Embed Size (px)
Citation preview
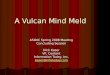
Representative photographs of the HE-stained liver sections of the normal, the placebo-treated, 10 mg/kg of TY-51469-treated, and 30 mg/kg of TY-51469-treated hamsters 24 hafter LPS/GalN injection. The original magnification was 400X. The scale bars are 50 μm.
Sa1013
Lambda Light Chain Myeloma-Related Hepatic Amyloidosis: A Rare Etiologyof Fatal Fulminant Liver FailureParit Mekaroonkamol, Manjula Balasubramanian, Simona Rossi
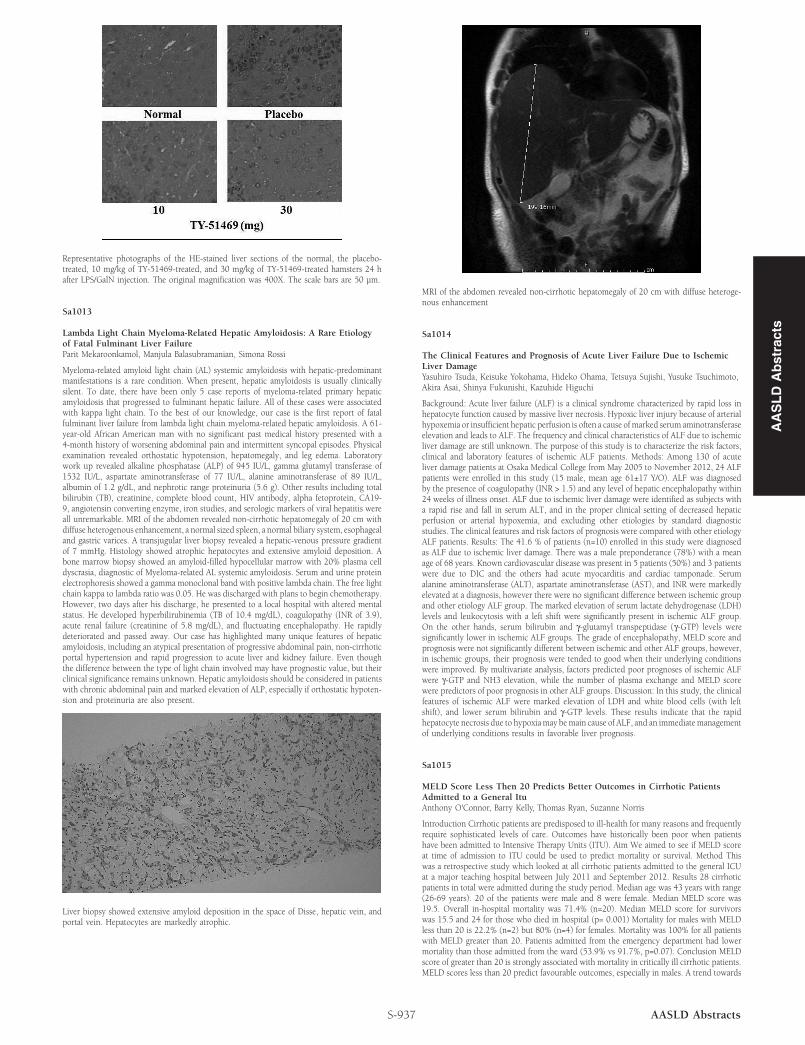
Myeloma-related amyloid light chain (AL) systemic amyloidosis with hepatic-predominantmanifestations is a rare condition. When present, hepatic amyloidosis is usually clinicallysilent. To date, there have been only 5 case reports of myeloma-related primary hepaticamyloidosis that progressed to fulminant hepatic failure. All of these cases were associatedwith kappa light chain. To the best of our knowledge, our case is the first report of fatalfulminant liver failure from lambda light chain myeloma-related hepatic amyloidosis. A 61-year-old African American man with no significant past medical history presented with a4-month history of worsening abdominal pain and intermittent syncopal episodes. Physicalexamination revealed orthostatic hypotension, hepatomegaly, and leg edema. Laboratorywork up revealed alkaline phosphatase (ALP) of 945 IU/L, gamma glutamyl transferase of1532 IU/L, aspartate aminotransferase of 77 IU/L, alanine aminotransferase of 89 IU/L,albumin of 1.2 g/dL, and nephrotic range proteinuria (5.6 g). Other results including totalbilirubin (TB), creatinine, complete blood count, HIV antibody, alpha fetoprotein, CA19-9, angiotensin converting enzyme, iron studies, and serologic markers of viral hepatitis wereall unremarkable. MRI of the abdomen revealed non-cirrhotic hepatomegaly of 20 cm withdiffuse heterogenous enhancement, a normal sized spleen, a normal biliary system, esophagealand gastric varices. A transjugular liver biopsy revealed a hepatic-venous pressure gradientof 7 mmHg. Histology showed atrophic hepatocytes and extensive amyloid deposition. Abone marrow biopsy showed an amyloid-filled hypocellular marrow with 20% plasma celldyscrasia, diagnostic of Myeloma-related AL systemic amyloidosis. Serum and urine proteinelectrophoresis showed a gamma monoclonal band with positive lambda chain. The free lightchain kappa to lambda ratio was 0.05. He was discharged with plans to begin chemotherapy.However, two days after his discharge, he presented to a local hospital with altered mentalstatus. He developed hyperbilirubinemia (TB of 10.4 mg/dL), coagulopathy (INR of 3.9),acute renal failure (creatinine of 5.8 mg/dL), and fluctuating encephalopathy. He rapidlydeteriorated and passed away. Our case has highlighted many unique features of hepaticamyloidosis, including an atypical presentation of progressive abdominal pain, non-cirrhoticportal hypertension and rapid progression to acute liver and kidney failure. Even thoughthe difference between the type of light chain involved may have prognostic value, but theirclinical significance remains unknown. Hepatic amyloidosis should be considered in patientswith chronic abdominal pain and marked elevation of ALP, especially if orthostatic hypoten-sion and proteinuria are also present.
Liver biopsy showed extensive amyloid deposition in the space of Disse, hepatic vein, andportal vein. Hepatocytes are markedly atrophic.
S-937 AASLD Abstracts
MRI of the abdomen revealed non-cirrhotic hepatomegaly of 20 cm with diffuse heteroge-nous enhancement
Sa1014
The Clinical Features and Prognosis of Acute Liver Failure Due to IschemicLiver DamageYasuhiro Tsuda, Keisuke Yokohama, Hideko Ohama, Tetsuya Sujishi, Yusuke Tsuchimoto,Akira Asai, Shinya Fukunishi, Kazuhide Higuchi
Background: Acute liver failure (ALF) is a clinical syndrome characterized by rapid loss inhepatocyte function caused by massive liver necrosis. Hypoxic liver injury because of arterialhypoxemia or insufficient hepatic perfusion is often a cause of marked serum aminotransferaseelevation and leads to ALF. The frequency and clinical characteristics of ALF due to ischemicliver damage are still unknown. The purpose of this study is to characterize the risk factors,clinical and laboratory features of ischemic ALF patients. Methods: Among 130 of acuteliver damage patients at Osaka Medical College from May 2005 to November 2012, 24 ALFpatients were enrolled in this study (15 male, mean age 61±17 Y/O). ALF was diagnosedby the presence of coagulopathy (INR > 1.5) and any level of hepatic encephalopathy within24 weeks of illness onset. ALF due to ischemic liver damage were identified as subjects witha rapid rise and fall in serum ALT, and in the proper clinical setting of decreased hepaticperfusion or arterial hypoxemia, and excluding other etiologies by standard diagnosticstudies. The clinical features and risk factors of prognosis were compared with other etiologyALF patients. Results: The 41.6 % of patients (n=10) enrolled in this study were diagnosedas ALF due to ischemic liver damage. There was a male preponderance (78%) with a meanage of 68 years. Known cardiovascular disease was present in 5 patients (50%) and 3 patientswere due to DIC and the others had acute myocarditis and cardiac tamponade. Serumalanine aminotransferase (ALT), aspartate aminotransferase (AST), and INR were markedlyelevated at a diagnosis, however there were no significant difference between ischemic groupand other etiology ALF group. The marked elevation of serum lactate dehydrogenase (LDH)levels and leukocytosis with a left shift were significantly present in ischemic ALF group.On the other hands, serum bilirubin and γ-glutamyl transpeptidase (γ-GTP) levels weresignificantly lower in ischemic ALF groups. The grade of encephalopathy, MELD score andprognosis were not significantly different between ischemic and other ALF groups, however,in ischemic groups, their prognosis were tended to good when their underlying conditionswere improved. By multivariate analysis, factors predicted poor prognoses of ischemic ALFwere γ-GTP and NH3 elevation, while the number of plasma exchange and MELD scorewere predictors of poor prognosis in other ALF groups. Discussion: In this study, the clinicalfeatures of ischemic ALF were marked elevation of LDH and white blood cells (with leftshift), and lower serum bilirubin and γ-GTP levels. These results indicate that the rapidhepatocyte necrosis due to hypoxia may be main cause of ALF, and an immediate managementof underlying conditions results in favorable liver prognosis.
Sa1015
MELD Score Less Then 20 Predicts Better Outcomes in Cirrhotic PatientsAdmitted to a General ItuAnthony O'Connor, Barry Kelly, Thomas Ryan, Suzanne Norris
Introduction Cirrhotic patients are predisposed to ill-health for many reasons and frequentlyrequire sophisticated levels of care. Outcomes have historically been poor when patientshave been admitted to Intensive Therapy Units (ITU). Aim We aimed to see if MELD scoreat time of admission to ITU could be used to predict mortality or survival. Method Thiswas a retrospective study which looked at all cirrhotic patients admitted to the general ICUat a major teaching hospital between July 2011 and September 2012. Results 28 cirrhoticpatients in total were admitted during the study period. Median age was 43 years with range(26-69 years). 20 of the patients were male and 8 were female. Median MELD score was19.5. Overall in-hospital mortality was 71.4% (n=20). Median MELD score for survivorswas 15.5 and 24 for those who died in hospital (p= 0.001) Mortality for males with MELDless than 20 is 22.2% (n=2) but 80% (n=4) for females. Mortality was 100% for all patientswith MELD greater than 20. Patients admitted from the emergency department had lowermortality than those admitted from the ward (53.9% vs 91.7%, p=0.07). Conclusion MELDscore of greater than 20 is strongly associated with mortality in critically ill cirrhotic patients.MELD scores less than 20 predict favourable outcomes, especially in males. A trend towards
AA
SL
DA
bst
ract
s

AA
SL
DA
bst
ract
sbetter outcomes in those admitted to ITU early in their presentation. Early ITU care isassociated with better outcomes for critically ill ITU patients with MELD scores less than 20.
Sa1016
Lessons Learned From Excess Mortality Due to Kpc-Producing Klebsiellapneumoniae in Liver Transplant RecipientsChristoph Lübbert, Arne C. Rodloff, Sven Laudi, Philipp Simon, Thilo Busch, JoachimMössner, Michael Bartels, Udo X. Kaisers
Background: Nosocomial infections in immunocompromised patients frequently originatefrom the Gram-negative bacterium Klebsiella pneumoniae (KP). Treatment options are con-siderably restricted by the emergence of carbapenem-resistant strains. Organ transplantrecipients are especially at risk for peri-interventional infections by multidrug-resistant bacte-ria, however, only little is known on the impact of K. pneumoniae carbapenemases (KPCs)producing pathogens in this setting yet. Materials & Methods: Among 103 patients eithercolonized or infected with KPC-2-producing KP (KPC-2-KP) during a large hospital outbreak,we identified 9 KPC-positive patients, who had undergone orthotopic liver transplantation(LTx) between 15.09.2010 and 14.09.2011 at the Leipzig University Hospital, Germany.Presence of KPC-2-KP was confirmed by culture and molecular typing was performed usingpulsed-field gel-electrophoresis (PFGE). The data from these n = 9 LTR were retrospectivelycompared to a matched cohort of n = 35 LTR (transplanted from 2008 to 2011) with proofof invasive infections due to carbapenem-susceptible Klebsiella spp. strains (69% KP, 31%K. oxytoca), including a high proportion of ESBL-producers (71%). All patients were followedup for 6 months after LTx. Results: 89% (8/9) of KPC-2-KP-positive LTR progressed toinfection (50% pneumonia, 25% surgical site infections, 25% tertiary peritonitis), and in 56%(5/9) bloodstream infection with KPC-2-KP was confirmed. Matched comparison showed ahospital mortality rate of 78% (LTR with KPC-2-KP) compared to 34% in the remainingpatients (P=0.027). Six-month survival in KPC-positive LTR (22%) was significantly lowercompared to LTR with sensitive Klebsiella strains (70%), and LTR with ESBL-producingKlebsiella strains (64%) (P<0.05) (FIGURE). Conclusion: We conclude that colonizationwith carbapenem-resistant Enterobacteriaceae (CRE) like KPC-2-KP in LTR leads to highinfection rates and excess mortality. Therefore, frequent screening for CRE in patients onLTx waiting lists appears reasonable. Although active surveillance studies have demonstratedhigh infection rates associated with excess mortality, colonization with CRE is so far notconsidered a contraindication to LTx. This position might need re-evaluation with respectto the fundamental difficulties of graft allocation due to severe organ shortage in countrieslike Germany. In our opinion, currently available data do not justify to consider patientswith end-stage liver disease and evidence of persistent colonization by CRE failing decoloniza-tion efforts for LTx.
FIGURE: Kaplan-Meier survival curves for LTR with invasive Klebsiella spp. infections. Six-month survival in LTR with KPC-2-KP was significantly lower compared to LTR with sensitiveKlebsiella strains (SEN Klebsiella spp., P=0.018) and patients with ESBL-producing Klebsiellastrains (ESBL Klebsiella spp., P=0.005) (Cox-Mantel log rank statistics including multiplecomparisons with application of the Holm-Bonferroni method).
Sa1017
Effects of Hyperbaric Oxygen Therapy on the Liver After Induction of theHepatic Ischemia/Reperfusion ComplexNathalia M. Cardoso, Daniela Antoniali, Ricardo Nejo Júnior, Leticia B. Baldim, Marina R.Silveira, Orlando Castro-e-Silva, Omar Feres
Introduction: Hyperbaric oxygen (HBO) therapy is a specific type of treatment of variousdisorders of hypoxia using oxygen under hyperbaric conditions, increasing the quantity ofoxygen dissolved in blood and in body tissues (Henry's Law) and promoting high tissueoxygen tension. Thus, the objective of the present study was to determine the effects ofHBO in rats submitted to hepatic ischemia/reperfusion. Method: Twenty-three Wistar ratswere divided at random into 3 groups:: SHAM, rats submitted to surgical and anestheticstress without the induction of hepatic ischemia and reperfusion (I/R); I/R, rats submittedto total ischemia of the hepatic pedicle for 25 min followed by 5 min of reperfusion; HBOI/R, rats submitted to 60 min of HBO therapy at the pressuure of 2 absolute atmospheresimmediately after the experimental I/R protocol. Hepatic function was determined by quanti-tating serum alanine aminotransferase (ALT) and aspartate aminotransferase (AST) and bythe determination of states 3 and 4 of mitochondrial respiration, of the respiratory controlratio (RCR) and of the transition of mitochondrial permeability (mitochondrial swelling).Data were analyzed statistically by the Mann-Whitney test, with the level of significance set
S-938AASLD Abstracts
at p <0.05. Results: there was a significant difference in state 3 values between the SHAMand I/R groups and between the IR and IRHBO groups, in state 4 values between the SHAMand IR groups, and in mitochondrial swelling between the the SHAM and I/RHBO, SHAMand I/R and IR and IRHBO groups. Conclusion: The use of HBO after IR increased theproduction of hepatocellular energy and also stabilized the permeability of the mitochondriaolmembrane, reducing the mitochondrial edema induced by I/R.
Sa1018
Description of Two New Formulas As a Predictive Index of Mortality AfterOrthotopic Liver Transplantation: MELD Lactate V3 and MELD Lactate V4Tiago Silva, Nathalia M. Cardoso, Daniela Antoniali, Anibal Basile-Filho, Enio DavidMente, Orlando Castro-e-Silva
Introduction: The Model for End Stage Liver Disease (MELD) has been used for organallocation and as a predictor of mortality after orthotopic liver transplantation (OLT). OLTshows survival rates of about 80%, ranging from 65 to 90% in the first 3 years and, dueto the high complexity of the surgery, the mortality rates during the first 30 postoperativedays range from 5 to 10%. Because of the limitations of MELD in predicting short-termpostoperative complications, several studies have been conducted in order to improve it asa predictive index, although still with important limitations. Objective: To elaborate a newmathematical model for the determination of prognosis during the first 30 days after OLTand to compare two versions of the model created. Method: The study was conducted on58 patients submitted to OLT at the University Hospital, between October 2008 and March2012. The last 29 patients who survived and the last 29 who died within the first 30postoperative days were selected. Lactate, INR, total bilirubin and creatinine concentrationswere determined in all patients during the immediate postoperative period. Original MELD,MELD lactate V3 and MELD lactate V4 values were calculated for the study groups. Results:The models elaborated were: MELD Lactate V3 = 6.80 x loge (creatinine) + 2.42 x loge(bilirubin) + 10.3 x loge (INR) + 9.8 x loge (lactate) and MELD Lactate V4 = MELD lactate =2.68 + 5.68 x loge (lactate) + 0.64 x (original MELD). When MELD V3 and V4 were used,statistically significant differences (P <0.05) were detected in the individual distribution ofthe values between survivors and non-survivors, with higher postoperative levels for thepatients who died. When the ROC curves for sensitivity and specificity were compared, anAUC of 0.80 was obtained for V3, of 0.85 for V4 and of 0.69 for the original MELD.Conclusion: Both MELD lactate formulas were more efficient than the original MELD forthe determination of post-OLT prognosis. The V4 version was significantly better as apredictive index of evolution during the first 30 postoperative days.
Sa1019
Evaluation of DELTA (MELD, Meld Lactate V3 and MELD Lactate V4)Tiago Silva, Nathalia M. Cardoso, Daniela Antoniali, Anibal Basile-Filho, Enio DavidMente, Orlando Castro-e-Silva
Intruduction: The Model for End Stage Liver Disease (MELD) has been used for organallocation and as a predictor of mortality after orthotopic liver transplantation (OLT). OLTshows survival rates of about 80%, ranging from 65 to 90% in the first 3 years and, dueto the high complexity of the surgery, the mortality rates during the first 30 postoperativedays range from 5 to 10%. Because of the limitations of MELD in predicting short-termpostoperative complications, several studies have been conducted in order to improve it asa predictive index, although still with important limitations.In a previous study, we deter-mined that both Meld Lactate V3 and Meld Lactate V4 proved to be sensitive as predictiveindices of patient evolution after OLT. Objective: In view of the importance of the effect ofhepatic ischemia in the ischemia and reperfusion phase, our objective was to determine thedifference between the preoperative and postoperative results of the original Meld, MeldLactate V3 and Meld Lactate V4. Method: The study was conducted on 78 patients submittedto OLT at between October 2008 and March 2012. The last 49 patients who survived andthe last 29 who died within the first 30 postoperative days were selected. Original Meld,Meld Lactate V3 and Meld Lactate V4 values were calculated before and immediately aftersurgery for the two groups. At the end, we also calculated the difference between the pre-and postoperative values (Delta = post-pre) for the two study groups. Results: The OriginalMeld did not differ significantly between the patients who survived and those who died(p>0.05). Both the Meld Lactate V3 and Meld Lactate V4 showed a significant differencebetween the patients who survived and those who died (p<0.05). Conclusion: Both versionsof the Meld Lactate formulas showed a significant difference between the Delta = post-prevalues of the patients who survived and those who died 30 days after OLT. Thus, V3 andV4 are more sensitive than the Origuinal Meld for the determination of prognosis 30 daysafter OLT.
Sa1020
Hyperoxic Preconditioning in Partial Liver IschemiaMaria Rita R. Margarido, Maria Eliza Jordani de Souza, Clarice F. Fina, Maria AparecidaNeves Cardoso Picinato, Maria Cecilia Jordani Gomes, José Carlos Vanni, Orlando Castro-e-Silva
INTRODUCTION: In ischemia-reperfusion (I/R), hepatic injury occurs due to temporarydeprivation of blood flow to the liver, as observed in hepatectomies and in liver transplants.Hyperbaric oxygen (HBO) is a specific type of treatment of several hypoxia disorders consist-ing of the use of oxygen under hyperbaric conditions, increasing the quantity of oxygendissolved in blood and in body tissues (Henry's Law) and promoting high tissue oxygentension. The objective of the present study was to use HBO as hyperoxic preconditioningin rats submitted to hepatic ischemia followed by reperfusion. METHOD: Twenty-threeWistar rats were divided at random into 3 groups: SHAM, rats submitted to surgical andanesthetic stress without the induction of I/R; I/R, rats submitted to partial ischemia of 70%of the liver, with 30% of hepatic tissue being perfused; HBOI/R, rats submitted to 60 minof HBO at the pressure of 2 absolute atmospheres immediately before the experimental I/







![Antibiotic prophylaxis for cirrhotic patients with upper ...[Intervention Review] Antibiotic prophylaxis for cirrhotic patients with upper gastrointestinal bleeding Norberto C Chavez-Tapia1,](https://img.pdfslide.net/doc/110x75/5e937e618bf0364d7d5b6953/antibiotic-prophylaxis-for-cirrhotic-patients-with-upper-intervention-review.jpg)