Embed Size (px)
Citation preview
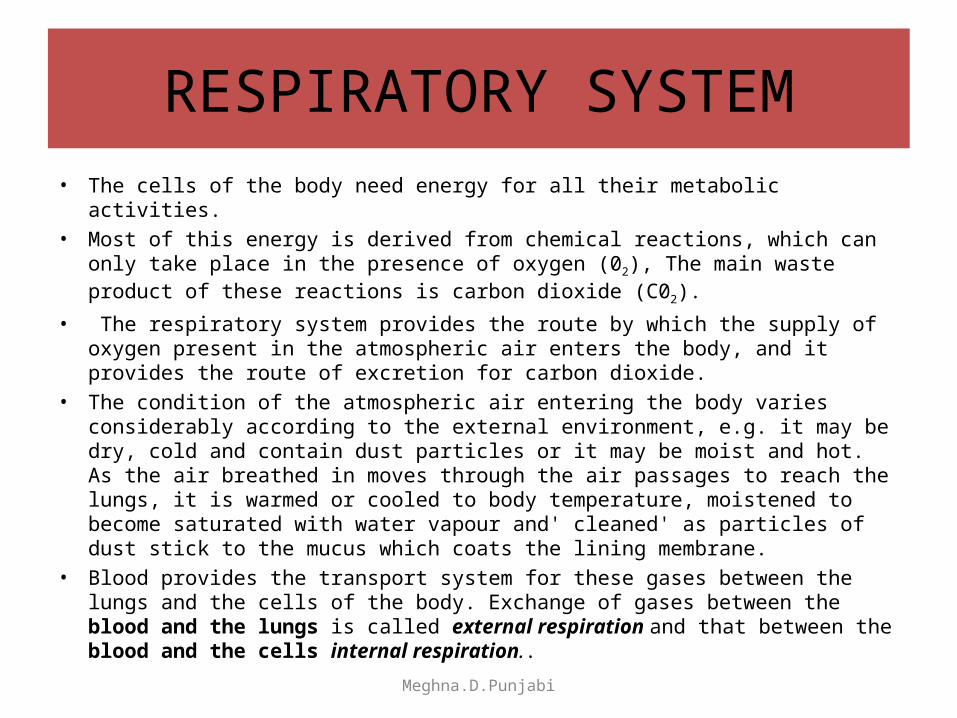
RESPIRATORY SYSTEM• The cells of the body need energy for all their metabolic activities. • Most of this energy is derived from chemical reactions, which can only take place
in the presence of oxygen (02), The main waste product of these reactions is carbon dioxide (C02).
• The respiratory system provides the route by which the supply of oxygen present in the atmospheric air enters the body, and it provides the route of excretion for carbon dioxide.
• The condition of the atmospheric air entering the body varies considerably according to the external environment, e.g. it may be dry, cold and contain dust particles or it may be moist and hot. As the air breathed in moves through the air passages to reach the lungs, it is warmed or cooled to body temperature, moistened to become saturated with water vapour and' cleaned' as particles of dust stick to the mucus which coats the lining membrane.
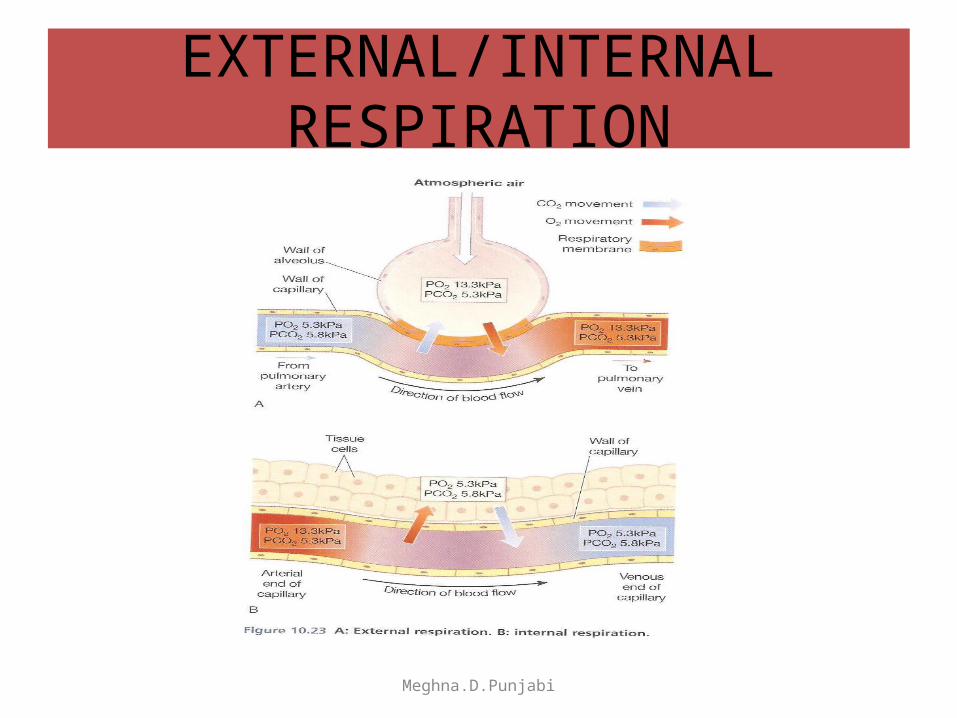
• Blood provides the transport system for these gases between the lungs and the cells of the body. Exchange of gases between the blood and the lungs is called external respiration and that between the blood and the cells internal respiration.. Meghna.D.Punjabi
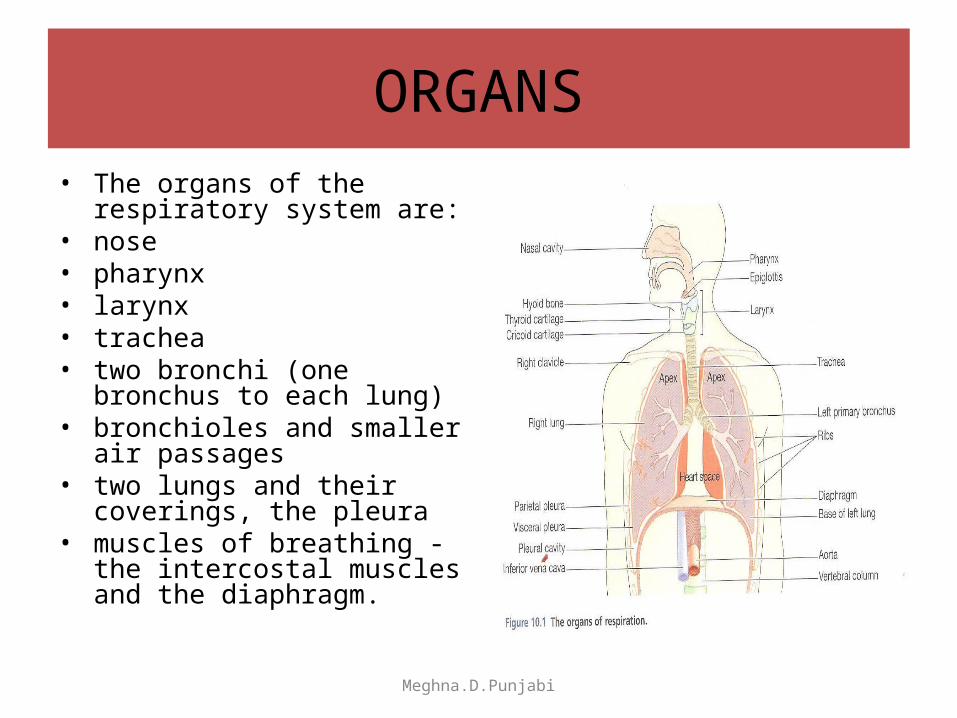
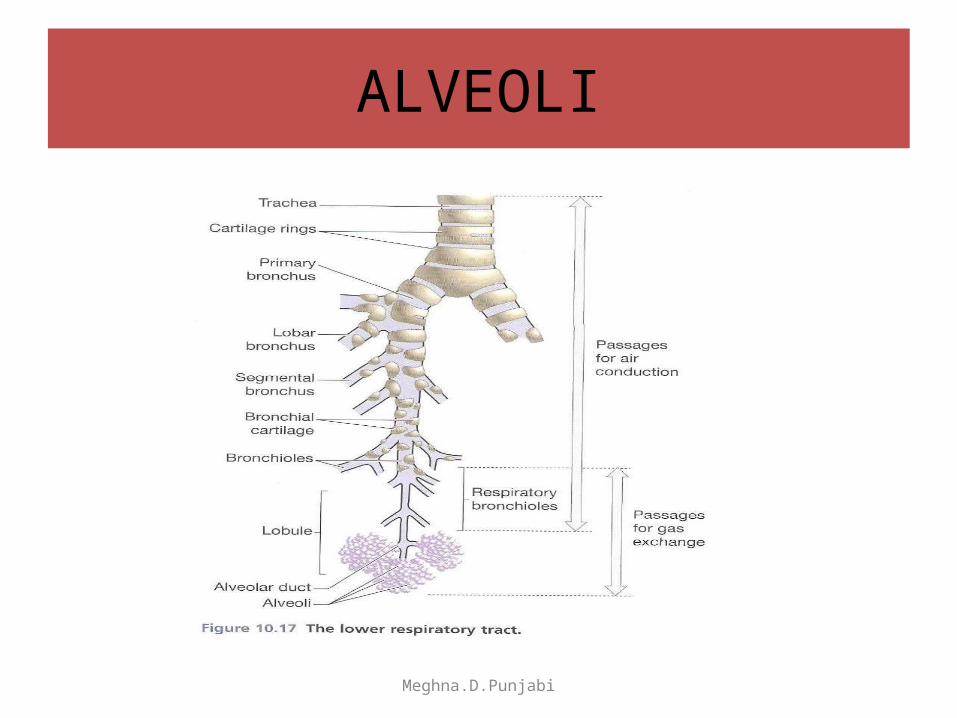
ORGANS• The organs of the respiratory
system are: • nose • pharynx • larynx • trachea • two bronchi (one bronchus to
each lung) • bronchioles and smaller air
passages • two lungs and their coverings, the
pleura • muscles of breathing - the
intercostal muscles and the diaphragm.
Meghna.D.Punjabi
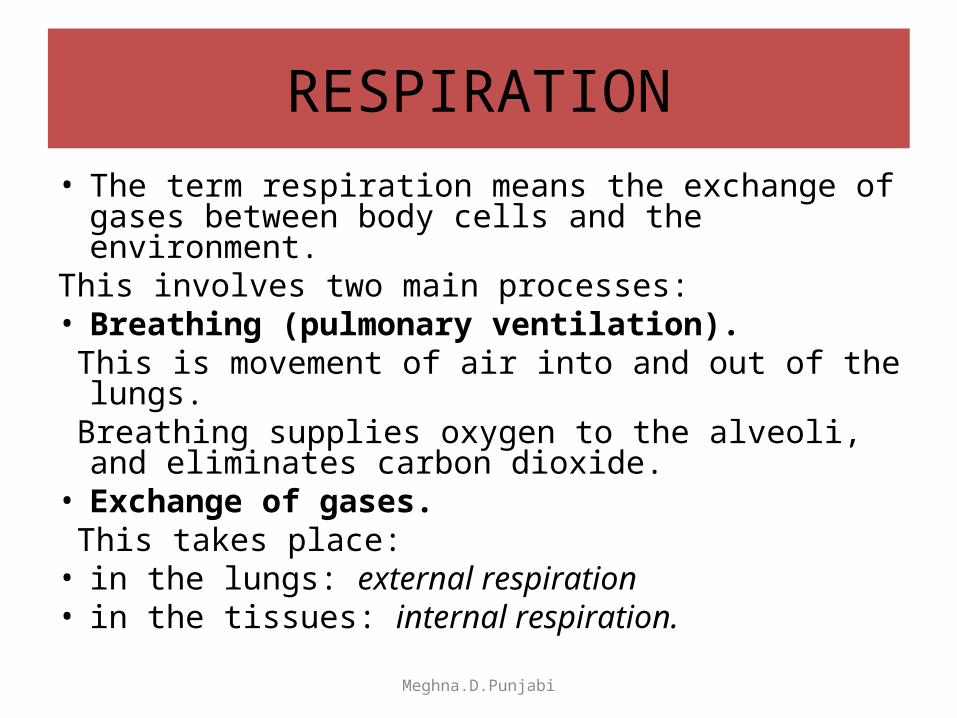
RESPIRATION• The term respiration means the exchange of gases
between body cells and the environment. This involves two main processes: • Breathing (pulmonary ventilation). This is movement of air into and out of the lungs. Breathing supplies oxygen to the alveoli, and eliminates
carbon dioxide. • Exchange of gases. This takes place: • in the lungs: external respiration • in the tissues: internal respiration.
Meghna.D.Punjabi
MUSCLES OF BREATHING
• Expansion of the chest during inspiration occurs as a result of muscular activity, partly voluntary and partly involuntary.
• The main muscles used in normal quiet breathing are the intercostal muscles and the diaphragm
• During difficult or deep breathing they are assisted by muscles of the neck, shoulders and abdomen.
Meghna.D.Punjabi
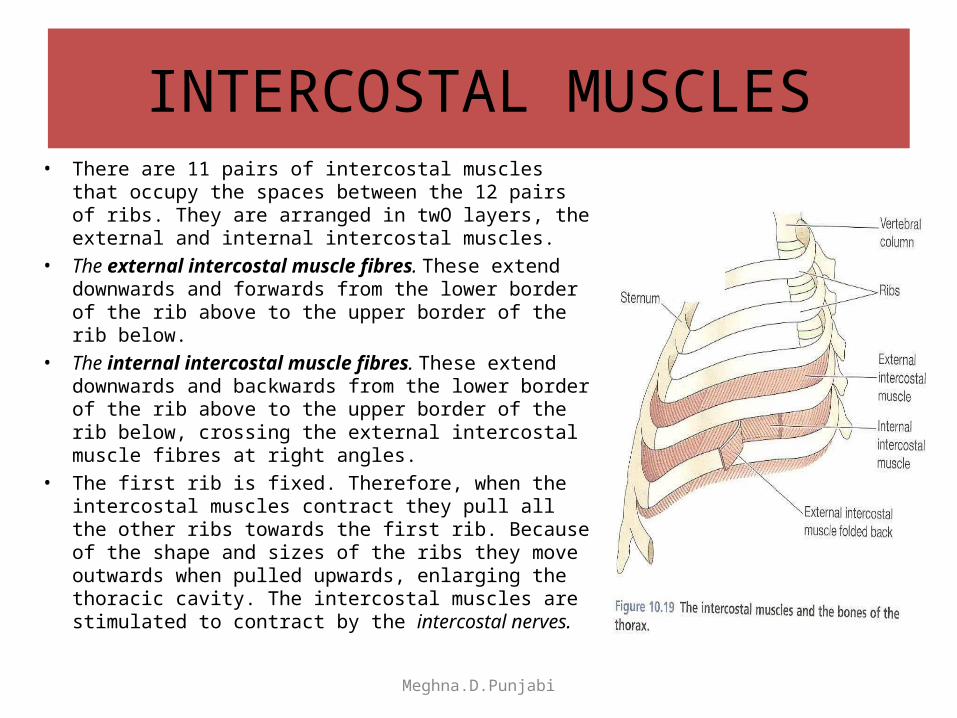
INTERCOSTAL MUSCLES• There are 11 pairs of intercostal muscles that occupy the
spaces between the 12 pairs of ribs. They are arranged in twO layers, the external and internal intercostal muscles.
• The external intercostal muscle fibres. These extend downwards and forwards from the lower border of the rib above to the upper border of the rib below.
• The internal intercostal muscle fibres. These extend downwards and backwards from the lower border of the rib above to the upper border of the rib below, crossing the external intercostal muscle fibres at right angles.
• The first rib is fixed. Therefore, when the intercostal muscles contract they pull all the other ribs towards the first rib. Because of the shape and sizes of the ribs they move outwards when pulled upwards, enlarging the thoracic cavity. The intercostal muscles are stimulated to contract by the intercostal nerves.
Meghna.D.Punjabi
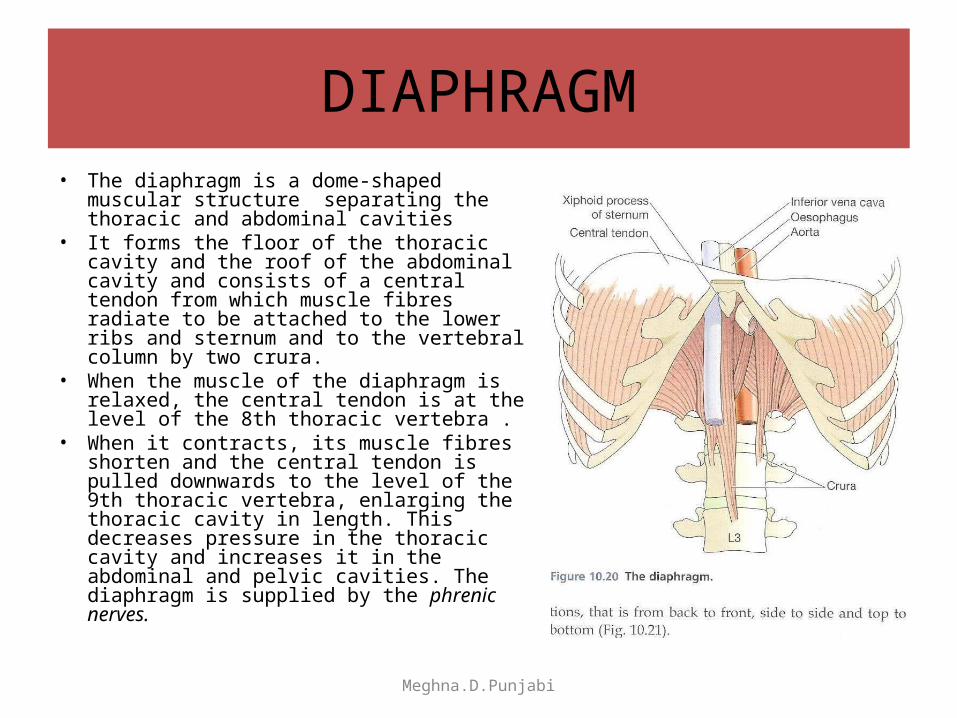
DIAPHRAGM• The diaphragm is a dome-shaped muscular
structure separating the thoracic and abdominal cavities
• It forms the floor of the thoracic cavity and the roof of the abdominal cavity and consists of a central tendon from which muscle fibres radiate to be attached to the lower ribs and sternum and to the vertebral column by two crura.
• When the muscle of the diaphragm is relaxed, the central tendon is at the level of the 8th thoracic vertebra .
• When it contracts, its muscle fibres shorten and the central tendon is pulled downwards to the level of the 9th thoracic vertebra, enlarging the thoracic cavity in length. This decreases pressure in the thoracic cavity and increases it in the abdominal and pelvic cavities. The diaphragm is supplied by the phrenic nerves.
Meghna.D.Punjabi
THORASIC CAVITY ENLARGED
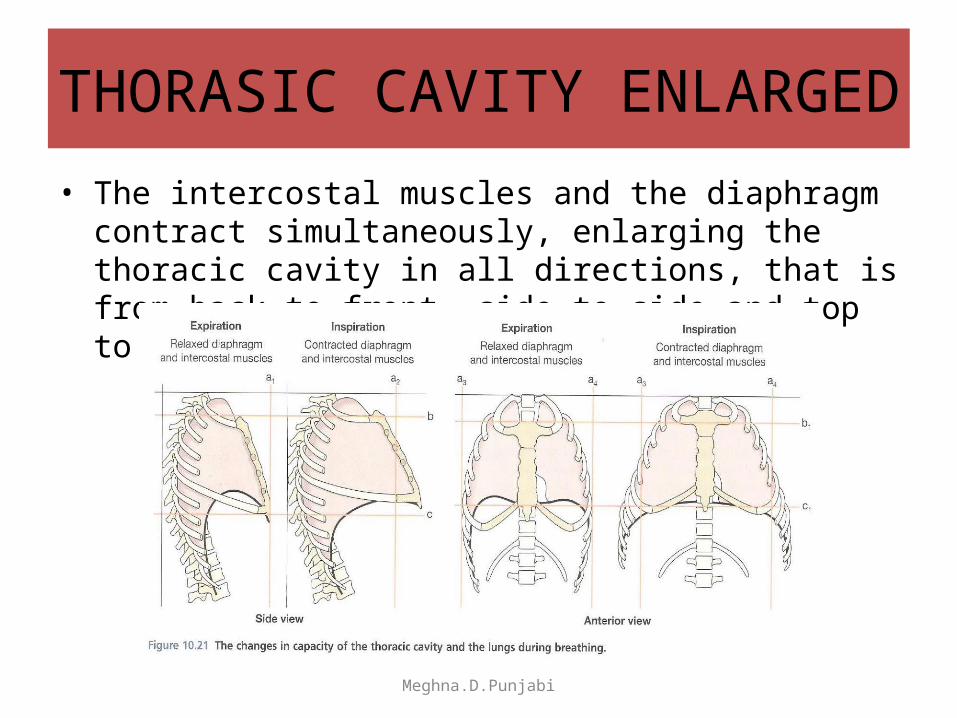
• The intercostal muscles and the diaphragm contract simultaneously, enlarging the thoracic cavity in all directions, that is from back to front, side to side and top to bottom
Meghna.D.Punjabi
PLEURA AND PLEURAL CAVITY
Meghna.D.Punjabi
ALVEOLI
Meghna.D.Punjabi
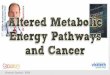
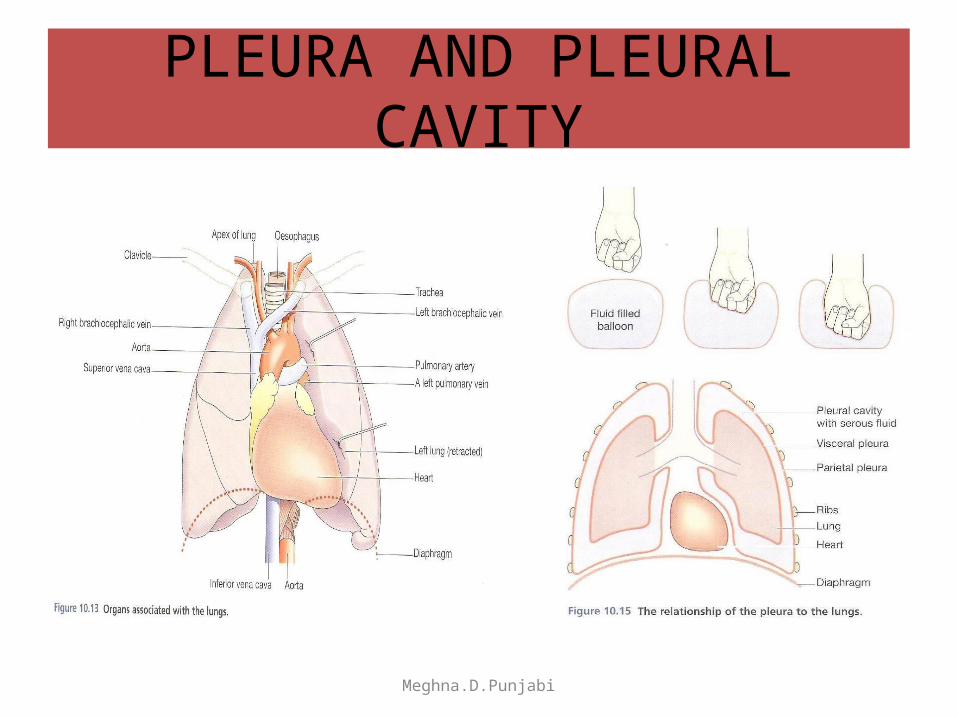
PLEURA AND PLEURAL CAVITY• The pleura consists of a closed sac of serous membrane (one for each lung) which
contains a small amount of serous fluid. The lung is invaginated (pushed into) into this sac so that it forms two layers: one adheres to the lung and the other to the wall of the thoracic cavity
• The visceral pleura. This is adherent to the lung, covering each lobe and passing into the fissures that separate them.
• The parietal pleura.. This is adherent to the inside of the chest wall and the thoracic surface of the diaphragm. It remains detached from the adjacent structures in the mediastinum and is continuous with the visceral pleura round the edges of the hilum
• The pleural cavity. This is only a potential space. In health, the two layers of pleura are separated by a thin film of serous fluid which allows them to glide over each other, preventing friction between them during breathing. The serous fluid is secreted by the epithelial cells of the membrane.
• The two layers of pleura, with serous fluid between them, behave in the same way as two pieces of glass separated by a thin film of water. They glide over each other easily but can be pulled apart only with difficulty, because of the surface tension between the membranes and the fluid. If either layer of pleura is punctured, the underlying lung collapses owing to its inherent property of elastic recoil.
Meghna.D.Punjabi
CYCLE OF BREATHING
• The average respiratory rate is 12 to 15 breaths per minute.
Each breath consists of three phases: • inspiration • expiration • pause.
Meghna.D.Punjabi
INSPIRATION• When the capacity of the thoracic cavity is increased by
simultaneous contraction of the intercostal muscles and the diaphragm, the parietal pleura moves with the walls of the thorax and the diaphragm.
• This reduces the pressure in the pleural cavity to a level considerably lower than atmospheric pressure. The visceral pleura follows the parietal pleura, pulling the lung with it. This expands the lungs and the pressure within the alveoli and in the air passages falls, drawing air into the lungs in an attempt to equalise the atmospheric and alveolar air pressures.
• The process of inspiration is active, as it needs energy for muscle contraction. The negative pressure created in the thoracic cavity aids venous return to the heart and is known as the respiratory pump.
• At rest, inspiration lasts about 2 seconds.
Meghna.D.Punjabi
EXPIRATION• Relaxation of the intercostal muscles and the
diaphragm results in downward and inward movement of the rib cage and elastic recoil of the lungs.
• As this occurs, pressure inside the lungs exceeds that in the atmosphere and so air is expelled from the respiratory tract.
• The lungs still contain some air, and are prevented from complete collapse by the intact pleura. This process is passive as it does not require the expenditure of energy.
• At rest, expiration lasts about 3 seconds, and after expiration there is a pause before the next cycle begins
Meghna.D.Punjabi
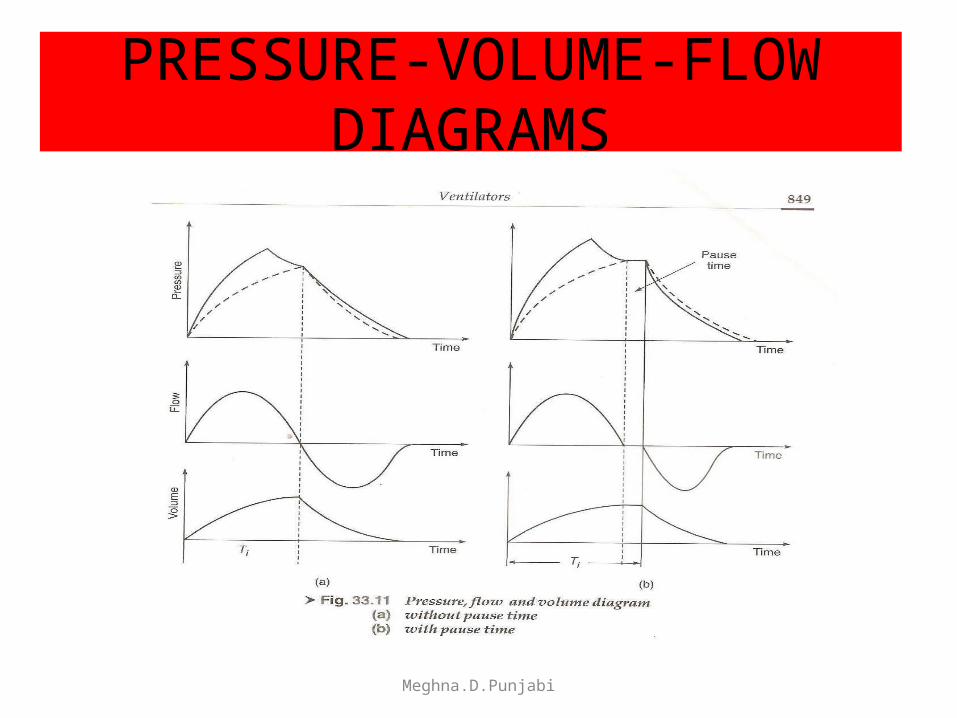
PRESSURE-VOLUME-FLOW DIAGRAMS
Meghna.D.Punjabi
PHYSIOLOGICAL VARIABLES AFFECTING BREATHING
• Elasticity. Elasticity is the term used to describe the ability of the lung to return to its normal shape after each breath. Loss of elasticity of the connective tissue in the lungs necessitates forced expiration and increased effort on inspiration.
• Compliance. This is a measure of the distensibility of the lungs, i.e. the effort required to inflate the alveoli. The healthy lung is very compliant, and inflates with very little effort. When compliance is low the effort needed to inflate the lungs is greater than normal, e.g. in some diseases where elasticity is reduced or when insufficient surfactant is present. It should be noted that compliance and elasticity are opposing forces.
• Airway resistance. When this is increased, e.g. in bronchoconstriction, more respiratory effort is required to inflate the lungs. Meghna.D.Punjabi
LUNG VOLUME AND CAPACITIES
• In normal quiet breathing there are about 15 complete respiratory cycles per minute.
• The lungs and the air passages are never empty and, as the exchange of gases takes place only across the walls of the alveolar ducts and alveoli, the remaining capacity of the respiratory passages is called the anatomical dead space (about 150 ml).
Meghna.D.Punjabi
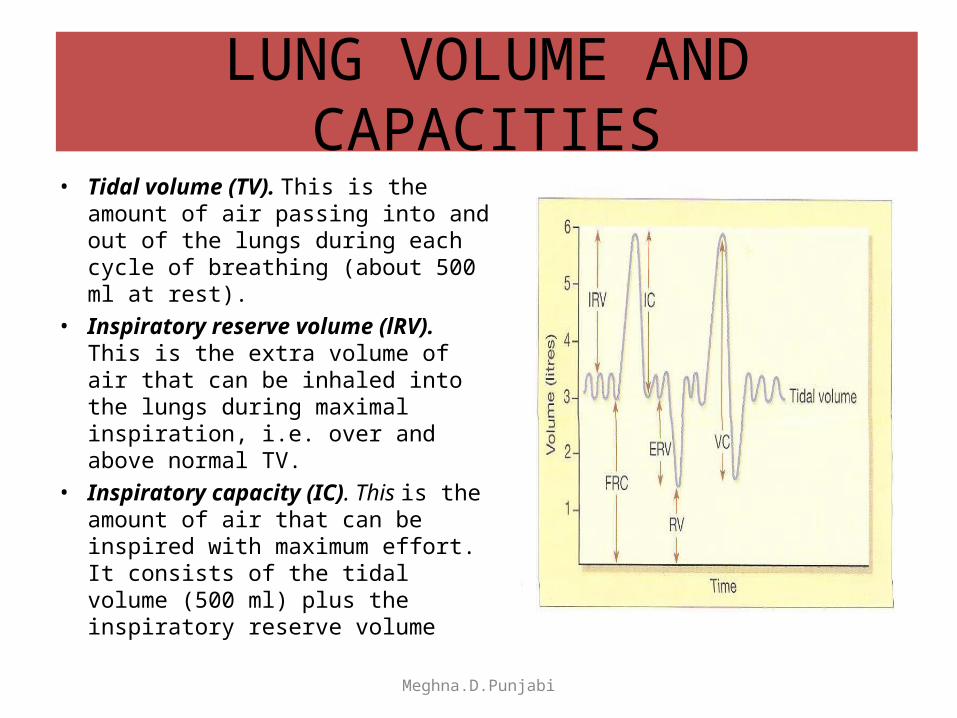
LUNG VOLUME AND CAPACITIES• Tidal volume (TV). This is the
amount of air passing into and out of the lungs during each cycle of breathing (about 500 ml at rest).
• Inspiratory reserve volume (lRV). This is the extra volume of air that can be inhaled into the lungs during maximal inspiration, i.e. over and above normal TV.
• Inspiratory capacity (IC). This is the amount of air that can be inspired with maximum effort. It consists of the tidal volume (500 ml) plus the inspiratory reserve volume
Meghna.D.Punjabi
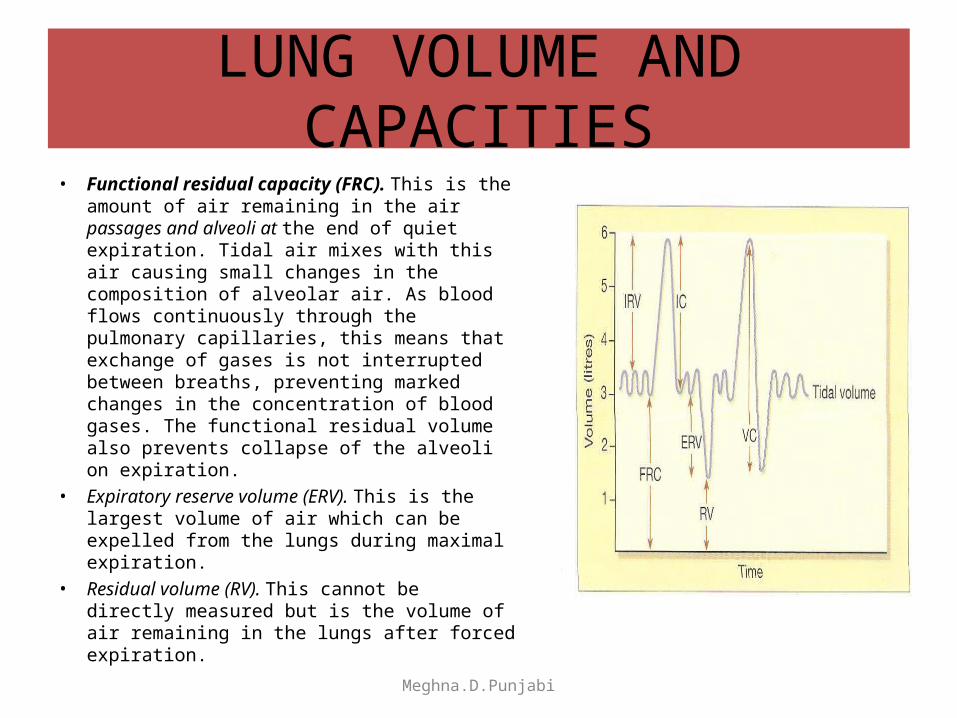
LUNG VOLUME AND CAPACITIES• Functional residual capacity (FRC). This is the
amount of air remaining in the air passages and alveoli at the end of quiet expiration. Tidal air mixes with this air causing small changes in the composition of alveolar air. As blood flows continuously through the pulmonary capillaries, this means that exchange of gases is not interrupted between breaths, preventing marked changes in the concentration of blood gases. The functional residual volume also prevents collapse of the alveoli on expiration.
• Expiratory reserve volume (ERV). This is the largest volume of air which can be expelled from the lungs during maximal expiration.
• Residual volume (RV). This cannot be directly meas ured but is the volume of air remaining in the lungs after forced expiration.
Meghna.D.Punjabi
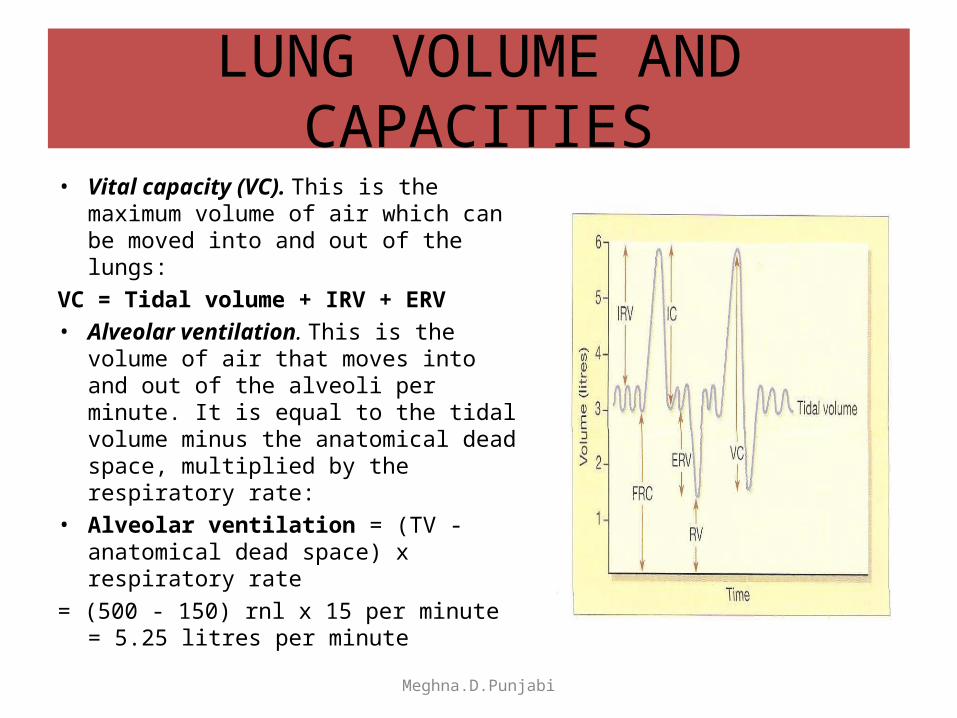
LUNG VOLUME AND CAPACITIES• Vital capacity (VC). This is the
maximum volume of air which can be moved into and out of the lungs:
VC = Tidal volume + IRV + ERV • Alveolar ventilation. This is the
volume of air that moves into and out of the alveoli per minute. It is equal to the tidal volume minus the anatomical dead space, multiplied by the respiratory rate:
• Alveolar ventilation = (TV - anatomical dead space) x respiratory rate
= (500 - 150) rnl x 15 per minute = 5.25 litres per minute
Meghna.D.Punjabi
EXCHANGE OF GASES
• Although breathing involves the alternating processes of inspiration and expiration
• Gas exchange at the respiratory membrane and in the tissues is a continuous and ongoing process.
• Diffusion of oxygen and carbon dioxide depends on pressure differences, e.g. between atmospheric air and the blood, or blood and the tissues.
Meghna.D.Punjabi
COMPOSITION OF AIR
• Air Pressure reduces as we go above sea level and increases in the sea.
• Air is a mixture of gases: nitrogen, oxygen, carbon dioxide, water vapour and small quantities of inert gases.
• Each gas in the mixture exerts a part of the total pressure proportional to its concentration, i.e. the partial pressure.This is denoted as, e.g. PO2, PCO2.
Meghna.D.Punjabi
ALVEOLAR AIR
• The composition of alveolar air remains fairly constant and is different from atmospheric air.
• It is saturated with water vapour and contains more carbon dioxide, and less oxygen. Saturation with water vapour provides 6.3 kPa (47 mmHg) thus reducing the partial pressure of all the other gases present.
• Gaseous exchange between the alveoli and the bloodstream (external respiration) is a continuous process, as the alveoli are never empty, so it is independent of the respiratory cycle. During each inspiration only some of the alveolar gases are exchanged.
Meghna.D.Punjabi
EXPIRED AIR
• This is a mixture of alveolar air and atmospheric air in the dead space .
• Exchange of gases occurs when a difference in partial pressure exists across a semipermeable membrane.
• Gases move by diffusion from the higher concentration to the lower until equilibrium is established .
• Atmospheric nitrogen is not used by the body so its partial pressure remains unchanged and is the same in inspired and expired air,alveolar air and in the blood
Meghna.D.Punjabi
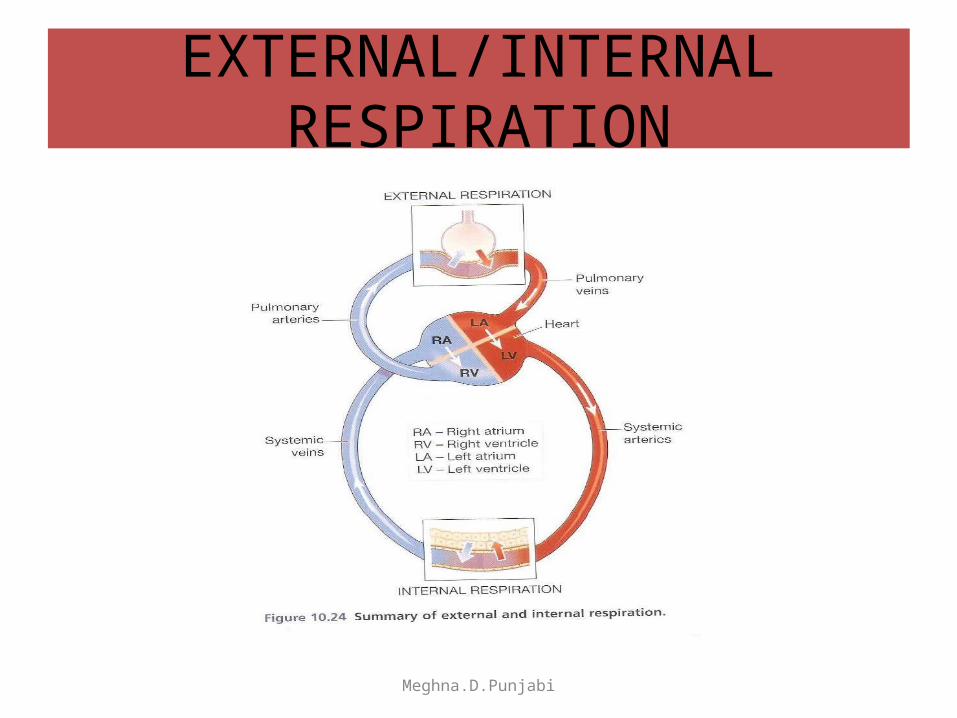
EXTERNAL/INTERNAL RESPIRATION
Meghna.D.Punjabi
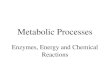
EXTERNAL RESPIRATION• This is exchange of gases by diffusion between the alveoli of the
lungs and the pulmonary blood capillaries .• It results in the conversion of deoxygenated blood coming from
heart to oxygenated blood returning to the heart.• During inspiration, atmospheric air containing oxygen enters the
alveoli. Deoxygenated blood is pumped from the right ventricle through the pulmonary artery into the pulmonary capillaries surrounding the alveoli.
• The pO2 of alveolar air is 105mm Hg .At rest po2 of deoxygenated blood entering your blood capillaries is only 40mm Hg.
• As a result of this difference in pO2 ,there is net diffusion of oxygen from alveoli into deoxygenated blood until equilibrium is reached, and the pO2 of now oxygenated blood is 105mm Hg.
Meghna.D.Punjabi
EXTERNAL RESPIRATION
• While O2 diffuses from the alveoli into deoxygenated blood , there is a net diffusion in CO2 in the opposite direction.
• The pCO2 of deoxygenated blood is 45 mm Hg whereas of alveolar air is 40 mm Hg due to this difference in pCO2 , carbon dioxide diffuses from the blood into the alveoli until the pCO2 of blood decreases to 40 mm Hg. This is the pCO2 of fully saturated blood.
• Thus the pO2 & pCO2 of oxygenated blood leaving the lungs are same as in the alveolar air.
• The carbon dioxide that diffuses into the alveoli is eliminated from the lungs during expiration.
Meghna.D.Punjabi
INTERNAL RESPIRATION• The left ventricle pumps oxygenated blood into aorta and through
systemic arteries to capillaries to tissue cells.• This is exchange of gases by diffusion between tissue blood capillaries
and tissue cells called internal respiration• It results in conversion of oxygenated blood to deoxygenated blood.• Oxygenated blood entering the tissue capillaries has a pO2 105mm Hg,
whereas tissue cells have an average pO2 40 mm Hg. Due to this difference in pO2 , oxygen diffuses from the oxygenated blood through interstitial fluid and into tissue cells until the pO2 of blood decreases to 40mm Hg. This is the average pO2 of deoxygenated blood entering tissue venules at rest.
• At rest, only about 25 % of the available oxygen in oxygenated blood actually enters tissue cells.This amount is sufficient to support the needs of resting cells.
Meghna.D.Punjabi
INTERNAL RESPIRATION• Thus deoxygenated blood still retains considerable oxygen.• During exercise, more oxygen diffuses from the blood into active cells.• While oxygen diffuses from the tissue blood capillaries into tissue
cells, carbon dioxide diffuses in the opposite direction.• The average pCO2 of tissue cells is 45mm Hg, whereas that of tissue
capillary oxygenated blood is 40mm Hg.• As a result, carbon dioxide diffuses from tissue cells through interstitial
fluid into oxygenated blood until pCO2 in the blood increases to 45mm Hg, the pCO2 of tissue capillary deoxygenated blood.
• The deoxygenated blood now returns to the heart.• From here it is pumped to the lungs for another cycle of external
respiration.
Meghna.D.Punjabi
EXTERNAL/INTERNAL RESPIRATION
Meghna.D.Punjabi
TRANSPORT OF GASES IN THE BLOOD STREAM
• Transport of blood oxygen and carbon dioxide is essential for internal respiration to occur. When oxygen and carbon dioxide enter blood, certain physical and chemical changes occur that aid in gas transport and exchange.
OxygenOxygen is carried in the blood in: • chemical combination with haemoglobin as oxyhaemoglobin (98.5 %) • solution in plasma water (1.5%) because • Oxyhaemoglobin is an unstable compound that under certain conditions
readily dissociates releasing oxygen. Factors that increase dissociation include low O2 levels, low pH and raised temperature. In active tissues there is increased production of carbon dioxide and heat, which leads to increased release of oxygen. In this way oxygen is available to tissues in greatest need. When oxygen leaves the erythrocyte, the deoxygenated haemoglobin turns purplish in colour
Meghna.D.Punjabi
TRANSPORT OF GASES IN THE BLOOD STREAM
Carbon dioxide Under normal resting conditions, each 100 ml of deoxygenated
blood contains about 5 ml of carbon dioxide.Carbon dioxide is one of the waste products of metabolism. It is
excreted by the lungs and is transported by three mechanisms:
• as bicarbonate ions (HC03-) in the plasma (70%)
• some is carried in erythrocytes, loosely combined with haemoglobin as carbaminohaemoglobin (23%).
• some is dissolved in the plasma (7%).
Meghna.D.Punjabi
SPIROMETER
• Ventilation deals with the measurement of the body as an air pump, determining its ability to move volumes of air and the speed with which it moves the air.
• The most widely performed measurement is ventilation.• This is performed using devices called spirometers that
measure volume displacement and the amount of gas moved in a specific time.
• Usually this requires the patient to take a deep breath and then exhale as rapidly and completely as possible.
• This is called forced vital capacity , this gives an indication of how much air can be moved by the lungs and how freely this air moves.
Meghna.D.Punjabi
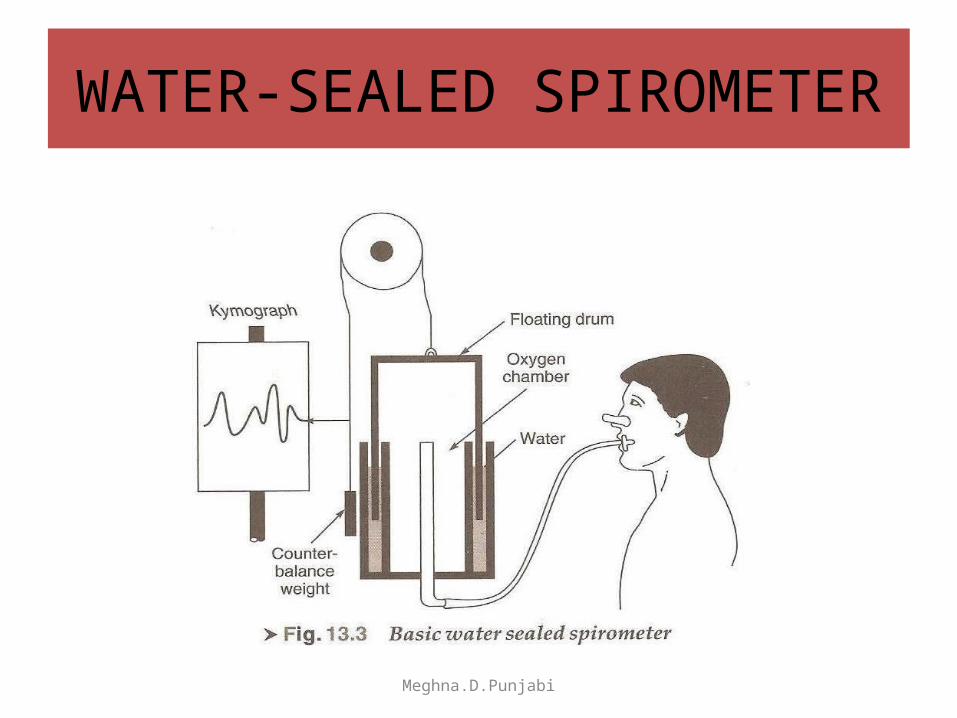
WATER-SEALED SPIROMETER
Meghna.D.Punjabi
SPIROMETER
• The instrument used to measure lung capacity and volume is called a spirometer. The record obtained from this device is called spirogram.
• Most of the respiratory measurement can be adequately carried out by the classic water-sealed spirometer.
• This consists of an upright, water filled cylinder containing an inverted counter weighted bell.
• Breathing into the bell changes the volume of gases trapped inside, and the change in volume is translated into vertical motion, which is recorded on the moving drum of a kymograph.
• The excursion( movement) of the bell will be proportional to tidal volume.
Meghna.D.Punjabi
PEAK FLOW METER
• A peak flow meter is a device that measures how well a person's lungs are working.
• A peak flow meter is a portable, inexpensive, hand-held device used to measure how air flows from your lungs in one "fast blast." In other words, the meter measures your ability to push air out of your lungs(i.e breathe out air).
• It measures the airflow through the bronchi and thus the degree of obstruction in the airways.
• If someone with asthma can't blow out as much air as usual, this may mean he or she is going to have an asthma flare-up.
• Many health care providers believe a peak flow meter may be of most help for people with moderate and severe asthma as they can adjust their daily medication.
Meghna.D.Punjabi
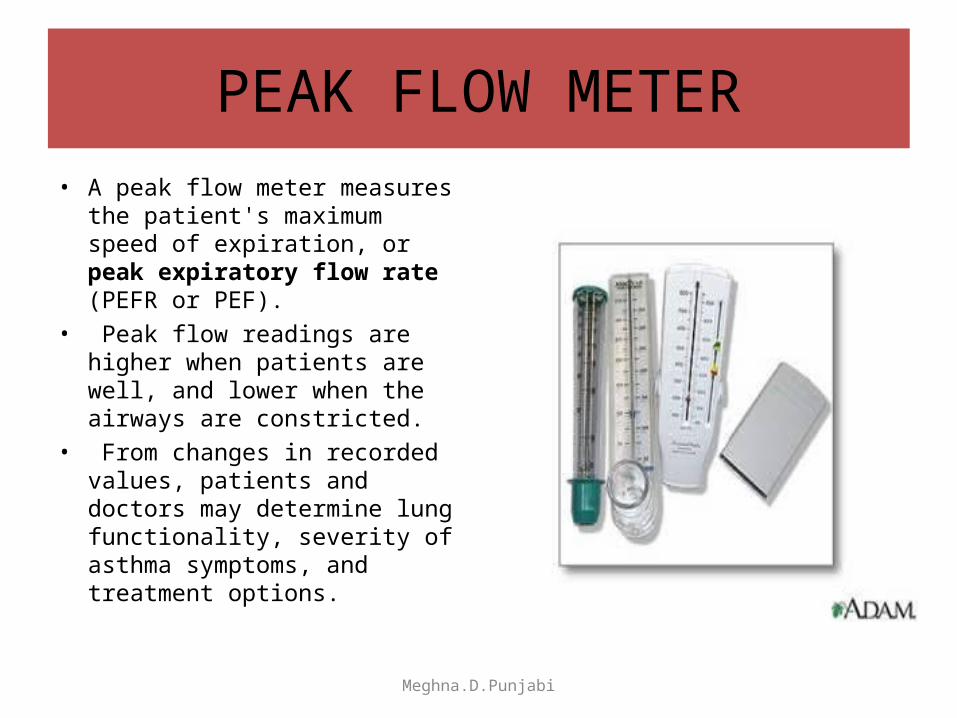
PEAK FLOW METER• A peak flow meter measures
the patient's maximum speed of expiration, or peak expiratory flow rate (PEFR or PEF).
• Peak flow readings are higher when patients are well, and lower when the airways are constricted.
• From changes in recorded values, patients and doctors may determine lung functionality, severity of asthma symptoms, and treatment options.
Meghna.D.Punjabi
HOW TO USE A PEAK FLOW METER?
Step 1: Before each use, make sure the sliding marker or arrow on the Peak Flow Meter is at the bottom of the numbered scale (zero or the lowest number on the scale).Step 2: Stand up straight. Remove gum or any food from your mouth. Take a deep breath (as deep as you can). Put the mouthpiece of the peak flow meter into your mouth. Close your lips tightly around the mouthpiece. Be sure to keep your tongue away from the mouthpiece. In one breath blow out as hard and as quickly as possible. Blow a "fast hard blast" rather than "slowly blowing" until you have emptied out nearly all of the air from your lungs. Step 3: The force of the air coming out of your lungs causes the marker to move along the numbered scale. Note the number on a piece of paper. Step 4: Repeat the entire routine three times. (You know you have done the routine correctly when the numbers from all three tries are very close together.)
Meghna.D.Punjabi
HOW TO USE A PEAK FLOW METER?
Step 5: Record the highest of the three ratings. Do not calculate an average. This is very important. You can't breathe out too much when using your peak flow meter but you can breathe out too little. Record your highest reading. Step 6: Measure your peak flow rate close to the same time each day. You and your health care provider can determine the best times. One suggestion is to measure your peak flow rate twice daily between 7and 9 a.m. and between 6 and 8 p.m. You may want to measure your peak flow rate before or after using your medicine. Some people measure peak flow both before and after taking medication. Try to do it the same way each time. Step 7: Keep a chart of your peak flow rates. Discuss the readings with your health care provider.
Meghna.D.Punjabi
SCALE OF A PEAK FLOW METER
• The best of three readings is used as the recorded value of the Peak Expiratory Flow Rate.
• It may be plotted out on graph paper charts together with a record of symptoms or using peak flow charting software. This allows patients to self-monitor and pass information back to their doctor or nurse.
• Peak flow readings are often classified into 3 zones of measurement according to the American Lung Association; green, yellow, and red. Doctors and health practitioners can develop an asthma management plan based on the green-yellow-red zones.
Meghna.D.Punjabi
Meghna.D.Punjabi
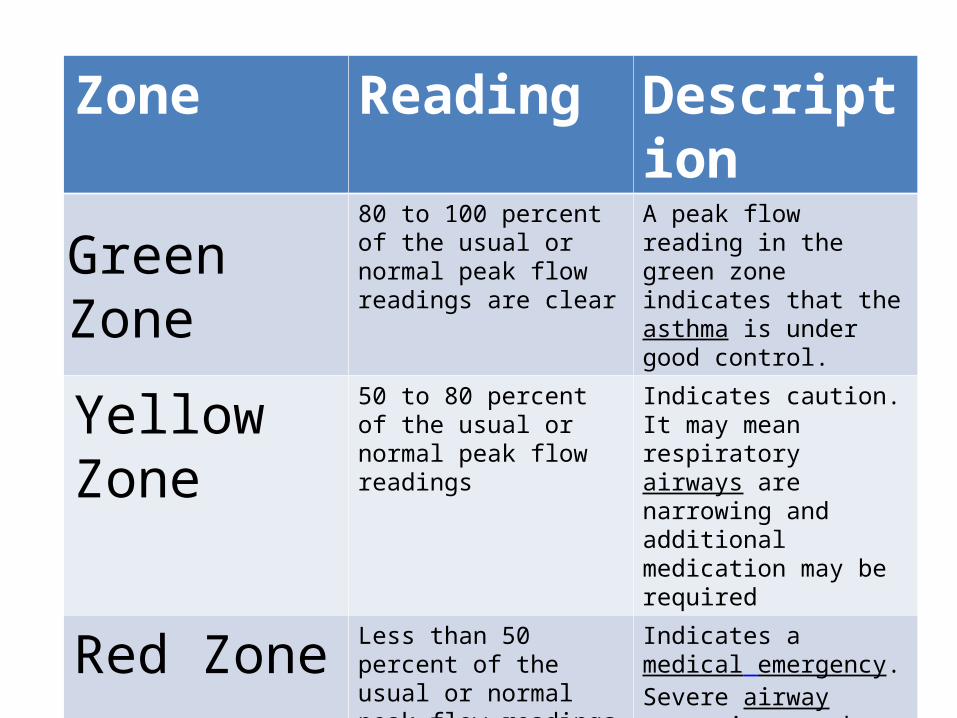
Zone Reading Description
Green Zone80 to 100 percent of the usual or normal peak flow readings are clear
A peak flow reading in the green zone indicates that the asthma is under good control.
Yellow Zone 50 to 80 percent of the usual or normal peak flow readings
Indicates caution. It may mean respiratory airways are narrowing and additional medication may be required
Red Zone Less than 50 percent of the usual or normal peak flow readings
Indicates a medical emergency. Severe airway narrowing may be occurring and immediate action needs to be taken. This would usually involve contacting a doctor or hospital.
ARTIFICIAL VENTILATION
Meghna.D.Punjabi
ARTIFICIAL VENTILLATION• Mechanical devices or artificial respirators are used in hospitals for
reduced breathing or respiratory failure.• These devices provide artificial ventilation, supply enough oxygen and
eliminate the right amount of carbon dioxide, maintain the desired arterial partial pressures of carbon dioxide and oxygen.
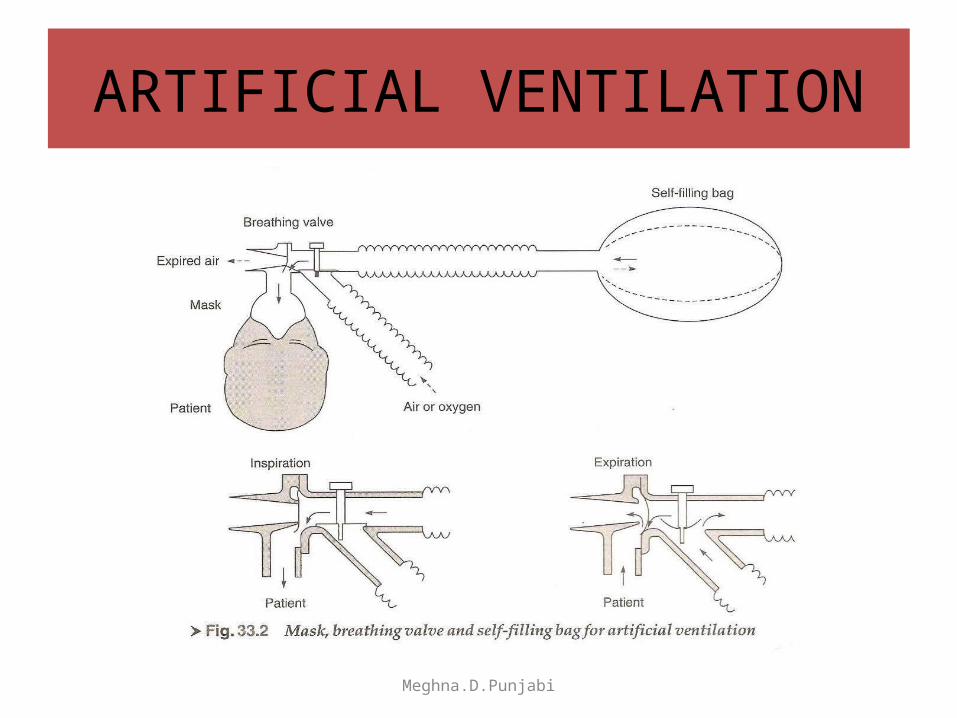
• Mechanical aids for manual artificial ventilation consists of a mask, breathing valve and self -filling bag.
• The mask, which is of soft rubber or plastic, is held firmly over the patient’s mouth and nose so that it fights tightly.
• The breathing valve serves to guide the air so that fresh air or air enriched with oxygen is supplied to the patient and expired air is conducted away.
• The bag is squeezed with one hand and functions as a pump. It is self-expanding and fills automatically with fresh air or oxygen when the patient breathes out.
Meghna.D.Punjabi
VENTILATORS
• When artificial ventilation is to be maintained for a long time or during anesthesia a ventilator is used.
• They are designed to match human breathing waveform/pattern.
• These are sophisticated equipment with a large number of controls which assist in maintaining proper and regulated breathing activity.
Meghna.D.Punjabi
NEGATIVE PRESSURE VENTILATORS• Natural inspiration is a result of negative pressure in the pleural cavity
generated by the movement of diaphragm, ventilators were initially designed to create the same effect.
• These ventilators are called negative-pressure ventilators.• In this design, the flow of air to lungs is facilitated by generating negative
pressure around the patient’s thorasic cage.• The negative pressure moves the thorasic walls outward, expanding the
intra-thorasic volume and dropping pressure inside the lungs, resulting in a pressure gradient between atmosphere and the lungs which causes the flow of atmospheric air into the lungs.
• The inspiratory and expiratory phases of the respiration are controlled by cycling the pressure inside the body chamber.
• Due to several engineering problems impeding the implementation of the concept and difficulty of accessing the patient for care and monitoring,these ventilators have not become popular.
Meghna.D.Punjabi
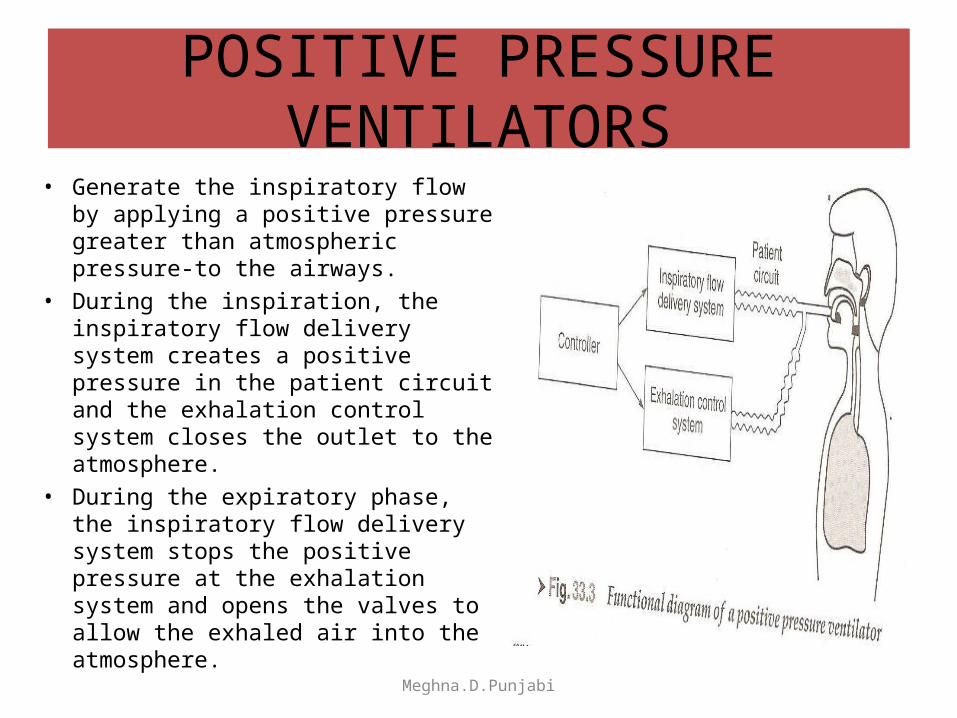
POSITIVE PRESSURE VENTILATORS• Generate the inspiratory flow by
applying a positive pressure greater than atmospheric pressure-to the airways.
• During the inspiration, the inspiratory flow delivery system creates a positive pressure in the patient circuit and the exhalation control system closes the outlet to the atmosphere.
• During the expiratory phase, the inspiratory flow delivery system stops the positive pressure at the exhalation system and opens the valves to allow the exhaled air into the atmosphere.
Meghna.D.Punjabi
MODES OF OPERATION IN POSITIVE PRESSURE VENTILATORS
Spontaneous mode.• In Spontaneous breath delivery, the ventilator
responds to the patient’s effort to breath independently.
• The patient can control the volume and rate of respiration.
• Spontaneous breath delivery is used for those patients who are on their way to full recovery but are not completely ready to breathe from the atmosphere without mechanical assistance.
Meghna.D.Punjabi
MODES OF OPERATION IN POSITIVE PRESSURE VENTILATORS
Mandatory Mode• When delivering mandatory breaths, the
ventilator controls all parameters of the breath such as tidal volume, inspiratiry flow waveform, respiration rate and oxygen content of the breath.
• Mandatory breaths are normally delivered to the patients who are incapable of breathing on their own.
Meghna.D.Punjabi
TYPES OF VENTILATORS
• ANAETHESIA VENTILATORSThey are generally small and simple equipments used
to give regular assisted breathing during an operation.
• INTENSIVE CARE VENTILATORSThey are more complicated, give accurate control over
a wide range of parameters and often incorporate ‘patient triggering facility’,
i .e. the ventilator delivers air to the patient when the patient tries to inhale.
Meghna.D.Punjabi

Meghna.D.Punjabi