Embed Size (px)
Citation preview
COMPLICATION AND TREATMENT OF ACUTE
RESPIRATORY DISTRESS
Treatment
• Start with Neonatal Resuscitation Program!

Surfactant Therapy
• most effectively in infants <30 weeks and those birthweight <1250g
• Who to give surfactant to?
• depressed preterm infants who have no spontaneous respiration after 30 s of ventilation
• preterm infants below 28 weeks gestation
• preterm infants between 28-32 weeks
• more mature or larger infants
Timing of Surfactant Therapy
• attempts to treat with surfactant before the infant can breathe resulted in more BPD
• there fore surfactant delivery within first minutes of life not indicated
• the first dose has to be given as early as possible to the preterm infants requiring mechanical ventilation.
• the repeat dose is given 4-6 hours later based on FiO2
Surfactants
• Survanta, a natural surfactant, bovine derived 4ml/kg/dose
• Curosur, a natural surfactant, porcine derived 1.25ml/kg/dose
Surfactant Therapy
• Multidose endotracheal instillation: 4ml/kg
• Treatment (rescue) is initiated as soon as possible n the 1st 24hour of life
• Dose repeated - via the ET tube 6-12 hourldy for a total 2-4 doses

• PaO2 should be maintained between 60-70mmHg
• pH should be maintained above 7.25
• if hypoxemia (PaO2 < 50mmHg) nCPAP should be added at 8 to 10 cmH20.
Supportive Treatment
• Avoid Hypothermia
• IV Fluids and Calories
• Warm Humidified O2
Ventilation
• Controlled
• if infant have no breathing effort, no option to override ventilator
• a preset peak inspiratory pressure is delivered to the patient at preset respiratory rate
• Supported
• Continous Positive Airway Pressure (CPAP) - infant has breathing effort and to prevent the collapse of the alveoli
• based on peak end expiratory flow (PEEP)
Prevention
• Prevention of prematurity
• Betamethasone to women 48 hour before delivery 12mg IM for 2 doses 12 hours apart
• cervical cerclage, bed rest treatment of infections, and administration of tocolytic medication
• prevention of neonatal cold stress, birth asphyxia and hypovolemia
Acute Complication
• Apnoea of Prematurity
• Air Leak
• Patent Ductus Arteriosus
• Infection
• Intracranial Haemorrhage
• Prmary Pulmonary Hypertension Newborn

Apnea of Prematurity• the cessation of pulmonary airflow for
specific time interval, usually longer than10-20s
• central apnea complete cessation air flow and respiratory effort with no chest movement
• obstructive apnoa no airflow but chest movement presents
• Common in premature infants, because they usually responds paradoxically to hypoxia by developing apnea rather than increasing in respiration as do mature infants
Pulmonary Air Leak• assisted ventilation with high PIP and PEEP can
cause overdistenstion of the alveoli and causing rupture
• should be suspected when child suddenly deteriorated with hypotension, apnea, or bradychardia or when metabolic acidosis persistent
• eg pneumomediastinum, pneumopericardium, interstitial emphysema, pneumothorax, subcutaneous emphysema
• pneumothorax can be diagnosed based on unequal transillumination of the chest
• diagnosis can be made through chest x ray
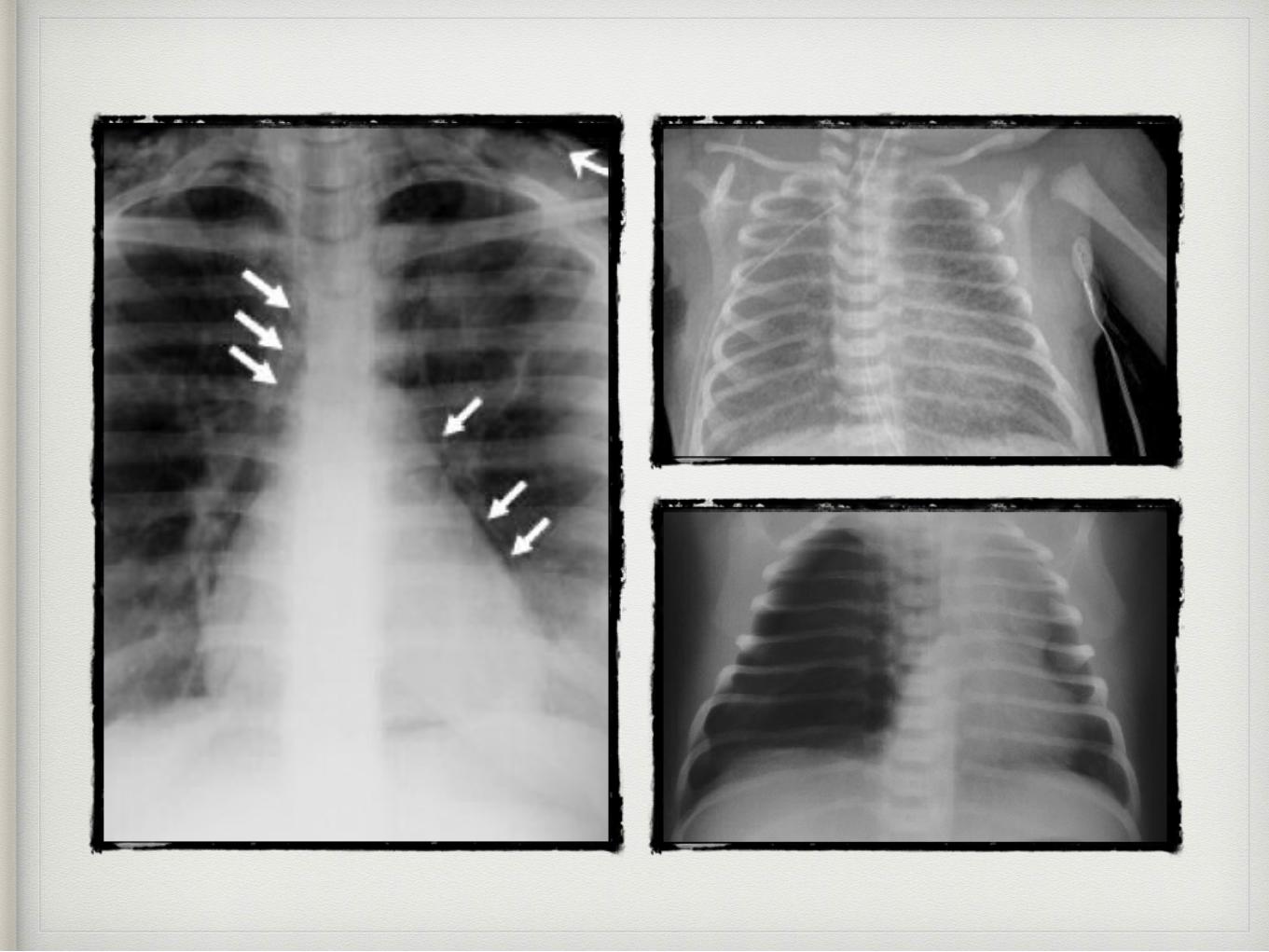
Patent Ductus Arteriosus
• in preterm complicated when hypoxemia of RDS, leads to persistent PDA that creates a shunt between pulmonary and systemic circulations.
• left to right shunt (systemic to pulmonary via PDA) lead to heart failure and pulmonary oedema
• clinical features, wide pulse pressure/ bounding pulse, systolic or continous murmur, apnea, hyperactive precordium
• confirm PDA with echo
• treatment, fluid restriction and diuretic administration + indometacin if no improvement after 24-48 hours.
• administered (0.2mg/kg) intravenously every 12 to 24 hours for three doses
Intracranial Hemorrhage
• intraventricular hemorrhage is observed in 20% to 40% of premature infants
• higher frequency in infants with RDS who require mechanical ventilation
• cranial ultrasonography is performed in premature neonates less than 32 weeks and 36 weeks or as indicated (suspected seizures)
Primary Pulmonary Hypertension of the Newborn
(PPHN)• characterized by severe hypoxemia
without evidence by parenchymal lung or structural heart disease.
• significant right to left shunt through patent foramen ovale, PDA and intrapulmonary channels is another characteristics.
• echo and cardiac catheterisation confirm the diagnosis
Infection• complicate the management of
respiratory distress syndrome in various of ways
• including the invasive procedures e.g. venepuncture, catheter or use respiratory equipment
• use of steroids provide access to microorganism as well
• increase incidence of septicaemia secondary to staph epidermis and/or candidal infection
Necrotising Enterocolitis
• suspect necrotising enterocolitis if abnormal abdominal finding and during physical examination.
• radiography can be done to confirm the diagnosis
Chronic Complication
• Retinopathy of Prematurity
• Bronchopulmonary Dysplasia
• Neurological Impairment
Retinopathy of Prematurity• caused by acute and chronic effects of O2
toxicity on the developing blood vessels of the premature infant retina
• cause vasoconstriction -> vaso-obliteration -> neovascularization
• increase risk of ROP if infants have a partial pressure O2 (PaO2) value more than 100mmhg
• to closely monitor and to maintain 50-70mmHg
Retinopathy of Prematurity
Bronchopulmonary Dysplasia• chronic lung disease define as requirement for oxygen
at corrected gestational age 36 weeks.
• BPD increase as gestational age decrease
• related directly with high volume and/or pressure used for mechanical ventilation or to manage infection, and inflammation
• failure RDS to improve after 2 weeks and the need prolonged mechanical ventilation at CGA 36 weeks are the characteristics of patient of RDS whom BPD develops
• clinical manifestation, O2 dependence,hypercapnia, compensatory metabolic alkalosis, pulmonary hypertension, poor growh and development right sided heart failure.
Neurological Impairment
• occurs approximately 10-70% of infants and is related with infant gestational age, the extent and type of intracranial pathology and presence of hypoxia and infections
• Hearing, visual and learning disability needed to be assessed.
–Johnny Appleseed
Thank You
Reference
• Paediatric Protocol 3rd edition
• Medscape
• Nelson Essentials of Paediatrics 5th edition