Embed Size (px)
Citation preview
Reuma, atherosclerose & anti-inflammatie
Prof.dr. Mike T. Nurmohamed, reumatoloog
Reade & VU Medisch Centrum
Reumatoïde artritis & Atherosclerose



Mortaliteit en doodsoorzaken bij RA
• Mortaliteit
• Verhoogde totale mortaliteit
• Verkorte levensverwachting: 4 - 7 jaar
• Zowel bij mannen als vrouwen
• Meeste studies: geen afname in laatste decaden
• Doodsoorzaken
• Infecties
• Lymfoproliferatieve ziekten
• Gastro-intestinale oorzaken
• Cardiovasculaire ziekten
• Belangrijkste doodsoorzaak
• RA-patiënt: verdubbelde kans op cardiovasculaire sterfte
CARRÉ-onderzoek*
• Prospectief
• Prevalente & incidente HVZ, risicofactoren voor HVZ
• RA-patiënten
• 1987 ACR criteria
• Leeftijd: 50 – 75 jaar
• Ziekteduur tot 12 jaar
• N = 353
• Gestart in 2001
• Follow-up: tenminste 18 jaar
*van Halm et al, Ann Rheum Dis 2009
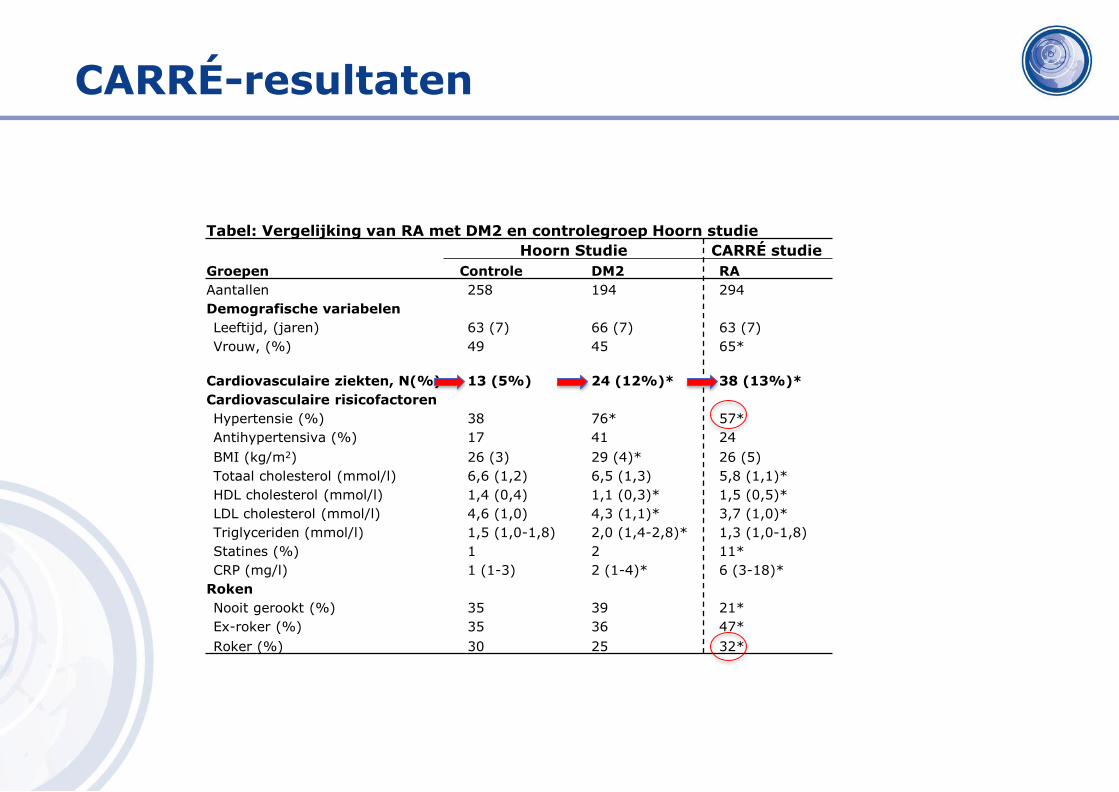
Tabel: Vergelijking van RA met DM2 en controlegroep Hoorn studie
Hoorn Studie CARRÉ studie
Groepen Controle DM2 RA
Aantallen 258 194 294
Demografische variabelen
Leeftijd, (jaren) 63 (7) 66 (7) 63 (7)
Vrouw, (%) 49 45 65*
Cardiovasculaire ziekten, N(%) 13 (5%) 24 (12%)* 38 (13%)*
Cardiovasculaire risicofactoren
Hypertensie (%) 38 76* 57*
Antihypertensiva (%) 17 41 24
BMI (kg/m2) 26 (3) 29 (4)* 26 (5)
Totaal cholesterol (mmol/l) 6,6 (1,2) 6,5 (1,3) 5,8 (1,1)*
HDL cholesterol (mmol/l) 1,4 (0,4) 1,1 (0,3)* 1,5 (0,5)*
LDL cholesterol (mmol/l) 4,6 (1,0) 4,3 (1,1)* 3,7 (1,0)*
Triglyceriden (mmol/l) 1,5 (1,0-1,8) 2,0 (1,4-2,8)* 1,3 (1,0-1,8)
Statines (%) 1 2 11*
CRP (mg/l) 1 (1-3) 2 (1-4)* 6 (3-18)*
Roken
Nooit gerookt (%) 35 39 21*
Ex-roker (%) 35 36 47*
Roker (%) 30 25 32*
CARRÉ-resultaten
* Peters et al. Arthritis Care Res 2009 ; NTVG 2010
CARRÉ-studie - Incidentie
• RA
• 3,3 % per jaar (95% BI: 2,7 – 3,9)
• Algemene populatie
• 1,5 % per jaar (95% BI: 1,2 – 1,8)
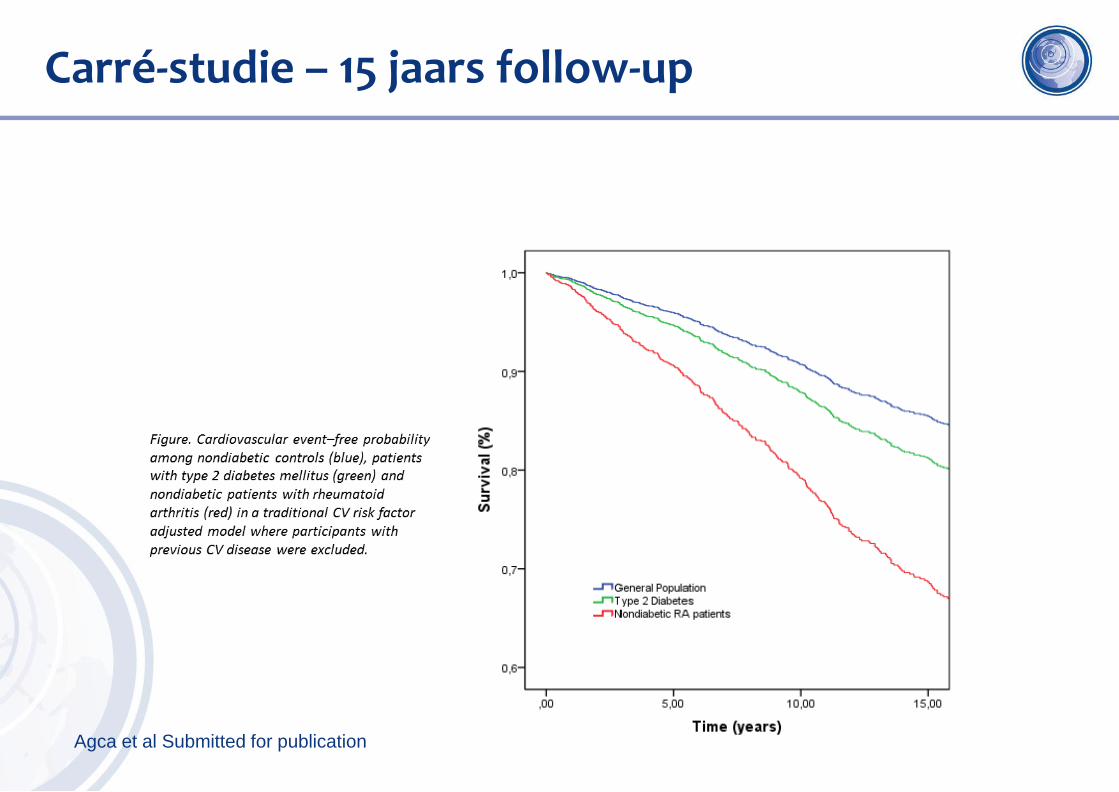
Carré-studie – 15 jaars follow-up
Agca et al Submitted for publication
* van Halm et al. Ann Rheum Dis 2009, **Peters et al. Arthritis Care Res 2009
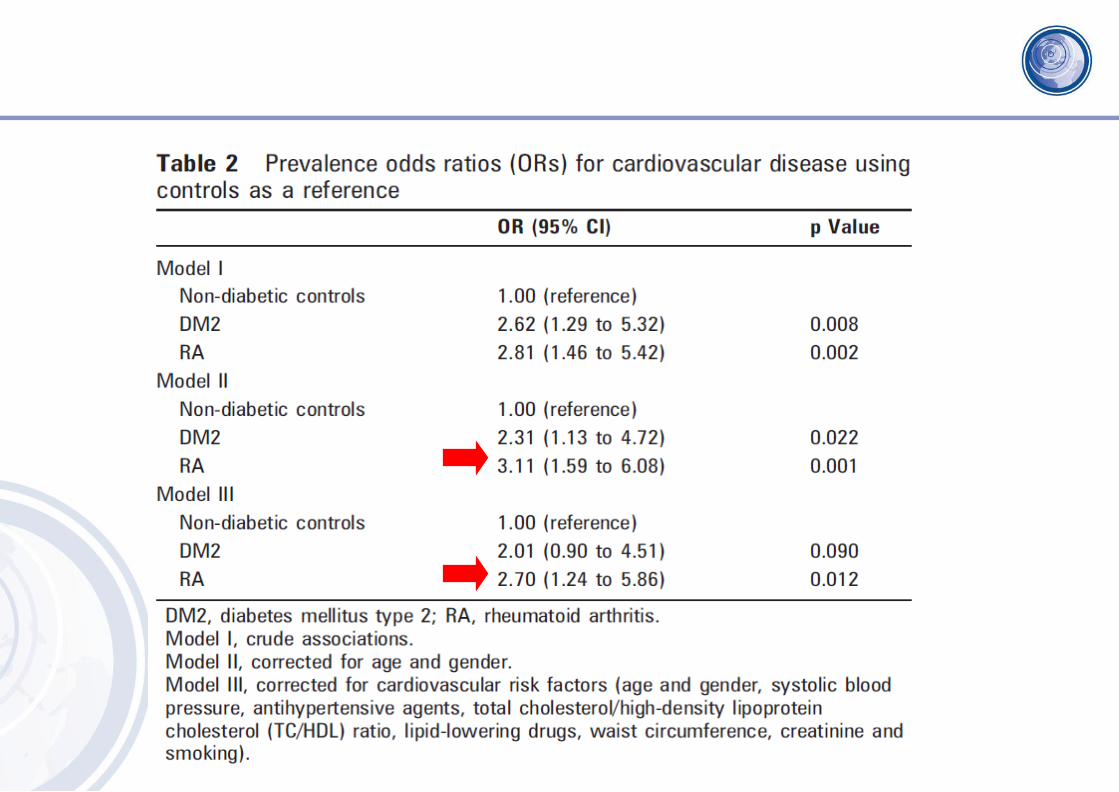
Risico op hart- en vaatziekten bij RA
• Toegenomen bij RA
• CARRÉ-onderzoek*,**
• Verdubbeld t.o.v. de algemene bevolking
• Vergelijkbaar met type 2 diabetes (suikerziekte)
• Maar deels verklaard door risicofactoren voor hart- en vaatziekten
RA = onafhankelijke risicofactor voor HVZ
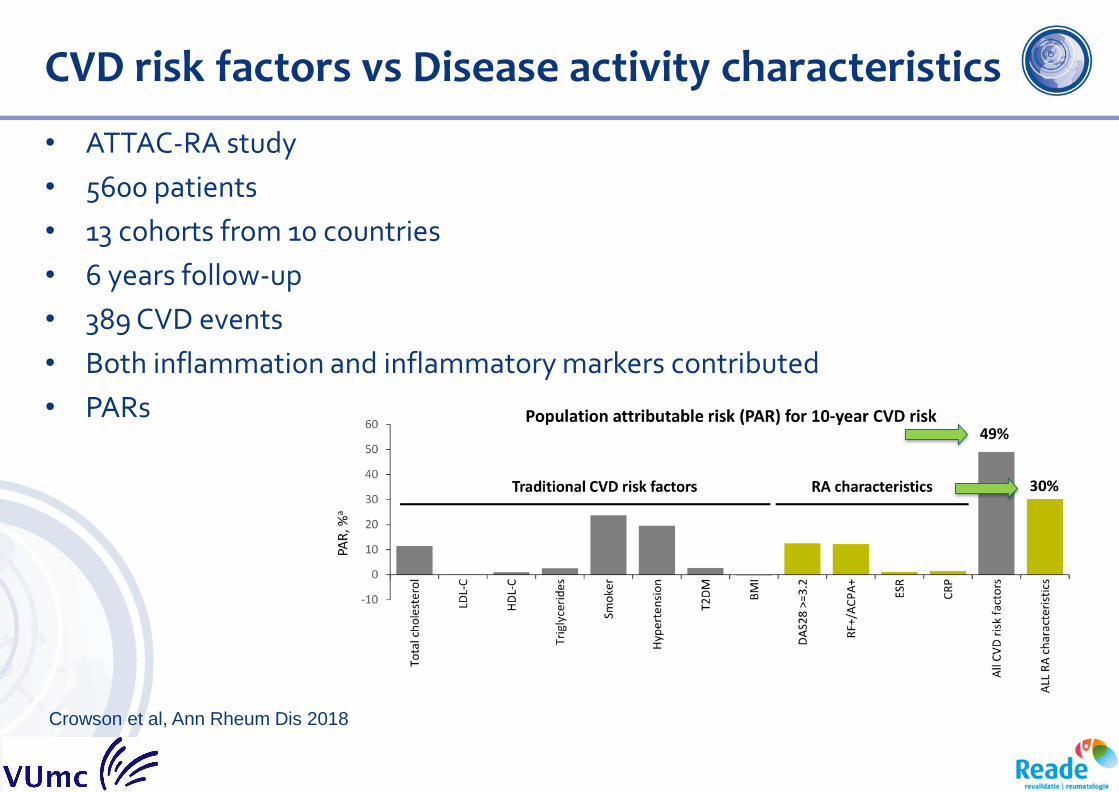
CVD risk factors vs Disease activity characteristics
• ATTAC-RA study
• 5600 patients
• 13 cohorts from 10 countries
• 6 years follow-up
• 389 CVD events
• Both inflammation and inflammatory markers contributed
• PARs
Crowson et al, Ann Rheum Dis 2018
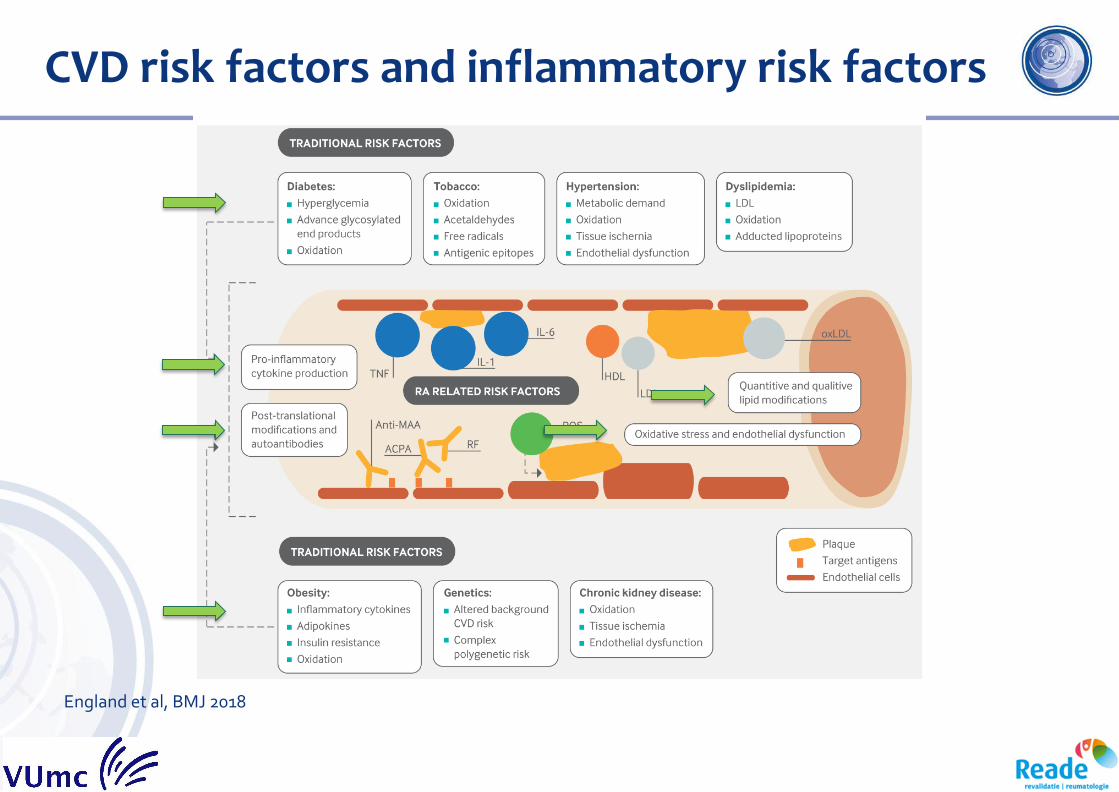
CVD risk factors and inflammatory risk factors
England et al, BMJ 2018
Cardiovasculair risicomanagement
• Cardiovasculair risicoprofiel
• Bloeddruk, lipidenprofiel, etc
• Bepaling van het 10-jaars risico op cardiovasculaire ziekten
• Framingham en SCORE risicofuncties
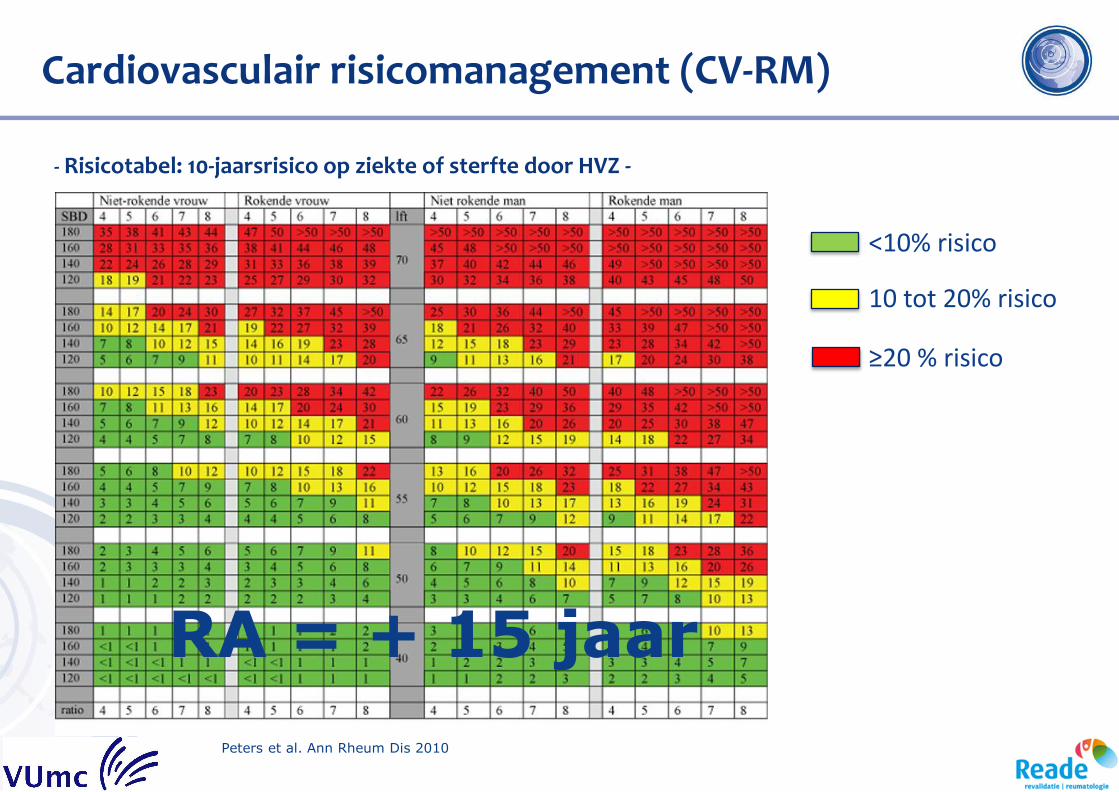
Cardiovasculair risicomanagement (CV-RM)
- Risicotabel: 10-jaarsrisico op ziekte of sterfte door HVZ -
Peters et al. Ann Rheum Dis 2010
RA = + 15 jaar
<10% risico
10 tot 20% risico
≥20 % risico
Anti-inflammatie & Atherosclerose
Methotrexate & CV-events
Anatol J Cardiol 2016
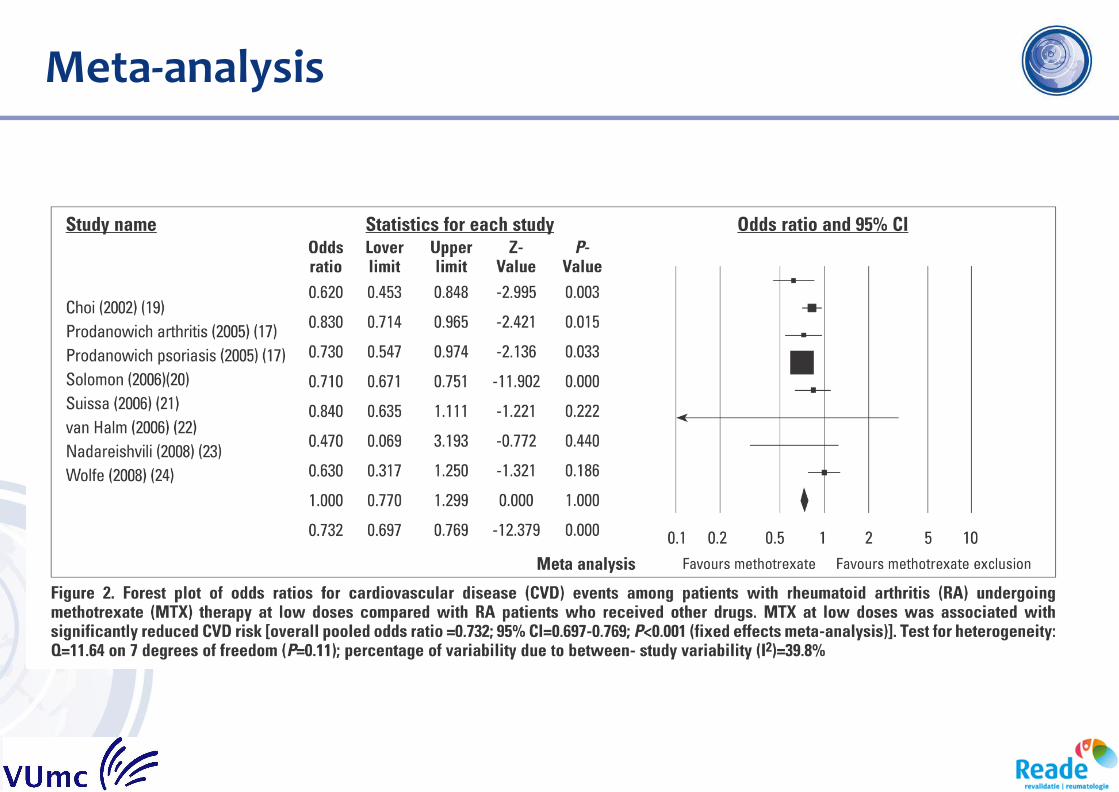
Meta-analysis
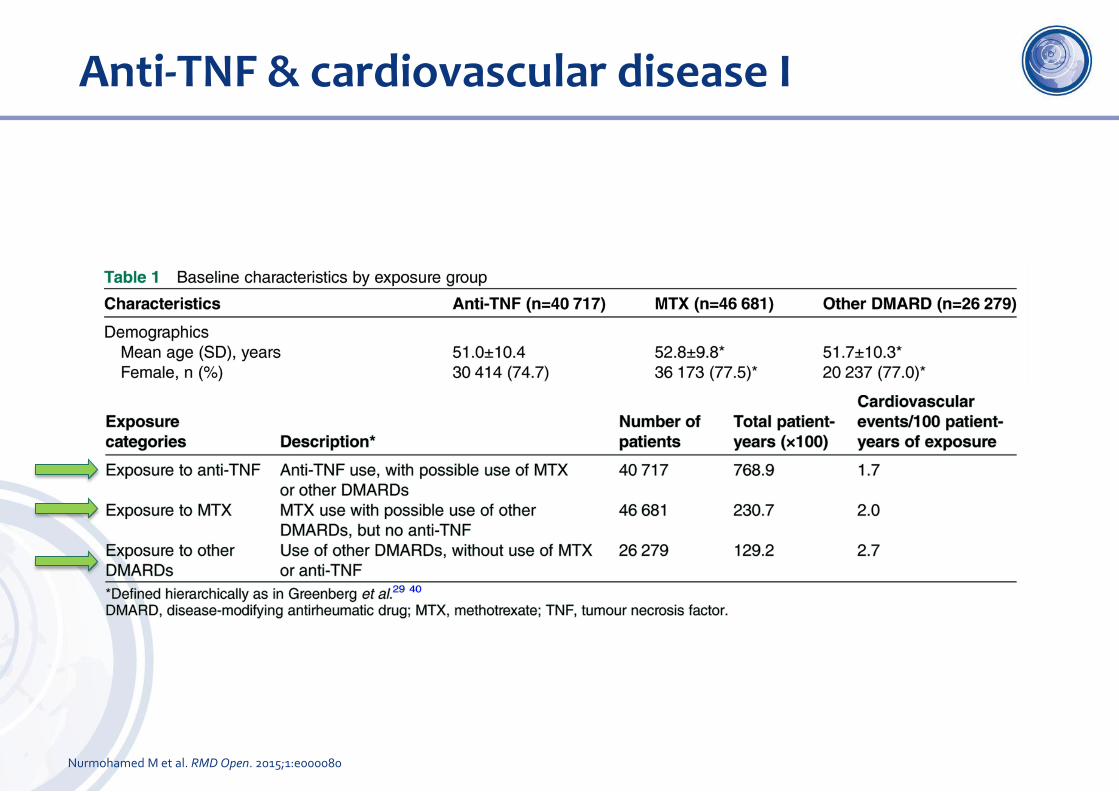
Anti-TNF & cardiovascular disease I
Nurmohamed M et al. RMD Open. 2015;1:e000080
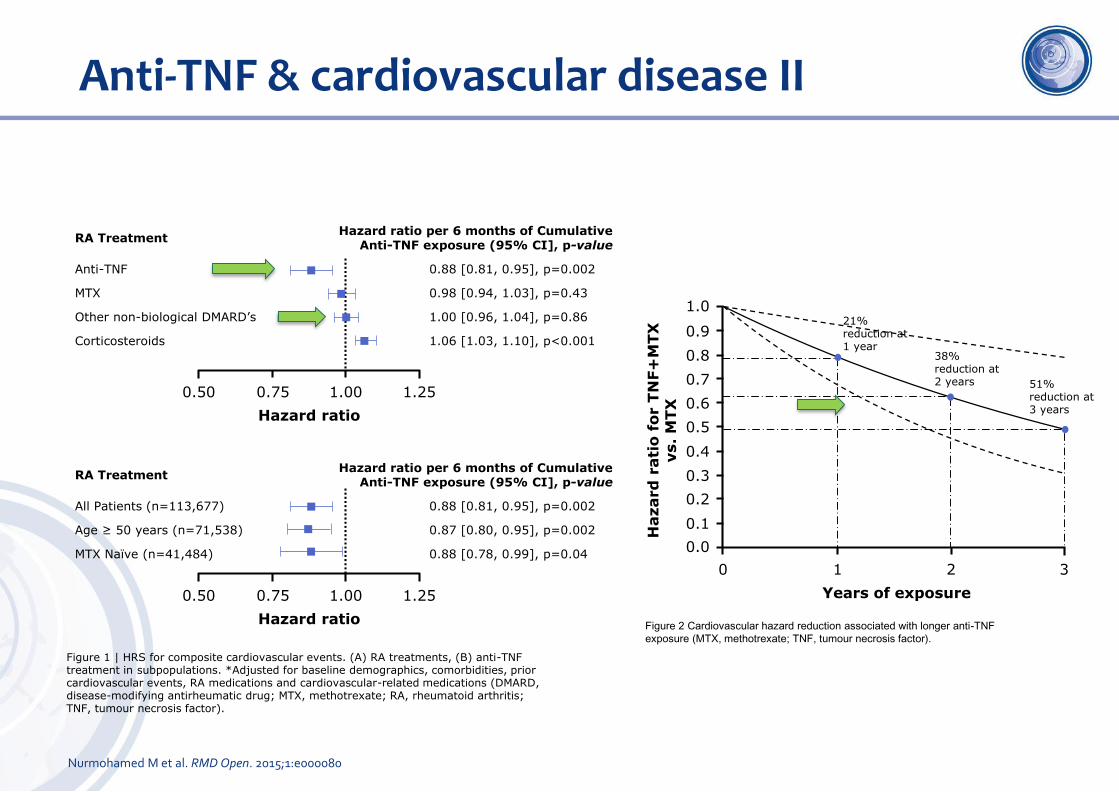
RA TreatmentHazard ratio per 6 months of Cumulative
Anti-TNF exposure (95% CI], p-value
Anti-TNF 0.88 [0.81, 0.95], p=0.002
MTX 0.98 [0.94, 1.03], p=0.43
Other non-biological DMARD’s 1.00 [0.96, 1.04], p=0.86
Corticosteroids 1.06 [1.03, 1.10], p<0.001
Anti-TNF & cardiovascular disease II
1.00
Hazard ratio
0.750.50 1.25
RA TreatmentHazard ratio per 6 months of Cumulative
Anti-TNF exposure (95% CI], p-value
All Patients (n=113,677) 0.88 [0.81, 0.95], p=0.002
Age ≥ 50 years (n=71,538) 0.87 [0.80, 0.95], p=0.002
MTX Naïve (n=41,484) 0.88 [0.78, 0.99], p=0.04
1.00
Hazard ratio
0.750.50 1.25
Figure 1 | HRS for composite cardiovascular events. (A) RA treatments, (B) anti-TNF treatment in subpopulations. *Adjusted for baseline demographics, comorbidities, prior cardiovascular events, RA medications and cardiovascular-related medications (DMARD, disease-modifying antirheumatic drug; MTX, methotrexate; RA, rheumatoid arthritis; TNF, tumour necrosis factor).
Years of exposure
1 2 30
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
Hazard
rati
o f
or T
NF+
MTX
vs.
MTX
21% reduction at 1 year
38% reduction at 2 years 51%
reduction at 3 years
Figure 2 Cardiovascular hazard reduction associated with longer anti-TNF
exposure (MTX, methotrexate; TNF, tumour necrosis factor).
Nurmohamed M et al. RMD Open. 2015;1:e000080
Ridker et al NEJM 10 nov 2018, online
Cardiovascular inflammation reduction trial (CIRT)
• RCT
• Patiënten
• Eerder MI of meervatslijden
• + DM of metabool syndroom
• MTX 15 – 20 mg vs placebo
• Sample Size
• MTX 23% minder MACE
• 530 MACEs
• 7000 ptn
• 1 dd 1 mg foliumzuur
• Uitkomst
• Samengesteld eindpunt
• Niet fatal MI of stroke of cardiovasculaire dood
• Op 13 maart 2018 gestopt….
PM Ridker et al. N Engl J Med 2018. DOI: 10.1056/NEJMoa1809798
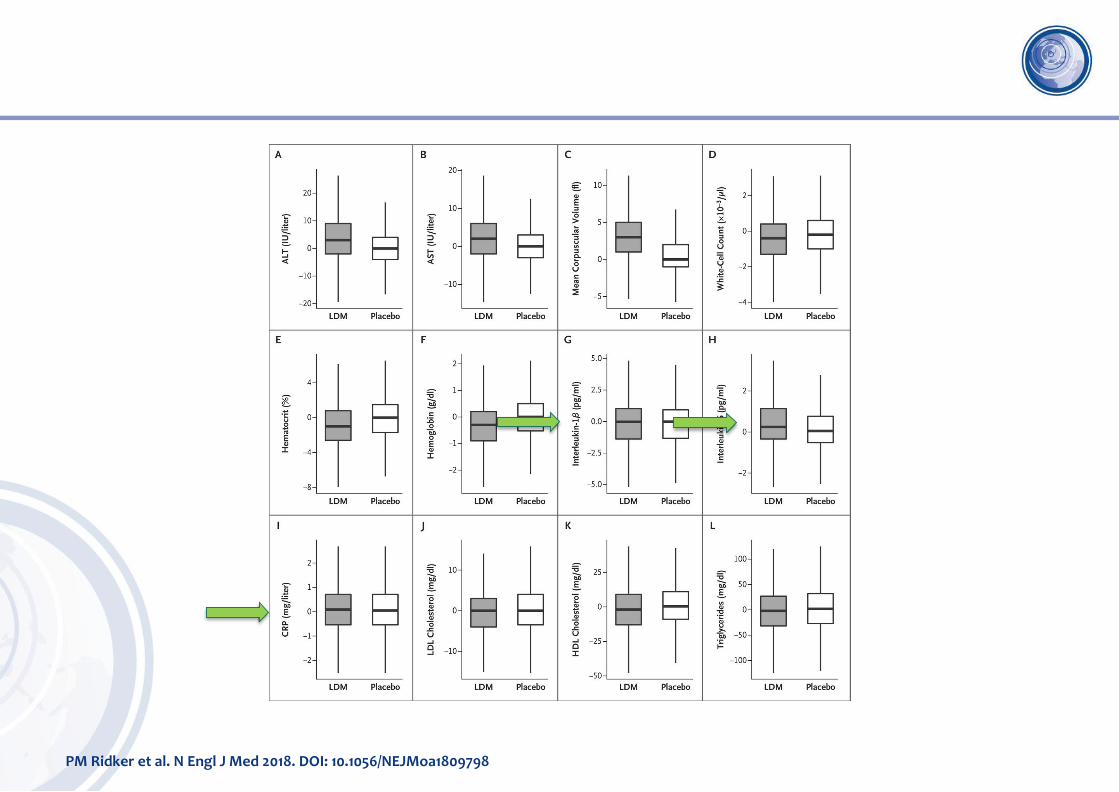
Laboratory Findings.
PM Ridker et al. N Engl J Med 2018. DOI: 10.1056/NEJMoa1809798
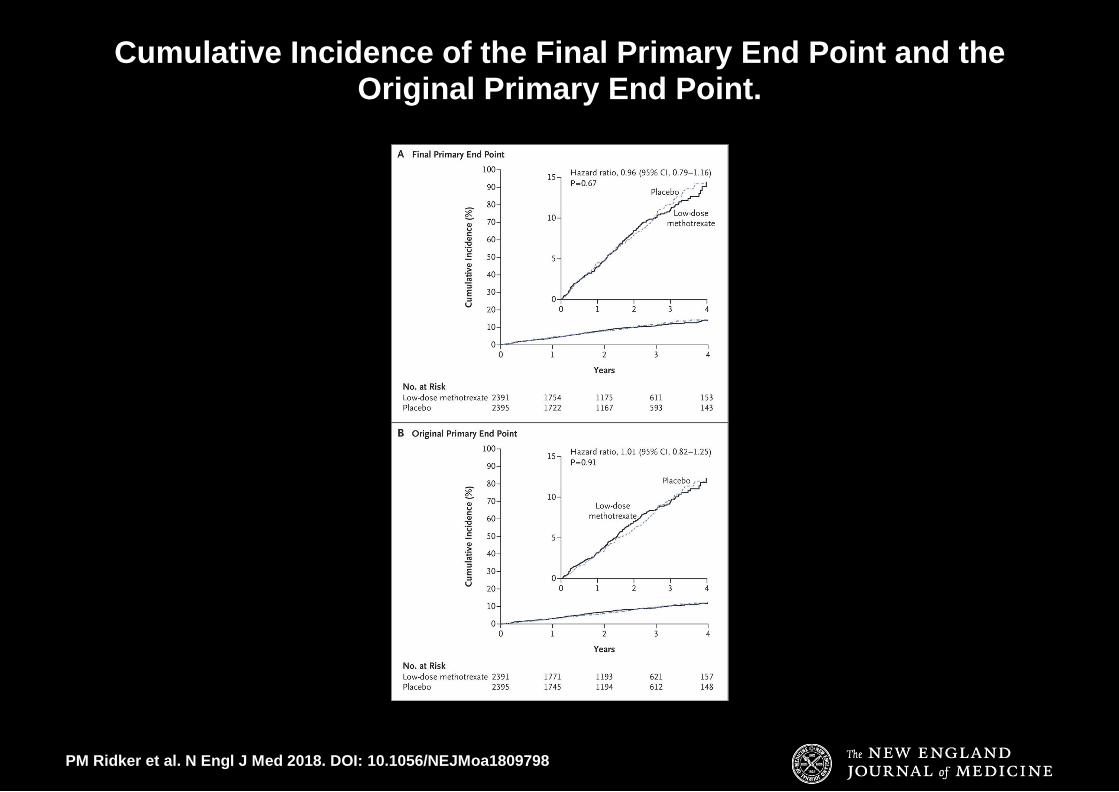
Cumulative Incidence of the Final Primary End Point and the Original Primary End Point.
Conclusies CIRT trial
• MTX geen effect : 201 MACEs bij MTX vs 207 MACEs bij placebo
• Verkeerde pathway?
• IL1/IL6 remming
• Wel reductie van HVZ (CANTOS*, canakinumab)
• Na MI, afname inflammatie en troponine release (tocilizumab*)
• Reden: MTX geen invloed op plaque stabiliteit?
Ridker et al N Engl J Med 2017
Kleveland et al Eur Heart J 2016
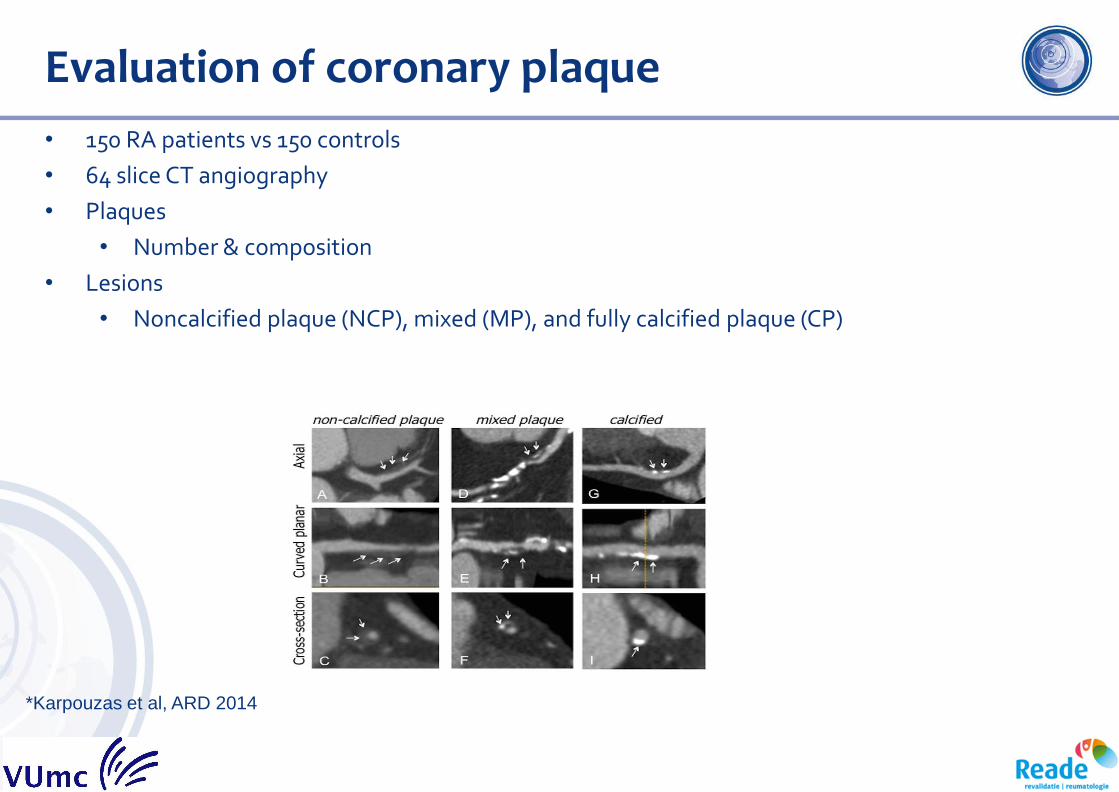
Evaluation of coronary plaque
• 150 RA patients vs 150 controls
• 64 slice CT angiography
• Plaques
• Number & composition
• Lesions
• Noncalcified plaque (NCP), mixed (MP), and fully calcified plaque (CP)
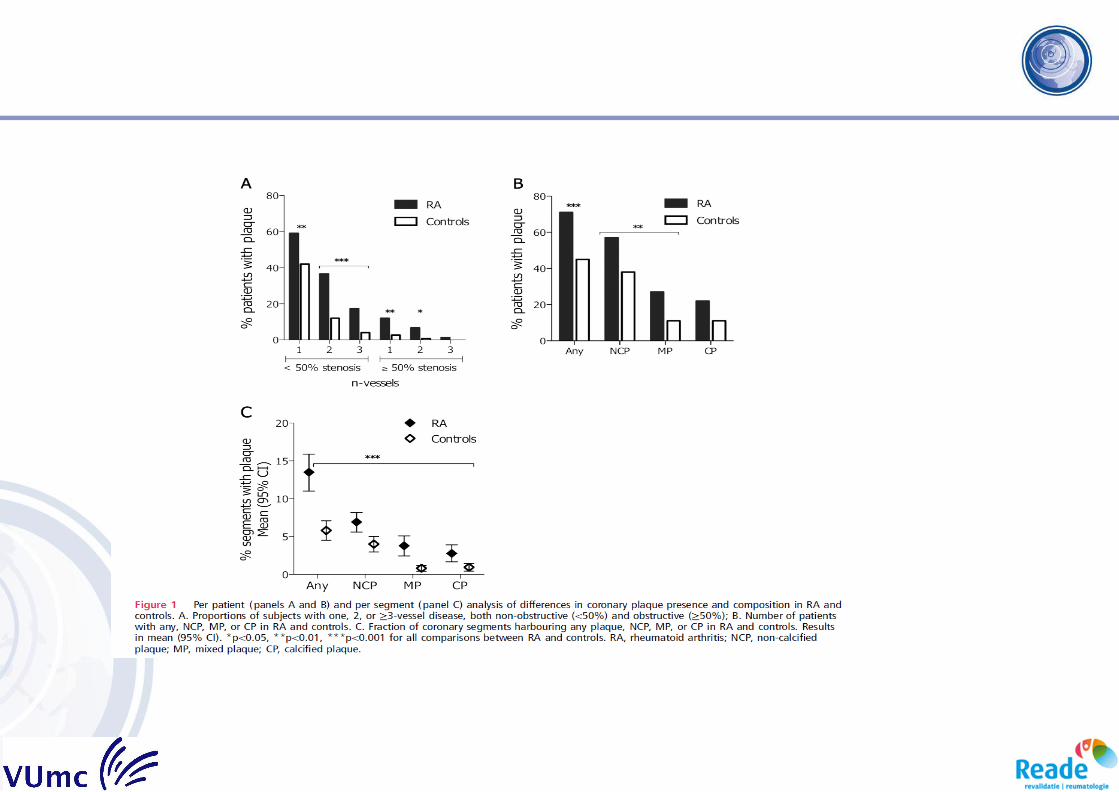
*Karpouzas et al, ARD 2014
Plaque-studie - Conclusies
• 60% van de RA ptn heeft asymptomatische coronaire plaques
• TNF-blokkers/MTX t.o.v. MTX alleen
• Significante afname van het aantal instabiele plaques
aTNF als secundaire preventie?
Conclusies & Take Home Messages I
• HVZ risico bij “reumatoïde artritis”: 1,7 – 2,0 x verhoogd
• Belangrijke oorzaak is de ontsteking versnelde atherosclerose
• Maar ook “traditionele” risico-factoren
• RA = nieuwe risicofactor voor hart- en vaatziekten
• Screening op risicofactoren voor hart- en vaatziekten/CVRM onontbeerlijk
Conclusies & Take Home Messages II
• Lipiden stijgen bij behandeling RA
• MTX geen CVD risico reductie in de “at risk” algemene populatie
• Andere pathways
• IL1/IL6 : duidelijk effect, maar kostbaar
• aTNF kan veel belovend zijn
• Biosimilars
• Helaas nog geen trials!





























