Embed Size (px)
Citation preview

Hindawi Publishing CorporationAnemiaVolume 2013 Article ID 617204 9 pageshttpdxdoiorg1011552013617204
Review ArticleBeta-Thalassemia Major and Female Fertility The Role of Ironand Iron-Induced Oxidative Stress
Paraskevi Roussou Nikolaos J Tsagarakis Dimitrios KountourasSarantis Livadas and Evanthia Diamanti-Kandarakis
Hematology Unit amp Endocrine Unit 3rd Department of Internal Medicine Medical School University of AthensldquoSotiriardquo General Hospital 152 Mesogeion Avenue 11527 Athens Greece
Correspondence should be addressed to Evanthia Diamanti-Kandarakis ediamantikandarakisgmailcom
Received 29 June 2013 Revised 22 October 2013 Accepted 11 November 2013
Academic Editor Fernando Ferreira Costa
Copyright copy 2013 Paraskevi Roussou et al This is an open access article distributed under the Creative Commons AttributionLicense which permits unrestricted use distribution and reproduction in any medium provided the original work is properlycited
Endocrine complications due to haemosiderosis are present in a significant number of patients with beta-thalassemiamajor (BTM)worldwide and often become barriers in their desire for parenthoodThus although spontaneous fertility can occur the majority offemales with BTM is infertile due to hypogonadotropic hypogonadism (HH) and need assisted reproductive techniques Infertilityin these women seems to be attributed to iron deposition and iron-induced oxidative stress (OS) in various endocrine organssuch as hypothalamus pituitary and female reproductive system but also through the iron effect on other organs such as liverand pancreas contributing to the impaired metabolism of hormones and serum antioxidants Nevertheless the gonadal functionof these patients is usually intact and fertility is usually retrievable Meanwhile a significant prooxidantsantioxidants imbalancewith subsequent increased (OS) exists in patients with BTM which is mainly caused by tissue injury due to overproduction of freeradicals by secondary iron overload but also due to alteration in serum trace elements and antioxidant enzymes Not only usingthe appropriate antioxidants essential trace elements andminerals but also regulating the advanced glycation end products couldprobably reduce the extent of oxidative damage and related complications and retrieve BTM womenrsquos infertility
1 Introduction
In beta-thalassemia major (BTM) iron overload is the jointoutcome of multiple blood transfusions and an inappropri-ately increased iron absorption associated with ineffectiveerythropoiesis [1] The outpouring of catabolic iron thatexceeds the iron-carrying capacity of transferrin results inthe emergence of nontransferrin-bound iron (NTBI) whichcatalyzes the formation of free radicals resulting in oxidativestress (OS) and damage to mitochondria lysosomes lipidmembranes proteins and DNA [1]Thus thalassemics are ina state of enhanced OS [2]
Meanwhile recent advances in the management of BTMhave significantly improved life expectancy and quality oflife of BTM patients with a consequent increase in theirreproductive potential and desire to have children [3] How-ever endocrine complications due to haemosiderosis arestill present in a significant number of patients worldwide
and often become a barrier in their desire for parenthood[4] Female patients with BTM usually suffer from hypog-onadotropic hypogonadism (HH) associated with amenor-rhea anovulation and infertility attributed to the iron effecton the pituitary gland as well as on the female reproductivesystem Early recognition and prevention of the endocrinecomplications by early and regular chelation therapy aremandatory for the improvement of the quality of life ofthese patients [5] Also treatment with combination ofantioxidants and iron chelators could probably neutralizethe deleterious effects of reactive oxygen species (ROS) [6]and probably reverse endocrine complications improvingreproductive ability and fertility potential
In this paper the published data on fertility potential offemales with BTM are reviewed trying to further associatethe determinant role of increased iron and iron-induced OSobserved in these patients with their respective reducedfertility potential The utility of substantial and theoretical
2 Anemia
therapeutic strategies is also discussed which could coun-teract iron-induced OS and preserve BTM femalesrsquo fertilitycapacity
2 BTM and Fertility Up-to-Date
BTM is a severe transfusion-dependent anemia that causesinfertility mainly due to iron deposition to endocrine organsafter overtransfusion [7] Spontaneous fertility can occurin well-chelated and transfused patients but the majorityare infertile due to HH and need assisted reproductivetechniques (ART) Safarinejad has previously evaluated thehypothalamic-pituitary-ovarian axis in female patients withBTM [8] In the thalassemic group the baseline and peaklevels after GnRH test of luteinizing hormone (LH) follicle-stimulating hormone (FSH) and estradiol were significantlylower than those in the control group [8] However ovarianfunction has been proposed to bemerely preserved inwomensuffering from primary or secondary amenorrhea (PA andSA resp) as they become able to conceive following a closelymonitored stimulation therapy [4] Overall the report ofa large number of successful pregnancies so far is highlyindicative of the relative safety of pregnancy in the iron-adjusted BTM woman [4] The iron-induced effect seemsto have a central role in the pathogenesis of the decreasedreproductive capacity [9]
Ovulation induction with gonadotropin has been suffi-ciently studied [10] Skordis et al have previously estimatedthe frequency of fertility among 50 women with BTM ofwhich 7 had PA 9 had SA and 34 had normal menstrualfunction (NM) [11] In all patients with PA and SA thepregnancies were induced while in most patients with NMpregnancies were achieved spontaneously [11] Additionallyin a previously published study Danesi et al showed thatby proper pharmacological stimulation the steroidogenicfunction of the gonads and even ovulation can be reinstated inhypogonadal thalassemic women [12] More recently Origaet al suggested that in women with HH gonadal functionis usually intact and fertility is usually retrievable [3] In thisstudy 46 women with BTM (58 pregnancies) were includedwhile conception was achieved after gonadotrophin-inducedovulation in 33 of them [3] Moreover Bajoria et al haverecently supported the feasibility and safety of pregnancy infemales with BTM reporting their experience on pregnancyfollowing ART in 11 women with BTM who had HH withfunctionally intact ovaries [13] However successful preg-nancy and fertility were also suggested to be feasible in BTMpatients with diminished gonadal reserves [14] The safety ofpregnancy for both mothers with BTM and their babies withproper care and guidance has been repeatedly proposed byseveral studies even in the case of intensive transfusion andchelation treatment [7 15 16] Meanwhile human GH as anadjunct to hMG and hCG seemed to be a sensible approachin the treatment of infertile homozygous BTM patients [17]
Based on the above it seems that irrespectively of thespontaneous or induced ovulation the current evidence-based knowledge on the outcome of attempted pregnancies
Iron deposition
Iron overload
Hypothalamus
Pituitary
Infertility
Increasedoxidative stress
Prooxidants
Alteration inserum traceelements andantioxidantenzymes
Antioxidants
Ovaries
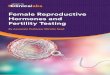
Figure 1 Infertility in female patients with BTM seems to beoriginated mainly by the direct and the indirect effect of ironoverload The combined effect of iron deposition and increasedOS (because of a significant prooxidantsantioxidants imbalance)results in the dysfunction of the female reproductive axis
in BTM female patients is optimistic Also the infertil-ity observed in this group of patients is probably mostlyattributed to impaired hypothalamic-pituitary-ovarian axisand less to gonadal dysfunction However there are minimaldata directly associating the role of iron iron-induced OSand antioxidant supplementation with the fertility potentialof these patients
3 Iron and Pathophysiology of BTM Infertility
Infertility in women with BTM is assumed to be mainlycaused by the direct or indirect effect of iron on thehypothalamic-pituitary-ovarian axis and the female repro-ductive system Indirect evidence suggests that the directeffect of iron is probably related to its direct deposition onthe hypothalamic-pituitary axis and the female reproductivesystemwhile direct evidence suggests that its indirect effect ismostly attributed to the iron-inducedOS (Figure 1) Howeverthere are limited data evaluating the pathophysiology ofiron-induced compromised fertility in which there is noclear discrimination between direct or indirect iron effectsNevertheless the most suitable model for speculating thedirect and indirect effect of iron on BTM womenrsquos fertilitycapacity is the model of hemochromatosis which will befurther discussed below Also the iron-mediated effect onfertility could be discriminated in its hypothalamic-pituitaryeffect and in its effect on the female reproductive system
31 Increased Oxidative Stress in BTMPatients BTMpatientsare under continuous blood transfusion which leads to aniron overload with a resultant increase in NTBI that causesgreater tissue toxicity than iron in other forms [2] Anothersource of iron accumulation results from increased duodenaliron absorption due to decreased expression of hepcidinthe main regulator of iron homeostasis [6] Iron generates
Anemia 3
production of ROS via the Fenton reaction hence ironoverload disrupts the redox balance of the cells causingchronic OS [18] OS leads to lipid peroxidation of unsaturatedfatty acids in membranes of cells and organelles Cytotoxicbyproducts of lipid peroxidation such as malondialdehyde(MDA) and 4-hydroxy-21015840-nonenal are produced and theseimpair cellular function and protein synthesis and damageDNA [19] Furthermore a crucial component in the oxidantsusceptibility of the thalassemic RBC is the release of hemeand iron from the excessive unpaired alpha-globin chains[2] This release initiates self-amplifying redox reactionswhich deplete the cellular reduction potential (eg glu-tathioneGSH) oxidize additional hemoglobin and acceler-ate RBC destruction [2]
Oxidativeantioxidative balance is one of themost impor-tant factors for homeostasis When the balance of ROSand antioxidants is disrupted towards an overabundanceof ROS OS occurs [20] The generation of ROS is asteady-state cellular event in respiring cells while theiruncontrolled production often leads to damage of cellularmacromolecules (DNA protein and lipids) and other smallantioxidant molecules [21] A number of major enzymaticand nonenzymatic defense mechanisms exist to neutralizeand combat the damaging effects of these reactive sub-stances [22] The enzymic system functions by direct orsequential removal of ROS (superoxide dismutaseSODcatalaseCAT and glutathione peroxidaseGPx) thereby ter-minating their activities Nonenzymic defense consists ofscavengingmolecules that are endogenously produced (GSHubiquinols and uric acid) or derived from the diet such asvitamins C and E [21] These antioxidant nutrients occupydistinct cellular compartments and among them there isactive recycling Antioxidative systems which protect fromperoxidative damage are also supposed to be under hormonalinfluence while antioxidative enzymes require the presenceof microelements in their active centers as well as concertaction of nonenzymatic antioxidants which support enzymesin their scavenging action [23]Meanwhile diet seems to havean impact on antioxidative system which requires appro-priate supplementation inmicroelements and vitamins for itseffective function leading to scavenging excess of free radi-cals [23]
According to the current evidence-based knowledge asignificant prooxidantsantioxidants imbalance with subse-quent increased OS exists in patients with BTM which ismainly caused by tissue injury due to overproduction of freeradicals by secondary iron overload alteration in serum traceelements and alteration in antioxidant enzymes level [24](Figure 1) The results of Wassem et al revealed that thelevels of vitamin E and antioxidant enzymes GPx and SODwere significantly lowered in BTM patients as comparedwith the control group indicating that thalassemics are ina state of enhanced OS [2] Another study revealed thatplasma thiobarbituric acid (TBA) reactive substances wereelevated in BTM children compared to controls togetherwith compensatory increase in SOD activity and decrease inCAT activity [25] At the same study serum ferritin showeda positive correlation with elevated TBA reactive substancesand SOD suggesting that iron overload is involved in the OS
shown in cells [25] A significant increase in the levels of lipidperoxide and iron and a significant decrease in the levels ofvitamin E total antioxidant capacity and total iron bindingcapacity were observed in a different study [26] suggestingthat OS and reduced antioxidant defense mechanism play animportant role in pathogenesis of BTM [26] FurthermoreLivrea et al have previously suggested that the measure-ment of peroxidation products matched with evaluation ofantioxidants may be a simple measure of iron toxicity inthalassemia in addition to the conventional indices of ironstatus [27] Their study showed that the mean concentrationsof conjugated diene lipid hydroperoxides (CD) lipoperoxidesevaluated as (MDATBA) adducts and protein carbonylsincreased about twofold with respect to control A net dropin the concentration of ascorbate vitamin E vitamin A beta-carotene and lycopene was also observed Serum levels ofvitamin E were inversely correlated with ferritin suggesting amajor consumption of this antioxidant under iron overloadwhile serum levels of vitamin E vitamin A and lycopenewere inversely correlated with the levels of transminases [27]On the other hand their results pointed out that the iron-induced liver damage in thalassemia may play a major rolein the depletion of lipid-soluble antioxidants [27] Later onChiou et al indicated that excessive lipid peroxidation and aprofound depletion of plasma vitaminsA E andC levels existin patients with BTM thus antioxidant supplementation forthe purpose of alleviating the OS may be warranted [28]They also found that HCV infection did play some role inaggravating the depletion of plasma vitamins E and C levelsin the BTM patients while it did not seem to alter the levelsof reduced GSH as well as antioxidant enzyme activities [28]
32 The Possible Impact of Oxidative Stress on BTM FemalesrsquoFertility Potential Although there is no direct evidence-based publication correlating the iron-inducedOSwith BTMwomenrsquos infertility existing published data on non-BTMpatients only permit the correlation of OS (not specificallyproduced through iron overload) with normal and abnormalprocesses of the female reproductive system Also there isno available publication connecting iron-induced OS withspecific altered signaling events in hypothalamic-pituitary-gonadal axis which subsequently could lead to infertilityThus until now only indirect evidence exists which supportsthe hypothesis that iron-induced OS is the main causal agentfor infertility in women with BTMThis is maybe happeningnot only through iron deposition and iron-induced OS invarious endocrine organs such as hypothalamus pituitaryand female reproductive system but also through its indirecteffect on other organs such as liver and pancreas contribut-ing to the impaired metabolism of hormones and serumantioxidants
Recently ROS have been shown to have an important rolein the normal functioning of reproductive system and in thepathogenesis of infertility in females [29] OS develops whenthere is an imbalance between the generation of ROS andthe scavenging capacity of antioxidants in the reproductivetract while it affects both natural and assisted fertility [29]ROS affect multiple physiological processes from oocyte
4 Anemia
maturation to fertilization embryo development and preg-nancy [20] There is sufficient evidence to hypothesize thatdietary antioxidants and OS may influence the timing andmaintenance of a viable pregnancy [30] Also physiologicallevels of ROS play an important regulatory role throughvarious signaling transduction pathways in folliculogenesisoocyte maturation endometrial cycle luteolysis implanta-tion embryogenesis and pregnancy [31] Proper functioningof the ovary is critical to maintain fertility and overall healthand ovarian function depends on the maintenance andnormal development of ovarian follicles [32] The potentialimpact of OS on the wellbeing of primordial growing andpreovulatory follicles as well as oocytes and early embryosexamining cell types and molecular targets has been exten-sively reviewed [32] Meanwhile ROS-induced apoptotic celldeath is involved in the mechanisms of corpus luteum (CL)regression that occurs at the end of the nonfertile cycle [33]
The role of OS in female reproduction is becomingincreasingly important as recent evidence suggests that itplays a part in conditions such as polycystic ovary syndrome(PCOS) endometriosis unexplained fertility spontaneousabortions preeclampsia hydatidiform mole embryopathiespreterm labor and intrauterine growth retardation [31] Agar-wal et al have recently reviewed the role of OS in normal andabnormal female reproductive physiological processes ana-lyzing the exact mechanisms of redox cell signaling and thepathophysiology of OS-related reproductive diseases [34] Aspecial comment should be made on endometriosis patientswhere iron overload has been demonstrated in the differentcompartments of the peritoneal cavity (peritoneal fluidendometriotic lesions peritoneum and macrophages) [35]This iron overload affects numerous mechanisms involvedin endometriosis development [35] Iron-induced OS maybe involved in endometriosis-associated infertility and mayplay a role in the regulation of the expression of genesencoding immunoregulators cytokines and cell adhesionmolecules implicated in the pathogenesis of endometriosis[36] Moreover a recent study investigated the relation-ship between OS and the underlying causes of infertilitypreovulatory ovarian hormones and ovarian response togonadotropin stimulation in patients undergoing ART [37]There was no significant relationship between plasma orfollicular fluid (FF) total antioxidant capacity (TAC) and theunderlying etiology of infertility [37] However there was astatistically significant positive association between FF E(2)levels and TAC OS has an impact on the production ofgranulosa cell steroid hormones in particular E(2) which isan important predictor of ovarian response [37] Thus thepossible impaired ovarian response in BTM women couldbe probably caused by dysregulation in the production ofgranulosa cell steroid hormones such as E(2) Meanwhile ithas been suggested that OSmodulates the age-related declinein fertility [20] Additionally a recent study indicated thatnonheme iron accumulation on ovarian stromal tissue maybe related to aging of the ovary due to increasing OS [38]Theage-related decline in fertility due to OS has a special impactin our group of patients because of their increased age aver-age due to significant improvements in chelation treatmentmodalities Furthermore remarkable is another study which
evaluated retinol and alpha-tocopherol natural antioxidantsthat inhibit lipid peroxidation and protect against cell damageinduced by OS and revealed that lower concentrations ofthese natural antioxidants were associated with abnormalsemen parameters in men and anovulation in women [39]
4 Evidence-Based Effect of Iron Overloadand Iron-Induced OS on Hypothalamic-Pituitary-Gonadal Axis and FemaleReproductive System
Although there are limited data directly correlating iron over-load with iron-induced OS on BTM femalesrsquo hypothalamic-pituitary-gonadal axis and ovarian reserve indirect conclu-sions could be obtained through the model of hemochro-matosis
41 The Model of Hemochromatosis Endocrinopathies arecommon in transfusion-associated haemochromatosis [40]while HH is the most frequent endocrine abnormality inhemochromatosis [41] The gonadotropin responsiveness to100 micrograms of LHRH was impaired or absent in patientswith hemochromatosis [42] Also in a cohort of 115 patientssuffering from genetic hemochromatosis hypogonadismwasevidenced in 42 of them inmost of which it was consideredas secondary to pituitary lesions as assessed by GnRH tests[43] Moreover in male patients with idiopathic hemochro-matosis testicular atrophy has been suggested to be causedby insufficient secretion of gonadotropins due to the selectiveaccumulation of iron in gonadotropic cells of the pituitarygland [44] Meanwhile subnormal gonadotropin responsesto GnRH but normal ovarian reserve as shown by normalfollicular stimulation with hMG were reported in a case ofHH in a female with biopsy-proven hemochromatosis [45]In another case report recovery of reproductive functionsdocumented by hormone measurements testicular biopsyand semen analysis was observed in a 37-year-old man withHH due to idiopathic hemochromatosis after phlebotomy[46] It has been also proposed that subjects with lesserdegrees of hepatic siderosis at diagnosis are unlikely todevelop hypogonadism [47] Furthermore the pituitary ofa 69-year-old man with hemochromatosis had been pre-viously removed at autopsy and was studied by histologyhistochemistry immunocytochemistry electron microscopyand X-ray diffraction [48] Preferential localization of irondeposits was demonstrated in gonadotrophs which at theultrastructural level displayed selective severe cellular injury[48] X-ray diffraction revealed the deposition of iron-accumulated lysosomes while iron storage was also notedin stellate cells [48] It should be also noted that in a groupof 7 young male patients with genetic hemochromatosis thenormal or high increments of LH after LHRH stimulationsuggested that secretion capacity of LH was intact andthat hypothalamic dysfunction could be responsible for theobserved preclinical gonadal deficiency [49] A similar resultwas obtained in another male patient where although thepituitary secretion of LH was normal in response to GnRHstimulation clomiphene administration did not produce an
Anemia 5
increase in LH and FSH suggesting that there was a defect inthe hypothalamic GnRH response [50]
In agreement with the hemochromatosis model abnor-malities of the hypothalamic-pituitary-gonadal axis are themost common endocrine abnormalities in patients withBTM as they require multiple blood transfusions leading tohemochromatosis [51] Thus based on the model of hemo-chromatosis that resembles iron-overloaded patients withBTM it seems that abnormalities of ovulation and menstru-ation in these patients are most likely because of inadequatepituitary responsiveness to GnRH [45]
42 Direct and Indirect Evidence for the Hypothalamic-Pitui-tary and the Gonadal Effect of Iron Patients with transfu-sional iron overload begin to develop pituitary iron overloadin the first decade of life however clinically significantvolume loss was not observed until the second decadeof life [52] Pituitary iron overload and volume loss wereindependently predictive of hypogonadism [52] Pituitary R2correlated significantly with serum ferritin as well as liverpancreatic and cardiac iron deposition by MRI [52] Manypatients with moderate-to-severe pituitary iron overloadretained normal gland volume and function representing apotential therapeutic window [52] According to a differentstudy BTM patients with severe organ damage and ironoverload are likely to be apulsatile with irreversible damageto their hypothalamic-pituitary axis while those with less-severe iron overload are likely to have potentially reversibleHH [53]The same study suggested that gonadotrophin pulseparameters rather than the gonadotrophin response to aGnRH bolus following prolonged pulsatile GnRH infusionmay be more useful in discriminating reversible from irre-versible HH [53] Furthermore in a study of 33 patients above15 years of age with transfusion-dependent BTM and ironoverload anterior pituitary function (GnRH stimulation test)correlated well with MRI results However no correlationwas found between the MRI measurements the GnRHstimulation test and the clinical status of the patients as 28out of the 33 patients achieved normal puberty [54] Anotherpossible mechanism of iron effect on hypothalamic-pituitaryaxis is through iron-induced OS with subsequent alterationson elongation factor-2 (eEF-2) levels The hypothalamic-pituitary system secretes peptide hormones whose synthesisrequires the integrity of the translation machinery Amongthe possible causes of the decline of translation in oldanimals are the modifications of eEF-2 [55] Iron-induced OScould be involved in the alterations of eEF-2 which formsadducts with MDA and 4-hydroxynonenal (HNE) [55] Thealterations of eEF-2 levels secondary to lipid peroxidationand adduct formation with these aldehydes could contributeto the suboptimal hormone production from these tissues[55] Moreover the possible concurrent GH deficiency maypotentiate the already present OS as patients with GHdeficiency have an increased degree of OS and endothelialdysfunction which possibly acts synergistically with iron-induced OS [56] Thus although there is limited evidenceon the exact pathophysiological mechanisms of iron effecton hypothalamic-pituitary axis it seems to be the basic
pathogenetic cause of the impaired hypothalamic-pituitarysystem
Meanwhile according to our knowledge only one studyexists which proves the iron deposition on the femalereproductive system in patients with BTM This particularstudy obtained histopathological evidence that depositionof haemosiderin occurred in the endometrial glandularepithelium of three patients with BTM [57] This depositionwas mainly evident in the apical part of these cells abovethe nuclei and should be taken into consideration as acontributing factor to the infertility in these patients byaltering endometrial receptivity for implantation [57] In twopatients who received effective iron chelating treatment withdesferrioxamine the endometrial haemosiderin depositseither disappeared or were significantly reduced [57]
43 Available Studies Directly Correlating Iron and Its Impacton Fertility in Women with BTM The pathophysiology ofiron-induced compromised fertility in women with BTMwas only recently evaluated [9] Low gonadotropin secretionresulted in reduced ovarian antral follicle count and ovarianvolume but levels of antimullerian hormone (AMH) a sensi-tive marker for ovarian reserve independent of gonadotropineffect were mostly normal AMH correlated with NTBI sug-gesting a role of labile iron in the pathogenesis of decreasedreproductive capacity possibly occurring in parallel to car-diac iron toxicity as cardiac iron was associated with thepresence of amenorrhea and with NTBI levels Thus AMHwas suggested to be valuable for future studies aiming atimproved chelation for fertility preservation whereas NTBIand labile plasma iron was suggested to be valuable formonitoring iron effect on the reproductive system [9] Thesame research team explored the relationship between liveriron concentration (LIC) and fertility status in 26 females(mean 30 years old) with BTM Seventeen (65) of themexperienced PA or SA Levels of LHFSH and estradiol werelow or undetectable in 48 and 35 of patients respectivelyand did not correlate with age presence of amenorrhea andLIC The fact that LHFSH and estradiol commonly usedfor assessment of fertility potential in thalassemia had apoor predictive value addressed the need for utilization ofcurrent available methods for assessment of fertility capacityin thalassemia [58]
5 Potential Antioxidants in BTM
Considering all the above we suggest that the enhancedOS observed in iron-overloaded patients with BTM mayplay a significant role in their reduced reproductive abilityThe investigation of the proper antioxidants for fertility andpregnancy in BTM female patients which are recognized aspatients of increased OS is of great value and importanceThe increased age average of this group of patients underlinesthe increased importance of OS on the female reproductivesystem as it has been also connected with aging Howeverdespite the clear identification of the oxidativeantioxidativeimbalance in patients with BTM there are few studies
6 Anemia
evaluating the effect of different antioxidant supplementationin BTM-related morbidities such as infertility
51 Antioxidant Supplements Used in BTM The benefits ofvitamin C and vitamin E as antioxidant supplements inBTMchildren have been previously determined [59] Twentychildren who had laboratory confirmation of BTM at least 6months with history of packed red cell transfusion withoutiron chelation were recruited It was suggested that vitaminC plus vitamin E supplementations have benefits more thanvitamin E alone in promoting antioxidant status and mayenhance liver function as total bilirubin tends to decrease[59] Furthermore curcuminoids extracted from the spiceturmeric are known to have antioxidant and iron-chelatingproperties and have been proposed as a potential upstreamtherapy of thalassemiaWeeraphan et al have recently appliedproteomic techniques to study the protein profile and oxida-tive damage in the plasma of beta-thalassemiaHb E patientsbefore and after treatment with curcuminoids Their studyindicated the ameliorating role of curcuminoids towards OSand iron overload in the plasma proteome [60] Glutaminealpha-lipoic acid acetyl-L-carnitine and N-acetylcysteineare also recently being studied as antioxidant supplements forsickle cell disease and thalassemia [61] Finally the value ofantioxidant supplements in the elimination of iron-inducedOS and subsequent infertility issues could be speculatedby the fact that various antioxidants (such as carnitinevitamin C vitamin E selenium carotenoids glutathioneN-acetylcysteine zinc folic acid and coenzyme Q10) arevariably effective in OS-induced male-factor infertility withrespect to improving semen parameters and pregnancy rates[62]
52 Chelation Treatments as Antioxidants in BTM Differentstudies have also focused on the antioxidant capacity of differ-ent chelation treatment modalities Increased evidence fromin vitro in vivo and clinical studies suggest that deferiprone(L1) can be used as a potent pharmaceutical antioxidant bymobilizing labile iron and copper andor inhibiting theircatalytic activity in the formation of free radicals and OS intissue damage [63] In contrast to L1 both desferrioxamine(DFO) and deferasirox (DFRA) were suggested to havemajordisadvantages in their use in noniron loading conditionsdue to toxicity implications [63] Meanwhile a subsequentstudy indicated that DFO chelation therapy does not nor-malize ferritin levels but attenuates oxidative damage andimproves total antioxidant level in Malaysian Chinese BTMpatients [64] The objective of this research was to studythe oxidant-antioxidant indices in BTM patients who wereon desferrioxamine-chelation or without chelation therapyBlood was collected from 39 Chinese patients and 20 con-trols Plasma and peripheral blood mononuclear cell lysates(PBMC) were extracted and biochemical tests to evaluate OSwere performedOSwas evident in these patients as advancedoxidized protein products (AOPP) and lipid hydroperoxideswere elevated whereas glutathione peroxidase activity andthe ferric reducing antioxidant power (FRAP) were reducedThe catalase activity in the patientsrsquo PBMC was elevated
possibly as a compensatory mechanism for the reducedglutathione peroxidase activity in both red blood cells andPBMC The lower FRAP and higher AOPP levels in thenonchelated patients compared with the chelated patientswere indicative of a lower OS level in the chelated patients[64] An additional study which assessed whether oxidant-stress and inflammation in BTM could be controlled byDFRA as effectively as by DFO revealed equal effectivenessin decreasing iron burden and levels of the oxidative-stressmarker MDA [65]
53 The Possible Effect of Advanced Glycation End Products(AGEs) Regulation on BTM Womenrsquos Ovarian Function andFertility Recent data have shown that OS is involved in thepathophysiology of anovulation [20 66 67] While the roleof OS in ovulatory dysfunction has been sufficiently studied[29 68] advanced glycation end products (AGEs) have beenrecognized as mediators of increased OS [69 70] Advancedglycation end products (AGEs) are a heterogeneous group ofbioactive molecules formed by the nonenzymatic glycationof proteins lipids and nucleic acids [71] There is increasingevidence that AGEs play a pivotal role in atherosclerosis andin diabetes and its complications while AGE accumulationis a measure of cumulative metabolic and OS and mayso represent the ldquometabolic memoryrdquo [72] Engagement oftheir receptor RAGE with AGEs is shown to activate itsdownstream signaling and evoke OS and inflammation indiabetes [73] AGEs have been found to induce OS andconversely OS stimulates AGEs formation [74ndash76]
AGEs deposition in ovary dysregulate ovarian functionthrough the induction of androgen production as well as OSgeneration through the induction ofNF-K120573pathway leadingto increased production of atherogenic and inflammatorymolecules AGEs have been implicated in the developmentof insulin resistance hyperandrogenism and anovulationin polycystic ovary syndrome (PCOS) and seem to have acentral role in PCOS pathophysiology either as a marker ofOS or through their specific actions after their ligation totheir specific receptor RAGE [77] Furthermore there is sub-stantial evidence that insulin resistance constitutes one of themain pathophysiological mechanisms leading to anovulationand ovarian hyperandrogenism in PCOS patients Regardingthe above also that iron has been implicated in abnormalinsulin secretion in patients with BTM or hemochromatosis[44 78] and that OS might be responsible for a decline ininsulin-mediated glucose uptake in BTM patients leadingto insulin resistance [79] we consider that the evaluationof AGEs as markers of OS in relation to iron overloadinsulin resistance and ovulation potential would be of greatvalue Reducing AGEs in BTM females could probably havebeneficial effects in insulin resistance and ovulation potentialand thus in fertility potential Finally it is remarkable thatthe iron chelator Desferal had a retardation effect on thefunctional and structural changes of Hb during fructation[80] It could prevent the AGEs and carbonyl formations andhelix depletion during theHb fructation processMoreover itcould preserve peroxidase and esterase activities of fructated
Anemia 7
Hb similar to native Hb Therefore desferal could be intro-duced as an antiglycation drug to prevent theAGEs formation[80]
6 Conclusions
On the basis of all the presented data it can be concludedthatOS plays amajor role in the pathophysiology of infertilityin females with thalassemia This OS is mainly caused bytissue injury due to overproduction of free radicals bysecondary iron overload alteration in serum trace elementsand alteration in antioxidant enzymes level Consequentlythere is a rationale for iron chelation to eliminate the free-iron species which in this respect act like antioxidantsAntioxidants are also capable of ameliorating increased OSparameters and given together with iron chelators mayprovide a substantial improvement in the pathophysiologyof thalassemia [81] However there is no study evaluatingthe efficacy of antioxidant supplementation on BTMwomenrsquosfertility potential In agreement with previous suggestionswe consider that the application of treatment strategies thatwould reduceOS in the reproductive tract could help infertilewomen with diseases such as BTM that are caused byROSantioxidants imbalance [29] In general research isin progress to identify the mechanisms that are involvedin the etiology of female reproductive diseases caused byROS and to create effective strategies that can counteractOS [29] while few are the trials investigating antioxidantsupplementation in female reproduction [20] The admin-istration of selective antioxidants along with essential traceelements and minerals to reduce the extent of oxidativedamage and related complications such as infertility in BTMpatients still needs further evaluation [24] However beforeclinicians recommend antioxidants randomized controlledtrials with sufficient power are necessary to prove the efficacyof antioxidant therapeutic strategies in disorders of femalereproduction [20] such as BTMThis is strongly emerged bythe fact of prolonged survival and the newly recognized issuesand challenges that adults with BTM face [82]
References
[1] C Hershko ldquoPathogenesis and management of iron toxicity inthalassemiardquo Annals of the New York Academy of Sciences vol1202 pp 1ndash9 2010
[2] F Waseem K A Khemomal and R Sajid ldquoAntioxidant statusin beta thalassemia major a single-center studyrdquo Indian Journalof Pathology and Microbiology vol 54 no 4 pp 761ndash763 2011
[3] R Origa A Piga G Quarta et al ldquoPregnancy and 120573-thalassemia an Italian multicenter experiencerdquoHaematologicavol 95 no 3 pp 376ndash381 2010
[4] N Skordis L Petrikkos M Toumba et al ldquoUpdate on fertilityin thalassaemia majorrdquo Pediatric Endocrinology Reviews vol 2supplement 2 pp 296ndash302 2004
[5] M Toumba A Sergis C Kanaris and N Skordis ldquoEndocrinecomplications in patients with thalassaemia majorrdquo PediatricEndocrinology Reviews vol 5 no 2 pp 642ndash648 2007
[6] E A Rachmilewitz O Weizer-Stern K Adamsky et al ldquoRoleof iron in inducing oxidative stress in thalassemia can it be
prevented by inhibition of absorption and by antioxidantsrdquoAnnals of the New York Academy of Sciences vol 1054 pp 118ndash123 2005
[7] S Ansari A Azarkeivan and A Tabaroki ldquoPregnancy inpatients treated for beta thalassemia major in two centers(Ali Asghar Childrenrsquos Hospital and Thalassemia Clinic) out-come for mothers and newborn infantsrdquo Pediatric Hematology-Oncology vol 23 no 1 pp 33ndash37 2006
[8] M R Safarinejad ldquoReproductive hormones and hypothalamic-pituitary-ovarian axis in female patients with homozygous 120573-thalassemia majorrdquo Journal of Pediatric HematologyOncologyvol 32 no 4 pp 259ndash266 2010
[9] S T Singer E P Vichinsky G Gildengorin J van DisseldorpM Rosen and M I Cedars ldquoReproductive capacity in ironoverloaded women with thalassemia majorrdquo Blood vol 118 no10 pp 2878ndash2881 2011
[10] G Vizziello D Carone E Caroppo A Vitti A Pasquad-ibisceglie and G Drsquoamato ldquoOvulation induction with gona-dotropin in patients with thalassemia pretreated with pulsatileGnRH outcomerdquoMinerva Ginecologica vol 56 no 5 pp 485ndash487 2004
[11] N Skordis S Christou M Koliou N Pavlides and M Angas-tiniotis ldquoFertility in female patients with thalassemiardquo Journalof Pediatric Endocrinology and Metabolism vol 11 supplement3 pp 935ndash943 1998
[12] LDanesiM Scacchi AMMiragoli et al ldquoInduction of folliclematuration and ovulation by gonadotropin administration inwomen with 120573-thalassemiardquo European Journal of Endocrinol-ogy vol 131 no 6 pp 602ndash606 1994
[13] R Bajoria and R Chatterjee ldquoCurrent perspectives of fertilityand pregnancy in thalassemiardquoHemoglobin vol 33 supplement1 pp S131ndashS135 2009
[14] R Bajoria and R Chatterjee ldquoHypogonadotrophic hypogo-nadism and diminished gonadal reserve accounts for dys-functional gametogenesis in thalassaemia patients with ironoverload presenting with infertilityrdquoHemoglobin vol 35 no 5-6 pp 636ndash642 2011
[15] M Karagiorga-Lagana ldquoFertility in thalassemia the Greekexperiencerdquo Journal of Pediatric Endocrinology andMetabolismvol 11 supplement 3 pp 945ndash951 1998
[16] S M Tuck ldquoFertility and pregnancy in thalassemia majorrdquoAnnals of the New York Academy of Sciences vol 1054 pp 300ndash307 2005
[17] D Surbek A Koller and N Pavic ldquoSuccessful twin pregnancyin homozygous 120573-thalassemia after ovulation induction withgrowth hormone and gonadotropinsrdquo Fertility and Sterility vol65 no 3 pp 670ndash672 1996
[18] K Yamaguchi M Mandai S Toyokuni et al ldquoContents ofendometriotic cysts especially the high concentration of freeiron are a possible cause of carcinogenesis in the cysts throughthe iron-induced persistent oxidative stressrdquo Clinical CancerResearch vol 14 no 1 pp 32ndash40 2008
[19] M C Kew ldquoHepatic iron overload and hepatocellular carci-nomardquo Cancer Letters vol 286 no 1 pp 38ndash43 2009
[20] AAgarwal S Gupta andRK Sharma ldquoRole of oxidative stressin female reproductionrdquo Reproductive Biology and Endocrinol-ogy vol 3 article 28 2005
[21] A C Chan C K Chow and D Chiu ldquoInteraction of antiox-idants and their implication in genetic anemiardquo Proceedings ofthe Society for Experimental Biology and Medicine vol 222 no3 pp 274ndash282 1999
8 Anemia
[22] A Agarwal A Aponte-Mellado B J Premkumar A Shamanand S Gupta ldquoThe effects of oxidative stress on female repro-duction a reviewrdquo Reproductive Biology and Endocrinology vol10 article 49 2012
[23] M Giergiel M Lopucki N Stachowicz and M KankoferldquoThe influence of age and gender on antioxidant enzymeactivities in humans and laboratory animalsrdquoAging Clinical andExperimental Research vol 24 pp 551ndash559 2012
[24] Q Shazia Z H Mohammad T Rahman and H U ShekharldquoCorrelation of oxidative stress with serum trace element levelsand antioxidant enzyme status in Beta thalassemia majorpatients a review of the literaturerdquo Anemia vol 2012 ArticleID 270923 7 pages 2012
[25] M Y Abdalla M Fawzi S R Al-Maloul N El-Banna R FTayyem and I M Ahmad ldquoIncreased oxidative stress and ironoverload in Jordanian120573-thalassemic childrenrdquoHemoglobin vol35 no 1 pp 67ndash79 2011
[26] R A Ghone K M Kumbar A N Suryakar R V Katkam andN G Joshi ldquoOxidative stress and disturbance in antioxidantbalance in beta thalassemia majorrdquo Indian Journal of ClinicalBiochemistry vol 23 no 4 pp 337ndash340 2008
[27] MA Livrea L Tesoriere AM Pintaudi et al ldquoOxidative stressand antioxidant status in 120573-thalassemia major iron overloadand depletion of lipid-soluble antioxidantsrdquo Blood vol 88 no9 pp 3608ndash3614 1996
[28] S-S Chiou T-T Chang S-P Tsai et al ldquoLipid peroxidationand antioxidative status in 120573-thalassemia major patients withor without hepatitis C virus infectionrdquo Clinical Chemistry andLaboratory Medicine vol 44 no 10 pp 1226ndash1233 2006
[29] A Agarwal and S S Allamaneni ldquoRole of free radicals in femalereproductive diseases and assisted reproductionrdquo ReproductiveBioMedicine Online vol 9 no 3 pp 338ndash347 2004
[30] E H Ruder T J Hartman J Blumberg and M B GoldmanldquoOxidative stress and antioxidants exposure and impact onfemale fertilityrdquoHuman Reproduction Update vol 14 no 4 pp345ndash357 2008
[31] A Agarwal S Gupta L Sekhon and R Shah ldquoRedox con-siderations in female reproductive function and assisted repro-duction from molecular mechanisms to health implicationsrdquoAntioxidants amp Redox Signaling vol 10 no 8 pp 1375ndash14032008
[32] P J Devine S D Perreault and U Luderer ldquoRoles of reactiveoxygen species and antioxidants in ovarian toxicityrdquo Biology ofReproduction vol 86 no 2 article 27 2012
[33] K H Al-Gubory C Garrel P Faure and N Sugino ldquoRolesof antioxidant enzymes in corpus luteum rescue from reac-tive oxygen species-induced oxidative stressrdquo ReproductiveBiomedicine Online vol 25 no 6 pp 551ndash560 2012
[34] A Agarwal A Aponte-Mellado B J Premkumar A Shamanand S Gupta ldquoThe effects of oxidative stress on female repro-duction a reviewrdquo Reproductive Biology and Endocrinology vol10 article 49 2012
[35] S Defrere R Gonzalez-Ramos J-C Lousse et al ldquoInsightsinto iron and nuclear factor-kappa B (NF-120581B) involvement inchronic inflammatory processes in peritoneal endometriosisrdquoHistology and Histopathology vol 26 no 8 pp 1083ndash1092 2011
[36] A van Langendonckt F Casanas-Roux and J Donnez ldquoOxida-tive stress and peritoneal endometriosisrdquo Fertility and Sterilityvol 77 no 5 pp 861ndash870 2002
[37] M Appasamy E Jauniaux P Serhal A Al-Qahtani N PGroome and S Muttukrishna ldquoEvaluation of the relationshipbetween follicular fluid oxidative stress ovarian hormones and
response to gonadotropin stimulationrdquo Fertility and Sterilityvol 89 no 4 pp 912ndash921 2008
[38] Y Asano ldquoAge-related accumulation of non-heme ferric andferrous iron in mouse ovarian stroma visualized by sensitivenon-heme iron histochemistryrdquo The Journal of Histochemistryamp Cytochemistry vol 60 no 3 pp 229ndash242 2012
[39] M K Al-Azemi A E Omu T Fatinikun N Mannazhathand S Abraham ldquoFactors contributing to gender differences inserum retinol and 120572-tocopherol in infertile couplesrdquo Reproduc-tive BioMedicine Online vol 19 no 4 pp 583ndash590 2009
[40] M K Kim J W Lee K H Baek et al ldquoEndocrinopathies intransfusion-associated iron overloadrdquo Clinical Endocrinologyvol 78 no 2 pp 271ndash277 2013
[41] L M Hempenius P S van Dam J J Marx and H PKoppeschaar ldquoMineralocorticoid status and endocrine dys-function in severe hemochromatosisrdquo Journal of Endocrinolog-ical Investigation vol 22 no 5 pp 369ndash376 1999
[42] J M Vasquez and R B Greenblatt ldquoPituitary responsiveness toluteinizing-hormone-releasing hormone in different reproduc-tive disorders a reviewrdquo Journal of ReproductiveMedicine for theObstetrician and Gynecologist vol 30 no 8 pp 591ndash600 1985
[43] I Paris M Hermans and M Buysschaert ldquoEndocrine compli-cations of genetic hemochromatosisrdquo Acta Clinica Belgica vol54 no 6 pp 334ndash345 1999
[44] W Stremmel C Niederau M Berger H-K Kley H-LKruskemper and G Strohmeyer ldquoAbnormalities in estrogenandrogen and insulin metabolism in idiopathic hemochro-matosisrdquo Annals of the New York Academy of Sciences vol 526pp 209ndash223 1988
[45] W R Meyer K A Hutchinson-Williams E E Jones and A HDecherney ldquoSecondary hypogonadism in hemochromatosisrdquoFertility and Sterility vol 54 no 4 pp 740ndash742 1990
[46] L J Siemons and C H Mahler ldquoHypogonadotropic hypogo-nadism in hemochromatosis recovery of reproductive functionafter iron depletionrdquo The Journal of Clinical Endocrinology andMetabolism vol 65 no 3 pp 585ndash587 1987
[47] J H McDermott and C H Walsh ldquoHypogonadism in hered-itary hemochromatosisrdquo The Journal of Clinical Endocrinologyand Metabolism vol 90 no 4 pp 2451ndash2455 2005
[48] G Kontogeorgos S Handy K Kovacs E Horvath and BW Scheithauer ldquoThe anterior pituitary in hemochromatosisrdquoEndocrine Pathology vol 7 no 2 pp 159ndash164 1996
[49] A Piperno M R Rivolta R Drsquoalba et al ldquoPreclinical hypog-onadism in genetic hemochromatosis in the early stage ofthe disease evidence of hypothalamic dysfunctionrdquo Journal ofEndocrinological Investigation vol 15 no 6 pp 423ndash428 1992
[50] K SiminoskiM Drsquocosta and P GWalfish ldquoHypogonadotropichypogonadism in idiopathic hemochromatosis evidence forcombined hypothalamic and pituitary involvementrdquo Journal ofEndocrinological Investigation vol 13 no 10 pp 849ndash853 1990
[51] K E Oerter G A Kamp P J Munson A W Nienhuis F GCassorla and P K Manasco ldquoMultiple hormone deficienciesin children with hemochromatosisrdquo The Journal of ClinicalEndocrinology and Metabolism vol 76 no 2 pp 357ndash361 1993
[52] L J Noetzli A Panigrahy S D Mittelman et al ldquoPituitaryiron and volume predict hypogonadism in transfusional ironoverloadrdquo American Journal of Hematology vol 87 no 2 pp167ndash171 2012
[53] R Chatterjee and M Katz ldquoReversible hypogonadotrophichypogonadism in sexually infantile male thalassaemic patientswith transfusional iron overloadrdquo Clinical Endocrinology vol53 no 1 pp 33ndash42 2000
Anemia 9
[54] M Berkovitch T Bistritzer S D Milone K Perlman WKucharczyk and N F Olivieri ldquoIron deposition in the anteriorpituitary in homozygous beta-thalassemia MRI evaluationand correlation with gonadal functionrdquo Journal of PediatricEndocrinology amp Metabolism vol 13 no 2 pp 179ndash184 2000
[55] S Arguelles M Cano A Machado and A Ayala ldquoEffect ofaging and oxidative stress on elongation factor-2 in hypothala-mus and hypophysisrdquo Mechanisms of Ageing and Developmentvol 132 no 1-2 pp 55ndash64 2011
[56] D Gonzalez-Duarte A Madrazo-Atutxa A Soto-Moreno andA Leal-Cerro ldquoMeasurement of oxidative stress and endothe-lial dysfunction in patients with hypopituitarism and severedeficiency adult growth hormone deficiencyrdquo Pituitary vol 15no 4 pp 589ndash597 2012
[57] A Birkenfeld A W Goldfarb E A Rachmilewitz J GSchenker andEOkon ldquoEndometrial glandular haemosiderosisin homozygous beta-thalassaemiardquo European Journal of Obstet-rics Gynecology and Reproductive Biology vol 31 no 2 pp 173ndash178 1989
[58] S T Singer N Sweeters O Vega A Higa E Vichinsky andM Cedars ldquoFertility potential in thalassemia major womencurrent findings and future diagnostic toolsrdquo Annals of the NewYork Academy of Sciences vol 1202 pp 226ndash230 2010
[59] T Dissayabutra P Tosukhowong and P Seksan ldquoThe benefitsof vitamin C and vitamin E in children with beta-thalassemiawith high oxidative stressrdquo Journal of the Medical Association ofThailand vol 88 supplement 4 pp S317ndash321 2005
[60] C Weeraphan C Srisomsap D Chokchaichamnankit et alldquoRole of curcuminoids in ameliorating oxidative modificationin beta-thalassemiaHb E plasma proteomerdquo The Journal ofNutritional Biochemistry vol 24 no 3 pp 578ndash585 2012
[61] E Vichinsky ldquoEmerging ldquoArdquo therapies in hemoglobinopathiesagonists antagonists antioxidants and argininerdquo HematologyAmerican Society Hematology Education Program vol 2012 no1 pp 271ndash275 2012
[62] C Mora-Esteves and D Shin ldquoNutrient supplementationimproving male fertility fourfoldrdquo Seminars in ReproductiveMedicine vol 31 no 4 pp 293ndash300 2013
[63] G J Kontoghiorghes A Efstathiou M Kleanthous YMichaelides and A Kolnagou ldquoRiskbenefit assessmentadvantages over other drugs and targeting methods in the useof deferiprone as a pharmaceutical antioxidant in iron loadingand non iron loading conditionsrdquo Hemoglobin vol 33 no 5pp 386ndash397 2009
[64] U R Kuppusamy and J A Tan ldquoChelation therapy withdesferrioxamine does not normalize ferritin level but attenu-ates oxidative damage and improves total antioxidant level inMalaysian Chinese beta-thalassaemia major patientsrdquoTheWestIndian Medical Journal vol 60 no 1 pp 3ndash8 2011
[65] P B Walter E A Macklin J Porter et al ldquoInflammationand oxidant-stress in 120573-thalassemia patients treated with ironchelators deferasirox (ICL670) or deferoxamine an ancillarystudy of the Novartis CICL670A0107 trialrdquo Haematologica vol93 no 6 pp 817ndash825 2008
[66] V Fenkci S Fenkci M Yilmazer and M Serteser ldquoDecreasedtotal antioxidant status and increased oxidative stress in womenwith polycystic ovary syndrome may contribute to the risk ofcardiovascular diseaserdquo Fertility and Sterility vol 80 no 1 pp123ndash127 2003
[67] C Tatone M C Carbone S Falone et al ldquoAge-dependentchanges in the expression of superoxide dismutases and catalaseare associated with ultrastructural modifications in human
granulosa cellsrdquoMolecular Human Reproduction vol 12 no 11pp 655ndash660 2006
[68] F Gonzalez N S Rote J Minium and J P Kirwan ldquoReactiveoxygen species-induced oxidative stress in the developmentof insulin resistance and hyperandrogenism in polycysticovary syndromerdquo The Journal of Clinical Endocrinology andMetabolism vol 91 no 1 pp 336ndash340 2006
[69] G Basta G Lazzerini M Massaro et al ldquoAdvanced gly-cation end products activate endothelium through signal-transduction receptor RAGE a mechanism for amplification ofinflammatory responsesrdquo Circulation vol 105 no 7 pp 816ndash822 2002
[70] E Devangelio F Santilli G Formoso et al ldquoSoluble RAGE intype 2 diabetes association with oxidative stressrdquo Free RadicalBiology and Medicine vol 43 no 4 pp 511ndash518 2007
[71] G Basta A M Schmidt and R de Caterina ldquoAdvancedglycation end products and vascular inflammation implica-tions for accelerated atherosclerosis in diabetesrdquoCardiovascularResearch vol 63 no 4 pp 582ndash592 2004
[72] R Meerwaldt T Links C Zeebregts R Tio J-L Hillebrandsand A Smit ldquoThe clinical relevance of assessing advanced gly-cation endproducts accumulation in diabetesrdquo CardiovascularDiabetology vol 7 article 29 2008
[73] H Unoki and S Yamagishi ldquoAdvanced glycation end productsand insulin resistancerdquo Current Pharmaceutical Design vol 14no 10 pp 987ndash989 2008
[74] E Diamanti-Kandarakis C Piperi A Kalofoutis and GCreatsas ldquoIncreased levels of serum advanced glycation end-products in women with polycystic ovary syndromerdquo ClinicalEndocrinology vol 62 no 1 pp 37ndash43 2005
[75] D R Mccance D G Dyer J A Dunn et al ldquoMaillardreaction products and their relation to complications in insulin-dependent diabetes mellitusrdquo Journal of Clinical Investigationvol 91 no 6 pp 2470ndash2478 1993
[76] R Singh A Barden TMori and L Beilin ldquoAdvanced glycationend-products a reviewrdquoDiabetologia vol 44 no 2 pp 129ndash1462001
[77] E Diamanti-Kandarakis A Piouka S Livadas et al ldquoAnti-mullerian hormone is associated with advanced glycosylatedend products in lean women with polycystic ovary syndromerdquoEuropean Journal of Endocrinology vol 160 no 5 pp 847ndash8532009
[78] R Chatterjee and R Bajoria ldquoNew concept in natural historyand management of diabetes mellitus in thalassemia majordiabetes and thalassaemiardquo Hemoglobin vol 33 supplement 1pp S127ndashS130 2009
[79] G Paolisso M R Tagliamonte M R Rizzo and D GiuglianoldquoAdvancing age and insulin resistance new facts about anancient historyrdquo European Journal of Clinical Investigation vol29 no 9 pp 758ndash769 1999
[80] N Sattarahmady H Heli and A A Moosavi-Movahedi ldquoDes-feral as improving agent for hemoglobin fructation structuraland functional impactsrdquo The Protein Journal vol 31 no 8 pp651ndash655 2012
[81] E Fibach and E A Rachmilewitz ldquoThe role of antioxidantsand iron chelators in the treatment of oxidative stress inthalassemiardquo Annals of the New York Academy of Sciences vol1202 pp 10ndash16 2010
[82] L M Compagno ldquoCaring for adults with thalassemia in apediatric worldrdquo Annals of the New York Academy of Sciencesvol 1054 pp 266ndash272 2005
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

2 Anemia
therapeutic strategies is also discussed which could coun-teract iron-induced OS and preserve BTM femalesrsquo fertilitycapacity
2 BTM and Fertility Up-to-Date
BTM is a severe transfusion-dependent anemia that causesinfertility mainly due to iron deposition to endocrine organsafter overtransfusion [7] Spontaneous fertility can occurin well-chelated and transfused patients but the majorityare infertile due to HH and need assisted reproductivetechniques (ART) Safarinejad has previously evaluated thehypothalamic-pituitary-ovarian axis in female patients withBTM [8] In the thalassemic group the baseline and peaklevels after GnRH test of luteinizing hormone (LH) follicle-stimulating hormone (FSH) and estradiol were significantlylower than those in the control group [8] However ovarianfunction has been proposed to bemerely preserved inwomensuffering from primary or secondary amenorrhea (PA andSA resp) as they become able to conceive following a closelymonitored stimulation therapy [4] Overall the report ofa large number of successful pregnancies so far is highlyindicative of the relative safety of pregnancy in the iron-adjusted BTM woman [4] The iron-induced effect seemsto have a central role in the pathogenesis of the decreasedreproductive capacity [9]
Ovulation induction with gonadotropin has been suffi-ciently studied [10] Skordis et al have previously estimatedthe frequency of fertility among 50 women with BTM ofwhich 7 had PA 9 had SA and 34 had normal menstrualfunction (NM) [11] In all patients with PA and SA thepregnancies were induced while in most patients with NMpregnancies were achieved spontaneously [11] Additionallyin a previously published study Danesi et al showed thatby proper pharmacological stimulation the steroidogenicfunction of the gonads and even ovulation can be reinstated inhypogonadal thalassemic women [12] More recently Origaet al suggested that in women with HH gonadal functionis usually intact and fertility is usually retrievable [3] In thisstudy 46 women with BTM (58 pregnancies) were includedwhile conception was achieved after gonadotrophin-inducedovulation in 33 of them [3] Moreover Bajoria et al haverecently supported the feasibility and safety of pregnancy infemales with BTM reporting their experience on pregnancyfollowing ART in 11 women with BTM who had HH withfunctionally intact ovaries [13] However successful preg-nancy and fertility were also suggested to be feasible in BTMpatients with diminished gonadal reserves [14] The safety ofpregnancy for both mothers with BTM and their babies withproper care and guidance has been repeatedly proposed byseveral studies even in the case of intensive transfusion andchelation treatment [7 15 16] Meanwhile human GH as anadjunct to hMG and hCG seemed to be a sensible approachin the treatment of infertile homozygous BTM patients [17]
Based on the above it seems that irrespectively of thespontaneous or induced ovulation the current evidence-based knowledge on the outcome of attempted pregnancies
Iron deposition
Iron overload
Hypothalamus
Pituitary
Infertility
Increasedoxidative stress
Prooxidants
Alteration inserum traceelements andantioxidantenzymes
Antioxidants
Ovaries
Figure 1 Infertility in female patients with BTM seems to beoriginated mainly by the direct and the indirect effect of ironoverload The combined effect of iron deposition and increasedOS (because of a significant prooxidantsantioxidants imbalance)results in the dysfunction of the female reproductive axis
in BTM female patients is optimistic Also the infertil-ity observed in this group of patients is probably mostlyattributed to impaired hypothalamic-pituitary-ovarian axisand less to gonadal dysfunction However there are minimaldata directly associating the role of iron iron-induced OSand antioxidant supplementation with the fertility potentialof these patients
3 Iron and Pathophysiology of BTM Infertility
Infertility in women with BTM is assumed to be mainlycaused by the direct or indirect effect of iron on thehypothalamic-pituitary-ovarian axis and the female repro-ductive system Indirect evidence suggests that the directeffect of iron is probably related to its direct deposition onthe hypothalamic-pituitary axis and the female reproductivesystemwhile direct evidence suggests that its indirect effect ismostly attributed to the iron-inducedOS (Figure 1) Howeverthere are limited data evaluating the pathophysiology ofiron-induced compromised fertility in which there is noclear discrimination between direct or indirect iron effectsNevertheless the most suitable model for speculating thedirect and indirect effect of iron on BTM womenrsquos fertilitycapacity is the model of hemochromatosis which will befurther discussed below Also the iron-mediated effect onfertility could be discriminated in its hypothalamic-pituitaryeffect and in its effect on the female reproductive system
31 Increased Oxidative Stress in BTMPatients BTMpatientsare under continuous blood transfusion which leads to aniron overload with a resultant increase in NTBI that causesgreater tissue toxicity than iron in other forms [2] Anothersource of iron accumulation results from increased duodenaliron absorption due to decreased expression of hepcidinthe main regulator of iron homeostasis [6] Iron generates
Anemia 3
production of ROS via the Fenton reaction hence ironoverload disrupts the redox balance of the cells causingchronic OS [18] OS leads to lipid peroxidation of unsaturatedfatty acids in membranes of cells and organelles Cytotoxicbyproducts of lipid peroxidation such as malondialdehyde(MDA) and 4-hydroxy-21015840-nonenal are produced and theseimpair cellular function and protein synthesis and damageDNA [19] Furthermore a crucial component in the oxidantsusceptibility of the thalassemic RBC is the release of hemeand iron from the excessive unpaired alpha-globin chains[2] This release initiates self-amplifying redox reactionswhich deplete the cellular reduction potential (eg glu-tathioneGSH) oxidize additional hemoglobin and acceler-ate RBC destruction [2]
Oxidativeantioxidative balance is one of themost impor-tant factors for homeostasis When the balance of ROSand antioxidants is disrupted towards an overabundanceof ROS OS occurs [20] The generation of ROS is asteady-state cellular event in respiring cells while theiruncontrolled production often leads to damage of cellularmacromolecules (DNA protein and lipids) and other smallantioxidant molecules [21] A number of major enzymaticand nonenzymatic defense mechanisms exist to neutralizeand combat the damaging effects of these reactive sub-stances [22] The enzymic system functions by direct orsequential removal of ROS (superoxide dismutaseSODcatalaseCAT and glutathione peroxidaseGPx) thereby ter-minating their activities Nonenzymic defense consists ofscavengingmolecules that are endogenously produced (GSHubiquinols and uric acid) or derived from the diet such asvitamins C and E [21] These antioxidant nutrients occupydistinct cellular compartments and among them there isactive recycling Antioxidative systems which protect fromperoxidative damage are also supposed to be under hormonalinfluence while antioxidative enzymes require the presenceof microelements in their active centers as well as concertaction of nonenzymatic antioxidants which support enzymesin their scavenging action [23]Meanwhile diet seems to havean impact on antioxidative system which requires appro-priate supplementation inmicroelements and vitamins for itseffective function leading to scavenging excess of free radi-cals [23]
According to the current evidence-based knowledge asignificant prooxidantsantioxidants imbalance with subse-quent increased OS exists in patients with BTM which ismainly caused by tissue injury due to overproduction of freeradicals by secondary iron overload alteration in serum traceelements and alteration in antioxidant enzymes level [24](Figure 1) The results of Wassem et al revealed that thelevels of vitamin E and antioxidant enzymes GPx and SODwere significantly lowered in BTM patients as comparedwith the control group indicating that thalassemics are ina state of enhanced OS [2] Another study revealed thatplasma thiobarbituric acid (TBA) reactive substances wereelevated in BTM children compared to controls togetherwith compensatory increase in SOD activity and decrease inCAT activity [25] At the same study serum ferritin showeda positive correlation with elevated TBA reactive substancesand SOD suggesting that iron overload is involved in the OS
shown in cells [25] A significant increase in the levels of lipidperoxide and iron and a significant decrease in the levels ofvitamin E total antioxidant capacity and total iron bindingcapacity were observed in a different study [26] suggestingthat OS and reduced antioxidant defense mechanism play animportant role in pathogenesis of BTM [26] FurthermoreLivrea et al have previously suggested that the measure-ment of peroxidation products matched with evaluation ofantioxidants may be a simple measure of iron toxicity inthalassemia in addition to the conventional indices of ironstatus [27] Their study showed that the mean concentrationsof conjugated diene lipid hydroperoxides (CD) lipoperoxidesevaluated as (MDATBA) adducts and protein carbonylsincreased about twofold with respect to control A net dropin the concentration of ascorbate vitamin E vitamin A beta-carotene and lycopene was also observed Serum levels ofvitamin E were inversely correlated with ferritin suggesting amajor consumption of this antioxidant under iron overloadwhile serum levels of vitamin E vitamin A and lycopenewere inversely correlated with the levels of transminases [27]On the other hand their results pointed out that the iron-induced liver damage in thalassemia may play a major rolein the depletion of lipid-soluble antioxidants [27] Later onChiou et al indicated that excessive lipid peroxidation and aprofound depletion of plasma vitaminsA E andC levels existin patients with BTM thus antioxidant supplementation forthe purpose of alleviating the OS may be warranted [28]They also found that HCV infection did play some role inaggravating the depletion of plasma vitamins E and C levelsin the BTM patients while it did not seem to alter the levelsof reduced GSH as well as antioxidant enzyme activities [28]
32 The Possible Impact of Oxidative Stress on BTM FemalesrsquoFertility Potential Although there is no direct evidence-based publication correlating the iron-inducedOSwith BTMwomenrsquos infertility existing published data on non-BTMpatients only permit the correlation of OS (not specificallyproduced through iron overload) with normal and abnormalprocesses of the female reproductive system Also there isno available publication connecting iron-induced OS withspecific altered signaling events in hypothalamic-pituitary-gonadal axis which subsequently could lead to infertilityThus until now only indirect evidence exists which supportsthe hypothesis that iron-induced OS is the main causal agentfor infertility in women with BTMThis is maybe happeningnot only through iron deposition and iron-induced OS invarious endocrine organs such as hypothalamus pituitaryand female reproductive system but also through its indirecteffect on other organs such as liver and pancreas contribut-ing to the impaired metabolism of hormones and serumantioxidants
Recently ROS have been shown to have an important rolein the normal functioning of reproductive system and in thepathogenesis of infertility in females [29] OS develops whenthere is an imbalance between the generation of ROS andthe scavenging capacity of antioxidants in the reproductivetract while it affects both natural and assisted fertility [29]ROS affect multiple physiological processes from oocyte
4 Anemia
maturation to fertilization embryo development and preg-nancy [20] There is sufficient evidence to hypothesize thatdietary antioxidants and OS may influence the timing andmaintenance of a viable pregnancy [30] Also physiologicallevels of ROS play an important regulatory role throughvarious signaling transduction pathways in folliculogenesisoocyte maturation endometrial cycle luteolysis implanta-tion embryogenesis and pregnancy [31] Proper functioningof the ovary is critical to maintain fertility and overall healthand ovarian function depends on the maintenance andnormal development of ovarian follicles [32] The potentialimpact of OS on the wellbeing of primordial growing andpreovulatory follicles as well as oocytes and early embryosexamining cell types and molecular targets has been exten-sively reviewed [32] Meanwhile ROS-induced apoptotic celldeath is involved in the mechanisms of corpus luteum (CL)regression that occurs at the end of the nonfertile cycle [33]
The role of OS in female reproduction is becomingincreasingly important as recent evidence suggests that itplays a part in conditions such as polycystic ovary syndrome(PCOS) endometriosis unexplained fertility spontaneousabortions preeclampsia hydatidiform mole embryopathiespreterm labor and intrauterine growth retardation [31] Agar-wal et al have recently reviewed the role of OS in normal andabnormal female reproductive physiological processes ana-lyzing the exact mechanisms of redox cell signaling and thepathophysiology of OS-related reproductive diseases [34] Aspecial comment should be made on endometriosis patientswhere iron overload has been demonstrated in the differentcompartments of the peritoneal cavity (peritoneal fluidendometriotic lesions peritoneum and macrophages) [35]This iron overload affects numerous mechanisms involvedin endometriosis development [35] Iron-induced OS maybe involved in endometriosis-associated infertility and mayplay a role in the regulation of the expression of genesencoding immunoregulators cytokines and cell adhesionmolecules implicated in the pathogenesis of endometriosis[36] Moreover a recent study investigated the relation-ship between OS and the underlying causes of infertilitypreovulatory ovarian hormones and ovarian response togonadotropin stimulation in patients undergoing ART [37]There was no significant relationship between plasma orfollicular fluid (FF) total antioxidant capacity (TAC) and theunderlying etiology of infertility [37] However there was astatistically significant positive association between FF E(2)levels and TAC OS has an impact on the production ofgranulosa cell steroid hormones in particular E(2) which isan important predictor of ovarian response [37] Thus thepossible impaired ovarian response in BTM women couldbe probably caused by dysregulation in the production ofgranulosa cell steroid hormones such as E(2) Meanwhile ithas been suggested that OSmodulates the age-related declinein fertility [20] Additionally a recent study indicated thatnonheme iron accumulation on ovarian stromal tissue maybe related to aging of the ovary due to increasing OS [38]Theage-related decline in fertility due to OS has a special impactin our group of patients because of their increased age aver-age due to significant improvements in chelation treatmentmodalities Furthermore remarkable is another study which
evaluated retinol and alpha-tocopherol natural antioxidantsthat inhibit lipid peroxidation and protect against cell damageinduced by OS and revealed that lower concentrations ofthese natural antioxidants were associated with abnormalsemen parameters in men and anovulation in women [39]
4 Evidence-Based Effect of Iron Overloadand Iron-Induced OS on Hypothalamic-Pituitary-Gonadal Axis and FemaleReproductive System
Although there are limited data directly correlating iron over-load with iron-induced OS on BTM femalesrsquo hypothalamic-pituitary-gonadal axis and ovarian reserve indirect conclu-sions could be obtained through the model of hemochro-matosis
41 The Model of Hemochromatosis Endocrinopathies arecommon in transfusion-associated haemochromatosis [40]while HH is the most frequent endocrine abnormality inhemochromatosis [41] The gonadotropin responsiveness to100 micrograms of LHRH was impaired or absent in patientswith hemochromatosis [42] Also in a cohort of 115 patientssuffering from genetic hemochromatosis hypogonadismwasevidenced in 42 of them inmost of which it was consideredas secondary to pituitary lesions as assessed by GnRH tests[43] Moreover in male patients with idiopathic hemochro-matosis testicular atrophy has been suggested to be causedby insufficient secretion of gonadotropins due to the selectiveaccumulation of iron in gonadotropic cells of the pituitarygland [44] Meanwhile subnormal gonadotropin responsesto GnRH but normal ovarian reserve as shown by normalfollicular stimulation with hMG were reported in a case ofHH in a female with biopsy-proven hemochromatosis [45]In another case report recovery of reproductive functionsdocumented by hormone measurements testicular biopsyand semen analysis was observed in a 37-year-old man withHH due to idiopathic hemochromatosis after phlebotomy[46] It has been also proposed that subjects with lesserdegrees of hepatic siderosis at diagnosis are unlikely todevelop hypogonadism [47] Furthermore the pituitary ofa 69-year-old man with hemochromatosis had been pre-viously removed at autopsy and was studied by histologyhistochemistry immunocytochemistry electron microscopyand X-ray diffraction [48] Preferential localization of irondeposits was demonstrated in gonadotrophs which at theultrastructural level displayed selective severe cellular injury[48] X-ray diffraction revealed the deposition of iron-accumulated lysosomes while iron storage was also notedin stellate cells [48] It should be also noted that in a groupof 7 young male patients with genetic hemochromatosis thenormal or high increments of LH after LHRH stimulationsuggested that secretion capacity of LH was intact andthat hypothalamic dysfunction could be responsible for theobserved preclinical gonadal deficiency [49] A similar resultwas obtained in another male patient where although thepituitary secretion of LH was normal in response to GnRHstimulation clomiphene administration did not produce an
Anemia 5
increase in LH and FSH suggesting that there was a defect inthe hypothalamic GnRH response [50]
In agreement with the hemochromatosis model abnor-malities of the hypothalamic-pituitary-gonadal axis are themost common endocrine abnormalities in patients withBTM as they require multiple blood transfusions leading tohemochromatosis [51] Thus based on the model of hemo-chromatosis that resembles iron-overloaded patients withBTM it seems that abnormalities of ovulation and menstru-ation in these patients are most likely because of inadequatepituitary responsiveness to GnRH [45]
42 Direct and Indirect Evidence for the Hypothalamic-Pitui-tary and the Gonadal Effect of Iron Patients with transfu-sional iron overload begin to develop pituitary iron overloadin the first decade of life however clinically significantvolume loss was not observed until the second decadeof life [52] Pituitary iron overload and volume loss wereindependently predictive of hypogonadism [52] Pituitary R2correlated significantly with serum ferritin as well as liverpancreatic and cardiac iron deposition by MRI [52] Manypatients with moderate-to-severe pituitary iron overloadretained normal gland volume and function representing apotential therapeutic window [52] According to a differentstudy BTM patients with severe organ damage and ironoverload are likely to be apulsatile with irreversible damageto their hypothalamic-pituitary axis while those with less-severe iron overload are likely to have potentially reversibleHH [53]The same study suggested that gonadotrophin pulseparameters rather than the gonadotrophin response to aGnRH bolus following prolonged pulsatile GnRH infusionmay be more useful in discriminating reversible from irre-versible HH [53] Furthermore in a study of 33 patients above15 years of age with transfusion-dependent BTM and ironoverload anterior pituitary function (GnRH stimulation test)correlated well with MRI results However no correlationwas found between the MRI measurements the GnRHstimulation test and the clinical status of the patients as 28out of the 33 patients achieved normal puberty [54] Anotherpossible mechanism of iron effect on hypothalamic-pituitaryaxis is through iron-induced OS with subsequent alterationson elongation factor-2 (eEF-2) levels The hypothalamic-pituitary system secretes peptide hormones whose synthesisrequires the integrity of the translation machinery Amongthe possible causes of the decline of translation in oldanimals are the modifications of eEF-2 [55] Iron-induced OScould be involved in the alterations of eEF-2 which formsadducts with MDA and 4-hydroxynonenal (HNE) [55] Thealterations of eEF-2 levels secondary to lipid peroxidationand adduct formation with these aldehydes could contributeto the suboptimal hormone production from these tissues[55] Moreover the possible concurrent GH deficiency maypotentiate the already present OS as patients with GHdeficiency have an increased degree of OS and endothelialdysfunction which possibly acts synergistically with iron-induced OS [56] Thus although there is limited evidenceon the exact pathophysiological mechanisms of iron effecton hypothalamic-pituitary axis it seems to be the basic
pathogenetic cause of the impaired hypothalamic-pituitarysystem
Meanwhile according to our knowledge only one studyexists which proves the iron deposition on the femalereproductive system in patients with BTM This particularstudy obtained histopathological evidence that depositionof haemosiderin occurred in the endometrial glandularepithelium of three patients with BTM [57] This depositionwas mainly evident in the apical part of these cells abovethe nuclei and should be taken into consideration as acontributing factor to the infertility in these patients byaltering endometrial receptivity for implantation [57] In twopatients who received effective iron chelating treatment withdesferrioxamine the endometrial haemosiderin depositseither disappeared or were significantly reduced [57]
43 Available Studies Directly Correlating Iron and Its Impacton Fertility in Women with BTM The pathophysiology ofiron-induced compromised fertility in women with BTMwas only recently evaluated [9] Low gonadotropin secretionresulted in reduced ovarian antral follicle count and ovarianvolume but levels of antimullerian hormone (AMH) a sensi-tive marker for ovarian reserve independent of gonadotropineffect were mostly normal AMH correlated with NTBI sug-gesting a role of labile iron in the pathogenesis of decreasedreproductive capacity possibly occurring in parallel to car-diac iron toxicity as cardiac iron was associated with thepresence of amenorrhea and with NTBI levels Thus AMHwas suggested to be valuable for future studies aiming atimproved chelation for fertility preservation whereas NTBIand labile plasma iron was suggested to be valuable formonitoring iron effect on the reproductive system [9] Thesame research team explored the relationship between liveriron concentration (LIC) and fertility status in 26 females(mean 30 years old) with BTM Seventeen (65) of themexperienced PA or SA Levels of LHFSH and estradiol werelow or undetectable in 48 and 35 of patients respectivelyand did not correlate with age presence of amenorrhea andLIC The fact that LHFSH and estradiol commonly usedfor assessment of fertility potential in thalassemia had apoor predictive value addressed the need for utilization ofcurrent available methods for assessment of fertility capacityin thalassemia [58]
5 Potential Antioxidants in BTM
Considering all the above we suggest that the enhancedOS observed in iron-overloaded patients with BTM mayplay a significant role in their reduced reproductive abilityThe investigation of the proper antioxidants for fertility andpregnancy in BTM female patients which are recognized aspatients of increased OS is of great value and importanceThe increased age average of this group of patients underlinesthe increased importance of OS on the female reproductivesystem as it has been also connected with aging Howeverdespite the clear identification of the oxidativeantioxidativeimbalance in patients with BTM there are few studies
6 Anemia
evaluating the effect of different antioxidant supplementationin BTM-related morbidities such as infertility
51 Antioxidant Supplements Used in BTM The benefits ofvitamin C and vitamin E as antioxidant supplements inBTMchildren have been previously determined [59] Twentychildren who had laboratory confirmation of BTM at least 6months with history of packed red cell transfusion withoutiron chelation were recruited It was suggested that vitaminC plus vitamin E supplementations have benefits more thanvitamin E alone in promoting antioxidant status and mayenhance liver function as total bilirubin tends to decrease[59] Furthermore curcuminoids extracted from the spiceturmeric are known to have antioxidant and iron-chelatingproperties and have been proposed as a potential upstreamtherapy of thalassemiaWeeraphan et al have recently appliedproteomic techniques to study the protein profile and oxida-tive damage in the plasma of beta-thalassemiaHb E patientsbefore and after treatment with curcuminoids Their studyindicated the ameliorating role of curcuminoids towards OSand iron overload in the plasma proteome [60] Glutaminealpha-lipoic acid acetyl-L-carnitine and N-acetylcysteineare also recently being studied as antioxidant supplements forsickle cell disease and thalassemia [61] Finally the value ofantioxidant supplements in the elimination of iron-inducedOS and subsequent infertility issues could be speculatedby the fact that various antioxidants (such as carnitinevitamin C vitamin E selenium carotenoids glutathioneN-acetylcysteine zinc folic acid and coenzyme Q10) arevariably effective in OS-induced male-factor infertility withrespect to improving semen parameters and pregnancy rates[62]
52 Chelation Treatments as Antioxidants in BTM Differentstudies have also focused on the antioxidant capacity of differ-ent chelation treatment modalities Increased evidence fromin vitro in vivo and clinical studies suggest that deferiprone(L1) can be used as a potent pharmaceutical antioxidant bymobilizing labile iron and copper andor inhibiting theircatalytic activity in the formation of free radicals and OS intissue damage [63] In contrast to L1 both desferrioxamine(DFO) and deferasirox (DFRA) were suggested to havemajordisadvantages in their use in noniron loading conditionsdue to toxicity implications [63] Meanwhile a subsequentstudy indicated that DFO chelation therapy does not nor-malize ferritin levels but attenuates oxidative damage andimproves total antioxidant level in Malaysian Chinese BTMpatients [64] The objective of this research was to studythe oxidant-antioxidant indices in BTM patients who wereon desferrioxamine-chelation or without chelation therapyBlood was collected from 39 Chinese patients and 20 con-trols Plasma and peripheral blood mononuclear cell lysates(PBMC) were extracted and biochemical tests to evaluate OSwere performedOSwas evident in these patients as advancedoxidized protein products (AOPP) and lipid hydroperoxideswere elevated whereas glutathione peroxidase activity andthe ferric reducing antioxidant power (FRAP) were reducedThe catalase activity in the patientsrsquo PBMC was elevated
possibly as a compensatory mechanism for the reducedglutathione peroxidase activity in both red blood cells andPBMC The lower FRAP and higher AOPP levels in thenonchelated patients compared with the chelated patientswere indicative of a lower OS level in the chelated patients[64] An additional study which assessed whether oxidant-stress and inflammation in BTM could be controlled byDFRA as effectively as by DFO revealed equal effectivenessin decreasing iron burden and levels of the oxidative-stressmarker MDA [65]
53 The Possible Effect of Advanced Glycation End Products(AGEs) Regulation on BTM Womenrsquos Ovarian Function andFertility Recent data have shown that OS is involved in thepathophysiology of anovulation [20 66 67] While the roleof OS in ovulatory dysfunction has been sufficiently studied[29 68] advanced glycation end products (AGEs) have beenrecognized as mediators of increased OS [69 70] Advancedglycation end products (AGEs) are a heterogeneous group ofbioactive molecules formed by the nonenzymatic glycationof proteins lipids and nucleic acids [71] There is increasingevidence that AGEs play a pivotal role in atherosclerosis andin diabetes and its complications while AGE accumulationis a measure of cumulative metabolic and OS and mayso represent the ldquometabolic memoryrdquo [72] Engagement oftheir receptor RAGE with AGEs is shown to activate itsdownstream signaling and evoke OS and inflammation indiabetes [73] AGEs have been found to induce OS andconversely OS stimulates AGEs formation [74ndash76]
AGEs deposition in ovary dysregulate ovarian functionthrough the induction of androgen production as well as OSgeneration through the induction ofNF-K120573pathway leadingto increased production of atherogenic and inflammatorymolecules AGEs have been implicated in the developmentof insulin resistance hyperandrogenism and anovulationin polycystic ovary syndrome (PCOS) and seem to have acentral role in PCOS pathophysiology either as a marker ofOS or through their specific actions after their ligation totheir specific receptor RAGE [77] Furthermore there is sub-stantial evidence that insulin resistance constitutes one of themain pathophysiological mechanisms leading to anovulationand ovarian hyperandrogenism in PCOS patients Regardingthe above also that iron has been implicated in abnormalinsulin secretion in patients with BTM or hemochromatosis[44 78] and that OS might be responsible for a decline ininsulin-mediated glucose uptake in BTM patients leadingto insulin resistance [79] we consider that the evaluationof AGEs as markers of OS in relation to iron overloadinsulin resistance and ovulation potential would be of greatvalue Reducing AGEs in BTM females could probably havebeneficial effects in insulin resistance and ovulation potentialand thus in fertility potential Finally it is remarkable thatthe iron chelator Desferal had a retardation effect on thefunctional and structural changes of Hb during fructation[80] It could prevent the AGEs and carbonyl formations andhelix depletion during theHb fructation processMoreover itcould preserve peroxidase and esterase activities of fructated
Anemia 7
Hb similar to native Hb Therefore desferal could be intro-duced as an antiglycation drug to prevent theAGEs formation[80]
6 Conclusions
On the basis of all the presented data it can be concludedthatOS plays amajor role in the pathophysiology of infertilityin females with thalassemia This OS is mainly caused bytissue injury due to overproduction of free radicals bysecondary iron overload alteration in serum trace elementsand alteration in antioxidant enzymes level Consequentlythere is a rationale for iron chelation to eliminate the free-iron species which in this respect act like antioxidantsAntioxidants are also capable of ameliorating increased OSparameters and given together with iron chelators mayprovide a substantial improvement in the pathophysiologyof thalassemia [81] However there is no study evaluatingthe efficacy of antioxidant supplementation on BTMwomenrsquosfertility potential In agreement with previous suggestionswe consider that the application of treatment strategies thatwould reduceOS in the reproductive tract could help infertilewomen with diseases such as BTM that are caused byROSantioxidants imbalance [29] In general research isin progress to identify the mechanisms that are involvedin the etiology of female reproductive diseases caused byROS and to create effective strategies that can counteractOS [29] while few are the trials investigating antioxidantsupplementation in female reproduction [20] The admin-istration of selective antioxidants along with essential traceelements and minerals to reduce the extent of oxidativedamage and related complications such as infertility in BTMpatients still needs further evaluation [24] However beforeclinicians recommend antioxidants randomized controlledtrials with sufficient power are necessary to prove the efficacyof antioxidant therapeutic strategies in disorders of femalereproduction [20] such as BTMThis is strongly emerged bythe fact of prolonged survival and the newly recognized issuesand challenges that adults with BTM face [82]
References
[1] C Hershko ldquoPathogenesis and management of iron toxicity inthalassemiardquo Annals of the New York Academy of Sciences vol1202 pp 1ndash9 2010
[2] F Waseem K A Khemomal and R Sajid ldquoAntioxidant statusin beta thalassemia major a single-center studyrdquo Indian Journalof Pathology and Microbiology vol 54 no 4 pp 761ndash763 2011
[3] R Origa A Piga G Quarta et al ldquoPregnancy and 120573-thalassemia an Italian multicenter experiencerdquoHaematologicavol 95 no 3 pp 376ndash381 2010
[4] N Skordis L Petrikkos M Toumba et al ldquoUpdate on fertilityin thalassaemia majorrdquo Pediatric Endocrinology Reviews vol 2supplement 2 pp 296ndash302 2004
[5] M Toumba A Sergis C Kanaris and N Skordis ldquoEndocrinecomplications in patients with thalassaemia majorrdquo PediatricEndocrinology Reviews vol 5 no 2 pp 642ndash648 2007
[6] E A Rachmilewitz O Weizer-Stern K Adamsky et al ldquoRoleof iron in inducing oxidative stress in thalassemia can it be
prevented by inhibition of absorption and by antioxidantsrdquoAnnals of the New York Academy of Sciences vol 1054 pp 118ndash123 2005
[7] S Ansari A Azarkeivan and A Tabaroki ldquoPregnancy inpatients treated for beta thalassemia major in two centers(Ali Asghar Childrenrsquos Hospital and Thalassemia Clinic) out-come for mothers and newborn infantsrdquo Pediatric Hematology-Oncology vol 23 no 1 pp 33ndash37 2006
[8] M R Safarinejad ldquoReproductive hormones and hypothalamic-pituitary-ovarian axis in female patients with homozygous 120573-thalassemia majorrdquo Journal of Pediatric HematologyOncologyvol 32 no 4 pp 259ndash266 2010
[9] S T Singer E P Vichinsky G Gildengorin J van DisseldorpM Rosen and M I Cedars ldquoReproductive capacity in ironoverloaded women with thalassemia majorrdquo Blood vol 118 no10 pp 2878ndash2881 2011
[10] G Vizziello D Carone E Caroppo A Vitti A Pasquad-ibisceglie and G Drsquoamato ldquoOvulation induction with gona-dotropin in patients with thalassemia pretreated with pulsatileGnRH outcomerdquoMinerva Ginecologica vol 56 no 5 pp 485ndash487 2004
[11] N Skordis S Christou M Koliou N Pavlides and M Angas-tiniotis ldquoFertility in female patients with thalassemiardquo Journalof Pediatric Endocrinology and Metabolism vol 11 supplement3 pp 935ndash943 1998
[12] LDanesiM Scacchi AMMiragoli et al ldquoInduction of folliclematuration and ovulation by gonadotropin administration inwomen with 120573-thalassemiardquo European Journal of Endocrinol-ogy vol 131 no 6 pp 602ndash606 1994
[13] R Bajoria and R Chatterjee ldquoCurrent perspectives of fertilityand pregnancy in thalassemiardquoHemoglobin vol 33 supplement1 pp S131ndashS135 2009
[14] R Bajoria and R Chatterjee ldquoHypogonadotrophic hypogo-nadism and diminished gonadal reserve accounts for dys-functional gametogenesis in thalassaemia patients with ironoverload presenting with infertilityrdquoHemoglobin vol 35 no 5-6 pp 636ndash642 2011
[15] M Karagiorga-Lagana ldquoFertility in thalassemia the Greekexperiencerdquo Journal of Pediatric Endocrinology andMetabolismvol 11 supplement 3 pp 945ndash951 1998
[16] S M Tuck ldquoFertility and pregnancy in thalassemia majorrdquoAnnals of the New York Academy of Sciences vol 1054 pp 300ndash307 2005
[17] D Surbek A Koller and N Pavic ldquoSuccessful twin pregnancyin homozygous 120573-thalassemia after ovulation induction withgrowth hormone and gonadotropinsrdquo Fertility and Sterility vol65 no 3 pp 670ndash672 1996
[18] K Yamaguchi M Mandai S Toyokuni et al ldquoContents ofendometriotic cysts especially the high concentration of freeiron are a possible cause of carcinogenesis in the cysts throughthe iron-induced persistent oxidative stressrdquo Clinical CancerResearch vol 14 no 1 pp 32ndash40 2008
[19] M C Kew ldquoHepatic iron overload and hepatocellular carci-nomardquo Cancer Letters vol 286 no 1 pp 38ndash43 2009
[20] AAgarwal S Gupta andRK Sharma ldquoRole of oxidative stressin female reproductionrdquo Reproductive Biology and Endocrinol-ogy vol 3 article 28 2005
[21] A C Chan C K Chow and D Chiu ldquoInteraction of antiox-idants and their implication in genetic anemiardquo Proceedings ofthe Society for Experimental Biology and Medicine vol 222 no3 pp 274ndash282 1999
8 Anemia
[22] A Agarwal A Aponte-Mellado B J Premkumar A Shamanand S Gupta ldquoThe effects of oxidative stress on female repro-duction a reviewrdquo Reproductive Biology and Endocrinology vol10 article 49 2012
[23] M Giergiel M Lopucki N Stachowicz and M KankoferldquoThe influence of age and gender on antioxidant enzymeactivities in humans and laboratory animalsrdquoAging Clinical andExperimental Research vol 24 pp 551ndash559 2012
[24] Q Shazia Z H Mohammad T Rahman and H U ShekharldquoCorrelation of oxidative stress with serum trace element levelsand antioxidant enzyme status in Beta thalassemia majorpatients a review of the literaturerdquo Anemia vol 2012 ArticleID 270923 7 pages 2012
[25] M Y Abdalla M Fawzi S R Al-Maloul N El-Banna R FTayyem and I M Ahmad ldquoIncreased oxidative stress and ironoverload in Jordanian120573-thalassemic childrenrdquoHemoglobin vol35 no 1 pp 67ndash79 2011
[26] R A Ghone K M Kumbar A N Suryakar R V Katkam andN G Joshi ldquoOxidative stress and disturbance in antioxidantbalance in beta thalassemia majorrdquo Indian Journal of ClinicalBiochemistry vol 23 no 4 pp 337ndash340 2008
[27] MA Livrea L Tesoriere AM Pintaudi et al ldquoOxidative stressand antioxidant status in 120573-thalassemia major iron overloadand depletion of lipid-soluble antioxidantsrdquo Blood vol 88 no9 pp 3608ndash3614 1996
[28] S-S Chiou T-T Chang S-P Tsai et al ldquoLipid peroxidationand antioxidative status in 120573-thalassemia major patients withor without hepatitis C virus infectionrdquo Clinical Chemistry andLaboratory Medicine vol 44 no 10 pp 1226ndash1233 2006
[29] A Agarwal and S S Allamaneni ldquoRole of free radicals in femalereproductive diseases and assisted reproductionrdquo ReproductiveBioMedicine Online vol 9 no 3 pp 338ndash347 2004
[30] E H Ruder T J Hartman J Blumberg and M B GoldmanldquoOxidative stress and antioxidants exposure and impact onfemale fertilityrdquoHuman Reproduction Update vol 14 no 4 pp345ndash357 2008
[31] A Agarwal S Gupta L Sekhon and R Shah ldquoRedox con-siderations in female reproductive function and assisted repro-duction from molecular mechanisms to health implicationsrdquoAntioxidants amp Redox Signaling vol 10 no 8 pp 1375ndash14032008
[32] P J Devine S D Perreault and U Luderer ldquoRoles of reactiveoxygen species and antioxidants in ovarian toxicityrdquo Biology ofReproduction vol 86 no 2 article 27 2012
[33] K H Al-Gubory C Garrel P Faure and N Sugino ldquoRolesof antioxidant enzymes in corpus luteum rescue from reac-tive oxygen species-induced oxidative stressrdquo ReproductiveBiomedicine Online vol 25 no 6 pp 551ndash560 2012
[34] A Agarwal A Aponte-Mellado B J Premkumar A Shamanand S Gupta ldquoThe effects of oxidative stress on female repro-duction a reviewrdquo Reproductive Biology and Endocrinology vol10 article 49 2012
[35] S Defrere R Gonzalez-Ramos J-C Lousse et al ldquoInsightsinto iron and nuclear factor-kappa B (NF-120581B) involvement inchronic inflammatory processes in peritoneal endometriosisrdquoHistology and Histopathology vol 26 no 8 pp 1083ndash1092 2011
[36] A van Langendonckt F Casanas-Roux and J Donnez ldquoOxida-tive stress and peritoneal endometriosisrdquo Fertility and Sterilityvol 77 no 5 pp 861ndash870 2002
[37] M Appasamy E Jauniaux P Serhal A Al-Qahtani N PGroome and S Muttukrishna ldquoEvaluation of the relationshipbetween follicular fluid oxidative stress ovarian hormones and
response to gonadotropin stimulationrdquo Fertility and Sterilityvol 89 no 4 pp 912ndash921 2008
[38] Y Asano ldquoAge-related accumulation of non-heme ferric andferrous iron in mouse ovarian stroma visualized by sensitivenon-heme iron histochemistryrdquo The Journal of Histochemistryamp Cytochemistry vol 60 no 3 pp 229ndash242 2012
[39] M K Al-Azemi A E Omu T Fatinikun N Mannazhathand S Abraham ldquoFactors contributing to gender differences inserum retinol and 120572-tocopherol in infertile couplesrdquo Reproduc-tive BioMedicine Online vol 19 no 4 pp 583ndash590 2009
[40] M K Kim J W Lee K H Baek et al ldquoEndocrinopathies intransfusion-associated iron overloadrdquo Clinical Endocrinologyvol 78 no 2 pp 271ndash277 2013
[41] L M Hempenius P S van Dam J J Marx and H PKoppeschaar ldquoMineralocorticoid status and endocrine dys-function in severe hemochromatosisrdquo Journal of Endocrinolog-ical Investigation vol 22 no 5 pp 369ndash376 1999
[42] J M Vasquez and R B Greenblatt ldquoPituitary responsiveness toluteinizing-hormone-releasing hormone in different reproduc-tive disorders a reviewrdquo Journal of ReproductiveMedicine for theObstetrician and Gynecologist vol 30 no 8 pp 591ndash600 1985
[43] I Paris M Hermans and M Buysschaert ldquoEndocrine compli-cations of genetic hemochromatosisrdquo Acta Clinica Belgica vol54 no 6 pp 334ndash345 1999
[44] W Stremmel C Niederau M Berger H-K Kley H-LKruskemper and G Strohmeyer ldquoAbnormalities in estrogenandrogen and insulin metabolism in idiopathic hemochro-matosisrdquo Annals of the New York Academy of Sciences vol 526pp 209ndash223 1988
[45] W R Meyer K A Hutchinson-Williams E E Jones and A HDecherney ldquoSecondary hypogonadism in hemochromatosisrdquoFertility and Sterility vol 54 no 4 pp 740ndash742 1990
[46] L J Siemons and C H Mahler ldquoHypogonadotropic hypogo-nadism in hemochromatosis recovery of reproductive functionafter iron depletionrdquo The Journal of Clinical Endocrinology andMetabolism vol 65 no 3 pp 585ndash587 1987
[47] J H McDermott and C H Walsh ldquoHypogonadism in hered-itary hemochromatosisrdquo The Journal of Clinical Endocrinologyand Metabolism vol 90 no 4 pp 2451ndash2455 2005
[48] G Kontogeorgos S Handy K Kovacs E Horvath and BW Scheithauer ldquoThe anterior pituitary in hemochromatosisrdquoEndocrine Pathology vol 7 no 2 pp 159ndash164 1996
[49] A Piperno M R Rivolta R Drsquoalba et al ldquoPreclinical hypog-onadism in genetic hemochromatosis in the early stage ofthe disease evidence of hypothalamic dysfunctionrdquo Journal ofEndocrinological Investigation vol 15 no 6 pp 423ndash428 1992
[50] K SiminoskiM Drsquocosta and P GWalfish ldquoHypogonadotropichypogonadism in idiopathic hemochromatosis evidence forcombined hypothalamic and pituitary involvementrdquo Journal ofEndocrinological Investigation vol 13 no 10 pp 849ndash853 1990
[51] K E Oerter G A Kamp P J Munson A W Nienhuis F GCassorla and P K Manasco ldquoMultiple hormone deficienciesin children with hemochromatosisrdquo The Journal of ClinicalEndocrinology and Metabolism vol 76 no 2 pp 357ndash361 1993
[52] L J Noetzli A Panigrahy S D Mittelman et al ldquoPituitaryiron and volume predict hypogonadism in transfusional ironoverloadrdquo American Journal of Hematology vol 87 no 2 pp167ndash171 2012
[53] R Chatterjee and M Katz ldquoReversible hypogonadotrophichypogonadism in sexually infantile male thalassaemic patientswith transfusional iron overloadrdquo Clinical Endocrinology vol53 no 1 pp 33ndash42 2000
Anemia 9
[54] M Berkovitch T Bistritzer S D Milone K Perlman WKucharczyk and N F Olivieri ldquoIron deposition in the anteriorpituitary in homozygous beta-thalassemia MRI evaluationand correlation with gonadal functionrdquo Journal of PediatricEndocrinology amp Metabolism vol 13 no 2 pp 179ndash184 2000
[55] S Arguelles M Cano A Machado and A Ayala ldquoEffect ofaging and oxidative stress on elongation factor-2 in hypothala-mus and hypophysisrdquo Mechanisms of Ageing and Developmentvol 132 no 1-2 pp 55ndash64 2011
[56] D Gonzalez-Duarte A Madrazo-Atutxa A Soto-Moreno andA Leal-Cerro ldquoMeasurement of oxidative stress and endothe-lial dysfunction in patients with hypopituitarism and severedeficiency adult growth hormone deficiencyrdquo Pituitary vol 15no 4 pp 589ndash597 2012
[57] A Birkenfeld A W Goldfarb E A Rachmilewitz J GSchenker andEOkon ldquoEndometrial glandular haemosiderosisin homozygous beta-thalassaemiardquo European Journal of Obstet-rics Gynecology and Reproductive Biology vol 31 no 2 pp 173ndash178 1989
[58] S T Singer N Sweeters O Vega A Higa E Vichinsky andM Cedars ldquoFertility potential in thalassemia major womencurrent findings and future diagnostic toolsrdquo Annals of the NewYork Academy of Sciences vol 1202 pp 226ndash230 2010
[59] T Dissayabutra P Tosukhowong and P Seksan ldquoThe benefitsof vitamin C and vitamin E in children with beta-thalassemiawith high oxidative stressrdquo Journal of the Medical Association ofThailand vol 88 supplement 4 pp S317ndash321 2005
[60] C Weeraphan C Srisomsap D Chokchaichamnankit et alldquoRole of curcuminoids in ameliorating oxidative modificationin beta-thalassemiaHb E plasma proteomerdquo The Journal ofNutritional Biochemistry vol 24 no 3 pp 578ndash585 2012
[61] E Vichinsky ldquoEmerging ldquoArdquo therapies in hemoglobinopathiesagonists antagonists antioxidants and argininerdquo HematologyAmerican Society Hematology Education Program vol 2012 no1 pp 271ndash275 2012
[62] C Mora-Esteves and D Shin ldquoNutrient supplementationimproving male fertility fourfoldrdquo Seminars in ReproductiveMedicine vol 31 no 4 pp 293ndash300 2013
[63] G J Kontoghiorghes A Efstathiou M Kleanthous YMichaelides and A Kolnagou ldquoRiskbenefit assessmentadvantages over other drugs and targeting methods in the useof deferiprone as a pharmaceutical antioxidant in iron loadingand non iron loading conditionsrdquo Hemoglobin vol 33 no 5pp 386ndash397 2009
[64] U R Kuppusamy and J A Tan ldquoChelation therapy withdesferrioxamine does not normalize ferritin level but attenu-ates oxidative damage and improves total antioxidant level inMalaysian Chinese beta-thalassaemia major patientsrdquoTheWestIndian Medical Journal vol 60 no 1 pp 3ndash8 2011
[65] P B Walter E A Macklin J Porter et al ldquoInflammationand oxidant-stress in 120573-thalassemia patients treated with ironchelators deferasirox (ICL670) or deferoxamine an ancillarystudy of the Novartis CICL670A0107 trialrdquo Haematologica vol93 no 6 pp 817ndash825 2008
[66] V Fenkci S Fenkci M Yilmazer and M Serteser ldquoDecreasedtotal antioxidant status and increased oxidative stress in womenwith polycystic ovary syndrome may contribute to the risk ofcardiovascular diseaserdquo Fertility and Sterility vol 80 no 1 pp123ndash127 2003
[67] C Tatone M C Carbone S Falone et al ldquoAge-dependentchanges in the expression of superoxide dismutases and catalaseare associated with ultrastructural modifications in human
granulosa cellsrdquoMolecular Human Reproduction vol 12 no 11pp 655ndash660 2006
[68] F Gonzalez N S Rote J Minium and J P Kirwan ldquoReactiveoxygen species-induced oxidative stress in the developmentof insulin resistance and hyperandrogenism in polycysticovary syndromerdquo The Journal of Clinical Endocrinology andMetabolism vol 91 no 1 pp 336ndash340 2006
[69] G Basta G Lazzerini M Massaro et al ldquoAdvanced gly-cation end products activate endothelium through signal-transduction receptor RAGE a mechanism for amplification ofinflammatory responsesrdquo Circulation vol 105 no 7 pp 816ndash822 2002
[70] E Devangelio F Santilli G Formoso et al ldquoSoluble RAGE intype 2 diabetes association with oxidative stressrdquo Free RadicalBiology and Medicine vol 43 no 4 pp 511ndash518 2007
[71] G Basta A M Schmidt and R de Caterina ldquoAdvancedglycation end products and vascular inflammation implica-tions for accelerated atherosclerosis in diabetesrdquoCardiovascularResearch vol 63 no 4 pp 582ndash592 2004
[72] R Meerwaldt T Links C Zeebregts R Tio J-L Hillebrandsand A Smit ldquoThe clinical relevance of assessing advanced gly-cation endproducts accumulation in diabetesrdquo CardiovascularDiabetology vol 7 article 29 2008
[73] H Unoki and S Yamagishi ldquoAdvanced glycation end productsand insulin resistancerdquo Current Pharmaceutical Design vol 14no 10 pp 987ndash989 2008
[74] E Diamanti-Kandarakis C Piperi A Kalofoutis and GCreatsas ldquoIncreased levels of serum advanced glycation end-products in women with polycystic ovary syndromerdquo ClinicalEndocrinology vol 62 no 1 pp 37ndash43 2005
[75] D R Mccance D G Dyer J A Dunn et al ldquoMaillardreaction products and their relation to complications in insulin-dependent diabetes mellitusrdquo Journal of Clinical Investigationvol 91 no 6 pp 2470ndash2478 1993
[76] R Singh A Barden TMori and L Beilin ldquoAdvanced glycationend-products a reviewrdquoDiabetologia vol 44 no 2 pp 129ndash1462001
[77] E Diamanti-Kandarakis A Piouka S Livadas et al ldquoAnti-mullerian hormone is associated with advanced glycosylatedend products in lean women with polycystic ovary syndromerdquoEuropean Journal of Endocrinology vol 160 no 5 pp 847ndash8532009
[78] R Chatterjee and R Bajoria ldquoNew concept in natural historyand management of diabetes mellitus in thalassemia majordiabetes and thalassaemiardquo Hemoglobin vol 33 supplement 1pp S127ndashS130 2009
[79] G Paolisso M R Tagliamonte M R Rizzo and D GiuglianoldquoAdvancing age and insulin resistance new facts about anancient historyrdquo European Journal of Clinical Investigation vol29 no 9 pp 758ndash769 1999
[80] N Sattarahmady H Heli and A A Moosavi-Movahedi ldquoDes-feral as improving agent for hemoglobin fructation structuraland functional impactsrdquo The Protein Journal vol 31 no 8 pp651ndash655 2012
[81] E Fibach and E A Rachmilewitz ldquoThe role of antioxidantsand iron chelators in the treatment of oxidative stress inthalassemiardquo Annals of the New York Academy of Sciences vol1202 pp 10ndash16 2010
[82] L M Compagno ldquoCaring for adults with thalassemia in apediatric worldrdquo Annals of the New York Academy of Sciencesvol 1054 pp 266ndash272 2005
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

Anemia 3
production of ROS via the Fenton reaction hence ironoverload disrupts the redox balance of the cells causingchronic OS [18] OS leads to lipid peroxidation of unsaturatedfatty acids in membranes of cells and organelles Cytotoxicbyproducts of lipid peroxidation such as malondialdehyde(MDA) and 4-hydroxy-21015840-nonenal are produced and theseimpair cellular function and protein synthesis and damageDNA [19] Furthermore a crucial component in the oxidantsusceptibility of the thalassemic RBC is the release of hemeand iron from the excessive unpaired alpha-globin chains[2] This release initiates self-amplifying redox reactionswhich deplete the cellular reduction potential (eg glu-tathioneGSH) oxidize additional hemoglobin and acceler-ate RBC destruction [2]
Oxidativeantioxidative balance is one of themost impor-tant factors for homeostasis When the balance of ROSand antioxidants is disrupted towards an overabundanceof ROS OS occurs [20] The generation of ROS is asteady-state cellular event in respiring cells while theiruncontrolled production often leads to damage of cellularmacromolecules (DNA protein and lipids) and other smallantioxidant molecules [21] A number of major enzymaticand nonenzymatic defense mechanisms exist to neutralizeand combat the damaging effects of these reactive sub-stances [22] The enzymic system functions by direct orsequential removal of ROS (superoxide dismutaseSODcatalaseCAT and glutathione peroxidaseGPx) thereby ter-minating their activities Nonenzymic defense consists ofscavengingmolecules that are endogenously produced (GSHubiquinols and uric acid) or derived from the diet such asvitamins C and E [21] These antioxidant nutrients occupydistinct cellular compartments and among them there isactive recycling Antioxidative systems which protect fromperoxidative damage are also supposed to be under hormonalinfluence while antioxidative enzymes require the presenceof microelements in their active centers as well as concertaction of nonenzymatic antioxidants which support enzymesin their scavenging action [23]Meanwhile diet seems to havean impact on antioxidative system which requires appro-priate supplementation inmicroelements and vitamins for itseffective function leading to scavenging excess of free radi-cals [23]
According to the current evidence-based knowledge asignificant prooxidantsantioxidants imbalance with subse-quent increased OS exists in patients with BTM which ismainly caused by tissue injury due to overproduction of freeradicals by secondary iron overload alteration in serum traceelements and alteration in antioxidant enzymes level [24](Figure 1) The results of Wassem et al revealed that thelevels of vitamin E and antioxidant enzymes GPx and SODwere significantly lowered in BTM patients as comparedwith the control group indicating that thalassemics are ina state of enhanced OS [2] Another study revealed thatplasma thiobarbituric acid (TBA) reactive substances wereelevated in BTM children compared to controls togetherwith compensatory increase in SOD activity and decrease inCAT activity [25] At the same study serum ferritin showeda positive correlation with elevated TBA reactive substancesand SOD suggesting that iron overload is involved in the OS
shown in cells [25] A significant increase in the levels of lipidperoxide and iron and a significant decrease in the levels ofvitamin E total antioxidant capacity and total iron bindingcapacity were observed in a different study [26] suggestingthat OS and reduced antioxidant defense mechanism play animportant role in pathogenesis of BTM [26] FurthermoreLivrea et al have previously suggested that the measure-ment of peroxidation products matched with evaluation ofantioxidants may be a simple measure of iron toxicity inthalassemia in addition to the conventional indices of ironstatus [27] Their study showed that the mean concentrationsof conjugated diene lipid hydroperoxides (CD) lipoperoxidesevaluated as (MDATBA) adducts and protein carbonylsincreased about twofold with respect to control A net dropin the concentration of ascorbate vitamin E vitamin A beta-carotene and lycopene was also observed Serum levels ofvitamin E were inversely correlated with ferritin suggesting amajor consumption of this antioxidant under iron overloadwhile serum levels of vitamin E vitamin A and lycopenewere inversely correlated with the levels of transminases [27]On the other hand their results pointed out that the iron-induced liver damage in thalassemia may play a major rolein the depletion of lipid-soluble antioxidants [27] Later onChiou et al indicated that excessive lipid peroxidation and aprofound depletion of plasma vitaminsA E andC levels existin patients with BTM thus antioxidant supplementation forthe purpose of alleviating the OS may be warranted [28]They also found that HCV infection did play some role inaggravating the depletion of plasma vitamins E and C levelsin the BTM patients while it did not seem to alter the levelsof reduced GSH as well as antioxidant enzyme activities [28]
32 The Possible Impact of Oxidative Stress on BTM FemalesrsquoFertility Potential Although there is no direct evidence-based publication correlating the iron-inducedOSwith BTMwomenrsquos infertility existing published data on non-BTMpatients only permit the correlation of OS (not specificallyproduced through iron overload) with normal and abnormalprocesses of the female reproductive system Also there isno available publication connecting iron-induced OS withspecific altered signaling events in hypothalamic-pituitary-gonadal axis which subsequently could lead to infertilityThus until now only indirect evidence exists which supportsthe hypothesis that iron-induced OS is the main causal agentfor infertility in women with BTMThis is maybe happeningnot only through iron deposition and iron-induced OS invarious endocrine organs such as hypothalamus pituitaryand female reproductive system but also through its indirecteffect on other organs such as liver and pancreas contribut-ing to the impaired metabolism of hormones and serumantioxidants
Recently ROS have been shown to have an important rolein the normal functioning of reproductive system and in thepathogenesis of infertility in females [29] OS develops whenthere is an imbalance between the generation of ROS andthe scavenging capacity of antioxidants in the reproductivetract while it affects both natural and assisted fertility [29]ROS affect multiple physiological processes from oocyte
4 Anemia
maturation to fertilization embryo development and preg-nancy [20] There is sufficient evidence to hypothesize thatdietary antioxidants and OS may influence the timing andmaintenance of a viable pregnancy [30] Also physiologicallevels of ROS play an important regulatory role throughvarious signaling transduction pathways in folliculogenesisoocyte maturation endometrial cycle luteolysis implanta-tion embryogenesis and pregnancy [31] Proper functioningof the ovary is critical to maintain fertility and overall healthand ovarian function depends on the maintenance andnormal development of ovarian follicles [32] The potentialimpact of OS on the wellbeing of primordial growing andpreovulatory follicles as well as oocytes and early embryosexamining cell types and molecular targets has been exten-sively reviewed [32] Meanwhile ROS-induced apoptotic celldeath is involved in the mechanisms of corpus luteum (CL)regression that occurs at the end of the nonfertile cycle [33]
The role of OS in female reproduction is becomingincreasingly important as recent evidence suggests that itplays a part in conditions such as polycystic ovary syndrome(PCOS) endometriosis unexplained fertility spontaneousabortions preeclampsia hydatidiform mole embryopathiespreterm labor and intrauterine growth retardation [31] Agar-wal et al have recently reviewed the role of OS in normal andabnormal female reproductive physiological processes ana-lyzing the exact mechanisms of redox cell signaling and thepathophysiology of OS-related reproductive diseases [34] Aspecial comment should be made on endometriosis patientswhere iron overload has been demonstrated in the differentcompartments of the peritoneal cavity (peritoneal fluidendometriotic lesions peritoneum and macrophages) [35]This iron overload affects numerous mechanisms involvedin endometriosis development [35] Iron-induced OS maybe involved in endometriosis-associated infertility and mayplay a role in the regulation of the expression of genesencoding immunoregulators cytokines and cell adhesionmolecules implicated in the pathogenesis of endometriosis[36] Moreover a recent study investigated the relation-ship between OS and the underlying causes of infertilitypreovulatory ovarian hormones and ovarian response togonadotropin stimulation in patients undergoing ART [37]There was no significant relationship between plasma orfollicular fluid (FF) total antioxidant capacity (TAC) and theunderlying etiology of infertility [37] However there was astatistically significant positive association between FF E(2)levels and TAC OS has an impact on the production ofgranulosa cell steroid hormones in particular E(2) which isan important predictor of ovarian response [37] Thus thepossible impaired ovarian response in BTM women couldbe probably caused by dysregulation in the production ofgranulosa cell steroid hormones such as E(2) Meanwhile ithas been suggested that OSmodulates the age-related declinein fertility [20] Additionally a recent study indicated thatnonheme iron accumulation on ovarian stromal tissue maybe related to aging of the ovary due to increasing OS [38]Theage-related decline in fertility due to OS has a special impactin our group of patients because of their increased age aver-age due to significant improvements in chelation treatmentmodalities Furthermore remarkable is another study which
evaluated retinol and alpha-tocopherol natural antioxidantsthat inhibit lipid peroxidation and protect against cell damageinduced by OS and revealed that lower concentrations ofthese natural antioxidants were associated with abnormalsemen parameters in men and anovulation in women [39]
4 Evidence-Based Effect of Iron Overloadand Iron-Induced OS on Hypothalamic-Pituitary-Gonadal Axis and FemaleReproductive System
Although there are limited data directly correlating iron over-load with iron-induced OS on BTM femalesrsquo hypothalamic-pituitary-gonadal axis and ovarian reserve indirect conclu-sions could be obtained through the model of hemochro-matosis
41 The Model of Hemochromatosis Endocrinopathies arecommon in transfusion-associated haemochromatosis [40]while HH is the most frequent endocrine abnormality inhemochromatosis [41] The gonadotropin responsiveness to100 micrograms of LHRH was impaired or absent in patientswith hemochromatosis [42] Also in a cohort of 115 patientssuffering from genetic hemochromatosis hypogonadismwasevidenced in 42 of them inmost of which it was consideredas secondary to pituitary lesions as assessed by GnRH tests[43] Moreover in male patients with idiopathic hemochro-matosis testicular atrophy has been suggested to be causedby insufficient secretion of gonadotropins due to the selectiveaccumulation of iron in gonadotropic cells of the pituitarygland [44] Meanwhile subnormal gonadotropin responsesto GnRH but normal ovarian reserve as shown by normalfollicular stimulation with hMG were reported in a case ofHH in a female with biopsy-proven hemochromatosis [45]In another case report recovery of reproductive functionsdocumented by hormone measurements testicular biopsyand semen analysis was observed in a 37-year-old man withHH due to idiopathic hemochromatosis after phlebotomy[46] It has been also proposed that subjects with lesserdegrees of hepatic siderosis at diagnosis are unlikely todevelop hypogonadism [47] Furthermore the pituitary ofa 69-year-old man with hemochromatosis had been pre-viously removed at autopsy and was studied by histologyhistochemistry immunocytochemistry electron microscopyand X-ray diffraction [48] Preferential localization of irondeposits was demonstrated in gonadotrophs which at theultrastructural level displayed selective severe cellular injury[48] X-ray diffraction revealed the deposition of iron-accumulated lysosomes while iron storage was also notedin stellate cells [48] It should be also noted that in a groupof 7 young male patients with genetic hemochromatosis thenormal or high increments of LH after LHRH stimulationsuggested that secretion capacity of LH was intact andthat hypothalamic dysfunction could be responsible for theobserved preclinical gonadal deficiency [49] A similar resultwas obtained in another male patient where although thepituitary secretion of LH was normal in response to GnRHstimulation clomiphene administration did not produce an
Anemia 5
increase in LH and FSH suggesting that there was a defect inthe hypothalamic GnRH response [50]
In agreement with the hemochromatosis model abnor-malities of the hypothalamic-pituitary-gonadal axis are themost common endocrine abnormalities in patients withBTM as they require multiple blood transfusions leading tohemochromatosis [51] Thus based on the model of hemo-chromatosis that resembles iron-overloaded patients withBTM it seems that abnormalities of ovulation and menstru-ation in these patients are most likely because of inadequatepituitary responsiveness to GnRH [45]
42 Direct and Indirect Evidence for the Hypothalamic-Pitui-tary and the Gonadal Effect of Iron Patients with transfu-sional iron overload begin to develop pituitary iron overloadin the first decade of life however clinically significantvolume loss was not observed until the second decadeof life [52] Pituitary iron overload and volume loss wereindependently predictive of hypogonadism [52] Pituitary R2correlated significantly with serum ferritin as well as liverpancreatic and cardiac iron deposition by MRI [52] Manypatients with moderate-to-severe pituitary iron overloadretained normal gland volume and function representing apotential therapeutic window [52] According to a differentstudy BTM patients with severe organ damage and ironoverload are likely to be apulsatile with irreversible damageto their hypothalamic-pituitary axis while those with less-severe iron overload are likely to have potentially reversibleHH [53]The same study suggested that gonadotrophin pulseparameters rather than the gonadotrophin response to aGnRH bolus following prolonged pulsatile GnRH infusionmay be more useful in discriminating reversible from irre-versible HH [53] Furthermore in a study of 33 patients above15 years of age with transfusion-dependent BTM and ironoverload anterior pituitary function (GnRH stimulation test)correlated well with MRI results However no correlationwas found between the MRI measurements the GnRHstimulation test and the clinical status of the patients as 28out of the 33 patients achieved normal puberty [54] Anotherpossible mechanism of iron effect on hypothalamic-pituitaryaxis is through iron-induced OS with subsequent alterationson elongation factor-2 (eEF-2) levels The hypothalamic-pituitary system secretes peptide hormones whose synthesisrequires the integrity of the translation machinery Amongthe possible causes of the decline of translation in oldanimals are the modifications of eEF-2 [55] Iron-induced OScould be involved in the alterations of eEF-2 which formsadducts with MDA and 4-hydroxynonenal (HNE) [55] Thealterations of eEF-2 levels secondary to lipid peroxidationand adduct formation with these aldehydes could contributeto the suboptimal hormone production from these tissues[55] Moreover the possible concurrent GH deficiency maypotentiate the already present OS as patients with GHdeficiency have an increased degree of OS and endothelialdysfunction which possibly acts synergistically with iron-induced OS [56] Thus although there is limited evidenceon the exact pathophysiological mechanisms of iron effecton hypothalamic-pituitary axis it seems to be the basic
pathogenetic cause of the impaired hypothalamic-pituitarysystem
Meanwhile according to our knowledge only one studyexists which proves the iron deposition on the femalereproductive system in patients with BTM This particularstudy obtained histopathological evidence that depositionof haemosiderin occurred in the endometrial glandularepithelium of three patients with BTM [57] This depositionwas mainly evident in the apical part of these cells abovethe nuclei and should be taken into consideration as acontributing factor to the infertility in these patients byaltering endometrial receptivity for implantation [57] In twopatients who received effective iron chelating treatment withdesferrioxamine the endometrial haemosiderin depositseither disappeared or were significantly reduced [57]
43 Available Studies Directly Correlating Iron and Its Impacton Fertility in Women with BTM The pathophysiology ofiron-induced compromised fertility in women with BTMwas only recently evaluated [9] Low gonadotropin secretionresulted in reduced ovarian antral follicle count and ovarianvolume but levels of antimullerian hormone (AMH) a sensi-tive marker for ovarian reserve independent of gonadotropineffect were mostly normal AMH correlated with NTBI sug-gesting a role of labile iron in the pathogenesis of decreasedreproductive capacity possibly occurring in parallel to car-diac iron toxicity as cardiac iron was associated with thepresence of amenorrhea and with NTBI levels Thus AMHwas suggested to be valuable for future studies aiming atimproved chelation for fertility preservation whereas NTBIand labile plasma iron was suggested to be valuable formonitoring iron effect on the reproductive system [9] Thesame research team explored the relationship between liveriron concentration (LIC) and fertility status in 26 females(mean 30 years old) with BTM Seventeen (65) of themexperienced PA or SA Levels of LHFSH and estradiol werelow or undetectable in 48 and 35 of patients respectivelyand did not correlate with age presence of amenorrhea andLIC The fact that LHFSH and estradiol commonly usedfor assessment of fertility potential in thalassemia had apoor predictive value addressed the need for utilization ofcurrent available methods for assessment of fertility capacityin thalassemia [58]
5 Potential Antioxidants in BTM
Considering all the above we suggest that the enhancedOS observed in iron-overloaded patients with BTM mayplay a significant role in their reduced reproductive abilityThe investigation of the proper antioxidants for fertility andpregnancy in BTM female patients which are recognized aspatients of increased OS is of great value and importanceThe increased age average of this group of patients underlinesthe increased importance of OS on the female reproductivesystem as it has been also connected with aging Howeverdespite the clear identification of the oxidativeantioxidativeimbalance in patients with BTM there are few studies
6 Anemia
evaluating the effect of different antioxidant supplementationin BTM-related morbidities such as infertility
51 Antioxidant Supplements Used in BTM The benefits ofvitamin C and vitamin E as antioxidant supplements inBTMchildren have been previously determined [59] Twentychildren who had laboratory confirmation of BTM at least 6months with history of packed red cell transfusion withoutiron chelation were recruited It was suggested that vitaminC plus vitamin E supplementations have benefits more thanvitamin E alone in promoting antioxidant status and mayenhance liver function as total bilirubin tends to decrease[59] Furthermore curcuminoids extracted from the spiceturmeric are known to have antioxidant and iron-chelatingproperties and have been proposed as a potential upstreamtherapy of thalassemiaWeeraphan et al have recently appliedproteomic techniques to study the protein profile and oxida-tive damage in the plasma of beta-thalassemiaHb E patientsbefore and after treatment with curcuminoids Their studyindicated the ameliorating role of curcuminoids towards OSand iron overload in the plasma proteome [60] Glutaminealpha-lipoic acid acetyl-L-carnitine and N-acetylcysteineare also recently being studied as antioxidant supplements forsickle cell disease and thalassemia [61] Finally the value ofantioxidant supplements in the elimination of iron-inducedOS and subsequent infertility issues could be speculatedby the fact that various antioxidants (such as carnitinevitamin C vitamin E selenium carotenoids glutathioneN-acetylcysteine zinc folic acid and coenzyme Q10) arevariably effective in OS-induced male-factor infertility withrespect to improving semen parameters and pregnancy rates[62]
52 Chelation Treatments as Antioxidants in BTM Differentstudies have also focused on the antioxidant capacity of differ-ent chelation treatment modalities Increased evidence fromin vitro in vivo and clinical studies suggest that deferiprone(L1) can be used as a potent pharmaceutical antioxidant bymobilizing labile iron and copper andor inhibiting theircatalytic activity in the formation of free radicals and OS intissue damage [63] In contrast to L1 both desferrioxamine(DFO) and deferasirox (DFRA) were suggested to havemajordisadvantages in their use in noniron loading conditionsdue to toxicity implications [63] Meanwhile a subsequentstudy indicated that DFO chelation therapy does not nor-malize ferritin levels but attenuates oxidative damage andimproves total antioxidant level in Malaysian Chinese BTMpatients [64] The objective of this research was to studythe oxidant-antioxidant indices in BTM patients who wereon desferrioxamine-chelation or without chelation therapyBlood was collected from 39 Chinese patients and 20 con-trols Plasma and peripheral blood mononuclear cell lysates(PBMC) were extracted and biochemical tests to evaluate OSwere performedOSwas evident in these patients as advancedoxidized protein products (AOPP) and lipid hydroperoxideswere elevated whereas glutathione peroxidase activity andthe ferric reducing antioxidant power (FRAP) were reducedThe catalase activity in the patientsrsquo PBMC was elevated
possibly as a compensatory mechanism for the reducedglutathione peroxidase activity in both red blood cells andPBMC The lower FRAP and higher AOPP levels in thenonchelated patients compared with the chelated patientswere indicative of a lower OS level in the chelated patients[64] An additional study which assessed whether oxidant-stress and inflammation in BTM could be controlled byDFRA as effectively as by DFO revealed equal effectivenessin decreasing iron burden and levels of the oxidative-stressmarker MDA [65]
53 The Possible Effect of Advanced Glycation End Products(AGEs) Regulation on BTM Womenrsquos Ovarian Function andFertility Recent data have shown that OS is involved in thepathophysiology of anovulation [20 66 67] While the roleof OS in ovulatory dysfunction has been sufficiently studied[29 68] advanced glycation end products (AGEs) have beenrecognized as mediators of increased OS [69 70] Advancedglycation end products (AGEs) are a heterogeneous group ofbioactive molecules formed by the nonenzymatic glycationof proteins lipids and nucleic acids [71] There is increasingevidence that AGEs play a pivotal role in atherosclerosis andin diabetes and its complications while AGE accumulationis a measure of cumulative metabolic and OS and mayso represent the ldquometabolic memoryrdquo [72] Engagement oftheir receptor RAGE with AGEs is shown to activate itsdownstream signaling and evoke OS and inflammation indiabetes [73] AGEs have been found to induce OS andconversely OS stimulates AGEs formation [74ndash76]
AGEs deposition in ovary dysregulate ovarian functionthrough the induction of androgen production as well as OSgeneration through the induction ofNF-K120573pathway leadingto increased production of atherogenic and inflammatorymolecules AGEs have been implicated in the developmentof insulin resistance hyperandrogenism and anovulationin polycystic ovary syndrome (PCOS) and seem to have acentral role in PCOS pathophysiology either as a marker ofOS or through their specific actions after their ligation totheir specific receptor RAGE [77] Furthermore there is sub-stantial evidence that insulin resistance constitutes one of themain pathophysiological mechanisms leading to anovulationand ovarian hyperandrogenism in PCOS patients Regardingthe above also that iron has been implicated in abnormalinsulin secretion in patients with BTM or hemochromatosis[44 78] and that OS might be responsible for a decline ininsulin-mediated glucose uptake in BTM patients leadingto insulin resistance [79] we consider that the evaluationof AGEs as markers of OS in relation to iron overloadinsulin resistance and ovulation potential would be of greatvalue Reducing AGEs in BTM females could probably havebeneficial effects in insulin resistance and ovulation potentialand thus in fertility potential Finally it is remarkable thatthe iron chelator Desferal had a retardation effect on thefunctional and structural changes of Hb during fructation[80] It could prevent the AGEs and carbonyl formations andhelix depletion during theHb fructation processMoreover itcould preserve peroxidase and esterase activities of fructated
Anemia 7
Hb similar to native Hb Therefore desferal could be intro-duced as an antiglycation drug to prevent theAGEs formation[80]
6 Conclusions
On the basis of all the presented data it can be concludedthatOS plays amajor role in the pathophysiology of infertilityin females with thalassemia This OS is mainly caused bytissue injury due to overproduction of free radicals bysecondary iron overload alteration in serum trace elementsand alteration in antioxidant enzymes level Consequentlythere is a rationale for iron chelation to eliminate the free-iron species which in this respect act like antioxidantsAntioxidants are also capable of ameliorating increased OSparameters and given together with iron chelators mayprovide a substantial improvement in the pathophysiologyof thalassemia [81] However there is no study evaluatingthe efficacy of antioxidant supplementation on BTMwomenrsquosfertility potential In agreement with previous suggestionswe consider that the application of treatment strategies thatwould reduceOS in the reproductive tract could help infertilewomen with diseases such as BTM that are caused byROSantioxidants imbalance [29] In general research isin progress to identify the mechanisms that are involvedin the etiology of female reproductive diseases caused byROS and to create effective strategies that can counteractOS [29] while few are the trials investigating antioxidantsupplementation in female reproduction [20] The admin-istration of selective antioxidants along with essential traceelements and minerals to reduce the extent of oxidativedamage and related complications such as infertility in BTMpatients still needs further evaluation [24] However beforeclinicians recommend antioxidants randomized controlledtrials with sufficient power are necessary to prove the efficacyof antioxidant therapeutic strategies in disorders of femalereproduction [20] such as BTMThis is strongly emerged bythe fact of prolonged survival and the newly recognized issuesand challenges that adults with BTM face [82]
References
[1] C Hershko ldquoPathogenesis and management of iron toxicity inthalassemiardquo Annals of the New York Academy of Sciences vol1202 pp 1ndash9 2010
[2] F Waseem K A Khemomal and R Sajid ldquoAntioxidant statusin beta thalassemia major a single-center studyrdquo Indian Journalof Pathology and Microbiology vol 54 no 4 pp 761ndash763 2011
[3] R Origa A Piga G Quarta et al ldquoPregnancy and 120573-thalassemia an Italian multicenter experiencerdquoHaematologicavol 95 no 3 pp 376ndash381 2010
[4] N Skordis L Petrikkos M Toumba et al ldquoUpdate on fertilityin thalassaemia majorrdquo Pediatric Endocrinology Reviews vol 2supplement 2 pp 296ndash302 2004
[5] M Toumba A Sergis C Kanaris and N Skordis ldquoEndocrinecomplications in patients with thalassaemia majorrdquo PediatricEndocrinology Reviews vol 5 no 2 pp 642ndash648 2007
[6] E A Rachmilewitz O Weizer-Stern K Adamsky et al ldquoRoleof iron in inducing oxidative stress in thalassemia can it be
prevented by inhibition of absorption and by antioxidantsrdquoAnnals of the New York Academy of Sciences vol 1054 pp 118ndash123 2005
[7] S Ansari A Azarkeivan and A Tabaroki ldquoPregnancy inpatients treated for beta thalassemia major in two centers(Ali Asghar Childrenrsquos Hospital and Thalassemia Clinic) out-come for mothers and newborn infantsrdquo Pediatric Hematology-Oncology vol 23 no 1 pp 33ndash37 2006
[8] M R Safarinejad ldquoReproductive hormones and hypothalamic-pituitary-ovarian axis in female patients with homozygous 120573-thalassemia majorrdquo Journal of Pediatric HematologyOncologyvol 32 no 4 pp 259ndash266 2010
[9] S T Singer E P Vichinsky G Gildengorin J van DisseldorpM Rosen and M I Cedars ldquoReproductive capacity in ironoverloaded women with thalassemia majorrdquo Blood vol 118 no10 pp 2878ndash2881 2011
[10] G Vizziello D Carone E Caroppo A Vitti A Pasquad-ibisceglie and G Drsquoamato ldquoOvulation induction with gona-dotropin in patients with thalassemia pretreated with pulsatileGnRH outcomerdquoMinerva Ginecologica vol 56 no 5 pp 485ndash487 2004
[11] N Skordis S Christou M Koliou N Pavlides and M Angas-tiniotis ldquoFertility in female patients with thalassemiardquo Journalof Pediatric Endocrinology and Metabolism vol 11 supplement3 pp 935ndash943 1998
[12] LDanesiM Scacchi AMMiragoli et al ldquoInduction of folliclematuration and ovulation by gonadotropin administration inwomen with 120573-thalassemiardquo European Journal of Endocrinol-ogy vol 131 no 6 pp 602ndash606 1994
[13] R Bajoria and R Chatterjee ldquoCurrent perspectives of fertilityand pregnancy in thalassemiardquoHemoglobin vol 33 supplement1 pp S131ndashS135 2009
[14] R Bajoria and R Chatterjee ldquoHypogonadotrophic hypogo-nadism and diminished gonadal reserve accounts for dys-functional gametogenesis in thalassaemia patients with ironoverload presenting with infertilityrdquoHemoglobin vol 35 no 5-6 pp 636ndash642 2011
[15] M Karagiorga-Lagana ldquoFertility in thalassemia the Greekexperiencerdquo Journal of Pediatric Endocrinology andMetabolismvol 11 supplement 3 pp 945ndash951 1998
[16] S M Tuck ldquoFertility and pregnancy in thalassemia majorrdquoAnnals of the New York Academy of Sciences vol 1054 pp 300ndash307 2005
[17] D Surbek A Koller and N Pavic ldquoSuccessful twin pregnancyin homozygous 120573-thalassemia after ovulation induction withgrowth hormone and gonadotropinsrdquo Fertility and Sterility vol65 no 3 pp 670ndash672 1996
[18] K Yamaguchi M Mandai S Toyokuni et al ldquoContents ofendometriotic cysts especially the high concentration of freeiron are a possible cause of carcinogenesis in the cysts throughthe iron-induced persistent oxidative stressrdquo Clinical CancerResearch vol 14 no 1 pp 32ndash40 2008
[19] M C Kew ldquoHepatic iron overload and hepatocellular carci-nomardquo Cancer Letters vol 286 no 1 pp 38ndash43 2009
[20] AAgarwal S Gupta andRK Sharma ldquoRole of oxidative stressin female reproductionrdquo Reproductive Biology and Endocrinol-ogy vol 3 article 28 2005
[21] A C Chan C K Chow and D Chiu ldquoInteraction of antiox-idants and their implication in genetic anemiardquo Proceedings ofthe Society for Experimental Biology and Medicine vol 222 no3 pp 274ndash282 1999
8 Anemia
[22] A Agarwal A Aponte-Mellado B J Premkumar A Shamanand S Gupta ldquoThe effects of oxidative stress on female repro-duction a reviewrdquo Reproductive Biology and Endocrinology vol10 article 49 2012
[23] M Giergiel M Lopucki N Stachowicz and M KankoferldquoThe influence of age and gender on antioxidant enzymeactivities in humans and laboratory animalsrdquoAging Clinical andExperimental Research vol 24 pp 551ndash559 2012
[24] Q Shazia Z H Mohammad T Rahman and H U ShekharldquoCorrelation of oxidative stress with serum trace element levelsand antioxidant enzyme status in Beta thalassemia majorpatients a review of the literaturerdquo Anemia vol 2012 ArticleID 270923 7 pages 2012
[25] M Y Abdalla M Fawzi S R Al-Maloul N El-Banna R FTayyem and I M Ahmad ldquoIncreased oxidative stress and ironoverload in Jordanian120573-thalassemic childrenrdquoHemoglobin vol35 no 1 pp 67ndash79 2011
[26] R A Ghone K M Kumbar A N Suryakar R V Katkam andN G Joshi ldquoOxidative stress and disturbance in antioxidantbalance in beta thalassemia majorrdquo Indian Journal of ClinicalBiochemistry vol 23 no 4 pp 337ndash340 2008
[27] MA Livrea L Tesoriere AM Pintaudi et al ldquoOxidative stressand antioxidant status in 120573-thalassemia major iron overloadand depletion of lipid-soluble antioxidantsrdquo Blood vol 88 no9 pp 3608ndash3614 1996
[28] S-S Chiou T-T Chang S-P Tsai et al ldquoLipid peroxidationand antioxidative status in 120573-thalassemia major patients withor without hepatitis C virus infectionrdquo Clinical Chemistry andLaboratory Medicine vol 44 no 10 pp 1226ndash1233 2006
[29] A Agarwal and S S Allamaneni ldquoRole of free radicals in femalereproductive diseases and assisted reproductionrdquo ReproductiveBioMedicine Online vol 9 no 3 pp 338ndash347 2004
[30] E H Ruder T J Hartman J Blumberg and M B GoldmanldquoOxidative stress and antioxidants exposure and impact onfemale fertilityrdquoHuman Reproduction Update vol 14 no 4 pp345ndash357 2008
[31] A Agarwal S Gupta L Sekhon and R Shah ldquoRedox con-siderations in female reproductive function and assisted repro-duction from molecular mechanisms to health implicationsrdquoAntioxidants amp Redox Signaling vol 10 no 8 pp 1375ndash14032008
[32] P J Devine S D Perreault and U Luderer ldquoRoles of reactiveoxygen species and antioxidants in ovarian toxicityrdquo Biology ofReproduction vol 86 no 2 article 27 2012
[33] K H Al-Gubory C Garrel P Faure and N Sugino ldquoRolesof antioxidant enzymes in corpus luteum rescue from reac-tive oxygen species-induced oxidative stressrdquo ReproductiveBiomedicine Online vol 25 no 6 pp 551ndash560 2012
[34] A Agarwal A Aponte-Mellado B J Premkumar A Shamanand S Gupta ldquoThe effects of oxidative stress on female repro-duction a reviewrdquo Reproductive Biology and Endocrinology vol10 article 49 2012
[35] S Defrere R Gonzalez-Ramos J-C Lousse et al ldquoInsightsinto iron and nuclear factor-kappa B (NF-120581B) involvement inchronic inflammatory processes in peritoneal endometriosisrdquoHistology and Histopathology vol 26 no 8 pp 1083ndash1092 2011
[36] A van Langendonckt F Casanas-Roux and J Donnez ldquoOxida-tive stress and peritoneal endometriosisrdquo Fertility and Sterilityvol 77 no 5 pp 861ndash870 2002
[37] M Appasamy E Jauniaux P Serhal A Al-Qahtani N PGroome and S Muttukrishna ldquoEvaluation of the relationshipbetween follicular fluid oxidative stress ovarian hormones and
response to gonadotropin stimulationrdquo Fertility and Sterilityvol 89 no 4 pp 912ndash921 2008
[38] Y Asano ldquoAge-related accumulation of non-heme ferric andferrous iron in mouse ovarian stroma visualized by sensitivenon-heme iron histochemistryrdquo The Journal of Histochemistryamp Cytochemistry vol 60 no 3 pp 229ndash242 2012
[39] M K Al-Azemi A E Omu T Fatinikun N Mannazhathand S Abraham ldquoFactors contributing to gender differences inserum retinol and 120572-tocopherol in infertile couplesrdquo Reproduc-tive BioMedicine Online vol 19 no 4 pp 583ndash590 2009
[40] M K Kim J W Lee K H Baek et al ldquoEndocrinopathies intransfusion-associated iron overloadrdquo Clinical Endocrinologyvol 78 no 2 pp 271ndash277 2013
[41] L M Hempenius P S van Dam J J Marx and H PKoppeschaar ldquoMineralocorticoid status and endocrine dys-function in severe hemochromatosisrdquo Journal of Endocrinolog-ical Investigation vol 22 no 5 pp 369ndash376 1999
[42] J M Vasquez and R B Greenblatt ldquoPituitary responsiveness toluteinizing-hormone-releasing hormone in different reproduc-tive disorders a reviewrdquo Journal of ReproductiveMedicine for theObstetrician and Gynecologist vol 30 no 8 pp 591ndash600 1985
[43] I Paris M Hermans and M Buysschaert ldquoEndocrine compli-cations of genetic hemochromatosisrdquo Acta Clinica Belgica vol54 no 6 pp 334ndash345 1999
[44] W Stremmel C Niederau M Berger H-K Kley H-LKruskemper and G Strohmeyer ldquoAbnormalities in estrogenandrogen and insulin metabolism in idiopathic hemochro-matosisrdquo Annals of the New York Academy of Sciences vol 526pp 209ndash223 1988
[45] W R Meyer K A Hutchinson-Williams E E Jones and A HDecherney ldquoSecondary hypogonadism in hemochromatosisrdquoFertility and Sterility vol 54 no 4 pp 740ndash742 1990
[46] L J Siemons and C H Mahler ldquoHypogonadotropic hypogo-nadism in hemochromatosis recovery of reproductive functionafter iron depletionrdquo The Journal of Clinical Endocrinology andMetabolism vol 65 no 3 pp 585ndash587 1987
[47] J H McDermott and C H Walsh ldquoHypogonadism in hered-itary hemochromatosisrdquo The Journal of Clinical Endocrinologyand Metabolism vol 90 no 4 pp 2451ndash2455 2005
[48] G Kontogeorgos S Handy K Kovacs E Horvath and BW Scheithauer ldquoThe anterior pituitary in hemochromatosisrdquoEndocrine Pathology vol 7 no 2 pp 159ndash164 1996
[49] A Piperno M R Rivolta R Drsquoalba et al ldquoPreclinical hypog-onadism in genetic hemochromatosis in the early stage ofthe disease evidence of hypothalamic dysfunctionrdquo Journal ofEndocrinological Investigation vol 15 no 6 pp 423ndash428 1992
[50] K SiminoskiM Drsquocosta and P GWalfish ldquoHypogonadotropichypogonadism in idiopathic hemochromatosis evidence forcombined hypothalamic and pituitary involvementrdquo Journal ofEndocrinological Investigation vol 13 no 10 pp 849ndash853 1990
[51] K E Oerter G A Kamp P J Munson A W Nienhuis F GCassorla and P K Manasco ldquoMultiple hormone deficienciesin children with hemochromatosisrdquo The Journal of ClinicalEndocrinology and Metabolism vol 76 no 2 pp 357ndash361 1993
[52] L J Noetzli A Panigrahy S D Mittelman et al ldquoPituitaryiron and volume predict hypogonadism in transfusional ironoverloadrdquo American Journal of Hematology vol 87 no 2 pp167ndash171 2012
[53] R Chatterjee and M Katz ldquoReversible hypogonadotrophichypogonadism in sexually infantile male thalassaemic patientswith transfusional iron overloadrdquo Clinical Endocrinology vol53 no 1 pp 33ndash42 2000
Anemia 9
[54] M Berkovitch T Bistritzer S D Milone K Perlman WKucharczyk and N F Olivieri ldquoIron deposition in the anteriorpituitary in homozygous beta-thalassemia MRI evaluationand correlation with gonadal functionrdquo Journal of PediatricEndocrinology amp Metabolism vol 13 no 2 pp 179ndash184 2000
[55] S Arguelles M Cano A Machado and A Ayala ldquoEffect ofaging and oxidative stress on elongation factor-2 in hypothala-mus and hypophysisrdquo Mechanisms of Ageing and Developmentvol 132 no 1-2 pp 55ndash64 2011
[56] D Gonzalez-Duarte A Madrazo-Atutxa A Soto-Moreno andA Leal-Cerro ldquoMeasurement of oxidative stress and endothe-lial dysfunction in patients with hypopituitarism and severedeficiency adult growth hormone deficiencyrdquo Pituitary vol 15no 4 pp 589ndash597 2012
[57] A Birkenfeld A W Goldfarb E A Rachmilewitz J GSchenker andEOkon ldquoEndometrial glandular haemosiderosisin homozygous beta-thalassaemiardquo European Journal of Obstet-rics Gynecology and Reproductive Biology vol 31 no 2 pp 173ndash178 1989
[58] S T Singer N Sweeters O Vega A Higa E Vichinsky andM Cedars ldquoFertility potential in thalassemia major womencurrent findings and future diagnostic toolsrdquo Annals of the NewYork Academy of Sciences vol 1202 pp 226ndash230 2010
[59] T Dissayabutra P Tosukhowong and P Seksan ldquoThe benefitsof vitamin C and vitamin E in children with beta-thalassemiawith high oxidative stressrdquo Journal of the Medical Association ofThailand vol 88 supplement 4 pp S317ndash321 2005
[60] C Weeraphan C Srisomsap D Chokchaichamnankit et alldquoRole of curcuminoids in ameliorating oxidative modificationin beta-thalassemiaHb E plasma proteomerdquo The Journal ofNutritional Biochemistry vol 24 no 3 pp 578ndash585 2012
[61] E Vichinsky ldquoEmerging ldquoArdquo therapies in hemoglobinopathiesagonists antagonists antioxidants and argininerdquo HematologyAmerican Society Hematology Education Program vol 2012 no1 pp 271ndash275 2012
[62] C Mora-Esteves and D Shin ldquoNutrient supplementationimproving male fertility fourfoldrdquo Seminars in ReproductiveMedicine vol 31 no 4 pp 293ndash300 2013
[63] G J Kontoghiorghes A Efstathiou M Kleanthous YMichaelides and A Kolnagou ldquoRiskbenefit assessmentadvantages over other drugs and targeting methods in the useof deferiprone as a pharmaceutical antioxidant in iron loadingand non iron loading conditionsrdquo Hemoglobin vol 33 no 5pp 386ndash397 2009
[64] U R Kuppusamy and J A Tan ldquoChelation therapy withdesferrioxamine does not normalize ferritin level but attenu-ates oxidative damage and improves total antioxidant level inMalaysian Chinese beta-thalassaemia major patientsrdquoTheWestIndian Medical Journal vol 60 no 1 pp 3ndash8 2011
[65] P B Walter E A Macklin J Porter et al ldquoInflammationand oxidant-stress in 120573-thalassemia patients treated with ironchelators deferasirox (ICL670) or deferoxamine an ancillarystudy of the Novartis CICL670A0107 trialrdquo Haematologica vol93 no 6 pp 817ndash825 2008
[66] V Fenkci S Fenkci M Yilmazer and M Serteser ldquoDecreasedtotal antioxidant status and increased oxidative stress in womenwith polycystic ovary syndrome may contribute to the risk ofcardiovascular diseaserdquo Fertility and Sterility vol 80 no 1 pp123ndash127 2003
[67] C Tatone M C Carbone S Falone et al ldquoAge-dependentchanges in the expression of superoxide dismutases and catalaseare associated with ultrastructural modifications in human
granulosa cellsrdquoMolecular Human Reproduction vol 12 no 11pp 655ndash660 2006
[68] F Gonzalez N S Rote J Minium and J P Kirwan ldquoReactiveoxygen species-induced oxidative stress in the developmentof insulin resistance and hyperandrogenism in polycysticovary syndromerdquo The Journal of Clinical Endocrinology andMetabolism vol 91 no 1 pp 336ndash340 2006
[69] G Basta G Lazzerini M Massaro et al ldquoAdvanced gly-cation end products activate endothelium through signal-transduction receptor RAGE a mechanism for amplification ofinflammatory responsesrdquo Circulation vol 105 no 7 pp 816ndash822 2002
[70] E Devangelio F Santilli G Formoso et al ldquoSoluble RAGE intype 2 diabetes association with oxidative stressrdquo Free RadicalBiology and Medicine vol 43 no 4 pp 511ndash518 2007
[71] G Basta A M Schmidt and R de Caterina ldquoAdvancedglycation end products and vascular inflammation implica-tions for accelerated atherosclerosis in diabetesrdquoCardiovascularResearch vol 63 no 4 pp 582ndash592 2004
[72] R Meerwaldt T Links C Zeebregts R Tio J-L Hillebrandsand A Smit ldquoThe clinical relevance of assessing advanced gly-cation endproducts accumulation in diabetesrdquo CardiovascularDiabetology vol 7 article 29 2008
[73] H Unoki and S Yamagishi ldquoAdvanced glycation end productsand insulin resistancerdquo Current Pharmaceutical Design vol 14no 10 pp 987ndash989 2008
[74] E Diamanti-Kandarakis C Piperi A Kalofoutis and GCreatsas ldquoIncreased levels of serum advanced glycation end-products in women with polycystic ovary syndromerdquo ClinicalEndocrinology vol 62 no 1 pp 37ndash43 2005
[75] D R Mccance D G Dyer J A Dunn et al ldquoMaillardreaction products and their relation to complications in insulin-dependent diabetes mellitusrdquo Journal of Clinical Investigationvol 91 no 6 pp 2470ndash2478 1993
[76] R Singh A Barden TMori and L Beilin ldquoAdvanced glycationend-products a reviewrdquoDiabetologia vol 44 no 2 pp 129ndash1462001
[77] E Diamanti-Kandarakis A Piouka S Livadas et al ldquoAnti-mullerian hormone is associated with advanced glycosylatedend products in lean women with polycystic ovary syndromerdquoEuropean Journal of Endocrinology vol 160 no 5 pp 847ndash8532009
[78] R Chatterjee and R Bajoria ldquoNew concept in natural historyand management of diabetes mellitus in thalassemia majordiabetes and thalassaemiardquo Hemoglobin vol 33 supplement 1pp S127ndashS130 2009
[79] G Paolisso M R Tagliamonte M R Rizzo and D GiuglianoldquoAdvancing age and insulin resistance new facts about anancient historyrdquo European Journal of Clinical Investigation vol29 no 9 pp 758ndash769 1999
[80] N Sattarahmady H Heli and A A Moosavi-Movahedi ldquoDes-feral as improving agent for hemoglobin fructation structuraland functional impactsrdquo The Protein Journal vol 31 no 8 pp651ndash655 2012
[81] E Fibach and E A Rachmilewitz ldquoThe role of antioxidantsand iron chelators in the treatment of oxidative stress inthalassemiardquo Annals of the New York Academy of Sciences vol1202 pp 10ndash16 2010
[82] L M Compagno ldquoCaring for adults with thalassemia in apediatric worldrdquo Annals of the New York Academy of Sciencesvol 1054 pp 266ndash272 2005
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

4 Anemia
maturation to fertilization embryo development and preg-nancy [20] There is sufficient evidence to hypothesize thatdietary antioxidants and OS may influence the timing andmaintenance of a viable pregnancy [30] Also physiologicallevels of ROS play an important regulatory role throughvarious signaling transduction pathways in folliculogenesisoocyte maturation endometrial cycle luteolysis implanta-tion embryogenesis and pregnancy [31] Proper functioningof the ovary is critical to maintain fertility and overall healthand ovarian function depends on the maintenance andnormal development of ovarian follicles [32] The potentialimpact of OS on the wellbeing of primordial growing andpreovulatory follicles as well as oocytes and early embryosexamining cell types and molecular targets has been exten-sively reviewed [32] Meanwhile ROS-induced apoptotic celldeath is involved in the mechanisms of corpus luteum (CL)regression that occurs at the end of the nonfertile cycle [33]
The role of OS in female reproduction is becomingincreasingly important as recent evidence suggests that itplays a part in conditions such as polycystic ovary syndrome(PCOS) endometriosis unexplained fertility spontaneousabortions preeclampsia hydatidiform mole embryopathiespreterm labor and intrauterine growth retardation [31] Agar-wal et al have recently reviewed the role of OS in normal andabnormal female reproductive physiological processes ana-lyzing the exact mechanisms of redox cell signaling and thepathophysiology of OS-related reproductive diseases [34] Aspecial comment should be made on endometriosis patientswhere iron overload has been demonstrated in the differentcompartments of the peritoneal cavity (peritoneal fluidendometriotic lesions peritoneum and macrophages) [35]This iron overload affects numerous mechanisms involvedin endometriosis development [35] Iron-induced OS maybe involved in endometriosis-associated infertility and mayplay a role in the regulation of the expression of genesencoding immunoregulators cytokines and cell adhesionmolecules implicated in the pathogenesis of endometriosis[36] Moreover a recent study investigated the relation-ship between OS and the underlying causes of infertilitypreovulatory ovarian hormones and ovarian response togonadotropin stimulation in patients undergoing ART [37]There was no significant relationship between plasma orfollicular fluid (FF) total antioxidant capacity (TAC) and theunderlying etiology of infertility [37] However there was astatistically significant positive association between FF E(2)levels and TAC OS has an impact on the production ofgranulosa cell steroid hormones in particular E(2) which isan important predictor of ovarian response [37] Thus thepossible impaired ovarian response in BTM women couldbe probably caused by dysregulation in the production ofgranulosa cell steroid hormones such as E(2) Meanwhile ithas been suggested that OSmodulates the age-related declinein fertility [20] Additionally a recent study indicated thatnonheme iron accumulation on ovarian stromal tissue maybe related to aging of the ovary due to increasing OS [38]Theage-related decline in fertility due to OS has a special impactin our group of patients because of their increased age aver-age due to significant improvements in chelation treatmentmodalities Furthermore remarkable is another study which
evaluated retinol and alpha-tocopherol natural antioxidantsthat inhibit lipid peroxidation and protect against cell damageinduced by OS and revealed that lower concentrations ofthese natural antioxidants were associated with abnormalsemen parameters in men and anovulation in women [39]
4 Evidence-Based Effect of Iron Overloadand Iron-Induced OS on Hypothalamic-Pituitary-Gonadal Axis and FemaleReproductive System
Although there are limited data directly correlating iron over-load with iron-induced OS on BTM femalesrsquo hypothalamic-pituitary-gonadal axis and ovarian reserve indirect conclu-sions could be obtained through the model of hemochro-matosis
41 The Model of Hemochromatosis Endocrinopathies arecommon in transfusion-associated haemochromatosis [40]while HH is the most frequent endocrine abnormality inhemochromatosis [41] The gonadotropin responsiveness to100 micrograms of LHRH was impaired or absent in patientswith hemochromatosis [42] Also in a cohort of 115 patientssuffering from genetic hemochromatosis hypogonadismwasevidenced in 42 of them inmost of which it was consideredas secondary to pituitary lesions as assessed by GnRH tests[43] Moreover in male patients with idiopathic hemochro-matosis testicular atrophy has been suggested to be causedby insufficient secretion of gonadotropins due to the selectiveaccumulation of iron in gonadotropic cells of the pituitarygland [44] Meanwhile subnormal gonadotropin responsesto GnRH but normal ovarian reserve as shown by normalfollicular stimulation with hMG were reported in a case ofHH in a female with biopsy-proven hemochromatosis [45]In another case report recovery of reproductive functionsdocumented by hormone measurements testicular biopsyand semen analysis was observed in a 37-year-old man withHH due to idiopathic hemochromatosis after phlebotomy[46] It has been also proposed that subjects with lesserdegrees of hepatic siderosis at diagnosis are unlikely todevelop hypogonadism [47] Furthermore the pituitary ofa 69-year-old man with hemochromatosis had been pre-viously removed at autopsy and was studied by histologyhistochemistry immunocytochemistry electron microscopyand X-ray diffraction [48] Preferential localization of irondeposits was demonstrated in gonadotrophs which at theultrastructural level displayed selective severe cellular injury[48] X-ray diffraction revealed the deposition of iron-accumulated lysosomes while iron storage was also notedin stellate cells [48] It should be also noted that in a groupof 7 young male patients with genetic hemochromatosis thenormal or high increments of LH after LHRH stimulationsuggested that secretion capacity of LH was intact andthat hypothalamic dysfunction could be responsible for theobserved preclinical gonadal deficiency [49] A similar resultwas obtained in another male patient where although thepituitary secretion of LH was normal in response to GnRHstimulation clomiphene administration did not produce an
Anemia 5
increase in LH and FSH suggesting that there was a defect inthe hypothalamic GnRH response [50]
In agreement with the hemochromatosis model abnor-malities of the hypothalamic-pituitary-gonadal axis are themost common endocrine abnormalities in patients withBTM as they require multiple blood transfusions leading tohemochromatosis [51] Thus based on the model of hemo-chromatosis that resembles iron-overloaded patients withBTM it seems that abnormalities of ovulation and menstru-ation in these patients are most likely because of inadequatepituitary responsiveness to GnRH [45]
42 Direct and Indirect Evidence for the Hypothalamic-Pitui-tary and the Gonadal Effect of Iron Patients with transfu-sional iron overload begin to develop pituitary iron overloadin the first decade of life however clinically significantvolume loss was not observed until the second decadeof life [52] Pituitary iron overload and volume loss wereindependently predictive of hypogonadism [52] Pituitary R2correlated significantly with serum ferritin as well as liverpancreatic and cardiac iron deposition by MRI [52] Manypatients with moderate-to-severe pituitary iron overloadretained normal gland volume and function representing apotential therapeutic window [52] According to a differentstudy BTM patients with severe organ damage and ironoverload are likely to be apulsatile with irreversible damageto their hypothalamic-pituitary axis while those with less-severe iron overload are likely to have potentially reversibleHH [53]The same study suggested that gonadotrophin pulseparameters rather than the gonadotrophin response to aGnRH bolus following prolonged pulsatile GnRH infusionmay be more useful in discriminating reversible from irre-versible HH [53] Furthermore in a study of 33 patients above15 years of age with transfusion-dependent BTM and ironoverload anterior pituitary function (GnRH stimulation test)correlated well with MRI results However no correlationwas found between the MRI measurements the GnRHstimulation test and the clinical status of the patients as 28out of the 33 patients achieved normal puberty [54] Anotherpossible mechanism of iron effect on hypothalamic-pituitaryaxis is through iron-induced OS with subsequent alterationson elongation factor-2 (eEF-2) levels The hypothalamic-pituitary system secretes peptide hormones whose synthesisrequires the integrity of the translation machinery Amongthe possible causes of the decline of translation in oldanimals are the modifications of eEF-2 [55] Iron-induced OScould be involved in the alterations of eEF-2 which formsadducts with MDA and 4-hydroxynonenal (HNE) [55] Thealterations of eEF-2 levels secondary to lipid peroxidationand adduct formation with these aldehydes could contributeto the suboptimal hormone production from these tissues[55] Moreover the possible concurrent GH deficiency maypotentiate the already present OS as patients with GHdeficiency have an increased degree of OS and endothelialdysfunction which possibly acts synergistically with iron-induced OS [56] Thus although there is limited evidenceon the exact pathophysiological mechanisms of iron effecton hypothalamic-pituitary axis it seems to be the basic
pathogenetic cause of the impaired hypothalamic-pituitarysystem
Meanwhile according to our knowledge only one studyexists which proves the iron deposition on the femalereproductive system in patients with BTM This particularstudy obtained histopathological evidence that depositionof haemosiderin occurred in the endometrial glandularepithelium of three patients with BTM [57] This depositionwas mainly evident in the apical part of these cells abovethe nuclei and should be taken into consideration as acontributing factor to the infertility in these patients byaltering endometrial receptivity for implantation [57] In twopatients who received effective iron chelating treatment withdesferrioxamine the endometrial haemosiderin depositseither disappeared or were significantly reduced [57]
43 Available Studies Directly Correlating Iron and Its Impacton Fertility in Women with BTM The pathophysiology ofiron-induced compromised fertility in women with BTMwas only recently evaluated [9] Low gonadotropin secretionresulted in reduced ovarian antral follicle count and ovarianvolume but levels of antimullerian hormone (AMH) a sensi-tive marker for ovarian reserve independent of gonadotropineffect were mostly normal AMH correlated with NTBI sug-gesting a role of labile iron in the pathogenesis of decreasedreproductive capacity possibly occurring in parallel to car-diac iron toxicity as cardiac iron was associated with thepresence of amenorrhea and with NTBI levels Thus AMHwas suggested to be valuable for future studies aiming atimproved chelation for fertility preservation whereas NTBIand labile plasma iron was suggested to be valuable formonitoring iron effect on the reproductive system [9] Thesame research team explored the relationship between liveriron concentration (LIC) and fertility status in 26 females(mean 30 years old) with BTM Seventeen (65) of themexperienced PA or SA Levels of LHFSH and estradiol werelow or undetectable in 48 and 35 of patients respectivelyand did not correlate with age presence of amenorrhea andLIC The fact that LHFSH and estradiol commonly usedfor assessment of fertility potential in thalassemia had apoor predictive value addressed the need for utilization ofcurrent available methods for assessment of fertility capacityin thalassemia [58]
5 Potential Antioxidants in BTM
Considering all the above we suggest that the enhancedOS observed in iron-overloaded patients with BTM mayplay a significant role in their reduced reproductive abilityThe investigation of the proper antioxidants for fertility andpregnancy in BTM female patients which are recognized aspatients of increased OS is of great value and importanceThe increased age average of this group of patients underlinesthe increased importance of OS on the female reproductivesystem as it has been also connected with aging Howeverdespite the clear identification of the oxidativeantioxidativeimbalance in patients with BTM there are few studies
6 Anemia
evaluating the effect of different antioxidant supplementationin BTM-related morbidities such as infertility
51 Antioxidant Supplements Used in BTM The benefits ofvitamin C and vitamin E as antioxidant supplements inBTMchildren have been previously determined [59] Twentychildren who had laboratory confirmation of BTM at least 6months with history of packed red cell transfusion withoutiron chelation were recruited It was suggested that vitaminC plus vitamin E supplementations have benefits more thanvitamin E alone in promoting antioxidant status and mayenhance liver function as total bilirubin tends to decrease[59] Furthermore curcuminoids extracted from the spiceturmeric are known to have antioxidant and iron-chelatingproperties and have been proposed as a potential upstreamtherapy of thalassemiaWeeraphan et al have recently appliedproteomic techniques to study the protein profile and oxida-tive damage in the plasma of beta-thalassemiaHb E patientsbefore and after treatment with curcuminoids Their studyindicated the ameliorating role of curcuminoids towards OSand iron overload in the plasma proteome [60] Glutaminealpha-lipoic acid acetyl-L-carnitine and N-acetylcysteineare also recently being studied as antioxidant supplements forsickle cell disease and thalassemia [61] Finally the value ofantioxidant supplements in the elimination of iron-inducedOS and subsequent infertility issues could be speculatedby the fact that various antioxidants (such as carnitinevitamin C vitamin E selenium carotenoids glutathioneN-acetylcysteine zinc folic acid and coenzyme Q10) arevariably effective in OS-induced male-factor infertility withrespect to improving semen parameters and pregnancy rates[62]
52 Chelation Treatments as Antioxidants in BTM Differentstudies have also focused on the antioxidant capacity of differ-ent chelation treatment modalities Increased evidence fromin vitro in vivo and clinical studies suggest that deferiprone(L1) can be used as a potent pharmaceutical antioxidant bymobilizing labile iron and copper andor inhibiting theircatalytic activity in the formation of free radicals and OS intissue damage [63] In contrast to L1 both desferrioxamine(DFO) and deferasirox (DFRA) were suggested to havemajordisadvantages in their use in noniron loading conditionsdue to toxicity implications [63] Meanwhile a subsequentstudy indicated that DFO chelation therapy does not nor-malize ferritin levels but attenuates oxidative damage andimproves total antioxidant level in Malaysian Chinese BTMpatients [64] The objective of this research was to studythe oxidant-antioxidant indices in BTM patients who wereon desferrioxamine-chelation or without chelation therapyBlood was collected from 39 Chinese patients and 20 con-trols Plasma and peripheral blood mononuclear cell lysates(PBMC) were extracted and biochemical tests to evaluate OSwere performedOSwas evident in these patients as advancedoxidized protein products (AOPP) and lipid hydroperoxideswere elevated whereas glutathione peroxidase activity andthe ferric reducing antioxidant power (FRAP) were reducedThe catalase activity in the patientsrsquo PBMC was elevated
possibly as a compensatory mechanism for the reducedglutathione peroxidase activity in both red blood cells andPBMC The lower FRAP and higher AOPP levels in thenonchelated patients compared with the chelated patientswere indicative of a lower OS level in the chelated patients[64] An additional study which assessed whether oxidant-stress and inflammation in BTM could be controlled byDFRA as effectively as by DFO revealed equal effectivenessin decreasing iron burden and levels of the oxidative-stressmarker MDA [65]
53 The Possible Effect of Advanced Glycation End Products(AGEs) Regulation on BTM Womenrsquos Ovarian Function andFertility Recent data have shown that OS is involved in thepathophysiology of anovulation [20 66 67] While the roleof OS in ovulatory dysfunction has been sufficiently studied[29 68] advanced glycation end products (AGEs) have beenrecognized as mediators of increased OS [69 70] Advancedglycation end products (AGEs) are a heterogeneous group ofbioactive molecules formed by the nonenzymatic glycationof proteins lipids and nucleic acids [71] There is increasingevidence that AGEs play a pivotal role in atherosclerosis andin diabetes and its complications while AGE accumulationis a measure of cumulative metabolic and OS and mayso represent the ldquometabolic memoryrdquo [72] Engagement oftheir receptor RAGE with AGEs is shown to activate itsdownstream signaling and evoke OS and inflammation indiabetes [73] AGEs have been found to induce OS andconversely OS stimulates AGEs formation [74ndash76]
AGEs deposition in ovary dysregulate ovarian functionthrough the induction of androgen production as well as OSgeneration through the induction ofNF-K120573pathway leadingto increased production of atherogenic and inflammatorymolecules AGEs have been implicated in the developmentof insulin resistance hyperandrogenism and anovulationin polycystic ovary syndrome (PCOS) and seem to have acentral role in PCOS pathophysiology either as a marker ofOS or through their specific actions after their ligation totheir specific receptor RAGE [77] Furthermore there is sub-stantial evidence that insulin resistance constitutes one of themain pathophysiological mechanisms leading to anovulationand ovarian hyperandrogenism in PCOS patients Regardingthe above also that iron has been implicated in abnormalinsulin secretion in patients with BTM or hemochromatosis[44 78] and that OS might be responsible for a decline ininsulin-mediated glucose uptake in BTM patients leadingto insulin resistance [79] we consider that the evaluationof AGEs as markers of OS in relation to iron overloadinsulin resistance and ovulation potential would be of greatvalue Reducing AGEs in BTM females could probably havebeneficial effects in insulin resistance and ovulation potentialand thus in fertility potential Finally it is remarkable thatthe iron chelator Desferal had a retardation effect on thefunctional and structural changes of Hb during fructation[80] It could prevent the AGEs and carbonyl formations andhelix depletion during theHb fructation processMoreover itcould preserve peroxidase and esterase activities of fructated
Anemia 7
Hb similar to native Hb Therefore desferal could be intro-duced as an antiglycation drug to prevent theAGEs formation[80]
6 Conclusions
On the basis of all the presented data it can be concludedthatOS plays amajor role in the pathophysiology of infertilityin females with thalassemia This OS is mainly caused bytissue injury due to overproduction of free radicals bysecondary iron overload alteration in serum trace elementsand alteration in antioxidant enzymes level Consequentlythere is a rationale for iron chelation to eliminate the free-iron species which in this respect act like antioxidantsAntioxidants are also capable of ameliorating increased OSparameters and given together with iron chelators mayprovide a substantial improvement in the pathophysiologyof thalassemia [81] However there is no study evaluatingthe efficacy of antioxidant supplementation on BTMwomenrsquosfertility potential In agreement with previous suggestionswe consider that the application of treatment strategies thatwould reduceOS in the reproductive tract could help infertilewomen with diseases such as BTM that are caused byROSantioxidants imbalance [29] In general research isin progress to identify the mechanisms that are involvedin the etiology of female reproductive diseases caused byROS and to create effective strategies that can counteractOS [29] while few are the trials investigating antioxidantsupplementation in female reproduction [20] The admin-istration of selective antioxidants along with essential traceelements and minerals to reduce the extent of oxidativedamage and related complications such as infertility in BTMpatients still needs further evaluation [24] However beforeclinicians recommend antioxidants randomized controlledtrials with sufficient power are necessary to prove the efficacyof antioxidant therapeutic strategies in disorders of femalereproduction [20] such as BTMThis is strongly emerged bythe fact of prolonged survival and the newly recognized issuesand challenges that adults with BTM face [82]
References
[1] C Hershko ldquoPathogenesis and management of iron toxicity inthalassemiardquo Annals of the New York Academy of Sciences vol1202 pp 1ndash9 2010
[2] F Waseem K A Khemomal and R Sajid ldquoAntioxidant statusin beta thalassemia major a single-center studyrdquo Indian Journalof Pathology and Microbiology vol 54 no 4 pp 761ndash763 2011
[3] R Origa A Piga G Quarta et al ldquoPregnancy and 120573-thalassemia an Italian multicenter experiencerdquoHaematologicavol 95 no 3 pp 376ndash381 2010
[4] N Skordis L Petrikkos M Toumba et al ldquoUpdate on fertilityin thalassaemia majorrdquo Pediatric Endocrinology Reviews vol 2supplement 2 pp 296ndash302 2004
[5] M Toumba A Sergis C Kanaris and N Skordis ldquoEndocrinecomplications in patients with thalassaemia majorrdquo PediatricEndocrinology Reviews vol 5 no 2 pp 642ndash648 2007
[6] E A Rachmilewitz O Weizer-Stern K Adamsky et al ldquoRoleof iron in inducing oxidative stress in thalassemia can it be
prevented by inhibition of absorption and by antioxidantsrdquoAnnals of the New York Academy of Sciences vol 1054 pp 118ndash123 2005
[7] S Ansari A Azarkeivan and A Tabaroki ldquoPregnancy inpatients treated for beta thalassemia major in two centers(Ali Asghar Childrenrsquos Hospital and Thalassemia Clinic) out-come for mothers and newborn infantsrdquo Pediatric Hematology-Oncology vol 23 no 1 pp 33ndash37 2006
[8] M R Safarinejad ldquoReproductive hormones and hypothalamic-pituitary-ovarian axis in female patients with homozygous 120573-thalassemia majorrdquo Journal of Pediatric HematologyOncologyvol 32 no 4 pp 259ndash266 2010
[9] S T Singer E P Vichinsky G Gildengorin J van DisseldorpM Rosen and M I Cedars ldquoReproductive capacity in ironoverloaded women with thalassemia majorrdquo Blood vol 118 no10 pp 2878ndash2881 2011
[10] G Vizziello D Carone E Caroppo A Vitti A Pasquad-ibisceglie and G Drsquoamato ldquoOvulation induction with gona-dotropin in patients with thalassemia pretreated with pulsatileGnRH outcomerdquoMinerva Ginecologica vol 56 no 5 pp 485ndash487 2004
[11] N Skordis S Christou M Koliou N Pavlides and M Angas-tiniotis ldquoFertility in female patients with thalassemiardquo Journalof Pediatric Endocrinology and Metabolism vol 11 supplement3 pp 935ndash943 1998
[12] LDanesiM Scacchi AMMiragoli et al ldquoInduction of folliclematuration and ovulation by gonadotropin administration inwomen with 120573-thalassemiardquo European Journal of Endocrinol-ogy vol 131 no 6 pp 602ndash606 1994
[13] R Bajoria and R Chatterjee ldquoCurrent perspectives of fertilityand pregnancy in thalassemiardquoHemoglobin vol 33 supplement1 pp S131ndashS135 2009
[14] R Bajoria and R Chatterjee ldquoHypogonadotrophic hypogo-nadism and diminished gonadal reserve accounts for dys-functional gametogenesis in thalassaemia patients with ironoverload presenting with infertilityrdquoHemoglobin vol 35 no 5-6 pp 636ndash642 2011
[15] M Karagiorga-Lagana ldquoFertility in thalassemia the Greekexperiencerdquo Journal of Pediatric Endocrinology andMetabolismvol 11 supplement 3 pp 945ndash951 1998
[16] S M Tuck ldquoFertility and pregnancy in thalassemia majorrdquoAnnals of the New York Academy of Sciences vol 1054 pp 300ndash307 2005
[17] D Surbek A Koller and N Pavic ldquoSuccessful twin pregnancyin homozygous 120573-thalassemia after ovulation induction withgrowth hormone and gonadotropinsrdquo Fertility and Sterility vol65 no 3 pp 670ndash672 1996
[18] K Yamaguchi M Mandai S Toyokuni et al ldquoContents ofendometriotic cysts especially the high concentration of freeiron are a possible cause of carcinogenesis in the cysts throughthe iron-induced persistent oxidative stressrdquo Clinical CancerResearch vol 14 no 1 pp 32ndash40 2008
[19] M C Kew ldquoHepatic iron overload and hepatocellular carci-nomardquo Cancer Letters vol 286 no 1 pp 38ndash43 2009
[20] AAgarwal S Gupta andRK Sharma ldquoRole of oxidative stressin female reproductionrdquo Reproductive Biology and Endocrinol-ogy vol 3 article 28 2005
[21] A C Chan C K Chow and D Chiu ldquoInteraction of antiox-idants and their implication in genetic anemiardquo Proceedings ofthe Society for Experimental Biology and Medicine vol 222 no3 pp 274ndash282 1999
8 Anemia
[22] A Agarwal A Aponte-Mellado B J Premkumar A Shamanand S Gupta ldquoThe effects of oxidative stress on female repro-duction a reviewrdquo Reproductive Biology and Endocrinology vol10 article 49 2012
[23] M Giergiel M Lopucki N Stachowicz and M KankoferldquoThe influence of age and gender on antioxidant enzymeactivities in humans and laboratory animalsrdquoAging Clinical andExperimental Research vol 24 pp 551ndash559 2012
[24] Q Shazia Z H Mohammad T Rahman and H U ShekharldquoCorrelation of oxidative stress with serum trace element levelsand antioxidant enzyme status in Beta thalassemia majorpatients a review of the literaturerdquo Anemia vol 2012 ArticleID 270923 7 pages 2012
[25] M Y Abdalla M Fawzi S R Al-Maloul N El-Banna R FTayyem and I M Ahmad ldquoIncreased oxidative stress and ironoverload in Jordanian120573-thalassemic childrenrdquoHemoglobin vol35 no 1 pp 67ndash79 2011
[26] R A Ghone K M Kumbar A N Suryakar R V Katkam andN G Joshi ldquoOxidative stress and disturbance in antioxidantbalance in beta thalassemia majorrdquo Indian Journal of ClinicalBiochemistry vol 23 no 4 pp 337ndash340 2008
[27] MA Livrea L Tesoriere AM Pintaudi et al ldquoOxidative stressand antioxidant status in 120573-thalassemia major iron overloadand depletion of lipid-soluble antioxidantsrdquo Blood vol 88 no9 pp 3608ndash3614 1996
[28] S-S Chiou T-T Chang S-P Tsai et al ldquoLipid peroxidationand antioxidative status in 120573-thalassemia major patients withor without hepatitis C virus infectionrdquo Clinical Chemistry andLaboratory Medicine vol 44 no 10 pp 1226ndash1233 2006
[29] A Agarwal and S S Allamaneni ldquoRole of free radicals in femalereproductive diseases and assisted reproductionrdquo ReproductiveBioMedicine Online vol 9 no 3 pp 338ndash347 2004
[30] E H Ruder T J Hartman J Blumberg and M B GoldmanldquoOxidative stress and antioxidants exposure and impact onfemale fertilityrdquoHuman Reproduction Update vol 14 no 4 pp345ndash357 2008
[31] A Agarwal S Gupta L Sekhon and R Shah ldquoRedox con-siderations in female reproductive function and assisted repro-duction from molecular mechanisms to health implicationsrdquoAntioxidants amp Redox Signaling vol 10 no 8 pp 1375ndash14032008
[32] P J Devine S D Perreault and U Luderer ldquoRoles of reactiveoxygen species and antioxidants in ovarian toxicityrdquo Biology ofReproduction vol 86 no 2 article 27 2012
[33] K H Al-Gubory C Garrel P Faure and N Sugino ldquoRolesof antioxidant enzymes in corpus luteum rescue from reac-tive oxygen species-induced oxidative stressrdquo ReproductiveBiomedicine Online vol 25 no 6 pp 551ndash560 2012
[34] A Agarwal A Aponte-Mellado B J Premkumar A Shamanand S Gupta ldquoThe effects of oxidative stress on female repro-duction a reviewrdquo Reproductive Biology and Endocrinology vol10 article 49 2012
[35] S Defrere R Gonzalez-Ramos J-C Lousse et al ldquoInsightsinto iron and nuclear factor-kappa B (NF-120581B) involvement inchronic inflammatory processes in peritoneal endometriosisrdquoHistology and Histopathology vol 26 no 8 pp 1083ndash1092 2011
[36] A van Langendonckt F Casanas-Roux and J Donnez ldquoOxida-tive stress and peritoneal endometriosisrdquo Fertility and Sterilityvol 77 no 5 pp 861ndash870 2002
[37] M Appasamy E Jauniaux P Serhal A Al-Qahtani N PGroome and S Muttukrishna ldquoEvaluation of the relationshipbetween follicular fluid oxidative stress ovarian hormones and
response to gonadotropin stimulationrdquo Fertility and Sterilityvol 89 no 4 pp 912ndash921 2008
[38] Y Asano ldquoAge-related accumulation of non-heme ferric andferrous iron in mouse ovarian stroma visualized by sensitivenon-heme iron histochemistryrdquo The Journal of Histochemistryamp Cytochemistry vol 60 no 3 pp 229ndash242 2012
[39] M K Al-Azemi A E Omu T Fatinikun N Mannazhathand S Abraham ldquoFactors contributing to gender differences inserum retinol and 120572-tocopherol in infertile couplesrdquo Reproduc-tive BioMedicine Online vol 19 no 4 pp 583ndash590 2009
[40] M K Kim J W Lee K H Baek et al ldquoEndocrinopathies intransfusion-associated iron overloadrdquo Clinical Endocrinologyvol 78 no 2 pp 271ndash277 2013
[41] L M Hempenius P S van Dam J J Marx and H PKoppeschaar ldquoMineralocorticoid status and endocrine dys-function in severe hemochromatosisrdquo Journal of Endocrinolog-ical Investigation vol 22 no 5 pp 369ndash376 1999
[42] J M Vasquez and R B Greenblatt ldquoPituitary responsiveness toluteinizing-hormone-releasing hormone in different reproduc-tive disorders a reviewrdquo Journal of ReproductiveMedicine for theObstetrician and Gynecologist vol 30 no 8 pp 591ndash600 1985
[43] I Paris M Hermans and M Buysschaert ldquoEndocrine compli-cations of genetic hemochromatosisrdquo Acta Clinica Belgica vol54 no 6 pp 334ndash345 1999
[44] W Stremmel C Niederau M Berger H-K Kley H-LKruskemper and G Strohmeyer ldquoAbnormalities in estrogenandrogen and insulin metabolism in idiopathic hemochro-matosisrdquo Annals of the New York Academy of Sciences vol 526pp 209ndash223 1988
[45] W R Meyer K A Hutchinson-Williams E E Jones and A HDecherney ldquoSecondary hypogonadism in hemochromatosisrdquoFertility and Sterility vol 54 no 4 pp 740ndash742 1990
[46] L J Siemons and C H Mahler ldquoHypogonadotropic hypogo-nadism in hemochromatosis recovery of reproductive functionafter iron depletionrdquo The Journal of Clinical Endocrinology andMetabolism vol 65 no 3 pp 585ndash587 1987
[47] J H McDermott and C H Walsh ldquoHypogonadism in hered-itary hemochromatosisrdquo The Journal of Clinical Endocrinologyand Metabolism vol 90 no 4 pp 2451ndash2455 2005
[48] G Kontogeorgos S Handy K Kovacs E Horvath and BW Scheithauer ldquoThe anterior pituitary in hemochromatosisrdquoEndocrine Pathology vol 7 no 2 pp 159ndash164 1996
[49] A Piperno M R Rivolta R Drsquoalba et al ldquoPreclinical hypog-onadism in genetic hemochromatosis in the early stage ofthe disease evidence of hypothalamic dysfunctionrdquo Journal ofEndocrinological Investigation vol 15 no 6 pp 423ndash428 1992
[50] K SiminoskiM Drsquocosta and P GWalfish ldquoHypogonadotropichypogonadism in idiopathic hemochromatosis evidence forcombined hypothalamic and pituitary involvementrdquo Journal ofEndocrinological Investigation vol 13 no 10 pp 849ndash853 1990
[51] K E Oerter G A Kamp P J Munson A W Nienhuis F GCassorla and P K Manasco ldquoMultiple hormone deficienciesin children with hemochromatosisrdquo The Journal of ClinicalEndocrinology and Metabolism vol 76 no 2 pp 357ndash361 1993
[52] L J Noetzli A Panigrahy S D Mittelman et al ldquoPituitaryiron and volume predict hypogonadism in transfusional ironoverloadrdquo American Journal of Hematology vol 87 no 2 pp167ndash171 2012
[53] R Chatterjee and M Katz ldquoReversible hypogonadotrophichypogonadism in sexually infantile male thalassaemic patientswith transfusional iron overloadrdquo Clinical Endocrinology vol53 no 1 pp 33ndash42 2000
Anemia 9
[54] M Berkovitch T Bistritzer S D Milone K Perlman WKucharczyk and N F Olivieri ldquoIron deposition in the anteriorpituitary in homozygous beta-thalassemia MRI evaluationand correlation with gonadal functionrdquo Journal of PediatricEndocrinology amp Metabolism vol 13 no 2 pp 179ndash184 2000
[55] S Arguelles M Cano A Machado and A Ayala ldquoEffect ofaging and oxidative stress on elongation factor-2 in hypothala-mus and hypophysisrdquo Mechanisms of Ageing and Developmentvol 132 no 1-2 pp 55ndash64 2011
[56] D Gonzalez-Duarte A Madrazo-Atutxa A Soto-Moreno andA Leal-Cerro ldquoMeasurement of oxidative stress and endothe-lial dysfunction in patients with hypopituitarism and severedeficiency adult growth hormone deficiencyrdquo Pituitary vol 15no 4 pp 589ndash597 2012
[57] A Birkenfeld A W Goldfarb E A Rachmilewitz J GSchenker andEOkon ldquoEndometrial glandular haemosiderosisin homozygous beta-thalassaemiardquo European Journal of Obstet-rics Gynecology and Reproductive Biology vol 31 no 2 pp 173ndash178 1989
[58] S T Singer N Sweeters O Vega A Higa E Vichinsky andM Cedars ldquoFertility potential in thalassemia major womencurrent findings and future diagnostic toolsrdquo Annals of the NewYork Academy of Sciences vol 1202 pp 226ndash230 2010
[59] T Dissayabutra P Tosukhowong and P Seksan ldquoThe benefitsof vitamin C and vitamin E in children with beta-thalassemiawith high oxidative stressrdquo Journal of the Medical Association ofThailand vol 88 supplement 4 pp S317ndash321 2005
[60] C Weeraphan C Srisomsap D Chokchaichamnankit et alldquoRole of curcuminoids in ameliorating oxidative modificationin beta-thalassemiaHb E plasma proteomerdquo The Journal ofNutritional Biochemistry vol 24 no 3 pp 578ndash585 2012
[61] E Vichinsky ldquoEmerging ldquoArdquo therapies in hemoglobinopathiesagonists antagonists antioxidants and argininerdquo HematologyAmerican Society Hematology Education Program vol 2012 no1 pp 271ndash275 2012
[62] C Mora-Esteves and D Shin ldquoNutrient supplementationimproving male fertility fourfoldrdquo Seminars in ReproductiveMedicine vol 31 no 4 pp 293ndash300 2013
[63] G J Kontoghiorghes A Efstathiou M Kleanthous YMichaelides and A Kolnagou ldquoRiskbenefit assessmentadvantages over other drugs and targeting methods in the useof deferiprone as a pharmaceutical antioxidant in iron loadingand non iron loading conditionsrdquo Hemoglobin vol 33 no 5pp 386ndash397 2009
[64] U R Kuppusamy and J A Tan ldquoChelation therapy withdesferrioxamine does not normalize ferritin level but attenu-ates oxidative damage and improves total antioxidant level inMalaysian Chinese beta-thalassaemia major patientsrdquoTheWestIndian Medical Journal vol 60 no 1 pp 3ndash8 2011
[65] P B Walter E A Macklin J Porter et al ldquoInflammationand oxidant-stress in 120573-thalassemia patients treated with ironchelators deferasirox (ICL670) or deferoxamine an ancillarystudy of the Novartis CICL670A0107 trialrdquo Haematologica vol93 no 6 pp 817ndash825 2008
[66] V Fenkci S Fenkci M Yilmazer and M Serteser ldquoDecreasedtotal antioxidant status and increased oxidative stress in womenwith polycystic ovary syndrome may contribute to the risk ofcardiovascular diseaserdquo Fertility and Sterility vol 80 no 1 pp123ndash127 2003
[67] C Tatone M C Carbone S Falone et al ldquoAge-dependentchanges in the expression of superoxide dismutases and catalaseare associated with ultrastructural modifications in human
granulosa cellsrdquoMolecular Human Reproduction vol 12 no 11pp 655ndash660 2006
[68] F Gonzalez N S Rote J Minium and J P Kirwan ldquoReactiveoxygen species-induced oxidative stress in the developmentof insulin resistance and hyperandrogenism in polycysticovary syndromerdquo The Journal of Clinical Endocrinology andMetabolism vol 91 no 1 pp 336ndash340 2006
[69] G Basta G Lazzerini M Massaro et al ldquoAdvanced gly-cation end products activate endothelium through signal-transduction receptor RAGE a mechanism for amplification ofinflammatory responsesrdquo Circulation vol 105 no 7 pp 816ndash822 2002
[70] E Devangelio F Santilli G Formoso et al ldquoSoluble RAGE intype 2 diabetes association with oxidative stressrdquo Free RadicalBiology and Medicine vol 43 no 4 pp 511ndash518 2007
[71] G Basta A M Schmidt and R de Caterina ldquoAdvancedglycation end products and vascular inflammation implica-tions for accelerated atherosclerosis in diabetesrdquoCardiovascularResearch vol 63 no 4 pp 582ndash592 2004
[72] R Meerwaldt T Links C Zeebregts R Tio J-L Hillebrandsand A Smit ldquoThe clinical relevance of assessing advanced gly-cation endproducts accumulation in diabetesrdquo CardiovascularDiabetology vol 7 article 29 2008
[73] H Unoki and S Yamagishi ldquoAdvanced glycation end productsand insulin resistancerdquo Current Pharmaceutical Design vol 14no 10 pp 987ndash989 2008
[74] E Diamanti-Kandarakis C Piperi A Kalofoutis and GCreatsas ldquoIncreased levels of serum advanced glycation end-products in women with polycystic ovary syndromerdquo ClinicalEndocrinology vol 62 no 1 pp 37ndash43 2005
[75] D R Mccance D G Dyer J A Dunn et al ldquoMaillardreaction products and their relation to complications in insulin-dependent diabetes mellitusrdquo Journal of Clinical Investigationvol 91 no 6 pp 2470ndash2478 1993
[76] R Singh A Barden TMori and L Beilin ldquoAdvanced glycationend-products a reviewrdquoDiabetologia vol 44 no 2 pp 129ndash1462001
[77] E Diamanti-Kandarakis A Piouka S Livadas et al ldquoAnti-mullerian hormone is associated with advanced glycosylatedend products in lean women with polycystic ovary syndromerdquoEuropean Journal of Endocrinology vol 160 no 5 pp 847ndash8532009
[78] R Chatterjee and R Bajoria ldquoNew concept in natural historyand management of diabetes mellitus in thalassemia majordiabetes and thalassaemiardquo Hemoglobin vol 33 supplement 1pp S127ndashS130 2009
[79] G Paolisso M R Tagliamonte M R Rizzo and D GiuglianoldquoAdvancing age and insulin resistance new facts about anancient historyrdquo European Journal of Clinical Investigation vol29 no 9 pp 758ndash769 1999
[80] N Sattarahmady H Heli and A A Moosavi-Movahedi ldquoDes-feral as improving agent for hemoglobin fructation structuraland functional impactsrdquo The Protein Journal vol 31 no 8 pp651ndash655 2012
[81] E Fibach and E A Rachmilewitz ldquoThe role of antioxidantsand iron chelators in the treatment of oxidative stress inthalassemiardquo Annals of the New York Academy of Sciences vol1202 pp 10ndash16 2010
[82] L M Compagno ldquoCaring for adults with thalassemia in apediatric worldrdquo Annals of the New York Academy of Sciencesvol 1054 pp 266ndash272 2005
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

Anemia 5
increase in LH and FSH suggesting that there was a defect inthe hypothalamic GnRH response [50]
In agreement with the hemochromatosis model abnor-malities of the hypothalamic-pituitary-gonadal axis are themost common endocrine abnormalities in patients withBTM as they require multiple blood transfusions leading tohemochromatosis [51] Thus based on the model of hemo-chromatosis that resembles iron-overloaded patients withBTM it seems that abnormalities of ovulation and menstru-ation in these patients are most likely because of inadequatepituitary responsiveness to GnRH [45]
42 Direct and Indirect Evidence for the Hypothalamic-Pitui-tary and the Gonadal Effect of Iron Patients with transfu-sional iron overload begin to develop pituitary iron overloadin the first decade of life however clinically significantvolume loss was not observed until the second decadeof life [52] Pituitary iron overload and volume loss wereindependently predictive of hypogonadism [52] Pituitary R2correlated significantly with serum ferritin as well as liverpancreatic and cardiac iron deposition by MRI [52] Manypatients with moderate-to-severe pituitary iron overloadretained normal gland volume and function representing apotential therapeutic window [52] According to a differentstudy BTM patients with severe organ damage and ironoverload are likely to be apulsatile with irreversible damageto their hypothalamic-pituitary axis while those with less-severe iron overload are likely to have potentially reversibleHH [53]The same study suggested that gonadotrophin pulseparameters rather than the gonadotrophin response to aGnRH bolus following prolonged pulsatile GnRH infusionmay be more useful in discriminating reversible from irre-versible HH [53] Furthermore in a study of 33 patients above15 years of age with transfusion-dependent BTM and ironoverload anterior pituitary function (GnRH stimulation test)correlated well with MRI results However no correlationwas found between the MRI measurements the GnRHstimulation test and the clinical status of the patients as 28out of the 33 patients achieved normal puberty [54] Anotherpossible mechanism of iron effect on hypothalamic-pituitaryaxis is through iron-induced OS with subsequent alterationson elongation factor-2 (eEF-2) levels The hypothalamic-pituitary system secretes peptide hormones whose synthesisrequires the integrity of the translation machinery Amongthe possible causes of the decline of translation in oldanimals are the modifications of eEF-2 [55] Iron-induced OScould be involved in the alterations of eEF-2 which formsadducts with MDA and 4-hydroxynonenal (HNE) [55] Thealterations of eEF-2 levels secondary to lipid peroxidationand adduct formation with these aldehydes could contributeto the suboptimal hormone production from these tissues[55] Moreover the possible concurrent GH deficiency maypotentiate the already present OS as patients with GHdeficiency have an increased degree of OS and endothelialdysfunction which possibly acts synergistically with iron-induced OS [56] Thus although there is limited evidenceon the exact pathophysiological mechanisms of iron effecton hypothalamic-pituitary axis it seems to be the basic
pathogenetic cause of the impaired hypothalamic-pituitarysystem
Meanwhile according to our knowledge only one studyexists which proves the iron deposition on the femalereproductive system in patients with BTM This particularstudy obtained histopathological evidence that depositionof haemosiderin occurred in the endometrial glandularepithelium of three patients with BTM [57] This depositionwas mainly evident in the apical part of these cells abovethe nuclei and should be taken into consideration as acontributing factor to the infertility in these patients byaltering endometrial receptivity for implantation [57] In twopatients who received effective iron chelating treatment withdesferrioxamine the endometrial haemosiderin depositseither disappeared or were significantly reduced [57]
43 Available Studies Directly Correlating Iron and Its Impacton Fertility in Women with BTM The pathophysiology ofiron-induced compromised fertility in women with BTMwas only recently evaluated [9] Low gonadotropin secretionresulted in reduced ovarian antral follicle count and ovarianvolume but levels of antimullerian hormone (AMH) a sensi-tive marker for ovarian reserve independent of gonadotropineffect were mostly normal AMH correlated with NTBI sug-gesting a role of labile iron in the pathogenesis of decreasedreproductive capacity possibly occurring in parallel to car-diac iron toxicity as cardiac iron was associated with thepresence of amenorrhea and with NTBI levels Thus AMHwas suggested to be valuable for future studies aiming atimproved chelation for fertility preservation whereas NTBIand labile plasma iron was suggested to be valuable formonitoring iron effect on the reproductive system [9] Thesame research team explored the relationship between liveriron concentration (LIC) and fertility status in 26 females(mean 30 years old) with BTM Seventeen (65) of themexperienced PA or SA Levels of LHFSH and estradiol werelow or undetectable in 48 and 35 of patients respectivelyand did not correlate with age presence of amenorrhea andLIC The fact that LHFSH and estradiol commonly usedfor assessment of fertility potential in thalassemia had apoor predictive value addressed the need for utilization ofcurrent available methods for assessment of fertility capacityin thalassemia [58]
5 Potential Antioxidants in BTM
Considering all the above we suggest that the enhancedOS observed in iron-overloaded patients with BTM mayplay a significant role in their reduced reproductive abilityThe investigation of the proper antioxidants for fertility andpregnancy in BTM female patients which are recognized aspatients of increased OS is of great value and importanceThe increased age average of this group of patients underlinesthe increased importance of OS on the female reproductivesystem as it has been also connected with aging Howeverdespite the clear identification of the oxidativeantioxidativeimbalance in patients with BTM there are few studies
6 Anemia
evaluating the effect of different antioxidant supplementationin BTM-related morbidities such as infertility
51 Antioxidant Supplements Used in BTM The benefits ofvitamin C and vitamin E as antioxidant supplements inBTMchildren have been previously determined [59] Twentychildren who had laboratory confirmation of BTM at least 6months with history of packed red cell transfusion withoutiron chelation were recruited It was suggested that vitaminC plus vitamin E supplementations have benefits more thanvitamin E alone in promoting antioxidant status and mayenhance liver function as total bilirubin tends to decrease[59] Furthermore curcuminoids extracted from the spiceturmeric are known to have antioxidant and iron-chelatingproperties and have been proposed as a potential upstreamtherapy of thalassemiaWeeraphan et al have recently appliedproteomic techniques to study the protein profile and oxida-tive damage in the plasma of beta-thalassemiaHb E patientsbefore and after treatment with curcuminoids Their studyindicated the ameliorating role of curcuminoids towards OSand iron overload in the plasma proteome [60] Glutaminealpha-lipoic acid acetyl-L-carnitine and N-acetylcysteineare also recently being studied as antioxidant supplements forsickle cell disease and thalassemia [61] Finally the value ofantioxidant supplements in the elimination of iron-inducedOS and subsequent infertility issues could be speculatedby the fact that various antioxidants (such as carnitinevitamin C vitamin E selenium carotenoids glutathioneN-acetylcysteine zinc folic acid and coenzyme Q10) arevariably effective in OS-induced male-factor infertility withrespect to improving semen parameters and pregnancy rates[62]
52 Chelation Treatments as Antioxidants in BTM Differentstudies have also focused on the antioxidant capacity of differ-ent chelation treatment modalities Increased evidence fromin vitro in vivo and clinical studies suggest that deferiprone(L1) can be used as a potent pharmaceutical antioxidant bymobilizing labile iron and copper andor inhibiting theircatalytic activity in the formation of free radicals and OS intissue damage [63] In contrast to L1 both desferrioxamine(DFO) and deferasirox (DFRA) were suggested to havemajordisadvantages in their use in noniron loading conditionsdue to toxicity implications [63] Meanwhile a subsequentstudy indicated that DFO chelation therapy does not nor-malize ferritin levels but attenuates oxidative damage andimproves total antioxidant level in Malaysian Chinese BTMpatients [64] The objective of this research was to studythe oxidant-antioxidant indices in BTM patients who wereon desferrioxamine-chelation or without chelation therapyBlood was collected from 39 Chinese patients and 20 con-trols Plasma and peripheral blood mononuclear cell lysates(PBMC) were extracted and biochemical tests to evaluate OSwere performedOSwas evident in these patients as advancedoxidized protein products (AOPP) and lipid hydroperoxideswere elevated whereas glutathione peroxidase activity andthe ferric reducing antioxidant power (FRAP) were reducedThe catalase activity in the patientsrsquo PBMC was elevated
possibly as a compensatory mechanism for the reducedglutathione peroxidase activity in both red blood cells andPBMC The lower FRAP and higher AOPP levels in thenonchelated patients compared with the chelated patientswere indicative of a lower OS level in the chelated patients[64] An additional study which assessed whether oxidant-stress and inflammation in BTM could be controlled byDFRA as effectively as by DFO revealed equal effectivenessin decreasing iron burden and levels of the oxidative-stressmarker MDA [65]
53 The Possible Effect of Advanced Glycation End Products(AGEs) Regulation on BTM Womenrsquos Ovarian Function andFertility Recent data have shown that OS is involved in thepathophysiology of anovulation [20 66 67] While the roleof OS in ovulatory dysfunction has been sufficiently studied[29 68] advanced glycation end products (AGEs) have beenrecognized as mediators of increased OS [69 70] Advancedglycation end products (AGEs) are a heterogeneous group ofbioactive molecules formed by the nonenzymatic glycationof proteins lipids and nucleic acids [71] There is increasingevidence that AGEs play a pivotal role in atherosclerosis andin diabetes and its complications while AGE accumulationis a measure of cumulative metabolic and OS and mayso represent the ldquometabolic memoryrdquo [72] Engagement oftheir receptor RAGE with AGEs is shown to activate itsdownstream signaling and evoke OS and inflammation indiabetes [73] AGEs have been found to induce OS andconversely OS stimulates AGEs formation [74ndash76]
AGEs deposition in ovary dysregulate ovarian functionthrough the induction of androgen production as well as OSgeneration through the induction ofNF-K120573pathway leadingto increased production of atherogenic and inflammatorymolecules AGEs have been implicated in the developmentof insulin resistance hyperandrogenism and anovulationin polycystic ovary syndrome (PCOS) and seem to have acentral role in PCOS pathophysiology either as a marker ofOS or through their specific actions after their ligation totheir specific receptor RAGE [77] Furthermore there is sub-stantial evidence that insulin resistance constitutes one of themain pathophysiological mechanisms leading to anovulationand ovarian hyperandrogenism in PCOS patients Regardingthe above also that iron has been implicated in abnormalinsulin secretion in patients with BTM or hemochromatosis[44 78] and that OS might be responsible for a decline ininsulin-mediated glucose uptake in BTM patients leadingto insulin resistance [79] we consider that the evaluationof AGEs as markers of OS in relation to iron overloadinsulin resistance and ovulation potential would be of greatvalue Reducing AGEs in BTM females could probably havebeneficial effects in insulin resistance and ovulation potentialand thus in fertility potential Finally it is remarkable thatthe iron chelator Desferal had a retardation effect on thefunctional and structural changes of Hb during fructation[80] It could prevent the AGEs and carbonyl formations andhelix depletion during theHb fructation processMoreover itcould preserve peroxidase and esterase activities of fructated
Anemia 7
Hb similar to native Hb Therefore desferal could be intro-duced as an antiglycation drug to prevent theAGEs formation[80]
6 Conclusions
On the basis of all the presented data it can be concludedthatOS plays amajor role in the pathophysiology of infertilityin females with thalassemia This OS is mainly caused bytissue injury due to overproduction of free radicals bysecondary iron overload alteration in serum trace elementsand alteration in antioxidant enzymes level Consequentlythere is a rationale for iron chelation to eliminate the free-iron species which in this respect act like antioxidantsAntioxidants are also capable of ameliorating increased OSparameters and given together with iron chelators mayprovide a substantial improvement in the pathophysiologyof thalassemia [81] However there is no study evaluatingthe efficacy of antioxidant supplementation on BTMwomenrsquosfertility potential In agreement with previous suggestionswe consider that the application of treatment strategies thatwould reduceOS in the reproductive tract could help infertilewomen with diseases such as BTM that are caused byROSantioxidants imbalance [29] In general research isin progress to identify the mechanisms that are involvedin the etiology of female reproductive diseases caused byROS and to create effective strategies that can counteractOS [29] while few are the trials investigating antioxidantsupplementation in female reproduction [20] The admin-istration of selective antioxidants along with essential traceelements and minerals to reduce the extent of oxidativedamage and related complications such as infertility in BTMpatients still needs further evaluation [24] However beforeclinicians recommend antioxidants randomized controlledtrials with sufficient power are necessary to prove the efficacyof antioxidant therapeutic strategies in disorders of femalereproduction [20] such as BTMThis is strongly emerged bythe fact of prolonged survival and the newly recognized issuesand challenges that adults with BTM face [82]
References
[1] C Hershko ldquoPathogenesis and management of iron toxicity inthalassemiardquo Annals of the New York Academy of Sciences vol1202 pp 1ndash9 2010
[2] F Waseem K A Khemomal and R Sajid ldquoAntioxidant statusin beta thalassemia major a single-center studyrdquo Indian Journalof Pathology and Microbiology vol 54 no 4 pp 761ndash763 2011
[3] R Origa A Piga G Quarta et al ldquoPregnancy and 120573-thalassemia an Italian multicenter experiencerdquoHaematologicavol 95 no 3 pp 376ndash381 2010
[4] N Skordis L Petrikkos M Toumba et al ldquoUpdate on fertilityin thalassaemia majorrdquo Pediatric Endocrinology Reviews vol 2supplement 2 pp 296ndash302 2004
[5] M Toumba A Sergis C Kanaris and N Skordis ldquoEndocrinecomplications in patients with thalassaemia majorrdquo PediatricEndocrinology Reviews vol 5 no 2 pp 642ndash648 2007
[6] E A Rachmilewitz O Weizer-Stern K Adamsky et al ldquoRoleof iron in inducing oxidative stress in thalassemia can it be
prevented by inhibition of absorption and by antioxidantsrdquoAnnals of the New York Academy of Sciences vol 1054 pp 118ndash123 2005
[7] S Ansari A Azarkeivan and A Tabaroki ldquoPregnancy inpatients treated for beta thalassemia major in two centers(Ali Asghar Childrenrsquos Hospital and Thalassemia Clinic) out-come for mothers and newborn infantsrdquo Pediatric Hematology-Oncology vol 23 no 1 pp 33ndash37 2006
[8] M R Safarinejad ldquoReproductive hormones and hypothalamic-pituitary-ovarian axis in female patients with homozygous 120573-thalassemia majorrdquo Journal of Pediatric HematologyOncologyvol 32 no 4 pp 259ndash266 2010
[9] S T Singer E P Vichinsky G Gildengorin J van DisseldorpM Rosen and M I Cedars ldquoReproductive capacity in ironoverloaded women with thalassemia majorrdquo Blood vol 118 no10 pp 2878ndash2881 2011
[10] G Vizziello D Carone E Caroppo A Vitti A Pasquad-ibisceglie and G Drsquoamato ldquoOvulation induction with gona-dotropin in patients with thalassemia pretreated with pulsatileGnRH outcomerdquoMinerva Ginecologica vol 56 no 5 pp 485ndash487 2004
[11] N Skordis S Christou M Koliou N Pavlides and M Angas-tiniotis ldquoFertility in female patients with thalassemiardquo Journalof Pediatric Endocrinology and Metabolism vol 11 supplement3 pp 935ndash943 1998
[12] LDanesiM Scacchi AMMiragoli et al ldquoInduction of folliclematuration and ovulation by gonadotropin administration inwomen with 120573-thalassemiardquo European Journal of Endocrinol-ogy vol 131 no 6 pp 602ndash606 1994
[13] R Bajoria and R Chatterjee ldquoCurrent perspectives of fertilityand pregnancy in thalassemiardquoHemoglobin vol 33 supplement1 pp S131ndashS135 2009
[14] R Bajoria and R Chatterjee ldquoHypogonadotrophic hypogo-nadism and diminished gonadal reserve accounts for dys-functional gametogenesis in thalassaemia patients with ironoverload presenting with infertilityrdquoHemoglobin vol 35 no 5-6 pp 636ndash642 2011
[15] M Karagiorga-Lagana ldquoFertility in thalassemia the Greekexperiencerdquo Journal of Pediatric Endocrinology andMetabolismvol 11 supplement 3 pp 945ndash951 1998
[16] S M Tuck ldquoFertility and pregnancy in thalassemia majorrdquoAnnals of the New York Academy of Sciences vol 1054 pp 300ndash307 2005
[17] D Surbek A Koller and N Pavic ldquoSuccessful twin pregnancyin homozygous 120573-thalassemia after ovulation induction withgrowth hormone and gonadotropinsrdquo Fertility and Sterility vol65 no 3 pp 670ndash672 1996
[18] K Yamaguchi M Mandai S Toyokuni et al ldquoContents ofendometriotic cysts especially the high concentration of freeiron are a possible cause of carcinogenesis in the cysts throughthe iron-induced persistent oxidative stressrdquo Clinical CancerResearch vol 14 no 1 pp 32ndash40 2008
[19] M C Kew ldquoHepatic iron overload and hepatocellular carci-nomardquo Cancer Letters vol 286 no 1 pp 38ndash43 2009
[20] AAgarwal S Gupta andRK Sharma ldquoRole of oxidative stressin female reproductionrdquo Reproductive Biology and Endocrinol-ogy vol 3 article 28 2005
[21] A C Chan C K Chow and D Chiu ldquoInteraction of antiox-idants and their implication in genetic anemiardquo Proceedings ofthe Society for Experimental Biology and Medicine vol 222 no3 pp 274ndash282 1999
8 Anemia
[22] A Agarwal A Aponte-Mellado B J Premkumar A Shamanand S Gupta ldquoThe effects of oxidative stress on female repro-duction a reviewrdquo Reproductive Biology and Endocrinology vol10 article 49 2012
[23] M Giergiel M Lopucki N Stachowicz and M KankoferldquoThe influence of age and gender on antioxidant enzymeactivities in humans and laboratory animalsrdquoAging Clinical andExperimental Research vol 24 pp 551ndash559 2012
[24] Q Shazia Z H Mohammad T Rahman and H U ShekharldquoCorrelation of oxidative stress with serum trace element levelsand antioxidant enzyme status in Beta thalassemia majorpatients a review of the literaturerdquo Anemia vol 2012 ArticleID 270923 7 pages 2012
[25] M Y Abdalla M Fawzi S R Al-Maloul N El-Banna R FTayyem and I M Ahmad ldquoIncreased oxidative stress and ironoverload in Jordanian120573-thalassemic childrenrdquoHemoglobin vol35 no 1 pp 67ndash79 2011
[26] R A Ghone K M Kumbar A N Suryakar R V Katkam andN G Joshi ldquoOxidative stress and disturbance in antioxidantbalance in beta thalassemia majorrdquo Indian Journal of ClinicalBiochemistry vol 23 no 4 pp 337ndash340 2008
[27] MA Livrea L Tesoriere AM Pintaudi et al ldquoOxidative stressand antioxidant status in 120573-thalassemia major iron overloadand depletion of lipid-soluble antioxidantsrdquo Blood vol 88 no9 pp 3608ndash3614 1996
[28] S-S Chiou T-T Chang S-P Tsai et al ldquoLipid peroxidationand antioxidative status in 120573-thalassemia major patients withor without hepatitis C virus infectionrdquo Clinical Chemistry andLaboratory Medicine vol 44 no 10 pp 1226ndash1233 2006
[29] A Agarwal and S S Allamaneni ldquoRole of free radicals in femalereproductive diseases and assisted reproductionrdquo ReproductiveBioMedicine Online vol 9 no 3 pp 338ndash347 2004
[30] E H Ruder T J Hartman J Blumberg and M B GoldmanldquoOxidative stress and antioxidants exposure and impact onfemale fertilityrdquoHuman Reproduction Update vol 14 no 4 pp345ndash357 2008
[31] A Agarwal S Gupta L Sekhon and R Shah ldquoRedox con-siderations in female reproductive function and assisted repro-duction from molecular mechanisms to health implicationsrdquoAntioxidants amp Redox Signaling vol 10 no 8 pp 1375ndash14032008
[32] P J Devine S D Perreault and U Luderer ldquoRoles of reactiveoxygen species and antioxidants in ovarian toxicityrdquo Biology ofReproduction vol 86 no 2 article 27 2012
[33] K H Al-Gubory C Garrel P Faure and N Sugino ldquoRolesof antioxidant enzymes in corpus luteum rescue from reac-tive oxygen species-induced oxidative stressrdquo ReproductiveBiomedicine Online vol 25 no 6 pp 551ndash560 2012
[34] A Agarwal A Aponte-Mellado B J Premkumar A Shamanand S Gupta ldquoThe effects of oxidative stress on female repro-duction a reviewrdquo Reproductive Biology and Endocrinology vol10 article 49 2012
[35] S Defrere R Gonzalez-Ramos J-C Lousse et al ldquoInsightsinto iron and nuclear factor-kappa B (NF-120581B) involvement inchronic inflammatory processes in peritoneal endometriosisrdquoHistology and Histopathology vol 26 no 8 pp 1083ndash1092 2011
[36] A van Langendonckt F Casanas-Roux and J Donnez ldquoOxida-tive stress and peritoneal endometriosisrdquo Fertility and Sterilityvol 77 no 5 pp 861ndash870 2002
[37] M Appasamy E Jauniaux P Serhal A Al-Qahtani N PGroome and S Muttukrishna ldquoEvaluation of the relationshipbetween follicular fluid oxidative stress ovarian hormones and
response to gonadotropin stimulationrdquo Fertility and Sterilityvol 89 no 4 pp 912ndash921 2008
[38] Y Asano ldquoAge-related accumulation of non-heme ferric andferrous iron in mouse ovarian stroma visualized by sensitivenon-heme iron histochemistryrdquo The Journal of Histochemistryamp Cytochemistry vol 60 no 3 pp 229ndash242 2012
[39] M K Al-Azemi A E Omu T Fatinikun N Mannazhathand S Abraham ldquoFactors contributing to gender differences inserum retinol and 120572-tocopherol in infertile couplesrdquo Reproduc-tive BioMedicine Online vol 19 no 4 pp 583ndash590 2009
[40] M K Kim J W Lee K H Baek et al ldquoEndocrinopathies intransfusion-associated iron overloadrdquo Clinical Endocrinologyvol 78 no 2 pp 271ndash277 2013
[41] L M Hempenius P S van Dam J J Marx and H PKoppeschaar ldquoMineralocorticoid status and endocrine dys-function in severe hemochromatosisrdquo Journal of Endocrinolog-ical Investigation vol 22 no 5 pp 369ndash376 1999
[42] J M Vasquez and R B Greenblatt ldquoPituitary responsiveness toluteinizing-hormone-releasing hormone in different reproduc-tive disorders a reviewrdquo Journal of ReproductiveMedicine for theObstetrician and Gynecologist vol 30 no 8 pp 591ndash600 1985
[43] I Paris M Hermans and M Buysschaert ldquoEndocrine compli-cations of genetic hemochromatosisrdquo Acta Clinica Belgica vol54 no 6 pp 334ndash345 1999
[44] W Stremmel C Niederau M Berger H-K Kley H-LKruskemper and G Strohmeyer ldquoAbnormalities in estrogenandrogen and insulin metabolism in idiopathic hemochro-matosisrdquo Annals of the New York Academy of Sciences vol 526pp 209ndash223 1988
[45] W R Meyer K A Hutchinson-Williams E E Jones and A HDecherney ldquoSecondary hypogonadism in hemochromatosisrdquoFertility and Sterility vol 54 no 4 pp 740ndash742 1990
[46] L J Siemons and C H Mahler ldquoHypogonadotropic hypogo-nadism in hemochromatosis recovery of reproductive functionafter iron depletionrdquo The Journal of Clinical Endocrinology andMetabolism vol 65 no 3 pp 585ndash587 1987
[47] J H McDermott and C H Walsh ldquoHypogonadism in hered-itary hemochromatosisrdquo The Journal of Clinical Endocrinologyand Metabolism vol 90 no 4 pp 2451ndash2455 2005
[48] G Kontogeorgos S Handy K Kovacs E Horvath and BW Scheithauer ldquoThe anterior pituitary in hemochromatosisrdquoEndocrine Pathology vol 7 no 2 pp 159ndash164 1996
[49] A Piperno M R Rivolta R Drsquoalba et al ldquoPreclinical hypog-onadism in genetic hemochromatosis in the early stage ofthe disease evidence of hypothalamic dysfunctionrdquo Journal ofEndocrinological Investigation vol 15 no 6 pp 423ndash428 1992
[50] K SiminoskiM Drsquocosta and P GWalfish ldquoHypogonadotropichypogonadism in idiopathic hemochromatosis evidence forcombined hypothalamic and pituitary involvementrdquo Journal ofEndocrinological Investigation vol 13 no 10 pp 849ndash853 1990
[51] K E Oerter G A Kamp P J Munson A W Nienhuis F GCassorla and P K Manasco ldquoMultiple hormone deficienciesin children with hemochromatosisrdquo The Journal of ClinicalEndocrinology and Metabolism vol 76 no 2 pp 357ndash361 1993
[52] L J Noetzli A Panigrahy S D Mittelman et al ldquoPituitaryiron and volume predict hypogonadism in transfusional ironoverloadrdquo American Journal of Hematology vol 87 no 2 pp167ndash171 2012
[53] R Chatterjee and M Katz ldquoReversible hypogonadotrophichypogonadism in sexually infantile male thalassaemic patientswith transfusional iron overloadrdquo Clinical Endocrinology vol53 no 1 pp 33ndash42 2000
Anemia 9
[54] M Berkovitch T Bistritzer S D Milone K Perlman WKucharczyk and N F Olivieri ldquoIron deposition in the anteriorpituitary in homozygous beta-thalassemia MRI evaluationand correlation with gonadal functionrdquo Journal of PediatricEndocrinology amp Metabolism vol 13 no 2 pp 179ndash184 2000
[55] S Arguelles M Cano A Machado and A Ayala ldquoEffect ofaging and oxidative stress on elongation factor-2 in hypothala-mus and hypophysisrdquo Mechanisms of Ageing and Developmentvol 132 no 1-2 pp 55ndash64 2011
[56] D Gonzalez-Duarte A Madrazo-Atutxa A Soto-Moreno andA Leal-Cerro ldquoMeasurement of oxidative stress and endothe-lial dysfunction in patients with hypopituitarism and severedeficiency adult growth hormone deficiencyrdquo Pituitary vol 15no 4 pp 589ndash597 2012
[57] A Birkenfeld A W Goldfarb E A Rachmilewitz J GSchenker andEOkon ldquoEndometrial glandular haemosiderosisin homozygous beta-thalassaemiardquo European Journal of Obstet-rics Gynecology and Reproductive Biology vol 31 no 2 pp 173ndash178 1989
[58] S T Singer N Sweeters O Vega A Higa E Vichinsky andM Cedars ldquoFertility potential in thalassemia major womencurrent findings and future diagnostic toolsrdquo Annals of the NewYork Academy of Sciences vol 1202 pp 226ndash230 2010
[59] T Dissayabutra P Tosukhowong and P Seksan ldquoThe benefitsof vitamin C and vitamin E in children with beta-thalassemiawith high oxidative stressrdquo Journal of the Medical Association ofThailand vol 88 supplement 4 pp S317ndash321 2005
[60] C Weeraphan C Srisomsap D Chokchaichamnankit et alldquoRole of curcuminoids in ameliorating oxidative modificationin beta-thalassemiaHb E plasma proteomerdquo The Journal ofNutritional Biochemistry vol 24 no 3 pp 578ndash585 2012
[61] E Vichinsky ldquoEmerging ldquoArdquo therapies in hemoglobinopathiesagonists antagonists antioxidants and argininerdquo HematologyAmerican Society Hematology Education Program vol 2012 no1 pp 271ndash275 2012
[62] C Mora-Esteves and D Shin ldquoNutrient supplementationimproving male fertility fourfoldrdquo Seminars in ReproductiveMedicine vol 31 no 4 pp 293ndash300 2013
[63] G J Kontoghiorghes A Efstathiou M Kleanthous YMichaelides and A Kolnagou ldquoRiskbenefit assessmentadvantages over other drugs and targeting methods in the useof deferiprone as a pharmaceutical antioxidant in iron loadingand non iron loading conditionsrdquo Hemoglobin vol 33 no 5pp 386ndash397 2009
[64] U R Kuppusamy and J A Tan ldquoChelation therapy withdesferrioxamine does not normalize ferritin level but attenu-ates oxidative damage and improves total antioxidant level inMalaysian Chinese beta-thalassaemia major patientsrdquoTheWestIndian Medical Journal vol 60 no 1 pp 3ndash8 2011
[65] P B Walter E A Macklin J Porter et al ldquoInflammationand oxidant-stress in 120573-thalassemia patients treated with ironchelators deferasirox (ICL670) or deferoxamine an ancillarystudy of the Novartis CICL670A0107 trialrdquo Haematologica vol93 no 6 pp 817ndash825 2008
[66] V Fenkci S Fenkci M Yilmazer and M Serteser ldquoDecreasedtotal antioxidant status and increased oxidative stress in womenwith polycystic ovary syndrome may contribute to the risk ofcardiovascular diseaserdquo Fertility and Sterility vol 80 no 1 pp123ndash127 2003
[67] C Tatone M C Carbone S Falone et al ldquoAge-dependentchanges in the expression of superoxide dismutases and catalaseare associated with ultrastructural modifications in human
granulosa cellsrdquoMolecular Human Reproduction vol 12 no 11pp 655ndash660 2006
[68] F Gonzalez N S Rote J Minium and J P Kirwan ldquoReactiveoxygen species-induced oxidative stress in the developmentof insulin resistance and hyperandrogenism in polycysticovary syndromerdquo The Journal of Clinical Endocrinology andMetabolism vol 91 no 1 pp 336ndash340 2006
[69] G Basta G Lazzerini M Massaro et al ldquoAdvanced gly-cation end products activate endothelium through signal-transduction receptor RAGE a mechanism for amplification ofinflammatory responsesrdquo Circulation vol 105 no 7 pp 816ndash822 2002
[70] E Devangelio F Santilli G Formoso et al ldquoSoluble RAGE intype 2 diabetes association with oxidative stressrdquo Free RadicalBiology and Medicine vol 43 no 4 pp 511ndash518 2007
[71] G Basta A M Schmidt and R de Caterina ldquoAdvancedglycation end products and vascular inflammation implica-tions for accelerated atherosclerosis in diabetesrdquoCardiovascularResearch vol 63 no 4 pp 582ndash592 2004
[72] R Meerwaldt T Links C Zeebregts R Tio J-L Hillebrandsand A Smit ldquoThe clinical relevance of assessing advanced gly-cation endproducts accumulation in diabetesrdquo CardiovascularDiabetology vol 7 article 29 2008
[73] H Unoki and S Yamagishi ldquoAdvanced glycation end productsand insulin resistancerdquo Current Pharmaceutical Design vol 14no 10 pp 987ndash989 2008
[74] E Diamanti-Kandarakis C Piperi A Kalofoutis and GCreatsas ldquoIncreased levels of serum advanced glycation end-products in women with polycystic ovary syndromerdquo ClinicalEndocrinology vol 62 no 1 pp 37ndash43 2005
[75] D R Mccance D G Dyer J A Dunn et al ldquoMaillardreaction products and their relation to complications in insulin-dependent diabetes mellitusrdquo Journal of Clinical Investigationvol 91 no 6 pp 2470ndash2478 1993
[76] R Singh A Barden TMori and L Beilin ldquoAdvanced glycationend-products a reviewrdquoDiabetologia vol 44 no 2 pp 129ndash1462001
[77] E Diamanti-Kandarakis A Piouka S Livadas et al ldquoAnti-mullerian hormone is associated with advanced glycosylatedend products in lean women with polycystic ovary syndromerdquoEuropean Journal of Endocrinology vol 160 no 5 pp 847ndash8532009
[78] R Chatterjee and R Bajoria ldquoNew concept in natural historyand management of diabetes mellitus in thalassemia majordiabetes and thalassaemiardquo Hemoglobin vol 33 supplement 1pp S127ndashS130 2009
[79] G Paolisso M R Tagliamonte M R Rizzo and D GiuglianoldquoAdvancing age and insulin resistance new facts about anancient historyrdquo European Journal of Clinical Investigation vol29 no 9 pp 758ndash769 1999
[80] N Sattarahmady H Heli and A A Moosavi-Movahedi ldquoDes-feral as improving agent for hemoglobin fructation structuraland functional impactsrdquo The Protein Journal vol 31 no 8 pp651ndash655 2012
[81] E Fibach and E A Rachmilewitz ldquoThe role of antioxidantsand iron chelators in the treatment of oxidative stress inthalassemiardquo Annals of the New York Academy of Sciences vol1202 pp 10ndash16 2010
[82] L M Compagno ldquoCaring for adults with thalassemia in apediatric worldrdquo Annals of the New York Academy of Sciencesvol 1054 pp 266ndash272 2005
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

6 Anemia
evaluating the effect of different antioxidant supplementationin BTM-related morbidities such as infertility
51 Antioxidant Supplements Used in BTM The benefits ofvitamin C and vitamin E as antioxidant supplements inBTMchildren have been previously determined [59] Twentychildren who had laboratory confirmation of BTM at least 6months with history of packed red cell transfusion withoutiron chelation were recruited It was suggested that vitaminC plus vitamin E supplementations have benefits more thanvitamin E alone in promoting antioxidant status and mayenhance liver function as total bilirubin tends to decrease[59] Furthermore curcuminoids extracted from the spiceturmeric are known to have antioxidant and iron-chelatingproperties and have been proposed as a potential upstreamtherapy of thalassemiaWeeraphan et al have recently appliedproteomic techniques to study the protein profile and oxida-tive damage in the plasma of beta-thalassemiaHb E patientsbefore and after treatment with curcuminoids Their studyindicated the ameliorating role of curcuminoids towards OSand iron overload in the plasma proteome [60] Glutaminealpha-lipoic acid acetyl-L-carnitine and N-acetylcysteineare also recently being studied as antioxidant supplements forsickle cell disease and thalassemia [61] Finally the value ofantioxidant supplements in the elimination of iron-inducedOS and subsequent infertility issues could be speculatedby the fact that various antioxidants (such as carnitinevitamin C vitamin E selenium carotenoids glutathioneN-acetylcysteine zinc folic acid and coenzyme Q10) arevariably effective in OS-induced male-factor infertility withrespect to improving semen parameters and pregnancy rates[62]
52 Chelation Treatments as Antioxidants in BTM Differentstudies have also focused on the antioxidant capacity of differ-ent chelation treatment modalities Increased evidence fromin vitro in vivo and clinical studies suggest that deferiprone(L1) can be used as a potent pharmaceutical antioxidant bymobilizing labile iron and copper andor inhibiting theircatalytic activity in the formation of free radicals and OS intissue damage [63] In contrast to L1 both desferrioxamine(DFO) and deferasirox (DFRA) were suggested to havemajordisadvantages in their use in noniron loading conditionsdue to toxicity implications [63] Meanwhile a subsequentstudy indicated that DFO chelation therapy does not nor-malize ferritin levels but attenuates oxidative damage andimproves total antioxidant level in Malaysian Chinese BTMpatients [64] The objective of this research was to studythe oxidant-antioxidant indices in BTM patients who wereon desferrioxamine-chelation or without chelation therapyBlood was collected from 39 Chinese patients and 20 con-trols Plasma and peripheral blood mononuclear cell lysates(PBMC) were extracted and biochemical tests to evaluate OSwere performedOSwas evident in these patients as advancedoxidized protein products (AOPP) and lipid hydroperoxideswere elevated whereas glutathione peroxidase activity andthe ferric reducing antioxidant power (FRAP) were reducedThe catalase activity in the patientsrsquo PBMC was elevated
possibly as a compensatory mechanism for the reducedglutathione peroxidase activity in both red blood cells andPBMC The lower FRAP and higher AOPP levels in thenonchelated patients compared with the chelated patientswere indicative of a lower OS level in the chelated patients[64] An additional study which assessed whether oxidant-stress and inflammation in BTM could be controlled byDFRA as effectively as by DFO revealed equal effectivenessin decreasing iron burden and levels of the oxidative-stressmarker MDA [65]
53 The Possible Effect of Advanced Glycation End Products(AGEs) Regulation on BTM Womenrsquos Ovarian Function andFertility Recent data have shown that OS is involved in thepathophysiology of anovulation [20 66 67] While the roleof OS in ovulatory dysfunction has been sufficiently studied[29 68] advanced glycation end products (AGEs) have beenrecognized as mediators of increased OS [69 70] Advancedglycation end products (AGEs) are a heterogeneous group ofbioactive molecules formed by the nonenzymatic glycationof proteins lipids and nucleic acids [71] There is increasingevidence that AGEs play a pivotal role in atherosclerosis andin diabetes and its complications while AGE accumulationis a measure of cumulative metabolic and OS and mayso represent the ldquometabolic memoryrdquo [72] Engagement oftheir receptor RAGE with AGEs is shown to activate itsdownstream signaling and evoke OS and inflammation indiabetes [73] AGEs have been found to induce OS andconversely OS stimulates AGEs formation [74ndash76]
AGEs deposition in ovary dysregulate ovarian functionthrough the induction of androgen production as well as OSgeneration through the induction ofNF-K120573pathway leadingto increased production of atherogenic and inflammatorymolecules AGEs have been implicated in the developmentof insulin resistance hyperandrogenism and anovulationin polycystic ovary syndrome (PCOS) and seem to have acentral role in PCOS pathophysiology either as a marker ofOS or through their specific actions after their ligation totheir specific receptor RAGE [77] Furthermore there is sub-stantial evidence that insulin resistance constitutes one of themain pathophysiological mechanisms leading to anovulationand ovarian hyperandrogenism in PCOS patients Regardingthe above also that iron has been implicated in abnormalinsulin secretion in patients with BTM or hemochromatosis[44 78] and that OS might be responsible for a decline ininsulin-mediated glucose uptake in BTM patients leadingto insulin resistance [79] we consider that the evaluationof AGEs as markers of OS in relation to iron overloadinsulin resistance and ovulation potential would be of greatvalue Reducing AGEs in BTM females could probably havebeneficial effects in insulin resistance and ovulation potentialand thus in fertility potential Finally it is remarkable thatthe iron chelator Desferal had a retardation effect on thefunctional and structural changes of Hb during fructation[80] It could prevent the AGEs and carbonyl formations andhelix depletion during theHb fructation processMoreover itcould preserve peroxidase and esterase activities of fructated
Anemia 7
Hb similar to native Hb Therefore desferal could be intro-duced as an antiglycation drug to prevent theAGEs formation[80]
6 Conclusions
On the basis of all the presented data it can be concludedthatOS plays amajor role in the pathophysiology of infertilityin females with thalassemia This OS is mainly caused bytissue injury due to overproduction of free radicals bysecondary iron overload alteration in serum trace elementsand alteration in antioxidant enzymes level Consequentlythere is a rationale for iron chelation to eliminate the free-iron species which in this respect act like antioxidantsAntioxidants are also capable of ameliorating increased OSparameters and given together with iron chelators mayprovide a substantial improvement in the pathophysiologyof thalassemia [81] However there is no study evaluatingthe efficacy of antioxidant supplementation on BTMwomenrsquosfertility potential In agreement with previous suggestionswe consider that the application of treatment strategies thatwould reduceOS in the reproductive tract could help infertilewomen with diseases such as BTM that are caused byROSantioxidants imbalance [29] In general research isin progress to identify the mechanisms that are involvedin the etiology of female reproductive diseases caused byROS and to create effective strategies that can counteractOS [29] while few are the trials investigating antioxidantsupplementation in female reproduction [20] The admin-istration of selective antioxidants along with essential traceelements and minerals to reduce the extent of oxidativedamage and related complications such as infertility in BTMpatients still needs further evaluation [24] However beforeclinicians recommend antioxidants randomized controlledtrials with sufficient power are necessary to prove the efficacyof antioxidant therapeutic strategies in disorders of femalereproduction [20] such as BTMThis is strongly emerged bythe fact of prolonged survival and the newly recognized issuesand challenges that adults with BTM face [82]
References
[1] C Hershko ldquoPathogenesis and management of iron toxicity inthalassemiardquo Annals of the New York Academy of Sciences vol1202 pp 1ndash9 2010
[2] F Waseem K A Khemomal and R Sajid ldquoAntioxidant statusin beta thalassemia major a single-center studyrdquo Indian Journalof Pathology and Microbiology vol 54 no 4 pp 761ndash763 2011
[3] R Origa A Piga G Quarta et al ldquoPregnancy and 120573-thalassemia an Italian multicenter experiencerdquoHaematologicavol 95 no 3 pp 376ndash381 2010
[4] N Skordis L Petrikkos M Toumba et al ldquoUpdate on fertilityin thalassaemia majorrdquo Pediatric Endocrinology Reviews vol 2supplement 2 pp 296ndash302 2004
[5] M Toumba A Sergis C Kanaris and N Skordis ldquoEndocrinecomplications in patients with thalassaemia majorrdquo PediatricEndocrinology Reviews vol 5 no 2 pp 642ndash648 2007
[6] E A Rachmilewitz O Weizer-Stern K Adamsky et al ldquoRoleof iron in inducing oxidative stress in thalassemia can it be
prevented by inhibition of absorption and by antioxidantsrdquoAnnals of the New York Academy of Sciences vol 1054 pp 118ndash123 2005
[7] S Ansari A Azarkeivan and A Tabaroki ldquoPregnancy inpatients treated for beta thalassemia major in two centers(Ali Asghar Childrenrsquos Hospital and Thalassemia Clinic) out-come for mothers and newborn infantsrdquo Pediatric Hematology-Oncology vol 23 no 1 pp 33ndash37 2006
[8] M R Safarinejad ldquoReproductive hormones and hypothalamic-pituitary-ovarian axis in female patients with homozygous 120573-thalassemia majorrdquo Journal of Pediatric HematologyOncologyvol 32 no 4 pp 259ndash266 2010
[9] S T Singer E P Vichinsky G Gildengorin J van DisseldorpM Rosen and M I Cedars ldquoReproductive capacity in ironoverloaded women with thalassemia majorrdquo Blood vol 118 no10 pp 2878ndash2881 2011
[10] G Vizziello D Carone E Caroppo A Vitti A Pasquad-ibisceglie and G Drsquoamato ldquoOvulation induction with gona-dotropin in patients with thalassemia pretreated with pulsatileGnRH outcomerdquoMinerva Ginecologica vol 56 no 5 pp 485ndash487 2004
[11] N Skordis S Christou M Koliou N Pavlides and M Angas-tiniotis ldquoFertility in female patients with thalassemiardquo Journalof Pediatric Endocrinology and Metabolism vol 11 supplement3 pp 935ndash943 1998
[12] LDanesiM Scacchi AMMiragoli et al ldquoInduction of folliclematuration and ovulation by gonadotropin administration inwomen with 120573-thalassemiardquo European Journal of Endocrinol-ogy vol 131 no 6 pp 602ndash606 1994
[13] R Bajoria and R Chatterjee ldquoCurrent perspectives of fertilityand pregnancy in thalassemiardquoHemoglobin vol 33 supplement1 pp S131ndashS135 2009
[14] R Bajoria and R Chatterjee ldquoHypogonadotrophic hypogo-nadism and diminished gonadal reserve accounts for dys-functional gametogenesis in thalassaemia patients with ironoverload presenting with infertilityrdquoHemoglobin vol 35 no 5-6 pp 636ndash642 2011
[15] M Karagiorga-Lagana ldquoFertility in thalassemia the Greekexperiencerdquo Journal of Pediatric Endocrinology andMetabolismvol 11 supplement 3 pp 945ndash951 1998
[16] S M Tuck ldquoFertility and pregnancy in thalassemia majorrdquoAnnals of the New York Academy of Sciences vol 1054 pp 300ndash307 2005
[17] D Surbek A Koller and N Pavic ldquoSuccessful twin pregnancyin homozygous 120573-thalassemia after ovulation induction withgrowth hormone and gonadotropinsrdquo Fertility and Sterility vol65 no 3 pp 670ndash672 1996
[18] K Yamaguchi M Mandai S Toyokuni et al ldquoContents ofendometriotic cysts especially the high concentration of freeiron are a possible cause of carcinogenesis in the cysts throughthe iron-induced persistent oxidative stressrdquo Clinical CancerResearch vol 14 no 1 pp 32ndash40 2008
[19] M C Kew ldquoHepatic iron overload and hepatocellular carci-nomardquo Cancer Letters vol 286 no 1 pp 38ndash43 2009
[20] AAgarwal S Gupta andRK Sharma ldquoRole of oxidative stressin female reproductionrdquo Reproductive Biology and Endocrinol-ogy vol 3 article 28 2005
[21] A C Chan C K Chow and D Chiu ldquoInteraction of antiox-idants and their implication in genetic anemiardquo Proceedings ofthe Society for Experimental Biology and Medicine vol 222 no3 pp 274ndash282 1999
8 Anemia
[22] A Agarwal A Aponte-Mellado B J Premkumar A Shamanand S Gupta ldquoThe effects of oxidative stress on female repro-duction a reviewrdquo Reproductive Biology and Endocrinology vol10 article 49 2012
[23] M Giergiel M Lopucki N Stachowicz and M KankoferldquoThe influence of age and gender on antioxidant enzymeactivities in humans and laboratory animalsrdquoAging Clinical andExperimental Research vol 24 pp 551ndash559 2012
[24] Q Shazia Z H Mohammad T Rahman and H U ShekharldquoCorrelation of oxidative stress with serum trace element levelsand antioxidant enzyme status in Beta thalassemia majorpatients a review of the literaturerdquo Anemia vol 2012 ArticleID 270923 7 pages 2012
[25] M Y Abdalla M Fawzi S R Al-Maloul N El-Banna R FTayyem and I M Ahmad ldquoIncreased oxidative stress and ironoverload in Jordanian120573-thalassemic childrenrdquoHemoglobin vol35 no 1 pp 67ndash79 2011
[26] R A Ghone K M Kumbar A N Suryakar R V Katkam andN G Joshi ldquoOxidative stress and disturbance in antioxidantbalance in beta thalassemia majorrdquo Indian Journal of ClinicalBiochemistry vol 23 no 4 pp 337ndash340 2008
[27] MA Livrea L Tesoriere AM Pintaudi et al ldquoOxidative stressand antioxidant status in 120573-thalassemia major iron overloadand depletion of lipid-soluble antioxidantsrdquo Blood vol 88 no9 pp 3608ndash3614 1996
[28] S-S Chiou T-T Chang S-P Tsai et al ldquoLipid peroxidationand antioxidative status in 120573-thalassemia major patients withor without hepatitis C virus infectionrdquo Clinical Chemistry andLaboratory Medicine vol 44 no 10 pp 1226ndash1233 2006
[29] A Agarwal and S S Allamaneni ldquoRole of free radicals in femalereproductive diseases and assisted reproductionrdquo ReproductiveBioMedicine Online vol 9 no 3 pp 338ndash347 2004
[30] E H Ruder T J Hartman J Blumberg and M B GoldmanldquoOxidative stress and antioxidants exposure and impact onfemale fertilityrdquoHuman Reproduction Update vol 14 no 4 pp345ndash357 2008
[31] A Agarwal S Gupta L Sekhon and R Shah ldquoRedox con-siderations in female reproductive function and assisted repro-duction from molecular mechanisms to health implicationsrdquoAntioxidants amp Redox Signaling vol 10 no 8 pp 1375ndash14032008
[32] P J Devine S D Perreault and U Luderer ldquoRoles of reactiveoxygen species and antioxidants in ovarian toxicityrdquo Biology ofReproduction vol 86 no 2 article 27 2012
[33] K H Al-Gubory C Garrel P Faure and N Sugino ldquoRolesof antioxidant enzymes in corpus luteum rescue from reac-tive oxygen species-induced oxidative stressrdquo ReproductiveBiomedicine Online vol 25 no 6 pp 551ndash560 2012
[34] A Agarwal A Aponte-Mellado B J Premkumar A Shamanand S Gupta ldquoThe effects of oxidative stress on female repro-duction a reviewrdquo Reproductive Biology and Endocrinology vol10 article 49 2012
[35] S Defrere R Gonzalez-Ramos J-C Lousse et al ldquoInsightsinto iron and nuclear factor-kappa B (NF-120581B) involvement inchronic inflammatory processes in peritoneal endometriosisrdquoHistology and Histopathology vol 26 no 8 pp 1083ndash1092 2011
[36] A van Langendonckt F Casanas-Roux and J Donnez ldquoOxida-tive stress and peritoneal endometriosisrdquo Fertility and Sterilityvol 77 no 5 pp 861ndash870 2002
[37] M Appasamy E Jauniaux P Serhal A Al-Qahtani N PGroome and S Muttukrishna ldquoEvaluation of the relationshipbetween follicular fluid oxidative stress ovarian hormones and
response to gonadotropin stimulationrdquo Fertility and Sterilityvol 89 no 4 pp 912ndash921 2008
[38] Y Asano ldquoAge-related accumulation of non-heme ferric andferrous iron in mouse ovarian stroma visualized by sensitivenon-heme iron histochemistryrdquo The Journal of Histochemistryamp Cytochemistry vol 60 no 3 pp 229ndash242 2012
[39] M K Al-Azemi A E Omu T Fatinikun N Mannazhathand S Abraham ldquoFactors contributing to gender differences inserum retinol and 120572-tocopherol in infertile couplesrdquo Reproduc-tive BioMedicine Online vol 19 no 4 pp 583ndash590 2009
[40] M K Kim J W Lee K H Baek et al ldquoEndocrinopathies intransfusion-associated iron overloadrdquo Clinical Endocrinologyvol 78 no 2 pp 271ndash277 2013
[41] L M Hempenius P S van Dam J J Marx and H PKoppeschaar ldquoMineralocorticoid status and endocrine dys-function in severe hemochromatosisrdquo Journal of Endocrinolog-ical Investigation vol 22 no 5 pp 369ndash376 1999
[42] J M Vasquez and R B Greenblatt ldquoPituitary responsiveness toluteinizing-hormone-releasing hormone in different reproduc-tive disorders a reviewrdquo Journal of ReproductiveMedicine for theObstetrician and Gynecologist vol 30 no 8 pp 591ndash600 1985
[43] I Paris M Hermans and M Buysschaert ldquoEndocrine compli-cations of genetic hemochromatosisrdquo Acta Clinica Belgica vol54 no 6 pp 334ndash345 1999
[44] W Stremmel C Niederau M Berger H-K Kley H-LKruskemper and G Strohmeyer ldquoAbnormalities in estrogenandrogen and insulin metabolism in idiopathic hemochro-matosisrdquo Annals of the New York Academy of Sciences vol 526pp 209ndash223 1988
[45] W R Meyer K A Hutchinson-Williams E E Jones and A HDecherney ldquoSecondary hypogonadism in hemochromatosisrdquoFertility and Sterility vol 54 no 4 pp 740ndash742 1990
[46] L J Siemons and C H Mahler ldquoHypogonadotropic hypogo-nadism in hemochromatosis recovery of reproductive functionafter iron depletionrdquo The Journal of Clinical Endocrinology andMetabolism vol 65 no 3 pp 585ndash587 1987
[47] J H McDermott and C H Walsh ldquoHypogonadism in hered-itary hemochromatosisrdquo The Journal of Clinical Endocrinologyand Metabolism vol 90 no 4 pp 2451ndash2455 2005
[48] G Kontogeorgos S Handy K Kovacs E Horvath and BW Scheithauer ldquoThe anterior pituitary in hemochromatosisrdquoEndocrine Pathology vol 7 no 2 pp 159ndash164 1996
[49] A Piperno M R Rivolta R Drsquoalba et al ldquoPreclinical hypog-onadism in genetic hemochromatosis in the early stage ofthe disease evidence of hypothalamic dysfunctionrdquo Journal ofEndocrinological Investigation vol 15 no 6 pp 423ndash428 1992
[50] K SiminoskiM Drsquocosta and P GWalfish ldquoHypogonadotropichypogonadism in idiopathic hemochromatosis evidence forcombined hypothalamic and pituitary involvementrdquo Journal ofEndocrinological Investigation vol 13 no 10 pp 849ndash853 1990
[51] K E Oerter G A Kamp P J Munson A W Nienhuis F GCassorla and P K Manasco ldquoMultiple hormone deficienciesin children with hemochromatosisrdquo The Journal of ClinicalEndocrinology and Metabolism vol 76 no 2 pp 357ndash361 1993
[52] L J Noetzli A Panigrahy S D Mittelman et al ldquoPituitaryiron and volume predict hypogonadism in transfusional ironoverloadrdquo American Journal of Hematology vol 87 no 2 pp167ndash171 2012
[53] R Chatterjee and M Katz ldquoReversible hypogonadotrophichypogonadism in sexually infantile male thalassaemic patientswith transfusional iron overloadrdquo Clinical Endocrinology vol53 no 1 pp 33ndash42 2000
Anemia 9
[54] M Berkovitch T Bistritzer S D Milone K Perlman WKucharczyk and N F Olivieri ldquoIron deposition in the anteriorpituitary in homozygous beta-thalassemia MRI evaluationand correlation with gonadal functionrdquo Journal of PediatricEndocrinology amp Metabolism vol 13 no 2 pp 179ndash184 2000
[55] S Arguelles M Cano A Machado and A Ayala ldquoEffect ofaging and oxidative stress on elongation factor-2 in hypothala-mus and hypophysisrdquo Mechanisms of Ageing and Developmentvol 132 no 1-2 pp 55ndash64 2011
[56] D Gonzalez-Duarte A Madrazo-Atutxa A Soto-Moreno andA Leal-Cerro ldquoMeasurement of oxidative stress and endothe-lial dysfunction in patients with hypopituitarism and severedeficiency adult growth hormone deficiencyrdquo Pituitary vol 15no 4 pp 589ndash597 2012
[57] A Birkenfeld A W Goldfarb E A Rachmilewitz J GSchenker andEOkon ldquoEndometrial glandular haemosiderosisin homozygous beta-thalassaemiardquo European Journal of Obstet-rics Gynecology and Reproductive Biology vol 31 no 2 pp 173ndash178 1989
[58] S T Singer N Sweeters O Vega A Higa E Vichinsky andM Cedars ldquoFertility potential in thalassemia major womencurrent findings and future diagnostic toolsrdquo Annals of the NewYork Academy of Sciences vol 1202 pp 226ndash230 2010
[59] T Dissayabutra P Tosukhowong and P Seksan ldquoThe benefitsof vitamin C and vitamin E in children with beta-thalassemiawith high oxidative stressrdquo Journal of the Medical Association ofThailand vol 88 supplement 4 pp S317ndash321 2005
[60] C Weeraphan C Srisomsap D Chokchaichamnankit et alldquoRole of curcuminoids in ameliorating oxidative modificationin beta-thalassemiaHb E plasma proteomerdquo The Journal ofNutritional Biochemistry vol 24 no 3 pp 578ndash585 2012
[61] E Vichinsky ldquoEmerging ldquoArdquo therapies in hemoglobinopathiesagonists antagonists antioxidants and argininerdquo HematologyAmerican Society Hematology Education Program vol 2012 no1 pp 271ndash275 2012
[62] C Mora-Esteves and D Shin ldquoNutrient supplementationimproving male fertility fourfoldrdquo Seminars in ReproductiveMedicine vol 31 no 4 pp 293ndash300 2013
[63] G J Kontoghiorghes A Efstathiou M Kleanthous YMichaelides and A Kolnagou ldquoRiskbenefit assessmentadvantages over other drugs and targeting methods in the useof deferiprone as a pharmaceutical antioxidant in iron loadingand non iron loading conditionsrdquo Hemoglobin vol 33 no 5pp 386ndash397 2009
[64] U R Kuppusamy and J A Tan ldquoChelation therapy withdesferrioxamine does not normalize ferritin level but attenu-ates oxidative damage and improves total antioxidant level inMalaysian Chinese beta-thalassaemia major patientsrdquoTheWestIndian Medical Journal vol 60 no 1 pp 3ndash8 2011
[65] P B Walter E A Macklin J Porter et al ldquoInflammationand oxidant-stress in 120573-thalassemia patients treated with ironchelators deferasirox (ICL670) or deferoxamine an ancillarystudy of the Novartis CICL670A0107 trialrdquo Haematologica vol93 no 6 pp 817ndash825 2008
[66] V Fenkci S Fenkci M Yilmazer and M Serteser ldquoDecreasedtotal antioxidant status and increased oxidative stress in womenwith polycystic ovary syndrome may contribute to the risk ofcardiovascular diseaserdquo Fertility and Sterility vol 80 no 1 pp123ndash127 2003
[67] C Tatone M C Carbone S Falone et al ldquoAge-dependentchanges in the expression of superoxide dismutases and catalaseare associated with ultrastructural modifications in human
granulosa cellsrdquoMolecular Human Reproduction vol 12 no 11pp 655ndash660 2006
[68] F Gonzalez N S Rote J Minium and J P Kirwan ldquoReactiveoxygen species-induced oxidative stress in the developmentof insulin resistance and hyperandrogenism in polycysticovary syndromerdquo The Journal of Clinical Endocrinology andMetabolism vol 91 no 1 pp 336ndash340 2006
[69] G Basta G Lazzerini M Massaro et al ldquoAdvanced gly-cation end products activate endothelium through signal-transduction receptor RAGE a mechanism for amplification ofinflammatory responsesrdquo Circulation vol 105 no 7 pp 816ndash822 2002
[70] E Devangelio F Santilli G Formoso et al ldquoSoluble RAGE intype 2 diabetes association with oxidative stressrdquo Free RadicalBiology and Medicine vol 43 no 4 pp 511ndash518 2007
[71] G Basta A M Schmidt and R de Caterina ldquoAdvancedglycation end products and vascular inflammation implica-tions for accelerated atherosclerosis in diabetesrdquoCardiovascularResearch vol 63 no 4 pp 582ndash592 2004
[72] R Meerwaldt T Links C Zeebregts R Tio J-L Hillebrandsand A Smit ldquoThe clinical relevance of assessing advanced gly-cation endproducts accumulation in diabetesrdquo CardiovascularDiabetology vol 7 article 29 2008
[73] H Unoki and S Yamagishi ldquoAdvanced glycation end productsand insulin resistancerdquo Current Pharmaceutical Design vol 14no 10 pp 987ndash989 2008
[74] E Diamanti-Kandarakis C Piperi A Kalofoutis and GCreatsas ldquoIncreased levels of serum advanced glycation end-products in women with polycystic ovary syndromerdquo ClinicalEndocrinology vol 62 no 1 pp 37ndash43 2005
[75] D R Mccance D G Dyer J A Dunn et al ldquoMaillardreaction products and their relation to complications in insulin-dependent diabetes mellitusrdquo Journal of Clinical Investigationvol 91 no 6 pp 2470ndash2478 1993
[76] R Singh A Barden TMori and L Beilin ldquoAdvanced glycationend-products a reviewrdquoDiabetologia vol 44 no 2 pp 129ndash1462001
[77] E Diamanti-Kandarakis A Piouka S Livadas et al ldquoAnti-mullerian hormone is associated with advanced glycosylatedend products in lean women with polycystic ovary syndromerdquoEuropean Journal of Endocrinology vol 160 no 5 pp 847ndash8532009
[78] R Chatterjee and R Bajoria ldquoNew concept in natural historyand management of diabetes mellitus in thalassemia majordiabetes and thalassaemiardquo Hemoglobin vol 33 supplement 1pp S127ndashS130 2009
[79] G Paolisso M R Tagliamonte M R Rizzo and D GiuglianoldquoAdvancing age and insulin resistance new facts about anancient historyrdquo European Journal of Clinical Investigation vol29 no 9 pp 758ndash769 1999
[80] N Sattarahmady H Heli and A A Moosavi-Movahedi ldquoDes-feral as improving agent for hemoglobin fructation structuraland functional impactsrdquo The Protein Journal vol 31 no 8 pp651ndash655 2012
[81] E Fibach and E A Rachmilewitz ldquoThe role of antioxidantsand iron chelators in the treatment of oxidative stress inthalassemiardquo Annals of the New York Academy of Sciences vol1202 pp 10ndash16 2010
[82] L M Compagno ldquoCaring for adults with thalassemia in apediatric worldrdquo Annals of the New York Academy of Sciencesvol 1054 pp 266ndash272 2005
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

Anemia 7
Hb similar to native Hb Therefore desferal could be intro-duced as an antiglycation drug to prevent theAGEs formation[80]
6 Conclusions
On the basis of all the presented data it can be concludedthatOS plays amajor role in the pathophysiology of infertilityin females with thalassemia This OS is mainly caused bytissue injury due to overproduction of free radicals bysecondary iron overload alteration in serum trace elementsand alteration in antioxidant enzymes level Consequentlythere is a rationale for iron chelation to eliminate the free-iron species which in this respect act like antioxidantsAntioxidants are also capable of ameliorating increased OSparameters and given together with iron chelators mayprovide a substantial improvement in the pathophysiologyof thalassemia [81] However there is no study evaluatingthe efficacy of antioxidant supplementation on BTMwomenrsquosfertility potential In agreement with previous suggestionswe consider that the application of treatment strategies thatwould reduceOS in the reproductive tract could help infertilewomen with diseases such as BTM that are caused byROSantioxidants imbalance [29] In general research isin progress to identify the mechanisms that are involvedin the etiology of female reproductive diseases caused byROS and to create effective strategies that can counteractOS [29] while few are the trials investigating antioxidantsupplementation in female reproduction [20] The admin-istration of selective antioxidants along with essential traceelements and minerals to reduce the extent of oxidativedamage and related complications such as infertility in BTMpatients still needs further evaluation [24] However beforeclinicians recommend antioxidants randomized controlledtrials with sufficient power are necessary to prove the efficacyof antioxidant therapeutic strategies in disorders of femalereproduction [20] such as BTMThis is strongly emerged bythe fact of prolonged survival and the newly recognized issuesand challenges that adults with BTM face [82]
References
[1] C Hershko ldquoPathogenesis and management of iron toxicity inthalassemiardquo Annals of the New York Academy of Sciences vol1202 pp 1ndash9 2010
[2] F Waseem K A Khemomal and R Sajid ldquoAntioxidant statusin beta thalassemia major a single-center studyrdquo Indian Journalof Pathology and Microbiology vol 54 no 4 pp 761ndash763 2011
[3] R Origa A Piga G Quarta et al ldquoPregnancy and 120573-thalassemia an Italian multicenter experiencerdquoHaematologicavol 95 no 3 pp 376ndash381 2010
[4] N Skordis L Petrikkos M Toumba et al ldquoUpdate on fertilityin thalassaemia majorrdquo Pediatric Endocrinology Reviews vol 2supplement 2 pp 296ndash302 2004
[5] M Toumba A Sergis C Kanaris and N Skordis ldquoEndocrinecomplications in patients with thalassaemia majorrdquo PediatricEndocrinology Reviews vol 5 no 2 pp 642ndash648 2007
[6] E A Rachmilewitz O Weizer-Stern K Adamsky et al ldquoRoleof iron in inducing oxidative stress in thalassemia can it be
prevented by inhibition of absorption and by antioxidantsrdquoAnnals of the New York Academy of Sciences vol 1054 pp 118ndash123 2005
[7] S Ansari A Azarkeivan and A Tabaroki ldquoPregnancy inpatients treated for beta thalassemia major in two centers(Ali Asghar Childrenrsquos Hospital and Thalassemia Clinic) out-come for mothers and newborn infantsrdquo Pediatric Hematology-Oncology vol 23 no 1 pp 33ndash37 2006
[8] M R Safarinejad ldquoReproductive hormones and hypothalamic-pituitary-ovarian axis in female patients with homozygous 120573-thalassemia majorrdquo Journal of Pediatric HematologyOncologyvol 32 no 4 pp 259ndash266 2010
[9] S T Singer E P Vichinsky G Gildengorin J van DisseldorpM Rosen and M I Cedars ldquoReproductive capacity in ironoverloaded women with thalassemia majorrdquo Blood vol 118 no10 pp 2878ndash2881 2011
[10] G Vizziello D Carone E Caroppo A Vitti A Pasquad-ibisceglie and G Drsquoamato ldquoOvulation induction with gona-dotropin in patients with thalassemia pretreated with pulsatileGnRH outcomerdquoMinerva Ginecologica vol 56 no 5 pp 485ndash487 2004
[11] N Skordis S Christou M Koliou N Pavlides and M Angas-tiniotis ldquoFertility in female patients with thalassemiardquo Journalof Pediatric Endocrinology and Metabolism vol 11 supplement3 pp 935ndash943 1998
[12] LDanesiM Scacchi AMMiragoli et al ldquoInduction of folliclematuration and ovulation by gonadotropin administration inwomen with 120573-thalassemiardquo European Journal of Endocrinol-ogy vol 131 no 6 pp 602ndash606 1994
[13] R Bajoria and R Chatterjee ldquoCurrent perspectives of fertilityand pregnancy in thalassemiardquoHemoglobin vol 33 supplement1 pp S131ndashS135 2009
[14] R Bajoria and R Chatterjee ldquoHypogonadotrophic hypogo-nadism and diminished gonadal reserve accounts for dys-functional gametogenesis in thalassaemia patients with ironoverload presenting with infertilityrdquoHemoglobin vol 35 no 5-6 pp 636ndash642 2011
[15] M Karagiorga-Lagana ldquoFertility in thalassemia the Greekexperiencerdquo Journal of Pediatric Endocrinology andMetabolismvol 11 supplement 3 pp 945ndash951 1998
[16] S M Tuck ldquoFertility and pregnancy in thalassemia majorrdquoAnnals of the New York Academy of Sciences vol 1054 pp 300ndash307 2005
[17] D Surbek A Koller and N Pavic ldquoSuccessful twin pregnancyin homozygous 120573-thalassemia after ovulation induction withgrowth hormone and gonadotropinsrdquo Fertility and Sterility vol65 no 3 pp 670ndash672 1996
[18] K Yamaguchi M Mandai S Toyokuni et al ldquoContents ofendometriotic cysts especially the high concentration of freeiron are a possible cause of carcinogenesis in the cysts throughthe iron-induced persistent oxidative stressrdquo Clinical CancerResearch vol 14 no 1 pp 32ndash40 2008
[19] M C Kew ldquoHepatic iron overload and hepatocellular carci-nomardquo Cancer Letters vol 286 no 1 pp 38ndash43 2009
[20] AAgarwal S Gupta andRK Sharma ldquoRole of oxidative stressin female reproductionrdquo Reproductive Biology and Endocrinol-ogy vol 3 article 28 2005
[21] A C Chan C K Chow and D Chiu ldquoInteraction of antiox-idants and their implication in genetic anemiardquo Proceedings ofthe Society for Experimental Biology and Medicine vol 222 no3 pp 274ndash282 1999
8 Anemia
[22] A Agarwal A Aponte-Mellado B J Premkumar A Shamanand S Gupta ldquoThe effects of oxidative stress on female repro-duction a reviewrdquo Reproductive Biology and Endocrinology vol10 article 49 2012
[23] M Giergiel M Lopucki N Stachowicz and M KankoferldquoThe influence of age and gender on antioxidant enzymeactivities in humans and laboratory animalsrdquoAging Clinical andExperimental Research vol 24 pp 551ndash559 2012
[24] Q Shazia Z H Mohammad T Rahman and H U ShekharldquoCorrelation of oxidative stress with serum trace element levelsand antioxidant enzyme status in Beta thalassemia majorpatients a review of the literaturerdquo Anemia vol 2012 ArticleID 270923 7 pages 2012
[25] M Y Abdalla M Fawzi S R Al-Maloul N El-Banna R FTayyem and I M Ahmad ldquoIncreased oxidative stress and ironoverload in Jordanian120573-thalassemic childrenrdquoHemoglobin vol35 no 1 pp 67ndash79 2011
[26] R A Ghone K M Kumbar A N Suryakar R V Katkam andN G Joshi ldquoOxidative stress and disturbance in antioxidantbalance in beta thalassemia majorrdquo Indian Journal of ClinicalBiochemistry vol 23 no 4 pp 337ndash340 2008
[27] MA Livrea L Tesoriere AM Pintaudi et al ldquoOxidative stressand antioxidant status in 120573-thalassemia major iron overloadand depletion of lipid-soluble antioxidantsrdquo Blood vol 88 no9 pp 3608ndash3614 1996
[28] S-S Chiou T-T Chang S-P Tsai et al ldquoLipid peroxidationand antioxidative status in 120573-thalassemia major patients withor without hepatitis C virus infectionrdquo Clinical Chemistry andLaboratory Medicine vol 44 no 10 pp 1226ndash1233 2006
[29] A Agarwal and S S Allamaneni ldquoRole of free radicals in femalereproductive diseases and assisted reproductionrdquo ReproductiveBioMedicine Online vol 9 no 3 pp 338ndash347 2004
[30] E H Ruder T J Hartman J Blumberg and M B GoldmanldquoOxidative stress and antioxidants exposure and impact onfemale fertilityrdquoHuman Reproduction Update vol 14 no 4 pp345ndash357 2008
[31] A Agarwal S Gupta L Sekhon and R Shah ldquoRedox con-siderations in female reproductive function and assisted repro-duction from molecular mechanisms to health implicationsrdquoAntioxidants amp Redox Signaling vol 10 no 8 pp 1375ndash14032008
[32] P J Devine S D Perreault and U Luderer ldquoRoles of reactiveoxygen species and antioxidants in ovarian toxicityrdquo Biology ofReproduction vol 86 no 2 article 27 2012
[33] K H Al-Gubory C Garrel P Faure and N Sugino ldquoRolesof antioxidant enzymes in corpus luteum rescue from reac-tive oxygen species-induced oxidative stressrdquo ReproductiveBiomedicine Online vol 25 no 6 pp 551ndash560 2012
[34] A Agarwal A Aponte-Mellado B J Premkumar A Shamanand S Gupta ldquoThe effects of oxidative stress on female repro-duction a reviewrdquo Reproductive Biology and Endocrinology vol10 article 49 2012
[35] S Defrere R Gonzalez-Ramos J-C Lousse et al ldquoInsightsinto iron and nuclear factor-kappa B (NF-120581B) involvement inchronic inflammatory processes in peritoneal endometriosisrdquoHistology and Histopathology vol 26 no 8 pp 1083ndash1092 2011
[36] A van Langendonckt F Casanas-Roux and J Donnez ldquoOxida-tive stress and peritoneal endometriosisrdquo Fertility and Sterilityvol 77 no 5 pp 861ndash870 2002
[37] M Appasamy E Jauniaux P Serhal A Al-Qahtani N PGroome and S Muttukrishna ldquoEvaluation of the relationshipbetween follicular fluid oxidative stress ovarian hormones and
response to gonadotropin stimulationrdquo Fertility and Sterilityvol 89 no 4 pp 912ndash921 2008
[38] Y Asano ldquoAge-related accumulation of non-heme ferric andferrous iron in mouse ovarian stroma visualized by sensitivenon-heme iron histochemistryrdquo The Journal of Histochemistryamp Cytochemistry vol 60 no 3 pp 229ndash242 2012
[39] M K Al-Azemi A E Omu T Fatinikun N Mannazhathand S Abraham ldquoFactors contributing to gender differences inserum retinol and 120572-tocopherol in infertile couplesrdquo Reproduc-tive BioMedicine Online vol 19 no 4 pp 583ndash590 2009
[40] M K Kim J W Lee K H Baek et al ldquoEndocrinopathies intransfusion-associated iron overloadrdquo Clinical Endocrinologyvol 78 no 2 pp 271ndash277 2013
[41] L M Hempenius P S van Dam J J Marx and H PKoppeschaar ldquoMineralocorticoid status and endocrine dys-function in severe hemochromatosisrdquo Journal of Endocrinolog-ical Investigation vol 22 no 5 pp 369ndash376 1999
[42] J M Vasquez and R B Greenblatt ldquoPituitary responsiveness toluteinizing-hormone-releasing hormone in different reproduc-tive disorders a reviewrdquo Journal of ReproductiveMedicine for theObstetrician and Gynecologist vol 30 no 8 pp 591ndash600 1985
[43] I Paris M Hermans and M Buysschaert ldquoEndocrine compli-cations of genetic hemochromatosisrdquo Acta Clinica Belgica vol54 no 6 pp 334ndash345 1999
[44] W Stremmel C Niederau M Berger H-K Kley H-LKruskemper and G Strohmeyer ldquoAbnormalities in estrogenandrogen and insulin metabolism in idiopathic hemochro-matosisrdquo Annals of the New York Academy of Sciences vol 526pp 209ndash223 1988
[45] W R Meyer K A Hutchinson-Williams E E Jones and A HDecherney ldquoSecondary hypogonadism in hemochromatosisrdquoFertility and Sterility vol 54 no 4 pp 740ndash742 1990
[46] L J Siemons and C H Mahler ldquoHypogonadotropic hypogo-nadism in hemochromatosis recovery of reproductive functionafter iron depletionrdquo The Journal of Clinical Endocrinology andMetabolism vol 65 no 3 pp 585ndash587 1987
[47] J H McDermott and C H Walsh ldquoHypogonadism in hered-itary hemochromatosisrdquo The Journal of Clinical Endocrinologyand Metabolism vol 90 no 4 pp 2451ndash2455 2005
[48] G Kontogeorgos S Handy K Kovacs E Horvath and BW Scheithauer ldquoThe anterior pituitary in hemochromatosisrdquoEndocrine Pathology vol 7 no 2 pp 159ndash164 1996
[49] A Piperno M R Rivolta R Drsquoalba et al ldquoPreclinical hypog-onadism in genetic hemochromatosis in the early stage ofthe disease evidence of hypothalamic dysfunctionrdquo Journal ofEndocrinological Investigation vol 15 no 6 pp 423ndash428 1992
[50] K SiminoskiM Drsquocosta and P GWalfish ldquoHypogonadotropichypogonadism in idiopathic hemochromatosis evidence forcombined hypothalamic and pituitary involvementrdquo Journal ofEndocrinological Investigation vol 13 no 10 pp 849ndash853 1990
[51] K E Oerter G A Kamp P J Munson A W Nienhuis F GCassorla and P K Manasco ldquoMultiple hormone deficienciesin children with hemochromatosisrdquo The Journal of ClinicalEndocrinology and Metabolism vol 76 no 2 pp 357ndash361 1993
[52] L J Noetzli A Panigrahy S D Mittelman et al ldquoPituitaryiron and volume predict hypogonadism in transfusional ironoverloadrdquo American Journal of Hematology vol 87 no 2 pp167ndash171 2012
[53] R Chatterjee and M Katz ldquoReversible hypogonadotrophichypogonadism in sexually infantile male thalassaemic patientswith transfusional iron overloadrdquo Clinical Endocrinology vol53 no 1 pp 33ndash42 2000
Anemia 9
[54] M Berkovitch T Bistritzer S D Milone K Perlman WKucharczyk and N F Olivieri ldquoIron deposition in the anteriorpituitary in homozygous beta-thalassemia MRI evaluationand correlation with gonadal functionrdquo Journal of PediatricEndocrinology amp Metabolism vol 13 no 2 pp 179ndash184 2000
[55] S Arguelles M Cano A Machado and A Ayala ldquoEffect ofaging and oxidative stress on elongation factor-2 in hypothala-mus and hypophysisrdquo Mechanisms of Ageing and Developmentvol 132 no 1-2 pp 55ndash64 2011
[56] D Gonzalez-Duarte A Madrazo-Atutxa A Soto-Moreno andA Leal-Cerro ldquoMeasurement of oxidative stress and endothe-lial dysfunction in patients with hypopituitarism and severedeficiency adult growth hormone deficiencyrdquo Pituitary vol 15no 4 pp 589ndash597 2012
[57] A Birkenfeld A W Goldfarb E A Rachmilewitz J GSchenker andEOkon ldquoEndometrial glandular haemosiderosisin homozygous beta-thalassaemiardquo European Journal of Obstet-rics Gynecology and Reproductive Biology vol 31 no 2 pp 173ndash178 1989
[58] S T Singer N Sweeters O Vega A Higa E Vichinsky andM Cedars ldquoFertility potential in thalassemia major womencurrent findings and future diagnostic toolsrdquo Annals of the NewYork Academy of Sciences vol 1202 pp 226ndash230 2010
[59] T Dissayabutra P Tosukhowong and P Seksan ldquoThe benefitsof vitamin C and vitamin E in children with beta-thalassemiawith high oxidative stressrdquo Journal of the Medical Association ofThailand vol 88 supplement 4 pp S317ndash321 2005
[60] C Weeraphan C Srisomsap D Chokchaichamnankit et alldquoRole of curcuminoids in ameliorating oxidative modificationin beta-thalassemiaHb E plasma proteomerdquo The Journal ofNutritional Biochemistry vol 24 no 3 pp 578ndash585 2012
[61] E Vichinsky ldquoEmerging ldquoArdquo therapies in hemoglobinopathiesagonists antagonists antioxidants and argininerdquo HematologyAmerican Society Hematology Education Program vol 2012 no1 pp 271ndash275 2012
[62] C Mora-Esteves and D Shin ldquoNutrient supplementationimproving male fertility fourfoldrdquo Seminars in ReproductiveMedicine vol 31 no 4 pp 293ndash300 2013
[63] G J Kontoghiorghes A Efstathiou M Kleanthous YMichaelides and A Kolnagou ldquoRiskbenefit assessmentadvantages over other drugs and targeting methods in the useof deferiprone as a pharmaceutical antioxidant in iron loadingand non iron loading conditionsrdquo Hemoglobin vol 33 no 5pp 386ndash397 2009
[64] U R Kuppusamy and J A Tan ldquoChelation therapy withdesferrioxamine does not normalize ferritin level but attenu-ates oxidative damage and improves total antioxidant level inMalaysian Chinese beta-thalassaemia major patientsrdquoTheWestIndian Medical Journal vol 60 no 1 pp 3ndash8 2011
[65] P B Walter E A Macklin J Porter et al ldquoInflammationand oxidant-stress in 120573-thalassemia patients treated with ironchelators deferasirox (ICL670) or deferoxamine an ancillarystudy of the Novartis CICL670A0107 trialrdquo Haematologica vol93 no 6 pp 817ndash825 2008
[66] V Fenkci S Fenkci M Yilmazer and M Serteser ldquoDecreasedtotal antioxidant status and increased oxidative stress in womenwith polycystic ovary syndrome may contribute to the risk ofcardiovascular diseaserdquo Fertility and Sterility vol 80 no 1 pp123ndash127 2003
[67] C Tatone M C Carbone S Falone et al ldquoAge-dependentchanges in the expression of superoxide dismutases and catalaseare associated with ultrastructural modifications in human
granulosa cellsrdquoMolecular Human Reproduction vol 12 no 11pp 655ndash660 2006
[68] F Gonzalez N S Rote J Minium and J P Kirwan ldquoReactiveoxygen species-induced oxidative stress in the developmentof insulin resistance and hyperandrogenism in polycysticovary syndromerdquo The Journal of Clinical Endocrinology andMetabolism vol 91 no 1 pp 336ndash340 2006
[69] G Basta G Lazzerini M Massaro et al ldquoAdvanced gly-cation end products activate endothelium through signal-transduction receptor RAGE a mechanism for amplification ofinflammatory responsesrdquo Circulation vol 105 no 7 pp 816ndash822 2002
[70] E Devangelio F Santilli G Formoso et al ldquoSoluble RAGE intype 2 diabetes association with oxidative stressrdquo Free RadicalBiology and Medicine vol 43 no 4 pp 511ndash518 2007
[71] G Basta A M Schmidt and R de Caterina ldquoAdvancedglycation end products and vascular inflammation implica-tions for accelerated atherosclerosis in diabetesrdquoCardiovascularResearch vol 63 no 4 pp 582ndash592 2004
[72] R Meerwaldt T Links C Zeebregts R Tio J-L Hillebrandsand A Smit ldquoThe clinical relevance of assessing advanced gly-cation endproducts accumulation in diabetesrdquo CardiovascularDiabetology vol 7 article 29 2008
[73] H Unoki and S Yamagishi ldquoAdvanced glycation end productsand insulin resistancerdquo Current Pharmaceutical Design vol 14no 10 pp 987ndash989 2008
[74] E Diamanti-Kandarakis C Piperi A Kalofoutis and GCreatsas ldquoIncreased levels of serum advanced glycation end-products in women with polycystic ovary syndromerdquo ClinicalEndocrinology vol 62 no 1 pp 37ndash43 2005
[75] D R Mccance D G Dyer J A Dunn et al ldquoMaillardreaction products and their relation to complications in insulin-dependent diabetes mellitusrdquo Journal of Clinical Investigationvol 91 no 6 pp 2470ndash2478 1993
[76] R Singh A Barden TMori and L Beilin ldquoAdvanced glycationend-products a reviewrdquoDiabetologia vol 44 no 2 pp 129ndash1462001
[77] E Diamanti-Kandarakis A Piouka S Livadas et al ldquoAnti-mullerian hormone is associated with advanced glycosylatedend products in lean women with polycystic ovary syndromerdquoEuropean Journal of Endocrinology vol 160 no 5 pp 847ndash8532009
[78] R Chatterjee and R Bajoria ldquoNew concept in natural historyand management of diabetes mellitus in thalassemia majordiabetes and thalassaemiardquo Hemoglobin vol 33 supplement 1pp S127ndashS130 2009
[79] G Paolisso M R Tagliamonte M R Rizzo and D GiuglianoldquoAdvancing age and insulin resistance new facts about anancient historyrdquo European Journal of Clinical Investigation vol29 no 9 pp 758ndash769 1999
[80] N Sattarahmady H Heli and A A Moosavi-Movahedi ldquoDes-feral as improving agent for hemoglobin fructation structuraland functional impactsrdquo The Protein Journal vol 31 no 8 pp651ndash655 2012
[81] E Fibach and E A Rachmilewitz ldquoThe role of antioxidantsand iron chelators in the treatment of oxidative stress inthalassemiardquo Annals of the New York Academy of Sciences vol1202 pp 10ndash16 2010
[82] L M Compagno ldquoCaring for adults with thalassemia in apediatric worldrdquo Annals of the New York Academy of Sciencesvol 1054 pp 266ndash272 2005
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

8 Anemia
[22] A Agarwal A Aponte-Mellado B J Premkumar A Shamanand S Gupta ldquoThe effects of oxidative stress on female repro-duction a reviewrdquo Reproductive Biology and Endocrinology vol10 article 49 2012
[23] M Giergiel M Lopucki N Stachowicz and M KankoferldquoThe influence of age and gender on antioxidant enzymeactivities in humans and laboratory animalsrdquoAging Clinical andExperimental Research vol 24 pp 551ndash559 2012
[24] Q Shazia Z H Mohammad T Rahman and H U ShekharldquoCorrelation of oxidative stress with serum trace element levelsand antioxidant enzyme status in Beta thalassemia majorpatients a review of the literaturerdquo Anemia vol 2012 ArticleID 270923 7 pages 2012
[25] M Y Abdalla M Fawzi S R Al-Maloul N El-Banna R FTayyem and I M Ahmad ldquoIncreased oxidative stress and ironoverload in Jordanian120573-thalassemic childrenrdquoHemoglobin vol35 no 1 pp 67ndash79 2011
[26] R A Ghone K M Kumbar A N Suryakar R V Katkam andN G Joshi ldquoOxidative stress and disturbance in antioxidantbalance in beta thalassemia majorrdquo Indian Journal of ClinicalBiochemistry vol 23 no 4 pp 337ndash340 2008
[27] MA Livrea L Tesoriere AM Pintaudi et al ldquoOxidative stressand antioxidant status in 120573-thalassemia major iron overloadand depletion of lipid-soluble antioxidantsrdquo Blood vol 88 no9 pp 3608ndash3614 1996
[28] S-S Chiou T-T Chang S-P Tsai et al ldquoLipid peroxidationand antioxidative status in 120573-thalassemia major patients withor without hepatitis C virus infectionrdquo Clinical Chemistry andLaboratory Medicine vol 44 no 10 pp 1226ndash1233 2006
[29] A Agarwal and S S Allamaneni ldquoRole of free radicals in femalereproductive diseases and assisted reproductionrdquo ReproductiveBioMedicine Online vol 9 no 3 pp 338ndash347 2004
[30] E H Ruder T J Hartman J Blumberg and M B GoldmanldquoOxidative stress and antioxidants exposure and impact onfemale fertilityrdquoHuman Reproduction Update vol 14 no 4 pp345ndash357 2008
[31] A Agarwal S Gupta L Sekhon and R Shah ldquoRedox con-siderations in female reproductive function and assisted repro-duction from molecular mechanisms to health implicationsrdquoAntioxidants amp Redox Signaling vol 10 no 8 pp 1375ndash14032008
[32] P J Devine S D Perreault and U Luderer ldquoRoles of reactiveoxygen species and antioxidants in ovarian toxicityrdquo Biology ofReproduction vol 86 no 2 article 27 2012
[33] K H Al-Gubory C Garrel P Faure and N Sugino ldquoRolesof antioxidant enzymes in corpus luteum rescue from reac-tive oxygen species-induced oxidative stressrdquo ReproductiveBiomedicine Online vol 25 no 6 pp 551ndash560 2012
[34] A Agarwal A Aponte-Mellado B J Premkumar A Shamanand S Gupta ldquoThe effects of oxidative stress on female repro-duction a reviewrdquo Reproductive Biology and Endocrinology vol10 article 49 2012
[35] S Defrere R Gonzalez-Ramos J-C Lousse et al ldquoInsightsinto iron and nuclear factor-kappa B (NF-120581B) involvement inchronic inflammatory processes in peritoneal endometriosisrdquoHistology and Histopathology vol 26 no 8 pp 1083ndash1092 2011
[36] A van Langendonckt F Casanas-Roux and J Donnez ldquoOxida-tive stress and peritoneal endometriosisrdquo Fertility and Sterilityvol 77 no 5 pp 861ndash870 2002
[37] M Appasamy E Jauniaux P Serhal A Al-Qahtani N PGroome and S Muttukrishna ldquoEvaluation of the relationshipbetween follicular fluid oxidative stress ovarian hormones and
response to gonadotropin stimulationrdquo Fertility and Sterilityvol 89 no 4 pp 912ndash921 2008
[38] Y Asano ldquoAge-related accumulation of non-heme ferric andferrous iron in mouse ovarian stroma visualized by sensitivenon-heme iron histochemistryrdquo The Journal of Histochemistryamp Cytochemistry vol 60 no 3 pp 229ndash242 2012
[39] M K Al-Azemi A E Omu T Fatinikun N Mannazhathand S Abraham ldquoFactors contributing to gender differences inserum retinol and 120572-tocopherol in infertile couplesrdquo Reproduc-tive BioMedicine Online vol 19 no 4 pp 583ndash590 2009
[40] M K Kim J W Lee K H Baek et al ldquoEndocrinopathies intransfusion-associated iron overloadrdquo Clinical Endocrinologyvol 78 no 2 pp 271ndash277 2013
[41] L M Hempenius P S van Dam J J Marx and H PKoppeschaar ldquoMineralocorticoid status and endocrine dys-function in severe hemochromatosisrdquo Journal of Endocrinolog-ical Investigation vol 22 no 5 pp 369ndash376 1999
[42] J M Vasquez and R B Greenblatt ldquoPituitary responsiveness toluteinizing-hormone-releasing hormone in different reproduc-tive disorders a reviewrdquo Journal of ReproductiveMedicine for theObstetrician and Gynecologist vol 30 no 8 pp 591ndash600 1985
[43] I Paris M Hermans and M Buysschaert ldquoEndocrine compli-cations of genetic hemochromatosisrdquo Acta Clinica Belgica vol54 no 6 pp 334ndash345 1999
[44] W Stremmel C Niederau M Berger H-K Kley H-LKruskemper and G Strohmeyer ldquoAbnormalities in estrogenandrogen and insulin metabolism in idiopathic hemochro-matosisrdquo Annals of the New York Academy of Sciences vol 526pp 209ndash223 1988
[45] W R Meyer K A Hutchinson-Williams E E Jones and A HDecherney ldquoSecondary hypogonadism in hemochromatosisrdquoFertility and Sterility vol 54 no 4 pp 740ndash742 1990
[46] L J Siemons and C H Mahler ldquoHypogonadotropic hypogo-nadism in hemochromatosis recovery of reproductive functionafter iron depletionrdquo The Journal of Clinical Endocrinology andMetabolism vol 65 no 3 pp 585ndash587 1987
[47] J H McDermott and C H Walsh ldquoHypogonadism in hered-itary hemochromatosisrdquo The Journal of Clinical Endocrinologyand Metabolism vol 90 no 4 pp 2451ndash2455 2005
[48] G Kontogeorgos S Handy K Kovacs E Horvath and BW Scheithauer ldquoThe anterior pituitary in hemochromatosisrdquoEndocrine Pathology vol 7 no 2 pp 159ndash164 1996
[49] A Piperno M R Rivolta R Drsquoalba et al ldquoPreclinical hypog-onadism in genetic hemochromatosis in the early stage ofthe disease evidence of hypothalamic dysfunctionrdquo Journal ofEndocrinological Investigation vol 15 no 6 pp 423ndash428 1992
[50] K SiminoskiM Drsquocosta and P GWalfish ldquoHypogonadotropichypogonadism in idiopathic hemochromatosis evidence forcombined hypothalamic and pituitary involvementrdquo Journal ofEndocrinological Investigation vol 13 no 10 pp 849ndash853 1990
[51] K E Oerter G A Kamp P J Munson A W Nienhuis F GCassorla and P K Manasco ldquoMultiple hormone deficienciesin children with hemochromatosisrdquo The Journal of ClinicalEndocrinology and Metabolism vol 76 no 2 pp 357ndash361 1993
[52] L J Noetzli A Panigrahy S D Mittelman et al ldquoPituitaryiron and volume predict hypogonadism in transfusional ironoverloadrdquo American Journal of Hematology vol 87 no 2 pp167ndash171 2012
[53] R Chatterjee and M Katz ldquoReversible hypogonadotrophichypogonadism in sexually infantile male thalassaemic patientswith transfusional iron overloadrdquo Clinical Endocrinology vol53 no 1 pp 33ndash42 2000
Anemia 9
[54] M Berkovitch T Bistritzer S D Milone K Perlman WKucharczyk and N F Olivieri ldquoIron deposition in the anteriorpituitary in homozygous beta-thalassemia MRI evaluationand correlation with gonadal functionrdquo Journal of PediatricEndocrinology amp Metabolism vol 13 no 2 pp 179ndash184 2000
[55] S Arguelles M Cano A Machado and A Ayala ldquoEffect ofaging and oxidative stress on elongation factor-2 in hypothala-mus and hypophysisrdquo Mechanisms of Ageing and Developmentvol 132 no 1-2 pp 55ndash64 2011
[56] D Gonzalez-Duarte A Madrazo-Atutxa A Soto-Moreno andA Leal-Cerro ldquoMeasurement of oxidative stress and endothe-lial dysfunction in patients with hypopituitarism and severedeficiency adult growth hormone deficiencyrdquo Pituitary vol 15no 4 pp 589ndash597 2012
[57] A Birkenfeld A W Goldfarb E A Rachmilewitz J GSchenker andEOkon ldquoEndometrial glandular haemosiderosisin homozygous beta-thalassaemiardquo European Journal of Obstet-rics Gynecology and Reproductive Biology vol 31 no 2 pp 173ndash178 1989
[58] S T Singer N Sweeters O Vega A Higa E Vichinsky andM Cedars ldquoFertility potential in thalassemia major womencurrent findings and future diagnostic toolsrdquo Annals of the NewYork Academy of Sciences vol 1202 pp 226ndash230 2010
[59] T Dissayabutra P Tosukhowong and P Seksan ldquoThe benefitsof vitamin C and vitamin E in children with beta-thalassemiawith high oxidative stressrdquo Journal of the Medical Association ofThailand vol 88 supplement 4 pp S317ndash321 2005
[60] C Weeraphan C Srisomsap D Chokchaichamnankit et alldquoRole of curcuminoids in ameliorating oxidative modificationin beta-thalassemiaHb E plasma proteomerdquo The Journal ofNutritional Biochemistry vol 24 no 3 pp 578ndash585 2012
[61] E Vichinsky ldquoEmerging ldquoArdquo therapies in hemoglobinopathiesagonists antagonists antioxidants and argininerdquo HematologyAmerican Society Hematology Education Program vol 2012 no1 pp 271ndash275 2012
[62] C Mora-Esteves and D Shin ldquoNutrient supplementationimproving male fertility fourfoldrdquo Seminars in ReproductiveMedicine vol 31 no 4 pp 293ndash300 2013
[63] G J Kontoghiorghes A Efstathiou M Kleanthous YMichaelides and A Kolnagou ldquoRiskbenefit assessmentadvantages over other drugs and targeting methods in the useof deferiprone as a pharmaceutical antioxidant in iron loadingand non iron loading conditionsrdquo Hemoglobin vol 33 no 5pp 386ndash397 2009
[64] U R Kuppusamy and J A Tan ldquoChelation therapy withdesferrioxamine does not normalize ferritin level but attenu-ates oxidative damage and improves total antioxidant level inMalaysian Chinese beta-thalassaemia major patientsrdquoTheWestIndian Medical Journal vol 60 no 1 pp 3ndash8 2011
[65] P B Walter E A Macklin J Porter et al ldquoInflammationand oxidant-stress in 120573-thalassemia patients treated with ironchelators deferasirox (ICL670) or deferoxamine an ancillarystudy of the Novartis CICL670A0107 trialrdquo Haematologica vol93 no 6 pp 817ndash825 2008
[66] V Fenkci S Fenkci M Yilmazer and M Serteser ldquoDecreasedtotal antioxidant status and increased oxidative stress in womenwith polycystic ovary syndrome may contribute to the risk ofcardiovascular diseaserdquo Fertility and Sterility vol 80 no 1 pp123ndash127 2003
[67] C Tatone M C Carbone S Falone et al ldquoAge-dependentchanges in the expression of superoxide dismutases and catalaseare associated with ultrastructural modifications in human
granulosa cellsrdquoMolecular Human Reproduction vol 12 no 11pp 655ndash660 2006
[68] F Gonzalez N S Rote J Minium and J P Kirwan ldquoReactiveoxygen species-induced oxidative stress in the developmentof insulin resistance and hyperandrogenism in polycysticovary syndromerdquo The Journal of Clinical Endocrinology andMetabolism vol 91 no 1 pp 336ndash340 2006
[69] G Basta G Lazzerini M Massaro et al ldquoAdvanced gly-cation end products activate endothelium through signal-transduction receptor RAGE a mechanism for amplification ofinflammatory responsesrdquo Circulation vol 105 no 7 pp 816ndash822 2002
[70] E Devangelio F Santilli G Formoso et al ldquoSoluble RAGE intype 2 diabetes association with oxidative stressrdquo Free RadicalBiology and Medicine vol 43 no 4 pp 511ndash518 2007
[71] G Basta A M Schmidt and R de Caterina ldquoAdvancedglycation end products and vascular inflammation implica-tions for accelerated atherosclerosis in diabetesrdquoCardiovascularResearch vol 63 no 4 pp 582ndash592 2004
[72] R Meerwaldt T Links C Zeebregts R Tio J-L Hillebrandsand A Smit ldquoThe clinical relevance of assessing advanced gly-cation endproducts accumulation in diabetesrdquo CardiovascularDiabetology vol 7 article 29 2008
[73] H Unoki and S Yamagishi ldquoAdvanced glycation end productsand insulin resistancerdquo Current Pharmaceutical Design vol 14no 10 pp 987ndash989 2008
[74] E Diamanti-Kandarakis C Piperi A Kalofoutis and GCreatsas ldquoIncreased levels of serum advanced glycation end-products in women with polycystic ovary syndromerdquo ClinicalEndocrinology vol 62 no 1 pp 37ndash43 2005
[75] D R Mccance D G Dyer J A Dunn et al ldquoMaillardreaction products and their relation to complications in insulin-dependent diabetes mellitusrdquo Journal of Clinical Investigationvol 91 no 6 pp 2470ndash2478 1993
[76] R Singh A Barden TMori and L Beilin ldquoAdvanced glycationend-products a reviewrdquoDiabetologia vol 44 no 2 pp 129ndash1462001
[77] E Diamanti-Kandarakis A Piouka S Livadas et al ldquoAnti-mullerian hormone is associated with advanced glycosylatedend products in lean women with polycystic ovary syndromerdquoEuropean Journal of Endocrinology vol 160 no 5 pp 847ndash8532009
[78] R Chatterjee and R Bajoria ldquoNew concept in natural historyand management of diabetes mellitus in thalassemia majordiabetes and thalassaemiardquo Hemoglobin vol 33 supplement 1pp S127ndashS130 2009
[79] G Paolisso M R Tagliamonte M R Rizzo and D GiuglianoldquoAdvancing age and insulin resistance new facts about anancient historyrdquo European Journal of Clinical Investigation vol29 no 9 pp 758ndash769 1999
[80] N Sattarahmady H Heli and A A Moosavi-Movahedi ldquoDes-feral as improving agent for hemoglobin fructation structuraland functional impactsrdquo The Protein Journal vol 31 no 8 pp651ndash655 2012
[81] E Fibach and E A Rachmilewitz ldquoThe role of antioxidantsand iron chelators in the treatment of oxidative stress inthalassemiardquo Annals of the New York Academy of Sciences vol1202 pp 10ndash16 2010
[82] L M Compagno ldquoCaring for adults with thalassemia in apediatric worldrdquo Annals of the New York Academy of Sciencesvol 1054 pp 266ndash272 2005
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

Anemia 9
[54] M Berkovitch T Bistritzer S D Milone K Perlman WKucharczyk and N F Olivieri ldquoIron deposition in the anteriorpituitary in homozygous beta-thalassemia MRI evaluationand correlation with gonadal functionrdquo Journal of PediatricEndocrinology amp Metabolism vol 13 no 2 pp 179ndash184 2000
[55] S Arguelles M Cano A Machado and A Ayala ldquoEffect ofaging and oxidative stress on elongation factor-2 in hypothala-mus and hypophysisrdquo Mechanisms of Ageing and Developmentvol 132 no 1-2 pp 55ndash64 2011
[56] D Gonzalez-Duarte A Madrazo-Atutxa A Soto-Moreno andA Leal-Cerro ldquoMeasurement of oxidative stress and endothe-lial dysfunction in patients with hypopituitarism and severedeficiency adult growth hormone deficiencyrdquo Pituitary vol 15no 4 pp 589ndash597 2012
[57] A Birkenfeld A W Goldfarb E A Rachmilewitz J GSchenker andEOkon ldquoEndometrial glandular haemosiderosisin homozygous beta-thalassaemiardquo European Journal of Obstet-rics Gynecology and Reproductive Biology vol 31 no 2 pp 173ndash178 1989
[58] S T Singer N Sweeters O Vega A Higa E Vichinsky andM Cedars ldquoFertility potential in thalassemia major womencurrent findings and future diagnostic toolsrdquo Annals of the NewYork Academy of Sciences vol 1202 pp 226ndash230 2010
[59] T Dissayabutra P Tosukhowong and P Seksan ldquoThe benefitsof vitamin C and vitamin E in children with beta-thalassemiawith high oxidative stressrdquo Journal of the Medical Association ofThailand vol 88 supplement 4 pp S317ndash321 2005
[60] C Weeraphan C Srisomsap D Chokchaichamnankit et alldquoRole of curcuminoids in ameliorating oxidative modificationin beta-thalassemiaHb E plasma proteomerdquo The Journal ofNutritional Biochemistry vol 24 no 3 pp 578ndash585 2012
[61] E Vichinsky ldquoEmerging ldquoArdquo therapies in hemoglobinopathiesagonists antagonists antioxidants and argininerdquo HematologyAmerican Society Hematology Education Program vol 2012 no1 pp 271ndash275 2012
[62] C Mora-Esteves and D Shin ldquoNutrient supplementationimproving male fertility fourfoldrdquo Seminars in ReproductiveMedicine vol 31 no 4 pp 293ndash300 2013
[63] G J Kontoghiorghes A Efstathiou M Kleanthous YMichaelides and A Kolnagou ldquoRiskbenefit assessmentadvantages over other drugs and targeting methods in the useof deferiprone as a pharmaceutical antioxidant in iron loadingand non iron loading conditionsrdquo Hemoglobin vol 33 no 5pp 386ndash397 2009
[64] U R Kuppusamy and J A Tan ldquoChelation therapy withdesferrioxamine does not normalize ferritin level but attenu-ates oxidative damage and improves total antioxidant level inMalaysian Chinese beta-thalassaemia major patientsrdquoTheWestIndian Medical Journal vol 60 no 1 pp 3ndash8 2011
[65] P B Walter E A Macklin J Porter et al ldquoInflammationand oxidant-stress in 120573-thalassemia patients treated with ironchelators deferasirox (ICL670) or deferoxamine an ancillarystudy of the Novartis CICL670A0107 trialrdquo Haematologica vol93 no 6 pp 817ndash825 2008
[66] V Fenkci S Fenkci M Yilmazer and M Serteser ldquoDecreasedtotal antioxidant status and increased oxidative stress in womenwith polycystic ovary syndrome may contribute to the risk ofcardiovascular diseaserdquo Fertility and Sterility vol 80 no 1 pp123ndash127 2003
[67] C Tatone M C Carbone S Falone et al ldquoAge-dependentchanges in the expression of superoxide dismutases and catalaseare associated with ultrastructural modifications in human
granulosa cellsrdquoMolecular Human Reproduction vol 12 no 11pp 655ndash660 2006
[68] F Gonzalez N S Rote J Minium and J P Kirwan ldquoReactiveoxygen species-induced oxidative stress in the developmentof insulin resistance and hyperandrogenism in polycysticovary syndromerdquo The Journal of Clinical Endocrinology andMetabolism vol 91 no 1 pp 336ndash340 2006
[69] G Basta G Lazzerini M Massaro et al ldquoAdvanced gly-cation end products activate endothelium through signal-transduction receptor RAGE a mechanism for amplification ofinflammatory responsesrdquo Circulation vol 105 no 7 pp 816ndash822 2002
[70] E Devangelio F Santilli G Formoso et al ldquoSoluble RAGE intype 2 diabetes association with oxidative stressrdquo Free RadicalBiology and Medicine vol 43 no 4 pp 511ndash518 2007
[71] G Basta A M Schmidt and R de Caterina ldquoAdvancedglycation end products and vascular inflammation implica-tions for accelerated atherosclerosis in diabetesrdquoCardiovascularResearch vol 63 no 4 pp 582ndash592 2004
[72] R Meerwaldt T Links C Zeebregts R Tio J-L Hillebrandsand A Smit ldquoThe clinical relevance of assessing advanced gly-cation endproducts accumulation in diabetesrdquo CardiovascularDiabetology vol 7 article 29 2008
[73] H Unoki and S Yamagishi ldquoAdvanced glycation end productsand insulin resistancerdquo Current Pharmaceutical Design vol 14no 10 pp 987ndash989 2008
[74] E Diamanti-Kandarakis C Piperi A Kalofoutis and GCreatsas ldquoIncreased levels of serum advanced glycation end-products in women with polycystic ovary syndromerdquo ClinicalEndocrinology vol 62 no 1 pp 37ndash43 2005
[75] D R Mccance D G Dyer J A Dunn et al ldquoMaillardreaction products and their relation to complications in insulin-dependent diabetes mellitusrdquo Journal of Clinical Investigationvol 91 no 6 pp 2470ndash2478 1993
[76] R Singh A Barden TMori and L Beilin ldquoAdvanced glycationend-products a reviewrdquoDiabetologia vol 44 no 2 pp 129ndash1462001
[77] E Diamanti-Kandarakis A Piouka S Livadas et al ldquoAnti-mullerian hormone is associated with advanced glycosylatedend products in lean women with polycystic ovary syndromerdquoEuropean Journal of Endocrinology vol 160 no 5 pp 847ndash8532009
[78] R Chatterjee and R Bajoria ldquoNew concept in natural historyand management of diabetes mellitus in thalassemia majordiabetes and thalassaemiardquo Hemoglobin vol 33 supplement 1pp S127ndashS130 2009
[79] G Paolisso M R Tagliamonte M R Rizzo and D GiuglianoldquoAdvancing age and insulin resistance new facts about anancient historyrdquo European Journal of Clinical Investigation vol29 no 9 pp 758ndash769 1999
[80] N Sattarahmady H Heli and A A Moosavi-Movahedi ldquoDes-feral as improving agent for hemoglobin fructation structuraland functional impactsrdquo The Protein Journal vol 31 no 8 pp651ndash655 2012
[81] E Fibach and E A Rachmilewitz ldquoThe role of antioxidantsand iron chelators in the treatment of oxidative stress inthalassemiardquo Annals of the New York Academy of Sciences vol1202 pp 10ndash16 2010
[82] L M Compagno ldquoCaring for adults with thalassemia in apediatric worldrdquo Annals of the New York Academy of Sciencesvol 1054 pp 266ndash272 2005
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom