Embed Size (px)
Citation preview
This article was downloaded by: [Flinders University of South Australia]On: 06 October 2014, At: 00:59Publisher: RoutledgeInforma Ltd Registered in England and Wales Registered Number: 1072954 Registeredoffice: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK
Counselling Psychology QuarterlyPublication details, including instructions for authors andsubscription information:http://www.tandfonline.com/loi/ccpq20
Road victim trauma: an investigationof the impact on the injured andbereavedNoreen Tehrani Dr, Managing Directora Assessment and Rehabilitation Consultants , Twickenham, UKPublished online: 22 Oct 2010.
To cite this article: Noreen Tehrani Dr, Managing Director (2004) Road victim trauma: aninvestigation of the impact on the injured and bereaved , Counselling Psychology Quarterly, 17:4,361-373, DOI: 10.1080/09515070412331331255
To link to this article: http://dx.doi.org/10.1080/09515070412331331255
PLEASE SCROLL DOWN FOR ARTICLE
Taylor & Francis makes every effort to ensure the accuracy of all the information (the“Content”) contained in the publications on our platform. However, Taylor & Francis,our agents, and our licensors make no representations or warranties whatsoever as tothe accuracy, completeness, or suitability for any purpose of the Content. Any opinionsand views expressed in this publication are the opinions and views of the authors,and are not the views of or endorsed by Taylor & Francis. The accuracy of the Contentshould not be relied upon and should be independently verified with primary sourcesof information. Taylor and Francis shall not be liable for any losses, actions, claims,proceedings, demands, costs, expenses, damages, and other liabilities whatsoeveror howsoever caused arising directly or indirectly in connection with, in relation to orarising out of the use of the Content.
This article may be used for research, teaching, and private study purposes. Anysubstantial or systematic reproduction, redistribution, reselling, loan, sub-licensing,systematic supply, or distribution in any form to anyone is expressly forbidden. Terms &Conditions of access and use can be found at http://www.tandfonline.com/page/terms-and-conditions
RESEARCH REPORT
Road Victim Trauma: aninvestigation of the impacton the injured and bereaved*
NOREEN TEHRANIAssessment and Rehabilitation Consultants, Twickenham, UK
abstract Every day in the United Kingdom ten people are killed and between 900 and
1,000 injured on the roads and, consequently, the health of large numbers of the victims, relatives
and friends are adversely affected. Yet despite the magnitude of the problem little has been done to
assess the full impact of road crashes on those involved, or to identify the best ways to provide help
and support. This paper describes the impact of road traffic incidents on a large group of injured
and bereaved victims, who approached Road Peace (a national charity for road traffic victims)
for support. The research that examined data collected over an eight-year period was able to
identify the nature of the impact of the traumatic exposure of these victims. The paper goes on to
examine the needs of the road crash victims and suggests ways that timely support and advice
could help to reduce the levels of distress.
Introduction
Until very recently little had been written about the psychological consequences of road
traffic crashes. Even today, the literature on the subject is small (Mayou, 1998). This lack
of systematic research and investigation into the subject is surprising given the numbers
of people affected by road crashes every day. Dealing with the psychosocial problems
related to the trauma of a road crash is a complex process which involves large numbers
and types of professional and other stakeholders. It is not surprising that injured
victims and distressed family members find it difficult to identify and access the best
information and support. Much of the post-crash distress is caused by failures in the
system to recognise the basic needs of the primary and secondary road crash victims
(Figley, 1995). This problem is compounded by failures in the delivery of the support in a
form that can be understood and accessed by anxious and distressed people. In many
*A study undertaken in co-operation with RoadPeace.
Correspondence to: Dr Noreen Tehrani, Managing Director, Assessment and Rehabilitation
Consultants, 12 Barensfield Road, Twickenham TW12QU, UK; e-mail: [email protected]
Counselling Psychology Quarterly,
Vol. 17, No. 4, 2004, pp. 361–373
Counselling Psychology Quarterly ISSN 0951–5070 print/ISSN 1469–3674 online # 2004 Taylor & Francis Ltd
http://www.tandf.co.uk/journals
DOI: 10.1080/09515070412331331255
Dow
nloa
ded
by [
Flin
ders
Uni
vers
ity o
f So
uth
Aus
tral
ia]
at 0
0:59
06
Oct
ober
201
4

ways, the victims of road crashes respond to trauma in the same way as victims of other
disasters. However, there is one major difference. Where an untimely or traumatic death
or injury occurs in a factory, ship, or mine the event is carefully investigated, causal
factors are identified and, where appropriate, action taken to reduce the likelihood of
similar incidents occurring again. In the case of death or injury on the road, post-incident
investigations are often minimal and occur in an atmosphere where road death is regarded
as an unavoidable outcome of a minor road traffic offence. The death or injury of the
victims is sometimes not seen as significant enough to warrant a mention in court. This
attitude of society has a profound impact on road crash victims and their
families who often feel let down and marginalised in their distress. A frequent cry
from victims of road crashes is for justice and an appropriate recognition of the pain
and suffering they have experienced.
Reactions to road traffic injury
It is important to recognise that while most people are resilient and cope well with the
physical pain and disability caused by a road crash, many road crash victims suffer
distressing psychological symptoms (Alexander, 1997). Post-trauma psychological symp-
toms vary in their type and magnitude and may continue to affect the victim long after the
physical scars have healed. Whilst it is difficult to predict who will suffer the most
following a road crash, the victims with pre-existing psychological (Blanchard et al., 1997)or social problems (Mayou, Tyndel & Bryant, 1997) have been shown to have more
difficulty in dealing with the stress and shock of bereavement. Supporting a disabled
family member, or becoming disabled oneself can be the cause of additional strain.
Unfortunately, the needs of families are frequently overlooked, with the result that the full
extent and cost of road crashes are significantly underestimated in terms of physical,
psychological and social disruption caused.
The quality of help and support provided for the victims and their families are critical
factors in the process of recovery, with social support being consistently found one of
the most important factors in facilitating recovery. It has been found (Perry, Difede,
Musngi & Jacobberg, 1992) that a lack of adequate psychosocial support has a greater
influence on the onset of post traumatic stress disorder (PTSD) than the severity of the
physical injury. A lack of social support has also been shown to increase the likelihood
of ‘late onset PTSD’ (Andersson, Dahlback & Allebeck, 1994). Late onset PTSD can
occur months or even years after the traumatic event in an individual who previously
appeared to be unaffected by the ordeal.
The psychological effect of serious injury or death on the road may be further
compounded by post-crash experiences. These experiences may include the insensitive
attitude of police, hospital personnel, mortuary attendants, coroners or magistrates.
Post-crash trauma (sanctuary trauma) occurs when an individual, having suffered a
traumatic event, encounters a person or situation expecting support or protection but
only experiences a lack of support or a malevolent attitude. The following case studies were
collected as part of the FEVR study (European Federation of Road Traffic Victims, 1997).
Case Study 1 gives an example of sanctuary trauma where the friend of a girl killed
by a car was distressed by the leniency of the courts.
362 Noreen Tehrani
Dow
nloa
ded
by [
Flin
ders
Uni
vers
ity o
f So
uth
Aus
tral
ia]
at 0
0:59
06
Oct
ober
201
4
Case Study 1 (Boyfriend of girl killed in road crash)
I don’t feel justice was done. The driver of the car that caused the death of my
girlfriend, through absolutely no fault of her own was not even banned from
driving for one year. If someone causes the death through dangerous driving
they should be automatically banned for at least a year. The driver was fined
£100. I feel that I am unable to depend on anything anymore.
Traumatic experiences such as a road crashes can shatter the fundamental beliefs on
which people build their lives. Many of our most deeply held beliefs are irrational,
reflecting a wish for how things should be, rather than how they are in reality. Some of the
commonly held beliefs that are shattered for victims of road crashes are illustrated in
Table I.
When, following a road crash, some or all of these beliefs are shattered the victim is
left feeling shocked, angry and abandoned in a world that they once experienced as being
predictable and safe. The failure of society to meet the victim’s expectations challenges
their basic values and can result in complex patterns of psychological symptoms including
post traumatic stress disorder (Janoff–Bulman, 1992). Case study 2 illustrates how a
bereaved mother reacted to the death of her daughter.
Case Study 2 (Mother of child killed by speeding car)
I felt alienated from the people who did not know what to do. Some friends
avoided contact with me, the good ones tried to cope with me. Initially my
family was good but when they thought that I should have got over it, they
stopped giving any support. Now I get no support from my family at all and
I have withdrawn from them. I feel isolated. I have problems sleeping and have
nightmares. I have lost all interest in everyday activities and in my profession.
I am depressed most of the time.
Post trauma symptoms
There is an increasing body of evidence that has identified a significant overlap between
Post Traumatic Stress Disorder (PTSD) and other psychiatric symptoms (Green, Lindy,
Grace & Leonard, 1992). Victims with pre-existing psychological conditions such
as anxiety or depression often find these conditions re-emerge following a road crash.
TABLE I. Common irrational beliefs
If I am careful I will come to no harm
The law always protects the innocent
Life is fair
The future is predictable
I can depend upon professional people to do a good job
The payment of damages will compensate my loss
Road Victim Trauma: an investigation of the impact on the injured and bereaved 363
Dow
nloa
ded
by [
Flin
ders
Uni
vers
ity o
f So
uth
Aus
tral
ia]
at 0
0:59
06
Oct
ober
201
4

Post trauma responses, physiology, personality, family environment and social stressors
interact to bring about a wide range of physical and psychological symptoms. Because the
post trauma symptoms may be delayed or lack any clear causal link to the road crash,
physicians often fail to recognise them as being part of a road crash syndrome (Bloom,
1998). In a study which compared trauma victims with PTSD with patients suffering
from a chronic depressive disorder, it was found that those with PTSD were more likely
to suffer from poor social support, more marital difficulties and occupational problems as
well as more financial problems (Landsman et al., 1990). When compared with patients
with chronic depression people with PTSD were also found to have a higher level of
physical illnesses, substance abuse, major depression, phobia, obsessive compulsive
disorder and depersonalisation (Solomon & Davidson, 1997). In Case Study 3 a father
describes the debilitating impact the death of his son had on his life.
Case Study 3 (Father of boy killed in road crash)
I am unable to put aside the vivid memories of our son lying on the pavement
dying. Nothing seems real or important except Gary. I have been unable to show
love to my other two sons, especially the youngest who was 8 months when Gary
was killed. There are constant reminders in our daily life of Gary. What would
he be doing now? Followed by memories of seeing Gary dead or seeing his
coffin. Not wanting to carry on, to walk away and cop out on life. I feel let down
by the law and society, and a burning desire to obtain justice, human justice!
I feel immediate anger and frustration when I see cars parked on the pavement
or speeding cars. I have flashbacks of how Gary was killed, a lack of sleep,
concentration, and a belief that I have no future, no prospects or hope.
Primary and secondary victims
Much of the research into the impact of road crashes has focussed on primary victims.
Primary victims are those people who were directly involved in the road crash (Blanchard
et al., 1997; Mayou et al., 1997). Where the research has looked at the impact of
road crashes on secondary victims it has focussed on the experiences and symptoms
of emergency workers, counsellors and other supporters (Figley, 1995). However, the
largest groups of secondary road crash victims are the families and friends of the injured
and bereaved. These two groups have had little investigation to assess the impact of
the road crash on their physical, psychological and social well-being. The mother in Case
Study 4 gives a typical response to a road crash bereavement.
Case Study 4 (Mother’s response to a road crash bereavment)
I cannot accept what happened to my Carolyn, although it is a year now.
The pain is as sore now as it was then. I cannot go anywhere in public without
364 Noreen Tehrani
Dow
nloa
ded
by [
Flin
ders
Uni
vers
ity o
f So
uth
Aus
tral
ia]
at 0
0:59
06
Oct
ober
201
4
the tears falling. Seeing mothers with their children. My stomach goes in knots
and I feel physically sick.
European research
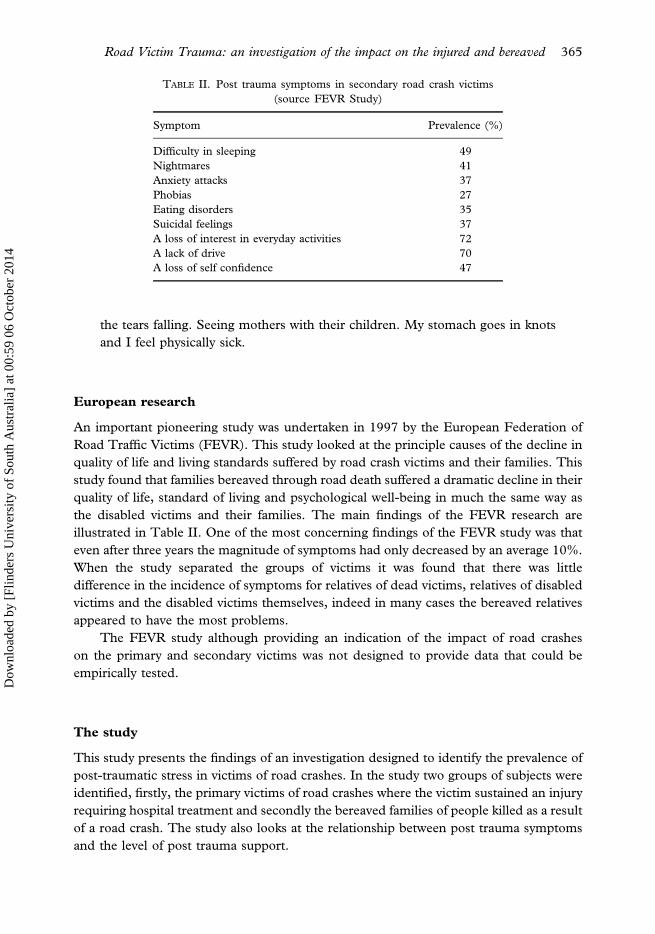
An important pioneering study was undertaken in 1997 by the European Federation of
Road Traffic Victims (FEVR). This study looked at the principle causes of the decline in
quality of life and living standards suffered by road crash victims and their families. This
study found that families bereaved through road death suffered a dramatic decline in their
quality of life, standard of living and psychological well-being in much the same way as
the disabled victims and their families. The main findings of the FEVR research are
illustrated in Table II. One of the most concerning findings of the FEVR study was that
even after three years the magnitude of symptoms had only decreased by an average 10%.
When the study separated the groups of victims it was found that there was little
difference in the incidence of symptoms for relatives of dead victims, relatives of disabled
victims and the disabled victims themselves, indeed in many cases the bereaved relatives
appeared to have the most problems.
The FEVR study although providing an indication of the impact of road crashes
on the primary and secondary victims was not designed to provide data that could be
empirically tested.
The study
This study presents the findings of an investigation designed to identify the prevalence of
post-traumatic stress in victims of road crashes. In the study two groups of subjects were
identified, firstly, the primary victims of road crashes where the victim sustained an injury
requiring hospital treatment and secondly the bereaved families of people killed as a result
of a road crash. The study also looks at the relationship between post trauma symptoms
and the level of post trauma support.
TABLE II. Post trauma symptoms in secondary road crash victims
(source FEVR Study)
Symptom Prevalence (%)
Difficulty in sleeping 49
Nightmares 41
Anxiety attacks 37
Phobias 27
Eating disorders 35
Suicidal feelings 37
A loss of interest in everyday activities 72
A lack of drive 70
A loss of self confidence 47
Road Victim Trauma: an investigation of the impact on the injured and bereaved 365
Dow
nloa
ded
by [
Flin
ders
Uni
vers
ity o
f So
uth
Aus
tral
ia]
at 0
0:59
06
Oct
ober
201
4
Method
The subjects for the study had all contacted the RoadPeace helpline following a road
crash. The purpose of the study was explained and the callers were invited to complete
a self-assessment questionnaire.
The questionnaire was made up of seven sections:
1. Demographic information.
2. A description of the crash.
3. The impact of the crash on those involved.
4. Where the subject placed the responsibility for the crash.
5. The IES-E questionnaire which measures post traumatic stress symptoms.
6. A life style questionnaire.
7. Information on the quality of the immediate and ongoing support.
Subjects
One hundred and fourteen subjects took place in the study. The subjects formed five
groups:
1. The families and friends of people killed on the road.
2. People injured in road crashes.
3. People injured and bereaved in a road crash.
4. Carers of the injured.
5. Witnesses to a road crash.
There were 46 subjects who were injured, 57 who had been bereaved, eight injured
and bereaved, two carers and one witness. (Due to the smallness of the numbers of
groups 3, 4 and 5, no further analysis of these data was undertaken.)
The mean age of the injured subjects was 37 years; there were 33 females and 13
males. The mean age of the bereaved subjects was 43 years; 48 were female and nine
male. The average time since the crash for the injured subjects was 5.5 years and for the
bereaved subjects 4.5 years. All subjects were aware that the information they provided
would be used for research purposes and that no personally identifiable information
would be revealed without their written permission.
Measures
The extended impact of events scale (IES-E) (Tehrani, Cox & Cox, 2002) was used to
measure the post trauma symptoms. This post traumatic stress instrument has been used
for measuring the level of post traumatic stress in a number of occupational groups
including a large study in the emergency services (Tyler, 1999) The IES-E measures the
three post trauma symptoms of avoidance, arousal and re-experience. The questionnaire
also examines a further 11 associated psychological symptoms. These symptoms were the
most commonly occurring symptoms taken from the written accounts of more than 200
road crash victims. The social impact of the road crash looked at financial, relationships,
366 Noreen Tehrani
Dow
nloa
ded
by [
Flin
ders
Uni
vers
ity o
f So
uth
Aus
tral
ia]
at 0
0:59
06
Oct
ober
201
4
social life, status and ability to work. The physical impact looked at the severity of the
injuries together with the pain, disability, disfigurement and length of hospital treatment.
The quality of support assessed the subjects perception of the quality of support provided
by the emergency services together with the follow up support in the areas of legal,
insurance, health and general well-being. The subjects were also given an opportunity to
provide further comments, which provide additional qualitative feedback.
Results
Results were calculated for each section of the questionnaire.
Responsibility for the crash
The other driver was almost entirely attributed with the blame for the crash with 94.6%
of the injured and 88.7% of bereaved subjects believing that the other driver had caused
the road crash. A total of 3.9% of subjects indicated that the road conditions were the
likely cause of the crash and a further 3.9% believed that there was some shared
responsibility for causing the crash.
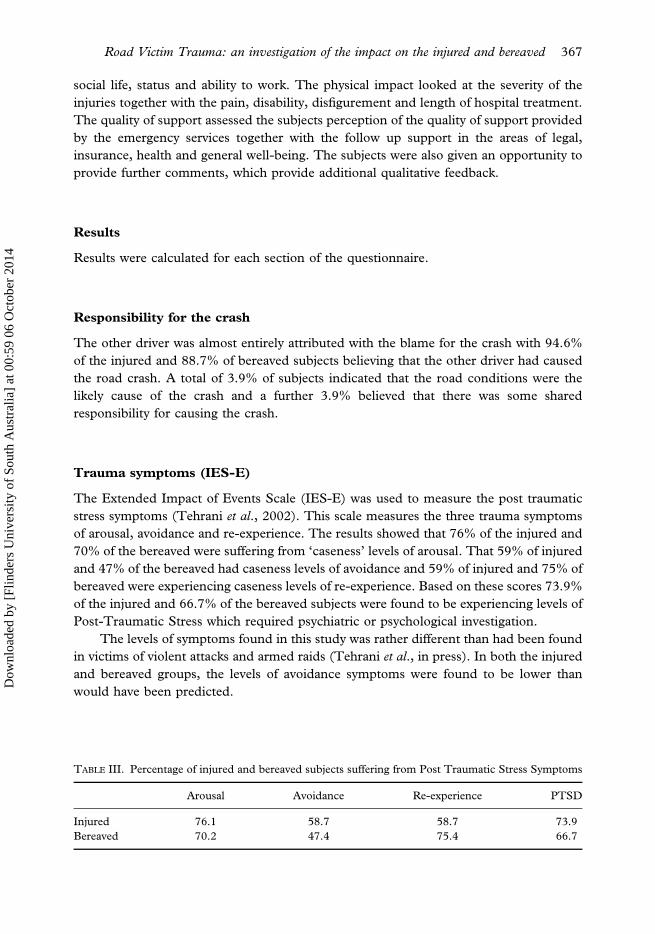
Trauma symptoms (IES-E)
The Extended Impact of Events Scale (IES-E) was used to measure the post traumatic
stress symptoms (Tehrani et al., 2002). This scale measures the three trauma symptoms
of arousal, avoidance and re-experience. The results showed that 76% of the injured and
70% of the bereaved were suffering from ‘caseness’ levels of arousal. That 59% of injured
and 47% of the bereaved had caseness levels of avoidance and 59% of injured and 75% of
bereaved were experiencing caseness levels of re-experience. Based on these scores 73.9%
of the injured and 66.7% of the bereaved subjects were found to be experiencing levels of
Post-Traumatic Stress which required psychiatric or psychological investigation.
The levels of symptoms found in this study was rather different than had been found
in victims of violent attacks and armed raids (Tehrani et al., in press). In both the injured
and bereaved groups, the levels of avoidance symptoms were found to be lower than
would have been predicted.
TABLE III. Percentage of injured and bereaved subjects suffering from Post Traumatic Stress Symptoms
Arousal Avoidance Re-experience PTSD
Injured 76.1 58.7 58.7 73.9
Bereaved 70.2 47.4 75.4 66.7
Road Victim Trauma: an investigation of the impact on the injured and bereaved 367
Dow
nloa
ded
by [
Flin
ders
Uni
vers
ity o
f So
uth
Aus
tral
ia]
at 0
0:59
06
Oct
ober
201
4
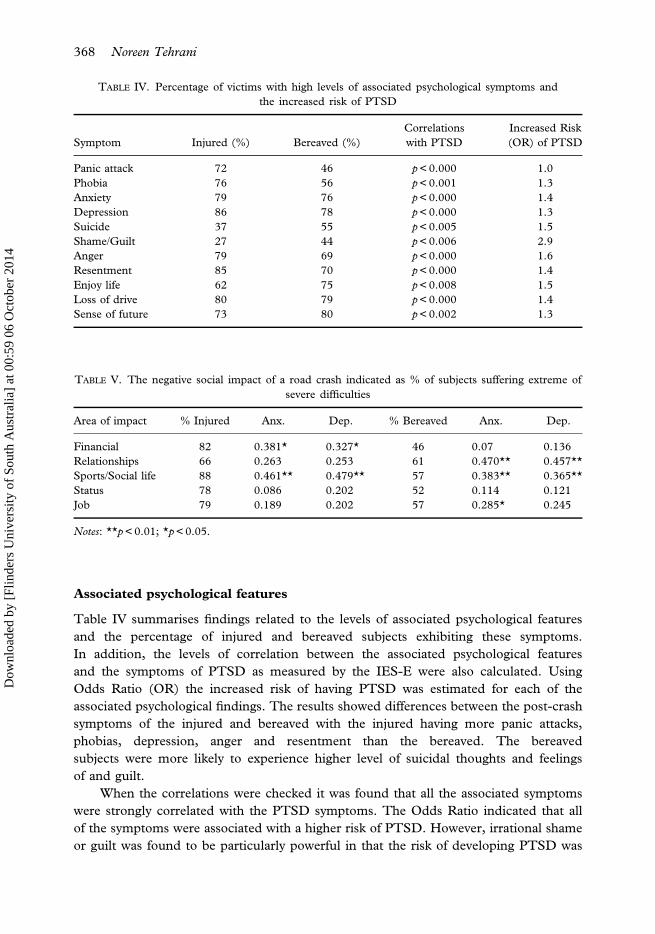
Associated psychological features
Table IV summarises findings related to the levels of associated psychological features
and the percentage of injured and bereaved subjects exhibiting these symptoms.
In addition, the levels of correlation between the associated psychological features
and the symptoms of PTSD as measured by the IES-E were also calculated. Using
Odds Ratio (OR) the increased risk of having PTSD was estimated for each of the
associated psychological findings. The results showed differences between the post-crash
symptoms of the injured and bereaved with the injured having more panic attacks,
phobias, depression, anger and resentment than the bereaved. The bereaved
subjects were more likely to experience higher level of suicidal thoughts and feelings
of and guilt.
When the correlations were checked it was found that all the associated symptoms
were strongly correlated with the PTSD symptoms. The Odds Ratio indicated that all
of the symptoms were associated with a higher risk of PTSD. However, irrational shame
or guilt was found to be particularly powerful in that the risk of developing PTSD was
TABLE IV. Percentage of victims with high levels of associated psychological symptoms and
the increased risk of PTSD
Symptom Injured (%) Bereaved (%)
Correlations
with PTSD
Increased Risk
(OR) of PTSD
Panic attack 72 46 p<0.000 1.0
Phobia 76 56 p<0.001 1.3
Anxiety 79 76 p<0.000 1.4
Depression 86 78 p<0.000 1.3
Suicide 37 55 p<0.005 1.5
Shame/Guilt 27 44 p<0.006 2.9
Anger 79 69 p<0.000 1.6
Resentment 85 70 p<0.000 1.4
Enjoy life 62 75 p<0.008 1.5
Loss of drive 80 79 p<0.000 1.4
Sense of future 73 80 p<0.002 1.3
TABLE V. The negative social impact of a road crash indicated as % of subjects suffering extreme of
severe difficulties
Area of impact % Injured Anx. Dep. % Bereaved Anx. Dep.
Financial 82 0.381* 0.327* 46 0.07 �0.136
Relationships 66 0.263 0.253 61 0.470** 0.457**
Sports/Social life 88 0.461** 0.479** 57 0.383** 0.365**
Status 78 0.086 �0.202 52 0.114 0.121
Job 79 0.189 0.202 57 0.285* 0.245
Notes: **p<0.01; *p<0.05.
368 Noreen Tehrani
Dow
nloa
ded
by [
Flin
ders
Uni
vers
ity o
f So
uth
Aus
tral
ia]
at 0
0:59
06
Oct
ober
201
4
almost three times greater in people experiencing irrational shame and guilt than for
subjects who did not have these thoughts.
Social impact
Involvement in a road crash has a large impact on the life of the victims. Table V shows
the percentage of injured and bereaved subjects that experienced social difficulties.
These social difficulties were correlated with levels of anxiety and depression. These
results showed some similarities and differences between the injured and bereaved
groups. The injured experienced more anxiety and depression regarding financial
problems than the bereaved. The bereaved experienced high levels of anxiety and
depression related to relationship problems. In addition, the bereaved subjects were
more anxious when they had difficulties with their work. Both groups experienced higher
levels of anxiety and depression associated with a lack of sports and social life.
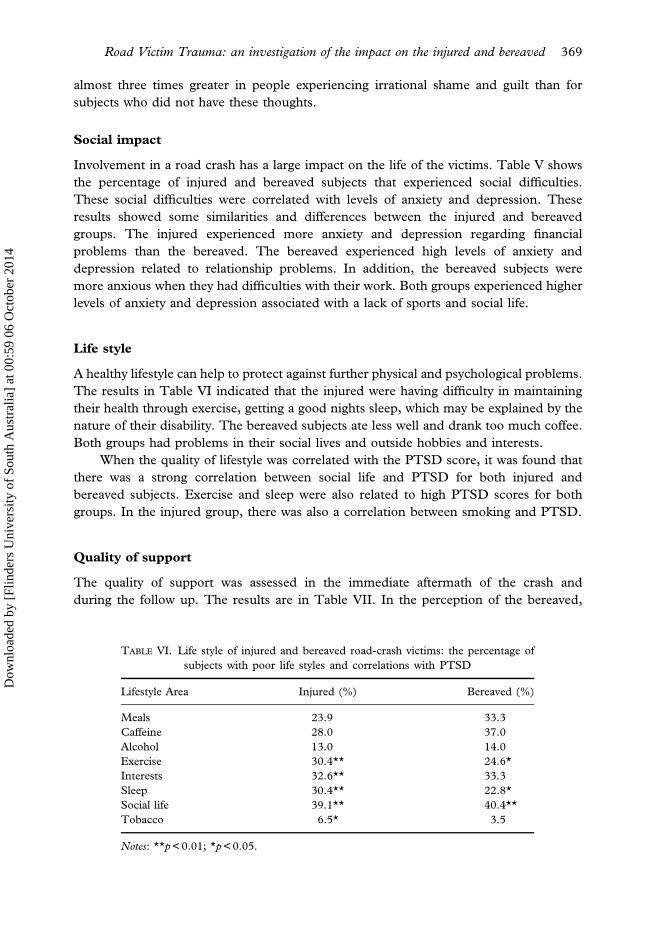
Life style
A healthy lifestyle can help to protect against further physical and psychological problems.
The results in Table VI indicated that the injured were having difficulty in maintaining
their health through exercise, getting a good nights sleep, which may be explained by the
nature of their disability. The bereaved subjects ate less well and drank too much coffee.
Both groups had problems in their social lives and outside hobbies and interests.
When the quality of lifestyle was correlated with the PTSD score, it was found that
there was a strong correlation between social life and PTSD for both injured and
bereaved subjects. Exercise and sleep were also related to high PTSD scores for both
groups. In the injured group, there was also a correlation between smoking and PTSD.
Quality of support
The quality of support was assessed in the immediate aftermath of the crash and
during the follow up. The results are in Table VII. In the perception of the bereaved,
TABLE VI. Life style of injured and bereaved road-crash victims: the percentage of
subjects with poor life styles and correlations with PTSD
Lifestyle Area Injured (%) Bereaved (%)
Meals 23.9 33.3
Caffeine 28.0 37.0
Alcohol 13.0 14.0
Exercise 30.4** 24.6*
Interests 32.6** 33.3
Sleep 30.4** 22.8*
Social life 39.1** 40.4**
Tobacco 6.5* 3.5
Notes: **p<0.01; *p<0.05.
Road Victim Trauma: an investigation of the impact on the injured and bereaved 369
Dow
nloa
ded
by [
Flin
ders
Uni
vers
ity o
f So
uth
Aus
tral
ia]
at 0
0:59
06
Oct
ober
201
4
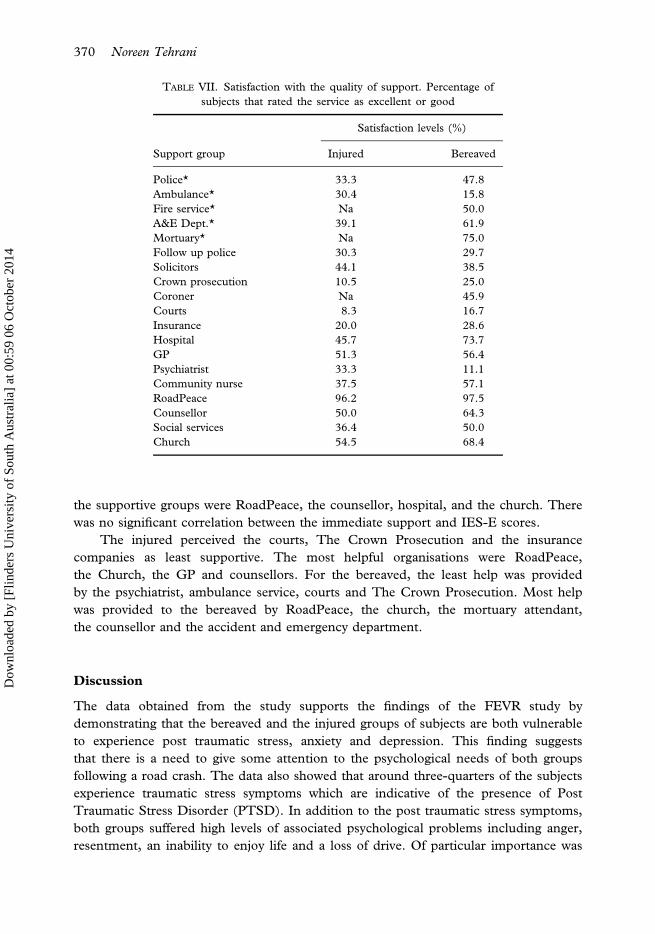
the supportive groups were RoadPeace, the counsellor, hospital, and the church. There
was no significant correlation between the immediate support and IES-E scores.
The injured perceived the courts, The Crown Prosecution and the insurance
companies as least supportive. The most helpful organisations were RoadPeace,
the Church, the GP and counsellors. For the bereaved, the least help was provided
by the psychiatrist, ambulance service, courts and The Crown Prosecution. Most help
was provided to the bereaved by RoadPeace, the church, the mortuary attendant,
the counsellor and the accident and emergency department.
Discussion
The data obtained from the study supports the findings of the FEVR study by
demonstrating that the bereaved and the injured groups of subjects are both vulnerable
to experience post traumatic stress, anxiety and depression. This finding suggests
that there is a need to give some attention to the psychological needs of both groups
following a road crash. The data also showed that around three-quarters of the subjects
experience traumatic stress symptoms which are indicative of the presence of Post
Traumatic Stress Disorder (PTSD). In addition to the post traumatic stress symptoms,
both groups suffered high levels of associated psychological problems including anger,
resentment, an inability to enjoy life and a loss of drive. Of particular importance was
TABLE VII. Satisfaction with the quality of support. Percentage of
subjects that rated the service as excellent or good
Satisfaction levels (%)
Support group Injured Bereaved
Police* 33.3 47.8
Ambulance* 30.4 15.8
Fire service* Na 50.0
A&E Dept.* 39.1 61.9
Mortuary* Na 75.0
Follow up police 30.3 29.7
Solicitors 44.1 38.5
Crown prosecution 10.5 25.0
Coroner Na 45.9
Courts 8.3 16.7
Insurance 20.0 28.6
Hospital 45.7 73.7
GP 51.3 56.4
Psychiatrist 33.3 11.1
Community nurse 37.5 57.1
RoadPeace 96.2 97.5
Counsellor 50.0 64.3
Social services 36.4 50.0
Church 54.5 68.4
370 Noreen Tehrani
Dow
nloa
ded
by [
Flin
ders
Uni
vers
ity o
f So
uth
Aus
tral
ia]
at 0
0:59
06
Oct
ober
201
4
the presence of irrational guilt, which was associated with almost three times the level
of post traumatic stress and panic attacks found in subjects who did not have these
irrational thoughts.
Despite these findings, only 45 of the 114 subjects had seen a counsellor and 22
subjects had seen a psychiatrist. The satisfaction with counsellors was higher for the
bereaved subjects than for injured subjects. However, the counselling did not appear to be
associated with a reduced level of traumatic stress symptoms. Injured subjects were less
likely to have seen a counsellor than bereaved subjects, it is possible that this is because of
the mobility problems that are faced by injured victims. There was a low level of
satisfaction with psychiatrists, among the bereaved. An inspection of comments made
on the questionnaires suggested that this dissatisfaction largely related to psychiatrists
being seen as part of the legal system used to assess the level of psychological injury for
insurance claims.
The social problems suffered by the injured victims of road crashes were found to
cause extreme or severe distress to over 75% of subjects. Social problems are strongly
correlated with high levels of anxiety and depression. Social support has repeatedly
been found a critical component of the recovery or lack of recovery of those involved in
a road crash. This finding confirms the work of Andersson et al. (1997) which showed
that poor social support is one of the main risk factors in the development of post
traumatic stress.
Severe financial hardship was reported by 70% of the subjects taking part in this
study. This data gives some indication of the magnitude of the economic problems
faced by many road crash victims. Whilst this may not be a totally representative
sample it is indicative of the problems that are facing a large number of families following
a road crash.
The life style patterns of the injured and bereaved were shown to be rather different
from each other. Overall, the injured road crash victims tended to eat more regularly
and drank less caffeine than the bereaved. On the other hand, the bereaved tended to
take more exercise and have more sleep than the injured. A healthy lifestyle was
associated with lower levels of post traumatic stress. From the data gathered it was
not possible to show whether the poor life style caused in the increased levels of post
traumatic stress or that people with post traumatic stress were more likely to have a poor
life style.
Whilst this study did not identify a direct link between the quality of support and
post traumatic stress this linkage has been demonstrated in many other studies
including that of Landsman et al. (1990). Landsman et al. showed that 3 years after the
traumatic experience the levels of psychological distress were predicted less by injury
severity than by the subsequent financial, employment, family and other social difficulties.
The road crash victims identified a wide difference in the level of care and
support provided. Some groups were seen as significantly more supportive than other
groups. Of particular note were the mortuary attendants where there was a 75% level of
satisfaction. In contrast, there was only a 15.8% level of satisfaction with the support
provided by ambulance staff. The results also showed a low level of satisfaction with the
legal services, particularly the courts and Crown Prosecution. As most road crash victims
Road Victim Trauma: an investigation of the impact on the injured and bereaved 371
Dow
nloa
ded
by [
Flin
ders
Uni
vers
ity o
f So
uth
Aus
tral
ia]
at 0
0:59
06
Oct
ober
201
4

will have some contact with the legal system, it is important that more effort is made to
ensure that these services become more sensitive to the needs of the road crash victims.
Of particular importance is the benefit of a self-help advice and guidance service such
as that provided by RoadPeace, together with support from the church and counsellors
this was seen positively by both groups of subjects. It is vital that the support provided
is long term and meets the personal, social and psychological needs of the road crash
victims. The provision of a single, isolated intervention such as debriefing and other
forms of crisis intervention has been shown to be inadequate (Paton et al., 1998). What
is required is a national programme of support that provides early assistance and
information followed by support resources which facilitate self-help and which sustains
and promotes positive personal growth and recovery.
Acknowledgements
I would like to offer my gratitude to all the victims of road crashes who took part in this
study and to RoadPeace for their support of this research.
References
ALEXANDER, D.A. (1997) Psychological aspects of trauma. In P.K. Greaves & D. Burke (Eds.) Key Topicsin Trauma. Oxford: Bios Scientific Publishers.
ANDERSSON, A., BUNKETORP, O., ALLEBECK, P. (1997) High rates of psychosocial complications after
road traffic injuries. Injury 28(8) 539–543.ANDERSSON, A., DAHLBACK, L. & ALLEBECK, P. (1994) Psychological consequences of traffic accidents:
a two-year follow up. Scandinavian Journal of Social Medicine, 22(4), 299–302.BLANCHARD, E.B., HICKLING, E.J., FORNERIS, C.A., TAYLOR, A.E., BUCKLEY, T.C., LOOS, W.R. &
JACCARD, J. (1997) Prediction of remission of acute posttraumatic stress disorder in motor vehicle
accident victims. Journal of Traumatic Stress, 10(2), 215–234.BLOOM, S.L. (1998) Motor vehicle accidents, co-morbidity and PTSD. A paper presented at a conference
Road Accidents and the Mind, 1–3 September, Lyons Davidson, Bristol, UK.
EUROPEAN FEDERATION OF ROAD TRAFFIC VICTIMS (1997) Impact of Road Death and Injury: Proposals forImprovements. Switzerland: FEVR.
FIGLEY, C.R. (1995) Compassion Fatigue. New York: Brunner Mazel.
GREEN, B.L., LINDY, J.D., GRACE, M.C. & LEONARD, A.C. (1992) Chronic post traumatic stress
disorder and diagnostic co-morbidity in the disaster sample. Journal of Nervous and Mental Disorders,180, 760–766.
JANOFF-BULMAN, R. (1992) Shattered Assumptions: Towards a New Psychology of Trauma, New York,
Free Press.
LANDSMAN, I.S., BAUM, C.G., ARNKOFF, D.B., CRAIG, M.J., LYNCH, I., COPES, W.S. & CHAMPION, H.R.
(1990) The psycho-social consequences of traumatic injury. Journal of Behavioural Medicine, 13(6),561–581.
MAYOU, R. (1998) Forces on the mind. Paper presented at the conference Road Accidents and the Mind,
Bristol, UK.
MAYOU, R., TYNDEL, S. & BRYANT, B. (1997) Long term outcome of motor vehicle accident injury.
Psychosomatic Medicine, 59(6), 578–584.PATON, D., SMITH, L.M. & STEPHENS, C. (1998) Work-related psychological trauma: a social psycho-
logical and organisational approach to understanding response and recovery. The Australian Journalof Disaster and Trauma Studies, 1. Available at http://www.massey.ac.nz
372 Noreen Tehrani
Dow
nloa
ded
by [
Flin
ders
Uni
vers
ity o
f So
uth
Aus
tral
ia]
at 0
0:59
06
Oct
ober
201
4

PERRY, S., DIFEDE, M.E., MUSNGI, G.F. & JACOBBERG, L., (1992) Predictors or posttraumatic stress
disorder after burn injury. American Journal of Psychiatry 149, 931–935.SOLOMON, S. & DAVIDSON, J.R.T. (1997) Trauma prevalence, impairment, service use, and cost. Journal
of Clinical Psychiatry, 58(supplement 9), 5–11.
TEHRANI, N., COX, T. & COX, S. (2002) Assessing the impact of stressful incidents in organisations: the
development of an extended impact of events scale. Counselling Psychology Quarterly 7, 15, 191–200.TYLER, G. (1999) Personality, general well-being and post traumatic stress disorder in the ambulance
service. The Occupational Psychologist, 37, 30–34.
Road Victim Trauma: an investigation of the impact on the injured and bereaved 373
Dow
nloa
ded
by [
Flin
ders
Uni
vers
ity o
f So
uth
Aus
tral
ia]
at 0
0:59
06
Oct
ober
201
4