Embed Size (px)
Citation preview

BJU International (1999), 83, 378–382
Resistive index in renal colic: a prospective studyA.A. SHOKEIR and M. ABDULMAABOUDNew Jeddah Clinic Hospital, Jeddah, Saudi Arabia
Objective To study the role of Doppler ultrasonography −0.001 (0.02), respectively (P<0.001). For all thepatients, RI was sensitive in 77% and specific in 83%,(DU) in the diagnosis of acute unilateral renal
obstruction. and DRI was sensitive in 88% and specific in 98%.Obstructed kidneys showing delayed pelvicalyceal fill-Patients and methods In all, 117 patients with suspected
renal colic were evaluated by intravenous urography ing with excretion of contrast medium (n=42) hadsignificantly higher values of RI and DRI than(IVU) and DU, with determination of the resistive
index (RI) and the diCerence between the RI of ipsilat- obstructed kidneys without delayed filling (n=26).The RI and DRI were more sensitive in the formereral and contralateral kidneys (DRI). RI and DRI were
considered positive with values of �0.70 and �0.06, group. Among patients with obstruction, the RI didnot relate to the time of delay of filling with contrastrespectively. IVU results were considered the ‘gold
standard’ with which renal DU findings were medium, the duration of renal colic or the level ofureteric obstruction.compared.
Results IVU showed both kidneys to be normal in 49 Conclusions Renal DU is a sensitive and highly specifictest that can contribute significantly to the diagnosispatients and unilateral ureteric obstruction with a
normal contralateral kidney in 68. The mean (sd) RI of acute unilateral renal obstruction. It can replacethe IVU, particularly in situations where IVU iswas 0.73 (0.05) in 68 obstructed kidneys, significantly
higher than the mean RI of 0.64 (0.05) in 166 normal undesirable.Keywords Renal obstruction, Doppler ultrasonography,kidneys (P<0.001). The DRI in patients with unilat-
eral obstruction was significantly higher than that in diagnosis, resistive indexpatients with both kidneys normal, at 0.09 (0.05) and
patients were prospectively evaluated using renal ultra-Introduction
sonography (US), followed by IVU. The US studies werecarried out during the attack of loin pain in all patients,Intrarenal Doppler ultrasonography (DU) has been sug-
gested as a possible adjunctive test in distinguishing and before giving any medication in most; in each case,the person performing US was unaware of the findingsobstructed from unobstructed chronically dilated col-
lecting systems [1–4], with the resistive index (RI) being on IVU. The US examination included real-time imagingand intrarenal DU, performed using an Aloka SSD-2000the variable most widely measured. However, there has
been a significant diversity of opinion about the reliability unit (Aloka, Tokyo, Japan) using a transducer frequencyof 3.5 MHz. The degree of pyelocaliectasis was assessedof RI in the diagnosis of acutely obstructed kidneys
[5–12]. Because of the obvious utility of an accurate, in each kidney on the grey-scale images. Pelvicalycealdilatation was subjectively graded as absent, mild, mod-noninvasive method for the diagnosis of acute obstruc-
tion, we carried out a prospective study using DU in the erate, or marked.At least five Doppler spectra were obtained from moreinitial assessment of patients with symptoms suggestive
of renal colic. than three regions in each kidney. Doppler signals wereobtained from arcuate arteries at the corticomedullaryjunctions, interlobar arteries along the border of the
Patients and methodsmedullary pyramids, or both. The Doppler waveformswere made using the lowest pulse repetition frequencyThe study included 117 patients (87 male and 30 female,
mean age 37.8 years, range 16–70) with 234 kidneys possible without aliasing. This maximized the size of theDoppler spectrum and decreased the percentage error inwho presented with unilateral loin pain suspected of
being renal colic. Immediately on presentation, all the measurements. In addition, the lowest possible wallfilter for each ultrasound scanner was used. The Dopplersample width was set at 2–5 mm. The renal RI wasAccepted for publication 13 October 1998
378 © 1999 BJU International
RESISTIVE INDEX IN RENAL COLIC 379
calculated as: (peak systolic velocity–end diastolic caliectasis, which was considered mild in 33 and moder-ate in three. All 36 obstructed kidneys showingvelocity)/peak systolic velocity, with the RI diCerence
(DRI) determined as the diCerence in RI of the corre- pyelocaliectasis on grey-scale US had an elevated RI.Patients with acute unilateral ureteric obstructionsponding and contralateral kidney. Values of RI and DRI
used for statistical analysis were means of the mean were further classified into two groups, the first compris-ing 42 with delayed pelvicalyceal filling with contrastmeasurements in individual patients.
The IVU was interpreted as negative with a normal medium (suggestive of complete obstruction) and thesecond comprising 26 with no delay in filling (suggestivereno-ureteric unit and positive with hydroureter proxi-
mal to a ureteric stone, with or without delayed pelvi- of partial obstruction). The respective mean (sd) RIs were0.75 (0.06) and 0.70 (0.04), and the respective DRIscalyceal filling with contrast medium. RI and DRI were
considered positive with values of �0.70 and �0.06, were 0.11 (0.04) and 0.07(0.04), both being signifi-cantly higher in the first group (P<0.01, Student’srespectively. The IVU results were considered the ‘gold
standard’ with which DU findings were compared. The t-test). The RI and DRI were more sensitive in the lattergroup; in both groups, DRI was more sensitive and moresensitivity and the specificity of DU values for the diag-
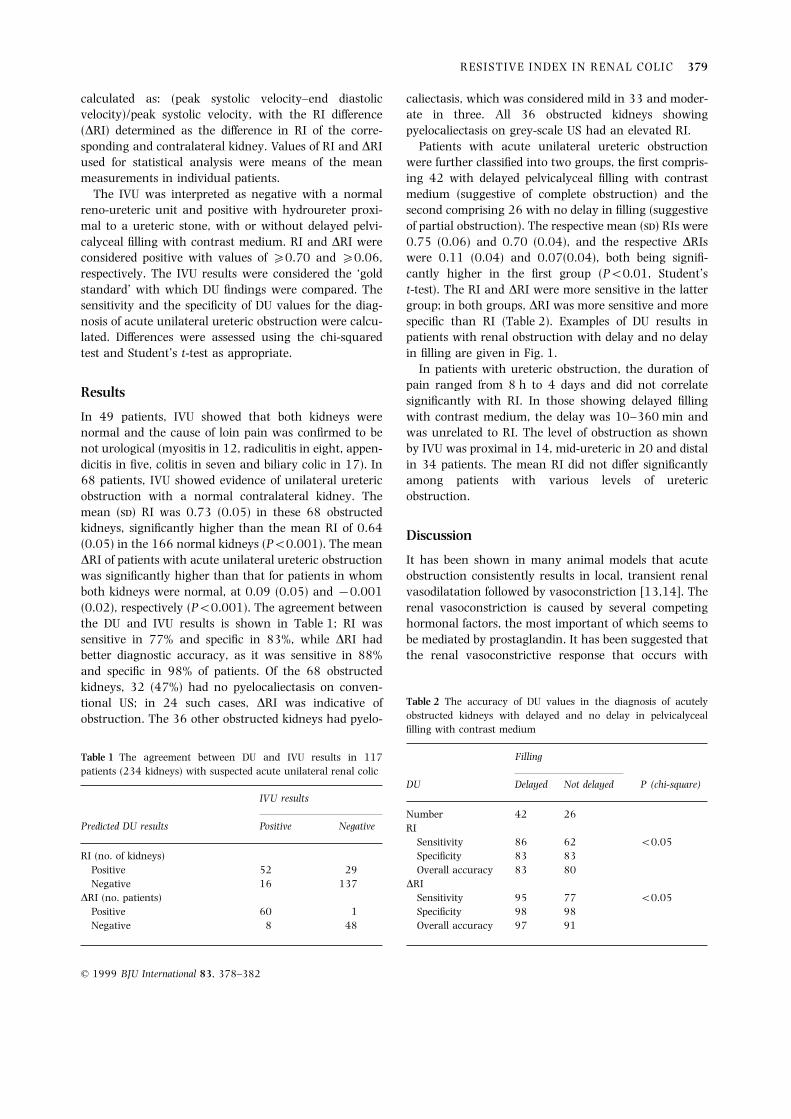
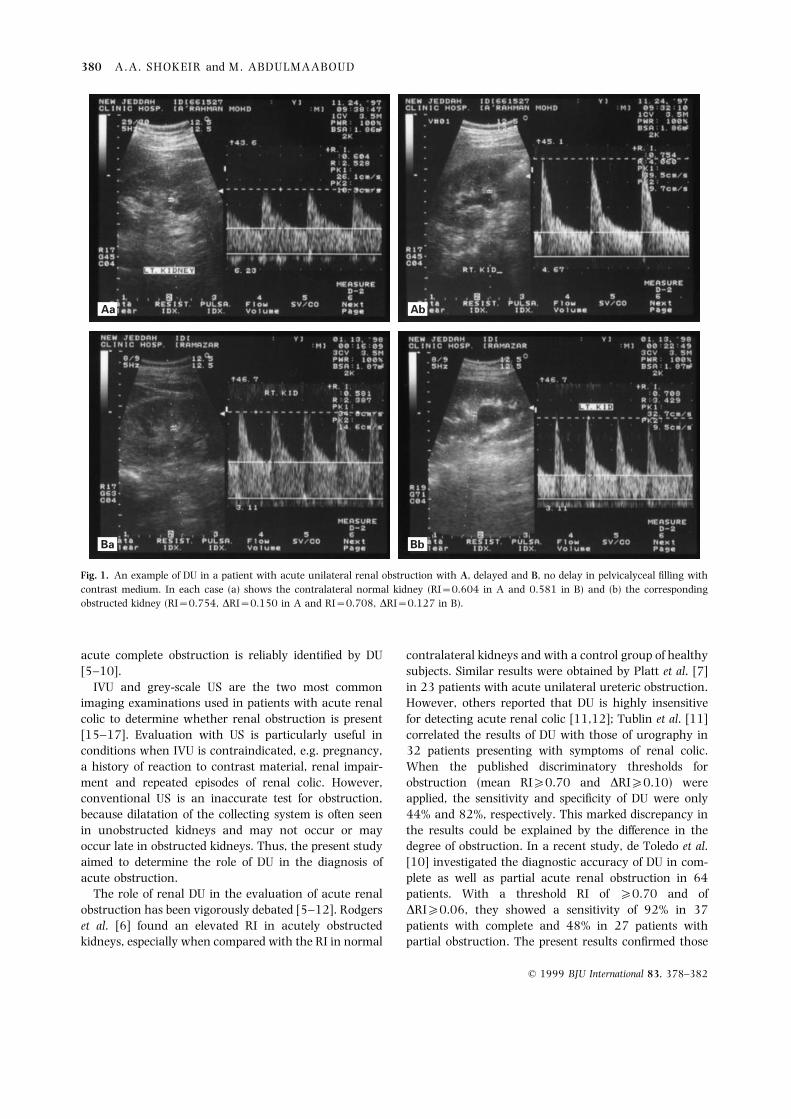
nosis of acute unilateral ureteric obstruction were calcu- specific than RI (Table 2). Examples of DU results inpatients with renal obstruction with delay and no delaylated. DiCerences were assessed using the chi-squared
test and Student’s t-test as appropriate. in filling are given in Fig. 1.In patients with ureteric obstruction, the duration of
pain ranged from 8 h to 4 days and did not correlateResults
significantly with RI. In those showing delayed fillingwith contrast medium, the delay was 10–360 min andIn 49 patients, IVU showed that both kidneys were
normal and the cause of loin pain was confirmed to be was unrelated to RI. The level of obstruction as shownby IVU was proximal in 14, mid-ureteric in 20 and distalnot urological (myositis in 12, radiculitis in eight, appen-
dicitis in five, colitis in seven and biliary colic in 17). In in 34 patients. The mean RI did not diCer significantlyamong patients with various levels of ureteric68 patients, IVU showed evidence of unilateral ureteric
obstruction with a normal contralateral kidney. The obstruction.mean (sd) RI was 0.73 (0.05) in these 68 obstructedkidneys, significantly higher than the mean RI of 0.64
Discussion(0.05) in the 166 normal kidneys (P<0.001). The meanDRI of patients with acute unilateral ureteric obstruction It has been shown in many animal models that acute
obstruction consistently results in local, transient renalwas significantly higher than that for patients in whomboth kidneys were normal, at 0.09 (0.05) and −0.001 vasodilatation followed by vasoconstriction [13,14]. The
renal vasoconstriction is caused by several competing(0.02), respectively (P<0.001). The agreement betweenthe DU and IVU results is shown in Table 1; RI was hormonal factors, the most important of which seems to
be mediated by prostaglandin. It has been suggested thatsensitive in 77% and specific in 83%, while DRI hadbetter diagnostic accuracy, as it was sensitive in 88% the renal vasoconstrictive response that occurs withand specific in 98% of patients. Of the 68 obstructedkidneys, 32 (47%) had no pyelocaliectasis on conven-
Table 2 The accuracy of DU values in the diagnosis of acutelytional US; in 24 such cases, DRI was indicative ofobstructed kidneys with delayed and no delay in pelvicalycealobstruction. The 36 other obstructed kidneys had pyelo-filling with contrast medium
FillingTable 1 The agreement between DU and IVU results in 117patients (234 kidneys) with suspected acute unilateral renal colic
DU Delayed Not delayed P (chi-square)IVU results
Number 42 26Predicted DU results Positive Negative RI
Sensitivity 86 62 <0.05Specificity 83 83RI (no. of kidneys)
Positive 52 29 Overall accuracy 83 80DRINegative 16 137
DRI (no. patients) Sensitivity 95 77 <0.05Specificity 98 98Positive 60 1
Negative 8 48 Overall accuracy 97 91
© 1999 BJU International 83, 378–382
380 A.A. SHOKEIR and M. ABDULMAABOUD
Aa Ab
Ba Bb
Fig. 1. An example of DU in a patient with acute unilateral renal obstruction with A, delayed and B, no delay in pelvicalyceal filling withcontrast medium. In each case (a) shows the contralateral normal kidney (RI=0.604 in A and 0.581 in B) and (b) the correspondingobstructed kidney (RI=0.754, DRI=0.150 in A and RI=0.708, DRI=0.127 in B).
acute complete obstruction is reliably identified by DU contralateral kidneys and with a control group of healthysubjects. Similar results were obtained by Platt et al. [7][5–10].
IVU and grey-scale US are the two most common in 23 patients with acute unilateral ureteric obstruction.However, others reported that DU is highly insensitiveimaging examinations used in patients with acute renal
colic to determine whether renal obstruction is present for detecting acute renal colic [11,12]; Tublin et al. [11]correlated the results of DU with those of urography in[15–17]. Evaluation with US is particularly useful in
conditions when IVU is contraindicated, e.g. pregnancy, 32 patients presenting with symptoms of renal colic.When the published discriminatory thresholds fora history of reaction to contrast material, renal impair-
ment and repeated episodes of renal colic. However, obstruction (mean RI�0.70 and DRI�0.10) wereapplied, the sensitivity and specificity of DU were onlyconventional US is an inaccurate test for obstruction,
because dilatation of the collecting system is often seen 44% and 82%, respectively. This marked discrepancy inthe results could be explained by the diCerence in thein unobstructed kidneys and may not occur or may
occur late in obstructed kidneys. Thus, the present study degree of obstruction. In a recent study, de Toledo et al.[10] investigated the diagnostic accuracy of DU in com-aimed to determine the role of DU in the diagnosis of
acute obstruction. plete as well as partial acute renal obstruction in 64patients. With a threshold RI of �0.70 and ofThe role of renal DU in the evaluation of acute renal
obstruction has been vigorously debated [5–12]. Rodgers DRI�0.06, they showed a sensitivity of 92% in 37patients with complete and 48% in 27 patients withet al. [6] found an elevated RI in acutely obstructed
kidneys, especially when compared with the RI in normal partial obstruction. The present results confirmed those
© 1999 BJU International 83, 378–382

RESISTIVE INDEX IN RENAL COLIC 381
of de Toledo et al.; DU is significantly more sensitive in waveforms barely deviating from the baseline; whenmeasured, these waveforms invariably result in an RIdiagnosing complete renal obstruction than partial
obstruction. that is calculated to lie within the normal range, evenwhen a true state of elevated renal arterial resistanceThe present high sensitivity for DRI of 88% and
specificity of 98% in diagnosing acute renal obstruction is present.The level of ureteric obstruction had no significantmay have arisen because DU was carried out during the
episode of renal colic and before giving any medication impact on the present values of RI, in agreement withPlatt et al. [7]. However, de Toledo et al. [10] havein most patients. Cronan and Tublin [12] discussed the
eCect of NSAIDs in the management of patients with shown that patients with proximal ureteric obstructionhad RIs higher than those with distal obstruction.acute renal colic. These drugs have been shown in
animal models to reverse both the early vasodilatation Previous reports suggest that 17–29% of patients withacute obstruction have abnormalities on DU, despiteand later vasoconstriction that occur with acute renal
obstruction [18,19]. Thus, their use may aCect the normal grey-scale US [6,7]; such abnormalities weredetected in 35% of the present patients. Therefore, whenexpected changes in renal RI; in previous studies, many
patients had received NSAIDs before imaging. The eCect US is used instead of IVU, renal DU is necessary toimprove the sensitivity in early obstruction and to pro-of pharmacological agents on renal RI merits further
study. vide functional information about an obstructed kidney[9].Previous investigators have shown that the increase
in RI occurred after as little as 6 h of clinical obstruction One relative limitation of the present study is thatthere were no cases of acute bilateral obstruction or[7]. This finding is supported by previous laboratory
research that in the earliest stage of obstruction there is acute obstruction of a solitary kidney. However, thepresent results and those of others [6] indicate that suchvasodilatation, with which a normal RI would be
expected [13,14]. However, admission to hospital in the cases are uncommon in clinical practice. Another poten-tial limitation of DU (not found in this study) is thefirst 5 h after the onset of renal colic is uncommon. In
such a situation, although the RI may not be high, a patient with intermittent but very acute renal colic. Ifthe obstruction is present for a few hours only and isDRI of � 0.06 suggests unilateral obstruction before the
RI reaches the 0.70 threshold. We were unable to then relieved, theoretical considerations would suggestthat the RI may not increase, even if this pattern ofinvestigate the shortest duration of acute renal obstruc-
tion that can cause elevation of RI, as all the present intermittent obstruction and relief persists for days [7,9].A third potential limitation of DU is that RI could bepatients presented with renal colic of >7 h duration.
In patients with renal colic for >6 h, conflicting elevated in conditions other than renal obstruction, e.g.chronic hypertension and renal medical diseases.results have been obtained about the eCect of duration
on RI. We agree with Platt et al. [7] that kidneys Therefore, in the setting of known renal medical diseasesand renal colic, an elevated RI could be caused by theobstructed for >12 h do not have a significantly higher
RI than those with obstruction of shorter duration. On renal disease or obstruction, thus limiting the value ofan abnormal RI in this particular situation. The impor-the other hand, de Toledo et al. [10] reported that the
RI was significantly higher in patients with renal colic tance of DRI in such a condition is also unknown.However, a normal RI in this setting would still befor >24 h. These diCerences could be attributable to the
duration of obstruction being based on the clinical helpful in arguing against the presence of obstruction[20].history in all previous studies. The precise duration of
obstruction in patients in a clinical series cannot be In conclusion, DU is a sensitive and highly specifictest that can contribute significantly to the diagnosisascertained.
The application of an adequate DU technique is essen- and management of acute unilateral renal obstruction,particularly in situations in which IVU is undesirable.tial for obtaining accurate results. The most common
reason for obtaining a normal RI in the presence ofsignificant obstruction is a technical error that is simple
Referencesto correct. As described previously, the use of the correct
1 Platt JF, Rubin JM, Ellis JH. Distinction between obstructivescale (pulse-repetition frequency) to expand the wave-and non-obstructive pyelocaliectasis with duplex Doppler
form size to fill as much of the available display assonography. Am J Roentgen 1989; 153: 997–1000
possible, without aliasing, is crucial [9]. With this strat- 2 Platt JF, Rubin JM, Ellis HM, DiPietro MA. Duplex Doppleregy, errors in measurements of RI are reduced and flow US of the kidney: diCerentiation of obstructive from non-at the end of diastole generally can be diCerentiated from obstructive dilatation. Radiology 1989; 17: 515–7background machine noise and the wall filter. Failure to 3 Shokeir AA, Provoost AP, El-Azab M, Dawaba M, Nijman
RJM. Renal Doppler ultrasound in children with obstructivemake this simple technical correction results in minute
© 1999 BJU International 83, 378–382

382 A.A. SHOKEIR and M. ABDULMAABOUD
uropathy: eCect of intravenous normal saline fluid load evaluation of acute renal obstruction. Am J Roentgen 1995;164: 377–8and furosemide. J Urol 1996; 159: 1455–8
4 Shokeir AA, Provoost AP, El-Azab M, Dawaba M, Shokeir 13 Murphy GP, Scott WW. The renal hemodynamic responseto acute and chronic ureteral obstruction. J Urol 1966;MA, Nijman RJ. Renal Doppler ultrasonography in children
with equivocal obstructive uropathy: eCect of intravenous 95: 636–5714 Moody TE, Vaughan ED, Gillenwater JY. Relationshipnormal saline fluid load and furosemide. Br J Urol 1997;
80: 313–8 between renal blood flow and ureteral pressure during 18hours of total unilateral ureteral occlusions. Invest Urol5 Gottlieb RH, Luhman K, Oates RP. Duplex ultrasound
evaluation of normal kidneys and native kidneys with 1975; 13: 246–5115 Erwin BC, Carroll BA, Sommer FG. Renal colic: the role ofurinary tract obstruction. J Ultrasound Med 1989; 8:
609–11 ultrasound in initial evaluation. Radiology 1984; 152:147–506 Rodgers PM, Bates JA, Irving HC. Intra-renal Doppler
ultrasound studies in normal and acutely obstructed 16 Laing FC, JeCrey RB, Wing VW. Ultrasound versus excretoryurography in evaluating acute flank pain. Radiology 1985;kidneys. Br J Radiol 1992; 65: 207–12
7 Platt JF, Rubin JM, Ellis JH. Acute renal obstruction: 154: 613–617 Hill MC, Rich JI, Mardiat JG, Finder CA. Sonography vsevaluation with intra-renal duplex Doppler and conven-
tional US. Radiology 1993; 186: 685–8 excretory urography in acute flank pain. Am J Roentgen1985; 144: 1235–88 Brkljacic B, Drinkovic I, Sabljar-Matovinovic M et al. Intra-
renal duplex Doppler sonographic evaluation of unilateral 18 Kawasaki A, Needleman P. Contribution of thromboxaneto renal resistance changes in the isolated perfusednative kidney obstruction. J Ultrasound Med 1994; 13:
197–204 hydronephrotic rabbit kidney. Circ Res 1982; 50: 486–9019 Wolfson AB, Yealy DM. Oral indomethacin for acute renal9 Platt JF, Ellis JH, Rubin JM. Role of renal Doppler imaging
in the evaluation of acute renal obstruction. Am J Roentgen colic. Am J Emerg Med 1991; 9: 16–920 Shokeir AA, Provoost AP, Nijman RJM. Resistive index in1995; 164: 379–80
10 de Toledo LS, Martinez-Berganza-Asensio T, de Cozcolluela- obstructive uropathy. Br J Urol 1997; 80: 195–200Cabrejas R, Gregorio-Ariza MA, Pardina-Cortina P, Ripa-Saldias L. Doppler-duplex ultrasound in renal colic. Eur
AuthorsJ Radiol 1996; 23: 143–811 Tublin ME, Dodd GD, Verdile VP. Acute renal colic: A.A. Shokeir, MD, Associate Professor of Urology.
M. Abdulmaaboud, MD, Associate Professor of Radiodiagnosis.diagnosis with duplex Doppler US. Radiology 1994; 193:697–701 Correspondence: Dr A.A. Shokeir, New Jeddah Clinic Hospital,
PO Box 7692, 21472 Jeddah, Saudi Arabia.12 Cronan JJ, Tublin ME. Role of the resistive index in the
© 1999 BJU International 83, 378–382