Embed Size (px)
Citation preview

ORTHOPEDICS | Healio.com/Orthopedics
n Feature Article
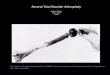
Figure: Anteroposterior (A) and lateral (B) radio-graphs of tibial and femoral metaphyseal sleeves with the P.F.C. Sigma Knee Revision System (DePuy, Warsaw, Indiana), TC3 Femur, and MBT revision tray.
Revision Total Knee Arthroplasty Using Metaphyseal Sleeves at Short-term Follow-upRonald Huang, Md; gustavo BaRRazueta, Bs; alvin ong, Md; FaBio oRozco, Md; MeHdi JaFaRi, Md; catelyn coyle, Bs; MattHew austin, Md
The treatment of bone loss in revision total knee arthroplasty (TKA) has involved using revision implants in association with cement, augments, particulate, and struc-tural allograft. Newer metaphyseal augments were introduced to allow for metaphy-seal fixation of the prosthesis while managing significant bone loss. The purpose of the current study was to evaluate the outcome of revision TKA using metaphyseal sleeves. The authors prospectively followed 96 knees that underwent revision TKA with metaphyseal sleeves. Eighty-three knees met the minimum 2-year criteria for follow-up. Thirty-six sleeves were used in femoral revisions and 83 sleeves were used in tibial revisions. The defects were classified according to the Anderson Ortho-paedic Research Institute classification. Femoral defects were classified as type I in 4 knees, type IIb in 25 knees, and type III in 7 knees. Tibial defects were classified as type I in 9 knees, type IIa in 1 knee, type IIb in 68 knees, and type III in 5 knees. The patients were followed for an average of 2.4 years (range, 2.0-3.7 years). Mean Knee Society function score improved from 47.9 to 61.1 points. Mean Short Form 36 phys-ical score improved from 43.3 to 56.3 points. Mean Western Ontario and McMaster Universities Arthritis Index improved from 55.3 to 25.9 points. None of the implants demonstrated progressive radiolucent lines around the metaphyseal sleeves. At final follow-up, only 2 (2.7%) tibial components required revision for aseptic loosening. At short-term follow-up, revision TKA with metaphyseal sleeves provided reliable fixation. This is especially encouraging given the severe nature of bone loss in the majority of patients in whom a metaphyseal sleeve was used. Long-term follow-up is needed to demonstrate the true effectiveness of these devices.
The authors are from the Rothman Institute, Thomas Jefferson University Hospital, Philadelphia, Pennsylvania.
Drs Huang and Jafari, Mr Barrazueta, and Ms Coyle have no relevant financial relationships to disclose. Dr Ong is a paid consultant for Stryker, Smith & Nephew, and Zimmer. Dr Orozco is a paid consultant for Stryker. Dr Austin receives royalties from Zimmer and research support from DePuy.
Correspondence should be addressed to: Matthew Austin, MD, Rothman Institute, Thomas Jefferson University Hospital, 925 Chestnut St, Philadelphia, PA 19107 ([email protected]).
Received: August 25, 2013; Accepted: January 30, 2014; Posted: September 9, 2014.doi: 10.3928/01477447-20140825-57
A B
abstractFull article available online at Healio.com/Orthopedics
e804

SEPTEMBER 2014 | Volume 37 • Number 9
n Feature Article
The number of revision total knee arthroplasty (TKA) procedures performed per year is expected
to rise from 38,300 in 2005 to 268,300 by the year 2030.1 In the United States, the most common type of revision TKA involves revision of all components.2 The method of reconstruction used for revision TKA depends on the remaining bone stock, integrity of the ligaments, and ability to balance the flexion and ex-tension gaps. The Anderson Orthopaedic Research Institute (AORI) classification provides a useful tool for classifying and predicting the method of reconstruction of bony defects associated with revision TKA.3 Type I defects involve an intact me-taphyseal rim and joint line with bone de-fects of less than 1 cm. These defects can be reconstructed with cement, morselized allograft, or metal augments. Type II de-fects involve significant cancellous bone loss with a relatively intact metaphyseal rim and require joint line restoration. Type II defects are stratified into type IIa and type IIb. Type IIa defects involve 1 con-dyle or side of the tibial plateau, whereas type IIb defects involve both condyles or both sides of the tibial plateau. Type II defects can be reconstructed with metal augments, impaction grafting, structural allograft, metaphyseal sleeves, or porous metal cones. Type III defects involve large metaphyseal rim defects with sig-nificant cancellous bone loss and can be reconstructed with impaction grafting, structural allograft, metaphyseal sleeves, porous metal cones, composite allograft, or so-called megaprostheses. The use of cement, metal augments, morselized al-lograft, structural allograft, impaction grafting, and porous metal cones has been previously reported with short- to mid-term follow-up.4-16
Metaphyseal-filling tantalum cones and sleeves are hypothesized to help re-store the joint line and provide implant stability in large bony defects by provid-ing a surface for fixation in the metaphy-sis, allowing surgeons to avoid excess
bone resection, and sharing intramedul-lary loading forces. These implants are 2 distinct technologies with different implantation techniques and philoso-phies. Multiple recent studies have dem-onstrated favorable short-term outcomes using tantalum cones.4,6,8,9,11 However, the clinical results of metaphyseal sleeves are relatively unknown. The use of metaphy-seal sleeves in 30 hinged revision TKAs with mid-term follow-up was reported by Jones et al,10 with no mechanical failures in the series. Alexander et al17 recently reported a smaller series of 30 tibial me-taphyseal sleeves with no failures at short-term follow-up. Metaphyseal sleeves were recently introduced for use with a modu-lar, mobile-bearing knee revision system (P.F.C. Sigma Knee Revision System; DePuy, Warsaw, Indiana). The current study represents the only report, to the authors’ knowledge, of the short-term re-sults of revision TKA with both femoral and tibial metaphyseal sleeves using both nonhinged and hinged designs.
Materials and MethodsInstitutional review board approval
was obtained from the authors’ institution for this study. Ninety-six consecutive re-vision TKAs using metaphyseal sleeves for tibial and/or femoral bone loss were performed by the senior author (M.A.) between January 2007 and June 2010. Perioperative data were prospectively col-lected on all patients. Seven patients were lost to follow-up, and 6 patients died prior to reaching 2-year follow-up. The 83 re-maining knees (79 patients, 119 sleeves) composed the study cohort. Average dura-tion of follow-up was 2.4 years (range, 2.0 to 3.7 years).
At the time of surgery, average patient age was 63.5 years and average body mass index was 33 kg/m2. There were 29 males and 50 females. The indications for revi-sion included aseptic loosening (51 knees), second-stage reimplantation for peripros-thetic infection (20 knees), instability (6 knees), periprosthetic fracture (4 knees),
and stiffness (2 knees). A modular, mobile-bearing, posterior-stabilized P.F.C. Sigma Knee Revision System (Figure 1) was used in 73 knees, and 10 knees were recon-structed using an S-ROM Noiles hinged prosthesis (DePuy; Figure 2).
Bone defects were classified using the AORI classification.1 Bone loss was evaluated using preoperative radiographs by 2 orthopedic surgeons (A.O., F.O.) not involved in the care of the patients. Meta- physeal sleeves were used in 36 femoral and 83 tibial revisions. Femoral defects were classified as type I in 4 knees, type
Figure 1: Anteroposterior (A) and lateral (B) radio-graphs of tibial and femoral metaphyseal sleeves with the P.F.C. Sigma Knee Revision System (DePuy, Warsaw, Indiana), TC3 Femur, and MBT revision tray.
A B
Figure 2: Anteroposterior (A) and lateral (B) radio-graphs of tibial and femoral metaphyseal sleeves with the S-ROM Noiles hinged knee (DePuy, War-saw, Indiana).
A B
e805

ORTHOPEDICS | Healio.com/Orthopedics
n Feature Article
IIb in 25 knees, and type III in 7 knees. Tibial defects were classified as type I in 9 knees, type IIa in 1 knee, type IIb in 68 knees, and type III in 5 knees. Pa-tients were evaluated preoperatively and at each postoperative visit using the Short Form 36 (SF-36), Western Ontario and McMaster Universities Arthritis Index (WOMAC), and functional Knee Society Score (KSS). Postoperative radiographic assessment was performed by 2 high- volume revision joint arthroplasty sur-geons (A.O., F.O.) not involved in the care of the patients, based on the Knee Society Total Knee Arthroplasty Roentgenograph-ic Evaluation.18 Disputes were resolved using review by a third joint arthroplasty surgeon. Only 1 case required review by a third surgeon to confirm evidence of ra-diographic loosening. Interobserver reli-ability analysis was performed using the kappa statistic to determine consistency in interpretation of loosening on postopera-tive radiographs. Interobserver reliability was found to be kappa=0.926 (P<.001; 95% confidence interval, 0.783 to 1.000). Minimum 1-year radiographic follow-up was unavailable for 8 of 83 knees, which were excluded from radiographic analy-sis.
surgical techniqueA medial parapatellar approach was
used for all cases. The components and cement were removed carefully with thin osteotomes, saws, and burrs. The femoral and tibial canals were hand reamed se-quentially until the reamer achieved firm endosteal contact. The stem length was determined by the ability to gain diaphy-seal fit. The remaining bone stock was assessed and the need for a sleeve was determined. Generally, tibial sleeves were used in all cases, whereas femoral sleeves were used in type IIb and III defects. In cases where a sleeve was used, a starter reamer was used to open the metaphyseal bone for the first broach. The metaphyseal bone was then broached sequentially until the broaches were axially and torsionally
stable. Trial components were inserted. Standard revision technique was followed to achieve appropriate alignment, restora-tion of the joint line, flexion-extension gap balancing, patella tracking, and range of motion. The final components were insert-ed using a press-fit sleeve and stem with cementation of the condylar portion of the femoral prosthesis distal to the sleeve or to the level of the metaphysis in cases where a sleeve was not used. The tibial tray was cemented, and the sleeve and stem were press fit. Patients were allowed weight bearing as tolerated with assistive devices immediately postoperatively.
resultsClinical Outcome
Mean Knee Society function score improved from 47.9 (range, 5 to 100) preoperatively to 61.1 (range, 0 to 100; P<.001) postoperatively. Mean SF-36 physical score improved from 43.3 (range, 12 to 75) preoperatively to 56.3 (range, 11 to 89; P<.001) postop-eratively, and mean SF-36 mental score improved from 61.8 (range, 17 to 93) preoperatively to 69.4 (range, 22 to 96; P=.024) postoperatively. Mean WOMAC improved from 55.3 (range, 23 to 98) preoperatively to 25.9 (range, 0 to 88; P<.001) postoperatively.
Radiographic OutcomePostoperative anteroposterior radio-
graphs were reviewed at last follow-up. Average tibiofemoral alignment was 4.3° valgus (range, 0° to 8.5°). Average femo-ral component alignment in the coronal plane was 4.6° valgus (range, 2° to 6.5°) in the entire cohort of patients and 4.5° valgus (range, 2° to 6.5°) in the cohort that had a femoral sleeve. In the patients with femoral metaphyseal sleeves, there were no outliers in femoral component coronal alignment (greater than 9° or less than 2° valgus from the anatomic axis). Average tibial component alignment in the coronal plane was 0.2° varus (range, 3.0° varus to 3.2° valgus). One tibial component was
considered an outlier (greater than 3° from neutral mechanical axis). Progres-sive radiolucent lines around the metaph-yseal sleeve were not seen in any of the 29 knees with femoral sleeves nor any of the 75 knees with tibial sleeves for which 1-year postoperative films were avail-able. Progressive radiolucent lines were seen around the femoral stem in 2 knees with femoral sleeves (2 of 29 knees with femoral sleeves) and around the femoral stem in 3 knees without femoral sleeves (3 of 46 knees without femoral sleeves). Progressive radiolucent lines were seen around the tibial stem in 7 knees with tibi-al sleeves (7 of 75 knees). No evidence of subsidence was seen in any knee.
ReoperationFourteen (16.9%) knees required reop-
eration after revision TKA with metaphy-seal sleeves (Table). Two (2.4%) patients developed aseptic loosening of the tibial metaphyseal sleeve 2 years postopera-tively. Another patient underwent iso-lated femoral component revision TKA for aseptic loosening (no femoral sleeve). Six (7.2%) knees developed peripros-thetic joint infection. Of these 6 knees, 3 underwent 2-stage exchange, 2 under-went irrigation and debridement, and 1 underwent irrigation and debridement and subsequent above-knee amputation. Five of the 6 knees that developed peripros-thetic joint infection following use of a metaphyseal sleeve were reimplantations of 2-stage revisions for infection. The incidence of reinfection following use of the sleeve in reimplantation was 5 (25%) of 20 knees, and incidence of infection in cases performed for aseptic etiologies was 1 (1.6%) of 63 knees. One (1.2%) patient underwent partial patellectomy following a patellar fracture, and the remaining 4 (4.8%) patients required a manipulation under anesthesia.
discussionThis study represents the only report,
to the authors’ knowledge, of the short-
e806

SEPTEMBER 2014 | Volume 37 • Number 9
n Feature Article
term results of revision TKA with both femoral and tibial metaphyseal sleeves using both nonhinged and hinged designs. There is a paucity of information in the literature regard-ing the outcomes of specific methods of reconstruction used in revision TKA. The short-term survivorship was 92.8% (77 of 83 knees). Only 2 tibial metaphyseal sleeves (2 [2.4%] of 83) were revised for aseptic loosening. No femoral component with a sleeve re-quired revision for aseptic loosening; therefore, survivorship of sleeves was 98.2% (111 of 113 sleeves not revised for infection). This was despite use in a high percentage of AORI type IIb and III defects (89.0% of femoral and 88.0% of tibial revisions). The authors’ short-term results demonstrate favor-able implant fixation and survivorship using metaphyseal sleeves in the face of massive bone loss.
The decision to use the sleeve was made at the discretion of the operat-ing surgeon based on quantitative and qualitative aspects of the host bone, constraint of the prosthesis to be used, and comfort with the method of re-construction. Unfortunately, a specific algorithm for use of these sleeves was not used. The authors acknowledge that cost is one important factor in determining the method of reconstruc-tion and recognize that other options exist for reconstruction of type I de-fects, including, but not limited to, so-called hybrid metaphyseal fixation with cement and fully cemented im-plants. The use of a sleeve adds ap-proximately 30% to the cost of each implant. The authors acknowledge that use of these implants should be restricted to cases of severe bone loss where conventional reconstruc-tive methods may not provide reliable long-term fixation.
Furthermore, the decision to use a sleeve was based on the need for fixa-tion, but implant positioning was also
Tabl
e
Reo
per
atio
n Fo
llow
ing
Rev
isio
n TK
A W
ith
Met
aphy
seal
Sle
eves
Pati
ent
No.
/Se
x/A
ge, y
BM
I, k
g/m
2In
dica
tion
for
Inde
x R
evis
ion
Tibi
al A
OR
I Ty
peFe
mor
al A
OR
I Ty
peSl
eeve
Hin
geIn
dica
tion
for
Reo
pera
tion
Reo
pera
tion
Tim
e to
R
eope
rati
on,
mo
1/M
/69
35A
sept
ic lo
osen
ing
2b1
T1
Infe
ctio
nR
esec
tion
TKA
and
sp
acer
12
2/M
/55
302n
d st
age
2b2b
T an
d F
0In
fect
ion
I&D
4
3/F/
8026
Inst
abili
ty2b
2bT
and
F1
Art
hrofi
bros
isM
UA
1
4/F/
4740
2nd
stag
e2b
2bT
0In
fect
ion
I&D
2
5/F/
6337
2nd
stag
e2b
2bT
0Pa
tella
r fr
actu
rePa
rtia
l pat
elle
ctom
y4
6/M
/67
332n
d st
age
2b2b
T0
Art
hrofi
bros
isM
UA
2
7/F/
5933
Ase
ptic
loos
enin
g2b
2bT
0A
sept
ic lo
osen
ing
Isol
ated
fem
oral
co
mpo
nent
rev
isio
n26
8/F/
4929
Ase
ptic
loos
enin
g1
1T
0A
rthr
ofibr
osis
MU
A2
9/M
/68
33A
sept
ic lo
osen
ing
2b2b
T0
Ase
ptic
loos
enin
g1-
stag
e re
visi
on T
KA
47
10/F
/69
342n
d st
age
2b2b
T0
Infe
ctio
nR
esec
tion
TKA
and
sp
acer
<1
11/M
/71
352n
d st
age
33
T an
d F
0In
fect
ion
Res
ectio
n TK
A a
nd
spac
er2
12/F
/79
31A
sept
ic lo
osen
ing
2b2b
T0
Ase
ptic
loos
enin
g1-
stag
e re
visi
on T
KA
22
13/F
/64
282n
d st
age
2b2b
T an
d F
0In
fect
ion
Res
ectio
n TK
A a
nd
spac
er 1
1
14/F
/49
43A
sept
ic lo
osen
ing
32b
T an
d F
0A
rthr
ofibr
osis
MU
A1
Abb
revi
atio
ns:
AO
RI,
And
erso
n O
rtho
paed
ic R
esea
rch
Inst
itut
e; B
MI,
bod
y m
ass
inde
x; F
, fem
oral
; I&
D, i
rrig
atio
n an
d de
brid
emen
t; M
, mal
e; M
UA
, man
ipul
atio
n un
der
anes
thes
ia;
T, ti
bial
; T
KA
, tot
al k
nee
arth
ropl
asty
.
e807

ORTHOPEDICS | Healio.com/Orthopedics
n Feature Article
an important factor. The sleeves may re-sult in imperfect component positioning, or the bone defect geometry that is present may force the component into a less-than-perfect position. Thus, the surgeon must perform proper preoperative planning and surgical execution to reduce the risk of malpositioning. Use of intraoperative ra-diographs or fluoroscopy may reduce the chance of malposition.
In the current study, alignment of 1 tibial stem and sleeve component was con-sidered an outlier (greater than 3° outside of neutral mechanical axis). Indication for revision in this case was the second stage of a 2-stage revision for periprosthetic joint infection. The patient had AORI type IIb bone loss in both the tibia and femur, and a tibial sleeve was used during reconstruc-tion. At 3-year follow-up, the patient’s ra-diographs demonstrated a tibial component in 5° of valgus from neutral mechanical axis and femoral component in 3° of val-gus, with an overall mechanical alignment of 8° of valgus. There was no evidence of radiographic loosening and no complica-tions related to component positioning.
In cases of loosening of metaphyseal sleeves requiring re-revision, the diffi-culty in removing metaphyseal sleeves depends on whether osseointegration has occurred. The vast majority of the ex-plantation procedures either occurred in the acute postoperative period prior to osseointegration or were performed for aseptic loosening, greatly facilitating re-moval of the sleeves. The senior author has removed several well-fixed sleeves that were not included in this study (they were implanted at an outside institution). Anecdotally, the femoral sleeves have required an anterior cortical window for removal, and the tibial sleeves have been less difficult to remove but have occasion-ally required a tibial tubercle osteotomy. The amount of bone loss encountered at the time of re-revision depends on mul-tiple variables, including host bone stock, fixation of the components, and the need to create a cortical defect.
There are a few significant limitations to this study. First, each patient presents unique challenges, which may have af-fected the results. This is a problem inher-ent to all studies involving revision TKA patients. Second, follow-up time was short (an average of 2.4 years [range, 2.0 to 3.7 years]). Third, the authors were not able to formally assess mechanical align-ment because full-length standing radio-graphs were not available for all patients. Finally, 7 patients were lost to follow-up, 6 died before reaching 2-year follow-up, and an additional 8 had no 1-year radio-graphs available. The authors found no radiolucencies around the metaphyseal sleeves that they were able to evaluate ra-diographically (75 knees), and it is pos-sible that 1 or more of the patients without radiographs may have had radiolucencies. However, they were not revised for asep-tic loosening at a minimum 2-year follow-up. Despite these limitations, this study’s strengths are that it is the first series, to the authors’ knowledge, to report outcomes of metaphyseal sleeves with this revision im-plant. Furthermore, the cohort of 83 revi-sion TKAs is a relatively large series.
The results of revision TKA are some-what unclear given the multiple methods of reconstruction, including the use of cement, metal augments, impaction bone grafting, structural bone graft, metaphy-seal sleeves, and porous in-growth com-ponents.1,4-13,15,16 In addition, prosthesis design factors, such as level of constraint and cemented vs uncemented stems, fur-ther add to the variability of reconstruc-tive methods and subsequent reporting of outcomes.
The literature on cement filling of de-fects in revision TKA is scarce. Dorr et al14 recommended bone grafting voids greater than 5 mm rather than filling with cement. Patel et al5 reported 79 AORI type II defects treated with metal augments at a mean follow-up of 7 years. The compo-nents were cemented in a hybrid fixation fashion. The survivorship of the compo-nents at 11 years was 92%. Lotke et al7 re-
ported the mid-term results of 48 revision knees treated with impaction grafting. They reported no mechanical failures, and all grafts incorporated and remodeled ra-diographically. The complication rate was 14%, including 2 periprosthetic fractures and 2 infections. The technique was not-ed to be technically demanding and time consuming. Clatworthy et al15 reported 52 revision knees at mid-term follow-up using structural allograft for uncontained defects. Thirteen knees failed, resulting in a 25% failure rate. Allograft survival was 72%. Ghazavi et al12 published a series of 30 knees with massive bone defects treated with bulk allograft at an average 50-month follow-up. Two patients failed due to tibial component loosening (in which allograft had been used), 1 patient failed due to graft fracture, and 1 patient failed due to graft nonunion. Bauman et al16 reported the Mayo Clinic experience with structural allograft in TKAs. They reported a 22.8% failure rate in a cohort of 70 knees. In contrast to these reports, Engh and Ammeen13 reported the mid-term results of 46 knees in which struc-tural allograft was used in revision tibial arthroplasty. Four patients in that series required reoperation, but none were di-rectly due to collapse or failure of the al-lograft.
To the current authors’ knowledge, there are limited data in the literature on results of stepped metaphyseal sleeves. Jones et al10 reported a series of 30 knees treated with the S-ROM hinged-knee sys-tem with metaphyseal sleeves. They dem-onstrated no mechanical failures at mid-term follow-up of 49 months. Alexander et al17 recently reported a smaller series of 30 tibial metaphyseal sleeves with no failures at short-term follow-up.
Other porous metal implants have been used with reported short-term success. Long and Scuderi8 reported a series of 16 cases using tantalum tibial cones in AORI type II and III defects with no mechanical failures at a minimum 2-year follow-up. Meneghini et al6 reported a series of 15
e808

SEPTEMBER 2014 | Volume 37 • Number 9
n Feature Article
porous tantalum cones used for tibial revi-sions with AORI type II and III defects. All implants showed evidence of osseo- integration at an average 34-month fol-low-up. Howard et al11 studied a series of 24 porous tantalum cones used for type IIb or greater femoral bone loss during TKA. At a mean 33-month follow-up, no mechanical failures were associated with the use of the cones. Recently, Lachie-wicz et al9 reported outcomes of 33 tan-talum cones (9 femoral and 24 tibial) in 27 patients. All cones except for 1 demon-strated evidence of osseointegration at an average 3.3-year follow-up. One knee in their series was revised for femoral cone and component loosening.
conclusionGiven the anticipated increase in revi-
sion burden in the United States to over 268,000 cases by the year 2030, a reli-able method to reconstruct a wide array of bone defects is paramount.2 The eco-nomic effect of these procedures will be substantial, with hospital charges for revision procedures accounting for $4.1 billion and surgical charges reaching $0.34 billion by the year 2015.3 The out-comes of these procedures will be close-ly monitored by payers in the future. The anticipated bone loss as assessed by radiographs often underestimates the actual intraoperative bone loss encoun-tered.19 Therefore, a system to accommo-date type I to type III defects would be ideal to allow for reconstruction within a single revision system. The P.F.C. Sigma
Knee and S-ROM Noiles hinged knee re-vision system with metaphyseal sleeves may offer such a method. However, long-term follow-up is required to support the early success seen with the use of these devices.
references 1. Engh GA, Ammeen DJ. Bone loss with revi-
sion total knee arthroplasty: defect classifica-tion and alternatives for reconstruction. Instr Course Lect. 1999; 48:167-175.
2. Kurtz S, Ong K, Lau E, Mowat F, Halpern M. Projections of primary and revision hip and knee arthroplasty in the United States from 2005 to 2030. J Bone Joint Surg Am. 2007; 89(4):780-785.
3. Kurtz SM, Ong KL, Schmier J, et al. Future clinical and economic impact of revision to-tal hip and knee arthroplasty. J Bone Joint Surg Am. 2007; 89(suppl 3):144-151.
4. Radnay CS, Scuderi GR. Management of bone loss: augments, cones, offset stems. Clin Orthop Relat Res. 2006; 446:83-92.
5. Patel JV, Masonis JL, Guerin J, Bourne RB, Rorabeck CH. The fate of augments to treat type-2 bone defects in revision knee arthroplasty. J Bone Joint Surg Br. 2004; 86(2):195-199.
6. Meneghini RM, Lewallen DG, Hanssen AD. Use of porous tantalum metaphyseal cones for severe tibial bone loss during revision to-tal knee replacement. J Bone Joint Surg Am. 2008; 90(1):78-84.
7. Lotke PA, Carolan GF, Puri N. Impaction grafting for bone defects in revision total knee arthroplasty. Clin Orthop Relat Res. 2006; 446:99-103.
8. Long WJ, Scuderi GR. Porous tantalum cones for large metaphyseal tibial defects in revision total knee arthroplasty: a mini-mum 2-year follow-up. J Arthroplasty. 2009; 24(7):1086-1092.
9. Lachiewicz PF, Bolognesi MP, Henderson RA, Soileau ES, Vail TP. Can tantalum cones
provide fixation in complex revision knee arthroplasty? Clin Orthop Relat Res. 2012; 470(1):199-204.
10. Jones RE, Barrack RL, Skedros J. Modular, mobile-bearing hinge total knee arthroplasty. Clin Orthop Relat Res. 2001; 392:306-314.
11. Howard JL, Kudera J, Lewallen DG, Hanssen AD. Early results of the use of tantalum fem-oral cones for revision total knee arthroplasty. J Bone Joint Surg Am. 2011; 93(5):478-484.
12. Ghazavi MT, Stockley I, Yee G, Davis A, Gross AE. Reconstruction of massive bone defects with allograft in revision total knee arthroplasty. J Bone Joint Surg Am. 1997; 79(1):17-25.
13. Engh GA, Ammeen DJ. Use of structural al-lograft in revision total knee arthroplasty in knees with severe tibial bone loss. J Bone Joint Surg Am. 2007; 89(12):2640-2647.
14. Dorr LD, Ranawat CS, Sculco TA, McK-askill B, Orisek BS. Bone graft for tibial defects in total knee arthroplasty. 1986. Clin Orthop Relat Res. 2006; 446:4-9.
15. Clatworthy MG, Ballance J, Brick GW, Chandler HP, Gross AE. The use of structural allograft for uncontained defects in revision total knee arthroplasty: a minimum five-year review. J Bone Joint Surg Am. 2001; 83(3):404-411.
16. Bauman RD, Lewallen DG, Hanssen AD. Limitations of structural allograft in revision total knee arthroplasty. Clin Orthop Relat Res. 2009; 467(3):818-824.
17. Alexander GE, Bernasek TL, Crank RL, Haidukewych GJ. Cementless metaphyseal sleeves used for large tibial defects in revi-sion total knee arthroplasty. J Arthroplasty. 2013; 28(4):604-607.
18. Ewald FC. The Knee Society total knee ar-throplasty roentgenographic evaluation and scoring system. Clin Orthop Relat Res. 1989; 248:9-12.
19. Mulhall KJ, Ghomrawi HM, Engh GA, Clark CR, Lotke P, Saleh KJ. Radiographic predic-tion of intraoperative bone loss in knee ar-throplasty revision. Clin Orthop Relat Res. 2006; 446:51-58.
e809


![WELCOME [arthroplasty-conference.org]arthroplasty-conference.org/pdf/(IAC-2020)ARTHROPLASTY-PROGRA… · KEYNOTE LECTURERS: Wael Barsoum President of Cleveland Clinic, Florida, USA](https://img.pdfslide.net/doc/110x75/5edc4a09ad6a402d6666e51c/welcome-arthroplasty-arthroplasty-iac-2020arthroplasty-progra-keynote-lecturers.jpg)