Embed Size (px)
Citation preview

Return to work after lower limb amputation
HELENA BURGER & CRT MARINCEK
Institute for Rehabilitation, Ljubljana, Slovenia
AbstractPurpose. To review the literature on return to work after lower limb amputation.Method. A comprehensive review of literature on return to work after lower limb amputation was carried out, searchingMEDLINE and PubMED.Results. Most authors found return-to-work rate to be about 66%. Between 22 and 67% of the subjects retained the sameoccupation, while the remainder had to change occupation. Post-amputation jobs were generally more complex with arequirement for a higher level of general educational development and were physically less demanding. The return to workdepends on: general factors, such as age, gender and educational level; factors related to impairments and disabilities due toamputation (amputation level, multiple amputations, comorbidity, reason for amputation, persistent stump problems, thetime from the injury to obtaining a permanent prosthesis, wearing comfort of the prosthesis, walking distance and restrictionsin mobility); and factors related to work and policies (salary, higher job involvement, good support from the implementingbody and the employer and social support network).Conclusions. Subjects have problems returning to work after lower limb amputation. Many have to change their work and/orwork only part-time. Vocational rehabilitation and counselling should become a part of rehabilitation programme for allsubjects who are of working age after lower limb amputation. Better cooperation between professionals, such as rehabilitationteam members, implementing bodies, company doctors and the employers, is necessary.
Keywords: Lower limb amputation, work, rehabilitation
Introduction
Incidence rates of acquired amputations vary greatly
between and within countries. They range from 1.2
per 10 000 women in Japan to 4.4 per 10 000 men in
the Navajo nation in the USA [1]. Amputation itself
is a change in body structure, but has a great in-
fluence on many activities, participation in activities
and quality of life [2 – 10]. The ultimate objective of
rehabilitation is to allow amputees to integrate into
the community as independent and productive
members [11], which also means allowing them to
work. In spite of that, reemployment is not included
in outcome measures that evaluate rehabilitation
outcome after lower limb amputation [12 – 15].
We found 31 studies on the reintegration of lower
limb amputees to work, the problems they have and
the factors that influence their reintegration to work
(Table I). Two are review articles [16,17]. The
oldest was carried out in 1978 [18] and included
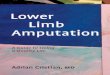
over 100 subjects. The number of these studies has
increased in the past few years (Figure 1).
The studies were performed in 13 different
countries on all five continents (Figure 2), but most
were in the USA, the Netherlands and Canada. Not
all report on inclusion criteria, but when reported the
criteria differ greatly. Seven include only subjects
after traumatic amputation, one includes only sub-
jects amputated due to malignant tumour, and one
includes only patients younger than 21 years at the
time of the amputation. Their results are therefore
very difficult to compare.
Successful return to work
The percentages of subjects who returned to work
successfully differ from study to study and are
difficult to compare. Bruins et al. [19] included only
Correspondence: Helena Burger, Institute for Rehabilitation, Linhartova 51, 1000 Ljubljana, Slovenia. Tel: þ 386 (0)1 47 58 100. Fax: þ 386 (0)1 43 76 589.
E-mail: [email protected]
Disability and Rehabilitation, September 2007; 29(17): 1323 – 1329
ISSN 0963-8288 print/ISSN 1464-5165 online ª 2007 Informa UK Ltd.
DOI: 10.1080/09638280701320797
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
SUN
Y S
tate
Uni
vers
ity o
f N
ew Y
ork
at S
tony
Bro
ok o
n 10
/25/
14Fo
r pe
rson
al u
se o
nly.

Tab
leI.
Stu
die
so
nth
ere
inte
gra
tio
no
flo
wer
lim
bam
pu
tees
tow
ork
.
Au
tho
rC
ou
ntr
yM
eth
od
No
.o
fp
atie
nts
Mea
nag
e(y
ears
)R
eem
plo
ymen
tra
te(%
)A
no
ther
wo
rkR
etir
ed
Tim
eto
retu
rn
tow
ork
Keg
el19
78
[18]
US
AP
ost
al
qu
esti
on
nai
re
13
44
56
0%
of
emp
loya
ble
age
4%
40
%–
Nar
ang
19
84
[2]
Ind
iaIn
terv
iew
50
02
55
9%
,3
.5%
un
able
tow
ork
,
4%
un
emp
loye
d
12
%sa
me
job
,4
7%
oth
erjo
b
––
Mills
tein
19
85
[21
]
Can
ada,
On
tari
o
Post
al
qu
esti
on
nai
re
10
10
35
atth
eti
me
of
amp
uta
tio
n,
49
atst
ud
y
87
%lo
wer
lim
b,
51
%fu
ll
tim
e,5
%p
art
tim
e,8%
un
emp
loye
d,
21
%
retu
rned
toth
eir
pre
amp
.
job
75
%7
%–
Po
hjo
lain
en
19
90
[3]
Fin
lan
dE
xam
inat
ionþ
med
ical
reco
rds
17
56
2O
fp
atie
nts
un
der
65
year
s:
17%
wo
rk,
5%
sick
leav
e,
7%
stu
den
ts
–7
1%
–
Nis
sen
19
92
[4]
US
A,
No
rth
Dak
ota
Tel
eph
on
e
inte
rvie
w
42
68
––
––
Jon
es1
993
[5]
Au
stra
lia
Inte
rvie
wo
r
wri
tten
qu
est
65
/53
at
follo
w-u
p
67
Of
20
atw
ork
ing
age:
3p
art
tim
e,1
stu
dy,
2fu
llti
me,
3d
ied
––
–
Liv
ingst
on
19
94
[30
]
US
A,
Oh
ioM
edic
alre
cord
s4
23
45
0%
wo
rker
sþ
3/5
stu
den
tsye
s,%
?1p
t1
4m
on
ths
Ped
erse
n
19
94
[7]
DK
Inte
rvie
w2
24
4at
stu
dy
10
/15þ
on
est
ud
ent
5/1
00
Do
ugh
erty
19
99
[25
]
US
AM
edic
al
reco
rdsþ
SF
–3
6b
y
po
st
30þ
145
con
tro
l
–7
0%
––
–
Pan
dia
n1
99
9
[16]
US
AR
evie
war
ticl
e
Pez
zin
20
00
[10]
US
AM
edic
al
reco
rdsþ
tele
ph
on
e
inte
rvie
w
78
/14
63
2.9
57
.7%
Nu
mb
eru
nkn
ow
n,
30
%d
ecre
ase
in
the
leve
lo
f
ph
ysic
al
req
uir
emen
t
Sch
op
pen
20
01
[20
]
NL
PO
wo
rksh
op
65
24
4.5
66
%o
fw
ork
ing
bef
ore
amp
uta
tio
n,
amo
ng
them
34%
par
tti
me
54
.6–
2.3
Sch
op
pen
20
01
[32
]
NL
Post
al
qu
esti
on
nai
re
32
24
67
9%
(25
4)
45
.9–
–
Ide
20
02
[37
]Ja
pan
Post
al
qu
esti
on
nai
re
10
13
7fu
ll,
3p
art,
self
12
,
un
kn
ow
n5
9–
retu
rnto
wo
rk5
6.6
%
––
–
(con
tinued
)
1324 H. Burger & C. Marin�cek
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
SUN
Y S
tate
Uni
vers
ity o
f N
ew Y
ork
at S
tony
Bro
ok o
n 10
/25/
14Fo
r pe
rson
al u
se o
nly.

Tab
leI.
(Con
tinued
).
Au
tho
rC
ou
ntr
yM
eth
od
No
.o
fp
atie
nts
Mea
nag
e(y
ears
)R
eem
plo
ymen
tra
te(%
)A
no
ther
wo
rkR
etir
ed
Tim
eto
retu
rn
tow
ork
Sch
op
pen
20
02
[34
]
NL
2p
ost
al
qu
esti
on
nai
res
14
4þ
14
4
con
tro
l
43
10
0%
––
–
Wh
yte
20
02
[22]
Sco
tlan
dP
ost
al
qu
esti
on
nai
re
31
54
3.8
43
.5%
No
nu
mb
ers,
gra
ph
inth
est
ud
y
––
Bru
ins
20
03
[19]
NL
Inte
rvie
w3
24
2.6
10
0%
–it
was
ad
eman
do
fa
stu
dy
for
incl
usi
on
,4
1%
par
t-ti
me
50
%o
ther
jobþ
31
%sa
me
job
,
oth
erw
ork
01
1.5
mo
nth
s,4
12
mo
nth
s–
41
%
Fer
nan
dez
20
03
[29
]
Sp
ain
P&
Ore
cord
s2
81
12
.6at
amp
uta
tio
n,
43
atst
ud
y
Mo
rere
tire
dan
d
un
emp
loye
d,
less
stu
den
tsth
anin
po
pu
lati
on
,m
ore
LL
reti
red
and
less
stu
den
ts
than
UL
–M
en30
.7,
Wo
men
14
.5
–
Fer
rap
ie2
00
3
[23]
Fra
nce
Med
ical
reco
rds
12
55
10
0%
––
–
Fis
her
20
03
[26]
UK
Inte
rvie
w1
00
47
66
%w
ork
,1
7%
no
t,4
%
retr
ain
ing,
14
%re
tire
d
43
%1
4%
17
%in
2ye
ars,
10
%in
1ye
ar
Mez
gh
ani-
Mas
mo
ud
i
20
04
[28
]
Tu
nis
iaH
eter
o
qu
esti
on
nai
re
85
48
35
ou
to
f6
0(5
8.3
3%
)12
ou
to
f3
5(3
4.5
%)
25
–
Wal
d2
00
4
[17]
Can
ada
Rev
iew
arti
cle
Sm
ith
20
05
[27]
US
AF
ollo
w-u
p3
2–
66
.7%
un
ilat
eral
amp
.,
21.4
%b
ilat
eral
amp
uta
tio
n
––
–
Heb
ert
20
06
[36]
Can
ada,
Alb
erta
Med
ical
reco
rds
88
34
22
.7%þ
19
.3%
fit
for
wo
rk16
ou
to
f5
1(3
1.4
%)
1ye
ar
Mac
Ken
zie
20
06
[35
]
US
AF
ollo
wu
p4
23
––
––
Est
imat
eat
12
mo
nth
42%
Ro
tter
20
06
[33]
Ch
ile
Med
ical
reco
rds
10
03
66
0%
retu
rnto
wo
rkin
1
year
1ye
ar
Return to work after lower limb amputation 1325
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
SUN
Y S
tate
Uni
vers
ity o
f N
ew Y
ork
at S
tony
Bro
ok o
n 10
/25/
14Fo
r pe
rson
al u
se o
nly.

subjects who returned to work, Kegel et al. [18],
Nissen and Newman [4] and Jones et al. [5] all
report the rate of employable age, Schoppen et al.
[20] included those who also worked before amputa-
tion, while Pojolainen et al. [3] included only
subjects younger than 65. The rate of employment
or unemployment depends on the definition selected
and varies in one single study from 71.5 to 88.4%
depending on the chosen definition [21]. The
reemployment rate ranges from 43.5% [22] to
100% for subjects amputated due to a tumour
[23]. Most reported it at around 66% or two-thirds
[20,24 – 26]. Smith et al, [27] reported it at 66.7%
for unilateral but only at 16% for bilateral amputees.
Mezghani-Masmoudi et al. [28] report the reem-
ployment rate at 58.3%. Additionally, they included
35.5% of subjects in a vocational rehabilitation pro-
gramme. They do not report how many were re-
employed later.
Only one study compares the employment rate of
amputees with the employment rate in the general
population [29]. The author found that among male
amputees there was a greater proportion of retired
and unemployed people and a smaller proportion of
students than in the general population of Asturias in
Spain. Male amputees also had lower educational
levels than the general population, whereas in
women no such differences were found.
Reemployment rate alone does not give us enough
information. Many subjects after amputation work
only part-time. The percentage of subjects who
worked part-time ranged from 34% [20] to 50%
[5,30]. Both studies with the highest percentage of
subjects working part-time only were carried out on a
small number (three out of six) [5]. The study by
Bruins et al. [19] reports 4% working part-time.
Two studies report the percentage of subjects who
were unable to work because of amputation. Kegel
et al. [18] found it to be 8% and Narang et al. [2]
only 3.5%. One-quarter of employed amputees
experienced periods of unemployment lasting more
than 6 months following amputation [21].
Type of work
The percentage of subjects who returned to the same
work also differs in various studies. It mainly
depends on the type of work the subjects did before
amputation and the level of amputation. Narang
et al. [2] report that only 12% of amputees returned
to the same job. Over half the subjects included in
their study had been soldiers before and had to
change their profession. In the USA, only 2.3% of
soldiers remained on active duty after amputation;
97% left the service [31]. However, leaving the
service did not mean that they were not working.
Curley et al. [24] report that 69% of Vietnam
veterans were employed and Dougherty [25] that
even 70% of bilateral transfemoral amputees from
the Vietnam war were employed.
Not only veterans but also civilians engaged in
physical labour before amputation have to seek
alternative jobs. The percentage of subjects who
retained the same occupation after amputation
ranges from 22 to 67% [7,18,19,21,26,32]. The
lowest percentage is reported by Kegel et al. [18], but
only 60% of his subjects were of employable age; the
highest percentage is reported by Schoppen et al.
[32] who calculated it only for subjects working at
the time of amputation. Subjects who changed their
occupation were more successfully reintegrated
(90%) than those who did not change (68%) [32].
Subjects with a very high physical workload who did
not change their job successfully returned to their
work in only 58% of cases. Some subjects changed
their jobs but stayed in the same workplace; others
changed their workplace as well [19,26].
Most subjects who kept the same job after
amputation had physically undemanding work
[19] and lower level of amputation, mainly at the
Figure 1. Number of articles on work reintegration of lower-limb
amputees in different years/decades.
Figure 2. Number of articles from different countries.
1326 H. Burger & C. Marin�cek
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
SUN
Y S
tate
Uni
vers
ity o
f N
ew Y
ork
at S
tony
Bro
ok o
n 10
/25/
14Fo
r pe
rson
al u
se o
nly.

trans-tibial level [18]. Post-amputation jobs were
generally more complex with a requirement for a
higher level of general educational development and
were physically less demanding [10,20,21,22]. While
only 1% were employed in a sedentary job prior to
injury, 16% secured a sedentary job after amputation
[21], and only 21% returned to their pre-amputation
job. Values measuring how demanding the job was
indicate a 30% decrease in the level of physical
requirement of jobs relative to the previous job [10].
The mean decrease in physical workload was 2.4 on
the VAS scale [32].
Time of return to work
The time of return to work is mentioned in only four
studies [19,20,30,33]. It ranges from 9 months for
subjects after trans-tibial amputation [19] up to 2.3
years in the study by Schoppen et al. [20] for all
subjects, independent of the amputation level. The
most frequent reasons for delay were stump pro-
blems and problems in wound healing (85%),
problems with the job reintegration process (46%)
and mental problems (23%) [19]. Fifty-five per cent
of amputees stopped working in the first 2 years after
amputation. Seventy-eight per cent of them of them
said that amputation-related factors played a role in
their decision [20].
Factors influencing return to work
Factors influencing return to work can be divided
into general factors, such as age, gender and educa-
tional level; factors related to impairments and dis-
abilities due to amputation [32]; and factors related
to work and policies.
General factors
Demographic factors such as sex and age at the time
of amputation [7,22,32,34,35] and being white
[10,35] were found to have an effect on employment
[21,20,26]. While Millstein et al. [21] report that
women had 2.5 times greater unemployment rate
than men, and older subjects were less successful in
their return to work, Schoppen et al. [20] found that
fewer older men were employed but that age had no
influence on the employment of women. Whyte and
Carroll [22] also found greater unemployment rate
in women than in men.
The unemployment rate for subjects under
45 years was 22% compared to 48% for those over
45 years of age [21] Only one out of five subjects who
lost their job after amputation was younger that 45
years [7]. Subjects who were older at the time of
amputation were more unsatisfied with reintegration
into work activities [4].
Subjects with lower pre-injury educational level
had lower reemployment rates and more of them
had to change their job [30,35]. MacKenzie et al.
[35] found non-smokers and people with higher self-
efficacy had a higher return-to-work rate.
Factors related to impairments and disabilities
due to amputation
Factors related to impairments and disabilities
due to amputation are: amputation level [5,25,
30,36], multiple amputations [21,30], comorbidity
[10,32], reason for amputation [32], persistent stump
problems [21,30], especially stump and phantom
pain [21,22,32,37], the time from the injury to
obtaining a permanent prosthesis [30], wearing
comfort of the prosthesis [32], walking distance and
restrictions in mobility [26,32]. They had a negative
impact on reemployment. Twenty-eight per cent
experienced problems finding work because of
amputation [20].
Higher amputation levels decrease reemployment
rate. Jones et al. [5] in a study on a very small
number of subjects found that two out of the three
working full-time had trans-tibial amputation and
one trans-femoral. On a slightly higher number of
subjects, Livingston et al. [30] found that none
returned to work after trans-femoral amputation,
whereas 48% of subjects did return after trans-tibial
amputation. Dougherty [25] included only bilateral
trans-femoral amputees from the Vietnam war.
Sixteen (70%) were or had been employed outside
the home even though the Veterans Administration
provides adequate compensation to support their
lifestyle [25]. Surprisingly, Fisher et al. [26] did not
find that the level of amputation and the cause of
amputation correlated with the score on the employ-
ment questionnaire.
Livingston et al. [30] found that inpatient rehabi-
litation had a negative influence on return to work on
a small number of subjects. In his study, only three
out of 14 patients who had inpatient rehabilitation
returned to work, in contrast to 14 out of 25 who had
outpatient therapy. He does not describe the criteria
for the decision on why someone was included into
in- or outpatient rehabilitation, which may influence
the result. On almost twice the number of subjects,
Pezzin et al. [10] reported that inpatient rehabilita-
tion improved the health and vocational prospects of
persons with trauma-related amputations. With
calculations he assumed that an additional 10 nights
of inpatient rehabilitation indicated a 14% decrease
in the number of amputees working fewer hours.
Only two out of 33 patients were referred to voca-
tional rehabilitation [30]. Vocational services posi-
tively affect return to work [21], but are not
developed or part of a rehabilitation programme in
Return to work after lower limb amputation 1327
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
SUN
Y S
tate
Uni
vers
ity o
f N
ew Y
ork
at S
tony
Bro
ok o
n 10
/25/
14Fo
r pe
rson
al u
se o
nly.

all countries. For example, they are largely lacking in
the UK [26].
Reemployment rate is lower for subjects who
sustained a work-related amputation [30].
Work and policy-related factors
Other factors that have been found to influence
return to work are salary [30], higher job involve-
ment [35], good support from the implementing
body and the employer [19,20] and social support
network [30].
Individuals who received social benefits and had a
low pre-injury income in a job which did not include
medical benefits less often returned to work [30].
More returned to work if they had a higher gross
annual income [36]. Almost one-third felt that they
had fewer possibilities for job promotion [20]. In the
study by Bruins et al. [19], 34% had fewer promo-
tion possibilities due to physical limitations and
because employers were afraid of sick leave in the
future. Most patients who returned to work stated
that their current salary was less than that before their
injury [21,30].
Forty-four per cent reported that job security was
adversely affected by amputation [21]. Only a small
number of amputees moved up on the occupational
classification scale, most moving down by one to
three levels [22]. Usually this resulted in change from
skilled to semi- or unskilled occupations [22].
In the study by Bruins et al. [19], subjects found
self-motivation as the essential factor for successful
job reintegration; good support from the implement-
ing body and the employer was also important.
Insufficient support from the employer and the
implementing body which supervises job reintegra-
tion were the most mentioned obstacles to job
reintegration [19]. Twenty-five per cent of subjects
did not experience any problems with work reinte-
gration at all. Eight out of 14 subjects were
unsatisfied with reintegration into work activities
[4]. Most of these subjects had amputations at the
end of their careers; their average age at the time of
amputation was 49 years (SD 4) [4].
Adjustments to the workplace are important for
enabling people to continue their work after amputa-
tion. Forty-three per cent of subjects working before
and after amputation mentioned modifications of
their job as a factor in continuing to work [20]. The
adjustments are divided into four categories: changes
in working time, getting aids (31%), changes in
workload (31%), and other tasks or extra training
[20]. When adjustments were necessary, most of the
subjects took the initiative for them by themselves;
they were seldom initiated by the rehabilitation team
[19]. Twenty-seven per cent of amputees said that
they were partially dependent on others [20] but
most colleagues and supervisors gave them sufficient
consideration.
Regarding older amputees, reduction of physical
workload and adaptations of workplace will be of
extra importance.
Seventy per cent of working subjects judged their
work life as good and 30% as unsatisfactory after
lower limb amputation [34]. Unsatisfied subjects had
more comorbidities, lower mobility level and wished
for more modifications to their workplace [34]. The
most important motives for returning to work were
the value of their work as a form of spending the day
and social contacts with colleagues and others [19].
Conclusion
Subjects have problems with returning to work after
lower limb amputation. Many have to change their
work and/or work only part-time. Some also need
modifications to their workplace. Their return to
work depends on general factors, such as age at the
time of amputation, sex and education, factors
related to impairments and disabilities due to
amputation and factors related to work and policies.
Vocational rehabilitation and counselling should
become a part of rehabilitation programme for all
subjects after lower limb amputation who are of
working age. Better cooperation between profes-
sionals, such as rehabilitation team members, im-
plementing bodies, company doctors and the
employers, is necessary.
There is no study based on the ICF regarding the
topics mentioned in the paper.
References
1. Ephraim PL, Dillingham R, Sector M, Pezzin LE,
MacKenzie EJ. Epidemiology of limb loss and congenital
limb deficiency: a review of the literature. Arch Phys Med
Rehabil 2003;84:747 – 761.
2. Narang IC, Mathur BP, Singh P, Jape VS. Functional
capabilities of lower limb amputees. Prosthet Orthot Int
1984;8:43 – 51.
3. Pohjolainen T, Alaranta H, Karkkainen M. Prosthetic use and
functional and social outcome following major lower limb
amputation. Prosthet Orthot Int 1990;14:75 – 79.
4. Nissen SJ, Newman WP. Factors influencing reintegration to
normal living after amputation. Arch Phys Med Rehabil
1992;73:548 – 551.
5. Jones L, Hall LM, Schuld W. Ability or disability? A study of
the functional outcome of 65 consecutive lower limb
amputees treated at the Royal South Sydney Hospital in
1988 – 1989. Disabil Rehabil 1993;15:184 – 188.
6. Kejlaa GH. Consumer concerns and the functional value of
prostheses to upper limb amputees. Prosthet Orthot Int
1993;17:57 – 163.
7. Pedersen P, Damholt V. Rehabilitation after amputation
following lower limb fracture. J Trauma 1994;36:195 – 197.
8. Burger H, Marin�cek C, Isakov E. Mobility of persons after
traumatic lower limb amputation. Disabil Rehabil 1997;19:
272 – 277.
1328 H. Burger & C. Marin�cek
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
SUN
Y S
tate
Uni
vers
ity o
f N
ew Y
ork
at S
tony
Bro
ok o
n 10
/25/
14Fo
r pe
rson
al u
se o
nly.

9. Burger H, Marin�cek C. The life style of young persons after
lower limb amputation caused by injury. Prosthet Orthot Int
1997;21:35 – 39.
10. Pezzin LE, Dillingham TR, MacKenzie EJ. Rehabilitation and
the long-term outcomes of persons with trauma-related
amputation. Arch Phys Med Rehabil 2000;81:292 – 300.
11. McColl MA, Davies D, Carlson P, Johnston J, Minnes P. The
community integration measure: development and prelimin-
ary validation. Arch Phys Med Rehabil 2001;82:429 – 434.
12. Grise MCL, Gauthier-Gagnon C, Myartineau GG. Prosthetic
profile of people with lower extremity amputation: conception
and design of a follow-up questionnaire. Arch Phys Med
Rehabil 1993;74:862 – 870.
13. Hougton A, Allen A, Luff R. Rehabiltation after lower limb
amputation: A comparative study of above-knee, through knee
and Gritti-Stokes amputations. Br J Surg 1989;76:622 – 624.
14. Miller WC, Deathe AB, Speechley M. Lower extremity
prosthetic mobility: a comparison of 3 self-reported scales.
Arch Phys Med Rehabil 2001;82:1432 – 1440.
15. Gailey RS, Roach KE, Applegate EB, Cho B, Cunniffe B,
Licht S, Maguire M, Nash M. The Amputee Mobility
Predictor: an instrument to assess determinants of the
lower-limb amputee’s ability to ambulate. Arch Phys Med
Rehabil 2002;83:613 – 627.
16. Pandian G, Kowalske K. Daily functioning of patients with an
amputated lower extremity. Clin Orthopaed Rel Res 1999;
361:91 – 97.
17. Wald J, Alvaro R. Psychological factors in work-related
amputation: considerations for rehabilitation counselors.
J Rehabil 2004;70:6 – 15.
18. Kegel B, Carpenter ML, Burgess EM. Functional capabilities
of lower extremity amputees. Arch Phys Med Rehabil
1978;59:109 – 120.
19. Bruins M, Geertzen JH, Groothoff JW, Schoppen T.
Vocational reintegration after a lower limb amputation: a
qualitative study. Prosthet Orthot Int 2003;27:4 – 10.
20. Schoppen T, Boonstra A, Groothoff JW, de Vries J,
Goeken LNH, Eisma WH. Employment status, job char-
acteristics, and work-related health experience of people with
a lower limb amputation in the Netherlands. Arch Phys Med
Rehabil 2001;82:239 – 245.
21. Whyte AS, Carroll LJ. A preliminary examination of the
relationship between employment, pain and disability in an
amputee population. Disabil Rehabil 2002;24:462 – 470.
22. Ferrapie AL, Brunel P, Besse W, Altermatt E, Bontoux L,
Richard I. Lower limb proximal amputation for a tumor: a
retrospective study of 12 patients. Prosthet Orthot Int 2003;
27:179 – 185.
23. Curley MD, Walsh JM, Triplett RG. Some adjustment
indices of oral – maxillofacial war casualties, limb amputees,
and noninjured veterans. Mil Med 1982;147:572 – 574.
24. Dougherty CP. Long-term follow-up study of bilateral above-
the-knee amputees from the Vietnam war. J Bone Joint Surg
1999;81-A:1384 – 1390.
25. Fisher K, Hanspal RS, Marks L. Return to work after lower
limb amputation. Int J Rehabil Res 2003;26:51 – 56.
26. Smith JJ, Agel D, Swiontkowski MF, Castillo R, Mackenzie E,
Kellam JM. Functional outcome of bilateral limb threatening
lower extremity injuries at two years postinjury. J Orthopaed
Trauma 2005;19:249 – 253.
27. Mezghani-Masmoudi M, Guermazi M, Feki H, Ennaouai A,
Dammak J, Elluch MH. Facteurs lies a l’avenir fonctionnel et
professionnel des amputes des members inferieurs appareilles.
Ann Readapt Med Phys 2004;47:114 – 118.
28. Fernandez A, Revilla C, Su IT, Garcia M. Social reintegration
of juvenile amputees: comparison with a general population.
Prosthet Orthot Int 1993;27:11 – 16.
29. Livingston DH, Keenan D, Kim D, Elcavage J,
Malagnoni MA. Extent of disability following traumatic
extremity amputation. J Trauma 1994;37:495 – 499.
30. Millstein S, Bain D, Hunter GA. A review of employment
patterns of industrial amputees – factors influencing rehabili-
tation. Prosthet Orthot Int 1985;9:69 – 78.
31. Kishbaugh D, Dillingham TR, Howard RS, Sinnott MW,
Belandres PV. Amputee soldiers and their return to active
duty. Mil Med 1995;160:82 – 84.
32. Schoppen T, Boonstra A, Groothoff JW, van Sonderen E,
Goeken LNH, Eisma WH. Factors related to successful job
reintegration of people with a lower limb amputation. Arch
Phys Med Rehabil 2001;82:1425 – 1431.
33. Rotter K, Sanhueza R, Robles K, Godoy M. A descriptive
study of traumatic lower limb amputees from the hospital del
Trabajador: clinical evolution from the accident until rehabi-
litation discharge. Prosthet Orthot Int 2006;30:81 – 86.
34. Schoppen T, Boonstra A, Groothoff JW, de Vries J,
Goeken LNH, Eisma WH. Job satisfaction and health
experience of people with a lower-limb amputation in
comparison with healthy colleagues. Arch Phys Med Rehabil
2002;83:628 – 634.
35. MacKenzie EJ, Bosse MJ, Kellam JF, Pollak AN, Webb LX,
Swiontkowski MF, Smith DG, et al. Early predictors of long-
term work disability after major limb trauma. J Trauma
2006;61:688 – 694.
36. Hebert JS, Ashworth NL. Predictors of return to work
following traumatic work-related lower extremity amputation.
Disabil Rehabil 2006;30:613 – 618.
37. Ide M, Obayashi T, Toyonaga T. Association of pain with
employment status and satisfaction among amputees in Japan.
Arch Phys Med Rehabil 2002:83;1394 – 1398.
Return to work after lower limb amputation 1329
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
SUN
Y S
tate
Uni
vers
ity o
f N
ew Y
ork
at S
tony
Bro
ok o
n 10
/25/
14Fo
r pe
rson
al u
se o
nly.