Embed Size (px)
Citation preview

J7ournal ofMedical Ethics 1998;24:376-381
Transfusion-free treatment ofJehovah'sWitnesses: respecting the autonomouspatient's motivesDavid Malyon Chairman, Hospital Liaison Committee for _ehovah's Witnesses, Luton
AbstractWhat makes Jehovah 's Witnesses tick? Whatmotivates practitioners of medicine? How isbenevolent human behaviour to be interpreted? Theexplanation that fear of censure, mind-controltechniques or enlightened self-interest are the realmotivators ofhuman conduct is questioned. Thosewho believe that man was created in "God's image",hold that humanity has the potential to rise aboveselfishly driven attitudes and actions, and reflect thequalities of love, kindness and justice that separate usfrom the beasts. A comparison ofgeneral medicalethics and disciplines, and those of the J7ehovah'sWitness community, is made in this context. The easycharge thatfrequent deaths resultfrom refusal ofblood transfusions is examined. The central source ofantipathy towards Jehovah 's Witnesses, namely thealleged imposition of extreme and even harmfulrefusal of blood therapy on our children is addressed.Of course, "... few dilemmas are likely to be resolvedwisely or satisfactorily by a blinkered adherence toabstract principles alone. Solutions to most cases willbe dictated by a combination offactors.' The supportof medical ethics by Jehovah's Witnesses, and theirwillingness to share in reasoned and ethical debate,while at the same time holdingfirm to their religiousand conscientious principles are emphasised.(Journal ofMedical Ethics 1998;24:376-381)Keywords: Disciplinary measures; blood alternatives; dis-sidents; moral motivation; Jehovah's Witnesses
IntroductionIn recent editions the journal has included two, inmy view erroneous and ill-considered attacks onmy faith and that of my fellow Jehovah'sWitnesses.2-3 Particularly offensive is the ascrip-tion of ulterior motives, attitudes and practices toour members. In my first responding paper4 Iconsidered the rights of Jehovah's Witnesses. Inthis second paper responding to Dr Muramoto, Igive an account of our faith and of our attitudesand motivation with regard to blood transfusions.
Religious, medical and personal motivesLike the rest of us, doctors must answer to theirconsciences. " . . . to thine own self be true . . .".5However, again like the rest of us doctors are alsogoverned by the criminal and civil law. They mustsatisfy their patients of their performance andethical integrity. In addition, they submit to thediscipline of examination by their peers in aprofessional body. In England this is the GeneralMedical Council (GMC) and disregard of suchlegal and professional constraints could result ineventual suspension or even revocation of thedoctor's licence. Without such discipline societywould lose confidence in the skill of doctors, theirpatients would seek other practitioners, their peerswould start to ignore them, and eventually theytoo would lose confidence in themselves and theirown ability. In a recent sad case an eminent heartsurgeon resigned in similar circumstances tothese.6
However, do these constraints form the under-lying ethical "bedrock" for the practice ofmedicine? Do doctors "behave themselves" onlybecause of fear of censure? Dawkins in the TheSelfish Gene argues that "genetic" self-interest isthe "modus operandi" for all of the natural world,including the human race.7 He affirms that "weare survival machines-robotic vehicles, blindlyprogrammed to preserve the selfish moleculesknow as genes. This is a truth which still fills mewith astonishment". (I share his astonishment thatall that is pure and beautiful can so easily be dis-missed!) This is an old debate! "Love seeketh notitself to please, nor for itself hath any care, but foranother gives its ease, and builds a heaven in hell'sdespair. . .".8The Christian believes that "love" is and must
be the principal motivation for upright conduct. Adesire to do good to their patients, to society, andto uphold the standards of their own colleaguesmust surely drive the majority of members of themedical profession rather than the cash benefits! Aleading consultant surgeon confirms: "Many ofmy colleagues and myself and the nursing staff,

Malyon 377
over many years have contributed well above whatwe are paid for in terms of time, hours, effort andexpertise. The reason? We believe and love theNHS as a concept".9 Is a man faithful to his wifebecause she is a good cook, a good conversation-alist, or even a good lover? Although such assetsmay have originally attracted him to her the greatdescription of love in The Bible is recognised bymany as the driving force in the closest, and inother, personal relationships. "Love is patient andkind; it is not jealous or conceited or proud; love isnot ill-mannered or selfish or irritable; love doesnot keep a record ofwrongs; love is not happy withevil, but is happy with the truth. Love never givesup, and its faith, hope and patience neverfail . . .'. The deficiency of law in keeping man-kind in order was revealed outstandingly by theteachings of Jesus Christ in the Sermon on theMount. "Do not kill" becomes "do not be angry","do not commit adultery" becomes "do not thinkabout it", "love your friends" becomes "love yourenemies". Jesus realised that the heart, or motiva-tion, must be pure if the actions are to belikewise." Parliament has long ago given up theVictorian thought of moral education by law. Asusual The Bible is so apt: "We know that the law isgood if it is used as it should be used. It must beremembered, of course, that laws are made, notfor good people, but for law-breakers andcriminals, for the godless and sinful . . . thepurpose of this order is to arouse the love thatcomes from a pure heart, a clear conscience and agenuine faith . . .".12 Mankind, the "flawedgenius", is rightly subject to law, however, andhumility causes many of us to admit that we haveslowed our speeding vehicles at the sight of arevolving blue light, and that the reduction ofspeed appears to last a little longer when the bluelight is replaced with a flashing camera!
The Watchtower states that "Jehovah's Witnessesare motivated by love for God, and their fellowhumans. True they are closely knit together by thebond of Christlike love as a worldwide associationof brothers. But as free moral agents, each one haspersonally decided to live by Bible standards.These are decisions that fall within the frameworkof a way of life freely chosen [my italics] by poten-tial Witnesses before they ever take the step ofChristian [baptism] ".'
Doctors may see some similarity in theirpersonal commitment to the Hippocratic Oath orthe International Code of Medical Ethics.'4 TheWitnesses regard themselves as performing a pub-lic service of education and of encouragement toadopt Christ's principles, which they feel are sobadly needed in the world today. We too mustanswer to our own consciences, we must keep the
law, and must show respect for all whom we seekto contact. Our ability to do our work effectively,depends to a large extent upon our reputation inthe community as honest and respectable people,whether our religious principles are accepted ornot. To believe that the procedure of "examinationby peers" which the Witness community uses touphold good conduct, and which can ultimatelylead to "excommunication" is the prime or eventhe only motivation for our religious activities, isto impugn our motives, and by implication themotives of other professionals who subscribe todisciplinary action. The parallel implied above canbe developed further. It is of interest that a largemajority of doctors who are struck off eventuallyreturn to the medical register, and that the GMCdisciplinary committee seeks to tailor the "punish-ment to the crime", taking into consideration suchfactors as intent, attitude and prior counselling.Outsiders not in possession of the full factsfrequently criticise their sincerely reached deci-sions, and even the procedure itself (a recent casein point being comments from the British Minis-ter of Health)!'
Similarly the disciplinary measures ofJehovah'sWitnesses carefully analyse the attitude of theoffender. Never is anyone disfellowshipped ifhe orshe displays a repentant attitude, and happily alarge number of those thus censured by this rarelyused procedure, are eventually restored to ourcongregations. Of course, Jesus' story of theprodigal son reveals the wisdom of excommunica-tion even though in this case it was voluntaryseparation on the son's part. The prodigalreturned only after he had realised what he hadlost, and the return to his own senses and to hisfather's love was indeed a warm one.
Risk/benefits in refusing bloodtransfusionsMuramoto's central assumption is that the lives of"many" Jehovah's Witnesses are lost because oftheir refusal to accept blood transfusions. Whereare his statistics? Kitchens"5 states that " . . . bloodis usually administered by physicians with thenearly unchallenged view that failure to transfusewould have dire consequences. Evidence support-ing that view is very difficult to obtain". Deathcertificates seldom mention negative reasons."Doctor arrived too late", "no cardiac unitavailable", "penicillin not yet discovered", are notacceptable as the primary reason for death.Inquests usually bring in a verdict of naturalcauses or misadventure even in cases whereextreme loss ofblood was obviously involved. Whyis Muramoto so certain that his assumption is

378 Transfusion-free treatment of_ehovah 's Witnesses: respecting the autonomous patient's motives
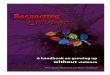
Table 1 J7ehovah 's Witnesses undergoing major surgerywithout blood transfusions
No of Deaths associatedPIrocedures operations with anaemia
Cardiovascular 542 15Cardiovascular 36 3Total hip replacement 107 0Total hip replacement 100 0Obstetrics/gynaecology 165 0Obstetrics/gynaecology 96 0General surgery 27 0Paediatric cancer 9 0CABG 46 0CABG 13 0Renal transplantation 11 0Paediatric cardiovascular 30 0Cardiovascular 13 0General surgery 78 1Paediatric cardiovascular 112 1Spinal fusion 19 0Total 1404 20 (1.4%)
American Journal ofMedicine volume 94:119 Editorial
correct? The American journal article referred toabove considered 16 studies involving 1404operations and reported that the authors16 " . . .
implicated a lack of blood as the primary cause ofdeath in 8 patients (0.6%) and contributing todeath in another 12 patients, yielding a total of 20deaths (1.4%) . . .. Other complications were notincreased in Jehovah's Witness patients comparedwith other patients ... . Less clear is how muchmorbidity and mortality are avoided by this prac-tice [refusal of blood], but they probably exceedthe risk of being transfused . . .. Rather thanreflexively administering blood, a physician mustconsider the risk-benefit ratio as they would forany [my italics] drug or procedure". See table 1. Isit surprising that the editorial was entitled Aretransfusions overrated? The Lancet further ob-served: "Because of the risks of transmittingdisease and compromising immune defences,transfusion of homologous blood should beavoided when possible, not only in adults but alsoin children".'7 Nielsen has 139 references toestablished medical papers as " . . . evidence sug-gesting that perioperative allogenic blood transfu-sion increases the risk of infectious complicationsafter major surgery and of cancer recurrence aftercurative operations . . . also contributing toimmuno-suppression".18 Are these authoritativestudies part of the "exaggerated negative cam-paign against blood transfusion" mentioned byMuramoto? Why are the international drug com-panies involved in a systematic search for recom-binant blood alternatives?When it comes to dying or living Judge Lady
Butler Sloss in the Court of Appeal stated " . . .
Jehovah's Witnesses accept and take advantage ofthe same medical treatment as those who do notsubscribe to their beliefs and are as anxious as
anyone else to recover from any illness from whichthey may suffer. There is no question of a right todie . . . Her colleague Lord Donaldsonconcurred: "This appeal is not in truth about theright to die, [rather] it is about the right to choosehow to live...". To summarise, if the Court ofAppeal in the recent caesarean case'o can allow anappeal which involved a pregnant woman with" .... an unusual, even apparently bizarre and irra-tional thinking process, and contrary to the viewsof the overwhelming majority of the community atlarge . . ." then how much more recognition mustbe given to an adult Jehovah's Witness whoserefusal of one single medical procedure is basedupon religious, ethical, and proven medical opin-ion. The "community at large" certainly has had amassive sea change of opinion against thetherapeutic use of blood.
Children and parentallmedicalresponsibilitiesChildren are not "owned" by their parents. How-ever, parents should feel a responsibility towardstheir children. They have the privilege of teachingthem their own moral principles in such a way thatthe children will feel free to develop their ownvalue systems from the background of theirparents. Wise parents allow freedom in suchdevelopment. Medical Ethics Today says: "Recentstudies appear to show also that when entrustedwith responsibilities children and young peopleoften respond well, but when perceived by othersas immature, respond accordingly. Such studieshave contributed to the increasing empowermentof children and young people". Indeed! Howmany of us can remember responding to theexhortation to "grow up" with a surly determina-tion not to! Jehovah's Witnesses accept suchresponsibilities towards their children with loveand consideration. They cannot and should not beexpected to consent to a medical treatment whichthey feel is against God's wishes and may bemedically questionable. Again, new overtures bythe hospital liaison committee network enable thedevelopment of trust between a child's doctor andthe parents. The doctor acknowledges the parents'refusal of blood, yet agrees to honour their refusalto the point in his opinion, of not allowing thechild to die or suffer injury. Jehovah's Witnessesand everyone else are bound by the presentunderstanding in law that doctors must act in thebest interest of the child as an overriding factor.Savulescu et at2' raised questions about the "bestinterests" doctrine in a case involving the donationof bone marrow by a six-year-old sister for thebenefit of her nine-year-old sibling. They argued

Malyon 379
that it might have been in the "best interests" ofthe nine-year-old, but questioned whether it wasin the "best interests" of the six-year-old, and howcould the consent of the parents for such a proce-dure be unquestioned? A more recent caseinvolved the refusal of a mother to accept a livertransplant for her severely damaged child, eventhough this refusal would inevitably lead to thechild's death. Surely such cases demonstrate thatthese medical dilemmas should be handled withsensitivity on a case-by-case basis, rather than by ablanket doctrinal approach.The hospital liaison committees are heard when
such cases arise, and Witness parents receive sup-port and advice, but also the medical professionalsare made aware of the ethical issues involved. Fre-quently such activity results in a satisfactory out-come for everyone involved, with the health of thechild being paramount. Of course, differing viewsabout mature minors, second opinions, and veryavant garde treatments may confuse such basicprinciples, but in fact few of our children are beingtransfused. Cooperative doctors, medical ad-vances and the proactive hospital liaison com-mittee network have obviated much of the contro-versy surrounding the treatment of Witnesschildren. Actually, a "child" cannot be one ofJehovah's Witnesses. We practise adult or mentallycompetent baptism following the pattern of JesusChrist. Of course, we are glad if our childrenespouse our beliefs, but as I reject Muramoto'sclaim of adult control, so I reject the thought thatWitness parents "indoctrinate" their children. Myown daughter, in company with the children of somany, could not be told what to do, certainly fromthe age of six months onwards, yet from the timeshe was a teenager has enthusiastically adoptedthe faith of her parents. Our two granddaughtersappear to have inherited their mother's lack ofmalleability.
Internet ethics and anonymiityProfessor Muramoto questions the motives of theWatchtower Society and also of the membershipat large. At least he has the honesty to declare hismotives on his public website on the Internet,where he openly admits to religious differenceswith his own Jehovah's Witness wife. To be utterlyforthright, I believe that such disclosure of interestshould have been made on publication of his firstarticle; none the less he has the merit of acceptingresponsibility. How can similar respect be ac-corded to anonymous dissidents, some of whomstill claim to be members of our fellowship? Usualpolice advice about the receipt of anonymous let-ters is to ignore them. Isn't that advice still goodwhen it comes to anonymous offerings on the
Internet? With so much accredited religious, legaland medical information on my faith readily avail-able in over 250 languages why should such wildand unfounded accusations as appear on theInternet be considered? Maybe Thurber's adviceis apt: "Get it right or leave it alone, the conclusionyou jump to, may be your own" !23
Blood semanticsMuramoto makes much of the argument thattransfusions are not "eating". My original articleexplained that the blood "laws" in The Bible arebased upon the reverence for life and itsassociation with blood. However, of interest is TheTimes law report24 entitled Consuming throughinjection. It discusses the case in which a personwas charged with driving with an excess of alcoholpresent in his body. The alcohol had been"consumed" when a doctor injected the defendantwith Kenalog containing a 1.5% benzyl alcohol.The law report defined that "'consuming' in itsusual context did not embrace sniffing, or absorb-ing by way of injection or some patch attached tothe body, but was capable of a variety of meaningsdepending on the context. The court was notentitled to restrict the meaning of consuming tothe act of drinking, and to no other mode of intro-duction or injection. .."
I am not medically qualified to discuss Mu-ramoto's convoluted reasoning about blood beinga cellular organ transplant further than tohighlight the danger of pedantically limiting wordmeanings. All law, as I have previously stated,must be kept in the spirit as much as in the letter!
Religious liberty in EuropeProfessor Massimo Introvigne'S25 thoughtful re-view suggested that a rise in intolerance againstreligious minorities is developing. Openness inmedicine, government, religion and almost every-thing else is becoming the criterion. Jehovah'sWitnesses welcome honest examination. Theirmeetings, literature, and branch and centraloffices are open to all sincere investigators. TheWitnesses subscribe to the view expressedabove-if you have nothing to hide why shouldyou need to be secretive? However, ProfessorIntrovigne believes that truth is distorted bylistening to the claims of ex-members of "sects" inisolation. Actually his study only mentionsJehovah's Witnesses once, in passing. His article isnot about Jehovah's Witnesses. He does, however,believe, in company with the vast majority, that:"Good ethics start with good facts . . .", and isconcerned that frequently only one side (and thenegative side at that) is heard. One small point

380 Transfusion-free treatment ofJehovah's Witnesses: respecting the autonomous patient's motives
gives the flavour of his paper: "Words are not neu-tral. Words such as 'cults' are easily used as toolsof hate and discrimination, and should beavoided . . . the most neutral term is 'religiousminorities"'. Respect for another point of view isalso part ofhuman rationality and conscience. TheTimesM6 has a profoundly moving story "of acouple who found a stranger, a boy, dying of knifewounds as they walked home. They held him intheir arms and spoke loving words, and when hegot home the man could not even bear to throwaway the water that rinsed his bloodstained shirt.He poured it onto a growing rosebush as aninstinctive gesture of respect for the boy's dyingbody . . .." Surely an illustration of an "intuitivemoral sense" associated with life, death and blood.Respect for life, blood, conscience, and liberty arethe bedrock of civilisation, let alone the faith ofJehovah's Witnesses.
Discussion ofMuramoto's hypotheticalreligion and appendixI believe that my two articles have demonstratedthat Muramoto's suggestions are unethicallybased, legally erroneous, medically dangerous,morally questionable and theologically superficial.The temerity of his appendix, a protocol which hesuggests doctors adopt in treating all non-emergency surgery Witness patients is nothingshort of an abusive transformation of the medicalrole of succour and care into that of "devil's advo-cate" and "trickster". For example in Appendix 3his argument is merely a cleverly worded duplica-tion of the view that "life must be saved at allcosts". Blood is sacred because it symbolises life,LIFE is sacred because - Christians hold - it is agift from God, and that life must be lived (or died)in the consciousness of this reality. Jehovah's Wit-nesses respect the gift of life by adopting healthylifestyles: we avoid nicotine, recreational drugs,alcohol abuse, sexual promiscuity AND "abstain"from blood. Are doctors interested in engaging in,or qualified to engage in, theological argumentwith patients already anxious and possibly vulner-able because of the need for medical treatment?Muramoto says: "Some may argue that thesequestions make a value judgment of religiousbeliefs under the guise of medical discussion ...
that posing those questions is manipulativetowards the patient's religious faith . . . ".' Exactlyright! I do believe Muramoto's appendix is anaffront to my faith, and an attempt to coerce ourmembers with complicated philosophical inquisi-tion. We welcome sincere questions. But no onewould welcome their deeply held convictionsbeing attacked under the cloak of sincerity.
Availability of alternativesThomas," concluding a major article entitled Theworldwide need for education in nonbloodmanagement in obstetrics and gynaecology, notedthat: "It should be clear from the foregoing thatmany viable alternatives to the use of blood trans-fusions do exist and are available to all practisingobstetricians and gynaecologists. It is not the lackof these facilities but perhaps a lack of knowledgeabout them, which may inhibit many practitionersfrom their useful application . . .". Probably theslow, progressive, careful advancement in medicalpractice is generally beneficial for patients.Waldenstrom28 has the salutary story of theinscription on a tombstone reading: "'I felt well,but wanted to feel better-therefore I am here!'The careful adjustment of therapy in order toobtain slow but steady improvement is oftensuperior to the dramatic results that seem morestriking. . .". This was with reference to the treat-ment specifically of the leukaemias. However,ignorance of now widely recognised and fre-quently employed techniques to avoid totally theuse of transfusions should no longer be the causeof tension between the medical community andJehovah's Witnesses. Medical literature is con-stantly presenting articles on blood conservationbenefits, the use of intra-operative blood salvage,haemodilution advances, plasma expanders andultrasonic tools, let alone advances with drugtherapies, including the use of erythropoietin,aprotinin, etc. The American Journal of Surgery 2'contains a useful 80-page review of the "state ofthe art" in bloodless medicine. Hospitals withprotocols for treating adult patients without bloodare legion throughout the world, with over 120such centres in the USA alone. Neonatal special-ists are developing new micro blood-samplingtechniques, including the use of an infrared-scanoptical probe. The Witnesses hospital liaisoncommittee network has information freely avail-able in a short fact sheet which itemises 105medical references to bloodless, medical and sur-gical strategies and I would be happy to supplysuch on request or reply to any comments.30 Suchongoing progress suggests to some that thegeneral use of transfusions will eventually becomeobsolete.
ConclusionThe charges against our views in a medicalcontext are clearly out of date! Our faithful adher-ence to Biblical tenets has resulted in the develop-ment of new surgical and medical techniques toobviate the use of blood therapy, which are in thevery forefront of medical developments. The

Malyon 381
atmosphere between members of our faith and themedical profession as a whole is becomingincreasingly relaxed and even friendly. Even whenmisunderstandings have arisen our members haveassumed that doctors and surgeons have beenwell-intentioned. History is full of examples ofhatred and conflict following behind suspicion ofpure motives. Surely our movement has the rightto expect that its members' actions as well as theirmotives be treated with optimism and respect.
Response to author's noteI was asked reply to Dr Muramoto's articles by thejournal's editor. I felt it wrong to ascribe badmotives to Dr Muramoto. However, his lateauthor's note3 does, I believe, reveal the extent ofhis mischief-making. After years of persecution,dating back to the second world war, an amicableagreement was brokered between the governmentof Bulgaria and Jehovah's Witnesses by the Euro-pean Commission for Human Rights. AlainGaray, Avocat a la cour, Paris was instructed byJehovah's Witnesses to be part of the negotiatingteam and he confirms that "it was accepted by allsides that the agreement reflected normal practicewithin the Jehovah's Witness religion around theworld" (personal communication from A Garay).As I have stated, we do not monitor the medicalchoices of our members, and even if we were tolearn one had accepted a blood transfusion ourministers would still offer pastoral care. TheCharter of the Christian Association of Jehovah'sWitnesses accepted by the Bulgarian governmentaccords with the unchanged and long establishedbeliefs of Jehovah's Witnesses internationally:"The Denomination of Jehovah's Witnesses ofBulgaria may not exercise any control over the freewill of believers but allows them to exercise theirconscience consistent with godly Bible principles.Nor does the Denomination arbitrarily applysanctions in connection with the medical care thatJehovah's Witnesses conscientiously seek forthemselves and their children. The Denominationadheres to the loving and righteous principles ofGod's Word in this aspect of Christian life." DatedJuly 15th 1998, confirmed October 7th 1998. Sixmillion Jehovah's Witnesses are not confused!
I feel like echoing the words of Anne Frank3."It's difficult in times like these: ideals, dreamsand cherished hopes rise within us, only to becrushed by grim reality. It's a wonder I haven'tabandoned all my ideals, they seem so absurd andimpractical. Yet I cling to them because I stillbelieve in spite of everything, that people are trulygood at heart".
AcknowledgementMy thanks to my patient "Secretary" FranSkinner
David Malyon is Chairman of the J7ehovah'sWitnesses Liaison Committee, Luton, Bedfordshire.
References1 British Medical Association. Medical ethics today. London: Brit-
ish Medical Association 1993:318.2 Muramoto 0. Bioethics of the refusal of blood by Jehovah's
Witnesses: part 1. Should bioethical deliberation considerdissidents' views? Journal ofMedical Ethics. 1998;24:223-30.
3 Muramoto 0. Bioethics of the refusal of blood by Jehovah'sWitnesses: part 2. A novel approach based on rationalnon-interventional paternalism. Journal of Medical Ethics.1998;24:295-301.
4 Malyon D. Transfusion-free treatment of Jehovah'sWitnesses-respecting the autonomous patient's rights. journalofMedical Ethics 1998;24:302-307.
5 Shakespeare W Hanzlet. Act 1 Scene 3.6 Treasure T. Lessons from the Bristol case. British Medical Jour-
nal 1998; 316:1085-6.7 Ridley M. Origins of virtue. Harmondsworth: Penguin,
1996:19.8 Blake W Songs of innocence. Oxford: Oxford University Press,
1789.9 Ritchie A. Good will keeps the NHS going. Sunday Timnes. 1998
Jul 5:5.10.10 The Bible. 1 Corinthians 13:4-7.11 The Bible. Matthew 6:22.12 The Bible. 1 Timothy 1:8,9,5.13 Anonymous. Living up to Christian dedication in freedom. The
Watchtower 1998 Mar 15: 20.14 See reference 1:326, 327.15 Kitchens CD. Are transfusions overrated?[editorial]. AmIerican
Jtournal ofMedicine 1993; 94:117-19.16 See reference 15 and table 1.17 van Iterson N et al. Systemic haemodynamic and oxygenation
during haemodilution in children. Lancet 1995;346: 1127.18 Nielsen HJ. Detrimental effects of perioperative blood transfu-
sion. British Journal of Surgery 1995:82:582-7.19 In Re T (Adult: refusal of treatment) 1993 Fam 95 CA.20 St George's NHS Trust v S; REG v Collins, Ex Parte S 1998 3
All ER 673.21 See reference 1:75.22 Savulescu J et al. Altruism by proxy: volunteering children for
bone marrow donation - substantial harm but substantial ben-efit. British Medical Journal 1996;312:242.
23 Thurber J. Vintage Thurber. London: Hamish Hamilton, 1963:401.
24 The Times Law Reports. Consuming through injection. 1996Feb 15. See also Director of Public Prosecutions v Johnson1995 1 WLR 728 DC.
25 Introvigne M. Religious liberty in Europe. Turin, Italy: Centre forStudies on New Religions, 1997:4.
26 Purvis L. This was a baby too far. The Times 1998 Jun 30: 20.27 Thomas JM. The worldwide need for education in nonblood
management in obstetrics and gynaecology. Journal of the Soci-ety of Obstetricians and Gynaecologists of Canada 1994;Mar:1486.
28 Waldenstrom J. To treat or not to treat, this is the real question.Medical Oncology & Tumour Pharnmacology 1986:3:3-4.
29 American Journal of Surgery 1995:170:6A. Consensusconference: Blood management, surgical practice guidelines.Guest editor, Spence RK. (The whole issue is devoted to thecoverage of this conference.)
30 Hospital Liaison Committees for Jehovah's Witnesses. Addressand contact details for correspondence, comment and requestfor literature: c/o David Malyon, 3 Rose Vale, Hoddesdon,Herts. EN 11 8NR. Tel: 01992 443104. Fax: 01992 470820.
31 Frank A. The diary of a young girl. Harmondsworth: Penguin,1997:330.