Embed Size (px)
Citation preview
NOTES, CASES, INSTRUMENTS 161
RETINAL LESIONS IN KALA-AZAR
WILLIAM S. TASSMAN, M.D. Philadelphia, Pennsylvania
DAVID D. O'BRIEN, M.D. AND
K U R T H A H N , M.D. Wiesbaden, Germany
Leishmania donovani, a protozoon parasite, was discovered in 1900 by Sir William Leishman.1 In 1903, Donovan confirmed the discovery and helped to establish the organism as the etiologic agent of kala-azar, a chronic infection which shows a special affinity for the reticulo-endothelial system.2
The parasite is found in two forms during its life cycle. In man it is about three microns long, oval, and without flagella. In insects it is 12 to 14 microns long, and prominent flagella are present.
The disease is endemic in Asia, Africa, and the Mediterranean area. It is transmitted by the phlebotomus sandfly.
Characteristically the most common symptoms of kala-azar are intermittent or remittent fever, anorexia, malaise, and occasionally purpura and bleeding from the nose or gums. Physical findings include fever, he-patosplenomegaly, and lymphadenopathy, while examination of the blood shows a macrocytic hyperchromic anemia and leuko-penia. Hyperglobulinemia may also be present.
While the above classical features of kala-azar have been amply described in the literature, no mention is made of retinal lesions. The case presented here is of interest because superficial retinal hemorrhages and cytoid bodies were noted.
CASE REPORT
F. F., a 30-year-old white man stationed in Madrid, Spain, was well until the evening of January 12, 1959, when he developed a fever. The fever subsided spontaneously in a few hours but was followed thereafter by daily spikes, usually in the late afternoon. After one week the patient became anorexic. He reported to his local hospital where a fever of 103.6°F. was noted. The pulse
was 100, and on physical examination the liver edge was palpated 3.5 cm. below the right costal margin. The spleen and axillary nodes were also palpable.
A hemogram revealed 2,300 leukocytes with 48 percent neutrophils and 52 percent lymphocytes. Hemoglobin was 9.4 gm.
Malarial smears were negative but a gram-negative rod was cultured from the blood. On the basis of the findings, typhoid fever was suspected and, on January 24, 1959 chloramphenicol and penicillin therapy was started. Despite treatment daily fever spikes to 104-105°F. continued.
Because of a continuing drop in red and white cells, blood transfusions were given on January 25, 1959, February 5, 1959, and February 7, 1959.
On February 9, 1959 the patient was transferred to the U.S.A.F. Hospital, Wiesbaden, Germany.
General physical examination at that time showed a well-developed, thin, white male, appearing chronically ill and pale. Blood pressure was 130/84 mm. Hg; pulse 96, temperature 101 °F. The skin was smooth and warm. No spiders or petechiae were noted. With the exception of the eyes, examination of the head and neck was not remarkable. The lung fields were clear. The PMI was just outside the left midclavicular line in the fifth intercostal space. A soft Grade 2 blowing apical systolic murmur was present. The abdomen was distended with a prominent venous pattern. The liver was palpable seven cm. below the right costal margin. It was smooth and tender. The spleen was palpable six cm. below the left costal margin but was not tender. Examination of the lymphatics revealed palpable axillary and posterior cervical nodes. The extremities had no palpable edema. The nails were pale. Genital, rectal, and neurologic examinations were not remarkable.
Eye examination. Visual acuity was: O.D., 6/6 without correction ; O.S., 6/6 without correction. Intraocular pressure was: O.D., 17 mm. Hg; O.S., 17 mm. Hg (Schio'tz').
External examination. The lids, cilia, lacrimai drainage apparatus, conjunctiva, and corneas were all normal. The anterior chambers were of normal depth and clear. The iris was normal in both eyes. The pupils were round, equal, and reacted to light directly and consensually.
Muscle balance was normal. Fundus examination showed the media to be
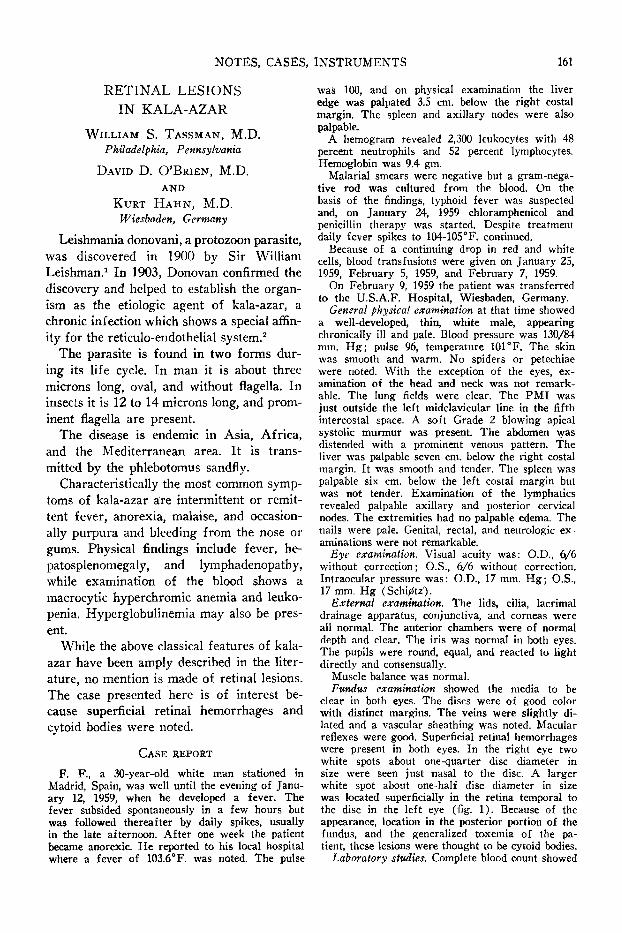
clear in both eyes. The discs were of good color with distinct margins. The veins were slightly dilated and a vascular sheathing was noted. Macular reflexes were good. Superficial retinal hemorrhages were present in both eyes. In the right eye two white spots about one-quarter disc diameter in size were seen just nasal to the disc. A larger white spot about one-half disc diameter in size was located superficially in the retina temporal to the disc in the left eye (fig. 1). Because of the appearance, location in the posterior portion of the fundus, and the generalized toxemia of the patient, these lesions were thought to be cytoid bodies.
Laboratory studies. Complete blood count showed
162 NOTES, CASES, INSTRUMENTS
Fig. 1 (Tassman). Appearance of fundus of left eye before therapy was started.
a hemoglobin of 9.4 gm. ; white blood cell count 5,900; differential count was segmented neutrophils 65 percent, lymphocytes 34 percent, and monocytes one percent. Total serum protein was 5.8 gm., albumin 3.4, globulin 2.4. Bilirubin was 0.56 mg. percent, thymol turbidity 9 units, and cephalin flocculation 3+ after 48 hours. Fasting blood sugar was 95 mg. ; sedimentation rate 17 mm. in 60 minutes. Lee and White coagulation time: 8 min., 40 sec, bleeding time 2 min., 15 sec. Serum protein electrophoresis revealed elevation of the alpha globulin and gamma globulin. Albumin was moderately depressed. Malarial smears and a preparation for lupus erythematosis were negative.
Urinalysis was normal. Stool examinations for ova and parasites were not remarkable.
Impression. At this point it was felt that there was strong evidence to indicate diffuse involvement of the reticuloendothelial system, possibly by a parasitic infestation. A bone marrow aspiration was therefore done but no parasites were found. On February 19, 1959, a liver biopsy was performed and many leishmania were discovered in the parenchymal cells.
On February 20, 1959, 2-hydroxy-stilbamidine, 225 mg. per day intravenously, was started. The patient had been acutely febrile with a double spiking fever throughout his hospitalization. Two days after starting stilbamidine therapy a gradual decrease in the spikes began. By March 1, 1959, no more fever was present.
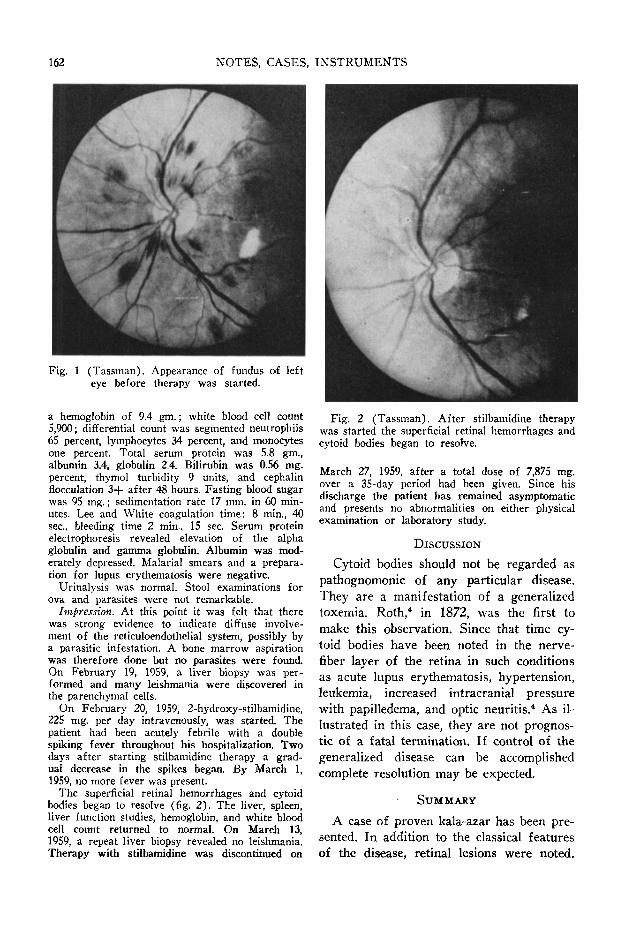
The superficial retinal hemorrhages and cytoid bodies began to resolve (fig. 2). The liver, spleen, liver function studies, hemoglobin, and white blood cell count returned to normal. On March 13, 1959, a repeat liver biopsy revealed no leishmania. Therapy with stilbamidine was discontinued on
Fig. 2 (Tassman). After stilbamidine therapy was started the superficial retinal hemorrhages and cytoid bodies began to resolve.
March 27, 1959, after a total dose of 7,875 mg. over a 35-day period had been given. Since his discharge the patient has remained asymptomatic and presents no abnormalities on either physical examination or laboratory study.
DISCUSSION
Cytoid bodies should not be regarded as pathognomonic of any particular disease. They are a manifestation of a generalized toxemia. Roth,4 in 1872, was the first to make this observation. Since that time cytoid bodies have been noted in the nerve-fiber layer of the retina in such conditions as acute lupus erythematosis, hypertension, leukemia, increased intracranial pressure with papilledema, and optic neuritis.4 As illustrated in this case, they are not prognostic of a fatal termination. If control of the generalized disease can be accomplished complete resolution may be expected.
SUMMARY
A case of proven kala-azar has been presented. In addition to the classical features of the disease, retinal lesions were noted.
NOTES, CASES, INSTRUMENTS 163
Many superficial retinal hemorrhages and three cytoid bodies were present. On stil-bamidine therapy the general condition of
HYPNOSIS AS AN ANESTHETIC IN OPHTHALMOLOGY*
OTHON R. GOMEZ RUIZ, M.D., AND ANTONIO FERNANDEZ, M.D.
Havana, Cuba
Hypnosis was used as an anesthetic in the following case.
CASE REPORT
Mr. R. R., white, aged 36 years, had an intumescent cataract, his vision being 20/500 in both eyes. All preoperative tests were favorable as well as the local condition of the eyes (light projection, motor reflexes, intraocular pressure, and so forth).
On January 24, 1959, the left eye was operated. Upon the application of one-percent pantocaine and retrobulbar injection of two-percent Novocaine, the patient showed an alarming degree of dyspnea, profuse lipothymia, with a blood pressure of 70/60 mm. Hg. The operation was interrupted and emergency treatment applied. After investigation, it was concluded that the patient was sensitive to all local anesthetics. In view of this we decided to use general anesthesia.
On February 10th, surgery was again attempted. The patient was a tall, heavy man with a short and thick neck and serious technical difficulties arose when the anesthetist tried to insert the tube in the trachea. Three attempts failed. During the second and third attempts, the patient became cyanotic, with marked respiratory difficulty. Since a fatal outcome or the possibility of central nervous system damage from anoxia was feared, we decided not to proceed with surgery this time either.
Acknowledging the impossibility of desensitizing for anesthetics, we decided to operate with the patient under deep hypnosis.
On May 19th, the first preoperative hypnotic session was started and continued at four-day intervals for three sessions. A deep trance was obtained, with anesthesia at superficial and deep levels.
♦From the League Against Blindness Hospital and Covadonga Hospital.
the patient markedly improved, and the retinal picture returned to normal.
1601 Spring Garden Street (30).
On June 10th, the patient was admitted to the hospital. The following day he was put under hypnosis in the operating room without any preopera-tive sedation (drugs). Five minutes later surgery was started.
The operation was conducted in the ordinary manner (corneal incision, scissors, iridectomy, eight sutures). The patient appeared completely relaxed and in good general condition, showing a complete loss of sensibility but preserving the oculomotor reflexes. At the end of the operation, when he was awakened, he showed no signs of pain or discomfort (due to the posthypnotic suggestions). The patient was under hypnosis for a total of 25 minutes.
On June 20th, 10 days after the operation, vision was 20/40 with a +10D. sph. On July 26th, vision was 20/20, Jl .
L No. 452, Vedado.
We wish to thank Dr. Tomas R. Yanes, Director of the League Against Blindness Hospital for his encouragement.
GLAUCOMATOCYCLITIC CRISES
DEREK G. SIMPSON, F.R.C.S. (Eng. and Edin.)
Vancouver, British Columbia
REVIEW
Glaucomatocyclitic crises were first named and described as a clinical entity by Posner and Schlossman in 1948.1 Earlier literature contains vague or incomplete descriptions of conditions which might have been glaucomatocyclitic crises.2-5 The condition soon attracted attention and recognition. Papers by several American authors6"9
have appeared and cases have been reported from other countries.10-14 The incidence is difficult to determine because more cases
REFERENCES 1. Corderò, A. A., and Corti, R. N. : Leishmaniosis. La Prensa Med. Argentina, 40:3467-3472, 1953. 2. Cecil, R. L., and Loeb, R. F . : Textbook of Medicine. Philadelphia and London, Saunders, 1951,
pp. 394-401. 3. Pestre, A. : Manifestations oculaires de la Leishmaniose cutanee. Algerie Med., 59:589-597, 1955. 4. Maumenee, A. E. : Retinal lesions in lupus erythematosis. Am. J. Ophth., 23 :9, 1940.





























