Embed Size (px)
Citation preview

Correspondence and Reprint requests : Dr. R. Hemalatha, MD,Deputy Director, Head, Department of Microbiology, NationalInstitute of Nutrition, Indian Council of Medical Research, JamaiOsmania (PO), Hyderabad- 50000 7, Andhra Pradesh, India.
[DOI-10.1007/s12098-010-0108-z]
[Received July 06, 2009; Accepted April 19, 2010]
Original Article
Respiratory Syncitial Virus in Children with AcuteRespiratory Infections
R. Hemalatha, G. Krishna Swetha, M. Seshacharyulu1 and K.V. Radhakrishna1
Departments of Microbiology and 1Clinical Division, National Institute of Nutrition, Jamia-Osmania, Hyderabad,India
ABSTRACT
Objective. To study the nutritional status of children with Respiratory Syncitial virus infection.
Methods. One hundred and twenty six children with acute respiratory infection, between the age of 4-24 months, wereinvestigated for RSV infection with bronchiolitis, pneumonia and upper respiratory tract infection. Nasopharyngeal aspirateswere collected and cytokine responses were determined by ELISA. Upper respiratory tract infections were detected in 16.66%,bronchiolitis in 30.15% and Pneumonia in 53.17% children.
Results. Of the 126 patients, 46.66% children were positive for RSV while 58.33% were negative for RSV. Children withbronchiolitis were more commonly positive for RSV compared to URTI and pneumonia. RSV was almost equally distributedamong boys (42.5%) and girls (48.7%). More children were RSV positive when the mean age lesser (8.4 mo) was comparedto RSV negative (9.93 mo). Well nourished children and children with normal birth weight had more RSV positives, thoughnot statistically significant. In a sub sample analysis of cytokines done (n=25), Interleukin-2 and Interleukin-8 levels were higherin the RSV positive children and these levels declined after 5 days of illness.
Conclusions. RSV is more commonly associated with bronchiolitis in younger infants with normal birth weight or more weightfor age (WFA). Proinflammatory cytokine IL-8 was secreted at high concentrations in the nasopharyngeal aspirate in all thechildren. [Indian J Pediatr 2010; 77 (7) : 755-758] E-mail: [email protected]
Key words : Respiratory syncitial virus (RSV); Bronchiolitis; Weight for age; Well nourished children; IL-8
RSV is the most common virus isolated in respiratoryinfections1 and is frequently detected in hospitalizedchildren.2 It is the main cause of bronchiolitis worldwideand causes up to 70-80% lower respiratory infectionsduring monsoon and winter.3 In India, studies based onthe isolation and sero survey have demonstrated RSV tobe the main virus responsible for lower respiratory tractinfections in children below 5 yrs of age.4 The severity ofRSV infection in young children varies from a non clinicalor mild respiratory infection to severe lower respiratorytract infection that may lead to hospitalization andoccasionally death. Though, the mechanisms underlyingthe highly variable disease course in children is stillpoorly understood, it is believed that children with severeRSV disease suffer from enhanced inflammatory lesions
rather than from virus induced cytopathy.5 Children whoexperience RSV infection in early in life, run a high risk ofsubsequent asthma and recurrent wheezing. Moreover,the sera and nasal secretions of the RSV infected infantsshow a marked increase in the levels of Th-2 cytokinesand chemokines.6
In vitro studies have shown that epithelial cells ormacrophages infected with RSV secrete high concentration ofIL-87. Studies on infants infected with RSV also show elevatedlevels of IL-8 in serum and nasopharyngeal aspirate and to thelarge number of neutrophils seen in the lavage fluid ofthese infants.8 It is now recognized that neutrophils play animportant role in viral respiratory tract infections, butimportance of their role in eliminating viral infection is stillunclear and indeed they may have little or no effect in limitingviral replication. However, there is evidence that they play animportant role in the causation of symptoms duringrespiratory viral infections.8 Several studies havesuggested that IL-2 is an appropriate means ofdetermining inflammatory response in patients withsevere acute viral bronchiolitis, in the acute phase of thedisease.9
Indian Journal of Pediatrics, Volume 77—July, 2010 755

R. Hemalatha et al
756 Indian Journal of Pediatrics, Volume 77—July, 2010
The mutually adverse interactions betweenmalnutrition and infection are complex and operatethrough various mechanisms. The immune response,especially cell mediated immunity is known to be poor inundernourished children. There are, however, very few studiesto show the relationship between RSV infection, nutritionalstatus of the children and local cytokine response which playsa key role in the outcome of the disease. The presentstudy was undertaken to investigate the nutritional statusof RSV infected children having respiratory infections,with special attention to body weight, age, hemoglobin,vitamin A and local IL-2 and IL-8 from nasopharyngealaspirate.
MATERIALS AND METHODS
The present cohort study was carried out at a tertiary carecentre, Niloufer Hospital, Hospital for Women and ChildHealth, Hyderabad from the months of August throughMarch 2007-2008. Inclusion criteria were: All childrenwith respiratory infection who had visited the outpatient(OP) department during the study period,diagnosis of Pneumonia, bronchiolitis or Upperrespiratory infection(URI) with history of illness not morethan five days. Exclusion criteria were: Children withcongenital heart disease, chronic lung disease, familyhistory of asthma, and other chronic disorders. This studywas approved by the Institutional Review Board (IRB)and written informed consent was taken.
Acute respiratory tract infection was defined as thepresence of cough with or without fever for less than 2wks. Bronchiolitis was diagnosed in those who presentedwith the prodromal symptoms of rhinorrhea, cough, lowgrade fever, followed by paroxysmal wheezy cough,dyspnea, with signs of air hunger, chest retractions,wheezing on physical examination and hyperinflation oflungs with patchy atelectasis on chest radiograph.Pneumonia was diagnosed in those who presented withhistory of poor feeding, respiratory distress with minimalwheeze, cough with chest retractions, shaking chillsaccompanied with fever, clinical findings of decreasedbreath sounds, consolidation or scattered rales heard allover the chest over the affected areas, and featuressuggestive of consolidation or patchy or interstitialinfiltration on chest radiography.
For all the cases, clinical history and physicalexamination was done and recorded. Weight wasmeasured to the nearest 100 g with an electronic scale(Secca). Infants were weighed with the help of aninfantometer. Low birth weight was defined as thoseinfants who were weighing ≤ 2499 g at birth, irrespectiveof gestational age. From all cases, 2 ml blood was collectedin a plain vial for measuring Hemoglobin (Hb) status andVitamin A levels. Vitamin A levels were determined by
High Performance Liquid chromatography (HPLC).Anthropometric measurements were taken to assess theirweight for age, using Gomez Classification.Nasopharyngeal Aspirate (NPA) was collected asepticallyby passing size 5 feeding tube into the nasopharynx andapplying gentle suction with a syringe. Secretions wererinsed into collecting vials with 1ml of phosphate buffer.After centrifugation of NPA to precipitate cells, thesupernatant was frozen at -700 until analyzed forcytokines and serum samples by ELISA (DiacloneResearch). Total protein from NPA was determined byModified Lowry’s method. Statistical analysis of the datawas done using SPSS software.
RESULTS
Over a period of eight months, a total of 126 children withacute respiratory infection were recruited. Of the 126children recruited, 21 had URTI, 38 had bronchiolitis and67 had pneumonia. A total of 56 children were positive forRSV while, 70 were negative. Distribution of clinical casesin the age groups <1 yr and ≥1 yr showed a significantlyhigher proportion of younger infants to be infected withRSV. The mean age of children with RSV was 8.4 monthsand 9.4 months for RSV negative children. Of the 126cases, 22 children were treated as outpatients, and 104were hospitalized. Of these 104, 99 children recovered andfive children (3 RSV + and 2 RSV -) had fatal outcomesand died in the hospital (Table 1).
Children with bronchiolitis (60.5%) were more commonlypositive for RSV compared to URTI (19%) and pneumonia
TABLE 1. RSV Prevalence and Its Association with VariousParameters
RSV +ve(56) RSV–ve (70)
Respiratory infection(n) n (%) n (%)URTI(21) 4 (19.0) 17 (81.0)Bronchiolitis(38) 23 (60.5) 15 (39.5)Pneumonia(67) 29 (43.3) 38 (56.7)
Outcome(n)Recovered(99) 48 (48.5) 51 (51.5)Death(5) 3 (60) 2 (40)OP(22) 5 (22) 17 (77.2)
Age (n)<1 yr(89) 47 (52.8) 42 (47.2)>1 yr(37) 9 (24.3) 28 (75.7)
Sex(n)Males(87) 37 (42.5) 50 (57.5)Females(39) 19 (48.7) 20 (51.3)
Wt/Age (n)<75% (71) 27 (38) 44 (62)>75 %(55) 29 (52.7) 26 (47.3)
Birth Weight (n)Low(26) 9 (34.6) 17 (65.4)Normal(94) 47 (50.0) 47 (50.0)
n followed by percentage in parenthesis

Respiratory Syncitial Virus in Children with Acute Respiratory Infections
Indian Journal of Pediatrics, Volume 77—July, 2010 757
(43.3%). RSV positive cases were almost equally distributedamong boys (42.5%) and girls (48.7%), (P=0.279). A higherproportion of younger children and well nourished childrenwere positive for RSV (Table 1). The mean WFA and theserum Vitamin A levels were higher in the RSV infectedchildren, while the hemoglobin status and height for agewas comparable.
DISCUSSION
In the present study, nutritional status of children withRSV infection, and the nasopharyngeal cytokine levels inthem were studied. In a number of studies on hospitalizedchildren with bronchiolitis or pneumonia, RSV has beenfound to be associated with a higher proportion ofbronchiolitis compared to pneumonia.10 Similarly in thepresent study, RSV was more commonly associated withbronchiolitis than pneumonia or upper respiratoryinfections (URTI). Earlier studies showed that RSVprevalence was found to be more in males than females11
and male gender was considered an independent riskfactor for the development of severe RSV infection. Incontrast, the authors observed an equal distribution ofRSV in boys and girls though association with youngerage was similar to that reported elsewhere.12 Thoughmalnutrition has been found to be a risk factor for acuteLRI,13 animal studies on RSV infection and nutritionshowed conflicting results.14 In the present study, goodnutritional status (WFA) and higher Vitamin A levelswere associated with RSV infection. A similar observationwas made by Clarios et al who reported good nutrition,obesity and over nutrition as risk factors for RSVinfection.11
The role of inflammatory mediators in thepathogenesis of RSV disease though not well-understood,has been studied by various people. In vitro studies haveshown that epithelial cells or macrophages infected withRSV secrete high concentration of IL-8.7,15,16 Similar to thepresent study, other studies on infants infected with RSValso showed elevated levels of IL-8 in serum andnasopharyngeal aspirate that has been suggested incontributing to large number of neutrophils recruited inthe lavage fluid of these infants.8 That neutrophils
clinical diagnosis
pneumonia bronchiolitis
IL-2
in p
g/gm
pro
tein
0
50
100
150
200
250
300
Il2 1st day Il2 5th day
a
a
b
a
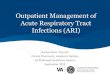
Fig. 1. IL-2 levels in children with pneumonia and bronchiolitison days 1 and 5.
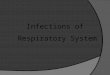
In a sub sample of 18 RSV positive and 7 RSV negativecases, nasopharyngeal IL-2 and IL-8 was done. The totalconcentration of IL-2 and IL-8 ranged from 45.4 to 722 pg/gtotal protein and 597 to 8127 pg/g total protein, respectively,with IL-2 being detectable in less than 50% of the cases( 12 outof 25). However, after 5 days, IL-2 was detectable in nearly allcases (22 out of 25 cases), but the total concentration decreasedfrom the initial level. The mean concentration of IL-2 and IL-8were higher in the RSV positive cases though not statisticallysignificant (Table 2). Categorizing the cases based on theirclinical outcome, it was found that on day 1, bronchiolitisand pneumonia cases had high IL-2 and IL-8 levels,however, children with bronchiolitis had relatively lowerconcentrations of IL-2 compared to children with pneumonia(Fig. 1). On day 5, children with pneumonia maintained sameconcentrations of IL-2 and IL-8 while children with bronchiolitissecreted lower IL-8 levels (Fig 2). Children with pneumonia,positive for RSV had significantly higher IL-8 concentrationscompared to those without RSV infection.
TABLE 2. RSV Infection and IL2, IL8 Response in Children withARI
RSV +ve RSV -ve
Vit A(µg/dl) 19.95 ± 1.513 16.42 ± 1.769Hb (g/dl) 11.01 ± 0.298 10.78 ± 0.237IL-2 day 1 285 ± 64.76 235.3 ± 29.18 day 5 213 ± 44.4 157.7 ± 33.21IL-8 day 1 3425.2 ± 436.5 2176.7 ± 666.84 day 5 2670.9 ± 384.8 1092.6 ± 180.5
IL-2 and IL-8: pg/gm of total protein. The values are Mean ± SE
clinical diagnosis
pneumonia bronchio litis0
1000
2000
3000
4000
5000
IL8 1st day Il8 5th day
a
a
a
b
Fig. 2. IL-8 levels in children with pneumonia and bronchiolitison days 1 and 5.
Means with different superscript are significantly different withP<0.05

R. Hemalatha et al
758 Indian Journal of Pediatrics, Volume 77—July, 2010
recruited by local IL-8 secretion might contribute to thesymptoms during viral infection has been demonstratedby correlating neutrophil myeloperoxidase product withseverity of upper respiratory tract symptoms.17 However,while some investigators suggested IL-8 polymorphism inthe pathogenesis of hypersensivity reaction, otherssuggested sensitization of airway epithelium toenvironmental lipopolysaccharide exposure by altered IL-8 expression in RSV infection.18, 19
Thus, even in mild to moderately nourished children,the airway inflammation that results from the viralinfection is associated with a marked increase in IL-8 inthe infected sites of the lung, which might contribute toincreased local leukocyte response and hypersensitivityreactions. Under nutrition does not seem to be a riskfactor for RSV infection, however, it does not seem todecrease the chances of these children developingsequelae at a later date.
Acknowledgements
We are grateful for the skillful assistance rendered by the nursingstaff Santoshamma and Rajakumari in sample collection at Nilouferhospital.
Contributions: R H; Study design, conceptualization, supervision oflab work, manuscript writing, G K S; Lab work, preparation ofmanuscript, K V R; Recruitment of subjects, diagnosis andmanagement of cases, M S; Lab work.
Conflict of Interest: None.
Role of Funding Source: None.
REFERENCES
1. John TJ, Cherian T, Steinhoff MC, Simoes EAF, John M.Etiology of Acute respiratory tract infections in children intropical south India. Rev Infect Dis 1991; 13: S463-S469.
2. Yeolekar LR, Damle RC, Kamat AN. Respiratory viruses inacute respiratory tract infections in Western India. Indian JPediatr 2008; 75: 341-345.
3. Simoes EA. Respiratory syncitial virus infection. Lancet 1999;354: 847-852.
4. Chattopadhya D, Chatterjee R, Anand VK. Lower respiratorytract infection in hospitalized children due to RSV during asuspected epidemic period of RSV in Delhi. J Trop Pediatr1992; 38: 68-73.
5. McNamara PS, Smyth RL. The pathogenesis ofrespiratory syncitial virus disease in childhood. Br Med Bull2002; 61: 13-28.
6. Zhao J, Takamura M, Yamoaka A et al. Altered eosinophillevels as a result of viral infection and asthma exacerbation inchildhood. Pediatr Allergy Immunol 2002; 13: 47-50.
7. Becker S, Quay J, Soukup J. Cytokine (TNF, IL-6, IL-8)production by respiratory syncitial virus infected humanalveolar macrophages. J Immunol 1991; 147: 4307-4312.
8. Abu-Harb M, Bell F, Finn A et al. IL-8 and neutrophil elastaselevels in the respiratory tract of infants with RSV bronchiolitis.Eur Respir J 1999; 14: 139-143.
9. Katia M, Giugno, Denise C et al. Concentrations of IL-2 in thenasopharyngeal secretions of children with acute respiratorysyncitial virus bronchiolitis. Journal de Pediatr 2004; 80(4)
10. Parrot RH et al. Epidemiology of RSV infection in WashingtonDC-Infection and disease with respect to age, immunologicalstatus, race, sex. Am J Epidemiol 1973; 98: 289-300.
11. Rivera Claros R, Marin V, Castillo-Duran C, Jara L, Guardio S.Nutritional status and clinical evaluation of hospitalizedChilean infants with infection by RSV. Arch Latinoam Nutr1999; 49: 326-332.
12. Simoes EA. Environmental and demographic risk factors forRSV lower respiratory tract disease. J Pediatr 2003; 143: S118-S126.
13. Savitha MR, Nandeeshwara SB, Pradeep Kumar MJ, Ul-Haque F, Raju CK. Modifiable risk factors fro acute lower RTI.Indian J Pediatr 2007; 74: 477-482.
14. Victor Pena Cruz, Carol R, McIntosh Kenneth. Effect of RSVinfection on mice with protein malnutrition. J Med Virol 1991;33: 219-223.
15. Becker S, Koren HS, Henke DC. Interleukin-8 expression innormal basal epithelium and its modulation by infection withRSV and cytokines TNF, IL-1, IL-6. Am J Respir Cell Mol Biol1993; 8: 20-27.
16. Arnold R, Humbert B, Werchau H, Gallati H, Konig W. IL-8,Il-6 and soluble TNF receptor type 1 release from a humanpulmonary epithelial cell line (A549) cells. Am J Physiol 1995;269: L865-L872.
17. Teran LM, Johnston SL, Schroder JM, Church MK, HolgateST. Role of nasal IL-8 in neutrophil recruitment and activationin children with virus induced asthma. Am J Respir Crit CareMed 1997; 155:1362-1366.
18. Stemmler S, Arinir U, Klein W et al . Association ofinterleukin-8 receptor alpha polmorphisms with chronicobstructive pulmonary disease and asthma. Genes Immun2005; 6: 225-230.
19. Serene Foster , Kirk J. Bedford , Melanie E. L. Gould , WilliamR. Coward & Colin R. A. Hewitt. Respiratory syncytial virusinfection and virus-induced inflammation are modified bycontaminants of indoor air. Immunology 2003; 108: 109-115.