Embed Size (px)
Citation preview

Thorax 1983;38:436-442
Right ventricular hypertrophy in a group ofcoalworkersJUNE M FERNIE, AN DOUGLAS, D LAMB, V ANNE RUCKLEY
From the Institute of Occupational Medicine, Edinburgh, and the Department of Pathology, University ofEdinburgh
ABSTRACr The prevalence of right ventricular hypertrophy was studied in necropsy material from215 coalworkers, a group which consisted of 115 men with simple or no pneumoconiosis and 100with progressive massive fibrosis. Right ventricular hypertrophy was considered to be present ifthe ratio of the weight of the left ventricle plus septum to that of the right ventricle was less than2:1. The prevalence of right ventricular hypertrophy was low (15%) in the absence of progressivemassive fibrosis and appeared to be related to emphysema or airways disease or both, and not tosimple pneumoconiosis. It was evident only in subjects who had smoked. In subjects with pro-gressive massive fibrosis the prevalence of right ventricular hypertrophy was higher (34%) and itwas occasionally seen in non-smokers. The prevalence increased with increasing size of lesion,and for any given size of lesion subjects with right ventricular hypertrophy had more panacinaremphysema than those without right ventricular hypertrophy. There was no relationship, how-ever, between the extent of massive lesions or amount and type of emphysema and the degree ofright ventricular hypertrophy.
Chronic airflow obstruction due to intrinsic airwaysdisease and emphysema is the most frequent causeof cor pulmonale, a term conventionally applied toright ventricular hypertrophy secondary to struc-tural or functional abnormality of the lung.'
In a study of coalworkers Gough found that com-plicated pneumoconiosis alone could be associatedwith cor pulmonale and suggested that this was dueto the destruction of large areas of the pulmonaryvascular bed resulting in pulmonary hypertension.2Simple pneumoconiosis, however, rarely gives riseto pulmonary hypertension in the absence of con-comitant obstructive lung disease or tuberculousscarring,23 although exceptions have been noted.4As emphysema and airways disease are found inconjunction with complicated pneumoconiosis it isdifficult to determine whether the cor pulmonale isdue to the industrial lung disease or to the airwaysdisease and emphysema, which may not be associ-ated with the dusty occupation.The aim of the present study was to verify obser-
vations of the prevalence of right ventricular hyper-trophy in coalworkers with simple or no
Address for reprint requests: June M Femie, Institute of Occupa-tional Medicine, 8 Roxburgh Place, Edinburgh EH8 9SU.
Accepted 8 February 1983436
pneumoconiosis. In addition, in these coalworkersand in coalworkers with complicated pneumo-coniosis the associations between right ventricularhypertrophy and the size of the massive lesion(where present), type and extent of emphysema,indicators of airways disease, and smoking habitwere investigated.
Methods
THE SUBJECTSThe study was carried out on the hearts and lungs of345 coalworkers who during life had taken part inthe pneumoconiosis field research5 of the NationalCoal Board. That research was based on 25 col-lieries selected as typical of the variety of under-ground conditions in British coalmines and com-prised surveys of all coalworkers in these collieriesat intervals of four to six years. Each survey includedchest radiography, pulmonary function testing,administration of a respiratory symptoms question-naire, and the taking of an occupational history.The 345 coalworkers form a subgroup of the 500
subjects examined in a necropsy study of coal-miners' lungs.67 Hearts were not available or wereunsuitable for dissection for the remaining 155 sub-jects.
on 25 May 2019 by guest. P
rotected by copyright.http://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.38.6.436 on 1 June 1983. D
ownloaded from

Right ventricular hypertrophy in a group of coalworkers
The main source of the material was thepneumoconiosis medical panels and thus subjectswere somewhat biased towards those with estab-lished disease. Nevertheless, some subjects with noradiographic evidence of coalworkers' pneumo-coniosis were obtained.
HEART EXAMINATIONHearts were dissected according to the method ofLamb8 based on the technique of Fulton et al.9Afterdissection the right ventricle (RV) and the left ven-tricle plus septum (LV + S) were weighed sepa-rately. The ratio of the weight of the LV + S to thatof the RV is considered to provide the most appro-priate method of assessing ventricular hypertro-phyl8 and in the present study a ratio of (LV +S):RV of less than 2:1 was taken as indicating indis-putable right ventricular hypertrophy.A subject was excluded from the study if on dis-
section of the heart any valvular abnormality or pre-vious myocardial damage (as shown by focal scar-ring measuring more than 1 cm in any plane) wasapparent (n = 66) or if the isolated LV + S weighed225 g or more (n = 51). A further 13 subjects wereexcluded for both reasons. Some subjects known tohave had systemic hypertension were included in theabsence of left ventricular hypertrophy since infor-mation about blood pressure was available for only aproportion of subjects and at varying times beforedeath. Application of these selection factors resultedin a total loss of 130 subjects, leaving 215 availablefor analysis.
LUNG EXAMINATIONLungs were inflated at necropsy; the pressures andduration of inflation were not known.
Transverse blocks from the lower-lobe bronchi,shown to be representative of the major bronchi,7were taken, embedded in paraffin, and sectioned at8 ,um. Weigart's elastic stain and a Van Giesoncounterstain were used. The mean bronchial gland-to-wall thickness ratio'0 was used to estimate thedegree of mucous gland enlargement.
In general, the lungs had been cut in some way atnecropsy. Slicing was completed, usually in the sagit-tal plane, at 1-cm intervals and a representativeslice was chosen for assessment from each of the pairof lungs. Initially subjects were divided into threepathological groups as follows: M-subjects inwhom all dust lesions were macules; F-subjects inwhom one or more fibrotic lesions with a minimumdiameter of 1 mm was present; and PMF (progres-sive massive fibrosis)-subjects in whom one ormore fibrotic lesions with a minimum diameter of 1cm was present.
Pathological groups M and F bear some relation
to the radiological categories of simplepneumoconiosis in that, on average, 83% of M sub-jects will be in category 0/0. In contrast, 70% of Fsubjects will show opacities typical of simplepneumoconiosis.Emphysema was defined as the presence of air
spaces of 1 mm or more in size and three main typeswere recognised. Centriacinar emphysema refers toany circumscribed emphysema separated from otherlesions and from the interlobular septa by normalalveolar tissue, however small in area this may be.Panacinar emphysema refers to emphysema affect-ing all air spaces within an anatomical lung lobule,and paraseptal emphysema is emphysema occurringagainst the interlobular septa, subpleurally or inrelation to the larger bronchi and blood vessels.For assessment of emphysema and lesions of
progressive massive fibrosis lung slices were dividedinto six zones as described by Heard." In non-PMFlungs the amount of emphysema in each of the sixzones was estimated on a scale of 0-5 (according tothe number of fifths of the zone affected); this gave atotal emphysema count expressed as thirtieths of thelung slice. Within each zone a visual assessment wasthen made of the relative contribution of the threetypes of emphysema (centriacinar, panacinar, andparaseptal) to the emphysema estimate for thatzone. This enabled a division to be made of the totalemphysema count into counts for each type.Although recorded, counts of paraseptalemphysema were not included in any analyses as theamounts present were usually negligible.
In PMF lungs the extent of the massive lesion orlesions in each zone was estimated on a scale of 0-5,the total PMF area count being expressed as thir-tieths of the lung slice.The method of estimating emphysema was modi-
fied slightly for PMF lungs to take into account areasof lung tissue destroyed by massive fibrosis. Thus theamount of emphysema was expressed not as a countout of 30 but as a count out of 30 minus the totalPMF area count; for example, given a total PMFarea count of 8/30 the amount of emphysema wouldbe expressed as a count out of 22. Counts ofemphysema were then recalculated and expressed asthe equivalent number of thirtieths of lung affectedto allow comparison with non-PMF lungs.Where both lungs had PMF area or emphysema
estimates, or both, the average was used; otherwiseestimates from a single lung were taken to representthe pair since in our experience estimates ofemphysema or area of PMF lesions did not differappreciably between left and right lungs. Subjectswith unilateral PMF are an exception to this, but 30of the 33 subjects with unilateral PMF included inthe study had complete data for both lungs. One
437
on 25 May 2019 by guest. P
rotected by copyright.http://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.38.6.436 on 1 June 1983. D
ownloaded from

438
subject had no PMF area or emphysema data and inthe two remaining subjects, both with a small unilat-eral lesion, the emphysema estimate used was thatof the lung with the PMF lesion.
RADIOGRAPHSChest radiographs taken within four years of deathwere available for 128 of the 215 subjects. Theseradiographs were obtained from thepneumoconiosis medical panels, hospitals, or thepneumoconiosis field research surveys and were
read according to the 1971 ILO U/C classification.'2For each subject the reading used was the average ofthe readings given by four National Coal Boarddoctors.6
PULMONARY FUNCTION DATAOf the 215 subjects studied, 70 had had measure-
ments of forced expiratory volume in one second(FEVy) and forced vital capacity (FVC) taken withinfive years of death. These 70 subjects were represen-
tative of the 215 in terms of mean emphysemacounts and bronchial gland-to-wall thickness ratios.The data were obtained from the pneumoconiosismedical panels or the pneumoconiosis field researchsurveys. As proportionately fewer of the subjects(non-PMF and PMF) with right ventricular hyper-trophy had FEV, measurements taken within fiveyears of death we decided to supplement the data inthese groups by including, for comment only, meas-
urements taken more than five years before death.The FEV, measurements were expressed as a per-
centage of the predicted values for age and height'3(FEV%) and these values were used as indicators ofthe degree of airflow obstruction present.Although FEV, may be reduced in restrictive as
well as obstructive lung disease it was apparent froman examination of the FVC% (FVC percentage ofpredicted value) and FEV,:FVC ratios of the 70subjects that obstructive lung disease was the pre-dominant type.
SMOKING HISTORIESMost of the smoking histories were obtained fromthe pneumoconiosis field research questionnaire
Table 1 Prevalence ofright ventricular hypertrophy(RVH) in three pathological groups
Pathological groups* Total
M F PMF
No of subjects with RVH 6 11 34 51Total No of subjects 39 76 100 215Prevalence of RVH (%) 15-4 14-5 34 23-7
*See text under "Methods-Lung examination" for definition ofthe groups.
Fernie, Douglas, Lamb, Ruckley
data supplemented by panel records. There wasgood agreement between the two sources. Smokinghistories were obtained for 204 of the 215 subjects,who were divided into three groups: smokers, ex-smokers, and life-long non-smokers.
Results
-RIGHT VENTRICULAR HYPERTROPHY INNON-PMF SUBJECTSAssociation with pneumoconiosisA total of 17 of the 115 non-PMF (M + F) subjectsshowed right ventricular hypertrophy and the pro-portions of M and F subjects with right ventricularhypertrophy were similar (table 1).
Chest radiographs taken within four years ofdeath were available for 63 of the 115 subjects.Right ventricular hypertrophy was present in 18%of the 28 subjects in category 0/0 and 17% of the 35in category 0/1 or above.
Association with emphysema, airways disease, andsmoking habitEmphysema was present in all 17 of the non-PMFsubjects with right ventricular hypertrophy, and as a.group those with right ventricular hypertrophy hadsignificantly more emphysema (p < 0-001, Student'st test) than those without.Among the subjects for whom data on centn-
acinar and panacinar emphysema were available,counts of both types were significantly increased (p< 0-001, Student's t test) in subjects with right ven-tricular hypertrophy (table 2).The pathological counterpart of the mucus
hypersecretion typical of chronic bronchitis isenlargement of the bronchial mucous glands. In thenon-PMF subjects there was no difference in themean bronchial gland-to-wall thickness ratio be-t-ween subjects with and without right ventricularhypertrophy.
All four of the subjects with right ventricularhypertrophy for whom recent FEV, data were avail-able had airways obstruction with an FEV% (FEVy
Table 2 Emphysema counts (means + SD) in 102non-PMF* subjects, with and without right ventricularhypertrophy (RVH), for whom data were available on thetype ofemphysema
RVH Emphysema countst
Total Centriacinar Panacinar
Present (n = 14) 8-5 + 3-9 3-6 + 1-7 4.7 + 3-6Absent (n = 88) 2-9 ± 4-1 1-5 + 2-1 1-3 + 3-0
*Progressive massive fibrosis-see under "Methods-Lungexamination."tExpressed as thirtieths.
on 25 May 2019 by guest. P
rotected by copyright.http://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.38.6.436 on 1 June 1983. D
ownloaded from

Right ventricular hypertrophy in a group of coalworkers
percentage of predicted value) of 30% or less. Less
recent FEVI data were available for a further sixsubjects in this group. All but one of these. had an
FEV% of 50% or less. These low values were notmatched by the 30 non-PMF subjects without rightventricular hypertrophy, for whom the mean FEV%was 71%.An examination of smoking habit in the non-PMF
group showed that right ventricular-hypertrophy wasabsent in all eight non-smokers and rarely present inthe ex-smokers (table 3).
RIGHT VENTRICULAR HYPERTROPHY IN PMFSUBJECTSThe prevalence of right ventricular hypertrophy insubjects with PMF was 34%, significantly higher (p< 0.001, x2 test) than in non-PMF subjects (table1).Of the 100 PMF subjects studied, 85 had com-
plete -PMF area estimates, emphysema estimates,and bronchial gland-to-wall thickness ratios.
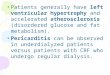
Association with extent of massive lesionWhen the 85 subjects were subdivided according tothe extent of PMF the prevalence of right ventricu-lar hypertrophy was seen -to be significantly -associ-ated (p < 0 001, x2 test) with the size of lesion. Insubjects with small PMF lesions (< 1/30) the pre-valence of right ventricular hypertrophy was thesame as in non-PMF -subjects, whereas in subjectswith lesions of greater than 10/30 the prevalence ofright ventricular hypertrophy was 83% (fig 1).
1001
0
I.
0
U-
z
-i
wiCZ
80-
60-
40-
20-
Table 3 Distribution ofsubjects with and withoutprogressive massive fibrosis (PMF) by smoking habit andpresence or absence ofright ventricular hypertrophy (RVH)
Smokitg habit; Non-RMF PMF
RVH RVH RVH RVHpresent absent present absent
Non-smoker - 8 2 5Ex-smoker 1 7 5 6Smoker 14 77 26 53Unknown 2 6 1 2
Association with emphysema, airways disease, andsmoking habitOf the 85 subjects with PMF, those with right ven-tricular hypertrophy had significantly more
emphysema than those without: this trend was simi-lar for each size grouping of PMF (table 4). The> 5-10 and > 10/30 PMF groups were combinedbecause of the small number of subjects in the lattergroup. When centriacinar and panacinar emphysemacounts were considered separately the increasedamount of emphysema in PMF subjects with rightventricular hypertrophy was due entirely to an
increased amount of panacinar emphysema. In the"all subjects" group, for example, the mean totalemphysema count of 8*6 in those with right ventricu-lar hypertrophy comprised 2-2 for centriacinar and6-1 for panacinar emphysema. In those subjectswithout right ventricular hypertrophy the mean totalemphysema count of 4-4 comprised 1-6 for centri-acinar and 2-5 for panacinar emphysema. The mean
6x
20x
Fig 1 Prevalence ofright ventricularhypertrophy in non-PMF and PMF subjectssubdivided by extent ofPMF (total numberofsubjects shown for each group).
32x
115 27x x
I I I I
0 < 1 1-5 >5-10 >10
PMF LESION AREA (thirtieths)
439
on 25 May 2019 by guest. P
rotected by copyright.http://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.38.6.436 on 1 June 1983. D
ownloaded from

Fernie, Douglas, Lamb, Ruckley
Table 4 Total emphysema counts (means ± SD) in 85subjects with progressive massive fibrosis (PMF), with andwithout right ventricular hypertrophy (RVH), subdivided byextent ofPMF
PMF Total emphysema count' ptarea count*
RVH present RVH absent
< 1 8-1 90 (4)t 3-2 45 (23) NS1-5 82 ±46 (9) 4-6+ 51 (23) NS> 5 89 7-9 (15) 63 5-4(11) NSAll subjects 8-6 + 73 (28) 4-4 49 (57) < 001
*Expressed as thirtieths.tProbability value (Student's t test).tNo of subjects in parentheses.NS-not significant.
centriacinar counts of the two groups were notsignificantly different but the mean panacinar countwas significantly increased (p < 0-01, Student's ttest) in those with right ventricular hypertrophy.As with the non-PMF subjects, there was no dif-
ference in the mean bronchial gland-to-wall thick-ness ratio of PMF subjects with and without rightventricular hypertrophy.FEV1 data obtained within five years of death
were available for 10 of the PMF subjects with rightventricular hypertrophy and 26 of those without.For these two groups the mean values of FEV,expressed as percentages of predicted values were54% and 69%. Although the difference was notsignificant (Student's t test), only 20% of those withright ventricular hypertrophy had FEV% values inwhat might be considered the normal range (FEV%> 80%), compared with 46% of those without rightventricular hypertrophy. Less recent FEV, datawere available for a further 22 of the PMF subjectswith right ventricular hypertrophy. These values
2. 0-
> 1.6-
+( 1.2-
-J-
° 0.8
0.4-
x
x
0x
x
showed the same distribution as the values obtainedwithin five years of death. Thus the FEV% values ofPMF subjects with right ventricular hypertrophy dif-fered considerably from those of the non-PMF sub-jects with right ventricular hypertrophy, althoughmean emphysema counts for the two groups weresimilar.When smoking habit was examined it was found
that right ventricular hypertrophy was present intwo of the seven non-smokers and in five of the 11ex-smokers in the PMF group (table 3).
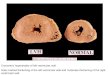
PMF SUBJECTS WITH RIGHT VENTRICULARHYPERTROPHYOf the 34 PMF subjects with right ventricular hyper-trophy, 28 had both PMF area data and completeemphysema data. In these subjects no relationshipcould be shown between the degree of right ven-tricular hypertrophy (that is, decreasing heartweight ratio) and the PMF lesion area (fig 2) or theextent and type of emphysema.
Discussion
The present study has shown no evidence that thereis an association between simple pneumoconiosisand right ventricular hypertrophy, the prevalence ofthe latter being the same in coalworkers with simplepneumoconiosis (defined in pathological orradiological terms) as in those with nopneumoconiosis. In these groups (the non-PMF sub-jects) the prevalence of right ventricular hyper-trophy was low (15%) and, where present, it wasassociated with evidence of severe airflow obstruc-tion during life. Similar findings have been reportedin other studies.23
x
x
x
0
x
x
x
x
x
Fig 2 Relationship between area ofPMFlesion and the heart:weight ratio in 28 PMFsubjects with right ventricular hypertrophy.0 indicates coincident points.
(r = 0.06)
I
2 4 6 8 10
PMF LESION AREA (thirtieths )
12 14I l--
440
x
on 25 May 2019 by guest. P
rotected by copyright.http://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.38.6.436 on 1 June 1983. D
ownloaded from

Right ventricular hypertrophy in a group of coalworkers
The possible causes of airflow obstruction andhence right ventricular hypertrophy are intrinsicairways disease and emphysema and in the non-PMF subjects there was evidence to suggest anassociation between emphysema and right ventricu-lar hypertrophy. Relationships between emphysemaand right ventricular hypertrophy have also beenobserved in miners and industrial workers withsilicosis'4 and in coalworkers in contact withbituminous coal.'5 Studies of right ventricular hyper-trophy in the general population,'6-24 however, haveresulted in a divergence of opinion concerning suchan association with disagreement, in particular,about whether the extent of emphysema and the sizeof the right ventricle are correlated and whether anyassociation applies to a specific type of emphysema.These disagreements are largely the result of differ-ent methods of assessing right ventricular hypertro-phy, one of which-the measurement of ventricularwall thickness-is considered to be unreliable.825Another contributing factor has been the tendencyof many workers to dismiss the fact that centriacinarand panacinar emphysema frequently coexist and toseparate individuals according to the predominanttype present. In the present study the types coexistbut are considered separately and the results haveshown that increased amounts of both centriacinarand panacinar emphysema are present in non-PMFsubjects with right ventricular hypertrophy. Theinterpretation of these results is somewhat difficult,however, as counts of centriacinar and panacinaremphysema are significantly correlated with thetotal emphysema count (r = 074 and 0.88 respec-tively) and also with each other (r = 0-35) in non-PMF subjects. For this reason it is impossible todetermine which, if either, of the two types isspecifically associated with right ventricular hyper-trophy. Some workers2022 have implicated centri-acinar and others23 24 panacinar emphysema.The absence, however, of right ventricular
hypertrophy in several subjects with gross emphy-sema, together with its presence in some with mildemphysema, precludes emphysema from being con-sidered the sole cause of right ventricular hypertro-phy in the non-PMF subjects and suggests that air-ways disease may also play a part. In fact, it has beenreported that in people dying of chronic obstructivelung disease right ventricular hypertrophy is gener-ally less noticeable or is altogether absent in thosewith extensive emphysema.26 The severity of theairflow obstruction seen in the non-PMF subjectswith right ventricular hypertrophy, some of whomhad minimal emphysema, is itself suggestive ofsevere airways disease.
In accord with other studies,2427 no relationshipcould be found between right ventricular hyper-
trophy and large airways disease as measured bybronchial mucous gland size.
It was interesting, but not altogether surprising, tofind that none of the non-smokers and few of theex-smokers in the non-PMF group had right ven-tricular hypertrophy. Cigarette smoking is known tobe associated with both emphysema and airflow ob-struction,2829 and these were common features ofthose subjects with right ventricular hypertrophy.When PMF is present the overall prevalence of
right ventricular hypertrophy is much higher, the34% found in the present study being similar to the44%30 and 42%3 previously reported. In this studythe prevalence of right ventricular hypertrophyincreased with the extent of massive fibrosis, whichis in accord with the report of an increased preval-ence of right ventricular hypertrophy with increasingdiameter of the largest PMF lesion.3' We have alsoshown that there is no direct quantitative relation-ship between extent of PMF and degree of rightventricular hypertrophy, which suggests that de-struction of the vascular bed by massive fibrosis isnot the sole cause of right ventricular hypertrophy inPMF subjects, but that other factors play a part.Again there was evidence for the role ofemphysema, specifically panacinar emphysema,which may reflect the fact that panacinaremphysema comprises a greater percentage of thetotal emphysema count in PMF subjects (64%) thanin non-PMF subjects (48%).
Right ventricular hypertrophy was present in fiveof the 11 ex-smokers in the PMF group and in twoof the seven non-smokers, both of whom had largePMF lesions; thus a greater percentage of the ex-smokers and non-smokers had right ventricularhypertrophy in the PMF group than in the non-PMFgroup. These differences were not, however,significant (exact test for 2 x 2 contingency tables),probably because of the small numbers of subjects.When we considered the PMF subjects individu-
ally, it seemed likely that in some cases right ven-tricular hypertrophy had developed simply throughdestruction of the vascular bed by massive fibrosis,whereas in others it was probably attributable toemphysema or severe airways disease or both. Thesewere the extreme cases, however, and probablymost subjects developed right ventricular hypertro-phy as a result of more than one process. It is note-worthy that some PMF subjects did not show rightventricular hypertrophy even when extensive PMFand severe emphysema were present. This lendsfurther support to the idea that there are otherfactors, specifically associated with chronic obstruc-tive lung disease, which may be more closely relatedto right ventricular hypertrophy. Relationshipsbetween right ventricular hypertrophy and
441
on 25 May 2019 by guest. P
rotected by copyright.http://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.38.6.436 on 1 June 1983. D
ownloaded from

442
disseminated bronchiolostenosis have already beenreported,3233 and in four subjects dying from chronicobstructive lung disease who had no emphysema corpulmonale was attributed to hypoxia.34 We realisethat these factors may show a closer association withright ventricular hypertpphy than those we studied.
We would like to thank the staff of thepneumoconiosis medical panels for supplying thenecropsy material and some of the chest radio-graphs, smoking histories, and pulmonary functiondata. We would also like to thank Miss SandraGauld for her statistical advice. The study wasjointly funded by the National Coal Board and theCommission of the European Communities.
References
1 World Health Organisation. Chronic cor pulmonale.Report of an expert committee (Geneva, 1960).Geneva: WHO, 1960. (Technical Report Series No213.)
2 Gough J. Pathological changes in the lungs associatedwith cor pulmonale. Bull NY Acad Med1965 ;41:927-41.
3Wells AL. Cor pulmonale in coalworkers'pneumoconiosis. Br Heart J 1954;16:74-8.
Ldapp NL, Seaton A, Kaplan KC, Hunsaker MR, MorganWKC. Pulmonary haemodynamics in coalworkers'pneumoconiosis. In: Walton WH, ed. Inhaled particlesIII. Old Woking, Surrey: Unwin Bros, 1971:645-56.
5Fay JWJ, Rae S. The Pneumoconiosis Field Research ofthe National Coal Board. Ann Occup Hyg1959;1: 149-61.
6 Davis JMG, Chapman J, Collings P, et al. Autopsystudies of coalminers' lungs. Edinburgh: Institute ofOccupational Medicine, 1979. (IOM Report TMI7919.)
Ruckley VA, Chapman JS, Collings PL, et al. Autopsystudies of coalminers' lungs-phase II. Edinburgh:Institute of Occupational Medicine, 1981. (IOMReport TM/81118.)
8 Lamb D. Heart weights and assessment of ventricularhypertrophy. In: Dyke SC, ed. Recent advances in clin-ical pathology. Series 6. Edinburgh: Churchill Living-stone, 1973:138-48.
9 Fulton RM, Hutchinson EC, Jones AM. Ventricularweight in cardiac hypertrophy. Br Heart J1952;14:413-20.
10 Reid L. Measurement of the bronchial mucous glandlayer: a diagnostic yardstick in chronic bronchitis.Thorax 1960;15:132-41.
Heard BE. Pathology of chronic bronchitis qndemphysema. London: J and A Churchill, 1969:11.
12 International Labour Office. ILO UIC internationalclassifiration of radiographs ofpneumoconioses, 1971.Geneva: ILO, 1972. (Occupational Safety and HealthSeries No 22.)
3 Cotes JE. Lung function. 4th ed. Oxford: Blackwell Sci-entific Publications, 1979:369.
4 Smidt U, Schnellbacher F. Right ventricular hypertro-phy, verified by autopsy, and symptoms of its
Fernie, Douglas, Lamb, Ruckley
development in patients with silicosis and coalworkers'pneumoconiosis. Prax Klin Pneumol 1978;32:407-16.
*s Naeye RL, Laqueur WA. Chronic cor pulmonale, itspathogenesis in Appalachian bituminous coalworkers.Arch Path 1970;90:487-93.
16 Burrows B, Fletcher CM, Heard BE, Jones NL, WootliffJS. The emphysematous and bronchial types of chronicairways obstruction. Lancet 1966;i:830-5.
17 Cromie JB. Correlation of anatomic pulmonaryemphysema and right ventricular hypertrophy. AmRev Respir Dis 1961;84:657-62.
18 Wyatt JP, Fischer VW, Sweet HC. The pathomorphol-ogy of the emphysema complex. Parts I and II. Am RevRespir Dis 1964;89:533-60.
19 Foraker AG, Bedrossian CWM, Anderson AE.Myocardial dimensions and.poportions in pulmonaryemphysema. Arch Path 1970;90:344-7.
20 Hicken P, Heath D, Brewer D. The relation between theweight of the right ventricle and the percent of abnor-mal air space in the lung in emphysema. J Pathol1966;92:519-46.
21 Hasleton PS. Right ventricular hypertrophy inemphysema. J Pathol 1973;110:27-36.
22 Dunnill MS. An assessment of the anatomical factor incor pulmonale and emphysema. J Clin Pathol1961;14:246-58.
23 Sweet HC, Wyatt JP, Fritsch AJ, Kinsella PW. Panlobu-lar and centrilobular emphysema. Correlation of clini-cal findings with pathological patterns. Ann Intern Med1961 ;55:565-81.
24 Scott KWM. A pathological study of the lungs and heartin fatal and non-fatal chronic airways obstruction.Thorax 1976;31:70-9.
25 Cullen JH, Kaemmerlen JT, Daoud A, Katz HL. Aprospective clinical-pathologic study of the lungs andheart in chronic obstructive lung disease. Am RevRespir Dis 1970;102:190-204.
26 Millard J. Pulmonary hypertension in chronic bronchitis.Thorax 1967;22:286 (abstract).
27 Dunnill MS. Morphometry of the human lung in healthand disease. In: Cumming G, Hunt LB, eds. Form andfunction in the human lung. Edinburgh: E and SLivingstone, 1968:24.
28 Fletcher C, Peto R, Tinker C, Speizer FE. The naturalhistory ofchronic bronchitis and emphysema. London:Oxford University Press, 1976.
29 Ryder RC, Dunnill MS, Anderson JA. A quantitativestudy of bronchial mucous gland volume, emphysemaand smoking in a necropsy population. J Pathol1971;104:59-71.
30 Coggin CB, Griggs DE, Stilson WL. The heart inpneumoconiosis. Am Heart J 1938;16:411-21.
31 James WRL, Thomas AJ. Cardiac hypertrophy in coal-workere pneumoconiosis. Br J Ind Med 1956;13:24-9.
32 Bignon , Khoury F, Even P, Andr6 J, Brouet (G. Mor-phometric study in chronic obstructive bronchopulmo-nary disease. Am Rev Respir Dis 1969;99:669-95.
33 Depierre A, Bignon J, Lebeau A, Brouet G. Quantita-tive study of parenchyma- and small conductive airwaysin chronic non-specific lung disease. Chest1972;62:699-708.
34 Hentel W, Longfield AN, Vincent TN, Filley GF, Mitch-ell RS. Fatal chronic bronchitis. Am Rev Respir Dis1963;87:216-27.
on 25 May 2019 by guest. P
rotected by copyright.http://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.38.6.436 on 1 June 1983. D
ownloaded from












![Hypertension Associated with Atherosclerosis Risk Factors ... · diabetes mellitus, left ventricular hypertrophy, psychosocial factorsbesides sy, s- tolic arterial hypertension [7]](https://img.pdfslide.net/doc/110x75/5d4edcdd88c99342288b9569/hypertension-associated-with-atherosclerosis-risk-factors-diabetes-mellitus.jpg)