Embed Size (px)
Citation preview
Rheumatic heart disease (RHD)
By : Dr. Sanjeev
Rheumatic heart disease The sequelae of rheumatic fever consist of
mitral, aortic and tricuspid valve disease The mitral valve involvement manifests
predominantly as mitral regurgitation and less common as mitral stenosis
The aortic and tricuspid valve involvement presents exclusively as aortic and tricuspid regurgitation
Rheumatic aortic stenosis has never been described below the age of 15 years.
Terms Regurgitation : results from failure of a
valve to close completely, thereby allowing reversed flow
Stenosis : failure of a valve to open completely, thereby impeding forward flow
Pure : only stenosis or regurgitation is present
Mixed : both stenosis and regurgitation coexist in the same valve, but one of these defects usually predominates
Heart sounds First heart sound : when AV valve
closed (mitral and tricuspid) Second heart sound : pulmonary
and aortic valve closed Third heart sound: increase volume
of blood within the ventricle Fourth heart sound : just after
atrial contraction at the end of diastole and immediately before S1.
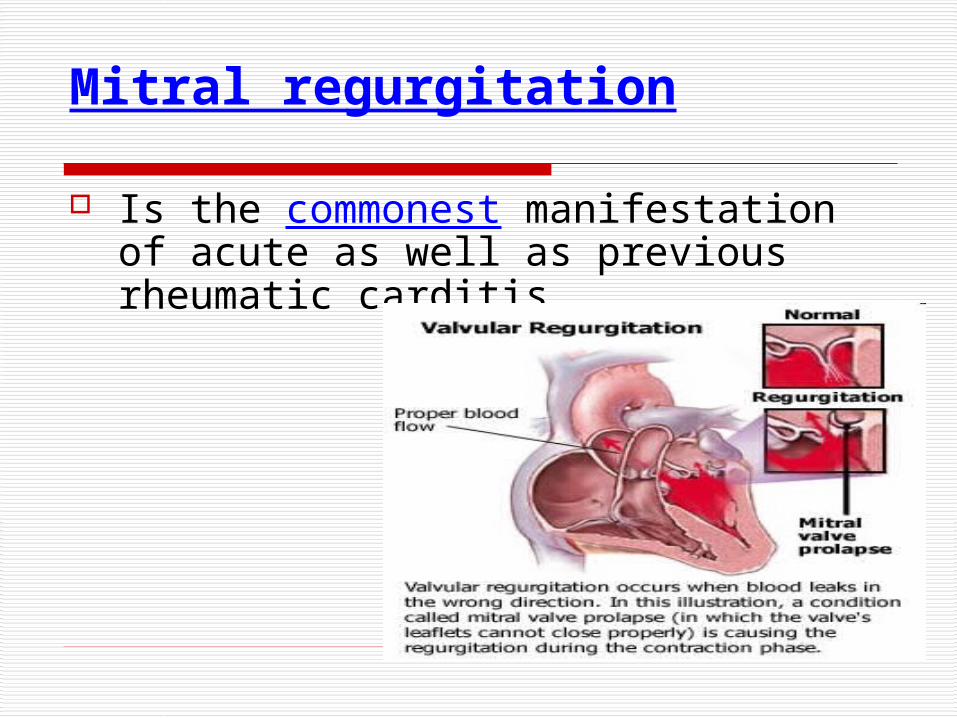
Mitral regurgitation
Is the commonest manifestation of acute as well as previous rheumatic carditis
Hemodynamics When mitral regurgitation is present -----
blood leaks backwards through the mitral valve and into the left atrium when the heart contracts (systolic phase) --- regurgitant volume of blood reaches the left atrium during ventricular systole, however, during diastole it can pass freely across the mitral valve ---- thus, mean atrial pressure = normal or is only slightly increased (because left atrial pressure increases during systole, it drops during diastole) ---- there is thus no increase in pulmonary venous pressure and no pulmonary congestion --------
Cont… ---- the increased volume of blood handled by the
left atrium and left ventricle results in an increase in the size of both these chambers -- Mitral regurgitation provides two exits for the left ventricular blood flow -- the forward flow through the aortic valve into the systemic circulation and the backward leak into the left atrium -- the forward output becomes insufficient during exertion -- this decrease in the systemic output results in fatigue, the commonest symptom of significant MR -- absence of pulmonary congestion prevents occurrence of dyspnea unless the MR is severe or the left ventricular myocardium is failing ----
Cont… With failing left ventricle, the left ventricular diastolic
pressure increases, the left atrial and pulmonary venous pressure increases and pulmonary congestion appears -- there is an increase in pulmonary arterial pressure and features of pulmonary arterial hypertension appear.
Presence of features of pulmonary arterial hypertension in a patient having pure MR suggests : 1. severe MR or 2. failing left ventricular myocardium, or 3. acute MR
Cont… MR developing during acute RF is of sudden onset. In
addition there is active myocarditis resulting in poorly functioning left ventricular myocardium. Thus the left ventricular failure can occur even with relatively moderate leaks during the acute illness.
The size of the left atrium also plays significant role in MR
With acute MR the left atrial size is normal and the increased volume reaching the left atrium increases the left atrial and the pulmonary venous pressure, resulting in pulmonary congestion and feature of left ventricular failure

Cont…. In long standing MR the left atrium increases in
size to accommodate the regurgitant volume without increasing the left atrial pressure and features of LVF are absent.
Another adjustment consists of decrease in the systemic vascular resistance to help increase the forward flow.
R = P/Q
where R is the vascular resistance (fluid resistance), P is the pressure difference, and Q is the rate of blood flow through it.
Cont…
The maximum ejection of blood into the aorta takes place during early systole. The combination of these two factors results in an increased systolic and decreased diastolic pressure in the systemic circuit . The pulse pressure is, therefore, increased resulting in the small water hammer pulse of MR
Aetiology
Dilatation of valve ring (Acute rheumatic fever, Cardiomyopathy)
Damage to the valve cusp and chordae (Rheumatic heart disease, Infective Endocarditis)
Damage to the papillary muscle (myocardial ischaemia , infarction)
Mitral valve prolapse (congenital, degenerative, connective tissue disease such as Marfan’s syndrome).
Trauma — Chest trauma can rarely cause breakage of the
chords that hold the mitral leaflets in their normal position. Untethered leaflets swing widely, allowing valve leakage.
Clinical featuresClinical features 1. Fatigue : when cardiac output starts to fall 2. Dysponea : when pulmonary venous
hypertension occurs, dysponea on exertion, orthopnea and paroxysmal nocturnal dysponea (PND) may ocuur
3. Pulse rate increased to maintain an adequate cardiac output
4. Features of left ventricular failure are absent and appear late unless the mitral regurgitation is acute, severe or left ventricular myocardium is failing
Cont.. 5. Heart size is dependent on the severity of MR as
well as the status of the left ventricular myocardium. 6. Apex beat is shifted down and out, farther than the
normal position, due to ventricular dilatation 7. Systolic thrill (<10 %) due to the direction of the
regurgitant stream which is backwards into the left atrium
8. Systolic murmur is heard over the cardiac apex (mitral area) with following characteristic : - 1. Pansystolic murmur extending from s1 to s2 2.High frequency murmur (diaphragm) 3. murmur radiates towards the left axilla and to the
back below the scapula
Cont… 9. First heart sound may be normal or
diminished in intensity 10. Severe MR, when a large amount of
blood flows downs suddenly from the left atrium to the left ventricle during diastole, a third sound (s3) or ventricular gallop is produced. Immediately after such a third sound, a short mid diastolic murmur may also be heard.
InvestigationsInvestigations
Chest X-Ray:
ECG
Echocardiography
Doppler
Cardiac catheterization
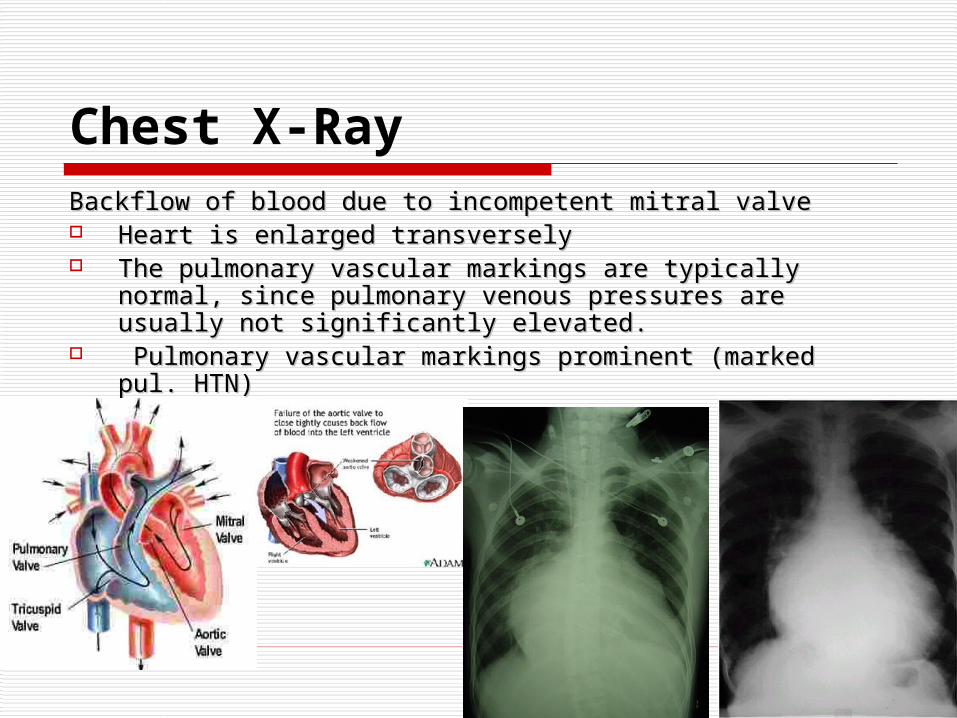
Chest X-RayBackflow of blood due to incompetent mitral valveBackflow of blood due to incompetent mitral valve Heart is enlarged transverselyHeart is enlarged transversely The pulmonary vascular markings are typically normal, The pulmonary vascular markings are typically normal,
since pulmonary venous pressures are usually not since pulmonary venous pressures are usually not significantly elevated.significantly elevated.
Pulmonary vascular markings prominent (marked pul. HTN)Pulmonary vascular markings prominent (marked pul. HTN)
Cont… ECG: Atrial fibrillation, left atrial
enlargement (if patient is in sinus rhythm). left ventricular hypertrophy can be seen
Echocardiography: Images mitral valve, left ventricular function and left atrial size. LA and LV will be dilated.
Doppler will quantify regurgitation Cardiac catheterization can be done for
pressure measurements
Differential diagnosis :-
Atrial septal defect Coarctation of aorta with MR
(congenital) Left ventricular fibroelastosis Myocarditis
Management : -Management : -
Medical Management : Low sodium diet Diuretics (patient with orthopnoea and
PND) Vasodilator: Sodium Nitroprusside or
Nitroglycerine may be used in acute and/or severe MR.
ACE inhibitors are used for treatment of chronic MR (decreased the after load).
Cont… Digoxin is used for patients with atrial
fibrillation or associated left ventricular failure. Anticoagulant for patients with atrial fibrillation,
for prevention of thromboembolism and who already developed features of systemic embolization to prevent further embolization.
Infective Endocarditis prophylaxis. Prophylaxis for Rheumatic fever if MR is of
rheumatic origin.
Cont…Surgical Management : Symptomatic patients despite optimal
medical therapy Asymptomatic or mildly symptomatic
patient in presence of progressive LV dysfunction.
Mitral valve repair (Annuloplasty with valve Reconstruction) can be done if valvular cusps and basic architecture is preserved.
Otherwise markedly deformed, with shrunken, calcified leaflets requires mitral valve replacement with a prosthesis.
Complications : Atrial fibrillation (in case of severe MR
and chronic long standing MR) Systemic embolization Infective endocarditis Congestive heart failure Pulmonary hypertension
Mitral stenosis Normal size: 5 sq. cmCardiac symptoms due to mitral stenosis start to
be appear only when the valve is reduced to 2 sq.cm
Severe stenosis < 1 cm2
Aetiology :• Acute RF with rheumatic endocarditis (99%)• Some due to calcification of senile mitral valve
apparatus• Congenital (very rare)
Pathophysiology : - Blood cannot flow freely from the left atrium to the left
ventricle during diastole -- left atrial pressure as well as volume increases --- increase in pressure and volume occurs in the pulmonary veins and capillaries --- when the pulmonary venous pressure exceeds the plasma oncotic pressure, fluid from the vessels flow out into the interstitial space and alveoli of the lungs --- leads to pulmonary arterial hypertension --- right ventricle has to work more during systole to push the blood into the pulmonary artery --- leads to right ventricular hypertrophy and later on to right ventricular dilatation -- if pulmonary HTN becomes severe, the amount of blood going to the left atrium from the right ventricle and pulmonary congestion tends to become less.
Clinical features : - Symptoms :
1. Dyspnoea (commonest symptom) : due to pulmonary venous congestion. Mild stenosis -dyspnoea occurs on exertion or when the
heart rate increases due to any reason. Severe stenosis -dyspnoea at rest May develop orthopnoea and PND
2. Cold extremities, with or without peripheral cyanosis and a smaller volume pulse -- decreased cadiac output in severe MS (recognized on the bed side)
Cont..
• 3. Fatigue (due to low cardiac output) • 4. Palpitation (Atrial fibrillation, Sinus
tachycardia)• 5. Haemoptysis (Pulmonary congestion,
Pulmonary embolism)• 6. Cough, chest pain• 7. Symptoms of Thromboembolism• 8. Oedema, ascites (right heart failure)

Signs• Irregularly irregular pulse (atrial fibrillation)
– Mitral facies (bluish pink hue over the malar prominences)
– Auscultation: Loud S1 , opening snap, mid diastolic murmur
– Signs of raised pulmonary capillary pressure: Basal crepitation, pulmonary oedema, and pleural effusion
– Signs of pulmonary hypertension: RV heave, loud P2
– Signs of right heart failure : E.g. Raised JVP, Hepatomegaly
– Signs of systemic Thromboembolism : E.g. Stroke, Acute limb ischaemia
Mitral FaciesMitral Facies
Investigations :
ECG : Atrial fibrillation,Left Atrial abnormality, Right ventricular enlargement
• Echocardiogram : Structural imaging of mitral valve, valve area, left atrial dimension, presence of thrombus in LA, pulmonary arterial pressure, RV dilatation.
3131Dr S Chakradhar Dr S Chakradhar
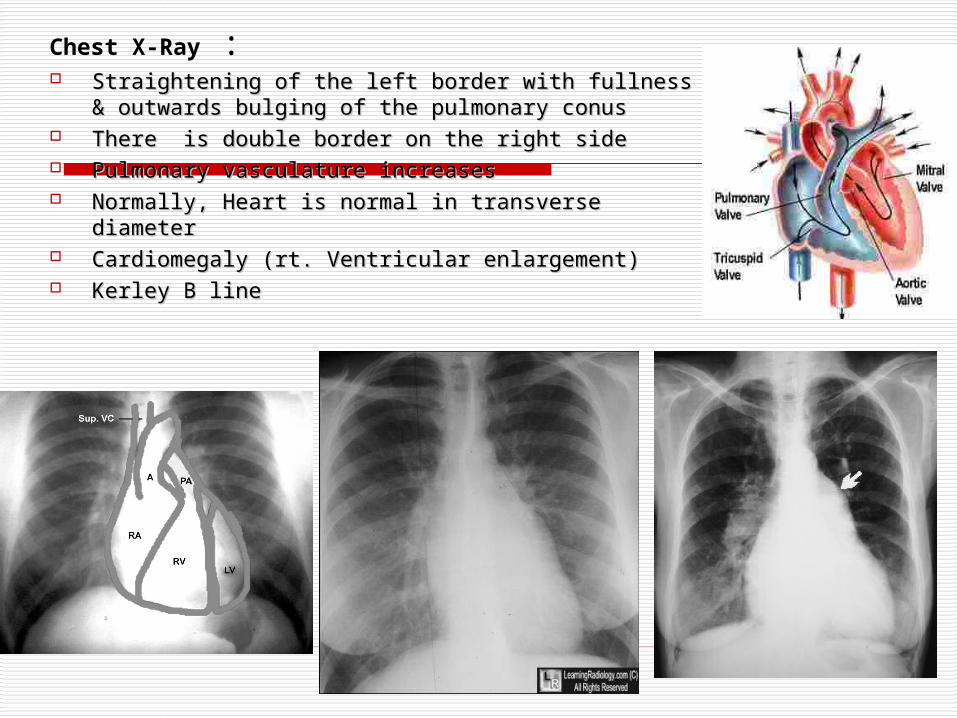
Chest X-Ray : Straightening of the left border with fullness & Straightening of the left border with fullness &
outwards bulging of the pulmonary conus outwards bulging of the pulmonary conus There is double border on the right sideThere is double border on the right side Pulmonary vasculature increases Pulmonary vasculature increases Normally, Heart is normal in transverse diameter Normally, Heart is normal in transverse diameter Cardiomegaly (rt. Ventricular enlargement)Cardiomegaly (rt. Ventricular enlargement) Kerley B lineKerley B line
ManagementManagement
1 . Medical management :• Penicillin prophylaxis for rheumatic fever.• Prophylaxis for infective endocarditis.• Low sodium intake, diuretics.• If patient is in Atrial fibrillation ---- use
digoxin low dose B-blocker.• Anticoagulation for at least 1 year for
patients who suffered Thromboembolism and permanently to those with AF.
2. Surgical management :
a. Mitral valvotomy : Symptomatic patients whose valve area is less
than 1.0 cm2/m2 body surface area. Two methods : 1. Percutaneous ballon mitral valvotomy and 2. Surgical valvotomy : Indicated in Re-stenosis ,
unsuccessful balloon valvotomy,. Restenosis is frequent. This procedure cannot be
done if there is significant regurgitation, calcification of the mitral valve or thrombus in left atrium.
b. Mitral valve replacement :
This is procedure of choice in : Critical mitral stenosis i.e. < 0.6 cm2/m2
body surface area Significant mitral regurgitation Calcified mitral valve leaflets
Complications
Atrial fibrillation Systemic emboli Pulmonary hypertension and Heart failure
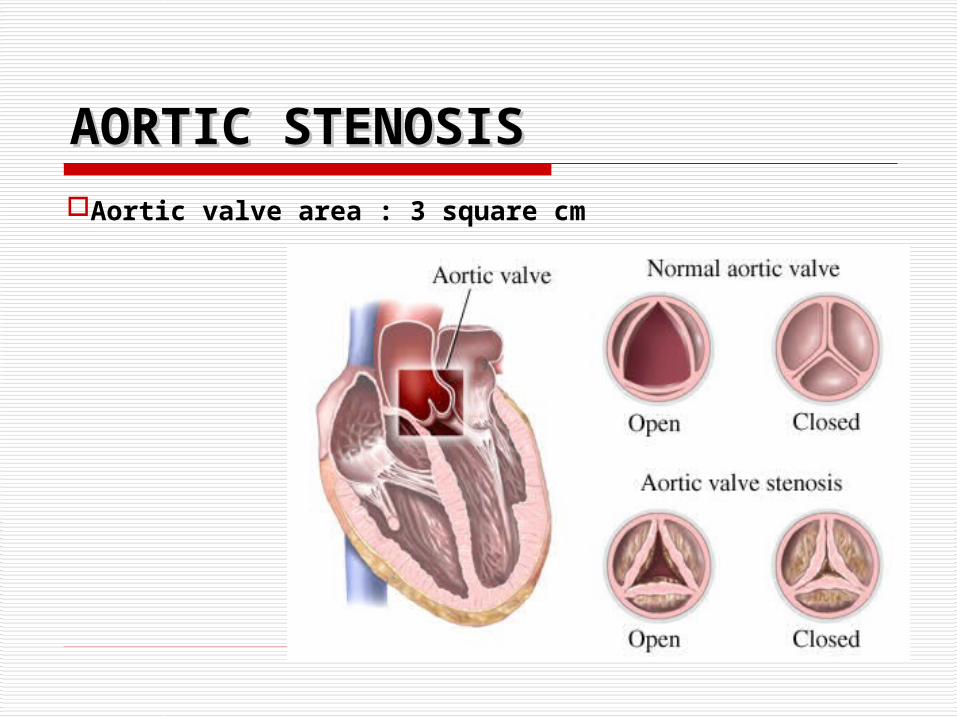
AORTIC STENOSISAORTIC STENOSISAortic valve area : 3 square cm
Aetiology :
Infants ,children, adolescents Congenital
1. Valvular aortic stenosis2. Subvalvular aortic stenosis3. Supravalvular aortic stenosis

Cont…
Young adults to middle aged Calcification and fibrosis of bicuspid
aortic valve Acute rheumatic fever with
endocarditis

Pathophysiology : - When it gets narrowed, left ventricle has to pump harder to
send blood across the narrowed aortic valve into the aorta - increased work load -left ventricular hypertrophy - hypertrophied ventricle manages to maintain the cardiac output inspite of stenosis - during atrial systole, plenty of blood comes to the left ventricle (atrial kick) - left ventricle becomes more stretched due to such atrial kicks and as per Frank Starling`s law, it now contracts more vigorously and thus more blood goes out of the ventricle into the aorta - gradually , the oxygen demand of the left ventricle increases - cause angina and sudden death - if left ventricle is overworked for prolonged period - LVF - aorta blood will be less -left ventricular end diastolic pressure and diastolic volume start to rise -left arterial and pulmonary venous pressure increases and the patient starts to feel dyspnoeic ( pulmonary congestion and hypertension)

Clinical features : -Clinical features : - Mild or moderate ----- Asymptomatic Cardinal symptoms like (1, 2, and 3)1. Exertional dyspnoea (signs of LVF):- initially exertional
dyspnoea later PND. 2. Angina3. Syncope : due to inadequate blood flow through the
stenosed aortic valve and arrhythmia.4. Fatigue and palpitation5. Apex beat : heaving or forceful and sustained type
(finger lifted up during systole, remains up for sometime and then falls down

Cont…
6. Auscultation : three main signs : Aortic ejection sound or click : heard over the
cardiac apex by the diaphragm, in early systole, immediately after the first sound.
Aortic ejection murmur : mid systolic murmur, heard over the right 2nd intercostal space by the side of the sternum, radiates to the neck towards both the carotids, and also called diamond shaped ejection systolic murmur.
Aortic component of the second sound is either late or soft

Cont… 7. Fourth heart sound : due to increased
stiffness of the left ventricle, the atrium contracts vigorously during atrial systole and pushes the a large amount of blood into the left ventricle, due to such strong ` atrial kick`, S4 becomes audible. It is a soft and low pitched sound and is heard just before S1. best heard over the cardiac apex by using the bell of the stethoscope.

Investigations : -Investigations : -
ECG: may show LV hypertrophy and ST depression and T wave inversion; left bundle branch block is common;
Chest X-Ray : may show LV enlargement in PA view and calcification of aortic valve in lateral view.
Echocardiography : will show abnormal aortic valve with left ventricular hypertrophy or dilatation.
Doppler echocardiography : will estimate the pressure gradient

enlargement of the ascending aorta(white arrow). left ventricle is enlarged (red arrow) and the heart is mildly enlarged overall. The lateral view on the right demonstrates calcifications in the region of the aortic valve leaflets (circle). generally, the aortic valve lies above a line drawn from the carina to the junction of the diaphragm with the anterior chest wall. The mitral valve lies below the line.

ManagementManagement Strenuous physical activity should be
avoided Sodium restriction, digitalis and diuretics
are used if there is heart failure. Vasodilators should be avoided or used with
extreme caution. Asymptomatic stenosis in elderly
conservative management is appropriate

Valve replacement in :
1. Patients with calcified AS with critical obstruction (valve area <0.5 cm2/m2 BSA).
2. Patients with symptomatic aortic stenosis (moderate to severe stenosis) even with normal cardiac output at rest.
3. Patients who exhibit LV dysfunction even they are asymptomatic.

Cont…• Penicillin prophylaxis for rheumatic
fever.• Prophylaxis for infective endocarditis.

Complications
Endocarditis Cardiac arrhythmias : atrial
fibrillation, ventricular arrhythmias, complete heart block
Left ventricular failure

Differential diagnosis
Hypertrophic cardiomyopathy Innocent systolic murmur eg. In
anemia, thyrotoxicosis Hypertension

AORTIC REGURGITATIONAORTIC REGURGITATION

Definition When the aortic valve is damaged
and cannot close completely during diastole, blood from the aorta regurgitates into the left ventricle, such a state is called AR.
Clinically pure aortic regurgitation – without associated mitral valve disease – is rare and occurs in 5 – 8 % patients

Pathophysiology : Blood regurgitates from the aorta into the
left ventricle during diastole -amount of blood regurgitating into the left ventricle depends upon :
1. size of the regurgitant hole in the aortic valve *
2. pressure gradiant between the aorta and the left ventricle during diastole
3. duration of the diastole

Cont… When blood regurgitates from the aorta into the left
ventricle during diastole it starts to dilate - hypertrophy of left ventricle - with progessive increase in the amount of regurgitant blood, the left ventriclar muscle fibre gets stretched further and as per Frank starling`s law, these fibres contract more vigorously, thereby increasing the stroke volume - but when the left ventricle is dilated too much and for a long period, its capacity to contract starts to decreased - stroke volume also decreases and the volume overload in the left ventricle increases further during diastole - peripheral vasodilation - hands and feet are warm and diastolic pressure is very low (not clear why there is peripheral vasodilation) -

Cont… later, when ventricular failure occurs, neuro
– hormonal activation leading to an increase in sympathetic vasoconstriction tone and increased intrinsic vascular stiffness and fall in cardiac output ---- when AR develops suddenly -- the left ventricular myocardium is failing and the left ventricular end diastolic pressure goes up - increase in left atrial pressure and pulmonary congestion.

Clinical features : -Clinical features : - 1. Palpitation (main symptom) : due to
increased force of contraction of the left ventricle
2. Dyspnoea, orthopnoea and PND 3. Sweating a lot when congestive failure
develops 4. Anigna pectoris due to :
1. low aortic diastolic pressure, due to which coronary blood flow is reduced
2. increase in oxygen demand of the left ventricle as a result of left ventricular dilatation and hypertrophy

Cont…. 5. Peripheral physical signs of aortic insufficiency are
related to the high pulse pressure and the rapid decrease in blood pressure during diastole due to blood returning to the heart from the aorta through the incompetent aortic valve :- 1. large-volume, 'collapsing' pulse also known as: Watson's water hammer pulse or Corrigan's pulse (rapid
upstroke and collapse of the carotid artery pulse) 2. De Musset's sign (head nodding in time with the heart
beat) 3. Quincke's sign (pulsation of the capillary bed in the nail) 4. Hill's sign (a ≥ 20 mmHg difference in popliteal and
brachial systolic cuff pressures)

Cont…. 5. Müller's sign (pulsations of uvula) 6. Traube's sign - two sound heard over femoral
arteries 7. Duroziez sign - Systolic-diastolic murmur produced
by compression of femoral artery with a stethoscope 8. Pistol shot - Loud systolic sound over femoral
arteries 9. Gerhardt's sign (enlarged spleen and pulsation felt
over the spleen) 10. Rosenbach's sign (pulsatile liver) 11. Landolfi's sign (alternating constriction &
dilatation of pupil)

Cont.. 6. cardiomegaly (inspection and palpation) : apex
beat shifted further down and out and is forceful and ill sustained (or hyperdynamic) in character.
Auscultation : 1. First and second heart sound both are normal 2. Third heart sound or ventricle gallop (severe AR)
due to large amount of blood suddenly coming to the left ventricle from the mitral and aortic valves during early diastole. Important sign in AR is early diastolic murmur : high frequency murmur, an early diastolic murmur, decrescendo murmur and best heard over the left side of the mid sternum over the second aortic area

Cont…
Many patients of AR have a mid diastolic rumbling murmur at the apex, as in MS, such murmur is called Austin Flint murmur -- when the blood regurgitates from the aorta into the left ventricle in AR, the regurgitant flow strikes the anterior leaflet of the mitral valve and gives rise to the Austin Flint murmur .

InvestigationsInvestigations
ECG: may show LV hypertrophy and ST depression and T wave inversion
Chest X-ray: may show cardiac and aortic dilatation. There may be features of left heart failure.
Echocardiogram: dilated LV with vigorous contraction. Vegetation may be visible if cause is infective endocarditis. There may be fluttering of AML (Anterior mitral leaflet)

ManagementManagement
Remove the treatable cause like infective endocarditis, Rheumatic fever
Medical therapy: low sodium diet, diuretics, and ACE inhibitors.
Surgery is advised if there is progressive LV dysfunction even when patient is asymptomatic or with mild symptoms.











![[PPT]RHEUMATIC HEART DISEASE · Web viewRHEUMATIC HEART DISEASE Rheumatic Heart Disease is a Notifiable disease Please contact the RHD register Central Australia Ph: 08 895 16909](https://img.pdfslide.net/doc/110x75/5acb00077f8b9acb7c8ea1d8/pptrheumatic-heart-viewrheumatic-heart-disease-rheumatic-heart-disease-is-a-notifiable.jpg)