Embed Size (px)
Citation preview
Revalidation
THE ROYAL COLLEGE OF ANAESTHETISTS
What, when and how
What?Responsibility of individual doctors (and
the GMC and Professional bodies)
When?Piloting in 2009, ready and delivered in 2010
How?Locally with RCoA support
Definition
‘Revalidation is a process where doctors will be required to “periodically demonstrate their continued fitness to practise … and for specialist doctors, to demonstrate that they meet the standards that apply to their particular medical specialty (DH 2007: 6). If demonstration fails then an evaluation (GMC guidance relating to Medical Act, 2002) of evidence would be required, progressing to assessment if it is deemed necessary’.
It is important to remember that …..
The purpose of revalidation and medical regulation is not solely to identify doctors whose performance is not of a sufficiently high standard
The vast majority of doctors are practicing medicine to a high standard
Revalidation should be a process that will support continuous quality improvement in standards and practice for both doctors and patients alike
What is it?
A combined process of public assurance about medical fitness to practice
Three elements:Registration LicensingCertification
Registration
Identified as a doctorNo rights
• To practice
• To prescribe
• To certify death
Licensing
Identified on register to practiceGeneral rights (pays Fee)No specialist recognitionRemains open after retirementRenewed every 5 years
• Local process
Certification
Identified as a specialist (or GP)All non-training post holders
• Consultants / SAS + Trust posts
• Independent sector doctors
Renewed every 5 years• Recommendation from RCoA to GMC
• Linked to local process
Summary so far
RegistrationAble to be called a doctor
License to practiceCan practice as a doctor
CertificationCan practice as a specialist (anaesthetist)
When?
2009All on GMC register issued a license to practiceClock starts
2010Recertification startsNot across all specialities20% each year - who will it be?
NB – no evidence older than 5 years is admissible
How?
Demonstration that we meet the standards depends on a cascade Stage 1 provide evidence >95% Stage 2 may need evaluation <>5%Stage 3 GMC assessment <>1%
Demonstrating Practice – 5 years, 5 appraisals, 5 types of evidence
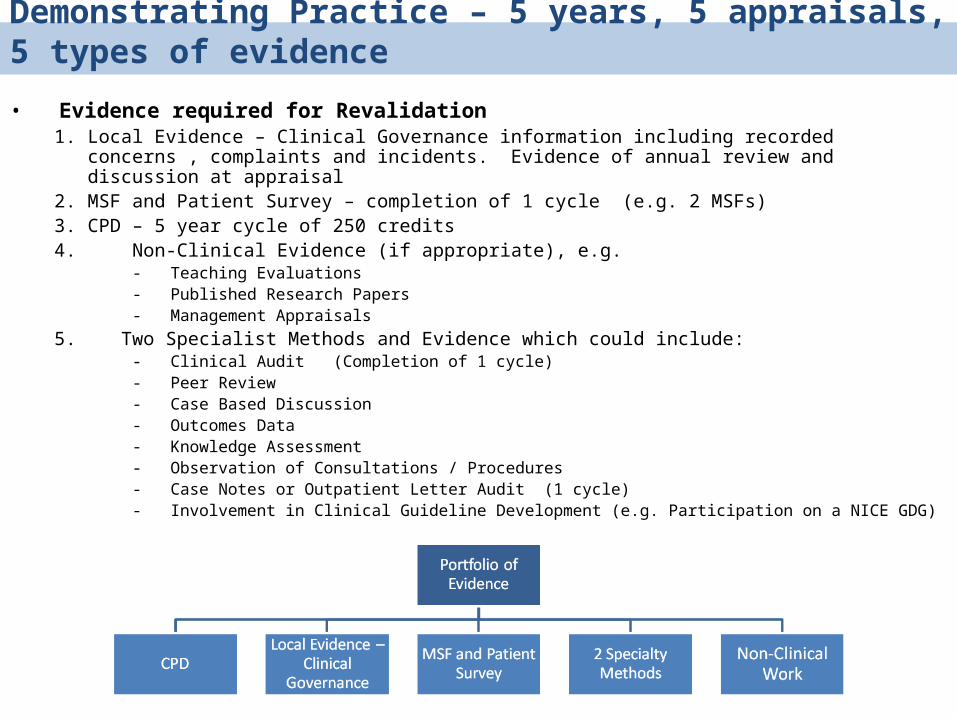
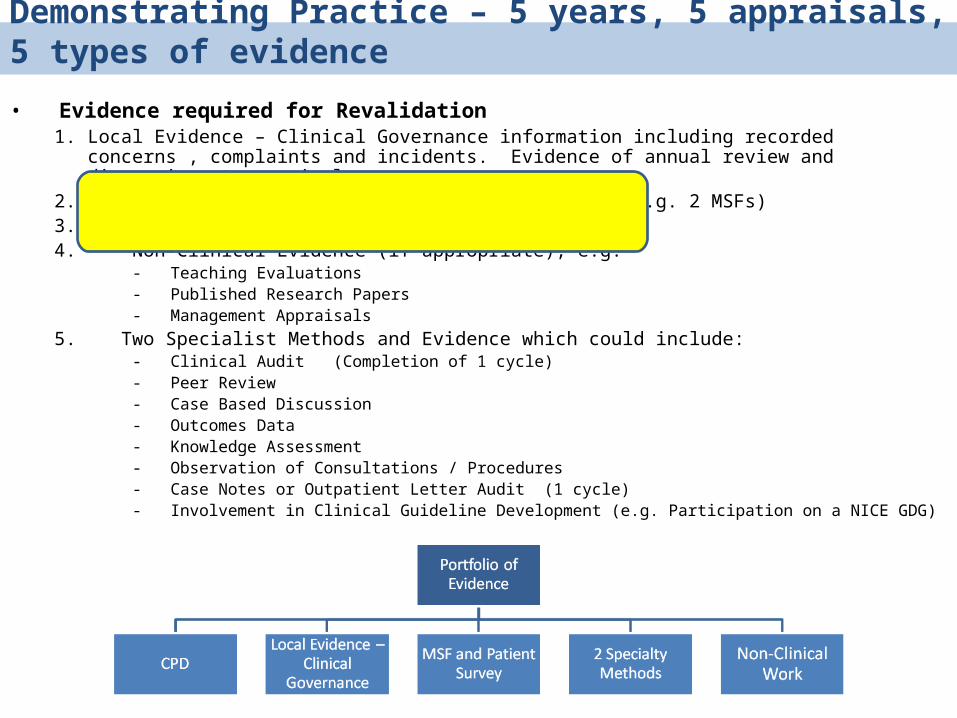
• Evidence required for Revalidation1. Local Evidence – Clinical Governance information including recorded concerns , complaints and incidents.
Evidence of annual review and discussion at appraisal2. MSF and Patient Survey – completion of 1 cycle (e.g. 2 MSFs)3. CPD – 5 year cycle of 250 credits4. Non-Clinical Evidence (if appropriate), e.g.
- Teaching Evaluations- Published Research Papers- Management Appraisals
5. Two Specialist Methods and Evidence which could include:- Clinical Audit (Completion of 1 cycle)- Peer Review- Case Based Discussion- Outcomes Data- Knowledge Assessment- Observation of Consultations / Procedures- Case Notes or Outpatient Letter Audit (1 cycle)- Involvement in Clinical Guideline Development (e.g. Participation on a NICE GDG)
Demonstrating Practice – 5 years, 5 appraisals, 5 types of evidence
• Evidence required for Revalidation1. Local Evidence – Clinical Governance information including recorded concerns , complaints and incidents.
Evidence of annual review and discussion at appraisal2. MSF and Patient Survey – completion of 1 cycle (e.g. 2 MSFs)3. CPD – 5 year cycle of 250 credits4. Non-Clinical Evidence (if appropriate), e.g.
- Teaching Evaluations- Published Research Papers- Management Appraisals
5. Two Specialist Methods and Evidence which could include:- Clinical Audit (Completion of 1 cycle)- Peer Review- Case Based Discussion- Outcomes Data- Knowledge Assessment- Observation of Consultations / Procedures- Case Notes or Outpatient Letter Audit (1 cycle)- Involvement in Clinical Guideline Development (e.g. Participation on a NICE GDG)
Colleges and Faculties: Roles and Responsibilities
1. Set Standards • Specialist Recertification• Specialty Service Provision and potentially Accreditation
2. Develop Specialty Tools and Methods
3. Train Appraisers in Specialty Standards and Methods
4. College/Faculty Role in Revalidation Recommendation • Quality assure local systems and processes leading to the Recommendation• Provide College Representatives to work at the Local level with the LRO to review appraisals and
evidence throughout the 5 year cycle and jointly confirm the Recommendation and send a Statement of Assurance to GMC
• College Regional Advisors?• Larger Colleges may need additional representatives in the larger regions
• Review all evidence portfolios and confirm Recommendation from LRO to GMC • Audit a proportion of evidence portfolios for quality assurance
5. Provide remediation support or advice for doctors identified as in need
Appraisal / assessment
We are well into the 5 year cycleThe evidence has to match the current
GMC Domains of Good Medical Practice (4 not initial 7)
Probity and health are for local use only
Specialist Standards for re-certification
4 Domains adapted from Good Medical Practice
Domain 1 - Knowledge, skills and performance
Domain 2 - Safety and quality Domain 3 - Communication, partnership and
teamwork Domain 4 – Maintaining Trust
Work Streams
These all interlink:CPDE-portfolioNon-clinical activityMSFRemediationDepartmental accreditation
CPD
Core topics are essential for all Primarily a knowledge based processLargely ‘internal’ process
Higher levels of CPD are necessary to demonstrate currency of practiceExternal process is likely to be necessary
CPD Process
Appropriate Recordable Verifiable
The ‘levels’ of CPD will varyThe content of CPD will vary
Definitions of CPD
Core topicsEssential knowledge for all practitionersRedefined from core topics agreed by
UEMS
Level 1Essential for safe practice when on callHospital specific
• May be evidenced by clinical activity or external CPD
Advanced CPD
Job planned clinical activityThe content of this specialised clinical work
has been defined by the relevant specialist societies
• It will be published on the CPD web-site• It will be used for evaluation if necessary• It will be a largely external process
Multi-source feedback
Two systemsThe precise nature will vary across
specialities• There is a minimum number of returns necessary• There is a maximum number of questions
Patient feedbackNot yet clearly defined for anaesthesia
Peer / teamMany commercial systems exist
Anaesthesia
Team systemsThese must inform the GMC Good
Medical Practice domains• They are often part of a Trust-wide
process• Most are poorly validated
Remedial process must be in place
Non-clinical activity
A process for identifying activity for the ‘wider’ NHSTeaching / trainingResearchCollege / AAGBI workAudit Writing / editing

Non-Clinical Activity
This will be considered as part of revalidationEvidence from the appraisal process
related to that activity will be usedNon-clinical activity does not replace the
CPD requirements for full-time practitioners
E-portfolio
This should underpin the entire processProvides the easiest method of completing
appraisal• Expensive• High security demands• Multi-speciality
Not likely to be fully functional on time
E-portfolio
More than a revalidation toolPersonal documentsLinked to e-CPD systemSecure Learning / reflective diaryLogbook dataTeaching / training activity
Departmental Accreditation
Part of healthcare regulationThe context for assessing
performance in revalidation• Evaluation of a doctor’s performance has to
include the environment in which they work• Local CPD activity may be recognised only
from accredited departments in the future
What should you do?
Today!Review your appraisalsIdentify any gaps in CPDCheck with your CD about opportunities
to ‘catch up’Start / continue to record logbook data
or identify systems that can
Planning
Find and organise the box-filesOne folder for each year
• Identify appraisals• Identify ‘themes’ from appraisals• Log praise / complaints• Collate CPD• Pilot / complete MSF
Where is the information
Links :http://aomrc.org.uk/revalidation.aspx
http://www.gmc.uk.org/about/reform/index.asp
http://www.rcoa.ac.uk/index.asp?SectionID=3