Embed Size (px)
Citation preview

Research ArticleComparison of Capsule Endoscopy Findings to SubsequentDouble Balloon Enteroscopy: A Dual Center Experience
Amandeep S. Kalra,1 Andrew J. Walker,2 Mark E. Benson,2 Anurag Soni,2
Nalini M. Guda,3 Mehak Misha,4 and Deepak V. Gopal2
1Division of Hospital Medicine, Department of Medicine, University of Wisconsin School of Medicine and Public Health,1685 Highland Avenue, MFCB 3116, Madison, WI 53705, USA2Division of Gastroenterology andHepatology, Department ofMedicine, University ofWisconsin School ofMedicine and Public Health,1685 Highland Avenue, MFCB 4223, Madison, WI 53705, USA3Division of Gastroenterology & Hepatology, University of Wisconsin School of Medicine & Public Health,GI Associates-Aurora St. Luke’s Medical Center, 2801 W Kinnickinnic River Pkwy, Suite 1030, Milwaukee, WI 53215, USA4Department of Gynecology, Manipal College of Medical Sciences, Pokhara 33700, Nepal
Correspondence should be addressed to Deepak V. Gopal; [email protected]
Received 7 July 2015; Accepted 16 August 2015
Academic Editor: Lars Aabakken
Copyright © 2015 Amandeep S. Kalra et al. This is an open access article distributed under the Creative Commons AttributionLicense, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properlycited.
Background. There has been a growing use of both capsule endoscopy (CE) and double balloon enteroscopy (DBE) to diagnoseand treat patients with obscure gastrointestinal blood loss and suspected small bowel pathology. Aim. To compare and correlatesequential CE and DBE findings in a large series of patients at two tertiary level hospitals inWisconsin.Methods. An IRB approvedretrospective study of patients who underwent sequential CE and DBE, at two separate tertiary care academic centers from May2007 to December 2011, was performed. Results. 116 patients were included in the study. The mean age ± SD was 66.6 ± 13.2 years.There were 56% males and 43.9% females. Measure of agreement between prior capsule and DBE findings was performed usingkappa statistics, which gave kappa value of 0.396 with 𝑃 < 0.001. Also contingency coefficient was calculated and was found tobe 0.732 (𝑃 < 0.001). Conclusions. Our study showed good overall agreement between DBE and CE. Findings of angioectasia hadmaximum agreement of 69%.
1. Introduction
After the introduction of double balloon enteroscopy (DBE)and capsule endoscopy (CE) in years 2000 and 2001, respec-tively, there has been significant improvement in the man-agement of obscure gastrointestinal bleeding (OGIB) [1, 2].OGIB accounts for 5 percent of total GI bleeding, but itresults in multiple transfusions and repeated hospitalization[2, 3]. Until the advent of wireless capsule endoscopy (CE)and balloon-assisted deep bowel enteroscopy in the lastfifteen years, this had been a difficult area to evaluate andintervene upon, and inmany cases the etiology of small bowelbleeding remained undiagnosed using standard endoscopicand imaging modalities. Wireless CE is generally the testof choice for patients with OGIB who have undergone
preceding upper endoscopy and colonoscopy because of itscapability to examine the entire small bowel with reasonableaccuracy and it is relatively noninvasive and well tolerated.Additionally, most capsule endoscopy studies (70–80%) areperformed for obscure small bowel bleeding [4]. Capsuleendoscopy is limited by its inability to biopsy the lesionor to do any therapeutic interventions [2]. For this reason,balloon-assisted deep enteroscopy is primarily performed inconjunction with CE. Despite being more invasive than CE,one method of balloon-assisted deep enteroscopy, DBE, hasbeen shown to be clinically impactful. For instance, one studydemonstrated that DBE could detect a source of GI bleedingin nearly 80% of cases and clinically control bleeding in 65%of cases [5].
Hindawi Publishing CorporationDiagnostic and erapeutic EndoscopyVolume 2015, Article ID 438757, 5 pageshttp://dx.doi.org/10.1155/2015/438757

2 Diagnostic andTherapeutic Endoscopy
Table 1: Correlation between CE and DBE findings.
𝑁 = number ofcorresponding findings
DBE findings TotalAVM Erosions Normal Polyp Stricture Ulcer Others
Capsule
AVM 55 0 11 2 0 0 1 69Erosions 1 1 1 0 0 0 0 3Normal 12 0 13 0 1 2 0 28Polyp 0 0 2 0 0 0 0 2
Stricture 0 0 1 0 0 0 0 1Ulcer 0 0 4 0 0 6 0 10Others 1 0 1 0 0 0 1 3Total 69 1 33 2 1 8 2 116
Prior investigations comparing the diagnostic yieldbetween CE and DBE have shown comparable diagnosticyield but have been limited by small sample size.The purposeof this study is to compare and correlate sequential CE andDBE findings of the small bowel in a large series of patientsat two tertiary level hospitals in Wisconsin.
2. Methods
2.1. Patients. A retrospective review at two tertiary medicalcenters was performed for all patients with OGIB whounderwentCE and sequentialDBE fromMay 2007 toDecem-ber 2011. Institutional Review Boards at both University ofWisconsinHospital andClinics andAurora St. LukesMedicalCenter approved the study in which 116 patients were iden-tified. All patients suffered from OGIB and had undergoneupper gastrointestinal endoscopy and colonoscopy withoutthe discovery of any identifiable lesion. OGIB was defined asovert bleeding or recurrent fecal occult bleeding with anemiaof unknown origin. DBE was preceded by CE within 1 year inall cases. The total number of patients in this study was 116,out of which 65 (56%)weremales and 51 (43.9%) females witha mean age of 66.6 ± 13.2 years.
2.2. CE. In CE the video capsules (Medtronic, Duluth, GA,USA) were propelled through the gastrointestinal tract byperistalsis. Prokinetics were not employed. Sensors wereactivated on patient’s abdomen and connected to mobilerecording system. Later during the same day the equipmentwas removed and data were uploaded onto a computersystem. The technical procedures and evaluation of capsuleimages have been previously described [6]. This was inter-preted by an experienced gastroenterology staff at Universityof Wisconsin Hospital and Aurora St. Lukes Medical Center.All reviewers had reviewed >10 capsule examinations prior toinitiation of the study.The locations of the lesions in the smallbowel were determined by means of transit times.
2.3. DBE. The DBE system (Fujifilm Medical System, Stan-ford, CT, USA) is a video endoscope that consists of a flexibleovertube and a balloon controller. Double balloon endoscopehas a 200 cm working length and 145 cm overtube, with
a diameter, which varies from 8.5mm within the workinglength of the tube to 12.5mm at the overtube. DBE was doneeither anterogradely (orally) or retrogradely (per rectum)or both. Patients were instructed not to eat anything afterthe midnight before the procedure. For retrograde DBEpatients underwent bowel preparation the night before theprocedure. Diagnostic biopsies or therapeutic procedureswere performed via a 2.2mm diameter-working channeland the site of most distal advancement was tattooed. DBEwas performed under general anesthesia. In anterogradeand retrograde DBE scope is inserted orally and rectally,respectively, and advanced in repetitive cycles of inflationand deflation. DBE followed CE in all cases. The lengthof small bowel investigated was estimated endoscopicallyduring introduction and withdrawal of the scope. DBE wasperformed by 4 different endoscopists (DVG, MB, AS, andNG), each had performed >10 prior exams. The tube is laterwithdrawn with inflation and deflation techniques.
2.4. Interpretation of Findings/Data Analysis. All cases wereexamined for findings that could explain blood loss. Theseincluded presence of active bleeding source or culprit lesionsuch as ulceration (NSAID, Crohn’s disease, and ischemiculceration), arteriovenous malformations (AVMs), polyp,erosion, diverticulum, tumor, or Dieulafoy lesion. A positivestudy was defined as the presence of one of the abovefeatures. The CE findings were directly compared with theDBE findings for agreement with the DBE findings actingas the gold standard. All DBE cases were also reviewed fortherapeutic intervention.
3. Results and Discussion
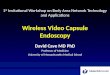
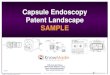
3.1. Results. 116 patients were included in the study.Themeanage ± SD was 66.6 ± 13.2 years. There were 56% males and43.9% females, respectively. Table 1 shows the cross tabulationof CE and DBE with various findings. Measure of agreementbetween prior capsule andDBEfindingswas performedusingkappa statistics, which gave kappa value of 0.396 (𝑃 < 0.001).Also contingency coefficient was calculated and was foundto be 0.732 (𝑃 < 0.001), indicating good overall agreement.AVMs had best agreement (69%; Figures 1(a), 1(b), and 1(c)),followed by ulcer disease (60%; Figures 2(a) and 2(b)).

Diagnostic andTherapeutic Endoscopy 3
(a) (b)
(c)
Figure 1: (a) 63-year-old male with bleeding jejunal AVM on CE. (b) 63-year-old male with corresponding AVM on DBE. (c) 63-year-oldmale with corresponding AVM treated with TouchSoft coagulation (Genii Inc., St. Paul, MN, USA) therapy with DBE.
(a) (b)
Figure 2: (a) CE of small bowel uclerations in distal jejunum/proximal ileum in 43-year-old female patient with severe iron deficiency anemiaand abdominal pain. (b) CorrespondingDBE in above patient ulcerated stricture consistent with a small bowel Crohn’s disease involving distaljejunum/proximal ileum.

4 Diagnostic andTherapeutic Endoscopy
Table 2: CE and DBE findings correlated based on findings (anemia versus OGIB).
Indication DBE findings TotalAVM Erosion Normal Polyp Stricture Ulcer Others
AnemiaPrior CEAVM 29 3 0 0 0 32Erosion 1 1 0 0 0 2Normal 7 9 1 1 0 18Polyp 0 1 0 0 0 1Stricture 0 1 0 0 0 1Ulcer 0 2 0 4 0 6Others 1 1 0 0 1 3Total 38 18 1 5 1 63
BleedingPrior CEAVM 26 0 8 2 0 1 37Erosion 0 1 0 0 0 0 1Normal 5 0 4 0 1 0 10Polyp 0 0 1 0 0 0 1Others 0 0 2 0 2 0 4Total 31 1 15 2 3 1 53
Interestingly, in our study, 42% of normal findings werefound to have AVMs on DBE. The two main indicationsof performance in both studies were anemia and bleeding(Table 2). Table 1 shows cross tabulation for individualindication of anemia and bleeding between DBE and CE.Contingency coefficient was calculated betweenCE andDBE,after splitting the number of cases with anemia and bleeding,which was found to be 0.736 and 0.772 indicating goodagreement with either indication.
3.2. Discussion. In our study we found that there is ahigh correlation between CE and DBE for small bowelangiodysplasias/AVMs at 69% followed by normal findings.These findings were similar to a retrospective study done byMarmo et al., which found a good agreement for vascularor inflammatory lesions but not for polyps or neoplasia [7].In a prospective study done by Matsumoto et al. in whichDBE was done prior to CE and CE observer was blinded tothe results, authors found good concordance in diagnosingOGIB between the two modalities, but DBE was superiorto CE in diagnosing small intestine polyps [8]. A meta-analysis from 2013 that looked in 12 studies, with 712 patients,who have undergone CE or DBE for OGIB found that CEand DBE had similar diagnostic capabilities for vascular,ulcerative, neoplastic, and inflammatory lesions [9]. In thesame meta-analysis, it was found that CE had significantlybetter diagnostic yield for fresh blood or clot whereas DBEhas better diagnostic yield for small bowel diverticular bleed.
Kameda et al. demonstrated a rate of agreement betweenCE andDBE thatwas 50%of all cases [10], whereaswe showedthat the total rate of agreement was 64.6%. In a previousstudy it was found by authors that CE has excellent negativepredictive value for lesions in small intestine, except for
polyps inwhichDBEhas better negative predictive value thanCE [11]. In our study the overall correlation for small bowellesions other than angiodysplasias/AVMs, ulcer disease, ornormal findings was suboptimal. One of the challenges withCE is the indefinite and nondiagnostic findings. In our study,CE showed indefinite abnormal results in 2.5% of patients.In our study no AVMs were detected in 14 cases of CE, butAVMs were found on subsequent DBE, out of which 12 caseshad normal findings on previous CE. In our study 42% ofall the normal CE studies had findings on subsequent DBEpotentially accounting for the patient symptoms.
In a previous single blind prospective study, 32 patientswith OGIB underwent CE followed by DBE determinedthat CE detected abnormal findings in 90.6% patients ascompared toDBEwhich detected abnormal findings in 65.6%[10]. We similarly showed that more abnormal findings wereseen on CE than DBE. In a meta-analysis done from 2007,which included 8 studies with 277 patients, the authorsnoted no significant difference in diagnostic yield of CEand complete DBE (anterograde and retrograde DBE), butdiagnostic yield of CE was found to be higher than eitheranterograde or retrograde approach alone [12]. In anothermeta-analysis done in 2008, which looked in 11 studies,comparing DBE and CE concluded that yield of CE and DBEin finding pathology of small bowel was similar [13].
4. Conclusions
Our study confirms that CE and DBE share a complementaryrole in diagnosing OGIB. CE that is performed first is usefulto direct the route of balloon-assisted enteroscopy when theindication is OGIB or anemia particularly when the findingsare AVMs, giving good agreement seen between the two

Diagnostic andTherapeutic Endoscopy 5
procedures in our study. As discussed above, AVMs demon-strate best agreement, which can be explained from the factthat most common indications for both studies are anemiaor OGIB with AVM being major cause of either indication.Previous studies have shown that when CE and DBE aredone together this provides a better diagnostic yield andbetter directed therapy [14]. Interestingly, in our study, 42% ofnormal findings were found to have angiodysplasias/AVMson DBE, which would argue towards proceeding with DBEin patients with normal findings on CE or even proceedingwith DBE without conducting CE if the indication is anemiaor bleeding with high suspicion of AVM. The merits of ourstudy over other previous studies are that it is a large dualcenter study with a large number of patients’ population withtwo only indications for CE and DBE being anemia or OGIB.The main limitation is the retrospective nature of our studyand the discrepancy between AVMs and any other findings.
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper.
References
[1] E. Rondonotti, K. Sunada, T. Yano, S. Paggi, and H. Yamamoto,“Double-balloon endoscopy in clinical practice: where are wenow?” Digestive Endoscopy, vol. 24, no. 4, pp. 209–219, 2012.
[2] P. Prabakaran, N. Guda, J. Thomas, C. Heise, and D. Gopal,“Clinical approach to obscure GI bleeding—diagnostic testingand management,” Journal of Digestive Endoscopy, vol. 4, no. 3,p. 61, 2013.
[3] M. K. Goenka, S. Majumder, S. Kumar, P. K. Sethy, and U.Goenka, “Single center experience of capsule endoscopy inpatients with obscure gastrointestinal bleeding,” World Journalof Gastroenterology, vol. 17, no. 6, pp. 774–778, 2011.
[4] T. Nakamura and A. Terano, “Capsule endoscopy: past, present,and future,” Journal of Gastroenterology, vol. 43, no. 2, pp. 93–99,2008.
[5] H. Yamamoto, H. Kita, K. Sunada et al., “Clinical outcomes ofdouble-balloon endoscopy for the diagnosis and treatment ofsmall-intestinal diseases,” Clinical Gastroenterology and Hepa-tology, vol. 2, no. 11, pp. 1010–1016, 2004.
[6] M. Nakamura, Y. Niwa, N. Ohmiya et al., “Preliminary compar-ison of capsule endoscopy and double-balloon enteroscopy inpatients with suspected small-bowel bleeding,” Endoscopy, vol.38, no. 1, pp. 59–66, 2006.
[7] R. Marmo, G. Rotondano, T. Casetti et al., “Degree of con-cordance between double-balloon enteroscopy and capsuleendoscopy in obscure gastrointestinal bleeding: a multicenterstudy,” Endoscopy, vol. 41, no. 7, pp. 587–592, 2009.
[8] T. Matsumoto, M. Esaki, T. Moriyama, S. Nakamura, and M.Iida, “Comparison of capsule endoscopy and enteroscopy withthe double-balloon method in patients with obscure bleedingand polyposis,” Endoscopy, vol. 37, no. 9, pp. 827–832, 2005.
[9] Q. Zhang, Q. He, J. Liu, F. Ma, F. Zhi, and Y. Bai, “Combined useof capsule endoscopy and double-balloon enteroscopy in thediagnosis of obscure gastrointestinal bleeding: meta-analysisand pooled analysis,” Hepato-Gastroenterology, vol. 60, no. 128,pp. 1885–1891, 2013.
[10] N. Kameda, K. Higuchi, M. Shiba et al., “A prospective, single-blind trial comparing wireless capsule endoscopy and double-balloon enteroscopy in patients with obscure gastrointestinalbleeding,” Journal of Gastroenterology, vol. 43, no. 6, pp. 434–440, 2008.
[11] X. Li, J. Dai, H. Lu, Y. Gao, H. Chen, and Z. Ge, “A prospectivestudy on evaluating the diagnostic yield of video capsuleendoscopy followed by directed double-balloon enteroscopyin patients with obscure gastrointestinal bleeding,” DigestiveDiseases and Sciences, vol. 55, no. 6, pp. 1704–1710, 2010.
[12] X. Chen, Z.-H. Ran, and J.-L. Tong, “Ameta-analysis of the yieldof capsule endoscopy compared to double-balloon enteroscopyin patients with small bowel diseases,” World Journal of Gas-troenterology, vol. 13, no. 32, pp. 4372–4378, 2007.
[13] S. F. Pasha, J. A. Leighton, A. Das et al., “Double-balloonenteroscopy and capsule endoscopy have comparable diag-nostic yield in small-bowel disease: a meta-analysis,” ClinicalGastroenterology and Hepatology, vol. 6, no. 6, pp. 671–676,2008.
[14] D. M. Cooley and A. J. Walker, “From capsule endoscopyto balloon-assisted deep enteroscopy: exploring small-bowelendoscopic imaging,”Gastroenterology&Hepatology, vol. 11, no.3, p. 143, 2015.

Submit your manuscripts athttp://www.hindawi.com
Stem CellsInternational
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Disease Markers
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation http://www.hindawi.com Volume 2014
Immunology ResearchHindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Parkinson’s Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttp://www.hindawi.com