Embed Size (px)
Citation preview
Journd of Communiiy P.yehdow, 1078, 7. 336-342.
ROLE PERCEPTIONS IN A COMMUNITY MENTAL HEALTH SETTING*
HERBERT HARARI, KAREN HOSEY, A N D PATRICIA SHEEDY
San Diego Stale Universiiy
The increasing trend of utilizing nonprofessional personnel in community mental health has led to considerable controversy. It is suggested that studies comparing the relative competence and efficacy of professional therapists to that of nonprofessional therapists may be counterproductive and in need of augmentation. The present study employed a role perception procedure in which members of three different randomly chosen groups ( 1 I professional therapists, 1 I nonprofessional therapists, and I I children-clients) from a community mental health program were asked to rank various aspects of the therapeutic relationship in order of importance to the children- clients’ improvement. It was hypothesized that (a) due to their relatively low self- concept, nonprofessionals would underestimate their own role importance in com- parison to that of the professionals; (b) professionals would overestimate their own role importance; and (c) children would selectively value certain aspects of each role without preferring one over the other. The last two hypotheses were supported, but the first hypothesis was not: nonprofessionals, in fact, showed the highest level of overestimation of their own role importance. A further analysis of the data showed that inexperienced nonprofessionals did not overestimate their own role performance. This suggested specific training procedures for nonprofessionals.
The upsurge of community programs aimed at alleviating the shortage of professional mental health personnel in recent years has resulted in the emergence of a variety of nonprofessional services in diverse roles and settings (Cowen, Chinsky, & Rap- paport, 1970; Gruver, 1971). After surveying the success and practicality of over 10,OOO nonprofessionals in over 185 NIMH projects across the United States, Sobey (1970) suggested that there was a “nonprofessional revolution in mental health .” This revolu- tion has provided an important source of manpower, but has also produced certain con- comitant problems and considerable controversy concerning the use and efficacy of non- professionals.
Opinions concerning the use of nonprofessionals are conflicting (Genther, 1974; Goldenberg, 1973; Gruver, 1971; Keniston, 1967; Mitchell, 1966), and in view of their current widespread employment this controversy becomes a serious issue. Some researchers have attempted to determine whether untrained therapists can do an effective therapeutic job (Blau, 1969; Guerney, 1969; Sobey, 1970) and have even directly com- pared their effectiveness with that of professionals (Durlak, 1973). Meltzoff and Kor- nreich ( 1970) in an extensive review of comparative professional-nonprofessional therapeutic effectiveness studies cited numerous methodological shortcomings, such as inappropriate use of statistics, lack of control groups, sampling biases, lack of random assignment, and effectiveness criteria, to conclude that “a good controlled comparison of the effectiveness of trained and untrained therapists has yet to be made” (p. 288).
We doubt whether this worthy goal will ever be achieved. There are increasing restrictions on the use of human subjects for psychological research, especially in clinical settings. There are ethical questions to be considered when treatment is denied through the establishment of control groups, and there are practical considerations due to the
+Send reprint requests to first author, Department of Psychology, San Diego State University, San Diego, California 92182.
335
336 H E R B E R T H A R A R I , KAREN HOSEY, A N D PATRICIA SHEEDY
limited feasibility of subjecting patients to untrained laypersons. Perhaps the time has come to accept the emergence of nonprofessionals in the field of mental health as an ac- complished fact. Our own belief is that both professionals and nonprofessionals have the potential to offer their own unique benefits to patients.
Our basic thesis is that social-psychological research exploring the values, roles, and interpersonal perception of all therapists is a valuable augmentation to controversial, and somewhat futile, comparative studies of who is “best.” We base this belief on our ex- perience of involvement over a period of four years in a college companionship program where undergraduate (nonprofessional) students worked on a one-to-one basis with children in therapy while under the direct supervision of the childrens’ (professional) therapists.
In addition to such wide scope social-psychological exploration, we feel that research should be directed toward the establishment of clear roles for the non- professionals. Within the companionship program, we have frequently encountered feelings of frustration and expressions of self-derogation among the students toward their role as nonprofessional therapists (“unpaid babysitters”), and we believe that their self- esteem and satisfaction could be enhanced by a clearer definition of their unique con- tributions. Block (1974) maintained that paraprofessionals’ lack of identity results in lower morale because they are often unaware of their place in the overall mental health picture.
Accordingly, the present study involved a role perception procedure in which ran- domly selected members of the companionship therapy program (professionals, non- professionals, and children in therapy) were asked to rank various aspects of the therapeutic relationship in order of importance to the child’s improvement. It was hypothesized that (a) the nonprofessionals (students), due to their relatively low self- concept, would underestimate their own role importance in comparison to that of the professionals (therapists); (b) the professionals would overestimate their own role impor- tance; and (c) the children would selectively value certain aspects of each role and therefore, no clear-cut pattern could be predicted. In addition to examining these hypotheses, the study was designed to provide specific expectations and counterexpec- tations and thus to provide valuable information about this three-sided therapeutic relationship, and about the supervisory role of professional therapists.
METHOD Participants. Three groups of persons participated in this study. The first group con-
sisted of eight female and three male undergraduate psychology majors enrolled at San Diego State University. The second group consisted of six male and five female children who were outpatients at a San Diego Community Mental Health facility (median age 8.5, classified according to the general DSM category of Behavior Disorders of Childhood and Adolescence). The third group consisted of seven male and four female therapists (three psychiatrists, four psychologists, four social workers) at the same facility. All persons were randomly selected and were participating in the student com- panionship program.
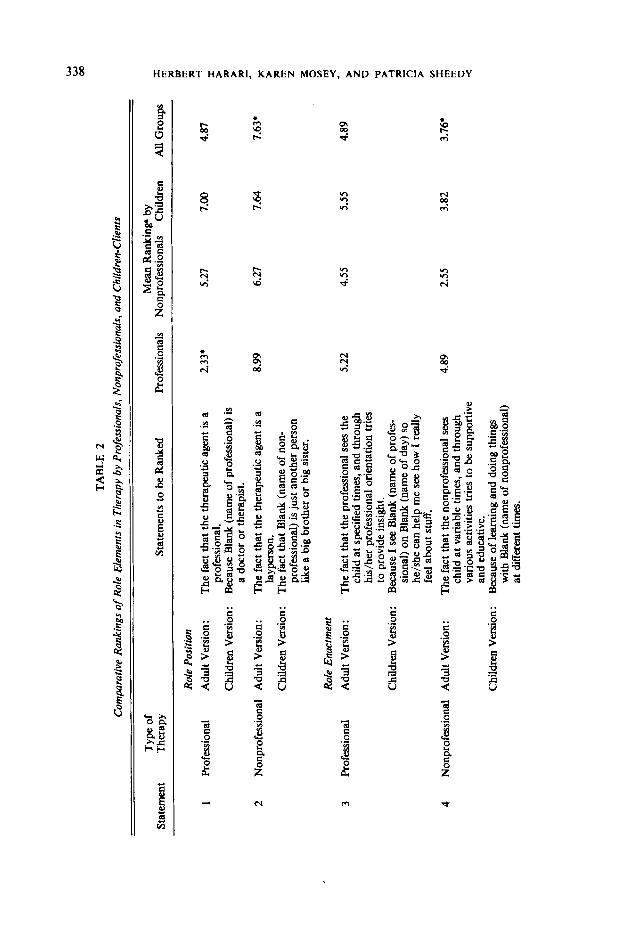
Apparatus. Mitchell’s ( 1966) structured elements of nonprofessional therapy (amicatherapy) and professional therapy were employed as the basic dependent measure. From a social-psychological perspective, these elements can be viewed as various aspects of role position, role enactment, role expectations, status, and environment. The elements were written as statements on ten cards, with one set for the students and the
337 VALUES A N D ROLES
therapists, and one with identical statements, but in simplified language, for the children (The full listing is in Table 2).
Procedure. After being informed that the present experiment was designed to find which areas in companionship therapy the person felt were the most influential factors in the child's improvement, participants were requested to rank the ten elements (five for nonprofessional therapy and five for professional therapy) in order of importance (a rank of one to the most important factor, and a rank of ten to the least important factor). To control for varying levels of reading proficiency, the cards were read aloud to each of the children who were then asked to place the cards according to their perceived importance. Stacks of cards were rearranged in random order between each person's use.
RESULTS
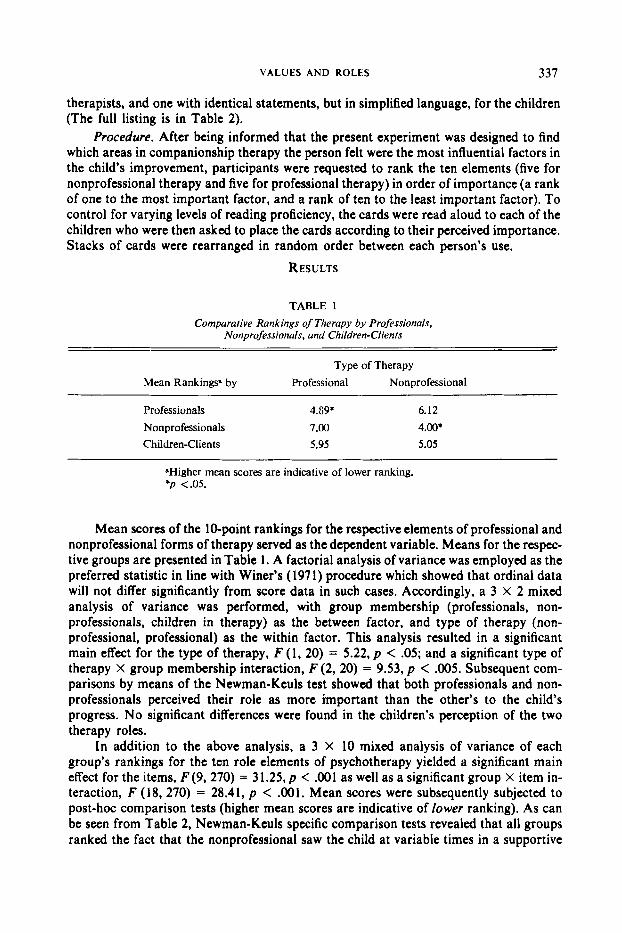
TABLE 1 Comparaiive Rankings of Therapy by Professionals,
Nonprofessionals, and Children- Clients - Type of Therapy
Mean Rankings" by Professional Nonprofessional
Professionals 4.G9*
Nonprofessionals 7.00 Children-Clients 5.95
6.12
4.00. 5.05
"Higher mean scores are indicative of lower ranking. *p <.05.
Mean scores of the 10-point rankings for the respective elements of professional and nonprofessional forms of therapy served as the dependent variable. Means for the respec- tive groups are presented in Table 1. A factorial analysis of variance was employed as the preferred statistic in line with Winer's (197 1) procedure which showed that ordinal data will not differ significantly from score data in such cases. Accordingly, a 3 X 2 mixed analysis of variance was performed, with group membership (professionals, non- professionals, children in therapy) as the between factor, and type of therapy (non- professional, professional) as the within factor. This analysis resulted in a significant main effect for the type of therapy, F (1, 20) = 5.22, p < .05; and a significant type of therapy X group membership interaction, F (2, 20) = 9.53, p < .005. Subsequent com- parisons by means of the Newman-Keuls test showed that both professionals and non- professionals perceived their role as more important than the other's to the child's progress. No significant differences were found in the children's perception of the two therapy roles.
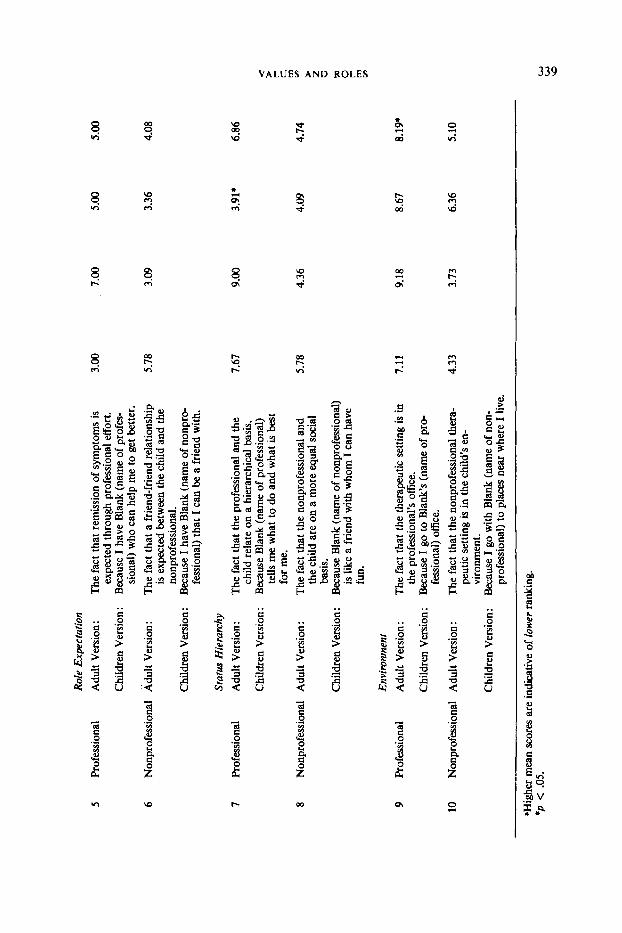
In addition to the above analysis, a 3 X 10 mixed analysis of variance of each group's rankings for the ten role elements of psychotherapy yielded a significant main effect for the items, F ( 9 , 270) = 31.25, p < .001 as well as a significant group X item in- teraction, F (18,270) = 28.41, p < .001. Mean scores were subsequently subjected to post-hoc comparison tests (higher mean scores are indicative of lower ranking). As can be seen from Table 2, Newman-Keuls specific comparison tests revealed that all groups ranked the fact that the nonprofessional saw the child at variable times in a supportive
TA
BL
E 2
Com
para
tive
Ran
king
s of
Rol
e E
lem
ents
in T
hera
py b
y Pr
ofes
sion
als,
Non
prof
essi
onal
s, an
d C
hild
ren-
Clie
nts
Typ
e of
M
ean
Ran
king
. by
St
atem
ent
The
rapy
St
atem
ents
to b
e R
anke
d Pr
ofes
sion
als
Non
prof
essi
onal
s C
hild
ren
All G
roup
s
Rol
e Po
sitio
n
1 Pr
ofes
sion
al
Adu
lt V
ersi
on:
The
fact
that
the
ther
apeu
tic a
gent
is a
pr
ofes
sion
al.
a do
ctor
or t
hera
pist
.
layp
erso
n.
The
fact
that
Bla
nk (
nam
e of
non-
pr
ofes
sion
al)
is ju
st a
noth
er p
erso
n lik
e a
big
brot
her
or b
ig s
iste
r.
Chi
ldre
n V
ersi
on:
Bec
ause
Bla
nk (
nam
e of
pro
fess
iona
l) is
2 N
onpr
ofes
sion
al
Adu
lt V
ersi
on:
The
fact
tha
t th
e th
erap
eutic
age
nt is
a
Chi
ldre
n V
ersi
on:
Rol
e E
nact
men
t
3 Pr
ofes
sion
al
Adu
lt V
ersi
on:
The
fact
tha
t the
pro
fess
iona
l se
es th
e ch
ild a
t spe
cifie
d tim
es, a
nd th
roug
h hi
s/he
r pr
ofes
sion
al o
rien
tatio
n tri
es
to p
rovi
de in
sigh
t. B
ecau
se I
see
Bla
nk (
nam
e of
pro
fes-
si
onal
) on
Bla
nk (
nam
e of
day
) so
he/s
he c
an h
elp
me
see
how
I re
ally
fe
el a
bout
stu
ff.
4 N
onpr
ofes
sion
al
Adu
lt V
ersi
on:
The
fact
tha
t the
non
prof
essi
onal
sees
child
at v
aria
ble
times
, and
thro
ugh
vario
us a
ctiv
ities
trie
s to
be
supp
ortiv
e an
d ed
ucat
ive.
with
Bla
nk (
nam
e of
non
prof
essi
onal
) at
diff
eren
t tim
es.
Chi
ldre
n V
ersi
on:
Chi
ldre
n V
ersi
on:
Bec
ause
of
lear
ning
and
doi
ng th
ings
2.33*
5.27
7.00
4.87
8.99
6.27
7.64
7.63*
5.22
4.89
4.55
2.55
5.55
4.89
3.82
3.76'
Role
Exp
ecta
tion
5 Pr
ofes
sion
al
Adu
lt V
ersi
on:
Chi
ldre
n V
ersi
on :
6 N
onpr
ofes
sion
al
Adu
lt V
ersi
on:
Chi
ldre
n V
ersi
on :
Stat
us H
iera
rchy
7
Prof
essi
onal
A
dult
Ver
sion
:
Chi
ldre
n V
ersi
on:
8 N
onpr
ofes
sion
al
Adu
lt V
ersi
on:
Chi
ldre
n V
ersi
on:
Envi
ronm
ent
9 Pr
ofes
sion
al
Adu
lt V
ersi
on:
Chi
ldre
n V
ersi
on:
10
Non
prof
essi
onal
A
dult
Ver
sion
:
Chi
ldre
n V
ersi
on:
The
fact
tha
t rem
issi
on o
f sy
mpt
oms
is
3.00
ex
pect
ed t
hrou
gh p
rofe
ssio
nal
effo
rt.
Bec
ause
I ha
ve B
lank
(na
me
of p
rofe
s-
sion
al)
who
can
hel
p m
e to
get
bet
ter.
The
fact
tha
t a fr
iend
-frie
nd r
elat
ions
hip
is ex
pect
ed b
etw
een
the
child
and
the
nonp
rofe
ssio
nal.
Bec
ause
I ha
ve B
lank
(na
me
of n
onpr
o-
fess
iona
l) th
at I
can b
e a
frie
nd w
ith.
5.78
The
fact
tha
t the
pro
fess
iona
l an
d th
e ch
ild r
elat
e on a
hie
rarc
hica
l ba
sis.
Bec
ause
Bla
nk (
nam
e of
pro
fess
iona
l) te
lls m
e w
hat t
o do
and
wha
t is
best
fo
r me.
T
he fa
ct th
at th
e no
npro
fess
iona
l and
th
e ch
ild a
re on
a m
ore
equa
l soc
ial
basi
s. B
ecau
se B
lank
(na
me
of n
onpr
ofes
sion
al)
is li
ke a
frie
nd w
ith w
hom
I c
an h
ave
fun.
7.67
5.78
The
fact
tha
t th
e th
erap
eutic
set
ting
is in
Bec
ause
I go
to
Blan
k's (
nam
e of
pro
-
7.11
th
e pr
ofes
sion
al's
offic
e.
fess
iona
l) of
fice.
peut
ic s
ettin
g is
in th
e ch
ild's
en-
viro
nmen
t.
prof
essi
onal
) to
pla
ces
near
whe
re I
live
.
The
fact
that
the
nonp
rofe
ssio
nal
ther
a-
4.33
Bec
ause
I go
with
Bla
nk (
nam
e of
non-
7.00
3.09
9.00
4.36
9.18
3.73
5.00
5.
00
3.36
4.
08
3.91
* 6.
86
0,
4.w
4.
74
8.67
8.
19*
6.36
5.
10
'Hig
her
mea
n scores a
re in
dica
tive
of lo
wer
rank
ing.
*p
< .0
5.
w
w
\o
340 H E R B E R T H A R A K I , K A R E N MOSEY, A N D P A T R I C I A S H E E D Y
and educative way (statement #4) as of the highest importance to the child’s progress. At the same time, the following were viewed as least important considerations for the child’s progress: the lay status of the nonprofessional (statement #2) and the office setting of the professional (statement #9). Because of the interaction effect, however, the exact mean- ing of the above main effect findings remains somewhat unclear. On the other hand, Tukey’s multiple comparison (Linton & Gallo, 1975, pp. 316-3 19) showed significant differences between groups: The children considered the status of the professional (state- ment #7) significantly more important than did both the professionals and the non- professionals; while the professionals considered their own role of “being a professional” (statement # I ) to be a more important variable than did the children and the non- professionals.
Discussio~ This study had two major purposes: first, to test specific hypotheses of role percep-
tion and, second, to gain a greater understanding of the participants’ perception of the various elements constituting the respective roles of professional and nonprofessional therapists. The results indicated support for two of the three hypotheses, namely, that the professionals would tend to overestimate their own role performance, and that the children would tend to selectively value different aspects of each type of therapy. The childrens’ judgments were selective but nevertheless balanced-i.e., they did not rank one type of therapy over the other as more important (see Table I ) . This was a remarkable accomplishment since the experimental manipulation had made it virtually impossible for them to exercise such impartiality deliberately. The childrens’ balanced views, in con- trast to that of the therapists who inflated their own role importance, may not necessarily indicate that “the client knows best”-but they do provide some food for thought.
The third hypothesis which predicted that the nonprofessionals would underestimate the importance of their own role, was not supported. In fact, they rated their own role as significantly more important than that of the professional’s. Our initial thought was to attribute these findings to cognitive dissonance (Festinger, 1954). Since the measures were taken at the conclusion of their nonprofessional experience, the displayed role infla- tion may have reflected the nonprofessionals’ attempts to justify their considerable work and efforts for which they received no financial reimbursement. The brouble with cognitive dissonance theory, however, is that it thrives on post-hoc reasoning. By the same token, for example, it could be possible to explain the professionals’ inflation of their role by suggesting that being paid for what was essentially routine outpatient work caused them dissonance, which in turn led to unwarranted attributions of importance to what they were doing. Our view is that the experiences which the nonprofessional students had accumulated as members of the companionship program could at least par- tially account for the inflation of their own role. These experiences could have bolstered their personal self-esteem since their unique therapeutic contributions were stressed throughout their training and supervision, and competitive feelings toward professional therapists were discouraged. Unfortunately, the only way to have established the nature of the students’ self-esteem in their nonprofessional role compared with that of the professional would have called for pre- and post-training assessments. As an addendum to this study, we decided to collect rankings from inexperienced nonprofessionals, i.e., students who had entered the companionship therapy program subsequent to the ter- mination of the present study. The results of a re-analysis of the data strengthened our
V A L U E S AND ROLES 34 I
belief that the nonprofessionals would perceive their own role in an increasingly favorable light as they continued in the program.’
I n terms of further understanding the various role aspects of the therapeutic relationship, the significant disparity between the children and their therapists concern- ing their view of the professional’s directive role (statement #7) is particularly meaningful. It could reflect the general acceptable aversion among therapists to be perceived as directive and manipulative. On the other hand, it could very well be in- dicative of a genuine need for structured guidance among children in therapy. Closely related to this viewpoint are the higher rankings among the professionals for their “being-a-professional” role (statement #l). Apparently both professionals and their children-clients believe that something in the title of “professional” is an important com- ponent of the therapeutic process.
Increased understanding was also seen in the higher overall rating by all groups for the supportive and educative function of the nonprofessional (statement #4). This finding has some implications for those who are involved in work with nonprofessionals. It suggests that nonprofessionals, through their work within the childrens’ environment, are in a unique position to directly observe troublesome interpersonal relationships and other problems that may not come to the attention of the professional in the traditional office setting. Furthermore, it appears that nonprofessionals can make their greatest contribu- tion by educating the patient in socially acceptable behaviors, and by providing suppor- tive friendship in areas where professionals cannot.
The limitations of this study are several. For example, a larger number of par- ticipants was needed, and the sex and status of the therapists should have been con- trolled. While it was possible to randomly choose and assign persons for this study, the applied settings did not allow for other controls. A matter of central importance is the impossibility of knowing how important professionals or nonprofessionals actually were, since the data were subjective judgments. For example, one might argue that the children’s judgment of what is important could not safely be taken as the standard. But then again, the question arises whether “subjective” role perceptions by therapists are in any way different in kind from their diagnostic labelling or selected courses of therapy. At least from a social-psychological perspective, these perceptions can be described as reflecting certain realities of the clinical milieu.
REFERENCES
BI A L , T. H . The professional in the community views the nonprofessional helper: Psychology. Projessionul
B I Och, V. The study of attitudes about mental health in the community mental health center. Community
Cowtw, E. L., C H I N S ~ Y . J . M. , & RAPPAPORT, J . An undergraduate practicum in community mental
P.~ychology, 1969, I . 25-31.
Menial Healrh Journal. 1974, 10, 216-220.
health. Communiry Menral Health Journul, 1970, 6(2), 91-100.
‘A 4 X 2 mixed analysis (professionals, untrained nonprofessionals, trained nonprofessionals, and children-clients as the between factor; and professional therapy and nonprofessional therapy as within factors) showed a main effect for type of therapy, F ( I , 43) = 12.97. p < ,001; and a group membership X type of therapy interaction. F(3.43) = 1 3 . 5 3 , ~ < ,001. Subsequent specific comparisons with Duncan’s multiple range test (higher mean scores being indicative of lower ranking) showed that the inexperienced nonprofessionals viewed their own role as less important (M = 5.16) than that of their experienced countcrparts ( M = 4.0).
342 H E R B E R T H A R A R I , K A R E N MOSEY, A N D P A T R I C I A S H E E D Y
DURI.AK, J. A. Myths concerning the nonprofessional therapist. Professional Psychology. 1973.4. 300-304. FESTINCER, L. A theory of social comparison processes. Human Relations, 1954, 7, 117-140. GENTHER, R. Evaluating the functioning of community-based hotlines. Professional Psychology, 1974,
5. 409-414. GOLDENBERG, H. GRIJVER, G. G. Gur:RvEY, B. J .
KENISTON, K. LINTON, M., & GALI-O, P. S . The practical sratistician. Monterey, CA: Brooks/Cole, 1975. MEI.TZOFF, J., & KORNREICH, M. MITCHEI.1.. W. E. Amicatherapy: Theoretical perspectives and an example of practice. Community Mental
SOBEY. F. The nonprofessional revolution in mental health. New York: Columbia University Press, 1970. WlNER, B. J. Statistical principles in experimental design (2nd 4.). New York: McGraw-Hill, 1971.
Contemporary clinical psychology. Monterey. CA: Brooks/Cole, 1973. College students as therapeutic agents. Psychological Bulletin, 1971, 76, I 1 1-127. Psychotherapeutic agenu: New roles for nonprofessionals, parents, and teachers. New
york: Holt, Rinehart & Winston, 1969. College students and children in developmental institutions. Children, 1967, 14, 2-7.
Research in psychotherapy. New York: Atherton, 1970.
Health Journal, 1966, 2. 307-314.





























