Embed Size (px)
Citation preview

Respiratory Syncytial Virus–AssociatedMortality in Hospitalized Infants andYoung ChildrenCarrie L. Byington, MDa, Jacob Wilkes, BSb, Kent Korgenski, MSb, Xiaoming Sheng, PhDa
abstractBACKGROUND AND OBJECTIVE: Respiratory syncytial virus (RSV) is a common cause of pediatrichospitalization, but the mortality rate and estimated annual deaths are based on decades-olddata. Our objective was to describe contemporary RSV-associated mortality in hospitalizedinfants and children aged ,2 years.
METHODS:We queried the Healthcare Cost and Utilization Project Kids’ Inpatient Database (KID)for 2000, 2003, 2006, and 2009 and the Pediatric Health Information System (PHIS)administrative data from 2000 to 2011 for hospitalizations with International Classification ofDiseases, Ninth Revision, Clinical Modification diagnosis codes for RSV infection and mortality.
RESULTS: The KID data sets identified 607 937 RSV-associated admissions and 550 deaths(9.0 deaths/10 000 admissions). The PHIS data set identified 264 721 RSV-associated admissionsand 671 deaths (25.4 deaths/10 000 admissions) (P, .001 compared with the KID data set). The2009 KID data set estimated 42.0 annual deaths (3.0 deaths/10 000 admissions) for those witha primary diagnosis of RSV. The PHIS data set identified 259 deaths with a primary diagnosis of RSV,with mortality rates peaking at 14.0/10 000 admissions in 2002 and 2003 and decreasing to 4.0/10000 patients by 2011 (odds ratio: 0.27 [95% confidence interval: 0.14–0.52]). The majority of deathsin both the KID and PHIS data sets occurred in infants with complex chronic conditions and in thosewith other acute conditions such as sepsis that could have contributed to their deaths.
CONCLUSIONS: Deaths associated with RSV are uncommon in the 21st century. Children withcomplex chronic conditions account for the majority of deaths, and the relative contribution ofRSV infection to their deaths is unclear.
WHAT’S KNOWN ON THIS SUBJECT: Respiratorysyncytial virus (RSV) infection is a commoncause of pediatric hospitalizations. Mortalityrates associated with RSV hospitalizations arebased on estimates from studies conducteddecades ago. Accurate understanding ofmortality is required for identifying high-riskinfants and children.
WHAT THIS STUDY ADDS: Mortality associatedwith RSV is uncommon in the 21st century, withannual deaths far lower than previous estimates.The majority of deaths occurred in infantswith complex chronic conditions or in those withlife-threatening conditions in addition to RSVinfection.
aDepartment of Pediatrics, University of Utah, Salt Lake City, Utah; and bIntermountain Healthcare, PediatricClinical Programs, Salt Lake City, Utah
Dr Byington conceptualized and designed the study, provided funding for the study, supervised thedata collection, analyzed the data, and drafted the initial manuscript; Mr Wilkes and Mr Korgenskiobtained and analyzed the data and critically reviewed the manuscript; and Dr Sheng performed thestatistical analyses and critically reviewed the manuscript. All authors approved the final manuscript.
www.pediatrics.org/cgi/doi/10.1542/peds.2014-2151
DOI: 10.1542/peds.2014-2151
Accepted for publication Oct 23, 2014
Address correspondence to Carrie L. Byington, MD, 26 South 2000 East, HSEB Suite 5515, Salt LakeCity, UT 84112. E-mail: [email protected]
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2015 by the American Academy of Pediatrics
PEDIATRICS Volume 135, number 1, January 2015 ARTICLE at UCSF Kalmanovitz Library & CKM on December 10, 2014pediatrics.aappublications.orgDownloaded from

Respiratory syncytial virus (RSV) isone of the most common infectionsof childhood. Almost all childrenexperience RSV infection by age2 years.1 In young children, RSVinfection often manifests asbronchiolitis or pneumonia and isa common cause of both outpatientvisits and hospital admission.2 RSVmay result in mortality.3,4 However,because public health agencies do notrequire deaths due to RSV to bereported (unlike influenza deaths inchildren), the relative contribution ofRSV infection to childhood mortalityis unclear.
Using data from a single tertiarycenter from 1976 to 1980, theInstitute of Medicine estimated thatthere were 4500 RSV-associateddeaths annually in children aged,5 years, with 60% of deaths(∼2700) occurring in infants.5 Theestimate was based on an assumptionthat 5% of infants and childrenhospitalized with RSV infection in theUnited States would die. Over thedecades, there have been significantimprovements in medical technology,and a mortality rate of 5% for USinfants and children hospitalized withRSV infection is unlikely to reflectcontemporary experience. Morerecent analyses found significantlylower estimates for bronchiolitis andRSV-associated mortality, withestimates of #510 deaths annually inchildren aged ,5 years, with 80%(#408) occurring in infants.4 Anotherstudy estimated 214 deaths in infantsaged ,1 year due to RSV and anadditional 132 deaths in childrenaged 1 to 4 years.3 These studiesmonitored trends only through the1990s. Data from the first decade ofthe 21st century demonstratea significant decline in bronchiolitishospitalizations in the United States.6
It is possible that trends in RSV-associated mortality have also changed.
Accurate estimates of RSV-associatedmortality may help to guideprevention and treatment strategies.Mortality is also an important
variable in cost-effectiveness studies.Recent studies of cost-effectivenessfor palivizumab have producedestimates that differ markedly.7
Differences in mortality estimatesincluded in the models stronglyinfluence the cost-effectiveness ratios,which in turn may influenceprophylaxis guidelines such as thosepublished by the American Academyof Pediatrics.8
Large administrative databases offeran opportunity to use data codedfrom inpatient encounters to monitortrends in health care utilization andoutcomes, including mortality. Theobjectives of the present study wereto describe contemporary RSVmortality rates and to identifyconditions associated with RSVmortality in hospitalized infants andchildren aged ,2 years. We used theAgency for Healthcare Research andQuality (AHRQ) and Healthcare CostUtilization Project (HCUP) Kids’Inpatient Database (KID) and thePediatric Health Information System(PHIS) database.
METHODS
Human Subjects
An AHRQ and HCUP data useagreement and training wascompleted for the KID data set. TheChildren’s Hospital Associationapproved use of the PHIS data set.The research was reviewed by theinstitutional review board of theUniversity of Utah and was deemedexempt and classified as non–humansubjects research.
Database Description and Queries
Two national pediatric databaseswere used to describe the annualnumber of inpatient admissions anddeaths associated with InternationalClassification of Diseases, NinthRevision, Clinical Modification(ICD-9-CM) codes for RSV infection.We queried the HCUP KID databasefor 2000, 2003, 2006, and 20099–12
and the PHIS administrative database
from 2000 to 2011.13 We identifiedhospitalizations with ICD-9-CMdiagnosis codes 480.1 (RSVpneumonia), 466.11 (RSVbronchiolitis), and 466.19(bronchiolitis, other) in infants andchildren aged ,2 years. The codeswere chosen to try and maximize thenumber of admissions and deathspotentially related to RSV.Bronchiolitis may be caused by manyviral pathogens,14 but RSV is the mostcommon, and diagnostic testing maynot always be performed. Althoughincluding ICD-9-CM code 466.19 forcase detection may falsely elevate theRSV mortality rate due to thepotential inclusion of deaths fromviruses other than RSV, this code iscommonly used when diagnostictesting is not performed and duringmonths when RSV is known to be themost common pathogen. We chose tofocus on the age range younger than2 years because the majority ofhospitalizations15 and deaths occur ininfants,3,4 and the American Academyof Pediatrics recommendations forthe use of palivizumab prophylaxiscurrently do not extend to childrenaged .2 years.8
HCUP KID
The KID is compiled by the AHRQ andis the only all-payer inpatient data setfor children in the United States. Theunweighted data include dischargeinformation for ∼3 million pediatrichospitalizations each year, andweighted estimates for ∼7 milliondischarges can be determined. Thelarge size and weighting allowcalculation of national estimates forboth rare and common conditions.16
We analyzed cross-sectional data forhospitalizations for the years 2000,2003, 2006, and 2009.9–12 States thatparticipate in HCUP providedischarge-level data for all inpatientdischarges for children from short-term, nonfederal general andspecialty hospitals. Data are availableevery 3 years. State participation inKID increased from 22 in 1997 to 44in 2009. In 2009, the KID database
2 BYINGTON et al at UCSF Kalmanovitz Library & CKM on December 10, 2014pediatrics.aappublications.orgDownloaded from
contained information on 7.4 millionweighted discharges from 4121community and children’s hospitals in44 states.
All admissions meeting theaforementioned criteria for RSV-associated hospitalization wereextracted from the KID database,including: sampling weight,admission year, admission month,discharge quarter, admission age,length of stay in days, dischargedisposition, flag for death, andICD-9-CM coding. The denominatorused to calculate an RSV mortalityrate was total RSV-associatedadmissions. To classify whether anRSV-associated admission or deathoccurred within the RSV season(November–March),17 we useddischarge quarter, length of stay, andadmit month.
PHIS Database
Operated by the Children’s HospitalAssociation, the PHIS is anadministrative database that capturesinpatient data from 44 specialtychildren’s hospitals in the UnitedStates.13 The PHIS data representa sample of children’s hospitals, andparticipating hospitals may choose tocontribute specific data elements. ThePHIS data set has not been designedto be a representative sample of allchildren’s hospitals and, unlike theKID data set, cannot be used togenerate national estimates.18 Thesame criteria used to identify RSV-associated admissions within the KIDdata set were applied to the PHISdatabase. RSV admissions, mortalityrate, total RSV deaths, and RSV deathsduring RSV season were calculated foreach year from 2000 through 2011.
Additional Data Obtained From KID andPHIS Data Sets
Additional information was gatheredfrom both data sets for infants andchildren with RSV-associated deaths,including: whether the death hada primary ICD-9-CM code for RSV;complex chronic conditions (CCC)19;surgical complications (using .300
ICD-9-CM codes); cardiac arrest,427.5 (cardiac arrest), 779.85(newborn cardiac arrest), V1253(history of cardiac arrest), 99.60(cardiopulmonary resuscitation),99.63 (closed chest cardiac massage);and sepsis, 995.91 (sepsis), 995.92(severe sepsis), 785.52 (septic shock),771.81 (newborn septicemia), 790.7(bacteremia), 04.184 (anaerobeinfection [necrotizing enterocolitis(NEC)]), 04.185 (Gram-negativebacterial infection NEC), 04.189(bacterial infection NEC), 038.0(streptococcal septicemia), 038.10(staphylococcal septicemia nototherwise specified), 038.11(methicillin-susceptibleStaphylococcus aureus septicemia),038.12 (methicillin-resistant S aureussepticemia), 038.19 (staphylococcalsepticemia NEC),038.2(pneumococcal septicemia), 038.3(anaerobic septicemia), 038.40(Gram-negative septicemia NEC),038.41 (Haemophilus influenzaesepticemia), 038.42 (Escherichia colisepticemia), 038.43 (Pseudomonassepticemia), 038.44 (Serratiasepticemia), 038.49 (Gram-negativesepticemia NEC), 038.8 (septicemiaNEC), 038.9 (septicemia nototherwise specified), and 040.0 (gasgangrene). Interfacility transfers werealso evaluated because thesetransfers could result in anunderestimation of mortality.
Statistical Analysis
We performed analyses taking intoaccount the complex sampling andweighting scheme of KID by usingsampling survey procedures in SASversion 9.3 (SAS Institute, Inc, Cary,NC). Numbers of RSV admissions, RSVdeaths, RSV mortality rates, andnumber of RSV deaths occurringduring RSV season were generated ineach of the study years. For mortalityrates, 95% confidence intervals (CIs)were calculated based on binomialdistribution. To calculate KID yearlyadmission and death estimates, weweighted our estimates by using thesampling weights from each of the
sample years. This method allowed usdescribe the RSV admissions anddeaths across the study period, whiletaking into account the differences inthe KID sampling frame across timeand the different numbers ofhospitals that contributed data to thePHIS database each year. To calculatePHIS yearly admission and deathestimates, we weighted our estimatesby using the total number of PHISRSV admissions for each study year.
To determine whether differencesbetween groups were significant,2-sample unpooled t tests withunequal variances were used and2-proportion unpooled z tests wereused to compare rates. A significancelevel of a = 0.05 was used todetermine statistical significance.Odds ratios (ORs) and 95% CIs werecalculated when a comparison wasmade between different years of study.
RESULTS
RSV-Associated Hospitalizations andMortality Rates in KID and PHIS DataSets
The KID data sets identified a total of607 937 RSV-associated admissionsand 550 deaths in the 2000, 2003,2006, and 2009 data sets (9.0 deaths/10 000 admissions). The PHIS dataset identified a total of 264 721RSV-associated admissions and 671deaths from 2000 to 2011 (25.4deaths/10 000 admissions) (P , .001compared with the KID data set).Interfacility transfers in the KID dataset occurred in 2.2% of encountersoverall, with 0.4% of encounters ina children’s hospital resulting ina transfer. The PHIS data setidentified that 1.3% of its overallemergency department volumeconsisted of interfacility transfers.20
All annual RSV-associatedadmissions, deaths, and mortalityrates for the KID and PHIS data setsare shown in Table 1. The annualmortality rates were higher in thePHIS data set for the years 2000,2003, 2006, and 2009 compared with
PEDIATRICS Volume 135, number 1, January 2015 3 at UCSF Kalmanovitz Library & CKM on December 10, 2014pediatrics.aappublications.orgDownloaded from
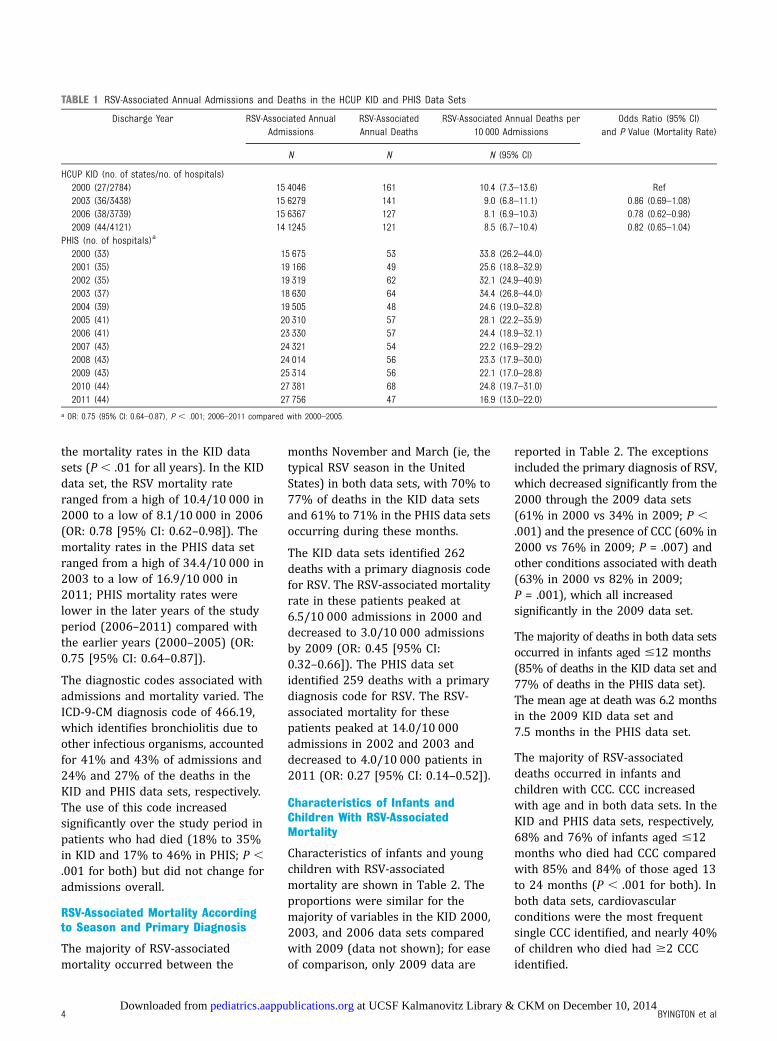
the mortality rates in the KID datasets (P , .01 for all years). In the KIDdata set, the RSV mortality rateranged from a high of 10.4/10 000 in2000 to a low of 8.1/10 000 in 2006(OR: 0.78 [95% CI: 0.62–0.98]). Themortality rates in the PHIS data setranged from a high of 34.4/10 000 in2003 to a low of 16.9/10 000 in2011; PHIS mortality rates werelower in the later years of the studyperiod (2006–2011) compared withthe earlier years (2000–2005) (OR:0.75 [95% CI: 0.64–0.87]).
The diagnostic codes associated withadmissions and mortality varied. TheICD-9-CM diagnosis code of 466.19,which identifies bronchiolitis due toother infectious organisms, accountedfor 41% and 43% of admissions and24% and 27% of the deaths in theKID and PHIS data sets, respectively.The use of this code increasedsignificantly over the study period inpatients who had died (18% to 35%in KID and 17% to 46% in PHIS; P ,.001 for both) but did not change foradmissions overall.
RSV-Associated Mortality Accordingto Season and Primary Diagnosis
The majority of RSV-associatedmortality occurred between the
months November and March (ie, thetypical RSV season in the UnitedStates) in both data sets, with 70% to77% of deaths in the KID data setsand 61% to 71% in the PHIS data setsoccurring during these months.
The KID data sets identified 262deaths with a primary diagnosis codefor RSV. The RSV-associated mortalityrate in these patients peaked at6.5/10 000 admissions in 2000 anddecreased to 3.0/10 000 admissionsby 2009 (OR: 0.45 [95% CI:0.32–0.66]). The PHIS data setidentified 259 deaths with a primarydiagnosis code for RSV. The RSV-associated mortality for thesepatients peaked at 14.0/10 000admissions in 2002 and 2003 anddecreased to 4.0/10 000 patients in2011 (OR: 0.27 [95% CI: 0.14–0.52]).
Characteristics of Infants andChildren With RSV-AssociatedMortality
Characteristics of infants and youngchildren with RSV-associatedmortality are shown in Table 2. Theproportions were similar for themajority of variables in the KID 2000,2003, and 2006 data sets comparedwith 2009 (data not shown); for easeof comparison, only 2009 data are
reported in Table 2. The exceptionsincluded the primary diagnosis of RSV,which decreased significantly from the2000 through the 2009 data sets(61% in 2000 vs 34% in 2009; P ,.001) and the presence of CCC (60% in2000 vs 76% in 2009; P = .007) andother conditions associated with death(63% in 2000 vs 82% in 2009;P = .001), which all increasedsignificantly in the 2009 data set.
The majority of deaths in both data setsoccurred in infants aged #12 months(85% of deaths in the KID data set and77% of deaths in the PHIS data set).The mean age at death was 6.2 monthsin the 2009 KID data set and7.5 months in the PHIS data set.
The majority of RSV-associateddeaths occurred in infants andchildren with CCC. CCC increasedwith age and in both data sets. In theKID and PHIS data sets, respectively,68% and 76% of infants aged #12months who died had CCC comparedwith 85% and 84% of those aged 13to 24 months (P , .001 for both). Inboth data sets, cardiovascularconditions were the most frequentsingle CCC identified, and nearly 40%of children who died had $2 CCCidentified.
TABLE 1 RSV-Associated Annual Admissions and Deaths in the HCUP KID and PHIS Data Sets
Discharge Year RSV-Associated AnnualAdmissions
RSV-AssociatedAnnual Deaths
RSV-Associated Annual Deaths per10 000 Admissions
Odds Ratio (95% CI)and P Value (Mortality Rate)
N N N (95% CI)
HCUP KID (no. of states/no. of hospitals)2000 (27/2784) 15 4046 161 10.4 (7.3–13.6) Ref2003 (36/3438) 15 6279 141 9.0 (6.8–11.1) 0.86 (0.69–1.08)2006 (38/3739) 15 6367 127 8.1 (6.9–10.3) 0.78 (0.62–0.98)2009 (44/4121) 14 1245 121 8.5 (6.7–10.4) 0.82 (0.65–1.04)
PHIS (no. of hospitals)a
2000 (33) 15 675 53 33.8 (26.2–44.0)2001 (35) 19 166 49 25.6 (18.8–32.9)2002 (35) 19 319 62 32.1 (24.9–40.9)2003 (37) 18 630 64 34.4 (26.8–44.0)2004 (39) 19 505 48 24.6 (19.0–32.8)2005 (41) 20 310 57 28.1 (22.2–35.9)2006 (41) 23 330 57 24.4 (18.9–32.1)2007 (43) 24 321 54 22.2 (16.9–29.2)2008 (43) 24 014 56 23.3 (17.9–30.0)2009 (43) 25 314 56 22.1 (17.0–28.8)2010 (44) 27 381 68 24.8 (19.7–31.0)2011 (44) 27 756 47 16.9 (13.0–22.0)
a OR: 0.75 (95% CI: 0.64–0.87), P , .001; 2006–2011 compared with 2000–2005.
4 BYINGTON et al at UCSF Kalmanovitz Library & CKM on December 10, 2014pediatrics.aappublications.orgDownloaded from

Those patients who died hadprolonged hospital stays, with a meanduration of 40.5 days in the 2009 KIDdata set and 40.2 days in the PHISdata set. Those who died outside ofthe typical RSV season (ie, who diedin April–October) had longer hospitalstays than those who died during thetypical season: 74.9 days comparedwith 25.7 days (P , .001) in the 2009KID data set and 63.5 days comparedwith 30.6 days (P , .001) in the PHISdata set. The majority of those whodied had ICD-9-CM codes forpotentially life-threatening conditionssuch as sepsis or surgicalcomplications in addition to RSVinfection.
DISCUSSION
We report estimates of RSV mortalityin infants and children aged ,2 yearsbased on 2 national data sources overthe course of the first decade of the21st century. RSV mortality ratesdeclined significantly in both datasets. They both indicated thatmortality during RSV-associatedhospitalizations is uncommon,occurring in 3 to 4/10 000 admissionsin those with a primary diagnosis ofRSV in the KID and PHIS data sets,respectively. The KID data set estimated121 deaths nationally in infantsand children with RSV-associated
admissions, 84 deaths during RSVseason, and 42 deaths with a primarydiagnosis of RSV in 2009. The PHISdata set had a mean of 56 deaths peryear, with 39 during RSV season and21 with a primary diagnosis of RSV.The annual deaths documented inthese contemporary data sources are5 to 100 times lower than 20thcentury estimates.3,4 Both data setsincreased in size during the studyperiod and identified characteristicsof infants and children who diedduring RSV-associatedhospitalizations that were almostidentical. The size of the data sets andthe concordance of the findingsenhance the generalizability of theresults. The majority of deathsoccurred in children who had CCCand other life-threatening conditionssuch as sepsis. Overall, RSV mortalitywas more common in the tertiarychildren’s hospitals of the PHIS dataset compared with the KID data,perhaps reflecting the medicalcomplexity of children cared for inthese facilities.21
RSV is one of the most significantcauses of infection andhospitalization in young children inthe United States and worldwide.17
The number of deaths in younginfants and children during RSV-associated hospitalizations is an
important public healthmeasurement. Our analysis providesmortality rates for infants andchildren aged ,2 years with RSV-associated hospitalizations. Both datasets provided mortality rates fora variety of situations, includingdeath during the traditional RSVseason, and for those with a primarydiagnosis of RSV. These mortalityrates are lower than previousestimates, which reported mortalityrates up to 5% of admissions.5 Forthose with a primary diagnosis ofRSV, mortality rates were similar inboth data sets at 3 to 4 deaths per10 000 admissions. The KID data set,estimates nationally, only 42 deathsannually with a primary diagnosis ofRSV. The number of deaths witha primary diagnosis of RSV iscomparable to the number of annualdeaths for children aged ,2 yearsassociated with influenza (9–56deaths/year reported during2004–2013 seasons),22 for whicheffective vaccines are available.
The relatively low RSV-associatedmortality identified in our analysismay have several explanations. Thefirst (and most likely) reason for thelow findings is the advances inmedical care that have occurred inthe decades since publication of thelast estimates. Advances in the care ofpreterm infants have resulted indecreased major morbidity in thispopulation, including less chroniclung disease, a major risk factor forsevere RSV infection.23 Second,advances in the care of infants andchildren outside of the NICUs havealso occurred, and much of the carefor those with bronchiolitis has beenmoved from the inpatient to theoutpatient setting.24 It is also possiblethat the virus itself has changed25,26
and that changes could have resultedin decreasing morbidity. The use ofpalivizumab, first licensed in theUnited States in 1998, is unlikely toaccount for the significant changesobserved in mortality. Palivizumabhas not been associated witha reduction in mortality in any
TABLE 2 Characteristics of Infants and Children With RSV-Associated Hospital Mortality
Variable No. (%) of RSV-Associated Deaths
KID 2009 PHIS 2000–2011
Annual deaths 121 (100) 56a
Deaths occurring in a children’s hospital 58 (48) 56 (100)Deaths during RSV season, November–March 84 (70) 39 (70)Deaths with a primary ICD-9-CM code for RSV 42 (34) 21 (38)Death associated with CCC, any 92 (76) 44 (79)Cardiovascular condition 45 (37) 25 (45)Neuromuscular condition 32 (26) 11 (20)Respiratory condition 26 (21) 10 (19)Congenital or genetic condition 15 (13) 11 (19)Multiple conditions, range: 2–5 47 (39) 21 (37)Other conditions associated with deathb 99 (82) 42 (74)Sepsis 50 (41) 24 (42)Cardiac arrest 41 (34) 18 (32)Surgical complication 33 (28) 18 (32)Hospital length of stay .30 days 45 (38) 21 (37)a Mean number of annual deaths.b Subjects may have had .1 condition.
PEDIATRICS Volume 135, number 1, January 2015 5 at UCSF Kalmanovitz Library & CKM on December 10, 2014pediatrics.aappublications.orgDownloaded from

randomized controlled trial.7,8
Furthermore, the number of infantsreceiving palivizumab each year issmall, and the greatest burden of RSVdisease is in previously healthy terminfants who are not eligible to receiveprophylaxis. In a recent study,,1% of the Medicaid birth cohortsin Florida and Texas receivedpalivizumab.27 In another multicenterstudy, only 9% of hospitalizedchildren had ever receivedpalivizumab.2 Finally, infants whoreceive palivizumab are generallythose with prematurity or CCC,conditions that may also predisposethem to death.28
Accurate estimates of mortality in the21st century can inform cost-effectiveness analyses for the use ofprophylaxis for the prevention of RSVin high-risk groups and can also beused in the evaluation ofexperimental preventive andtreatment strategies.29 Mortality is animportant variable in economicmodels. In models that examine thecost-effectiveness of differentprophylaxis strategies for theprevention of RSV, mortality rates(when included) drive final cost-effectiveness ratios and should not bebased on unsupported assumptions.7
The present study identified manyimportant characteristics of infantsand children with RSV-associatedmortality. Our confidence in theresults was strengthened by theconsistency seen in the KID and PHISdata sets. First, as demonstrated inprevious studies,3,4 the majority ofdeaths identified in children occurredin infants. Infants represented 85% ofdeaths in the KID data set and 77% inthe PHIS data set. Infants andchildren who died also commonly hadCCC, with cardiovascular andneuromuscular conditions the mostcommon. Nearly 40% of the deaths inboth data sets occurred in medicallyfragile infants and children with$2 CCC. Those infants and childrenwith RSV-associated deaths had longhospital stays, which further
illustrates their medical fragility.Although the mean hospital stay forinfants and young children with RSVbronchiolitis is ∼2.5 days,6 infantsand children with RSV-associatedmortality in our study had hospitalsstays that were ∼40 days in both theKID and PHIS data sets. Those whosedeaths occurred outside of thetraditional RSV season had evenlonger stays.
The duration of hospitalization beforedeath raises questions regarding therole of RSV in the deaths of thesechildren. The duration ofhospitalization may indicate that RSVinfection was present during thehospitalization but may have beenremote from the actual death. Ourfinding that the majority of childrenwho died had other potentially life-threatening conditions (includingbacterial sepsis and surgicalcomplications during their RSV-associated hospitalizations) supportsthis possibility. The administrativedata sets do not allow us to identifythe exact cause of death for eachchild; however, ∼30% of deathsoccurred outside of the typical RSVseason and ,40% of those who diedregistered in either of the data setshad a primary diagnosis code for RSV.
The present study had severallimitations. First, we used ICD-9-CMdiagnosis codes to identify RSV-associated hospitalizations. Thesecodes potentially include all causes ofbronchiolitis and may overestimateRSV infections. However, our goal wasto identify all deaths potentiallyassociated with RSV hospitalization.The mortality rates were low in bothdata sets, and the total annual deathspredicted by using the KID data setwere orders of magnitude lower thanprevious estimates. Our mortalityrates were similar to recent resultsfrom the KID data set forbronchiolitis.6 This finding is notunexpected because bronchiolitis isthe most common presentation ofRSV infection in this age group, andRSV is the most common cause of
bronchiolitis. Second, we were notable to capture all transfers thatoccurred between facilities. However,the proportions of childrentransferred were low in both datasets. In the KID data set, transfersfrom community hospitals to tertiarychildren’s hospitals accounted for themajority of transfers. By including thePHIS data set, we may have captureda portion of these transfers thatresulted in mortality. Third, we werenot able to confirm RSV infection inall cases. The ICD-9-CM code 466.19(bronchiolitis, other) increasedsignificantly over the study period.The increase may reflect the move tomolecular diagnostic testing inhospital settings and theidentification of viral pathogens otherthan RSV associated withbronchiolitis admissions.14 If deathswere due to other viruses, theimportance of RSV as a cause ofmortality in young children is evenless than we report. Fourth, we werenot able to capture palivizumab use.However, because palivizumab hasnever been shown to decreasemortality and is used infrequently,variation in palivizumabadministration is unlikely to accountfor the changes in mortality ratesobserved. Fifth, we could not identifynosocomial RSV infections. Finally, wecould not confirm the exact cause ofdeath in the cases identified. It islikely that, given the medicalcomplexity of the majority of infantsand children who died, multiplefactors other than RSV infection mayhave contributed to their deaths.Consideration of making RSV-associated mortality in childrena reportable condition, similar toinfluenza, is indicated.
CONCLUSIONS
Despite these limitations, we are ableto draw several conclusions. First,RSV-associated hospitalization andmortality have decreased in the 21stcentury. Although our data mayoverestimate the number of
6 BYINGTON et al at UCSF Kalmanovitz Library & CKM on December 10, 2014pediatrics.aappublications.orgDownloaded from

RSV-associated deaths, the number ofannual deaths in the United States islow. Infants, especially those withCCC, represent the majority of RSV-associated deaths in the UnitedStates. Infants with CCC represent
a vulnerable population who, alongwith the elderly, experience thegreatest mortality burden fromRSV.3,30 These populations should beprioritized if a safe and effective RSVvaccine is developed. Our findings
may help to inform policy makers asthey model the costs associated withRSV prevention and treatmentstrategies, including palivizumab andinvestigational therapeutics andvaccines under development.
FINANCIAL DISCLOSURE: Dr Byington has intellectual property in and receives royalties from BioFire Diagnostics, Inc; Mr Wilkes, Mr Korgenski, and Dr Sheng have
indicated they have no financial relationships relevant to this article to disclose.
FUNDING: Dr Byington and Mr Wilkes received funding from the H.A. and Edna Benning Presidential Endowment; and Dr Byington and Dr Sheng received funding
from the National Center for Advancing Translational Sciences of the National Institutes of Health under award 1ULTR001067. The content is solely the responsibility
of the authors and does not necessarily represent the official views of the National Institutes of Health. Funded by the National Institutes of Health (NIH).
POTENTIAL CONFLICT OF INTEREST: The authors have indicated they have no potential conflicts of interest to disclose.
REFERENCES
1. Glezen WP, Taber LH, Frank AL, Kasel JA.Risk of primary infection and reinfectionwith respiratory syncytial virus. Am J DisChild. 1986;140(6):543–546
2. Hall CB, Weinberg GA, Iwane MK, et al.The burden of respiratory syncytial virusinfection in young children. N Engl J Med.2009;360(6):588–598
3. Thompson WW, Shay DK, Weintraub E,et al. Mortality associated with influenzaand respiratory syncytial virus inthe United States. JAMA. 2003;289(2):179–186
4. Shay DK, Holman RC, Roosevelt GE, ClarkeMJ, Anderson LJ. Bronchiolitis-associated mortality and estimates ofrespiratory syncytial virus-associateddeaths among US children, 1979-1997.J Infect Dis. 2001;183(1):16–22
5. Institute of Medicine. The prospects forimmunizing against respiratory syncytialvirus. New Vaccine Development:Establishing Priorities. Vol. 1.Washington, DC: National AcademiesPress; 1986;397–409
6. Hasegawa K, Tsugawa Y, Brown DF,Mansbach JM, Camargo CA Jr. Trends inbronchiolitis hospitalizations in theUnited States, 2000-2009. Pediatrics.2013;132(1):28–36
7. Andabaka T, Nickerson JW, Rojas-ReyesMX, Rueda JD, Bacic Vrca V, Barsic B.Monoclonal antibody for reducing therisk of respiratory syncytial virusinfection in children. Cochrane DatabaseSyst Rev. 2013;4:CD006602
8. American Academy of PediatricsCommittee on Infectious Diseases;
American Academy of PediatricsBronchiolitis Guidelines Committee.Updated guidance for palivizumabprophylaxis among infants and youngchildren at increased risk ofhospitalization for respiratory syncytialvirus infection. Pediatrics. 2014;134(2):415–420
9. Healthcare Cost and Utilization Project.Kids’ Inpatient Database, 2000. Rockville,MD: Agency for Health Care Researchand Quality; 2003
10. Healthcare Cost and Utilization Project.Kids’ Inpatient Database 2003. Rockville,MD: Agency for Health Care Researchand Quality; 2005
11. Healthcare Cost and Utilization Project.Kids Inpatient Database 2006. Rockville,MD: Agency for Health Care Researchand Quality; 2008
12. Healthcare Cost and Utilization Project.Kids’ Inpatient Database 2011. Rockville,MD: Agency for Health Care Researchand Quality; 2011
13. Kittle K, Currier K, Dyk L, Newman K.Using a pediatric database to drivequality improvement. Semin PediatrSurg. 2002;11(1):60–63
14. Stempel HE, Martin ET, Kuypers J,Englund JA, Zerr DM. Multiple viralrespiratory pathogens in children withbronchiolitis. Acta Paediatr. 2009;98(1):123–126
15. Zhou H, Thompson WW, Viboud CG, et al.Hospitalizations associated withinfluenza and respiratory syncytial virusin the United States, 1993-2008. ClinInfect Dis. 2012;54(10):1427–1436
16. Healthcare Cost and Utilization Project.Overview of the Kids’ Inpatient Database(KID). Available at: www.hcup-us.ahrq.gov/kidoverview.jsp. AccessedSeptember 26, 2014
17. Langley GF, Anderson LJ. Epidemiologyand prevention of respiratory syncytialvirus infections among infants andyoung children. Pediatr Infect Dis J. 2011;30(6):510–517
18. Children’s Hospital Association. PHIS+:augmenting the Pediatric HealthInformation System with clinical data.Available at: www.childrenshospitals.org/phisplus/index.html. AccessedSeptember 26, 2014
19. Feudtner C, Hays RM, Haynes G, Geyer JR,Neff JM, Koepsell TD. Deaths attributed topediatric complex chronic conditions:national trends and implications forsupportive care services. Pediatrics.2001;107(6). Available at: www.pediatrics.org/cgi/content/full/107/6/e99
20. Li J, Monuteaux MC, Bachur RG.Interfacility transfers of noncritically illchildren to academic pediatricemergency departments. Pediatrics.2012;130(1):83–92
21. Berry JG, Hall M, Hall DE, et al. Inpatientgrowth and resource use in 28 children’shospitals: a longitudinal, multi-institutional study. JAMA Pediatr. 2013;167(2):170–177
22. Centers for Disease Control andPrevention. FluView. Influenza-associatedpediatric mortality. Available at: http://gis.cdc.gov/GRASP/Fluview/PedFluDeath.html. Accessed September 26, 2014
PEDIATRICS Volume 135, number 1, January 2015 7 at UCSF Kalmanovitz Library & CKM on December 10, 2014pediatrics.aappublications.orgDownloaded from

23. Horbar JD, Carpenter JH, Badger GJ, et al.Mortality and neonatal morbidity amonginfants 501 to 1500 grams from 2000 to2009. Pediatrics. 2012;129(6):1019–1026
24. Sandweiss DR, Mundorff MB, Hill T, et al.Decreasing hospital length of stay forbronchiolitis by using an observationunit and home oxygen therapy. JAMAPediatr. 2013;167(5):422–428
25. Melero JA, Moore ML. Influence ofrespiratory syncytial virus straindifferences on pathogenesis andimmunity. Curr Top Microbiol Immunol.2013;372:59–82
26. Pretorius MA, van Niekerk S, Tempia S,et al; SARI Surveillance Group. Replacementand positive evolution of subtype A and Brespiratory syncytial virus G-proteingenotypes from 1997-2012 in South Africa.J Infect Dis. 2013;208(suppl 3):S227–S237
27. Winterstein AG, Knox CA, Kubilis P, HamppC. Appropriateness of age thresholds forrespiratory syncytial virusimmunoprophylaxis in moderate-preterm infants: a cohort study. JAMAPediatr. 2013;167(12):1118–1124
28. Mohan AK, Braun MM, Ellenberg S, HedjeJ, Coté TR. Deaths among children less
than two years of age receivingpalivizumab: an analysis ofcomorbidities. Pediatr Infect Dis J. 2004;23(4):342–345
29. Turner TL, Kopp BT, Paul G, LandgraveLC, Hayes D Jr, Thompson R.Respiratory syncytial virus: currentand emerging treatment options.Clinicoecon Outcomes Res. 2014;6:217–225
30. Hall CB, SimTes EA, Anderson LJ. Clinicaland epidemiologic features ofrespiratory syncytial virus. Curr TopMicrobiol Immunol. 2013;372:39–57
8 BYINGTON et al at UCSF Kalmanovitz Library & CKM on December 10, 2014pediatrics.aappublications.orgDownloaded from

DOI: 10.1542/peds.2014-2151; originally published online December 8, 2014;Pediatrics
Carrie L. Byington, Jacob Wilkes, Kent Korgenski and Xiaoming ShengYoung Children
Associated Mortality in Hospitalized Infants and−Respiratory Syncytial Virus
ServicesUpdated Information &
/peds.2014-2151http://pediatrics.aappublications.org/content/early/2014/12/02including high resolution figures, can be found at:
Permissions & Licensing
tmlhttp://pediatrics.aappublications.org/site/misc/Permissions.xhtables) or in its entirety can be found online at: Information about reproducing this article in parts (figures,
Reprints http://pediatrics.aappublications.org/site/misc/reprints.xhtml
Information about ordering reprints can be found online:
rights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275.Grove Village, Illinois, 60007. Copyright © 2014 by the American Academy of Pediatrics. All and trademarked by the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elkpublication, it has been published continuously since 1948. PEDIATRICS is owned, published, PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly
at UCSF Kalmanovitz Library & CKM on December 10, 2014pediatrics.aappublications.orgDownloaded from
DOI: 10.1542/peds.2014-2151; originally published online December 8, 2014;Pediatrics
Carrie L. Byington, Jacob Wilkes, Kent Korgenski and Xiaoming ShengYoung Children
Associated Mortality in Hospitalized Infants and−Respiratory Syncytial Virus
http://pediatrics.aappublications.org/content/early/2014/12/02/peds.2014-2151
located on the World Wide Web at: The online version of this article, along with updated information and services, is
of Pediatrics. All rights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275.Boulevard, Elk Grove Village, Illinois, 60007. Copyright © 2014 by the American Academy published, and trademarked by the American Academy of Pediatrics, 141 Northwest Pointpublication, it has been published continuously since 1948. PEDIATRICS is owned, PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly
at UCSF Kalmanovitz Library & CKM on December 10, 2014pediatrics.aappublications.orgDownloaded from





























![IMAGEN Respiratory Syncytial Virus (RSV) [PT]...IMAGEN Respiratory Syncytial Virus (RSV) 1. UTILIZAÇÃO PREVISTA O IMAGEN Respiratory Syncytial Virus (RSV) é um teste qualitativo](https://img.pdfslide.net/doc/110x75/609c20ca1e0ebf036346e66d/imagen-respiratory-syncytial-virus-rsv-pt-imagen-respiratory-syncytial-virus.jpg)