)algorithm, categorizes DLBCL into activated B-cell (ABC) andgerminal center B-cell (GCB)-like subgroups through gene expres-sion profiling. Recently developed immunohistochemical (IHC)techniques and other established methodologies can deliverdiscordant results and have various technical limitations. Weevaluated the NanoString nCounter gene expression system toaddress issues with current platforms.
Experimental Design: We devised a scoring system using 145genes from published datasets to categorize DLBCL samples. Aftercell line validation, clinical tissue segmentation was tested usingcommercially available diagnostic DLBCL samples. Finally, we pro-filedbiopsies frompatientswith relapsed/refractoryDLBCLenrolledin the fostamatinib phase IIb clinical trial using three independentRNA expression platforms: NanoString, Affymetrix, and qNPA.
Results: Diagnostic samples showed a typical spread of sub-types with consistent gene expression profiles across matchedfresh, frozen, and formalin-fixed paraffin-embedded tissues.Results from biopsy samples across platforms were remarkablyconsistent, in contrast to published IHC data. Interestingly, COOsegmentation of longitudinal fostamatinib biopsies taken atinitial diagnosis and then again at primary relapse showed88% concordance (15/17), suggesting that COO designationremains stable over the course of disease progression.
Conclusions:DLBCL segmentationof patient tumor samples ispossible using a number of expression platforms. However, wefound that NanoString offers the most flexibility and fewestlimitations in regards to robust clinical tissue subtype character-ization. These subtype distinctions should help guide diseaseprognosis and treatment options within DLBCL clinical practice.Clin Cancer Res; 21(10); 2367–78. �2014 AACR.
See related commentary by Rimsza, p. 2204
IntroductionDiffuse large B-cell lymphoma (DLBCL) is the most common
type of lymphoma, accounting for nearly 40%ofnewly diagnosedcases (1). Although approximately 50% of DLBCLs are curablethrough standard treatment, there is an urgent need for newtherapies as most relapsed patients will eventually die from theirdisease . DLBCL has been long recognized as a heterogeneousdisease with diverse genetic features and variable clinical out-comes. Gene expression profiling (GEP) techniques have beenused for over a decade to classify DLBCL into distinct molecularsubtypes, some of which carry significant prognostic value (2–5).The most well-established expression signature is the "Cell ofOrigin" (COO) algorithm, which divides DLBCL into activated
B-cell (ABC) and germinal center B-cell (GCB)-like subgroups.The COO signature can be refined to 12 distinct genes capable ofaccurately subtyping DLBCL with little loss of specificity orsensitivity (4). The continued refinement and potential prognos-tic value of COOprofiling has led to its incorporation into patientselection strategies for emerging targeted therapeutics. Both ibru-tinib (Pharmacyclics) and bortezomib (Millennium) haveapplied retrospective ABC/GCB patient profiling to phase I andII clinical trials (6, 7).
COO (and other) expression profiling approaches willundoubtedly lead to continued investment in personalized med-icine opportunities inDLBCL (8). Anobstacle tomorewidespreadclinical profiling has been the limited availability of snap frozenDLBCL biopsies that yield high quality tumor RNA. Standardclinical practice usually results in collection of formalin-fixed,paraffin-embedded (FFPE) diagnostic tissue that yields fragmen-ted RNA. Such RNA is not the preferred input type for microarray-based approaches (i.e., Affymetrix) historically used for COOprofiling. Because of this limitation, alternatives to classic micro-arrays have emerged to enable COO profiling of diagnostic FFPEspecimens. Numerous immunohistochemical (IHC) classifiershave been developed over the last decade (9). The original IHCalgorithm is the "Hans" approach based on expression of threeprotein markers that have been widely adopted within segmentsof the clinical DLBCL community (10). Being an immunohis-tochemistry-based assay, the Hans methodology is subject to
1AstraZeneca Oncology Innovative Medicines, Macclesfield, UnitedKingdom. 2AstraZeneca Oncology Innovative Medicines, Waltham,Massachusetts. 3AstraZeneca Discovery Sciences, Macclesfield,United Kingdom.
Note: Supplementary data for this article are available at Clinical CancerResearch Online (http://clincancerres.aacrjournals.org/).
Corresponding Author: Kenneth S. Thress, AstraZeneca Oncology InnovativeMedicines, 35 Gatehouse Drive, Waltham, MA 02451. Phone: 781-375-6185; Fax:781-839-4550; E-mail: [email protected]
doi: 10.1158/1078-0432.CCR-14-0357
�2014 American Association for Cancer Research.
ClinicalCancerResearch
www.aacrjournals.org 2367

antibody limitations, pathologist subjectivity, and is relativelynonquantitative in its scoring. Not surprisingly, Hans IHC andAffymetrix GEP have been shown to lack full concordance whentested concurrently on a blinded set of biopsies (11). Morerecently, the quantitative nuclease protection assay (qNPA; HTGMolecular Diagnostics) has emerged as another technology forDLBCL segmentation as it canmeasure gene expression fromFFPEmaterial in a fully quantitative manner (12, 13). While qNPA hassome distinct advantages, the current platform is limited in itsability for multiplex analysis of a large number of genes. WhileAffymetrix can monitor thousands of genes, qNPA monitors lessthan 50 in a single run.
The desire to develop an approach that provides a flexible,robust, and fully quantitative method for DLBCL segmentationled us to evaluate the recently described NanoString system forgene expression (14–16). NanoString technology uses digital,color-coded barcodes (codesets) that are attached to sequencespecific probes, allowing for fully quantitative and direct mea-surement of mRNA without amplification. The nonenzymaticnature of NanoString allows for accurate and reproducible quan-tification of as little as 100 ng of input mRNA from FFPE clinicalsamples. A key differentiating feature of the NanoString systemfrom IHC and qNPA-based approaches is its ability for multiplexanalyses of up to 800 distinct targets. To evaluate the NanoStringsystem for DLBCL subtyping, we designed a custom codeset ofmore than 300 genes, consisting of 145 COO signature genes andadditional genes from alternative DLBCL segmentation signa-tures. We tested these codesets on the NanoString against DLBCLcell lines with known COO designation and then against a set ofcommercially procured de novo DLBCL patient samples. Finally,we applied the NanoString codeset to biopsies from an ongoing60 patient clinical trial evaluating the effectiveness of fostamati-nib (Syk inhibitor) in relapsed-refractory DLBCL (17). Throughthe course of the evaluation, we directly tested many samplesagainst other relevant platforms, including Affymetrix microarray
and qNPA, to allow for both relative expression data and COOdesignation comparisons.
Materials and MethodsCell line and tissue samples
DLBCL cell lines were purchased from Cambridge Enterprise(DSMZ) in 2010 unless otherwise noted. HBL-1 (provided byDaniel Krappmann, German Research Center for EnvironmentalHealth), SU-DHL-10, Karpas 422, RC-K8, and SU-DHL-4 werecultured in RPMI with 10% to 15% FBS and 1% L-glutamine.TMD8 (provided by Shuji Tohda, Tokyo Medical and DentalUniversity) and OCI-Ly19 were cultured in a-Eagle's minimumessential medium with 10% FBS and 1% L-glutamine . OCI-Ly4and OCI-Ly10 (both provided by Mark Minden, Ontario CancerInstitute) were cultured in Iscove's modified Dulbecco's mediumwith 20% FBS, 1% L-glutamine, and 50 mmol/L b-mercaptoetha-nol. Each vial of cells was used for no more than six passages.Cells were maintained in 5% CO2 at 37�C. All cell lines weretested for authenticity by genotyping in 2010 before use; onlythose cell lines confirmed to carry the genetic profiles as describedpreviously were used in data presentation.
Commercially available DLBCL tissue samples (RNA; desig-nated as fresh, frozen, and FFPE) were purchased from OriGene.All required consents for these exploratory analyses wereacquired. Before processing, each sample was reviewed by aninternal certified pathologist to confirm disease diagnosis andverify tumor content.
Fostamatinib phase IIb clinical trial (NCT01499303) pretreat-ment frozen core needle biopsies and archival FFPE tissue sectionswere shipped from recruitment centers with required consent andhandled according to AstraZeneca Human Biological Samplespolicies and procedures. Before analysis, an hematoxylin andeosin–stained section fromeach samplewas assessedby a certifiedpathologist to confirm disease diagnoses and verify tumor con-tent. A titration study between two frozenDLBCLbiopsies (one ofeach subtype) and benign lymphoid tissue showed a linearrelationship between reduction in tumor content and the effecton the gene signature score (data not shown). These resultssupport an arbitraryminimumcutoff of 70% tumor,with samplesdeemed unevaluable if containing less than 70% tumor tissue. Allclinical samples used throughout this study were determined tocontain at least 70% DLBCL.
Sample preparation and RNA extractionUnder material transfer agreement, total RNA from all nine
DLBCL cell lines was isolated using standard procedures andprovided by colleagues at AstraZeneca Gatehouse Park. Replicatebatches of total RNAwere isolated from sixDLBCL cell lines (HBL-1, TMD8, SU-DHL-4, SU-DHL-10, OCI-Ly19, and Karpas 422)using the RNeasyMini Kit (Qiagen). Frozen tissues obtained fromOriGenewere processed as 2� 8mmcurls. Fostamatinib phase IIbtrial frozen core needle biopsies were sectioned to at least 5mm inlength and, if size allowed, processed and analyzed in biologicduplicates. Processed frozen tissue sectionswere homogenized onthe TissueLyser II system (Qiagen). Total RNA was isolated usingthe RNeasyMini Kit. FFPE tissues were processed as two to five 10-mm sections and total RNA isolated using the RecoverAll FFPERNA Isolation Kit (Ambion). Quality of tissue RNA was assessedusing the RNA 6000 Nano Kit (Agilent) and the quantity assessedon the NanoDrop 2000.
Translational Relevance
Diffuse large B-cell lymphoma (DLBCL) is a heterogeneousdisease that can be classified into two major molecular sub-types: activated B-cell–like (ABC) and germinal center B-cell–like (GCB)DLBCL. Clinical trials of targeted therapies are nowunderway using ABC/GCB segmentation as a patient stratifi-cation approach. Both gene expression profiling (GEP) andimmunohistochemistry (IHC) have historically been used tosegment ABC from GCB-type DLBCL. Although the accurateclassification of patients is essential for data interpretation,commonly used GEP and immunohistochemical methodol-ogies suffer from several limitations. We developed a DLBCLassay on the NanoString gene expression system that accu-rately and reproducibly categorized multiple DLBCL sampletypes, including both fresh and formalin-fixed patient tumortissue. After comparing against IHC and several other standardgene expression methodologies, the NanoString offered sev-eral key advantages, including sensitivity, flexibility, and clin-ical applicability. The NanoString platform should be stronglyconsidered for both DLBCL research and patient managementactivities.
Veldman-Jones et al.
Clin Cancer Res; 21(10) May 15, 2015 Clinical Cancer Research2368

NanoString codeset design and expression quantificationCOO and consensus clustering (CC) signature and housekeep-
ing genes were included in the codeset based on previouslydescribed publications (Supplementary Table S1). Input totalRNA amount was determined by titration studies to show com-parable and reliable gene expression data at 100 ng for highquality (cell lines, fresh, and frozen tissue) and at 400 ng for lowquality (FFPE tissue) samples based on detection levels, linearityof genes, and binding density (data not shown). Data werenormalized through an internally developed Pipeline Pilot Tool(publicly available for use on the Comprehensive R ArchiveNetwork, CRAN). In brief, data were log2 transformed after beingnormalized in two steps: raw NanoString counts were first back-groundadjustedwith aTruncatedPoisson correctionusingnegativecontrol spikes followed by a technical normalization using positivecontrol spikes.Datawere then corrected for input amount variationthrough a Sigmoid shrunken slope normalization step using theGEO mean expression of housekeeping genes. A transcript wasdesignated as not expressed if the raw count was below the averageof the internal negative control raw counts plus two SDs.
Microarray (Affymetrix) quantificationTotal RNAwas extracted from fresh and frozen samples using a
standard protocol. At least 250 ng of total RNA from each samplewith OD 260/280 ratio between 1.68 and 2.08 and concentration>50 ng/mL was submitted to Almac Diagnostics. Gene expressionprofiling was conducted using Affymetrix U133 plus 2.0 chipaccording to manufacturer recommendations. The CEL files wereanalyzed using Bioconductor's Affy package in R. Expression wasnormalized using MAS5.0 method with scaling factor set to 100.The signals were then log2 transformed before downstream anal-ysis. When a gene hadmore than one probeset, the probeset withthe highest mean signal was selected to represent the gene.
qNPATwo 5-mm FFPE sections per patient were delivered to HTG
Molecular Diagnostics for processing and qNPA analysis. Allsamples were run against HTG's 12-gene COO signature arrayconsisting of the following genes: CD10, LRMP, CCND2, ITPKB,PIM1, IL16, IRF4, FUT8, BCL6, LMO2, CD39, and MYBL1. Allprocessing and data analyses were conducted as described (13).
Quantitative real-time RT-PCRGene expression assays for 12 genes [FUT8, IL16, IRF4,CCND2,
PIM1, CD39 (ENTPD1), ITPKB, LMO2, LRMP, CD10 (MME),MYBL1, and BCL6] were ordered from Applied Biosystems (Sup-plementary Fig. S1A). For normalization purposes, IPO8 wasselected from a screen of 16 housekeeping genes based on itsrobust stability and low SD across a panel of six DLBCL cell lines(Supplementary Fig. S1B andS1C). Reverse transcription of 100ngRNAwasperformedusing the Superscript ViloKit (Invitrogen) andquantitative real-time PCR amplification of cDNA was performedon the 7900HT TaqMan (Applied Biosystems) in 10 mL reactionscontaining TaqMan Gene Expression master mix and assays(Applied Biosystems). Samples were amplified with three exper-imental replicates. No template controls were reliably negative.
DLBCL COO subtype classification using signature scoresWe calculated a composite score of our COO signature, using a
method previously described (18). The unweighted average scorewas calculated from gene expressions within a cohort after house-
keeping gene normalization and log2 transformation. Signaturescores were then calculated as the mean expression of genesassociated with ABC subtypeminus themean expression of genesassociated with GCB subtype; a higher score thus indicating amore ABC-like sample.
We then assessed the ability of our COO signature scores topredict the COO subtypes in 32 DLBCL cell lines and publiclyavailable datasets of DLBCL patient expression profiles. Highsignature score cell lines were almost exclusively ABC, withTOLEDO the only exception (Supplementary Fig. S2A). We fur-ther applied the method to two datasets (GSE10846 andGSE4732, available in GEO), and found them to be correlatedwell with ABC and GCB subtypes assigned by study authors(Supplementary Fig. S2B and S2C). We also found unclassifiedDLBCL to bemainly concentrated in themiddle. We thus decidedto assign an empirical cut off for samples to ABC if the signaturescores were above 0.7, to GCB if below 0, and unclassified ifbetween 0 and 0.7.
ResultsDefinition of NanoString and RT-PCR gene lists for DLBCLsegmentation
A comprehensive list of 307 genes was compiled from twoliterature-established methodologies: COO and CC (Fig. 1).For COO segmentation, multiple predictors have been des-cribed in the literature (4, 13, 19). By combining uniquepredictors from these studies, a list of 51 distinct genes wasobtained (Fig. 1A). From four publicly available gene expres-sion profiles of patients with DLBCL with ABC and GCBannotations [Lymphoma (3); Lymphoma 2-GSE4732 (20);Lymphoma-GSE4475 (21); Lymphoma-GSE10874 (5)] inOncomine (22), we selected 126 genes that were differentiallyexpressed in at least two of the four studies (Fig. 1B). Combinedwith the 51 predictor genes, we derived 145 unique genes thatwere associated with either ABC or GCB subtypes. For CCclassification, we relied on the original publication (23), whichused 150 probes, representing 133 unique genes (Fig. 1C). Tocorrect for batch effects and normalize samples analyzed overtime in several different test sets, we included in the codeset 33housekeeping genes whose expressions were moderate to highand showed little variance across datasets (Fig. 1D). The finalNanoString gene list (codeset) contained 307 unique genes(Supplementary Table S1). To compare NanoString with anestablished quantitative technique, real-time PCR (RT-PCR)primer-probe sets were created for a 12 gene subset of the mostrefined version of the COO signature, as previously described(4, 13) (Supplementary Table S1 and Fig. S1B).
Validation of NanoString codeset for disease segmentation inDLBCL cell lines and clinical samples
We examined nine DLBCL cell lines with literature-establishedCOO designations (24, 25). To confirm that inhouse cell lineswere representative of those in the literature, we used a previouslydescribed (18) RT-PCR method and applied a COO signaturescore (detailed in Materials and Methods); a high scoring sample(>0.7) signified an ABC subtype, low scoring samples (<0) a GCBsubtype, and those in between (>0–<0.7) as unclassified. Reversetranscription and RT-PCR was performed using the refined 12-gene COO subset on eight DLBCL cell lines and DCt values (meanof triplicate) were scored and ranked. The results confirmed the
Molecular Subtyping of DLBCL Samples with NanoString
www.aacrjournals.org Clin Cancer Res; 21(10) May 15, 2015 2369

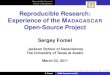
expected COO designation (Supplementary Fig. S2D) and corre-lated well to NanoString data (Supplementary Fig. S2E and S2F).We then assessed the reproducibility of the NanoString platform.Replicates of all nine DLBCL cell lines were used to investigatetechnical reproducibility (intra- and inter-assay) and correlationswere found to be extremely tight, with biologic reproducibilityonly slightly inferior (Fig. 2A and B). In addition, agreementbetween replicates was confirmed using an intraclass correlationcoefficient (ICC) pooled over genes from a mixed effects modelwith gene as a fixed effect and cell line within gene and residualvariation as random effects (ICC technical replicates 0.965, ICCbiologic replicates 0.873). From these data, we concluded thatbiologic replicates should be used in favor of technical replicateswhenever possible.
After establishing the reproducibility of the platform andverifying the DLBCL cell line COO designations, cellular RNAwas profiled using the complete DLBCL codeset. By examiningrelative expression levels of 145 COO genes as measured byNanoString, two distinct subgroups of cell lines (ABC and GCB)were clearly identifiable (Fig. 2C). The COO signature scores ofthe nine DLBCL cell lines show near-perfect correlation with eachdesignation of cell line in the literature and by RT-PCR (Fig. 2D).One potential outlier, OCI-Ly19, appeared to have elements ofboth subtypes according to the 145-gene COO signature score,but has been called GCB by various methodologies in the liter-ature. Culturing our OCI-Ly19 cell line in the presence of FBSrather than human plasma as previously described (26) couldhave resulted in slightly altered gene expression and an affectedCOO profile. However, publicly available RNA-seq data alsoclustered OCI-Ly19 between ABC and GCB subtypes, corrobo-rating our findings (27). The DLBCL cell lines were also simul-taneously profiled against the 133 genes reported to define the CCalgorithm (23). Despite repeated attempts, we were unable tosegregate the cell lines into their reported CC bins (BCR, HR, andOxPhos) using the 133-geneNanoString expression data. Becauseearly attempts with clinical samples also failed, we decided toabandon additional efforts related to the CC algorithm.
To evaluate NanoString and theDLBCL codeset, we examined aset of commercially available diagnostic clinical DLBCL samples,which included 14 FFPE tissue blocks (FFPE), 36 RNA samplesprepared from fresh DLCBL biopsies (fresh), and 24 flash-frozenexcisional DLBCL biopsies (frozen; Fig. 3A). Importantly, thesethree sample types were almost entirely paired and patient-matched, enabling cross-matrix comparisons. First, we profiledthe 36 fresh RNA samples and generated COO signature scores onthe NanoString platform. These scores showed the expectedsubtype distribution of a pretherapy (diagnostic) DLBCL popu-lation with 47% GCB, 25% ABC, and 28% unclassified (Fig. 3B).Together with the cell line dataset, this gave confidence in theability of the NanoString platform to identify and classify DLBCLsubgroups using fresh RNA. Patient biopsy material is most oftencollected as FFPE tissue at clinical sites so we proceeded to profileRNA extracted from FFPE tissue of 13 patients alongside matchedfresh RNA from the same patients (Fig. 3C) and five matchedfrozen biopsies (Supplementary Fig. S3A). The quantitative cor-relation was shown to be very robust, establishing that Nano-String could generate high-quality data on FFPEmaterial to allowfor clinically relevant DLBCL segmentation. The same sample setwas also evaluated using RT-PCR (12 COO signature genes) withstrong correlations observed between the two platforms furthervalidating the NanoString results (data not shown). These datademonstrate that tissue preparation and processing does notcompromise the gene expression signatures generated fromNanoString.
Correlation betweenNanoString quantification and alternativeplatforms using OriGene samples
There are several existing and emerging methodologies forCOO classification of clinical DLBCL tissue (Fig. 4A). Aftervalidating the NanoString platform as another viable approach,we compared NanoString outputs to other established tech-nologies using the OriGene clinical DLBCLmatched sample set.The Hans IHC algorithm, the most widely used clinical COOsegmentation tool, is based on three antibodies (CD10, Bcl-6,
A) COO: ABC/GCB predictors
Rimsza 2011 (14)
Blenk 2007 (24)
Wright 2003 LC (26)
Wright 2003 Affy (30)
B) COO: ABC/GCB differentiators from microarray profiling
2000 (51)Alizadeh
Dave 2006 GSE4732 (200)
Hummel 2007 GSE4475 (188)
Lenz 2008 GSE10874 (200)
C) CC: BCR consensus clustering
D) Housekeeping genes
Monti 2005 (133; 37 BCR, 50 HR, 46 OxPhos)
51Unique genes
126Genes identified in at least 2 studies
145Unique genes
Various (33; selected on expression and low variance in DLBCL)
276Unique genes
307Unique genes in total
Figure 1.The process of deriving the 307-genelist for NanoString profiling. Numbersin brackets indicate the number ofgenes identified from each search;numbers in boxes show the number ofunique genes from pooled datasetswith overlapping genes omitted. HR,host response; OxPhos, oxidativephosphorylation.
Veldman-Jones et al.
Clin Cancer Res; 21(10) May 15, 2015 Clinical Cancer Research2370

Mum1) and uses FFPE diagnostic tissue (10). We profiled theFFPE samples from 10 different patients through both the HansIHC (Phenopath Inc.) and NanoString platforms and observeda 90% concordance rate of finalized COO signature calls(Supplementary Fig. S3B).
Although not often employed for clinical segmentation, Affy-metrix GEP is the most well-established methodology for COOsubtyping and is an important comparator for NanoString eval-uation (28). Thirty-four fresh RNA samples were profiled con-currently across NanoString and Affymetrix using the full Nano-StringDLBCL codeset and theU133plus 2.0 array (Affymetrix). Incontrast to Hans IHC, both Affymetrix and NanoString providefully quantitative outputs, thus allowing formore robust analyses.The COO score correlations derived from the same 145 COOgenes were impressive across the two platforms (Fig. 4B), as were
the gene expression correlations and COO designations (Supple-mentary Fig. S3A and S3C).
A qNPA from HTG Molecular Diagnostics is another COOsegmentation methodology that has been described in the liter-ature (12). Because qNPA has already been used to segmentDLBCL patients in a clinical trial, we wished to directly comparethe twomethodologies (13, 29–31). Thirty-one samples (18 fresh,13 FFPE), representing 26 distinct patients, were profiled throughHTG's COO array consisting of the same 12 COO genes used forthe RT-PCR profiling described previously. The quantitative cor-relations betweenNanoString andqNPAdatasetswere very robustand, importantly, tight correlations were observed for both FFPEand fresh RNA samples (Fig. 4C and Supplementary Fig. S3D).
Any misclassifications between platforms can be explained bythe use of different classifiers to create COO scores (12 vs. 145
Color keyA B
C D
Not detected in bothDetected in one or the otherDetected in both
Nan
oS
trin
g-n
orm
aliz
ed e
xpre
ssio
n le
vel f
or
tech
nic
al r
eplic
ate
2 (l
og
2 sc
ale)
NanoString-normalized expression level for technical replicate 1 (log2 scale)
Nan
oS
trin
g-n
orm
aliz
ed e
xpre
ssio
n le
vel f
or
bio
log
ical
rep
licat
e 2
(lo
g2
scal
e)
NanoString-normalized expression level for biological replicate 1 (log2 scale)
Color keyNot detected in bothDetected in one or the otherDetected in both
Kar
pas
422
SubtypesColor key
MaxAverageMin
ABC/GCB
SU
-DH
L-1
0
SU
-DH
L-4
OC
I-L
y4
OC
I-L
y19
RC
K8
HB
L-1
TM
D8
OC
I-L
y10
145-
Gen
e co
des
et
–3–2–1
012345
OC
ILy1
0
HB
L-1
TM
D8
RC
K8
OC
I-L
y19
OC
ILy4
SU
-DH
L-1
0
SU
-DH
L-4
Kar
pas
422
145-
Gen
e C
OO
sco
reSubtypesABC/GCB
15
14
13
12
11
10
9
8
7
6
5
4
3
15
14
13
12
11
10
9
8
7
6
5
4
3
3 4 5 6 7 8 9 10 11 12 13 14 153 4 5 6 7 8 9 10 11 12 13 14 15
Figure 2A, NanoString correlation plot showing technical replicates of six cell line samples. Normalized log2 values of 287 genes are shown. Level of detection (LOD) wasset at mean þ two SDs of the eight negative spiked-in controls. Pearson correlation is 0.981. B, NanoString correlation plot showing biologic replicates of sixcell line samples. Normalized log2 values of 287 genes are shown. LODwas set at meanþ 2 SDs of the eight negative spiked-in controls. Pearson correlation is 0.933.C, heatmap of NanoString relative expression data illustrating unsupervised hierarchical clustering of nine DLBCL cell lines (four ABC and five GCB subtypes):horizontal columns represent individual genes (log2 count of 145 gene codeset), vertical columns individual cell lines. ABC and GCB DLBCL cell lines with knownCOO designations are clustered together as expected except for OCI-Ly19, which is classified as a GCB subtype but is clustered together with the ABC cell lines.D, the waterfall plot of NanoString data illustrating 145-gene COO scores of nine DLBCL cell lines with literature-associated designations (red, ABC;blue, GCB). Shaded area shows arbitrary scoring cut off (>0.7 ¼ ABC, <0.0 ¼ GCB, 0.0–0.7 ¼ unclassified).
Molecular Subtyping of DLBCL Samples with NanoString
www.aacrjournals.org Clin Cancer Res; 21(10) May 15, 2015 2371

genes). As expected, the correlation is better between matchingand larger classifiers (qNPA vs. RT-PCR, NanoString vs. Affyme-trix). In addition, the target RNA sequences used were not iden-tical between platforms, which can lead to different expressionpatterns that affect the COO designation. Of note, many discor-dant cases were due to those classifications bordering the cut-offcriteria.
Application of NanoString-based DLBCL segmentation tofostamatinib relapsed-refractory DLBCL phase IIb trial samples
The NanoString platform and DLBCL codeset were applied tobiopsy samples from an ongoing clinical trial of the Syk inhibitor,fostamatinib. The randomized, double-blind phase IIb study, is atrial of 60 patients designed to evaluate the efficacy of fostama-tinib in patients with relapsed or refractory DLBCL (31). Based onemerging preclinical data, an objective of the study was to explorewhether DLBCL subtype might predict response to fostamatinib.Flash-frozen core needle tumor biopsies were collected from allrelapsed/refractory participants before fostamatinib dosing, aswell as the original diagnostic (FFPE) biopsy. Because predose
biopsies would best represent the patient's tumor biology at thestart of fostamatinib therapy (following R-CHOP relapse), RNAwas first extracted from the evaluable core-needle biopsies (n ¼59) and subsequently profiled on NanoString to enable COOsegmentation. The COO signature scores of these patients withrelapsed/refractory DLBCL (Fig. 5A) displayed a distributionsimilar to that seen from diagnostic (pretherapy) biopsiesdescribed in the literature (32). The same RNA from 48 patientsthat passed QC criteria and profiled across the Affymetrix U1332.0 gene chip displayed strong quantitative and COO scoreconcordance with the NanoString output (Fig. 5B). Diagnostictumor material (FFPE slide or block) was available for a subset ofthe patients on the fostamatinib study providing the opportunityto explore whether COO designation might evolve during thecourse of R-CHOP therapy in patient-matched tissue. Eighteenpatients provided evaluable diagnostic (FFPE) and fresh prefos-tamatinib biopsy material that were run on the qNPA and Nano-String platforms, respectively. An 88% concordance (15/17) wasobserved in the COO calls between the two sample types (Fig.5C), suggesting that COO designation remains stable from initial
ABC(9/36 = 25.0%)
Unclassified(10/36 = 27.8%)
GCB(17/36 = 47.2%)
Fresh
A
C
B
(36)
Frozen(24)
FFPE(13)
(1)
NanoString log2 count for fresh RNA OriGene samples
Nan
oS
trin
glo
g2
cou
nt
for
FF
PE
Ori
Gen
esa
mp
les
14
13
12
11
10
9
8
7
6
5
4
3
2
1
2 3 4 5 6 7 8 9 10 11 12 13 14
Figure 3A, overview of OriGene clinical DLBCLsamples: 14 FFPE blocks (14/14 havematched fresh RNA, 13/14 havematched frozen RNA), 24 frozentissues (24/24 have matched RNA,13/24havematchedFFPEblocks), and36 fresh RNA samples (13/36 havebothmatched FFPE and frozen). B, Piechart showing expected spread ofDLBCL classifications of 36 fresh RNAsamples based on 145-gene COOscores. C, scatter plot showingNanoString data correlation betweenfreshly prepared RNA and FFPE-derived RNA. Normalized log2 valuesof 287 genes from 13 OriGene samplepairs are shown in different shades ofgray. Pearson correlation is 0.954.
Veldman-Jones et al.
Clin Cancer Res; 21(10) May 15, 2015 Clinical Cancer Research2372

Methodology Input Vendor A
B
C
Preferred sample type
Markers/genes examined
10,000+ FF GEP mRNA Affymetrix
800FF and FFPE GEP mRNA NanoString
3FFPE IHC Protein PhenoPath
48FF and FFPE qNPA mRNA HTG
NanoString 145-gene COO scores
Aff
ymet
rix
145-
gen
e C
OO
sco
res
Color key
X:
0.00
X:
0.70
ABCGCBUnclassified
Legend
Fresh RNAFFPE
1.8
1.4
1
0.6
0.2
–0.2
–0.6
–1
–1.4
–1.8–2.5 –2 –1.5 –1 –0.5 0 0.5 1 1.5 2 2.5
3.5
3
2.5
2
1.5
1
0.5
0
–0.5
–1
–1.5
–2
–1 –0.5 0 0.5 1 1.5
NanoString 12-gene COO score
qN
PA
12-
gen
e C
OO
sco
re
2 2.5 3 3.5 4
Figure 4A, comparison of platforms used forCOO profiling. FF, fresh frozen; GEP,gene expression profiling. B,correlation plot between NanoStringand Affymetrix platforms based on145-gene COO scores calculated from34 fresh RNA samples. Pearsoncorrelation is 0.993. C, correlation plotbetween NanoString and qNPAplatforms based on 12-gene COOscores calculated from 31 OriGenesamples. Connected lines indicatesamples were derived from the samepatient. Pearson correlation is 0.956.
Molecular Subtyping of DLBCL Samples with NanoString
www.aacrjournals.org Clin Cancer Res; 21(10) May 15, 2015 2373

–3
–2
–1
0
1
2
3A
B
C
37 10 29 23 34 54 35 36 56 3 52 28 39 25 4 40 18 11 13 50 16 26 14 44 42 17 32 60 22 51 45 47 24 43 20 33 61 57 41 5 53 38 30 48 58 27 7 49 59 6 8 9 46 31 1 21 15 12 55
Nan
oS
trin
g 1
45-g
ene
CO
O s
core
s
Color key
ABC
GCB
Unclassified
NanoString 145-gene COO scores
Aff
ymet
rix
145-
gen
e C
OO
sco
res
Color keyABCDiscordantGCBUnclassified
Patient numberDiagnostic
(qNPA, 12 genes) R-CHOP relapsed
(Nanostring, 145 genes)
ABCABC3
ABCABC10
ABCABC34
ABCABC18
ABCABC23
GCBGCB32
GCBGCB1
GCBGCB9
GCBGCB12
GCBGCB31
GCBGCB15
GCBGCB21
GCBUnclassified22
GCBUnclassified33
GCBGCB27
UnclassifiedUnclassified14
UnclassifiedUnclassified26
<70% tumor contentGCB2
<70% tumor contentND63
ABCND28
ABCND35
GCBND19
GCBND20
3
2.5
2
1.5
1
0.5
0
–0.5
–1
–1.5
–1.5–2 –1 –0.5 0 0.5 1 1.5 2 2.5 3
X:
0.70
X:
0.00
Figure 5A, waterfall plot of NanoString data illustrating 145-gene COO scores and subtype designations of 59 patients. Arbitrary scoring cut-off was setat >0.7 ¼ ABC, <0.0 ¼ GCB, and 0.0–0.7 ¼ unclassified. B, correlation between NanoString and Affymetrix platforms based on 145-gene COOscores calculated from 48 patients. Pearson correlation is 0.995. C, COO designation is maintained over the course of standard DLBCL therapy.Patients marked in bold show discordant COO designation and patients marked in italics could not be correlated due to sample QC issues. ND, notdetermined.
Veldman-Jones et al.
Clin Cancer Res; 21(10) May 15, 2015 Clinical Cancer Research2374

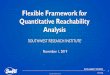
diagnosis through primary relapse. In addition to COO profiling,specific 50 and 30 NanoString probes were designed to detect thepresence of BCL2-IGH t(14:18) gene fusions known to occur inDLBCL (33). Using the OCI-Ly8 cell line with known BCL2-IGHfusion as apositive control,wedetectedputativeBCL2 gene fusionevents in 25% of fostamatinib DLBCL samples (Fig. 6; Supple-mentary Table S2).
DiscussionThe heterogeneous nature of DLBCL has prompted many
efforts at disease segmentation to inform prognosis or predictefficacy of specific therapies. The original description of the COOalgorithm, indicating that patients withGCB showed significantlybetter overall survival than patients with ABC, led to numerousreports aimed at confirming and extending the original findings(3). In that time, several COO profiling methodologies haveemerged that have influenced both research and clinical practice.Use ofmicroarrays is well established at the research level but highquality microarray data require RNA isolated from frozen tissue.Because themajority of clinical DLBCL diagnostic tissues are FFPEsamples,microarray-basedCOOprofiling canbe challenging. As away to enable widespread clinical utility, many IHC-basedapproaches for COO segmentation have been developed andadopted by clinical practitioners. IHC is attractive as a rapid,cost-effective, and accessible platform, commonly available inmost clinical centers. While IHC algorithms for COO segmenta-tion have shown reasonable concordance with microarray-based
approaches (10, 34, 35), the subjective nature of IHC scoringallows for inherent variability. Indeed, recent data have shownthat various iterations of nine related IHC algorithms do notcorrelate well with one another (9). A robust and reliable meth-odology for COO profiling, applicable to both research andclinical samples, is required to enable the successful discoveryand development of targeted therapies for DLBCL.
In this study, we evaluated the NanoString gene expressionplatform for the molecular classification of DLBCL specimens.The NanoString system generated high quality, reproducible, andfully quantitative results on a rangeof samples, including cell linesand clinical specimens. Importantly, inclusion of paired samplesets allowed us to demonstrate a strong concordance betweenpatient-matched frozen and FFPE material, showing the applica-bility of theNanoString platform to themost commonly availabletype of DLBCL patient tissue. Sample processing and turnaroundtime were user friendly; RNA input requirements were minimaland achievable from a single 10 mm clinical section.
Affymetrix microarray profiling is the most well-establishedCOO subclassification methodology and considered the goldstandard. To compare NanoString with Affymetrix, we profileda set of 34 well-annotated DLBCL clinical samples, with resultingCOO scores showing remarkable concordance. We extended thiscomparative analysis by profiling 48 additional patient samplesfrom the fostamatinib clinical trial across both platforms withsimilarly concordant COO scores. Any discordant COO designa-tions were due to small changes in the COO score around thecutoffs and highlights the importance of considering the score in
Shape and color key
ABCGCBIntermediateFFPEFrozen
12
11
10
9
8
7
6
5
4
3
5 6 7 8
BCL2 upstream
OCI-Ly8
BC
L2
3¢ U
TR
9 10 11 12 13
Figure 6.Identification of potential BCL2 translocation events from 59 patients in a fostamatinib phase IIb trial using NanoString technology. Two probes spanningcommon BCL2 fusion breakpoints were designed to identify patients with potential BCL2 translocation, which typically results in the loss of the BCL2 30 UTR. Thescatter plot shows the expression of these two probes, where the x-axis is the probe upstream of the breakpoints, and the y-axis is the probe at the 30 UTRdownstream of the breakpoints. The solid line is the correlation between these two probeswhen there is no translocation. The dashed lines indicate 4-fold deviationfrom the regression line. Each point represents a patient. Patients at the lower right outside the dashed line are potential BCL2 translocation candidates. Cellline OCI-Ly8, which is known to carry the BCL2-IGH translocation, is highlighted. Thirteen of the 15 BCL2 translocations are classified as GCB subtype, which isconsistent with the literature.
Molecular Subtyping of DLBCL Samples with NanoString
www.aacrjournals.org Clin Cancer Res; 21(10) May 15, 2015 2375

conjunctionwith thedesignation todistinguishbetween clear andmarginal GCB/ABC classifications. These data are in close agree-ment with a recent report using a small 20 gene NanoStringcodeset (36).
The frequent clinical use of the Hans IHC algorithm promptedus to compare a subset of 10 FFPE samples across bothNanoStringand IHC. The Hans COO designations showed a 90% concor-dance with designations from NanoString profiling of 145 genes.While concordance in this small sample set is high, it is importantto recognize differences in the data output between these twoplatforms despite the identical sample input demand (one FFPEsection). The Hans approach delivered qualitative expression onjust three proteins while NanoString returned fully quantitativedata on more than 300 genes. Our cross-platform results com-paring NanoString with IHC and Affymetrix are consistent with arecently published report using a smaller DLBCL sample set (37).
NanoString is not the only quantitative, FFPE-applicabletechnology that has been used for COO segmentation ofDLBCL. The qNPA platform uses a 12-gene COO panel andrequires similar sample inputs as NanoString without needingRNA extraction (13). To compare qNPA and NanoString direct-ly, 31 clinical samples (frozen and FFPE) were evaluated. COOscores were tightly correlated in both FFPE and frozen tissueand unlike the Affymetrix platform, relative gene expressiondata also showed strong correlation, even for genes at lowerexpression level (data not shown). While qNPA data comparedfavorably with NanoString, the setup of the current qNPA arrayis limited in its ability to multiplex large numbers of genes. Atpresent, single qNPA arrays are restricted to a maximum of 48genes while NanoString's upper limit is 800 and Affymetrixarrays can multiplex thousands. Depending on the application,the ability to profile large numbers of genes may be an advan-tage of NanoString, especially for exploratory approaches. AsCOO signatures have already been refined multiple times overthe past years, this particular feature may be less important forDLBCL segmentation. To ensure increased coverage of biology,we have chosen to be inclusive with our 145-gene COONanoString codeset. Scott and colleagues have recently pub-lished a 20-gene version of a NanoString codeset for COOsegmentation (36) and our analyses of 14 overlapping genescommon to both codesets showed highly correlated COOscores (Supplementary Fig. S4), suggesting our 145-gene code-set could be further refined.
The robust pilot data and promising comparative findings ofNanoString versus other established methodologies gave us theconfidence to profile patient samples from an active DLBCLclinical trial. The clinical activity of fostamatinib is beingassessed in patients with DLBCL who have progressed on R-CHOP therapy in a 60 patient phase IIb study (17). As pre-clinical data suggested that ABC-type cell lines may be prefer-entially sensitive to fostamatinib, COO segmentation of patientDLBCL tissue was considered key to a possible patient selectionstrategy (ref. 25; AstraZeneca unpublished data). Fresh, predoseDLBCL tumor biopsies (core needle) were successfully collectedfrom nearly all patients during prescreening. These flash-frozentissues were processed for NanoString and Affymetrix analyses.Fifty-nine samples were successfully profiled on NanoStringusing the complete 307-gene codeset. The NanoString-derivedCOO designations of these 59 relapsed/refractory samplesshowed a 31% ABC and 56% GCB split, numbers comparablewith those previously reported for diagnostic (pre-R-CHOP)
DLBCL tissue. To our knowledge, these represent the largestCOO dataset reported in tumor tissue from second line R-CHOP relapsed DLBCL. With the caveats associated with asample set of only 59 patients, these data could suggest thatR-CHOP treatment may not selectively enrich for ABC-typedisease. Additional profiling of relapsed biopsies will be need-ed to corroborate this hypothesis. Furthermore, by comparingdiagnostic tissue (pre-R-CHOP) from 18 patients to patient-matched rebiopsies (post-R-CHOP), we were able to show thatnearly 90% maintained a stable COO designation during thecourse of extended R-CHOP therapy. This observation couldhave implications for future targeted agents that may intend toselectively treat ABC or GCB-type patients upon relapse to R-CHOP (i.e., ibrutinib). In this setting, patient rebiopsies may berequested. Our data suggest that diagnostic tissue may representa suitable alternative to an invasive rebiopsy, at least in regardsto COO classification.
In addition to expression profiling, the flexibility of the Nano-String system allows for detection of disease-relevant genefusions/translocations. Several groups have reported successfulfusion detection using NanoString with 50 and 30 probes thatspan the specific breakpoint of the gene under investigation (38,39). Using a similar strategy, we designed NanoString probesaimed at detecting BCL2 translocation events within the fosta-matinib clinical trial sample set. The BCL2-IGH t (14;18) fusionis known to occur in DLBCL with an incidence of up to 30%; themajority are associated with the GCB subtype (33, 40). Wedetected putative BCL2 gene fusion events in 25% of fostama-tinib DLBCL samples, prevalence similar to that previouslyreported for BCL2-IGH (Fig. 6). All but two of these occurredin a sample with a GCB subtype, again consistent with theliterature. The specific BCL2 NanoString assay used to detectBCL2 in the fostamatinib samples was designed to detect onlymajor break points within the 30UTR that result in truncatedBCL2 transcripts. Because the assay was not designed to detectintermediate and minor break points, we cannot rule out thepossibility that other BCL2 translocations may have gone unde-tected. While additional profiling is underway to confirm thespecific BCL2 fusion partner and expand the analyses, theseobservations demonstrate the flexibility of the NanoString plat-form compared with other methodologies.
Additional NanoString analyses from fostamatinib biopsies,including COO subtype, BCL2 fusion incidence and/or baselinegene expression correlation to clinical response are ongoing andwill be reported separately.
The findings from this study indicate that the NanoStringsystem is a robust platform for molecular classification ofDLBCL. NanoString offers several advantages to establishedtechniques for COO segmentation, including multiplexing alarge number of genes, low RNA input requirements, goodreproducibility, complex genomic analysis (fusions) and sam-ple type flexibility (FFPE and frozen) giving access to greaternumbers of clinical samples. We have successfully appliedNanoString to a large set of relapsed/refractory DLBCL biopsiesobtained from an ongoing clinical trial. The resulting dataconfirmed the robust COO classification outputs from Nano-String and demonstrated the promise of the system to generatedata not otherwise achievable using other techniques. TheNanoString system should be strongly considered alongsideother established approaches for the molecular characterizationof DLBCL.
Clin Cancer Res; 21(10) May 15, 2015 Clinical Cancer Research2376
Veldman-Jones et al.

Disclosure of Potential Conflicts of InterestNo potential conflicts of interest were disclosed.
Authors' ContributionsConception anddesign:M.H. Veldman-Jones, Z. Lai, C.G.Harbron, J.C. Barrett,E.A. Harrington, K.S. ThressDevelopment of methodology:M.H. Veldman-Jones, Z. Lai, M. Wappett, C.G.Harbron, J.C. Barrett, E.A. HarringtonAcquisition of data (provided animals, acquired and managed patients,provided facilities, etc.): M.H. Veldman-Jones, K.S. ThressAnalysis and interpretation of data (e.g., statistical analysis, biostatistics,computational analysis): M.H. Veldman-Jones, Z. Lai, M. Wappett, C.G.Harbron, J.C. Barrett, E.A. Harrington, K.S. ThressWriting, review, and/or revision of the manuscript: M.H. Veldman-Jones,Z. Lai, C.G. Harbron, J.C. Barrett, E.A. Harrington, K.S. ThressAdministrative, technical, or material support (i.e., reporting or organizingdata, constructing databases): M.H. Veldman-Jones, K.S. Thress
Study supervision: M.H. Veldman-Jones, J.C. Barrett, E.A. Harrington, K.S.Thress
AcknowledgmentsThe authors thank the following AstraZeneca colleagues for technical assis-
tance: Chris Womack, Alison Pritchard, Doug McKechnie, Michael Dymond,Sarah Ali, Fred Zheng, and Kate Byth.
Grant SupportThis study was entirely funded by AstraZeneca.The costs of publication of this articlewere defrayed inpart by the payment of
page charges. This article must therefore be hereby marked advertisement inaccordance with 18 U.S.C. Section 1734 solely to indicate this fact.
Received February 11, 2014; revised September 3, 2014; accepted October 3,2014; published OnlineFirst October 9, 2014.
References1. Shaffer AL III, Young RM, Staudt LM. Pathogenesis of human B cell
lymphomas. Annu Rev Immunol 2012;30:565–610.2. Bea S, Zettl A,Wright G, Salaverria I, Jehn P,MorenoV, et al. Diffuse large B-
cell lymphoma subgroups have distinct genetic profiles that influencetumor biology and improve gene-expression-based survival prediction.Blood 2005;106:3183–90.
3. Alizadeh AA, Eisen MB, Davis RE, Ma C, Lossos IS, Rosenwald A, et al.Distinct types of diffuse large B-cell lymphoma identified by gene expres-sion profiling. Nature 2000;403:503–11.
4. Wright G, Tan B, Rosenwald A, Hurt EH, Wiestner A, Staudt LM. A geneexpression-based method to diagnose clinically distinct subgroups ofdiffuse large B cell lymphoma. Proc Natl Acad Sci U S A 2003;100:9991–6.
5. Lenz G, Wright GW, Emre NCT, Kohlhammer H, Dave SS, Davis RE, et al.Molecular subtypes of diffuse large B-cell lymphoma arise by distinctgenetic pathways. Proc Natl Acad Sci U S A 2008;105:13520–5.
6. Dunleavy K, Pittaluga S, Czuczman MS, Dave SS, Wright G, Grant N, et al.Differential efficacy of bortezomib plus chemotherapy within molecularsubtypes of diffuse large B-cell lymphoma. Blood 2009;113:6069–76.
7. deVos S,WilsonW, Gerecitano J, Goy A, Kenkre V, Barr P, et al.The Bruton'styrosine kinase (BTK) inhibitor, ibrutinib (PCI-32765), has preferentialactivity in the activated B cell-like (ABC) subtype of relapse/refractory (R/R)DLBCL: interim phase 2 results [abstract]. In: Proceedings of the 18thCongress of the European Hematology Association; 2013 Jun 13–16;Stockholm, Sweden. The Hague, the Netherlands: EHA; 2013. Abstract nrS1180.
8. Zhang J, Grubor V, Love CL, Banerjee A, Richards KL,Mieczkowski PA, et al.Genetic heterogeneity of diffuse large B-cell lymphoma. Proc Natl Acad SciU S A 2013;110:1398–403.
9. Coutinho R, Clear AJ, Owen A, Wilson A, Matthews J, Lee A, et al. Poorconcordance among nine immunohistochemistry classifiers of cell-of-origin for diffuse large B-cell lymphoma: implications for therapeuticstrategies. Clin Cancer Res 2013;19:6686–95.
10. Hans CP, Weisenburger DD, Greiner TC, Gascoyne RD, Delabie J, Ott G,et al. Confirmation of the molecular classification of diffuse large B-celllymphoma by immunohistochemistry using a tissue microarray. Blood2004;103:275–82.
11. Ott G, Ziepert M, Klapper W, Horn H, Szczepanowski M, Bernd HW, et al.Immunoblastic morphology but not the immunohistochemical GCB/nonGCB classifier predicts outcome in diffuse large B-cell lymphoma inthe RICOVER-60 trial of the DSHNHL. Blood 2010;116:4916–25.
12. Roberts RA, Sabalos CM, LeBlanc ML, Martel RR, Frutiger YM, UngerJM, et al. Quantitative nuclease protection assay in paraffin-embeddedtissue replicates prognostic microarray gene expression in diffuselarge-B-cell lymphoma. Lab Invest 2007;87:979–97.
13. Rimsza LM, Wright G, Schwartz M, ChanWC, Jaffe ES, Gascoyne RD, et al.Accurate classification of diffuse large B-cell lymphoma into germinalcenter and activated B-cell subtypes using a nuclease protection assay on
formalin-fixed, paraffin-embedded tissues. Clin Cancer Res 2011;17:3727–32.
14. Beard RE, Abate-Daga D, Rosati SF, Zheng Z,Wunderlich JR, Rosenberg SA,et al. Gene expression profiling using nanostring digital RNA counting toidentify potential target antigens for melanoma immunotherapy. ClinCancer Res 2013;19:4941–50.
15. Reis PP, Waldron L, Goswami RS, Xu W, Xuan Y, Perez-Ordonez B, et al.mRNA transcript quantification in archival samples using multiplexed,color-coded probes. BMC Biotechnol 2011;11:46.
16. Northcott PA, Shih DJ, Remke M, Cho YJ, Kool M, Hawkins C, et al.Rapid, reliable, and reproducible molecular sub-grouping of clinicalmedulloblastoma samples. Acta Neuropathol 2012;123:615–26.
17. AstraZeneca. Study to learn if 200 mg test drug (fostamatinib) helpspeople with large B-cell lymphoma, a type of blood cancer [Internet];[cited 2014 Feb 4]. Available from: http://clinicaltrials.gov/show/NCT01499303.
18. Loboda A, Nebozhyn M, Cheng C, Vessey R, Huang P, Dai H, et al.Biomarker discovery: identification of a growth factor gene signature.Clin Pharmacol Ther 2009;86:92–6.
19. Blenk S, Engelmann J, Weniger M, Schultz J, Dittrich M, Rosenwald A,et al. Germinal center B cell-like (GCB) and activated B cell-like (ABC)type of diffuse large B cell lymphoma (DLBCL): analysis of molecularpredictors, signatures, cell cycle state and patient survival. CancerInform 2007;3:399–420.
20. Dave SS, Fu K, Wright GW, Lam LT, Kluin P, Boerma E-J, et al. MolecularDiagnosis of Burkitt's Lymphoma. N Engl J Med 2006;354:2431–42.
21. HummelM, Bentink S, Berger H, KlapperW,Wessendorf S, Barth TFE, et al.A Biologic Definition of Burkitt's Lymphoma from Transcriptional andGenomic Profiling. N Engl J Med 2006;354:2419–30.
22. https://www.oncomine.org/resource/login.html.23. Monti S, Savage KJ, Kutok JL, Feuerhake F, Kurtin P, Mihm M, et al.
Molecular profiling of diffuse large B-cell lymphoma identifies robustsubtypes including one characterized by host inflammatory response.Blood 2005;105:1851–61.
24. Ngo VN, Young RM, Schmitz R, Jhavar S, Xiao W, Lim KH, et al. Onco-genically active MYD88 mutations in human lymphoma. Nature2011;470:115–9.
25. Naylor TL, TangH, Ratsch BA, Enns A, LooA, Chen L, et al. Protein kinase Cinhibitor sotrastaurin selectively inhibits the growth of CD79 mutantdiffuse large B-cell lymphomas. Cancer Res 2011;71:2643–53.
26. Ngo VN, Davis RE, Lamy L, Yu X, Zhao H, Lenz G, et al. A loss-of-functionRNA interference screen for molecular targets in cancer. Nature 2006;441:106–10.
27. http://www.ncbi.nlm.nih.gov/geo/query/acc.cgi?acc¼GSM1227194.28. Linton K, Howarth C, Wappett M, Newton G, Lachel C, Iqbal J, et al.
Microarray gene expression analysis of fixed archival tissue permits molec-ular classification and identification of potential therapeutic targets indiffuse large B-cell lymphoma. J Mol Diagn 2012;14:223–32.
www.aacrjournals.org Clin Cancer Res; 21(10) May 15, 2015 2377
Molecular Subtyping of DLBCL Samples with NanoString

29. Rimsza LM, LeblancML, Unger JM,Miller TP, Grogan TM, Persky DO, et al.Gene expression predicts overall survival in paraffin-embedded tissues ofdiffuse large B-cell lymphoma treated with R-CHOP. Blood 2008;112:3425–33.
30. Southwest Oncology Group; NCI. Studying genes in samples frompatients with limited or advanced diffuse large B-cell lymphoma [inter-net]; [cited 2014 Feb 4]. Available from: http://clinicaltrials.gov/show/NCT01563861.
31. Eastern Cooperative Oncology Group; NCI. Biomarkers in patients withdiffuse large B-cell lymphoma treated with combination chemotherapywith or without rituximab [internet]; [cited 2014 Feb 4]. Available from:http://clinicaltrials.gov/show/NCT01131208.
32. Rosenwald A, Wright G, Chan WC, Connors JM, Campo E, Fisher RI,et al. The use of molecular profiling to predict survival after chemo-therapy for diffuse large-B-cell lymphoma. N Engl J Med 2002;346:1937–47.
33. Weiss LM,Warnke RA, Sklar J, ClearyML.Molecular analysis of the t(14;18)chromosomal translocation in malignant lymphomas. N Engl J Med1987;317:1185–9.
34. Choi WL, Weisenburger DD, Greiner TC, et al. A new immunostainalgorithm classifies diffuse large B-cell lymphoma intomolecular subtypeswith high accuracy. Clin Cancer Res 2009;15:5494.
35. Haarer CF, Roberts RA, Frutiger YM, Grogan TM, Rimsza LM. Immu-nohistochemical classification of de novo, transformed, and relapseddiffuse large B-cell lymphoma into germinal center B-cell and non-germinal center B-cell subtypes correlates with gene expression profileand patient survival. Arch Pathol Lab Med 2006;130:1819–24
36. Scott DW, Wright GW, Williams PM, Lih C-J, Walsh W, Jaffe ES, et al.Determining cell-of-origin subtypes of diffuse large B-cell lymphomausinggene expression in formalin-fixed paraffin embedded tissue. Blood2014;123:1214–7.
37. Masque-Soler N, Szczepanowski M, Kohler CW, Spang R, Klapper W.Molecular classification of mature aggressive B-cell lymphoma usingdigital multiplexed gene expression on formalin-fixed paraffin-embeddedbiopsy specimens. Blood 2013;122:1985–6.
38. Lira ME, Kim TM, Huang D, Deng S, Koh Y, Jang B, et al. Multiplexed geneexpression and fusion transcript analysis to detect ALK fusions in lungcancer. J Mol Diagn 2013;15:51–61.
39. Sun J-M, Lira M, Pandya K, Choi Y-L, Ahn JS, Mao M, et al. Clinicalcharacteristics associated with ALK rearrangements in never-smokers withpulmonary adenocarcinoma. Lung Cancer 2014;83:259–64.
40. Iqbal J, Sanger WG, Horsman DE, Rosenwald A, Pickering DL, Dave B, et al.BCL2 translocation defines a unique tumor subsetwithin the germinal centerB-cell-like diffuse large B-cell lymphoma. Am J Pathol 2004;165:159–66.
Clin Cancer Res; 21(10) May 15, 2015 Clinical Cancer Research2378
Veldman-Jones et al.