Embed Size (px)
Citation preview
Original Research—Sinonasal Disorders
Retromaxillary Pneumatization ofPosterior Ethmoid Air Cells: NovelDescription and Surgical Implications
Otolaryngology–Head and Neck Surgery2016, Vol. 155(2) 340–346� American Academy ofOtolaryngology—Head and NeckSurgery Foundation 2016Reprints and permission:sagepub.com/journalsPermissions.navDOI: 10.1177/0194599816639943http://otojournal.org
Islam R. Herzallah, MD, PhD1,2, Faisal A. Saati, MD2,3,Osama A. Marglani, MD, FRCSC2,4, and Rehab F. Simsim, MD2
No sponsorships or competing interests have been disclosed for this article.
Abstract
Objective. Retromaxillary pneumatization of posterior eth-moid (PE) air cells is an area that is yet to have appropriatedescription in rhinologic literature.
Study Design. Case series with chart review.
Setting. Tertiary care hospital.
Subjects and Methods. First, 524 sides in 262 paranasal sinuscomputed tomography scans were analyzed: 350 normalsides were examined for PE pneumatization lateral to thesagittal plane of the medial wall of maxillary sinus posteriorly,and 174 diseased sides were similarly reviewed to check howpathology may affect identification and measurements. Followingthat, 153 operated sides in 84 cases prepared for revision endo-scopic sinus surgery (ESS) were studied for residual diseasedcells at different anatomic locations.
Results. Overall, retromaxillary PE pneumatization was identi-fiable in 416 of the 524 sides (79.4%). Lateral retromaxillaryextension varied from 0.5 to 12.3 mm (mean 6 SD, 4.8 6
2.3 mm). This area of pneumatization is bounded anteroinfer-iorly by the junction between the posterior and superiorwalls of the maxillary sinus. Three cell types were describeddepending on the degree of lateral extension (type I, \3 mm;type II, 3-6 mm; type III, .6 mm). This cell, which we referto as the Herzallah cell, was distinguishable from the anteriorethmoid Haller cell and was found to have residual disease in50.3% of cases prepared for revision ESS.
Conclusion. Retromaxillary extension of PE air cells varies con-siderably and requires attention during ESS. Residual undis-sected retromaxillary cell is a common finding in revision ESSand can contribute to inadequate disease clearance.
Keywords
posterior ethmoids, paranasal sinus, anatomy variations, ana-tomical classification, lamina papyracea, Haller cell, ethmo-maxillary sinus, sphenomaxillary plate, lateral sphenoidrecess, revision functional endoscopic sinus surgery, preven-tion of residual disease, chronic rhinosinusitis, computed
tomography, imaging, radiology, nasal polyps, allergic fungalsinusitis
Received December 21, 2015; revised February 11, 2016; accepted
February 29, 2016.
Understanding endoscopic paranasal sinus (PNS) anat-
omy is the key for safe and effective endoscopic
sinus surgery (ESS). Identification of anatomic varia-
tions is equally important in preoperative planning and intrao-
perative orientation. Therefore, rhinologic literature is rich
with studies that describe endoscopic landmarks and the dif-
ferent anatomic scenarios that surgeons may encounter.1-4
Endoscopic, radiologic, and anatomic studies that have
helped surgeons better perform ESS are numerous. Examples
include description of agger nasi and frontal sinus infundibular
cells, providing surgeons with better orientation during the
endonasal frontal sinus approach.5-7 Description of Onodi and
Haller cells was similarly valuable in helping appropriate and
safer clearance of ethmoid air cells as well as proper sphenoid
and maxillary sinusotomies, respectively.8-10 For the same
reason, we have maintained a focus on exploring the endo-
scopic anatomy in several projects over the past decade.11-13
Despite these anatomic descriptions, residual disease
after ESS continues to occur and is not uncommon.14-16 A
recent study showed that missed ethmoid cells over the
lamina papyracea (LP) and skull base is one of the most
common findings in revision sinus surgery.14
The recent classification of LP position in the endoscopic
field was introduced to help surgeons address anterior
1Department of Otorhinolaryngology, Faculty of Medicine, Zagazig
University, Zagazig, Egypt2ENT Department, King Abdullah Medical City, Makkah, Saudi Arabia3Department of Otolaryngology, Al-Hada Armed Forces Hospital, Taif,
Saudi Arabia4Department of Otolaryngology, Umm Al-Qura University, Makkah, Saudi
Arabia
Corresponding Author:
Islam R. Herzallah, MD, PhD, Department of Otorhinolaryngology, Faculty
of Medicine, Zagazig University, Egypt.
Email: [email protected]
at SOCIEDADE BRASILEIRA DE CIRUR on August 5, 2016oto.sagepub.comDownloaded from
ethmoid disease more safely and effectively.17 Retromaxillary
pneumatization of posterior ethmoid (PE) cells is yet another
endoscopically important area that seems to be poorly recog-
nized and frequently missed during ESS, particularly for resi-
dents and surgeons with less experience. The lack of studies
describing this anatomic location easily explains the paucity of
knowledge to appropriately tackle this region. Therefore, we
have conducted this extensive work to describe this pneumati-
zation of PE air cells and to investigate its importance from
the endoscopic perspective.
Subjects and Methods
Study Design
We conducted a retrospective analysis of PNS computed
tomography (CT) scans that were obtained for adult patients
as part of evaluation for their sinonasal or anatomically
related disorders. Enrollment criteria included adult PNS
CT scans performed at our institution, King Abdullah
Medical City, between January 2013 and August 2015, at 1-
mm section thickness and interval, with the exclusion of
those with sinonasal neoplasms, invasive fungal sinusitis, or
craniofacial abnormalities.
First, a total of 524 sides in 262 PNS CT scans were
reviewed: 350 normal sides that had clear ethmoid sinuses
on PNS imaging for different purposes (eg, headache, nasal
septal deviation, preoperative evaluation for endoscopic
dacryocystorhinostomy, or unilateral pathology on the other
side) and 174 sides with different ethmoid pathologies, with
the above exclusion criteria. Following that, we reviewed
153 operated sides in 84 patients who had their CT scans as
part of their evaluation for persistent symptoms and preo-
perative preparation for revision ESS. The retrospective
analysis was approved by the Institutional Review Board at
King Abdullah Medical City before commencement of the
study.
CT Examination and Analysis
All PNS CT scans reviewed at our institution were performed
with a 64-slice Siemens Somatom Definition Scanner (Syngo
CT 2012B; Siemens Healthcare, Forchheim, Germany). CT
scans were obtained at 1-mm section thickness and interval,
120 to 320 mA, 120 kV, 1-second rotation time, and a 16- to
18-cm field of view.
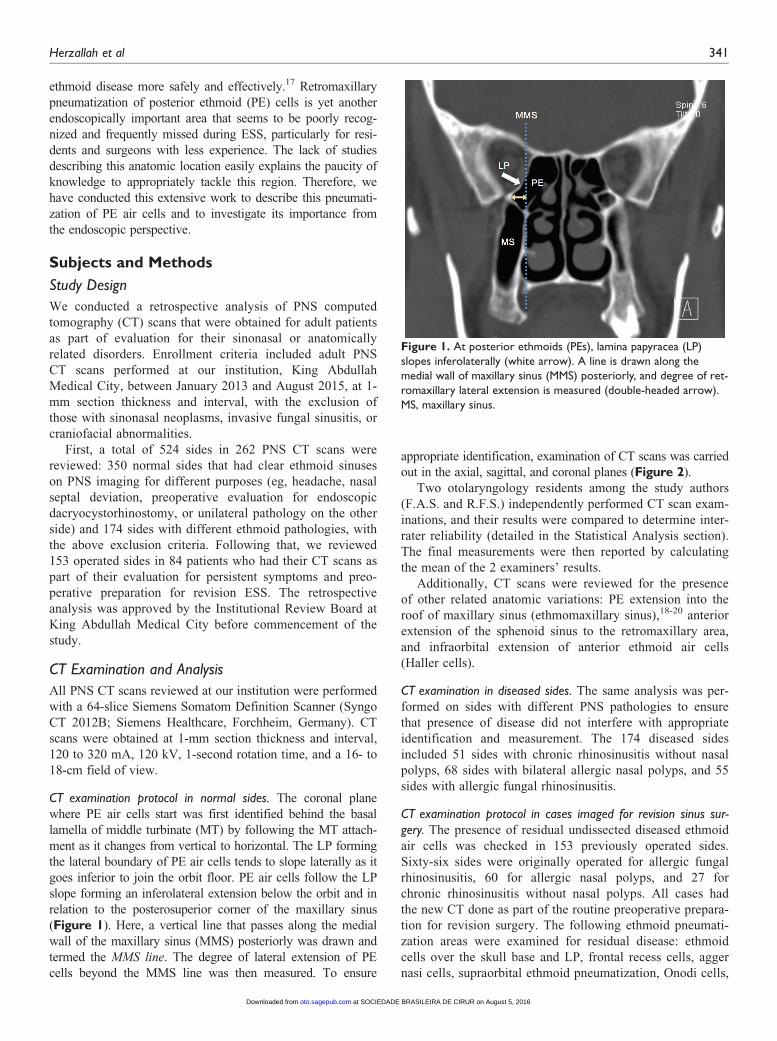
CT examination protocol in normal sides. The coronal plane
where PE air cells start was first identified behind the basal
lamella of middle turbinate (MT) by following the MT attach-
ment as it changes from vertical to horizontal. The LP forming
the lateral boundary of PE air cells tends to slope laterally as it
goes inferior to join the orbit floor. PE air cells follow the LP
slope forming an inferolateral extension below the orbit and in
relation to the posterosuperior corner of the maxillary sinus
(Figure 1). Here, a vertical line that passes along the medial
wall of the maxillary sinus (MMS) posteriorly was drawn and
termed the MMS line. The degree of lateral extension of PE
cells beyond the MMS line was then measured. To ensure
appropriate identification, examination of CT scans was carried
out in the axial, sagittal, and coronal planes (Figure 2).
Two otolaryngology residents among the study authors
(F.A.S. and R.F.S.) independently performed CT scan exam-
inations, and their results were compared to determine inter-
rater reliability (detailed in the Statistical Analysis section).
The final measurements were then reported by calculating
the mean of the 2 examiners’ results.
Additionally, CT scans were reviewed for the presence
of other related anatomic variations: PE extension into the
roof of maxillary sinus (ethmomaxillary sinus),18-20 anterior
extension of the sphenoid sinus to the retromaxillary area,
and infraorbital extension of anterior ethmoid air cells
(Haller cells).
CT examination in diseased sides. The same analysis was per-
formed on sides with different PNS pathologies to ensure
that presence of disease did not interfere with appropriate
identification and measurement. The 174 diseased sides
included 51 sides with chronic rhinosinusitis without nasal
polyps, 68 sides with bilateral allergic nasal polyps, and 55
sides with allergic fungal rhinosinusitis.
CT examination protocol in cases imaged for revision sinus sur-gery. The presence of residual undissected diseased ethmoid
air cells was checked in 153 previously operated sides.
Sixty-six sides were originally operated for allergic fungal
rhinosinusitis, 60 for allergic nasal polyps, and 27 for
chronic rhinosinusitis without nasal polyps. All cases had
the new CT done as part of the routine preoperative prepara-
tion for revision surgery. The following ethmoid pneumati-
zation areas were examined for residual disease: ethmoid
cells over the skull base and LP, frontal recess cells, agger
nasi cells, supraorbital ethmoid pneumatization, Onodi cells,
Figure 1. At posterior ethmoids (PEs), lamina papyracea (LP)slopes inferolaterally (white arrow). A line is drawn along themedial wall of maxillary sinus (MMS) posteriorly, and degree of ret-romaxillary lateral extension is measured (double-headed arrow).MS, maxillary sinus.
Herzallah et al 341
at SOCIEDADE BRASILEIRA DE CIRUR on August 5, 2016oto.sagepub.comDownloaded from
and Haller cells. Retromaxillary pneumatization was also
analyzed in this study.
Statistical Analysis
Statistical analyses were performed with SPSS 22.0 for
Windows (IBM Corp, Armonk, New York). Interrater relia-
bility was examined via the intraclass correlation coefficient
(ICC) to determine the degree of agreement on measure-
ments between the 2 observers. Measurements were also
compared between right and left sides through paired-
samples t test and between the normal and diseased sides
through independent-samples t test. The significance level
was set at P \ .05.
Results
The average 6 SD age of the 262 patients (524 sides) was
38.6 6 16.0 and 37.02 6 14.9 years in the normal and dis-
eased groups, respectively, with no significant difference
between the 2 groups (P . .05; range, 18-88 and 18-79
years, respectively). Overall, 58.4% of patients were men
and 41.6% women, again with no significant difference in
sex distribution between groups (P . .05).
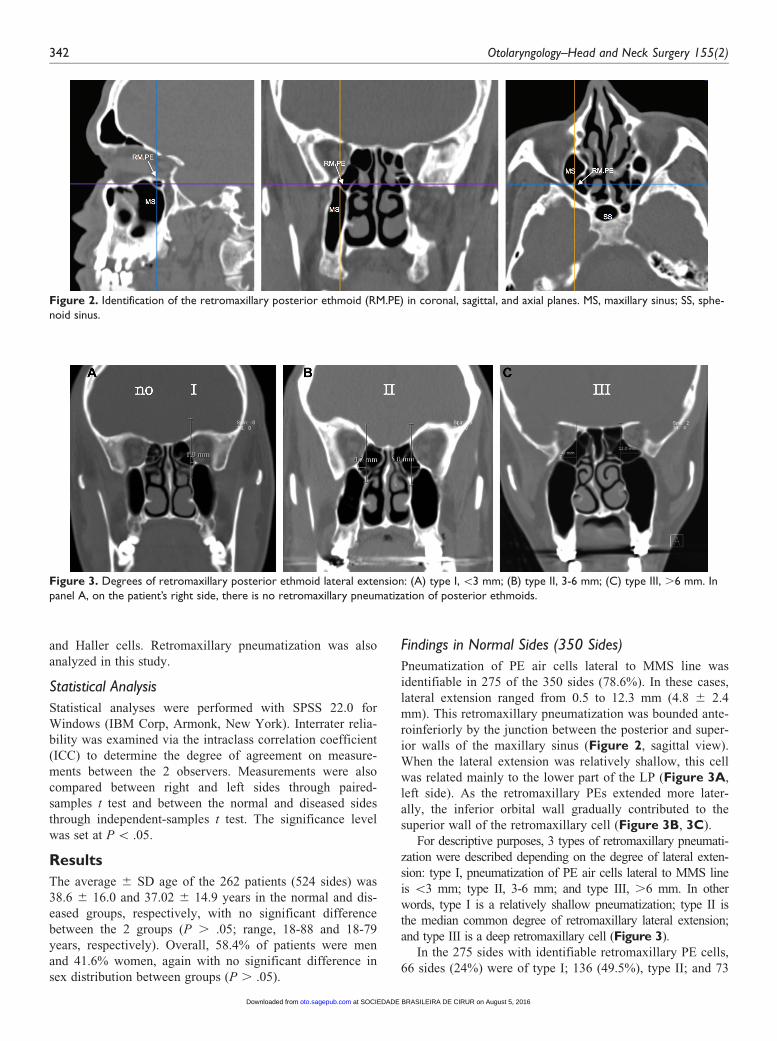
Findings in Normal Sides (350 Sides)
Pneumatization of PE air cells lateral to MMS line was
identifiable in 275 of the 350 sides (78.6%). In these cases,
lateral extension ranged from 0.5 to 12.3 mm (4.8 6 2.4
mm). This retromaxillary pneumatization was bounded ante-
roinferiorly by the junction between the posterior and super-
ior walls of the maxillary sinus (Figure 2, sagittal view).
When the lateral extension was relatively shallow, this cell
was related mainly to the lower part of the LP (Figure 3A,
left side). As the retromaxillary PEs extended more later-
ally, the inferior orbital wall gradually contributed to the
superior wall of the retromaxillary cell (Figure 3B, 3C).
For descriptive purposes, 3 types of retromaxillary pneumati-
zation were described depending on the degree of lateral exten-
sion: type I, pneumatization of PE air cells lateral to MMS line
is \3 mm; type II, 3-6 mm; and type III, .6 mm. In other
words, type I is a relatively shallow pneumatization; type II is
the median common degree of retromaxillary lateral extension;
and type III is a deep retromaxillary cell (Figure 3).
In the 275 sides with identifiable retromaxillary PE cells,
66 sides (24%) were of type I; 136 (49.5%), type II; and 73
Figure 2. Identification of the retromaxillary posterior ethmoid (RM.PE) in coronal, sagittal, and axial planes. MS, maxillary sinus; SS, sphe-noid sinus.
Figure 3. Degrees of retromaxillary posterior ethmoid lateral extension: (A) type I, \3 mm; (B) type II, 3-6 mm; (C) type III, .6 mm. Inpanel A, on the patient’s right side, there is no retromaxillary pneumatization of posterior ethmoids.
342 Otolaryngology–Head and Neck Surgery 155(2)
at SOCIEDADE BRASILEIRA DE CIRUR on August 5, 2016oto.sagepub.comDownloaded from

(26.5%), type III. Twelve sides had ethmomaxillary sinus,
all of which were of type III pneumatization.
In 59 of 350 sides (16.9%), retromaxillary pneumatiza-
tion was not part of the PEs but was rather caused by ante-
rior extension of the sphenoid into the retromaxillary area
(Figure 4). In the remaining 16 sides (4.6%), no retromax-
illary pneumatization was identifiable, neither from the PEs
nor from the sphenoid sinus (Figure 3A, right side).
The retromaxillary PE air cell, which we also refer to as
Herzallah cell, was distinguishable from the infraorbital
anterior ethmoid pneumatization known as Haller cell,
which is part of the anterior group of ethmoid cells and was
identified in 26 (7.4%) of the examined normal sides
(Figure 5).
The ICC for measurements of PE retromaxillary lateral
extension as taken by the 2 examiners was 0.88 (95% confi-
dence interval: 0.86-0.91) at a P value \.001, indicating
high interrater reliability with statistical significance. There
was no statistically significant difference in measurements
between right and left sides (P . .05).
Findings in Diseased Sides (174 Sides)
Pneumatization of PE air cells lateral to MMS line was identi-
fiable in 141 of the 174 diseased sides (81%). In these cases,
lateral extension ranged from 0.65 to 10.4 mm (4.8 6 2.2
mm). In 25 of 174 sides (14.4%), retromaxillary pneumatiza-
tion was formed by anterior extension of the sphenoid sinus,
while in the remaining 8 sides (4.6%), no retromaxillary pneu-
matization was identifiable, neither from the PEs nor from the
sphenoid sinus. In 6 of the 25 sides with retromaxillary sphe-
noid extension (24%), this area of pneumatization was spared
of the disease that involves the PE air cells (Figure 4).
In the 141 diseased sides with identifiable retromaxillary
PE cells, 34 sides (24.1%) were of type I; 67 (47.5%), type
II; and 40 (28.4%), type III. Five sides had ethmomaxillary
sinus, all of which were of type III pneumatization.
The ICC for measurements of PE retromaxillary lateral
extension as taken by the 2 examiners was 0.87 (95% confi-
dence interval: 0.82-0.90) at a P value \.001, indicating high
interrater reliability with statistical significance. Additionally,
there was no statistically significant difference in the
Figure 5. Although retromaxillary posterior ethmoids (Herzallah [Hz] cells) are partly related to the inferior orbital wall, these should bedifferentiated from the infraorbital anterior ethmoid air cells (Haller [Ha] cells).
Figure 4. Anterior extension (asterisk) of sphenoid sinus (SS) to the posterior wall of the maxillary sinus (MS). RM.PE, retromaxillary pos-terior ethmoid pneumatization: note relationship to lateral sphenoid extension (LS) and upper pterygopalatine fossa (PPF).
Herzallah et al 343
at SOCIEDADE BRASILEIRA DE CIRUR on August 5, 2016oto.sagepub.comDownloaded from

measurements between the normal and diseased sides (P =
.94), indicating that the presence of pathology did not inter-
fere with proper identification and measurement.
Findings in All Examined Sides Combined (524 Sides)
Overall, retromaxillary PE pneumatization was identifiable
in 416 of the 524 examined sides (79.4%). Lateral retromax-
illary extension varied from 0.5 to 12.3 mm (4.8 6 2.3
mm). In 84 of 524 sides (16%), retromaxillary pneumatiza-
tion was formed by anterior extension of the sphenoid sinus.
In the remaining 24 of 524 sides (4.6%), no retromaxillary
pneumatization was identifiable, neither from the PEs nor
from the sphenoid sinus.
In the 416 sides with identifiable retromaxillary PE cells,
100 sides (24%) were categorized as type I, 203 (48.8%) as
type II, and 113 (27.2%) as type III. Seventeen sides had
ethmomaxillary sinus, all of which were of type III pneuma-
tization. Haller cells were identifiable in 36 of the 524
examined sides (6.9%).
Findings in Operated Sides Prepared for Revision ESS(153 Sides)
The average age of the 84 patients was 34.4 6 14.0 years.
Forty-eight patients (57.1%) were men and 36 (42.9%)
women. The highest prevalence of residual undissected cells
was in the anterior ethmoid air cells along the LP (97 sides,
63.4%), anterior ethmoid cells along the skull base (61.4%),
PE cells along the LP (60.8%), PE cells along the skull base
(57.5%), frontal recess cells (56.2%), agger nasi cells
(54.2%), and PE retromaxillary cells in 77 sides (50.3%).
Pneumatization of PE air cells lateral to MMS line was
identifiable in 119 of the 153 sides (77.8%). In these cases,
33 sides (27.7%) were of type I PE retromaxillary pneumati-
zation; 54 (45.4%), type II; and 32 (26.9%), type III.
Residual PE retromaxillary cells were found in 20 sides
(60.6%) of type I pneumatization, 35 (64.8%) of type II,
and 22 (68.8%) of type III. No statistically significant dif-
ference was found in the prevalence of residual cells among
the 3 categories of PE retromaxillary pneumatization (P .
.05).
Other, less common ethmoid pneumatization areas that
had residual disease included Onodi cells (16.3%), supraor-
bital ethmoid pneumatization (9.8%), and Haller cells
(5.2%). Retromaxillary sphenoid extension had residual dis-
ease in 10.5% of the examined sides.
Discussion
Residual ethmoid disease continues to be one of the
common findings in revision ESS.14-16 This fact needs to be
acknowledged and should alert us that further understanding
of the endoscopic ethmoid anatomy is necessary to help the
training of less experienced surgeons. Fortunately, the cur-
rent progress in sinonasal imaging and the increasing use of
intraoperative navigation are continuously helping us in the
3-dimensional understanding of the endoscopic anatomy.
Figure 6 demonstrates intraoperative identification of the
retromaxillary PE cell along with CT navigation in different
planes. Video 1 (at www.otojournal.org/supplemental) also
demonstrates intraoperative dissection of a retromaxillary
PE cell along with other closely related landmarks.
Figure 6. Intraoperative identification of retromaxillary posterior ethmoids. MS, maxillary sinus; SS, sphenoid sinus opening.
344 Otolaryngology–Head and Neck Surgery 155(2)
at SOCIEDADE BRASILEIRA DE CIRUR on August 5, 2016oto.sagepub.comDownloaded from

Retromaxillary PE pneumatization is an area that has
received poor attention in the rhinologic literature as com-
pared with other anatomic variations. In fact, one could
hardly find any article that specifically addresses this pneu-
matization or describes its different anatomic scenarios. Yet,
Haller cells—or infraorbital pneumatization of the anterior
ethmoids in the region of the ostiomeatal complex—have
been extensively described before, with a prevalence that
usually lies in the range of 3% to 18%.21-24 Although retro-
maxillary PEs are also partly located in relation to the orbit
floor, these should be differentiated from Haller cells given
the different anatomic location that makes each of them of
particular importance during ESS. However, we have come
across studies on sinonasal anatomic variations in which ret-
romaxillary PEs were misinterpreted as Haller cells.25,26
This can be explained by the lack of appropriate description
and has guided us to use the term Herzallah cell to distin-
guish them from their Haller counterpart (Figure 5).
Anterior extension of the sphenoid sinus to form retro-
maxillary pneumatization has been described.21,22,26,27 In
such cases, the intervening wall between the maxillary and
sphenoid sinuses was termed the sphenomaxillary plate, and
this variation was reported in 11% to 15% of cases.21,22
However, the current study shows that retromaxillary PE
pneumatization is, by far, more common the sphenoid one
(79.4% vs 16%). This differentiation is important, since
sphenoid retromaxillary extension can be spared in cases of
PE disease, an observation that was reported in 24% of the
diseased sides with sphenoid retromaxillary extension in our
series (Figure 4). We have to mention that retromaxillary
pneumatization should also be differentiated from the lateral
sphenoid recess, which is rather a pneumatization in the
pterygoid base behind the upper part of the pterygopalatine
fossa (Figure 4).
In this study, we have demonstrated different lateral
extension degrees of the retromaxillary PEs and typed them
accordingly. Although an ethmomaxillary sinus has been
described in about 2% of cases,18-20 it has received limited
citation, which may be explained by the lack of thorough
analysis of this variation. Therefore, we believe the current
description of retromaxillary PE pneumatization signifi-
cantly clarifies the variations in this region.
For descriptive purposes, we have proposed to classify
the depth of retromaxillary cell lateral extension for easier
comparison among sides. The middle group (3-6 mm) was
chosen since it roughly represents the mean depth 6 0.5 SD
and thus constitutes the most common category that sur-
geons may encounter. The other 2 groups (\3 and .6 mm)
represent relatively shallow and deep retromaxillary PE
pneumatization, respectively. The categorization presented
in this study is not meant to ask the surgeon to take intrao-
perative measurements but rather to appreciate the relative
depth of retromaxillary PE pneumatization, to help him or
her appropriately tackle this region. Note, however, that no
statistically significant difference was cited in the prevalence
of residual disease among the 3 types in revision cases.
In accordance with our results, several investigators have
found residual undissected ethmoid air cells over the LP
and skull base in .60% of patients undergoing revision
ESS.14-16 The current study shows that retromaxillary PE
cells are as likely to be left undissected as other major eth-
moid cells. Since retromaxillary PE cells are in direct rela-
tionship with the lower part of the LP, this would explain
why missing this region would contribute to the frequent
finding of residual disease over the LP. Proper orientation
to and dissection of the retromaxillary PE cells would
ensure proper clearance of the ethmoid disease over the
LP. Furthermore, since this area of pneumatization is
located anterior to the lateral sphenoid pneumatization,
proper dissection of the retromaxillary cell would help in
better exposure of the lateral sphenoid extension. Although
no statistically significant difference was found in the rate
of residual cells among the 3 degrees of PE retromaxillary
extension, attention to the relative depth of the retromaxil-
lary PE cell should help surgeons and residents perform
the closely related endoscopic work more safely and
effectively.
Conclusion
The current study introduces a novel description of the ret-
romaxillary PE pneumatization. Residual undissected retro-
maxillary cell is a common finding in revision ESS. The
recognition of this anatomic variation should help residents
in training and would improve surgeons’ ability to perform
better clearance of ethmoid air cells.
Acknowledgments
We thank Mr Ammar Alwaheib, RT, and the staff at Radiodiagnosis
Department in King Abdullah Medical City for their conscientious
assistance and help.
Author Contributions
Islam R. Herzallah, inventing and developing the research idea,
reviewing literature, defining the study protocol and methodology,
preparing Institutional Review Board forms, designing computed
tomography (CT) analysis and measurement protocol, mentoring
work implementation, thorough review and examination of CTs,
performing statistical analysis, writing the manuscript and preparing
figures; Faisal A. Saati, preparing a list of available CTs, performing
CT measurements, data collection, contribution to manuscript writing,
data interpretation, statistical analysis and figures preparation, and
review and approval of the final manuscript; Osama A. Marglani,
contribution to manuscript writing and data interpretation and analy-
sis, assistance in preparing a list of available CTs, review and
approval of the final manuscript; Rehab F. Simsim, performing CT
measurements and data collection, contribution to manuscript writing,
figures preparation, data interpretation and analysis, and review and
approval of the final manuscript.
Disclosures
Competing interests: None.
Sponsorships: None.
Funding source: None.
Herzallah et al 345
at SOCIEDADE BRASILEIRA DE CIRUR on August 5, 2016oto.sagepub.comDownloaded from
References
1. Amine MA, Anand V. Anatomy and complications: safe sinus.
Otolaryngol Clin North Am. 2015;48:739-748.
2. Lund VJ, Stammberger H, Fokkens WJ, et al. European posi-
tion paper on the anatomical terminology of the internal nose
and paranasal sinuses. Rhinol Suppl. 2014;(24):1-34.
3. Nouraei SA, Elisay AR, Dimarco A, et al. Variations in para-
nasal sinus anatomy: implications for the pathophysiology of
chronic rhinosinusitis and safety of endoscopic sinus surgery. J
Otolaryngol Head Neck Surg. 2009;38:32-37.
4. Kantarci M, Karasen RM, Alper F, Onbas O, Okur A,
Karaman A. Remarkable anatomic variations in paranasal
sinus region and their clinical importance. Eur J Radiol. 2004;
50:296-302.
5. Wormald PJ. The agger nasi cell: the key to understanding the
anatomy of the frontal recess. Otolaryngol Head Neck Surg.
2003;129:497-507.
6. Brunner E, Jacobs JB, Shpizner BA, Lebowitz RA, Holliday
RA. Role of the agger nasi cell in chronic frontal sinusitis.
Ann Otol Rhinol Laryngol. 1996;105:694-700.
7. Bent JP, Cuilty-Siller C, Kuhn FA. The frontal cell as a cause
of frontal sinus obstruction. Am J Rhinol. 1994;8:185-191.
8. Caversaccio M, Boschung U, Mudry A. Historical review of
Haller’s cells. Ann Anat. 2011;193:185-190.
9. Wada K, Moriyama H, Edamatsu H, et al. Identification of
Onodi cell and new classification of sphenoid sinus for endo-
scopic sinus surgery. Int Forum Allergy Rhinol. 2015;5:1068-
1076.
10. Unal B, Bademci G, Bilgili YK, Batay F, Avci E. Risky ana-
tomic variations of sphenoid sinus for surgery. Surg Radiol
Anat. 2006;28:195-201.
11. Herzallah IR, Casiano RR. Endoscopic endonasal study of the
internal carotid artery course and variation. Am J Rhinol.
2007;21:262-270.
12. Herzallah IR, Germani R, Casiano RR. Transnasal endoscopic
study of the infratemporal fossa: a new orientation.
Otolaryngol Head Neck Surg. 2009;140:861-865.
13. Casiano RR, Herzallah IR, Anstead A, et al. Advanced endo-
scopic sinonasal dissection. In: Casiano RR, ed. Endoscopic
Sinonasal Dissection Guide. New York, NY: Thieme Medical
Publishers Inc; 2012:59-99.
14. Gore MR, Ebert CS Jr, Zanation AM, Senior BA. Beyond the
‘‘central sinus’’: radiographic findings in patients undergoing
revision functional endoscopic sinus surgery. Int Forum
Allergy Rhinol. 2013;3:139-146.
15. Khalil HS, Eweiss AZ, Clifton N. Radiological findings in
patients undergoing revision endoscopic sinus surgery: a retro-
spective case series study. BMC Ear Nose Throat Disord.
2011;7:11:4.
16. Musy PY, Kountakis SE. Anatomic findings in patients under-
going revision endoscopic sinus surgery. Am J Otolaryngol.
2004;25:418-422.
17. Herzallah IR, Marglani OA, Shaikh AM. Variations of lamina
papyracea position from the endoscopic view: a retrospective
computed tomography analysis. Int Forum Allergy Rhinol.
2015;5:263-270.
18. Sirikcxi A, Bayazit YA, Bayram M, Kanlikama M.
Ethmomaxillary sinus: a particular anatomic variation of the
paranasal sinuses. Eur Radiol. 2004;14:281-285.
19. Ozcan KM, Selcuk A, Oruk V, Sarikaya Y, Dere H.
Ethmomaxillary sinus. Eur Arch Otorhinolaryngol. 2008;265:
185-188.
20. Khanobthamchai K, Shankar L, Hawke M, Bingham B.
Ethmomaxillary sinus and hypoplasia of maxillary sinus. J
Otolaryngol. 1991;20:425-427
21. Nouraei SA, Elisay AR, Dimarco A, et al. Variations in para-
nasal sinus anatomy: implications for the pathophysiology of
chronic rhinosinusitis and safety of endoscopic sinus surgery. J
Otolaryngol Head Neck Surg. 2009;38:32-37.
22. Kantarci M, Karasen RM, Alper F, Onbas O, Okur A,
Karaman A. Remarkable anatomic variations in paranasal
sinus region and their clinical importance. Eur J Radiol. 2004;
50:296-302.
23. Perez-Pinas I, Sabate J, Carmona A, Catalina-Herrera CJ,
Jimenez-Castellanos J. Anatomical variations in the human
paranasal sinus region studied by CT. J Anat. 2000;197:221-
227.
24. Kennedy DW, Zinreich SJ. Functional endoscopic approach to
inflammatory sinus disease: current perspectives and technique
modifications. Am J Rhinol. 1998;2:89-96.
25. Arslan H, Aydinlioglu A, Bozkurt M, Egeli E. Anatomic varia-
tions of the paranasal sinuses: CT examination for endoscopic
sinus surgery. Auris Nasus Larynx. 1999;26:39-48.
26. Meloni F, Mini R, Rovasio S, Stomeo F, Teatini GP.
Anatomic variations of surgical importance in ethmoid labyr-
inth and sphenoid sinus: a study of radiological anatomy. Surg
Radiol Anat. 1992;14:65-70.
27. Selcuk A, Ozcan KM, Akdogan O, Bilal N, Dere H.
Variations of maxillary sinus and accompanying anatomical
and pathological structures. Craniofac Surg. 2008;19:159-164.
346 Otolaryngology–Head and Neck Surgery 155(2)
at SOCIEDADE BRASILEIRA DE CIRUR on August 5, 2016oto.sagepub.comDownloaded from