Embed Size (px)
Citation preview

NATURE BIOTECHNOLOGY VOL 19 JANUARY 2001 http://biotech.nature.com 35
Malignant gliomas are highly aggressive tumors with a medianpatient survival time of 12–18 months1. They are characterized byrapidly dividing cells, invasion into normal brain, and a high degreeof vascularity. The histological grade of malignant gliomas, based onvascular proliferation, endothelial cell hyperplasia, and microvesselcount, has been shown to be inversely related to prognosis2.
Recent experimental evidence indicates that tumor-related angio-genesis contributes significantly to the malignant phenotype. Theconcept of angiogenesis-dependent tumor growth was introducedand experimentally demonstrated by Folkman and others3–8.Angiogenesis is a complex process that includes the activation, prolif-eration, and migration of endothelial cells. In tumorigenesis, thisprocess also involves disruption of the vascular basement membrane,formation of vascular tubes and networks, and linkage to preexistingvascular networks. Inhibition of these angiogenic processes may pro-vide a powerful approach to combat solid tumor growth. To date,several angiogenic inhibitors have been isolated and tested for theirability to inhibit brain tumors including platelet factor 4, TNP-40, heparin, penicillamine, hydrocortisone, and angiostatin9–15.Recently, O'Reilly et al. identified an endogenous specific inhibitor oftumor-related endothelial cell proliferation, endostatin16. Endostatinis a 20 kDa cleavage product of the C-terminal domain of collagenXVIII and was purified from murine hemangioendothelioma cells.
Human endostatin is rapidly cleared from the blood. To achievesignificant tumor regression, 2.5 mg/kg recombinant hES wasadministered once daily for 16 days in a Lewis lung carcinomamodel16. The quantities of protein needed for this therapy, the
purification procedure for large-scale production, and the attendantcosts of these processes, suggest that alternative delivery methodsmay be required for efficient therapeutic use of endostatin.Alginate–PLL microcapsules have been used extensively for differentapplications, particularly for the encapsulation of pancreatic isletcells and insulin delivery17,18. This method has also been used for theencapsulation of cells that release cytokines, hormones, and otheragents for gene therapy19–24. The alginate–PLL membranes allow thefree exchange of nutrients and oxygen between the implanted cellsand the host while preventing the escape and elimination of encap-sulated cells. More importantly, this approach provides a prolongedsustained delivery of recombinant protein produced by the cells,thus maintaining high levels of the agent.
In the present study, baby hamster kidney cells (BHK-21) engi-neered to continuously secrete high levels of hES were encapsulatedwith alginate PLL alginate (APA). The ability of this system tosecrete biologically active endostatin capable of inhibiting thegrowth of a human glioblastoma xenograft in the nude mouse wasinvestigated.
ResultsIn vitro expression and release of endostatin from encapsulatedBHK-21 cells. BHK-21 cells were transfected with a hES expressionvector (Fig. 1A), and clonal populations of stably transfected BHK-21 cells were obtained (BHK-endo). For these studies micro-capsules of 23 kDa PLL and 1.2% of ultrapure alginate with highguluronic acid content (>65%) were used. The microcapsules have
Continuous release of endostatin frommicroencapsulated engineered cells for
tumor therapyTatsuhiro Joki1,2,3 † , Marcelle Machluf4 †, Anthony Atala4, Jianhong Zhu1,2, Nicholas T. Seyfried1,2,
Ian F. Dunn1,2, Toshiaki Abe3, Rona S. Carroll1,2*, and Peter McL. Black1,2
1Brain Tumor Laboratory, Department of Neurosurgery, Department of Surgery, Brigham and Women’s Hospital, Harvard Medical School, Boston, MA 02115.2Children’s Hospital, Harvard Medical School, Boston, MA 02115. 3Department of Neurosurgery, Jikei University School of Medicine, Tokyo, Japan. 4Department of
Urology, The Children's Hospital, Harvard Medical School, Boston, MA 02115. *Corresponding author ([email protected]) †These authors contributed equally to this work.
Received 24 May 2000; accepted 18 September 2000
Research studies suggest that tumor-related angiogenesis contributes to the phenotype of malignantgliomas. We assessed the effect of local delivery of the angiogenesis inhibitor endostatin on humanglioma cell line (U-87MG) xenografts. Baby hamster kidney (BHK) cells were stably transfected with ahuman endostatin (hES) expression vector and were encapsulated in alginate-poly L-lysine (PLL) micro-capsules for long-term delivery of hES. The release of biologically active endostatin was confirmed usingassays of bovine capillary endothelial (BCE) proliferation and of tube formation. Human endostatinreleased from the microcapsules brought about a 67.2% inhibition of BCE proliferation. Furthermore,secreted hES was able to inhibit tube formation in KDR/PAE cells (porcine aortic endothelial cells stablytransfected with KDR, a tyrosine kinase) treated with conditioned U-87MG medium. A single local injec-tion of encapsulated endostatin-secreting cells in a nude mouse model resulted in a 72.3% reduction insubcutaneous U87 xenografts' weight 21 days post treatment. This inhibition was achieved by only 150.8 ng/ml human endostatin secreted from 2 × 105 encapsulated cells. Encapsulated endostatin-secreting cells are effective for the treatment of human glioblastoma xenografts. Continuous local deliv-ery of endostatin may offer an effective therapeutic approach to the treatment of a variety of tumor types.
Keywords: Endostatin, encapsulation, angiogenesis, glioma
RESEARCH ARTICLES©
2001
Nat
ure
Pu
blis
hin
g G
rou
p
htt
p:/
/bio
tech
.nat
ure
.co
m© 2001 Nature Publishing Group http://biotech.nature.com

an average diameter of 0.7 mm ± 0.08 mm (Fig. 1B). EncapsulatedBHK-endo cells and nonencapsulated BHK-endo cells were culturedin vitro, and the conditioned medium was collected every week forsix weeks. The encapsulated cells were viable in culture as deter-mined by MTT assay (see Experimental Protocol; data not shown).Western blot analysis of hES in the conditioned medium collected atall time points detected high levels of endostatin, as shown in Figure1C. In addition, an enzyme-linked immunosorbent assay (ELISA)was performed on medium collected weekly for six weeks from thecultured BHK-endo and BHK-neo capsules. The average concentra-tion of endostatin secreted by 2 × 105 cultured encapsulated BHK-endo cells over a six-week period was 150.2 ± 11.4 ng/ml/week.Similarly, cultured endostatin-transfected monolayer cells secretedhES at a concentration of 172.1 ± 19.0 ng/ml per 2 × 105 cells. Noendostatin protein was detected in media collected from the control,neomycin-resistant gene-transfected BHK-21 cells (BHK-neo).
Inhibition of bovine endothelial cell proliferation by endostatinsecreted from encapsulated BHK-endo cells. An endothelial cellproliferation assay was used to determine the biological activity ofrecombinant hES secreted from encapsulated BHK-endo cells.Transwells were used for these experiments to prevent direct contactbetween microcapsules and endothelial cells, thus eliminating thepossibility that the polymers would affect the proliferation rate.
Human endostatin released from microcapsules containingBHK-endo cells inhibited endothelial cell proliferation by threefoldwhen compared to medium alone or medium from microcapsulescontaining BHK-neo cells (Fig. 2A). These results indicate that theinhibition of endothelial cell proliferation is due to the secreted hES,and not to other factors that the BHK-21 cells may secrete.
Angiogenic assay with endostatin. A tube formation assay wasused to determine the biological activity of recombinant hES secret-ed from BHK-endo cells. Tumor cell-conditioned medium containsboth angiogenic and anti-angiogenic factors. The effect of the vari-ous growth factors in the conditioned medium on the proliferationand behavior of endothelial cells can be modified by using an addi-tional inhibitor, such as endostatin. KDR/PAE cells left untreated forfive days in appropriate medium (Ham’s F-12–10% fetal bovine
serum (FBS), condition 1, Fig. 2B-a) had no tube formation.Cells incubated with conditioned medium from BHK-neo cells(condition 2), followed by treatment with U87MG-conditioned medium, displayed spindle-like morphology.PAE/KDR cells formed tubelike structures (10 tubes/well) fourdays after U87MG-conditioned medium was added (condition2, Fig. 2B-b). KDR/PAE cells incubated for 1 h with condi-tioned medium from BHK-endo cells followed by incubationwith U87MG-conditioned media did not form tubelike struc-tures (condition 3, Fig. 2B-c). Thus secreted recombinant hESis able to inhibit U87MG-mediated tube formation.
Effects of encapsulated BHK-21 cells releasing endostatinon subcutaneous human glioma xenografts. Mice were inocu-lated with a right flank subcutaneous injection of U87MG cells.The tumors reached a size of 290.0 ± 65.8 mm3, 10 days postinoculation. The growth of U87MG glioma xenografts was sig-nificantly inhibited by a single dose of microcapsules contain-ing BHK-endo cells when compared to both control groups(Fig. 3A). In comparison to controls, the growth of the gliomatumors was suppressed by 62.2% by 21 days post administra-tion of the encapsulated BHK-endo cells. Tumors from thecontrol groups ulcerated within 30 days after initial tumorinjection, and animals were killed.
Animals were killed at 21 days post administration of theencapsulated cells, and tumors were harvested and weighed(Fig. 3B). Tumors taken from animals receiving microcapsulescontaining BHK-endo cells showed a 72.3% reduction in weightwhen compared to the control groups. Injected microcapsules
were harvested from animals and recultured for two weeks; the medi-um was positive for recombinant hES as measured by western blotanalysis (Fig. 4A). Tumor xenografts harvested from animals treatedwith BHK-endo capsules were positive for endostatin as measured bywestern blot analysis (Fig. 4B). No endostatin was detected in theBHK-neo-treated tumors. These experiments were conducted fourtimes, and the data were pooled for statistical analysis.
Immunohistochemistry. Tumors treated with BHK-endo cap-sules had less vascularization than tumors treated with BHK-neocapsules, as seen by hematoxylin and eosin (H&E) staining (Fig. 5A,B). This phenomenon was confirmed by CD31 immunohistochem-istry (Fig. 5 C, D). Furthermore, sections of tumors from BHK-neocapsules-treated mice were characterized by high microvessel densi-ty, as seen by von Willebrand factor (vWF) staining (Fig. 5E). In con-trast, tumors treated with BHK-endo capsules had significantlyfewer numbers of vessels (Table 1, Fig. 5F). The apoptotic index wassignificantly increased in tumors treated with BHK-endo cells (13.1)when compared to BHK-neo-treated tumor (3.7) using the TUNELmethod (Table 1; see Experimental Protocol). Proliferative indicesmeasured after staining for Ki-67 nuclear antigen revealed no differ-ences between tumors treated with BHK-endo capsule and BHK-neo capsule controls (data not shown).
DiscussionMalignant gliomas often recur locally within 2 cm of the originaltumor core25–27 and are rarely metastatic. Evidence suggests thattumor-related angiogenesis contributes to the malignant phenotypeof gliomas2. The finding that a reduction in angiogenesis of solid
36 NATURE BIOTECHNOLOGY VOL 19 JANUARY 2001 http://biotech.nature.com
RESEARCH ARTICLES
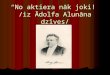
Figure 1. Endostatin encapsulation. (A) Schematic representation of theendostatin expression plasmid. CMV enhancer/promoter as indicated by anarrow. The solid lines indicate plasmid backbone containing bacterialreplication origin. (B) Phase-contrast microscopy of cell-loadedmicrocapsules shows the uniform size and cell distribution (average capsulediameter 700 µm). (C) Expression of endostatin protein (20 kDa) determinedby western blot analysis. Lane 1, hES secreted from BHK-endo monolayercells. Lanes 2 and 3, control cells (BHK-neo) in monolayer culture orencapsulated in APA. Lanes 4–6, time course of endostatin release fromencapsulated BHK-endo cells.
Table 1. Vessel count and apoptotic index quantification
Cell Vessel count Apoptotic index (%)
BHK-endo 7.34 ± 5.30a 13.1± 0.6b
BHK-neo 36.22 ± 5.99 3.7 ± 2.6
aP < 0.001 (BHK-endo versus BHK-neo).bP < 0.05 (BHK-endo versus BHK-neo).
A
B C
©20
01 N
atu
re P
ub
lish
ing
Gro
up
h
ttp
://b
iote
ch.n
atu
re.c
om
© 2001 Nature Publishing Group http://biotech.nature.com

NATURE BIOTECHNOLOGY VOL 19 JANUARY 2001 http://biotech.nature.com 37
tumors is cytostatic rather than cytotoxic to the tumor indicates thatprolonged administration of an anti-angiogenic therapy may benecessary to obtain long-term suppression of tumor growth8,28,29.However, many anticancer chemotherapies present difficulties inachieving effective therapeutic levels for tumor inhibition30,31.Therefore, local delivery of a potent angiogenic inhibitor may be avaluable treatment strategy for tumors such as glioblastoma, leadingto an accumulation of the anti-angiogenic proteins at the tumor sitein the brain.
Endostatin is a specific inhibitor of endothelial cell proliferationand is a potent angiogenesis inhibitor16,29,32,33. Achieving concentra-tions of endostatin that are sufficient to combat tumor growth iscomplicated by the exceedingly short half-life of the protein (7 h;personal communication, J. Folkman). Reaching and maintainingtherapeutically efficacious levels of endostatin may be achievedeither by continuous or repeated injections, or by a mechanismwhereby the protein is continuously secreted by an implanteddevice. We developed a promising approach for continuous long-term delivery of hES by a single administration of APA microcap-sules containing cells secreting hES. Using this system, lower dosesof the effective antiangiogenic protein may achieve significanttumor suppression.
An in vitro proliferation assay performed on BCE cells usingencapsulated BHK-endo cells resulted in 67.2% inhibition in prolif-eration over a three-day time period. In comparison, previous pro-liferation experiments showed a 25% inhibition when the sameamount of endostatin was added daily to cultured cells16. Thepotent inhibition of BCE proliferation may be explained by contin-uous release of endostatin during the course of the experiment asopposed to being added exogenously once at the beginning of theassay. The inhibition of tube formation by human endostatinreleased from monolayer BHK-endo cells demonstrates the activityof the protein and the potential effect on a human glioblastoma cellline (U-87). Using conditioned medium from U-87 cells stimulatedtube formation (10 tubes/well), indicating the potential angiogenicactivity of factors released from U-87 cells. The anti-angiogenicactivity of the released endostatin was confirmed by the observa-
tion that no tube formation was detected in KDR/PAE cells treatedwith U-87MG medium.
Daily systemic administration of 2.5 mg/kg endostatin for morethan 16 days resulted in a 53% inhibition in tumor growth in a Lewislung carcinoma model16. In a renal cell carcinoma model, recombi-nant human endostatin injected daily subcutaneously (10 µg/kg/day) around the tumor for four days led to a 61% inhibi-tion of tumor growth after 20 days32. Intramuscular injection ofnaked mouse endostatin expression plasmid combined withpolyvinylpyrrolidone (Pladsone) once a week for a period of twoweeks led to a 20% inhibition of tumor growth 18 days post treat-ment33. The present study demonstrates that a single administrationof microencapsulated engineered BHK cells that continuouslysecrete endostatin significantly inhibited human glioblastomaxenografts. Animals treated with encapsulated BHK-endo cellsexhibit a 72% inhibition in tumor growth 21 days post microcapsuleinjection. Western blot analysis performed on the harvested capsulesfrom U87MG human glioma xenografts treated with BHK-endoencapsulated cells had detectable endostatin. In contrast, endostatin
RESEARCH ARTICLES
Figure 2. The biological activity of endostatin on endothelial cells. (A) The effect of encapsulated BHK-endo and BHK-neo cells on theproliferation of BCE cells in culture. (B) Tube formation assay forrecombinant hES in PAE/KDR cells. Panel a (condition 1), cells grownin Ham’s F-12/10% FBS; panel b (condition 2), cells pretreated for 1 hwith BHK-neo conditioned medium followed by incubation withU87MG conditioned medium; panel c (condition 3), cells pretreatedwith BHK-endo conditioned medium for 1 h followed by incubationwith U87MG conditioned medium.
Figure 3. The effect of encapsulated BHK-endo on tumor growth invivo. (A) Inhibition of subcutaneous U87MG human glioma cellxenograft. Mice bearing U87MG tumors were treated withencapsulated BHK-neo (�), BHK-endo cells (�), or control (�). *P < 0.01. (B) At day 21 after treatment, U87MG tumors wereharvested and weighed. Errors are standard error of the mean(s.e.m.). P < 0.001.
*
0
2000
4000
6000
8000
0 4 8 12 16 21
control
BHK-neoBHK-endo
Tum
or s
ize
(mm
3 )
*
Days
0
1.0
2.0
3.0
4.0
BHK-endo BHK-neo Control
Tum
or w
eigh
t (g)
A
B
A
B
Figure 4. Western blot analysis of recombinant endostatin. (A) Injected microcapsules were harvested within close proximity tothe tumor and recultured for two weeks to confirm the release ofrecombinant hES as measured by western blot analysis. (B) Tumorxenografts adjacent to the BHK-endo capsules were positive forendostatin by western blot analysis.
hES
BH
K-e
ndo
caps
ule
Har
vest
edB
HK
-end
o ca
psul
e
BH
K-e
ndo
Tre
ated
tum
or
BH
K-n
eoT
reat
ed tu
mor
Tubulin
hES
A B
©20
01 N
atu
re P
ub
lish
ing
Gro
up
h
ttp
://b
iote
ch.n
atu
re.c
om
© 2001 Nature Publishing Group http://biotech.nature.com

was not measured in the tumors retrieved from the control group,emphasizing the efficiency of continuously delivering biologicallyactive endostatin. The same amount of encapsulated BHK-endocells has been shown to release an average of 150.8 ng/ml/week invitro, which may give a indication for the concentration of endo-statin released in vivo.
In the present study the vascular density decreased, the apoptoticrate increased, and there was no change in the proliferation rate intumors treated with endostatin compared to controls. These changesare similar to what has previously been reported in tumors treatedwith angiostatin15,28.
These results demonstrate the advantages of this delivery system,which allows continuous release of biologically active human endostatin for the treatment of glioma. This system may overcomeobstacles such as the short half-life of endostatin, repeated adminis-tration, high doses, and cost. This delivery system may be useful forthe treatment of brain tumors, wherein the blood–brain barrier canimpede systemic treatment of anti-angiogenic agents. Controllingthe amount of encapsulated cells may permit a higher concentrationof hES to be obtained. Preliminary in vitro proliferation studies per-formed in our laboratory have shown that endostatin secreted froman increased number of encapsulated BHK-endo cells (0.5 × 106)
brought about a 90% inhibition of BCE cell proliferation in culture.These results indicate that using a higher amount of encapsulatedcells may lead to higher tumor inhibition. Additional studies usingintracranial tumor models are presently underway to further assessthe efficacy of this microencapsulated cell endostatin delivery system.
Experimental protocolEndostatin plasmid construction. A plasmid containing an expression cas-sette for human endostatin was constructed as follows. The human endo-statin complementary DNA (cDNA; gift from J. Folkman, Children’sHospital, Harvard Medical School, Boston, MA) was inserted into the SalIsite of pTG 9530 (ref. 34) to generate pRP-hES. A pRP-hES plasmid contain-ing the human endostatin cDNA, which encodes the COOH-terminal 184 residues of collagen XVIIIα, was fused with a sequence for the signalpeptide of the human growth hormone (hGH) gene. The hGH-endostatinwas linked to a 543 bp fragment from the human β-globin gene containingintervening sequence 2 (IVS2) under the control of the humancytomegalovirus (CMV). The polyadenylation signal for transcription termination in this cassette was derived from a 760 bp long fragment of the
3′-untranslated region of the human β-globin gene.BHK-21 cell transfection. Baby hamster kidney cells (BHK-21) were
obtained from the American Type Culture Collection (ATCC, Rockville,MD) and maintained in Dulbecco's minimal Eagle medium (DMEM) sup-plemented with 10% FBS (Life Technologies, Grand Island, NY). BHK-21cells were stably transfected with pRP-hES plasmid DNA and a resistant geneexpression vector (neo) using Lipofectamine (Life Technologies).Conditioned medium was collected from individual clones and analyzed forhES expression by western blot analysis. Transfected BHK-21 cells (BHK-endo) were maintained as described above with the addition of 1 mg/ml ofgeneticin. Wild-type clones were chosen for control cell lines (BHK-neo).
Microencapsulation of BHK-endo and BHK-neo cells. BHK-endo andBHK-neo cells were encapsulated within microspheres composed of Ca2+-alginate, and a polyelectrolyte PLL (ref. 23). Briefly, cells were resus-pended in sodium alginate–saline (1.2% wt/vol), Pronova Ultra Pure MVG(Pronova Biopolymer, Drammen, Norway), to a final ratio of 0.5 × 106
cells/ml of alginate. The suspension was sprayed through a 22G needle locat-ed inside an air jet-head droplet-forming apparatus, into a solution of (N-[2-hydroxyethyl]piperazine-N-[2-ethanesulfonic acid])-buffered calci-um chloride (13 mM HEPES, 1.5% (wt/vol) CaCl2, pH 7.4, Sigma, St. Louis,MO), where they were allowed to gel for 20 min. The alginate microsphereswere coated with 0.1% (wt/vol) PLL of 23 kDa (Sigma) in saline for 12 minwith gentle agitation. The capsules were recoated with 0.125% alginate for 10 min, washed three times with HEPES and cultured. The number of cellsencapsulated and the viability of the cells in the microcapsules was evaluatedweekly using a modified MTT assay (MTT is 3-(4,5)-dimethylthiazol-2-yl)-2,5-diphenyl-tetrazolium bromide).
In vitro release of endostatin from encapsulated BHK-endo cells.Microencapsulated BHK-endo cells were suspended in DMEM supplement-ed with 10% FBS at a density of 2 × 105 cells/well and incubated at 37°C, 5% CO2. The medium was changed every week for six weeks and assayed forhES using western blot analysis and ELISA assay (Cytoimmune Sciences,College Park, MD). Medium from BHK-endo monolayer cells was used as apositive control. For western blot analysis, samples were boiled for 5 min, andanalyzed by sodium dodecyl sulfate–polyacrylamide gel (12% acrylamide)electrophoresis (SDS–PAGE). Proteins were electrophoretically blotted ontoImmobilon-P membranes (Millipore, Bedford, MA) and blocked at roomtemperature (RT) with 5% nonfat milk in Tris-buffered saline (TBS; 10 mMTris pH 8, 0.9% NaCl) containing 0.1% Tween-20 (TBST) for 1 h at RT. Blotswere incubated for 1 h at RT with an anti-endostatin antibody (a gift from Dr.Folkman). The blots were incubated with the secondary anti-rabbit horse-radish peroxidase-conjugated antibody for 1 h at RT. Detection of antibodieswas done by chemiluminescence using an ECL-Plus system (Amersham LifeScience, Arlington, IL).
Capillary endothelial cell proliferation assay. We used BCE for the prolif-eration assay as described by O'Reilly et al.16, with slight modifications. Cellsuspensions (2.5 × 104 cell/ml) were plated in gelatinized 24-transwell plates(3 µm filter size; Costar Corp., Cambridge, MA) and incubated (37°C, 10%CO2) for 24 h with DMEM and 10% bovine calf serum (BCS). The mediumwas replaced with 0.5 ml of DMEM with no BCS to achieve a final concentra-tion of 5% BCS, and basic fibrolblast growth factor (bFGF) (1 ng/ml) wasadded. Microcapsules containing BHK-endo cells or BHK-neo cells (0.2 × 105 cells/well as measured by MTT) were added on the filter. After 48 hincubation, [3H]thymidine (1 µCi/ml) was added for 12–14 h. The sampleswere suspended in liquid scintillation fluid and counts per minute (c.p.m.)were determined by β-counter. The results represent the average of four wells,and the experiments were repeated three times.
Angiogenic assay. The angiogenic assay was performed as described byDeroanne et al.35 with slight modifications. Porcine aortic endothelial cellsstably transfected with KDR (PAE/KDR) (a gift from Dr. Lena Claesson-Welsh, Ludwig Institute, Uppsala, Sweden) were used instead of bovinemicrovascular endothelial cells. The cells were cultured in Ham’s F-12 medium supplemented with 10% FBS and 1,000 U/ml penicillin/strepto-mycin (Life Technologies). This cell line has similar biological characteristicsto human umbilical vein endothelial cells in morphology, kinetics, chemo-tactic response, mitogenicity, and pattern of phosphorylation36. PAE/KDRcells were seeded in six-well dishes coated with 0.5 mm thick type I collagengel (4 × 104 cells/cm2) and allowed to attach and spread for 3 h. The seededKDR/PAE cells were subjected to three different conditions: condition 1, cellsgrown in Ham’s F-12/10% FBS; condition 2, cells pretreated for 1 h withBHK-neo conditioned medium followed by incubation with U87MG condi-tioned medium; condition 3, cells pretreated with BHK-endo conditioned
38 NATURE BIOTECHNOLOGY VOL 19 JANUARY 2001 http://biotech.nature.com
RESEARCH ARTICLES
Figure 5. Immunochemistry of tumors treated with BHK-neo or BHK-endo encapsulated cells. (A, B) H&E staining at 200× for BHK-neo (A) and BHK-endo (B). (C, D) CD31 staining at 200× in BHK-neo- (C) orBHK-endo-treated tumors (D). (E, F) Von Willebrand factor stainingvisualized at 200× magnification in BHK-neo- (E) or BHK-endo-capsule (F) treated tumors.
A B
C D
E F
©20
01 N
atu
re P
ub
lish
ing
Gro
up
h
ttp
://b
iote
ch.n
atu
re.c
om
© 2001 Nature Publishing Group http://biotech.nature.com

NATURE BIOTECHNOLOGY VOL 19 JANUARY 2001 http://biotech.nature.com 39
media for 1 h followed by incubation with U87MG conditioned medium. Atthe conclusion of the assay the number of tubes per well was recorded.
Animal studies. Male Swiss nude mice, four to six weeks old (TaconicFarms Inc., Germantown, NY) were inoculated subcutaneously with humanglioma U87MG cells (5 × 106 tumor cells/injection). Ten days later, when pri-mary tumors were ∼ 300 mm3 in size, animals were randomly divided intothree groups of five animals each. The first group received a single subcuta-neous injection of microcapsules containing BHK-endo cells within 0.5 cmfrom the observed tumor (2 × 105 encapsulated cells/animal). The secondgroup received a single subcutaneous injection of microcapsules containingBHK-neo cells (2 × 105 cells), and the third group did not receive any treat-ment (control). Subcutaneous tumor growth was measured transcutaneous-ly with a caliber every 4 days for 21 days, and the tumor volume was then cal-culated16. All animals were sacrificed 21 days post injection, and tumors wereresected and weighed. Statistically significant differences in tumor growthamong the groups were analyzed by analysis of variance (ANOVA). In allcases a P < 0.01 was considered to be statistically significant.
Microcapsules from the different treatment groups were harvested at thetime of sacrifice. The capsules were washed and cultured, and two weeks laterwestern blot analysis was done on the medium.
Western blot analysis and immunohistochemistry. For western blotanalysis, one-third of each tumor specimen was crushed and then suspendedin 3 ml of cold Nonidet P-40 lysis buffer37. The amount of protein was quan-tified (Bio-Rad protein analysis; Bio-Rad Laboratories, Hercules, CA), andstored at –70°C. 100 µg of protein lysate from each sample was analyzed bywestern blot analysis as described above.
For immunohistochemistry, tumor specimens were embedded in O.C.T.(Tissue-Tek; Miles, Elkhart, IN), frozen on dry ice/butane, and stored at–80°C. Frozen sections (6 µm) were cut using a cryostat (IEC Microtome,Needham, MA). Sections of each specimen were stained using H&E.Immunohistochemistry was carried out using the Vectastain Elite ABC kit(Vector Laboratories, Burlingame, CA). Primary antibodies included CD31(R&D Systems, Minneapolis, MN), von Willebrand Factor (Dako,Carpinteria, CA), and Ki-67 nuclear antigen (Dako). Detection was carriedout using a DAB chromogen, which resulted in a positive brown staining.Sections were counterstained with hematoxylin, dehydrated in ethanol, andmounted with glass coverslips. Negative control slides were obtained by omit-ting the primary antibody. Ki-67 staining was quantified by counting thenumber of positively stained cells of all nuclei in 20 randomly chosen fields.
In situ detection of apoptosis was measured by the terminal deoxinu-cleotidyltransferase (TdT)-mediated dUTP nick end-labeling (TUNEL)method using the ApopTag Plus Kit (Intergen, Gaithersburg, MD) followedby counterstaining with 1% methyl green. Apoptosis was quantified by deter-mining the percentage of positively stained cells for all nuclei in 20 randomlychosen fields per section at 200× magnification.
Tumor vascular density. Quantitation of vessel count was performed by aprocedure described by Weidner et al38. The blood vessels were counted ran-domly from non-necrotic areas in each tumor section in a 200× microscopefield (1.0 mm2) (Olympus BH2, Tokyo, Japan), on vWF-stained tissue sec-tions. Vascular density was defined by averaging the number of vessels in atleast five of the most vascular areas.
AcknowledgmentsWe wish to thank Dr. Judah Folkman for his helpful suggestions in the prepara-tion of the manuscript. This work is supported by a grant from the BostonNeurosurgical Foundation. T.J. is a recipient of a fellowship from JikeiUniversity School of Medicine.
1. Black, P.M. Brain tumor. Part 2. N. Engl. J. Med. 324, 1555–1564 (1991).2. Leon, S.P., Folkerth, R.D. & Black, P.M. Microvessel density is a prognostic indi-
cator for patients with astroglial brain tumors. Cancer 77, 362–372 (1996).3. Folkman, J. Angiogenesis inhibitors generated by tumors. Mol. Med. 1, 120–122
(1995).4. Hanahan, D. & Folkman, J. Patterns and emerging mechanisms of the angio-
genic switch during tumorigenesis. Cell 86, 353–364 (1996).5. Kerbel, R.S. A cancer therapy resistant to resistance. Nature 390, 335–336
(1997).6. Hanahan, D. A flanking attack on cancer. Nat. Med. 4, 13–14 (1998).
7. Brem, S., Brem, H., Folkman, J., Finkelstein, D. & Patz, A. Prolonged tumor dor-mancy by prevention of neovascularization in the vitreous. Cancer Res. 36,2807–2812 (1976).
8. Holmgren, L., O'Reilly, M.S. & Folkman, J. Dormancy of micrometastases: bal-anced proliferation and apoptosis in the presence of angiogenesis suppression.Nat. Med. 1, 149–153 (1995).
9. Tanaka, T., Manome, Y., Wen, P., Kufe, D.W. & Fine, H.A. Viral vector-mediatedtransduction of a modified platelet factor 4 cDNA inhibits angiogenesis andtumor growth. Nat. Med. 3, 437–442 (1997).
10. Takamiya, Y., Brem, H., Ojeifo, J., Mineta, T. & Martuza, R.L. AGM-1470 inhibitsthe growth of human glioblastoma cells in vitro and in vivo. Neurosurgery 34,869–875 (1994).
11. Takamiya, Y., Friedlander, R.M., Brem, H., Malick, A. & Martuza, R.L. Inhibition ofangiogenesis and growth of human nerve-sheath tumors by AGM-1470. J.Neurosurg. 78, 470–476 (1993).
12. Lee, J.K., Choi, B., Sobel, R.A., Chiocca, E.A. & Martuza, R.L. Inhibition of growthand angiogenesis of human neurofibrosarcoma by heparin and hydrocortisone. JNeurosurg. 73, 429–435 (1990).
13. Tamargo, R.J., Leong, K.W. & Brem, H. Growth inhibition of the 9L glioma usingpolymers to release heparin and cortisone acetate. J Neurooncol. 9, 131–138(1990).
14. O'Reilly, M.S. et al. Angiostatin: a novel angiogenesis inhibitor that mediates thesuppression of metastases by a Lewis lung carcinoma. Cell 79, 315–328 (1994).
15. Kirsch, M. et al. Angiostatin suppresses malignant glioma growth in vivo. CancerRes. 58, 4654–4659 (1998).
16. O'Reilly, M.S. et al. Endostatin: an endogenous inhibitor of angiogenesis andtumor growth. Cell 88, 277–285 (1997).
17. Lim, F. & Sun, A.M. Microencapsulated islets as bioartificial endocrine pancreas.Science 210, 908–910 (1980).
18. Soon-Shiong, P. et al. Insulin independence in a type 1 diabetic patient afterencapsulated islets transplantation. Lancet 143, 950–955 (1994).
19. Lanza, R.P., Hayes, J.L. & Chick, W.L. Encapsulated cell technology. Nat.Biotechnol. 14, 1107–1111 (1996).
20. Ismail, N., Hortelano, G. & Al-Hendy, A. Growth hormone gene therapy usingEncapsulated myoblast. In Cell encapsulation technology and therapeutics. (edsKuhetreiber, W.M., Lanza, R.P. & Chick, W.L.) 343–350 (Birkhauser, Boston, MA;1999).
21. Machluf, M., Orsola, A. & Atala, A. Controlled release of therapeutic agents: slowdelivery and cell encapsulation. World J. Urol. 18, 80–83 (2000).
22. Savelkoul, H.F.J. et al. Modulation of systemic cytokine levels by implantation ofalginate-encapsulated cells. J. Immunol. Methods 170, 185–196 (1994).
23. Machluf, M., Regev, O., Peled, Y., Kost, J. & Cohen, S. Characterization ofmicroencapsulated liposome systems for the controlled delivery of liposome-associated macromolecules. J. Contr. Release 43, 35–45 (1996).
24. Prakash, S. & Chang, T.M.S. Microencapsulated genetically engineered live E.coli DH5 cells administered orally to maintain normal plasma urea level in uremicrats. Nat. Med. 2, 883–887 (1996).
25. Gasper, L.E. et al. Supratentorial malignant glioma: patterns of recurrence andimplications for external beam local treatment. Int. J. Radiat. Oncol. Biol. Phys.24, 55–57 (1992).
26. Liang, B.C., Thornton, A.F. Jr., Sandler, H.M. & Greenberg, H.S. Malignant astro-cytomas: focal tumor recurrence after focal external beam radiation therapy. J.Neurosurg. 75, 559–563 (1991).
27. Sneed, P.K. et al. Patterns of recurrence of glioblastoma multiforme after externalirradiation followed by implant boost. Int. J. Radiat. Oncol. Biol. Phys. 29,719–727 (1994).
28. O'Reilly, M.S., Holmgren, L., Chen, C. & Folkman, J. Angiostatin induces and sus-tains dormancy of human primary tumors in mice. Nat. Med. 2, 689–692 (1996).
29. Boehm, T., Folkman, J., Browder, T. & O'Reilly, M.S. Antiangiogenic therapy ofexperimental cancer does not induce acquired drug resistance. Nature 390,404–407 (1997).
30. Fenstermacher, J.D., Blasberg, R.G. & Patlak, C.S. Methods for quantifying thetransport of drugs across brain barrier systems. Pharmacol. Ther. 14, 217–248(1981).
31. Jain, R.K. Haemodynamic and transport barriers to the treatment of solidtumours. Int. J. Radiat. Biol. 60, 85–100 (1991).
32. Yamaguchi, N. et al. Endostatin inhibits VEGF-induced endothelial cell migrationand tumor growth independently of zinc binding. EMBO J. 18, 4414–4423 (1999).
33. Blezinger, P. et al. Systemic inhibition of tumor growth and tumor metastases byintramuscular administration of the endostatin gene. Nat. Biotechnol. 17,343–348 (1999).
34. Chartier, C., Degryse, M., Dieterle, A., Pavirani, A. & Mehtali, M. Efficient genera-tion of recombinant adenovirus vectors by homologous recombination inEscherichia coli. J. Virol. 113, 178–183 (1991).
35. Deroanne, C.F., Hajitou, A., Calberg-Bacq, C.M., Nusgens, B.V. & Lapiere, C.M.Angiogenesis by fibroblast growth factor 4 is mediated through an autocrine up-regulation of vascular endothelial growth factor expression. Cancer Res. 57,5590–5597 (1997).
36. Waltenberger, J., Claesson-Welsh, L., Siegbahn, A., Shibuya, M. & Heldin, C.H.Different signal transduction properties of KDR and Flt1, two receptors for vas-cular endothelial growth factor. J. Biol. Chem. 269, 26988–26995 (1994).
37. Carroll, R.S. et al. KDR activation in astrocytic neoplasms. Cancer. 7, 1335–1341(1999).
38. Weidner, N., Semple, J.P., Welch, W.R. & Folkman, J. Tumor angiogenesis and metas-tasis—correlation in invasive breast carcinoma. N. Engl. J. Med. 324, 1–8 (1991).
RESEARCH ARTICLES©
2001
Nat
ure
Pu
blis
hin
g G
rou
p
htt
p:/
/bio
tech
.nat
ure
.co
m© 2001 Nature Publishing Group http://biotech.nature.com





![Joki katalog-2019 web (1)...2020/01/03 · ^ o ] u o ( # 1 - & / ( % / - ! ! ( / # & * # / ! ( * ( ( &](https://img.pdfslide.net/doc/110x75/60bc853f56d42031286db7d7/joki-katalog-2019-web-1-20200103-o-u-o-1-.jpg)