Embed Size (px)
Citation preview

Retinal Detachment after Keratoprosthesis Placement:
Incidence, Predisposing Factors, and Visual and Anatomic Outcomes
M. Stephanie R. Jardeleza, M.D.Marc-Andre Rheaume, M.D.James Chodosh, M.D., MPH
Claes H. Dohlman, M.D., Ph.D.Lucy Young, M.D., Ph.D.
The authors have no financial interests to disclose.

Introduction
• The Boston Keratoprosthesis (K-Pro) is a viable option after multiple failed corneal grafts or in patients who are poor prognostic candidates for primary penetrating keratoplasty
• Secondary co-morbidities such as advanced glaucoma and vitreo-retinal pathology often led to severe visual loss and failure of visual acuity to improve after keratoprosthesis implantation

Purpose
1. Knowledge of predisposing factors to retinal detachments in certain patient populations undergoing K-Pro implantation can guide surgical planning and patient counseling
2. Knowledge of timing of retinal detachments and surgical outcomes of retinal detachment repair can optimize post-operative care in patients undergoing K-Pro implantation

Methods
Research Design:• Retrospective, noncomparative, interventional case series
Data Collection:• A review of 170 patients (205 eyes) who underwent Boston
keratoprosthesis implantation at the Massachusetts Eye and Ear Infirmary from April 1993 and June 2009
• Wilcoxon rank sum test and Fisher’s exact test used to determine significant differences between K-Pro patients who developed a retinal detachment and those who remained attached after surgery

Results
• Age range: 18-94 years old (mean 59.6 y.o.)• Mean number of K-Pro implanted per eye: 1.3
(range of 1-4)• Average follow up after first surgery: 3.9 years• Calculated incidence of RD in the entire study
population: 8.3% per 1 year

Results
• Forty four eyes (21.5%) developed a retinal detachment with a mean follow up of 2.6 years (range 1 month – 9.5 years)
• Timing of retinal detachment after K-Pro:– First year: 14 (32.6%) – Within 3 years: 26 (60.5%) – Within 5 years: 37 (86%)

Results
Category Number of Eyes
With K-Pro
Eyes with RD
after K-Pro*
Autoimmune systemic disease 65 27 (42%)
Chemical burns 19 5 (26%)
Non-autoimmune etiology 121 12 (10%)
*Mean follow up: 2.6 years

Significant predictive risk factors for Retinal Detachment after K-Pro
• History of autoimmune or systemic disease (p<0.001)• Formation of a retroprosthetic membrane (p<0.001)• Sterile vitritis (p<0.001)• Endophthalmitis (p=0.002)• History of K-Pro replacement in the same eye or multiple
K-Pro implantations (p=0.006)• Post-surgical wound leak or hypotony (p<0.001)

Surgical outcomes of RD after K-Pro
Retinal Retinal detachments (RD)detachments (RD)
RD repaired 15 (34%)
Irreparable RD 29 (66%)
Total RD 44
Outcomes of Outcomes of repairrepair
Attached 8 (53%)
Detached/Phthisis 7 (47%)
Total patients 15

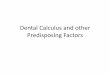
Visual outcomes of retinal detachment after Boston K-Pro surgery
48%
32%
7%
2%
11%
No light perception
Light perception
Hand motion
Count fingers
20/400 or better

Conclusion1. Retinal detachment following K-Pro implantation is more frequent in patients with
autoimmune disease (where K-Pro should be undertaken only after careful consideration).
2. Majority of retinal detachments after K-Pro implantation are irreparable at the time of diagnosis and anatomical outcomes of surgical repair remain poor.
3. Autoimmune systemic disease, post-operative endophthalmitis, sterile vitritis, formation of retroprosthetic membranes and hypotony predispose to retinal detachments in K-Pro patients. Patients with these risk factors should be co-managed with a vitreoretinal specialist.
4. Retinal detachment in K-Pro patients portend a poor visual prognosis with majority of patients having final visual acuities worse than 20/400.
5. The next frontier will be prophylaxis against development of RD after K-Pro placement i.e. aggressive control of autoimmune disease and/or performing a concomitant pars plana vitrectomy with or without 360 degree endolaser or scleral buckle placement during K-Pro implantation.

References• Aldave AJ, Kamal KM, Vo RC, Yu F. The Boston Type I
Keratoprosthesis: improving outcomes and expanding indications.Ophthalmology. 2009 April. 116(4):640-51.
• Dohlman, et al. Expert Rev Ophthalmol. 2006; 1(1),41-8.• Dohlman CH and Terada H. Keratoprosthesis in pemphigoid and
Stevens Johnson syndrome. Adv Exp Med Biol. 1998; 438:1021-5.• Ray S, Khan BF, Dohlman CH, D'Amico DJ. Management of
vitreoretinal complications in eyes with permanent keratoprosthesis. Arch Ophthalmol. 2002 May. 120(5); 559-66.
• Zerbe BL, Belin MW, Ciolino JB, Boston Type I Keratoprosthesis Study Group. Results from the multicenter Boston Type I Keratoprosthesis Study. Ophthalmology. 2006 Oct. 113(10):1779.e1-7.

Thank you
Claes H. Dohlman, M.D., Ph.D.
Lucy Young, M.D., Ph.D. James Chodosh, M.D., MPH
M. Stephanie R. Jardeleza, M.D. Marc-Andre Rheaume, M.D.