Embed Size (px)
Citation preview

Research ArticleInfluence of the Clinical Status on Stress ReticulocytesCD 36 and CD 49d of SSFA
2Homozygous Sickle Cell Patients
Followed in Abidjan
Duni Sawadogo12 Assata Tolo-Dilkeacutebieacute3 Mahawa Sangareacute12 Nelly Agueacutehoundeacute1
Hermance Kassi4 and Toussaint Latte4
1 Department of Hematology Faculty of Pharmacy University Felix Houphouet Boigny Cocody BP 2308 Abidjan 08 Cote DrsquoIvoire2 Unit of Hematology Central Laboratory Teaching Hospital of Yopougon BP 632 Abidjan 21 Cote DrsquoIvoire3 Clinic Hematology Service Teaching Hospital of Yopougon BP 632 Abidjan 21 Cote DrsquoIvoire4AIDS Biological Unit Central Laboratory Teaching Hospital of Yopougon BP 632 Abidjan 21 Cote DrsquoIvoire
Correspondence should be addressed to Duni Sawadogo dunisawadogoyahoofr
Received 25 August 2013 Revised 12 January 2014 Accepted 12 January 2014 Published 27 February 2014
Academic Editor Aldo Roccaro
Copyright copy 2014 Duni Sawadogo et alThis is an open access article distributed under the Creative CommonsAttribution Licensewhich permits unrestricted use distribution and reproduction in any medium provided the original work is properly cited
Background and Objectives Interactions between sickle cells involving CD 49d CD36 and the vascular endothelium may initiatevasoocclusion leading to acute painful episodes and multiple organ failure Materials and Methods We selected 60 SS patientswho had never been treated by hydroxyurea We performed a total blood count We identified with immunophenotyping by flowcytometry total reticulocytes their distribution according to the degree of maturity (mature intermediate very immature) and CD36+ and CD 49d+ antigens Stress reticulocytes corresponded to the sum of intermediate and immature cells Results Subjects incrisis had more total reticulocytes and very immature reticulocytes than subjects in stationary phase (119875 lt 005) During the crisistotal CD 36+ reticulocytes (214 870 plusmn 107 584120583L versus 148 878 plusmn 115 024120583L119875 lt 005) and the very immature CD 36+ reticulocytes(289 plusmn 79 versus 230 plusmn 64 119875 lt 005) increased The clinical status had no impact on CD 49d+ reticulocytes ConclusionTherates of stress reticulocytes in general and those expressing CD 49d and CD 36 were very high The clinical status had an influenceon CD 36+ reticulocytes The expression of adhesion molecules is only one of the parameters involved in sickle cell disease crisis
1 Introduction
Sickle cell anemia (SCA) is a pathology characterized by acutepain and various organ failures related to frequent vasooc-clusive episodes The mechanism that leads to these vasooc-clusive events is not yet clearly defined Vasoocclusion maybe due to an interaction between sickle cells and the vascularendothelium The result is a longer transit time of sickle cellsin the capillary system [1ndash3] Some of the molecules involvedin these interactions have been identified for example CD47 basal cell adhesion molecule-1Lutheran (B-CAM-1Lu)intercellular cell adhesionmolecule 4 (ICAM-4) [3ndash5] In thispaper we focused on 120572
4(CD 49d) 120573
1(CD 29) integrin or
very late activation antigen (VLA) 4 and CD 36 which areexclusively present on stress reticulocytes [1ndash5]
Hydroxyurea (HU) is a cancer chemotherapy agent thatdecreases the frequency of SCA crises HUmay exert its ther-apeutic effect by generating nitric oxide (anti-inflammatory)and increasing the level of antisickling fetal hemoglobin(Hb F) [3 5 6] Higher levels of Hb F result in clinicallymilder sickle cell disease [3 6] HU also led to a significantdecrease in the expression of the CD 36 CD 49d and CD 29genes [7]
Lee et al [8] and Trinh-Trang-Tan et al [9] found that thepresence or absence of CD 36 had no effect on the clinicalmanifestations of SCA Browne and Hebbel [2] and Styles etal [3] had a completely different point of view
InCote drsquoIvoire the frequency ofHb S hovers around 14with 2 of major forms [10] HU is not part of the armamen-tarium used for the treatment of sickle cell patients Patients
Hindawi Publishing CorporationAdvances in HematologyVolume 2014 Article ID 273860 6 pageshttpdxdoiorg1011552014273860
2 Advances in Hematology
exclusively treated in Cote drsquoIvoire have never received HUMaintenance treatment is based on folic acid and vasodilators[10] Crises are treated by nonsteroidal anti-inflammatorydrugs particularly ketoprofen [10 11]
It is not common to find studies with a populationcomposed only of SS patients clearly showing the results ofthe subjects in steady state or in crisisThis is whywe set a goalto investigate whether the clinical status namely the crisis orthe steady state had an impact on total reticulocytes stressreticulocytes and the expression of adhesion molecules andCD 36 and CD 49 d in SS black African patients never treatedby HU in Abidjan
2 Materials and Methods
This was a cross-sectional study carried out in the centrallaboratory and in the Department of Clinical Hematologyof the University Hospital of Yopougon in Abidjan Thestudy population consisted of 60 SCA (Hb SS) patients whoprovided their informed consent for participation of these30 were in steady state and 30 were in crisis Steady state wasdefined by a period of at least 1 month since the patientrsquoslast crisis [8 12] Patients had been exclusively treated inCote drsquoIvoire They never had received HU We did notinclude subjects who were transfused in the three monthspreceding the investigation If the samples were hemolyzed ifthey contained clot or if the immunophenotyping tests werenot perform within 48 h the patients were not also selected[8 12]The samples were taken as soon as the patients in crisiswere admitted the first day of the hospitalization
Blood was collected by venipuncture performed at theelbow in a tube containing an anticoagulant the Ethylen-diaminetetraacetic acid (EDTA) We performed a completeblood count with Sysmex XT-2000i analyzer The deter-mination of the rate of reticulocytes and their degree ofmaturity was performed with immunophenotyping by flowcytometry with the FACSCalibur Flow Cytometer BectonDickinson We used the same device to demonstrate the CD36 and CD 49d antigens on the surface of reticulocytes Atleast 20 000 cells were analyzed on each samples We usedthe following reagents anti-CD 36 monoclonal antibodiescoupled to fluorescein isothiocyanate (FITC) IgM isotopekappa (FITC) anti-CD 49d monoclonal antibodies coupledto phycoerythrin (PE) IgG1 isotype kappa (PE) Retic-Countor thiazole orange saline phosphate bovine serum albuminand the fragment F (ab1015840) 2 IgG1 [3 8]
The distribution of reticulocytes according to the degreeof maturity with thiazole orange can be subdivided intomature reticulocytes (low fluorescence area or LFR) in retic-ulocytes of intermediate maturity (moderate fluorescencearea or MFR) and in very immature reticulocytes (highfluorescence region or HFR) Stress reticulocytes correspondto the immature reticulocytes fraction (IRF) constituted bythe sum of reticulocytes MFR and HFR [13] The meanfluorescence intensity (MFI) was also measured
VLA-4 is composed of CD 49d (1205724integrin) and CD 29
(1205731integrin) Both components weremeasured by Styles et al
[3] using flow cytometryThey found that that the expression
of CD 49d and CD 29 were virtually identical On this basiswe only sought the expression of CD 49d [3]
Data were compared using Studentrsquos 119905-test or Chi-Squaretest A 119875 value lt005 indicated a significant difference
3 Results
60 SS patients (32 male and 28 female) were studied Theaverage age was 1512 plusmn 1057 (2ndash43 years) We separatedpatients according to clinical status crisis or steady state(Table 1) Patients in crisis or in steady state had a similardistributionwith regard to age sex ratio and theHb fractions(Table 1) On the other hand in terms of clinical historysubjects in crisis had had a longer length of hospital stay anda higher number of transfusions (119875 lt 005) than subjects insteady state Clinical status had an impact on most elementsof the complete blood count (Table 1) Severe anemia andleukocytosis with neutrophilia were the highlights of thecomplete blood count (Table 1)
Subjects in crisis had statistically significantly moretotal reticulocytes (absolute and relative values) and veryimmature reticulocytes HFR than subjects in steady state(Table 2)
All patients (6060) had expressed CD 49d on thereticulocytes The distribution according to the degree ofmaturity was similar during the crisis or the steady state Veryimmature cells predominated (Table 3)
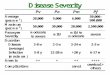
80 (4860) of patients expressed the CD 36 The meanfluorescence intensity (MFI) for the stress reticulocytes was120 plusmn 10 whereas for the more mature reticulocytes MFI itwas lower (35 plusmn 7) Stress reticulocytes were strongly stainedThe relative and absolute rates of CD 36+ reticulocytes werehigher in crisis than in steady state (Table 4) Steady state wasassociated with an increase of CD 36+ intermediate maturityreticulocytes Immature reticulocytes valuewas higher for theSS patients in crisis (Table 4)
4 Comments
Data on age and sex were similar to the other studies carriedout in Abidjan which stressed that sickle cell patients weremostly teenagers or young male adults [10 11]
Clinical history showed that patients who were recruitedwhen they were in crisis receivedmore transfusions and werehospitalized longer (Table 1) The frequency of painful crisesrequiring hospitalization and the length of hospital stay areclinical criteria used to assess the severity of SCA Platt et al[14] showed that the number of painful episodes in a year isa measure of the clinical severity of the disease and that itis associated with early death especially in patients over 20years
Indeed SCA is associated with an abnormal inflamma-tory reaction which is even more important during crises[4 10 12] Since thework of Sangare et al [10] that has demon-strated the beneficial effect of nonsteroidal anti-inflammatorydrugs ketoprofen is used for treating seizures in AbidjanIt is associated with a vasodilator pentoxifylline This anti-inflammatory drug shortened significantly and without any
Advances in Hematology 3
Table 1 Influence of clinical status on epidemiological clinical and biological parameters
Parameters Painful crisis (119899 = 30) Steady state (119899 = 30)119875
m plusmn sd (minndashmax) m plusmn sd (minndashmax)Age 139 plusmn 9 (2ndash37) 164 plusmn 119 (2ndash43) 0364Sex (MF) 114 114 0795Number of crisesyear 25 plusmn 101 (1ndash4) 23 plusmn 084 (1ndash4) 0406Hospitalization daysyear 14 plusmn 101 (0ndash6) 047 plusmn 063 (0ndash2) 00002Transfusionsyear 093 plusmn 052 (0ndash2) 043 plusmn 05 (0-1) 00004Hb S () 868 plusmn 57 (76ndash95) 861 plusmn 45 (736ndash936) 0622Hb F () 188 plusmn 51 (25ndash232) 115 plusmn 44 (39ndash236) 0595Hb A2 () 23 plusmn 101 (1ndash4) 24 plusmn 06 (15ndash42) 0599Red blood cells120583L 2 011 000 plusmn 698 000 2 593 000 plusmn 605 000 0001Hemoglobin (gdL) 564 plusmn 181 698 plusmn 147 00024Hematocrit () 1783 plusmn 512 2101 plusmn 403 001Mean cell volume (fL) 9102 plusmn 1094 8242 plusmn 1109 0004MCH (pg) 2843 plusmn 315 2732 plusmn 384 0224MCHC () 3132 plusmn 222 3315 plusmn 157 00005Leukocytes120583L 23 778 plusmn 13 038 14 206 plusmn 11 515 0004Neutrophils120583L 13 046 plusmn 6 685 5 838 plusmn 3 013 10minus6
Platelets120583L 323 133 plusmn 159 263 407 867 plusmn 173 572 053m plusmn sd (minndashmax) mean plusmn standard deviation (minimumndashmaximum)MCV mean cell volumeMVH mean cell hemoglobinMCHC mean cell hemoglobin concentration119875 Studentrsquos 119905-test
Table 2 Distribution of reticulocytes according to their degree of maturity and to the clinical status
Parameters Painful crisis (119899 = 30) Steady state (119899 = 30)119875
m plusmn sd m plusmn sdTotal reticulocytes () 155 plusmn 10 84 plusmn 49 0003Total reticulocytes (120583L) 283 678 plusmn 153 711 200 721 plusmn 10 708 0002LFR 515 plusmn 159 566 plusmn 75 03MFR 379 plusmn 10 367 plusmn 54 018HFR () 107 plusmn 99 67 plusmn 35 0012IRF () 486 plusmn 159 434 plusmn 75 03m plusmn sd mean plusmn standard deviation119875 Chi-Square testLFR low fluorescence reticulocytes or mature reticulocytesMFR medium fluorescence reticulocytes or semimature reticulocytesHFR high fluorescence reticulocytes or immature reticulocytesIRF index reticulocytes fraction or stress reticulocytes (MFR + HFR)
side effects the duration of sickle cell crisis and had an effectgreater than that of a major opioid analgesic Patients neverhad been treated by HU
The clinical status namely the vasoocclusive crisis hadan impact on almost all parameters of the complete bloodcount except for the level of platelets (Table 1) The completeblood count has demonstrated abnormalities commonly de-scribed as severe anemia and leukocytosis [3 8 10 15] Inthe patients followed in the present study a higher leukocytecount in the peripheral circulation and infections wereshown Infections related to the increase of white blood cellswere often associated with the occurrence of vasoocclusiveepisodes Sluggish flow increased transit time hypoxia and
therefore sickling may be due to the probable interactionbetween sickle cells and leukocytes in the microcirculation[5] A newmultistepmodel for vasoocclusion in sickle diseaseis thus proposed In this model sickle cells or secondaryinflammatory stimuli induced endothelial activation lead-ing to recruitment of adherent leukocytes These leuko-cytes interacted with red blood sickle cells thus hamperingmicrovascular blood flow In the end sickle cells are trappedleading to vasoocclusion as shown by Frenette [16]
The values of total reticulocytes (Table 2) were closeto the results of other authors such as Styles et al [3]Lee et al [8] and Maier-Redelsperger et al [15] whichhighlighted a hyperreticulocytosis ranging from 259 000120583L
4 Advances in Hematology
Table 3 Profile of CD 49d+ reticulocytes according to their degree of maturity and the clinical status
CD 49d+ patients
Parameters Painful crisis (119899 = 30) Steady state (119899 = 30)119875
m plusmn sd m plusmn sdTotal reticulocytes () 441 plusmn 177 409 plusmn 77 013Total reticulocytes (120583L) 134 604 plusmn 108 223 83 782 plusmn 54 222 006LFR 99 plusmn 196 58 plusmn 21 091MFR 264 plusmn 85 284 plusmn 65 08HFR () 637 plusmn 181 658 plusmn 76 019IRF () 901 plusmn 196 942 plusmn 21 065m plusmn sd mean plusmn standard deviation119875 Chi-Square testLFR low fluorescence reticulocytes or mature reticulocytesMFR medium fluorescence reticulocytes or semimature reticulocytesHFR high fluorescence reticulocytes or immature reticulocytesIRF index reticulocytes fraction or stress reticulocytes (MFR + HFR)
Table 4 Distribution of CD 36+ reticulocytes according to their degree of maturity and the clinical status
CD 36+ patients
Parameters Painful crisis (119899 = 23) Steady state (119899 = 25)119875
m plusmn sd m plusmn sdTotal reticulocytes () 534 plusmn 143 461 plusmn 114 0006Total reticulocytes (120583L) 214 870 plusmn 107 584 144 878 plusmn 115 024 10minus5
LFR 92 plusmn 74 89 plusmn 64 032MFR 619 plusmn 89 681 plusmn 62 0001HFR () 289 plusmn 79 23 plusmn 64 0002IRF () 908 plusmn 74 912 plusmn 64 03m plusmn sd mean plusmn standard deviation119875 Chi-Square testLFR low fluorescence reticulocytes or mature reticulocytesMFR medium fluorescence reticulocytes or semimature reticulocytesHFR high fluorescence reticulocytes or immature reticulocytesIRF index reticulocytes fraction or stress reticulocytes (MFR + HFR)
[8] to 320 000120583L [3 15] Crisis resulted in a statisticallysignificant increase in relative and absolute values of totalreticulocytes (Table 2) On the other hand the clinical statushad no effect on the rate of stress reticulocytes (IFR) whichwas high This result was surprising but it could be possiblethat some biological alterations still persisted at one monthafter the crisis even if the patients were in steady state
Among the stress reticulocytes the fraction of veryimmature cells was higher during crises than during steadystate (107 plusmn 99 versus 67 plusmn 35 119875 = 004) These valueswere lower than those of Maier-Redelsperger et al [15] whofound a frequency of 13 for very immature reticulocytes inSS patients [15] Hebbel [1] was the first to show in 1980 thatthe red blood cells of SS patients had pathological adhesionto vascular endothelium J L Wautier and M P Wautier [17]also noted that the adhesion was more important if the bloodwas collected in the vaso-occlusive crisis According to Trinh-Trang-Tan et al [9] reticulocytes which are more abundantand express more adhesion molecules may contribute to thehyperadhesiveness
We only sought the expression of CD 49d which was pos-itive for all patients (Table 2) The percentage of reticulocytesexpressing CD 49d was 441 plusmn 177 for the painful crisis and409 plusmn 77 for the steady state (Table 3) The difference wasnot significant (119875 = 037) Styles et al [3] also found that thecrisis or stationary phase did not influence the relative valueof CD 49d+ reticulocytes However our results were higherthan those of Styles et al [3] and Lee et al [8] Styles et al [3]had found that the percentage of reticulocytes expressing CD49d was 290 plusmn 59 that is 129 000 plusmn 39 000120583L Lee et al[8] showed that 22 plusmn 2 reticulocytes carried CD 49d Thesehigh rates could be explained by the fact that the subjects weselected were much more anemic
For CD 36+ subjects the level of total reticulocytes was534 plusmn 143 for subjects in crisis and 461 plusmn 114 forsubjects in steady state (Table 4) These results differed fromthose of Lee et al [8] who only found 24 plusmn 81 CD 36+reticulocytes They were close to those of Styles et al [3]with 553 plusmn 64 CD 36+ reticulocytes before HU treatmentBrowne and Hebbel [2] obtained 398 plusmn 219 for the total
Advances in Hematology 5
reticulocytes of CD 36+ patients This value was lower thanthe results of Lee [8] but higher than the percentage given byStyles et al [3]
We investigated SCApatients who never receivedHUWecompared the results with authors [3 8] who had worked onSS patients treated by HU It is well documented that HUdecreases CD 49d and CD 36 expression even after months[3 8] In fact Lee et al [8] collected the samples before theintroduction of HU treatment Styles et al [3] followed theSCA patients from the onset of therapy with HU
According to Styles et al [3] we found that CD 36expression on reticulocytes was higher than that of CD49d Nevertheless these authors emphasized that adhesionmediated by VLA-4 or 120572
4(CD 49d) 120573
1(CD 29) integrin
would be more tenacious than that involving the CD 36 [3]The contribution of CD 36 has been called into question
with the finding that sickle cell patients who have a CD 36deficiency of reticulocytes and mature red blood cells canhave a normal clinical course [8 9] Trinh-Trang-Tan et al[9] showed that there is dissociation between adhesivenessand adhesion molecules It is therefore conceivable that CD36 although in reduced amounts might be activated byabnormal constitutive phosphorylation [9]
Blood flow is compromised in sickle microcirculationUnder low flow sickle cell adherence to endotheliumincreasedwith contact time in the absence of endothelial acti-vation or adhesive protein addition Contact time betweensickle cells and endothelium seemed a more importantdeterminant of adherence than high-affinity receptor-ligandinteractions [18]
The signalization cascade leading to receptor activationrather than the expression level only of adhesion moleculesshould also play an important role in the adhesion of sicklecells to the blood vessels [4]
5 Conclusion
In SCA the clinical statusmdashcrisis or steady statemdashhad animpact on the clinical history namely the number of hospitaldays and the number of transfusions Anemia leukocytosisand total and immature reticulocytes were higher in patientsin crisis than those in steady state There was no differencebetween subjects in crisis and those in steady state for CD49d+ reticulocytes Concerning the CD 36+ subjects thecrisis had resulted in an increase in total reticulocytes andvery immature reticulocytes
SCA is the result of complex mechanism involvingadhesion molecules such as CD 49d and CD 36 There isa correlation between the adhesion systems and the stressreticulocytes However these facts are not sufficient to predictthe occurrence and severity of sickle cell crisis
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
References
[1] R P Hebbel M A B Boogaerts J W Eaton and M HSteinberg ldquoErythrocyte adherence to endothelium in sickle-cellanemia A possible determinant of disease severityrdquo The NewEngland Journal of Medicine vol 302 no 18 pp 992ndash995 1980
[2] P V Browne and R P Hebbel ldquoCD36-positive stress reticulo-cytosis in sickle cell anemiardquo Journal of Laboratory and ClinicalMedicine vol 127 no 4 pp 340ndash347 1996
[3] L A Styles B Lubin E Vichinsky et al ldquoDecrease of verylate activation antigen-4 and CD36 on reticulocytes in sicklecell patients treated with hydroxyureardquo Blood vol 89 no 7 pp2554ndash2559 1997
[4] J-P Cartron and J Elion ldquoErythroid adhesion molecules insickle cell disease effect of hydroxyureardquo Transfusion Cliniqueet Biologique vol 15 no 1-2 pp 39ndash50 2008
[5] D K Kau E Finnegan and G A Barabino ldquoSickle red cell-endothelium interactionsrdquo Microcirculation vol 16 no 1 pp97ndash111 2009
[6] S Charache M L Terrin R D Moore et al ldquoEffect ofhydroxyurea on the frequency of painful crises in Sickle cellanemiardquoThe New England Journal of Medicine vol 332 no 20pp 1317ndash1322 1995
[7] S Gambero A A Canalli F Traina et al ldquoTherapy withhydroxyurea is associatedwith reduced adhesionmolecule geneand protein expression in sickle red cells with a concomitantreduction in adhesive propertiesrdquo European Journal of Haema-tology vol 78 no 2 pp 144ndash151 2007
[8] K Lee P Gane F Roudot-Thoraval et al ldquoThe nonexpressionof CD36 on reticulocytes and mature red blood cells does notmodify the clinical course of patients with sickle cell anemiardquoBlood vol 98 no 4 pp 966ndash971 2001
[9] M-M Trinh-Trang-Tan C Vilela-Lamego J Picot M-P Wau-tier and J-P Cartron ldquoIntercellular adhesion molecule-4 andCD36 are implicated in the abnormal adhesiveness of sickle cellSAD mouse erythrocytes to endotheliumrdquo Haematologica vol95 no 5 pp 730ndash737 2010
[10] A Sangare K G Koffi O Allangba et al ldquoEtude comparativedu Ketoprofene et de la Buprenorphine dans le traitement descrises douloureuses drepanocytairesrdquoMedecine drsquoAfrique Noirevol 44 pp 138ndash143 1998
[11] A Tolo-Diebkile K G Koffi D C Nanho et al ldquoDrepanocy-tose homozygote chez lrsquoadulte ivoirien de plus de 21 ansrdquoCahiersdrsquoEtudes et de Recherches FrancophonesSante vol 20 pp 63ndash672010
[12] A A Solovey A N Solovey J Harkness and R P HebbelldquoModulation of endothelial cell activation in sickle cell diseasea pilot studyrdquo Blood vol 97 no 7 pp 1937ndash1941 2001
[13] B H Davis M DiCorato N C Bigelow andM H LangweilerldquoProposal for standardization of flow cytometric reticulocytematurity index (RMI) measurementsrdquo Cytometry vol 14 no 3pp 318ndash326 1993
[14] O S Platt B DThorington D J Brambilla et al ldquoPain in sicklecell diseasemdashrates and risk factorsrdquoTheNew England Journal ofMedicine vol 325 no 1 pp 11ndash16 1991
[15] M Maier-Redelsperger A Flahault M G Neonato R Girotand D Labie ldquoAutomated analysis of mature red blood cells andreticulocytes in SS and SC diseaserdquo Blood Cells Molecules andDiseases vol 33 no 1 pp 15ndash24 2004
[16] P S Frenette ldquoSickle cell vaso-occlusion multistep and multi-cellular paradigmrdquo Current Opinion in Hematology vol 9 no2 pp 101ndash106 2002
6 Advances in Hematology
[17] J L Wautier and M P Wautier ldquoMolecular basis of erythrocyteadhesion to endothelial cells in diseasesrdquoClinical Hemorheologyand Microcirculation vol 53 pp 11ndash21 2013
[18] R A OMontes J R Eckman L L Hsu and TMWick ldquoSickleerythrocyte adherence to endothelium at low shear role ofshear stress in propagation of vaso-occlusionrdquoAmerican Journalof Hematology vol 70 no 3 pp 216ndash227 2002
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

2 Advances in Hematology
exclusively treated in Cote drsquoIvoire have never received HUMaintenance treatment is based on folic acid and vasodilators[10] Crises are treated by nonsteroidal anti-inflammatorydrugs particularly ketoprofen [10 11]
It is not common to find studies with a populationcomposed only of SS patients clearly showing the results ofthe subjects in steady state or in crisisThis is whywe set a goalto investigate whether the clinical status namely the crisis orthe steady state had an impact on total reticulocytes stressreticulocytes and the expression of adhesion molecules andCD 36 and CD 49 d in SS black African patients never treatedby HU in Abidjan
2 Materials and Methods
This was a cross-sectional study carried out in the centrallaboratory and in the Department of Clinical Hematologyof the University Hospital of Yopougon in Abidjan Thestudy population consisted of 60 SCA (Hb SS) patients whoprovided their informed consent for participation of these30 were in steady state and 30 were in crisis Steady state wasdefined by a period of at least 1 month since the patientrsquoslast crisis [8 12] Patients had been exclusively treated inCote drsquoIvoire They never had received HU We did notinclude subjects who were transfused in the three monthspreceding the investigation If the samples were hemolyzed ifthey contained clot or if the immunophenotyping tests werenot perform within 48 h the patients were not also selected[8 12]The samples were taken as soon as the patients in crisiswere admitted the first day of the hospitalization
Blood was collected by venipuncture performed at theelbow in a tube containing an anticoagulant the Ethylen-diaminetetraacetic acid (EDTA) We performed a completeblood count with Sysmex XT-2000i analyzer The deter-mination of the rate of reticulocytes and their degree ofmaturity was performed with immunophenotyping by flowcytometry with the FACSCalibur Flow Cytometer BectonDickinson We used the same device to demonstrate the CD36 and CD 49d antigens on the surface of reticulocytes Atleast 20 000 cells were analyzed on each samples We usedthe following reagents anti-CD 36 monoclonal antibodiescoupled to fluorescein isothiocyanate (FITC) IgM isotopekappa (FITC) anti-CD 49d monoclonal antibodies coupledto phycoerythrin (PE) IgG1 isotype kappa (PE) Retic-Countor thiazole orange saline phosphate bovine serum albuminand the fragment F (ab1015840) 2 IgG1 [3 8]
The distribution of reticulocytes according to the degreeof maturity with thiazole orange can be subdivided intomature reticulocytes (low fluorescence area or LFR) in retic-ulocytes of intermediate maturity (moderate fluorescencearea or MFR) and in very immature reticulocytes (highfluorescence region or HFR) Stress reticulocytes correspondto the immature reticulocytes fraction (IRF) constituted bythe sum of reticulocytes MFR and HFR [13] The meanfluorescence intensity (MFI) was also measured
VLA-4 is composed of CD 49d (1205724integrin) and CD 29
(1205731integrin) Both components weremeasured by Styles et al
[3] using flow cytometryThey found that that the expression
of CD 49d and CD 29 were virtually identical On this basiswe only sought the expression of CD 49d [3]
Data were compared using Studentrsquos 119905-test or Chi-Squaretest A 119875 value lt005 indicated a significant difference
3 Results
60 SS patients (32 male and 28 female) were studied Theaverage age was 1512 plusmn 1057 (2ndash43 years) We separatedpatients according to clinical status crisis or steady state(Table 1) Patients in crisis or in steady state had a similardistributionwith regard to age sex ratio and theHb fractions(Table 1) On the other hand in terms of clinical historysubjects in crisis had had a longer length of hospital stay anda higher number of transfusions (119875 lt 005) than subjects insteady state Clinical status had an impact on most elementsof the complete blood count (Table 1) Severe anemia andleukocytosis with neutrophilia were the highlights of thecomplete blood count (Table 1)
Subjects in crisis had statistically significantly moretotal reticulocytes (absolute and relative values) and veryimmature reticulocytes HFR than subjects in steady state(Table 2)
All patients (6060) had expressed CD 49d on thereticulocytes The distribution according to the degree ofmaturity was similar during the crisis or the steady state Veryimmature cells predominated (Table 3)
80 (4860) of patients expressed the CD 36 The meanfluorescence intensity (MFI) for the stress reticulocytes was120 plusmn 10 whereas for the more mature reticulocytes MFI itwas lower (35 plusmn 7) Stress reticulocytes were strongly stainedThe relative and absolute rates of CD 36+ reticulocytes werehigher in crisis than in steady state (Table 4) Steady state wasassociated with an increase of CD 36+ intermediate maturityreticulocytes Immature reticulocytes valuewas higher for theSS patients in crisis (Table 4)
4 Comments
Data on age and sex were similar to the other studies carriedout in Abidjan which stressed that sickle cell patients weremostly teenagers or young male adults [10 11]
Clinical history showed that patients who were recruitedwhen they were in crisis receivedmore transfusions and werehospitalized longer (Table 1) The frequency of painful crisesrequiring hospitalization and the length of hospital stay areclinical criteria used to assess the severity of SCA Platt et al[14] showed that the number of painful episodes in a year isa measure of the clinical severity of the disease and that itis associated with early death especially in patients over 20years
Indeed SCA is associated with an abnormal inflamma-tory reaction which is even more important during crises[4 10 12] Since thework of Sangare et al [10] that has demon-strated the beneficial effect of nonsteroidal anti-inflammatorydrugs ketoprofen is used for treating seizures in AbidjanIt is associated with a vasodilator pentoxifylline This anti-inflammatory drug shortened significantly and without any
Advances in Hematology 3
Table 1 Influence of clinical status on epidemiological clinical and biological parameters
Parameters Painful crisis (119899 = 30) Steady state (119899 = 30)119875
m plusmn sd (minndashmax) m plusmn sd (minndashmax)Age 139 plusmn 9 (2ndash37) 164 plusmn 119 (2ndash43) 0364Sex (MF) 114 114 0795Number of crisesyear 25 plusmn 101 (1ndash4) 23 plusmn 084 (1ndash4) 0406Hospitalization daysyear 14 plusmn 101 (0ndash6) 047 plusmn 063 (0ndash2) 00002Transfusionsyear 093 plusmn 052 (0ndash2) 043 plusmn 05 (0-1) 00004Hb S () 868 plusmn 57 (76ndash95) 861 plusmn 45 (736ndash936) 0622Hb F () 188 plusmn 51 (25ndash232) 115 plusmn 44 (39ndash236) 0595Hb A2 () 23 plusmn 101 (1ndash4) 24 plusmn 06 (15ndash42) 0599Red blood cells120583L 2 011 000 plusmn 698 000 2 593 000 plusmn 605 000 0001Hemoglobin (gdL) 564 plusmn 181 698 plusmn 147 00024Hematocrit () 1783 plusmn 512 2101 plusmn 403 001Mean cell volume (fL) 9102 plusmn 1094 8242 plusmn 1109 0004MCH (pg) 2843 plusmn 315 2732 plusmn 384 0224MCHC () 3132 plusmn 222 3315 plusmn 157 00005Leukocytes120583L 23 778 plusmn 13 038 14 206 plusmn 11 515 0004Neutrophils120583L 13 046 plusmn 6 685 5 838 plusmn 3 013 10minus6
Platelets120583L 323 133 plusmn 159 263 407 867 plusmn 173 572 053m plusmn sd (minndashmax) mean plusmn standard deviation (minimumndashmaximum)MCV mean cell volumeMVH mean cell hemoglobinMCHC mean cell hemoglobin concentration119875 Studentrsquos 119905-test
Table 2 Distribution of reticulocytes according to their degree of maturity and to the clinical status
Parameters Painful crisis (119899 = 30) Steady state (119899 = 30)119875
m plusmn sd m plusmn sdTotal reticulocytes () 155 plusmn 10 84 plusmn 49 0003Total reticulocytes (120583L) 283 678 plusmn 153 711 200 721 plusmn 10 708 0002LFR 515 plusmn 159 566 plusmn 75 03MFR 379 plusmn 10 367 plusmn 54 018HFR () 107 plusmn 99 67 plusmn 35 0012IRF () 486 plusmn 159 434 plusmn 75 03m plusmn sd mean plusmn standard deviation119875 Chi-Square testLFR low fluorescence reticulocytes or mature reticulocytesMFR medium fluorescence reticulocytes or semimature reticulocytesHFR high fluorescence reticulocytes or immature reticulocytesIRF index reticulocytes fraction or stress reticulocytes (MFR + HFR)
side effects the duration of sickle cell crisis and had an effectgreater than that of a major opioid analgesic Patients neverhad been treated by HU
The clinical status namely the vasoocclusive crisis hadan impact on almost all parameters of the complete bloodcount except for the level of platelets (Table 1) The completeblood count has demonstrated abnormalities commonly de-scribed as severe anemia and leukocytosis [3 8 10 15] Inthe patients followed in the present study a higher leukocytecount in the peripheral circulation and infections wereshown Infections related to the increase of white blood cellswere often associated with the occurrence of vasoocclusiveepisodes Sluggish flow increased transit time hypoxia and
therefore sickling may be due to the probable interactionbetween sickle cells and leukocytes in the microcirculation[5] A newmultistepmodel for vasoocclusion in sickle diseaseis thus proposed In this model sickle cells or secondaryinflammatory stimuli induced endothelial activation lead-ing to recruitment of adherent leukocytes These leuko-cytes interacted with red blood sickle cells thus hamperingmicrovascular blood flow In the end sickle cells are trappedleading to vasoocclusion as shown by Frenette [16]
The values of total reticulocytes (Table 2) were closeto the results of other authors such as Styles et al [3]Lee et al [8] and Maier-Redelsperger et al [15] whichhighlighted a hyperreticulocytosis ranging from 259 000120583L
4 Advances in Hematology
Table 3 Profile of CD 49d+ reticulocytes according to their degree of maturity and the clinical status
CD 49d+ patients
Parameters Painful crisis (119899 = 30) Steady state (119899 = 30)119875
m plusmn sd m plusmn sdTotal reticulocytes () 441 plusmn 177 409 plusmn 77 013Total reticulocytes (120583L) 134 604 plusmn 108 223 83 782 plusmn 54 222 006LFR 99 plusmn 196 58 plusmn 21 091MFR 264 plusmn 85 284 plusmn 65 08HFR () 637 plusmn 181 658 plusmn 76 019IRF () 901 plusmn 196 942 plusmn 21 065m plusmn sd mean plusmn standard deviation119875 Chi-Square testLFR low fluorescence reticulocytes or mature reticulocytesMFR medium fluorescence reticulocytes or semimature reticulocytesHFR high fluorescence reticulocytes or immature reticulocytesIRF index reticulocytes fraction or stress reticulocytes (MFR + HFR)
Table 4 Distribution of CD 36+ reticulocytes according to their degree of maturity and the clinical status
CD 36+ patients
Parameters Painful crisis (119899 = 23) Steady state (119899 = 25)119875
m plusmn sd m plusmn sdTotal reticulocytes () 534 plusmn 143 461 plusmn 114 0006Total reticulocytes (120583L) 214 870 plusmn 107 584 144 878 plusmn 115 024 10minus5
LFR 92 plusmn 74 89 plusmn 64 032MFR 619 plusmn 89 681 plusmn 62 0001HFR () 289 plusmn 79 23 plusmn 64 0002IRF () 908 plusmn 74 912 plusmn 64 03m plusmn sd mean plusmn standard deviation119875 Chi-Square testLFR low fluorescence reticulocytes or mature reticulocytesMFR medium fluorescence reticulocytes or semimature reticulocytesHFR high fluorescence reticulocytes or immature reticulocytesIRF index reticulocytes fraction or stress reticulocytes (MFR + HFR)
[8] to 320 000120583L [3 15] Crisis resulted in a statisticallysignificant increase in relative and absolute values of totalreticulocytes (Table 2) On the other hand the clinical statushad no effect on the rate of stress reticulocytes (IFR) whichwas high This result was surprising but it could be possiblethat some biological alterations still persisted at one monthafter the crisis even if the patients were in steady state
Among the stress reticulocytes the fraction of veryimmature cells was higher during crises than during steadystate (107 plusmn 99 versus 67 plusmn 35 119875 = 004) These valueswere lower than those of Maier-Redelsperger et al [15] whofound a frequency of 13 for very immature reticulocytes inSS patients [15] Hebbel [1] was the first to show in 1980 thatthe red blood cells of SS patients had pathological adhesionto vascular endothelium J L Wautier and M P Wautier [17]also noted that the adhesion was more important if the bloodwas collected in the vaso-occlusive crisis According to Trinh-Trang-Tan et al [9] reticulocytes which are more abundantand express more adhesion molecules may contribute to thehyperadhesiveness
We only sought the expression of CD 49d which was pos-itive for all patients (Table 2) The percentage of reticulocytesexpressing CD 49d was 441 plusmn 177 for the painful crisis and409 plusmn 77 for the steady state (Table 3) The difference wasnot significant (119875 = 037) Styles et al [3] also found that thecrisis or stationary phase did not influence the relative valueof CD 49d+ reticulocytes However our results were higherthan those of Styles et al [3] and Lee et al [8] Styles et al [3]had found that the percentage of reticulocytes expressing CD49d was 290 plusmn 59 that is 129 000 plusmn 39 000120583L Lee et al[8] showed that 22 plusmn 2 reticulocytes carried CD 49d Thesehigh rates could be explained by the fact that the subjects weselected were much more anemic
For CD 36+ subjects the level of total reticulocytes was534 plusmn 143 for subjects in crisis and 461 plusmn 114 forsubjects in steady state (Table 4) These results differed fromthose of Lee et al [8] who only found 24 plusmn 81 CD 36+reticulocytes They were close to those of Styles et al [3]with 553 plusmn 64 CD 36+ reticulocytes before HU treatmentBrowne and Hebbel [2] obtained 398 plusmn 219 for the total
Advances in Hematology 5
reticulocytes of CD 36+ patients This value was lower thanthe results of Lee [8] but higher than the percentage given byStyles et al [3]
We investigated SCApatients who never receivedHUWecompared the results with authors [3 8] who had worked onSS patients treated by HU It is well documented that HUdecreases CD 49d and CD 36 expression even after months[3 8] In fact Lee et al [8] collected the samples before theintroduction of HU treatment Styles et al [3] followed theSCA patients from the onset of therapy with HU
According to Styles et al [3] we found that CD 36expression on reticulocytes was higher than that of CD49d Nevertheless these authors emphasized that adhesionmediated by VLA-4 or 120572
4(CD 49d) 120573
1(CD 29) integrin
would be more tenacious than that involving the CD 36 [3]The contribution of CD 36 has been called into question
with the finding that sickle cell patients who have a CD 36deficiency of reticulocytes and mature red blood cells canhave a normal clinical course [8 9] Trinh-Trang-Tan et al[9] showed that there is dissociation between adhesivenessand adhesion molecules It is therefore conceivable that CD36 although in reduced amounts might be activated byabnormal constitutive phosphorylation [9]
Blood flow is compromised in sickle microcirculationUnder low flow sickle cell adherence to endotheliumincreasedwith contact time in the absence of endothelial acti-vation or adhesive protein addition Contact time betweensickle cells and endothelium seemed a more importantdeterminant of adherence than high-affinity receptor-ligandinteractions [18]
The signalization cascade leading to receptor activationrather than the expression level only of adhesion moleculesshould also play an important role in the adhesion of sicklecells to the blood vessels [4]
5 Conclusion
In SCA the clinical statusmdashcrisis or steady statemdashhad animpact on the clinical history namely the number of hospitaldays and the number of transfusions Anemia leukocytosisand total and immature reticulocytes were higher in patientsin crisis than those in steady state There was no differencebetween subjects in crisis and those in steady state for CD49d+ reticulocytes Concerning the CD 36+ subjects thecrisis had resulted in an increase in total reticulocytes andvery immature reticulocytes
SCA is the result of complex mechanism involvingadhesion molecules such as CD 49d and CD 36 There isa correlation between the adhesion systems and the stressreticulocytes However these facts are not sufficient to predictthe occurrence and severity of sickle cell crisis
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
References
[1] R P Hebbel M A B Boogaerts J W Eaton and M HSteinberg ldquoErythrocyte adherence to endothelium in sickle-cellanemia A possible determinant of disease severityrdquo The NewEngland Journal of Medicine vol 302 no 18 pp 992ndash995 1980
[2] P V Browne and R P Hebbel ldquoCD36-positive stress reticulo-cytosis in sickle cell anemiardquo Journal of Laboratory and ClinicalMedicine vol 127 no 4 pp 340ndash347 1996
[3] L A Styles B Lubin E Vichinsky et al ldquoDecrease of verylate activation antigen-4 and CD36 on reticulocytes in sicklecell patients treated with hydroxyureardquo Blood vol 89 no 7 pp2554ndash2559 1997
[4] J-P Cartron and J Elion ldquoErythroid adhesion molecules insickle cell disease effect of hydroxyureardquo Transfusion Cliniqueet Biologique vol 15 no 1-2 pp 39ndash50 2008
[5] D K Kau E Finnegan and G A Barabino ldquoSickle red cell-endothelium interactionsrdquo Microcirculation vol 16 no 1 pp97ndash111 2009
[6] S Charache M L Terrin R D Moore et al ldquoEffect ofhydroxyurea on the frequency of painful crises in Sickle cellanemiardquoThe New England Journal of Medicine vol 332 no 20pp 1317ndash1322 1995
[7] S Gambero A A Canalli F Traina et al ldquoTherapy withhydroxyurea is associatedwith reduced adhesionmolecule geneand protein expression in sickle red cells with a concomitantreduction in adhesive propertiesrdquo European Journal of Haema-tology vol 78 no 2 pp 144ndash151 2007
[8] K Lee P Gane F Roudot-Thoraval et al ldquoThe nonexpressionof CD36 on reticulocytes and mature red blood cells does notmodify the clinical course of patients with sickle cell anemiardquoBlood vol 98 no 4 pp 966ndash971 2001
[9] M-M Trinh-Trang-Tan C Vilela-Lamego J Picot M-P Wau-tier and J-P Cartron ldquoIntercellular adhesion molecule-4 andCD36 are implicated in the abnormal adhesiveness of sickle cellSAD mouse erythrocytes to endotheliumrdquo Haematologica vol95 no 5 pp 730ndash737 2010
[10] A Sangare K G Koffi O Allangba et al ldquoEtude comparativedu Ketoprofene et de la Buprenorphine dans le traitement descrises douloureuses drepanocytairesrdquoMedecine drsquoAfrique Noirevol 44 pp 138ndash143 1998
[11] A Tolo-Diebkile K G Koffi D C Nanho et al ldquoDrepanocy-tose homozygote chez lrsquoadulte ivoirien de plus de 21 ansrdquoCahiersdrsquoEtudes et de Recherches FrancophonesSante vol 20 pp 63ndash672010
[12] A A Solovey A N Solovey J Harkness and R P HebbelldquoModulation of endothelial cell activation in sickle cell diseasea pilot studyrdquo Blood vol 97 no 7 pp 1937ndash1941 2001
[13] B H Davis M DiCorato N C Bigelow andM H LangweilerldquoProposal for standardization of flow cytometric reticulocytematurity index (RMI) measurementsrdquo Cytometry vol 14 no 3pp 318ndash326 1993
[14] O S Platt B DThorington D J Brambilla et al ldquoPain in sicklecell diseasemdashrates and risk factorsrdquoTheNew England Journal ofMedicine vol 325 no 1 pp 11ndash16 1991
[15] M Maier-Redelsperger A Flahault M G Neonato R Girotand D Labie ldquoAutomated analysis of mature red blood cells andreticulocytes in SS and SC diseaserdquo Blood Cells Molecules andDiseases vol 33 no 1 pp 15ndash24 2004
[16] P S Frenette ldquoSickle cell vaso-occlusion multistep and multi-cellular paradigmrdquo Current Opinion in Hematology vol 9 no2 pp 101ndash106 2002
6 Advances in Hematology
[17] J L Wautier and M P Wautier ldquoMolecular basis of erythrocyteadhesion to endothelial cells in diseasesrdquoClinical Hemorheologyand Microcirculation vol 53 pp 11ndash21 2013
[18] R A OMontes J R Eckman L L Hsu and TMWick ldquoSickleerythrocyte adherence to endothelium at low shear role ofshear stress in propagation of vaso-occlusionrdquoAmerican Journalof Hematology vol 70 no 3 pp 216ndash227 2002
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

Advances in Hematology 3
Table 1 Influence of clinical status on epidemiological clinical and biological parameters
Parameters Painful crisis (119899 = 30) Steady state (119899 = 30)119875
m plusmn sd (minndashmax) m plusmn sd (minndashmax)Age 139 plusmn 9 (2ndash37) 164 plusmn 119 (2ndash43) 0364Sex (MF) 114 114 0795Number of crisesyear 25 plusmn 101 (1ndash4) 23 plusmn 084 (1ndash4) 0406Hospitalization daysyear 14 plusmn 101 (0ndash6) 047 plusmn 063 (0ndash2) 00002Transfusionsyear 093 plusmn 052 (0ndash2) 043 plusmn 05 (0-1) 00004Hb S () 868 plusmn 57 (76ndash95) 861 plusmn 45 (736ndash936) 0622Hb F () 188 plusmn 51 (25ndash232) 115 plusmn 44 (39ndash236) 0595Hb A2 () 23 plusmn 101 (1ndash4) 24 plusmn 06 (15ndash42) 0599Red blood cells120583L 2 011 000 plusmn 698 000 2 593 000 plusmn 605 000 0001Hemoglobin (gdL) 564 plusmn 181 698 plusmn 147 00024Hematocrit () 1783 plusmn 512 2101 plusmn 403 001Mean cell volume (fL) 9102 plusmn 1094 8242 plusmn 1109 0004MCH (pg) 2843 plusmn 315 2732 plusmn 384 0224MCHC () 3132 plusmn 222 3315 plusmn 157 00005Leukocytes120583L 23 778 plusmn 13 038 14 206 plusmn 11 515 0004Neutrophils120583L 13 046 plusmn 6 685 5 838 plusmn 3 013 10minus6
Platelets120583L 323 133 plusmn 159 263 407 867 plusmn 173 572 053m plusmn sd (minndashmax) mean plusmn standard deviation (minimumndashmaximum)MCV mean cell volumeMVH mean cell hemoglobinMCHC mean cell hemoglobin concentration119875 Studentrsquos 119905-test
Table 2 Distribution of reticulocytes according to their degree of maturity and to the clinical status
Parameters Painful crisis (119899 = 30) Steady state (119899 = 30)119875
m plusmn sd m plusmn sdTotal reticulocytes () 155 plusmn 10 84 plusmn 49 0003Total reticulocytes (120583L) 283 678 plusmn 153 711 200 721 plusmn 10 708 0002LFR 515 plusmn 159 566 plusmn 75 03MFR 379 plusmn 10 367 plusmn 54 018HFR () 107 plusmn 99 67 plusmn 35 0012IRF () 486 plusmn 159 434 plusmn 75 03m plusmn sd mean plusmn standard deviation119875 Chi-Square testLFR low fluorescence reticulocytes or mature reticulocytesMFR medium fluorescence reticulocytes or semimature reticulocytesHFR high fluorescence reticulocytes or immature reticulocytesIRF index reticulocytes fraction or stress reticulocytes (MFR + HFR)
side effects the duration of sickle cell crisis and had an effectgreater than that of a major opioid analgesic Patients neverhad been treated by HU
The clinical status namely the vasoocclusive crisis hadan impact on almost all parameters of the complete bloodcount except for the level of platelets (Table 1) The completeblood count has demonstrated abnormalities commonly de-scribed as severe anemia and leukocytosis [3 8 10 15] Inthe patients followed in the present study a higher leukocytecount in the peripheral circulation and infections wereshown Infections related to the increase of white blood cellswere often associated with the occurrence of vasoocclusiveepisodes Sluggish flow increased transit time hypoxia and
therefore sickling may be due to the probable interactionbetween sickle cells and leukocytes in the microcirculation[5] A newmultistepmodel for vasoocclusion in sickle diseaseis thus proposed In this model sickle cells or secondaryinflammatory stimuli induced endothelial activation lead-ing to recruitment of adherent leukocytes These leuko-cytes interacted with red blood sickle cells thus hamperingmicrovascular blood flow In the end sickle cells are trappedleading to vasoocclusion as shown by Frenette [16]
The values of total reticulocytes (Table 2) were closeto the results of other authors such as Styles et al [3]Lee et al [8] and Maier-Redelsperger et al [15] whichhighlighted a hyperreticulocytosis ranging from 259 000120583L
4 Advances in Hematology
Table 3 Profile of CD 49d+ reticulocytes according to their degree of maturity and the clinical status
CD 49d+ patients
Parameters Painful crisis (119899 = 30) Steady state (119899 = 30)119875
m plusmn sd m plusmn sdTotal reticulocytes () 441 plusmn 177 409 plusmn 77 013Total reticulocytes (120583L) 134 604 plusmn 108 223 83 782 plusmn 54 222 006LFR 99 plusmn 196 58 plusmn 21 091MFR 264 plusmn 85 284 plusmn 65 08HFR () 637 plusmn 181 658 plusmn 76 019IRF () 901 plusmn 196 942 plusmn 21 065m plusmn sd mean plusmn standard deviation119875 Chi-Square testLFR low fluorescence reticulocytes or mature reticulocytesMFR medium fluorescence reticulocytes or semimature reticulocytesHFR high fluorescence reticulocytes or immature reticulocytesIRF index reticulocytes fraction or stress reticulocytes (MFR + HFR)
Table 4 Distribution of CD 36+ reticulocytes according to their degree of maturity and the clinical status
CD 36+ patients
Parameters Painful crisis (119899 = 23) Steady state (119899 = 25)119875
m plusmn sd m plusmn sdTotal reticulocytes () 534 plusmn 143 461 plusmn 114 0006Total reticulocytes (120583L) 214 870 plusmn 107 584 144 878 plusmn 115 024 10minus5
LFR 92 plusmn 74 89 plusmn 64 032MFR 619 plusmn 89 681 plusmn 62 0001HFR () 289 plusmn 79 23 plusmn 64 0002IRF () 908 plusmn 74 912 plusmn 64 03m plusmn sd mean plusmn standard deviation119875 Chi-Square testLFR low fluorescence reticulocytes or mature reticulocytesMFR medium fluorescence reticulocytes or semimature reticulocytesHFR high fluorescence reticulocytes or immature reticulocytesIRF index reticulocytes fraction or stress reticulocytes (MFR + HFR)
[8] to 320 000120583L [3 15] Crisis resulted in a statisticallysignificant increase in relative and absolute values of totalreticulocytes (Table 2) On the other hand the clinical statushad no effect on the rate of stress reticulocytes (IFR) whichwas high This result was surprising but it could be possiblethat some biological alterations still persisted at one monthafter the crisis even if the patients were in steady state
Among the stress reticulocytes the fraction of veryimmature cells was higher during crises than during steadystate (107 plusmn 99 versus 67 plusmn 35 119875 = 004) These valueswere lower than those of Maier-Redelsperger et al [15] whofound a frequency of 13 for very immature reticulocytes inSS patients [15] Hebbel [1] was the first to show in 1980 thatthe red blood cells of SS patients had pathological adhesionto vascular endothelium J L Wautier and M P Wautier [17]also noted that the adhesion was more important if the bloodwas collected in the vaso-occlusive crisis According to Trinh-Trang-Tan et al [9] reticulocytes which are more abundantand express more adhesion molecules may contribute to thehyperadhesiveness
We only sought the expression of CD 49d which was pos-itive for all patients (Table 2) The percentage of reticulocytesexpressing CD 49d was 441 plusmn 177 for the painful crisis and409 plusmn 77 for the steady state (Table 3) The difference wasnot significant (119875 = 037) Styles et al [3] also found that thecrisis or stationary phase did not influence the relative valueof CD 49d+ reticulocytes However our results were higherthan those of Styles et al [3] and Lee et al [8] Styles et al [3]had found that the percentage of reticulocytes expressing CD49d was 290 plusmn 59 that is 129 000 plusmn 39 000120583L Lee et al[8] showed that 22 plusmn 2 reticulocytes carried CD 49d Thesehigh rates could be explained by the fact that the subjects weselected were much more anemic
For CD 36+ subjects the level of total reticulocytes was534 plusmn 143 for subjects in crisis and 461 plusmn 114 forsubjects in steady state (Table 4) These results differed fromthose of Lee et al [8] who only found 24 plusmn 81 CD 36+reticulocytes They were close to those of Styles et al [3]with 553 plusmn 64 CD 36+ reticulocytes before HU treatmentBrowne and Hebbel [2] obtained 398 plusmn 219 for the total
Advances in Hematology 5
reticulocytes of CD 36+ patients This value was lower thanthe results of Lee [8] but higher than the percentage given byStyles et al [3]
We investigated SCApatients who never receivedHUWecompared the results with authors [3 8] who had worked onSS patients treated by HU It is well documented that HUdecreases CD 49d and CD 36 expression even after months[3 8] In fact Lee et al [8] collected the samples before theintroduction of HU treatment Styles et al [3] followed theSCA patients from the onset of therapy with HU
According to Styles et al [3] we found that CD 36expression on reticulocytes was higher than that of CD49d Nevertheless these authors emphasized that adhesionmediated by VLA-4 or 120572
4(CD 49d) 120573
1(CD 29) integrin
would be more tenacious than that involving the CD 36 [3]The contribution of CD 36 has been called into question
with the finding that sickle cell patients who have a CD 36deficiency of reticulocytes and mature red blood cells canhave a normal clinical course [8 9] Trinh-Trang-Tan et al[9] showed that there is dissociation between adhesivenessand adhesion molecules It is therefore conceivable that CD36 although in reduced amounts might be activated byabnormal constitutive phosphorylation [9]
Blood flow is compromised in sickle microcirculationUnder low flow sickle cell adherence to endotheliumincreasedwith contact time in the absence of endothelial acti-vation or adhesive protein addition Contact time betweensickle cells and endothelium seemed a more importantdeterminant of adherence than high-affinity receptor-ligandinteractions [18]
The signalization cascade leading to receptor activationrather than the expression level only of adhesion moleculesshould also play an important role in the adhesion of sicklecells to the blood vessels [4]
5 Conclusion
In SCA the clinical statusmdashcrisis or steady statemdashhad animpact on the clinical history namely the number of hospitaldays and the number of transfusions Anemia leukocytosisand total and immature reticulocytes were higher in patientsin crisis than those in steady state There was no differencebetween subjects in crisis and those in steady state for CD49d+ reticulocytes Concerning the CD 36+ subjects thecrisis had resulted in an increase in total reticulocytes andvery immature reticulocytes
SCA is the result of complex mechanism involvingadhesion molecules such as CD 49d and CD 36 There isa correlation between the adhesion systems and the stressreticulocytes However these facts are not sufficient to predictthe occurrence and severity of sickle cell crisis
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
References
[1] R P Hebbel M A B Boogaerts J W Eaton and M HSteinberg ldquoErythrocyte adherence to endothelium in sickle-cellanemia A possible determinant of disease severityrdquo The NewEngland Journal of Medicine vol 302 no 18 pp 992ndash995 1980
[2] P V Browne and R P Hebbel ldquoCD36-positive stress reticulo-cytosis in sickle cell anemiardquo Journal of Laboratory and ClinicalMedicine vol 127 no 4 pp 340ndash347 1996
[3] L A Styles B Lubin E Vichinsky et al ldquoDecrease of verylate activation antigen-4 and CD36 on reticulocytes in sicklecell patients treated with hydroxyureardquo Blood vol 89 no 7 pp2554ndash2559 1997
[4] J-P Cartron and J Elion ldquoErythroid adhesion molecules insickle cell disease effect of hydroxyureardquo Transfusion Cliniqueet Biologique vol 15 no 1-2 pp 39ndash50 2008
[5] D K Kau E Finnegan and G A Barabino ldquoSickle red cell-endothelium interactionsrdquo Microcirculation vol 16 no 1 pp97ndash111 2009
[6] S Charache M L Terrin R D Moore et al ldquoEffect ofhydroxyurea on the frequency of painful crises in Sickle cellanemiardquoThe New England Journal of Medicine vol 332 no 20pp 1317ndash1322 1995
[7] S Gambero A A Canalli F Traina et al ldquoTherapy withhydroxyurea is associatedwith reduced adhesionmolecule geneand protein expression in sickle red cells with a concomitantreduction in adhesive propertiesrdquo European Journal of Haema-tology vol 78 no 2 pp 144ndash151 2007
[8] K Lee P Gane F Roudot-Thoraval et al ldquoThe nonexpressionof CD36 on reticulocytes and mature red blood cells does notmodify the clinical course of patients with sickle cell anemiardquoBlood vol 98 no 4 pp 966ndash971 2001
[9] M-M Trinh-Trang-Tan C Vilela-Lamego J Picot M-P Wau-tier and J-P Cartron ldquoIntercellular adhesion molecule-4 andCD36 are implicated in the abnormal adhesiveness of sickle cellSAD mouse erythrocytes to endotheliumrdquo Haematologica vol95 no 5 pp 730ndash737 2010
[10] A Sangare K G Koffi O Allangba et al ldquoEtude comparativedu Ketoprofene et de la Buprenorphine dans le traitement descrises douloureuses drepanocytairesrdquoMedecine drsquoAfrique Noirevol 44 pp 138ndash143 1998
[11] A Tolo-Diebkile K G Koffi D C Nanho et al ldquoDrepanocy-tose homozygote chez lrsquoadulte ivoirien de plus de 21 ansrdquoCahiersdrsquoEtudes et de Recherches FrancophonesSante vol 20 pp 63ndash672010
[12] A A Solovey A N Solovey J Harkness and R P HebbelldquoModulation of endothelial cell activation in sickle cell diseasea pilot studyrdquo Blood vol 97 no 7 pp 1937ndash1941 2001
[13] B H Davis M DiCorato N C Bigelow andM H LangweilerldquoProposal for standardization of flow cytometric reticulocytematurity index (RMI) measurementsrdquo Cytometry vol 14 no 3pp 318ndash326 1993
[14] O S Platt B DThorington D J Brambilla et al ldquoPain in sicklecell diseasemdashrates and risk factorsrdquoTheNew England Journal ofMedicine vol 325 no 1 pp 11ndash16 1991
[15] M Maier-Redelsperger A Flahault M G Neonato R Girotand D Labie ldquoAutomated analysis of mature red blood cells andreticulocytes in SS and SC diseaserdquo Blood Cells Molecules andDiseases vol 33 no 1 pp 15ndash24 2004
[16] P S Frenette ldquoSickle cell vaso-occlusion multistep and multi-cellular paradigmrdquo Current Opinion in Hematology vol 9 no2 pp 101ndash106 2002
6 Advances in Hematology
[17] J L Wautier and M P Wautier ldquoMolecular basis of erythrocyteadhesion to endothelial cells in diseasesrdquoClinical Hemorheologyand Microcirculation vol 53 pp 11ndash21 2013
[18] R A OMontes J R Eckman L L Hsu and TMWick ldquoSickleerythrocyte adherence to endothelium at low shear role ofshear stress in propagation of vaso-occlusionrdquoAmerican Journalof Hematology vol 70 no 3 pp 216ndash227 2002
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

4 Advances in Hematology
Table 3 Profile of CD 49d+ reticulocytes according to their degree of maturity and the clinical status
CD 49d+ patients
Parameters Painful crisis (119899 = 30) Steady state (119899 = 30)119875
m plusmn sd m plusmn sdTotal reticulocytes () 441 plusmn 177 409 plusmn 77 013Total reticulocytes (120583L) 134 604 plusmn 108 223 83 782 plusmn 54 222 006LFR 99 plusmn 196 58 plusmn 21 091MFR 264 plusmn 85 284 plusmn 65 08HFR () 637 plusmn 181 658 plusmn 76 019IRF () 901 plusmn 196 942 plusmn 21 065m plusmn sd mean plusmn standard deviation119875 Chi-Square testLFR low fluorescence reticulocytes or mature reticulocytesMFR medium fluorescence reticulocytes or semimature reticulocytesHFR high fluorescence reticulocytes or immature reticulocytesIRF index reticulocytes fraction or stress reticulocytes (MFR + HFR)
Table 4 Distribution of CD 36+ reticulocytes according to their degree of maturity and the clinical status
CD 36+ patients
Parameters Painful crisis (119899 = 23) Steady state (119899 = 25)119875
m plusmn sd m plusmn sdTotal reticulocytes () 534 plusmn 143 461 plusmn 114 0006Total reticulocytes (120583L) 214 870 plusmn 107 584 144 878 plusmn 115 024 10minus5
LFR 92 plusmn 74 89 plusmn 64 032MFR 619 plusmn 89 681 plusmn 62 0001HFR () 289 plusmn 79 23 plusmn 64 0002IRF () 908 plusmn 74 912 plusmn 64 03m plusmn sd mean plusmn standard deviation119875 Chi-Square testLFR low fluorescence reticulocytes or mature reticulocytesMFR medium fluorescence reticulocytes or semimature reticulocytesHFR high fluorescence reticulocytes or immature reticulocytesIRF index reticulocytes fraction or stress reticulocytes (MFR + HFR)
[8] to 320 000120583L [3 15] Crisis resulted in a statisticallysignificant increase in relative and absolute values of totalreticulocytes (Table 2) On the other hand the clinical statushad no effect on the rate of stress reticulocytes (IFR) whichwas high This result was surprising but it could be possiblethat some biological alterations still persisted at one monthafter the crisis even if the patients were in steady state
Among the stress reticulocytes the fraction of veryimmature cells was higher during crises than during steadystate (107 plusmn 99 versus 67 plusmn 35 119875 = 004) These valueswere lower than those of Maier-Redelsperger et al [15] whofound a frequency of 13 for very immature reticulocytes inSS patients [15] Hebbel [1] was the first to show in 1980 thatthe red blood cells of SS patients had pathological adhesionto vascular endothelium J L Wautier and M P Wautier [17]also noted that the adhesion was more important if the bloodwas collected in the vaso-occlusive crisis According to Trinh-Trang-Tan et al [9] reticulocytes which are more abundantand express more adhesion molecules may contribute to thehyperadhesiveness
We only sought the expression of CD 49d which was pos-itive for all patients (Table 2) The percentage of reticulocytesexpressing CD 49d was 441 plusmn 177 for the painful crisis and409 plusmn 77 for the steady state (Table 3) The difference wasnot significant (119875 = 037) Styles et al [3] also found that thecrisis or stationary phase did not influence the relative valueof CD 49d+ reticulocytes However our results were higherthan those of Styles et al [3] and Lee et al [8] Styles et al [3]had found that the percentage of reticulocytes expressing CD49d was 290 plusmn 59 that is 129 000 plusmn 39 000120583L Lee et al[8] showed that 22 plusmn 2 reticulocytes carried CD 49d Thesehigh rates could be explained by the fact that the subjects weselected were much more anemic
For CD 36+ subjects the level of total reticulocytes was534 plusmn 143 for subjects in crisis and 461 plusmn 114 forsubjects in steady state (Table 4) These results differed fromthose of Lee et al [8] who only found 24 plusmn 81 CD 36+reticulocytes They were close to those of Styles et al [3]with 553 plusmn 64 CD 36+ reticulocytes before HU treatmentBrowne and Hebbel [2] obtained 398 plusmn 219 for the total
Advances in Hematology 5
reticulocytes of CD 36+ patients This value was lower thanthe results of Lee [8] but higher than the percentage given byStyles et al [3]
We investigated SCApatients who never receivedHUWecompared the results with authors [3 8] who had worked onSS patients treated by HU It is well documented that HUdecreases CD 49d and CD 36 expression even after months[3 8] In fact Lee et al [8] collected the samples before theintroduction of HU treatment Styles et al [3] followed theSCA patients from the onset of therapy with HU
According to Styles et al [3] we found that CD 36expression on reticulocytes was higher than that of CD49d Nevertheless these authors emphasized that adhesionmediated by VLA-4 or 120572
4(CD 49d) 120573
1(CD 29) integrin
would be more tenacious than that involving the CD 36 [3]The contribution of CD 36 has been called into question
with the finding that sickle cell patients who have a CD 36deficiency of reticulocytes and mature red blood cells canhave a normal clinical course [8 9] Trinh-Trang-Tan et al[9] showed that there is dissociation between adhesivenessand adhesion molecules It is therefore conceivable that CD36 although in reduced amounts might be activated byabnormal constitutive phosphorylation [9]
Blood flow is compromised in sickle microcirculationUnder low flow sickle cell adherence to endotheliumincreasedwith contact time in the absence of endothelial acti-vation or adhesive protein addition Contact time betweensickle cells and endothelium seemed a more importantdeterminant of adherence than high-affinity receptor-ligandinteractions [18]
The signalization cascade leading to receptor activationrather than the expression level only of adhesion moleculesshould also play an important role in the adhesion of sicklecells to the blood vessels [4]
5 Conclusion
In SCA the clinical statusmdashcrisis or steady statemdashhad animpact on the clinical history namely the number of hospitaldays and the number of transfusions Anemia leukocytosisand total and immature reticulocytes were higher in patientsin crisis than those in steady state There was no differencebetween subjects in crisis and those in steady state for CD49d+ reticulocytes Concerning the CD 36+ subjects thecrisis had resulted in an increase in total reticulocytes andvery immature reticulocytes
SCA is the result of complex mechanism involvingadhesion molecules such as CD 49d and CD 36 There isa correlation between the adhesion systems and the stressreticulocytes However these facts are not sufficient to predictthe occurrence and severity of sickle cell crisis
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
References
[1] R P Hebbel M A B Boogaerts J W Eaton and M HSteinberg ldquoErythrocyte adherence to endothelium in sickle-cellanemia A possible determinant of disease severityrdquo The NewEngland Journal of Medicine vol 302 no 18 pp 992ndash995 1980
[2] P V Browne and R P Hebbel ldquoCD36-positive stress reticulo-cytosis in sickle cell anemiardquo Journal of Laboratory and ClinicalMedicine vol 127 no 4 pp 340ndash347 1996
[3] L A Styles B Lubin E Vichinsky et al ldquoDecrease of verylate activation antigen-4 and CD36 on reticulocytes in sicklecell patients treated with hydroxyureardquo Blood vol 89 no 7 pp2554ndash2559 1997
[4] J-P Cartron and J Elion ldquoErythroid adhesion molecules insickle cell disease effect of hydroxyureardquo Transfusion Cliniqueet Biologique vol 15 no 1-2 pp 39ndash50 2008
[5] D K Kau E Finnegan and G A Barabino ldquoSickle red cell-endothelium interactionsrdquo Microcirculation vol 16 no 1 pp97ndash111 2009
[6] S Charache M L Terrin R D Moore et al ldquoEffect ofhydroxyurea on the frequency of painful crises in Sickle cellanemiardquoThe New England Journal of Medicine vol 332 no 20pp 1317ndash1322 1995
[7] S Gambero A A Canalli F Traina et al ldquoTherapy withhydroxyurea is associatedwith reduced adhesionmolecule geneand protein expression in sickle red cells with a concomitantreduction in adhesive propertiesrdquo European Journal of Haema-tology vol 78 no 2 pp 144ndash151 2007
[8] K Lee P Gane F Roudot-Thoraval et al ldquoThe nonexpressionof CD36 on reticulocytes and mature red blood cells does notmodify the clinical course of patients with sickle cell anemiardquoBlood vol 98 no 4 pp 966ndash971 2001
[9] M-M Trinh-Trang-Tan C Vilela-Lamego J Picot M-P Wau-tier and J-P Cartron ldquoIntercellular adhesion molecule-4 andCD36 are implicated in the abnormal adhesiveness of sickle cellSAD mouse erythrocytes to endotheliumrdquo Haematologica vol95 no 5 pp 730ndash737 2010
[10] A Sangare K G Koffi O Allangba et al ldquoEtude comparativedu Ketoprofene et de la Buprenorphine dans le traitement descrises douloureuses drepanocytairesrdquoMedecine drsquoAfrique Noirevol 44 pp 138ndash143 1998
[11] A Tolo-Diebkile K G Koffi D C Nanho et al ldquoDrepanocy-tose homozygote chez lrsquoadulte ivoirien de plus de 21 ansrdquoCahiersdrsquoEtudes et de Recherches FrancophonesSante vol 20 pp 63ndash672010
[12] A A Solovey A N Solovey J Harkness and R P HebbelldquoModulation of endothelial cell activation in sickle cell diseasea pilot studyrdquo Blood vol 97 no 7 pp 1937ndash1941 2001
[13] B H Davis M DiCorato N C Bigelow andM H LangweilerldquoProposal for standardization of flow cytometric reticulocytematurity index (RMI) measurementsrdquo Cytometry vol 14 no 3pp 318ndash326 1993
[14] O S Platt B DThorington D J Brambilla et al ldquoPain in sicklecell diseasemdashrates and risk factorsrdquoTheNew England Journal ofMedicine vol 325 no 1 pp 11ndash16 1991
[15] M Maier-Redelsperger A Flahault M G Neonato R Girotand D Labie ldquoAutomated analysis of mature red blood cells andreticulocytes in SS and SC diseaserdquo Blood Cells Molecules andDiseases vol 33 no 1 pp 15ndash24 2004
[16] P S Frenette ldquoSickle cell vaso-occlusion multistep and multi-cellular paradigmrdquo Current Opinion in Hematology vol 9 no2 pp 101ndash106 2002
6 Advances in Hematology
[17] J L Wautier and M P Wautier ldquoMolecular basis of erythrocyteadhesion to endothelial cells in diseasesrdquoClinical Hemorheologyand Microcirculation vol 53 pp 11ndash21 2013
[18] R A OMontes J R Eckman L L Hsu and TMWick ldquoSickleerythrocyte adherence to endothelium at low shear role ofshear stress in propagation of vaso-occlusionrdquoAmerican Journalof Hematology vol 70 no 3 pp 216ndash227 2002
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

Advances in Hematology 5
reticulocytes of CD 36+ patients This value was lower thanthe results of Lee [8] but higher than the percentage given byStyles et al [3]
We investigated SCApatients who never receivedHUWecompared the results with authors [3 8] who had worked onSS patients treated by HU It is well documented that HUdecreases CD 49d and CD 36 expression even after months[3 8] In fact Lee et al [8] collected the samples before theintroduction of HU treatment Styles et al [3] followed theSCA patients from the onset of therapy with HU
According to Styles et al [3] we found that CD 36expression on reticulocytes was higher than that of CD49d Nevertheless these authors emphasized that adhesionmediated by VLA-4 or 120572
4(CD 49d) 120573
1(CD 29) integrin
would be more tenacious than that involving the CD 36 [3]The contribution of CD 36 has been called into question
with the finding that sickle cell patients who have a CD 36deficiency of reticulocytes and mature red blood cells canhave a normal clinical course [8 9] Trinh-Trang-Tan et al[9] showed that there is dissociation between adhesivenessand adhesion molecules It is therefore conceivable that CD36 although in reduced amounts might be activated byabnormal constitutive phosphorylation [9]
Blood flow is compromised in sickle microcirculationUnder low flow sickle cell adherence to endotheliumincreasedwith contact time in the absence of endothelial acti-vation or adhesive protein addition Contact time betweensickle cells and endothelium seemed a more importantdeterminant of adherence than high-affinity receptor-ligandinteractions [18]
The signalization cascade leading to receptor activationrather than the expression level only of adhesion moleculesshould also play an important role in the adhesion of sicklecells to the blood vessels [4]
5 Conclusion
In SCA the clinical statusmdashcrisis or steady statemdashhad animpact on the clinical history namely the number of hospitaldays and the number of transfusions Anemia leukocytosisand total and immature reticulocytes were higher in patientsin crisis than those in steady state There was no differencebetween subjects in crisis and those in steady state for CD49d+ reticulocytes Concerning the CD 36+ subjects thecrisis had resulted in an increase in total reticulocytes andvery immature reticulocytes
SCA is the result of complex mechanism involvingadhesion molecules such as CD 49d and CD 36 There isa correlation between the adhesion systems and the stressreticulocytes However these facts are not sufficient to predictthe occurrence and severity of sickle cell crisis
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
References
[1] R P Hebbel M A B Boogaerts J W Eaton and M HSteinberg ldquoErythrocyte adherence to endothelium in sickle-cellanemia A possible determinant of disease severityrdquo The NewEngland Journal of Medicine vol 302 no 18 pp 992ndash995 1980
[2] P V Browne and R P Hebbel ldquoCD36-positive stress reticulo-cytosis in sickle cell anemiardquo Journal of Laboratory and ClinicalMedicine vol 127 no 4 pp 340ndash347 1996
[3] L A Styles B Lubin E Vichinsky et al ldquoDecrease of verylate activation antigen-4 and CD36 on reticulocytes in sicklecell patients treated with hydroxyureardquo Blood vol 89 no 7 pp2554ndash2559 1997
[4] J-P Cartron and J Elion ldquoErythroid adhesion molecules insickle cell disease effect of hydroxyureardquo Transfusion Cliniqueet Biologique vol 15 no 1-2 pp 39ndash50 2008
[5] D K Kau E Finnegan and G A Barabino ldquoSickle red cell-endothelium interactionsrdquo Microcirculation vol 16 no 1 pp97ndash111 2009
[6] S Charache M L Terrin R D Moore et al ldquoEffect ofhydroxyurea on the frequency of painful crises in Sickle cellanemiardquoThe New England Journal of Medicine vol 332 no 20pp 1317ndash1322 1995
[7] S Gambero A A Canalli F Traina et al ldquoTherapy withhydroxyurea is associatedwith reduced adhesionmolecule geneand protein expression in sickle red cells with a concomitantreduction in adhesive propertiesrdquo European Journal of Haema-tology vol 78 no 2 pp 144ndash151 2007
[8] K Lee P Gane F Roudot-Thoraval et al ldquoThe nonexpressionof CD36 on reticulocytes and mature red blood cells does notmodify the clinical course of patients with sickle cell anemiardquoBlood vol 98 no 4 pp 966ndash971 2001
[9] M-M Trinh-Trang-Tan C Vilela-Lamego J Picot M-P Wau-tier and J-P Cartron ldquoIntercellular adhesion molecule-4 andCD36 are implicated in the abnormal adhesiveness of sickle cellSAD mouse erythrocytes to endotheliumrdquo Haematologica vol95 no 5 pp 730ndash737 2010
[10] A Sangare K G Koffi O Allangba et al ldquoEtude comparativedu Ketoprofene et de la Buprenorphine dans le traitement descrises douloureuses drepanocytairesrdquoMedecine drsquoAfrique Noirevol 44 pp 138ndash143 1998
[11] A Tolo-Diebkile K G Koffi D C Nanho et al ldquoDrepanocy-tose homozygote chez lrsquoadulte ivoirien de plus de 21 ansrdquoCahiersdrsquoEtudes et de Recherches FrancophonesSante vol 20 pp 63ndash672010
[12] A A Solovey A N Solovey J Harkness and R P HebbelldquoModulation of endothelial cell activation in sickle cell diseasea pilot studyrdquo Blood vol 97 no 7 pp 1937ndash1941 2001
[13] B H Davis M DiCorato N C Bigelow andM H LangweilerldquoProposal for standardization of flow cytometric reticulocytematurity index (RMI) measurementsrdquo Cytometry vol 14 no 3pp 318ndash326 1993
[14] O S Platt B DThorington D J Brambilla et al ldquoPain in sicklecell diseasemdashrates and risk factorsrdquoTheNew England Journal ofMedicine vol 325 no 1 pp 11ndash16 1991
[15] M Maier-Redelsperger A Flahault M G Neonato R Girotand D Labie ldquoAutomated analysis of mature red blood cells andreticulocytes in SS and SC diseaserdquo Blood Cells Molecules andDiseases vol 33 no 1 pp 15ndash24 2004
[16] P S Frenette ldquoSickle cell vaso-occlusion multistep and multi-cellular paradigmrdquo Current Opinion in Hematology vol 9 no2 pp 101ndash106 2002
6 Advances in Hematology
[17] J L Wautier and M P Wautier ldquoMolecular basis of erythrocyteadhesion to endothelial cells in diseasesrdquoClinical Hemorheologyand Microcirculation vol 53 pp 11ndash21 2013
[18] R A OMontes J R Eckman L L Hsu and TMWick ldquoSickleerythrocyte adherence to endothelium at low shear role ofshear stress in propagation of vaso-occlusionrdquoAmerican Journalof Hematology vol 70 no 3 pp 216ndash227 2002
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

6 Advances in Hematology
[17] J L Wautier and M P Wautier ldquoMolecular basis of erythrocyteadhesion to endothelial cells in diseasesrdquoClinical Hemorheologyand Microcirculation vol 53 pp 11ndash21 2013
[18] R A OMontes J R Eckman L L Hsu and TMWick ldquoSickleerythrocyte adherence to endothelium at low shear role ofshear stress in propagation of vaso-occlusionrdquoAmerican Journalof Hematology vol 70 no 3 pp 216ndash227 2002
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom