Embed Size (px)
Citation preview
Safety of Vaccines Used for Routine Immunization ofUS Children: A Systematic Review
abstractBACKGROUND: Concerns about vaccine safety have led some parentsto decline recommended vaccination of their children, leading to theresurgence of diseases. Reassurance of vaccine safety remains criticalfor population health. This study systematically reviewed the literatureon the safety of routine vaccines recommended for children in theUnited States.
METHODS: Data sources included PubMed, Advisory Committee on Im-munization Practices statements, package inserts, existing reviews,manufacturer information packets, and the 2011 Institute of Medicineconsensus report on vaccine safety. We augmented the Institute of Med-icine report with more recent studies and increased the scope to in-clude more vaccines. Only studies that used active surveillance and hada control mechanism were included. Formulations not used in theUnited States were excluded. Adverse events and patient and vaccinecharacteristics were abstracted. Adverse event collection and report-ing was evaluated by using the McHarm scale. We were unable to poolresults. Strength of evidence was rated as high, moderate, low, or in-sufficient.
RESULTS: Of 20 478 titles identified, 67 were included. Strength ofevidence was high for measles/mumps/rubella (MMR) vaccine andfebrile seizures; the varicella vaccine was associated with complicationsin immunodeficient individuals. There is strong evidence that MMRvaccine is not associated with autism. There is moderate evidencethat rotavirus vaccines are associated with intussusception. Limitationsof the study include that the majority of studies did not investigate oridentify risk factors for AEs; and the severity of AEs was inconsistentlyreported.
CONCLUSIONS: We found evidence that some vaccines are associatedwith serious AEs; however, these events are extremely rare and mustbe weighed against the protective benefits that vaccines provide.Pediatrics 2014;134:1–13
AUTHORS: Margaret A. Maglione, MPP,a Lopamudra Das,MPH,a Laura Raaen, MPH,a Alexandria Smith, MPH,a RamyaChari, PhD,a Sydne Newberry, PhD,a Roberta Shanman,MLS,a Tanja Perry, BHM,a Matthew Bidwell Goetz, MD,b andCourtney Gidengil, MD, MPHa,c
aRAND Corporation, Santa Monica, California; bVA Greater LosAngeles Healthcare System and David Geffen School of Medicine,University of California, Los Angeles, Los Angeles, California; andcBoston Children’s Hospital, Boston, Massachusetts
KEY WORDSevidence-based medicine, vaccine/immunization, infectiousdisease
ABBREVIATIONSAEs—adverse eventsAHRQ—Agency for Healthcare Research and QualityCI—confidence intervalDTaP—diphtheria, tetanus, and acellular pertussisH1N1—Swine FluHib—Haemophilus influenza type bILI—influenza-like illnessIOM—Institute of MedicineIPV—inactivated poliovirusIRR—incidence rate ratioLAIV—live attenuated vaccineMMR—measles/mumps/rubellaOka VZV—Oka strain varicella zoster virusOR—odds ratioPCV—pneumococcal conjugate vaccinePRISM—Post-Licensure Rapid Immunization Safety MonitoringTd—tetanus-diphtheriaTIV—trivalent inactivated vaccineVSD—Vaccine Safety Datalink
Ms Maglione conceptualized and designed the study, oversawthe abstraction of data, interpreted the results, and drafted themanuscript; Ms Das abstracted data, interpreted results, andrevised the manuscript; Ms Raaen abstracted data, interpretedresults, and revised the manuscript; Ms Smith designed datacollection instruments, analyzed data, and revised themanuscript; Dr Chari abstracted data, interpreted results, andrevised the manuscript; Dr Newberry revised the manuscript forimportant content and approved the final manuscript assubmitted; Ms Shanman developed the literature searchstrategy, conducted electronic literature searches, and acquireddata; Ms Perry acquired data and designed screening and dataabstraction forms; Dr Goetz contributed to the conceptualizationand design of the study, interpreted results, and criticallyreviewed and revised the manuscript; Dr Gidengil participatedin study design, interpreted the results, drafted part of themanuscript, and critically reviewed the manuscript, and allauthors approved the final manuscript as submitted.
(Continued on last page)
PEDIATRICS Volume 134, Number 2, August 2014 1
REVIEW ARTICLE
by guest on September 8, 2018www.aappublications.org/newsDownloaded from

Vaccines are considered one of thegreatest public health achievements ofthe 20th century for their role ineradicating smallpox and controllingpolio, measles, rubella, and other in-fectious diseases in the United States.1
Despite their effectiveness in prevent-ing and eradicating disease, routinechildhood vaccine uptake remains sub-optimal. Parent refusal of vaccines hascontributed to outbreaks of vaccine-preventable diseases such as measles2
and pertussis.3 In addition, althoughmultiple large studies have confirmedthe lack of association betweenmeasles/mumps/rubella (MMR) and autism, pa-rental worries about the safety of vac-cines persist.
The Agency for Healthcare Researchand Quality (AHRQ) requested an evi-dence report on the safety of vaccinesrecommended for routine immuniza-tion of adults (including pregnantwomen), children, and adolescents tobe used by the Office of the AssistantSecretary of Health to identify the gapsin evidence. This article addresses thesafety of vaccines recommended forroutineuse in childrenaged6 yearsandyounger: DTaP (diphtheria, tetanus, andacellular pertussis), hepatitis A, hepa-titis B, Haemophilus influenza type b(Hib), influenza (live attenuated andinactivated), meningococcal (conjugateor polysaccharide), MMR, pneumococ-cal (conjugate or polysaccharide), ro-tavirus, and varicella. It represents theresults of a comprehensive and sys-tematic review of scientific evidence,describes statistical associations be-tween vaccines and adverse events(AEs), and reports on any risk factorsidentified.
METHODS
In 2011, the Institute of Medicine (IOM)published a consensus report titled Ad-verse Effects of Vaccines: Evidence andCausality.4 That report evaluated thescientific evidence for AEs potentially
associated with varicella, influenza, hep-atitis A, hepatitis B, human papilloma-virus, MMR, meningococcal, tetanus,diphtheria, and pertussis vaccines. Wereport the IOM findings regardingchildren and update those findings byidentifying and evaluating studiespublished after the IOM searches. Wealso identify studies and evaluate evi-dence on pneumococcal, rotavirus,Hib, and inactivated poliovirus (IPV)vaccines because these are recom-mended for children aged 6 years andyounger.
The following databaseswere searched:DARE (Database of Abstracts of Reviewsof Effects), the Cochrane Database ofSystematic Reviews, CENTRAL, PubMed,Embase, CINAHL (Cumulative Index toNursing and Allied Health), TOXLINE(Toxicology Literature Online), andTOXFILE. The IOM report, AdvisoryCommittee on Immunization Practicesstatements, vaccine package inserts,and review articles were mined forstudies. Using the IOM keyword searchstrategy, we updated their searches toidentify more recently publishedstudies. The following structure wasused: “vaccine term” AND “health term,”where vaccine terms include the tech-nical vaccine name, general descrip-tions of the vaccine of interest (eg,rotavirus AND vaccine), or manufac-turer names; health terms include a listof AEs potentially associated with thevaccine. We also added more general AEkeywords to the list of health termssuch as “safe” or “safety,” “side effect”or “harm.” We searched from a yearbefore the publication of the IOM reportthrough August 2013. Using this ap-proach, we developed new searchstrategies for the vaccines not originallyincluded in the IOM report and searchedeach database from its inceptionthrough August 2013. AE terms werebased on AEs reported in systemssuch as the Vaccine Injury Compensa-tion Program, Vaccine Adverse Event
Reporting System, and the Food andDrug Administration’s Mini-SentinelProgram. A Technical Expert Panelreviewed the draft list of AEs andsuggested additional AEs of interest.
We included studies that used activesurveillance and had a control mech-anism; eligible designs were controlledtrials, cohorts comparing a vaccinatedwith nonvaccinated group, case–controlstudies, self-controlled case series,and observational studies that usedregression to control for confoundersand test multiple relationships simul-taneously (multivariate risk factoranalyses). Common sources of dataincluded medical records, health in-surance claims, and government reg-istries.
To maintain applicability to the currentUS context, we excluded studies ofvaccine formulations never used or nolonger available in the United States;examples include whole cell pertussisvaccine, oral polio vaccine, and pneu-mococcal conjugate vaccine (PCV)7vaccine. The recent IOM report, TheChildhood Immunization Schedule andSafety: Stakeholder Concerns, Scien-tific Evidence, and Future Studies,5
makes recommendations for future re-search on childhood vaccine schedulesand cumulative effect, so the currentproject focused on specific vaccines,rather than any cumulative effect.
Two researchers experienced in sys-tematic review methodology inde-pendently reviewed the titles andabstracts identified. The union of theirselections was retrieved. These re-searchers independently reviewed thefull text of study reports and met toreach consensus regarding exclusion/inclusion. Disputes were settled bythe lead investigators and team physi-cian experts. Patient and study char-acteristics were abstracted by singleresearchers and confirmed by theproject leader. If a study reported se-verity or if adequate information was
2 MAGLIONE et al by guest on September 8, 2018www.aappublications.org/newsDownloaded from

provided for our investigators to cate-gorize severity, we used the CommonTerminology Criteria for Adverse Eventsclassification system6 to characterizeAEs. The definition of “serious” differsby AE type; each category of AE (ie fever,headache) is rated on a 5-point scale,with 1 being very mild and 5 beingdeath due to the event.
The McHarm instrument7 was used toevaluate the quality of the studies withregard to their assessment of AEs.Studies that reported timing and se-verity and defined AEs using standard,precise definitions were rated higherthan those that did not. We assessedthe overall strength of evidence by us-ing guidance suggested by AHRQ for itsEffective Health Care Program8 as of2013. (The guidance has since beenmodified slightly.) The method is basedon one developed by the Grading ofRecommendations Assessment Work-ing Group9 and classifies the evidencebased on risk of bias, consistency, di-rectness, precision, dose–response,plausible confounders that would de-crease the observed effect, strength ofassociation, and publication bias. Pos-sible ratings are as follows:
High = High confidence that the ev-idence reflects the true effect. Fur-ther research is very unlikely tochange our confidence in the esti-mate of effect.
Moderate = Moderate confidencethat the evidence reflects the trueeffect. Further research may changeour confidence in the estimate ofeffect and may change the estimate.
Low = Low confidence that the ev-idence reflects the true effect. Fur-ther research is likely to changeour confidence in the estimate ofeffect and is likely to change theestimate.
Insufficient = Evidence either is un-available or does not permit a con-clusion.
It is important to note that the 2011 IOMreport used different terminology toclassify the strength of evidence; evi-dence was classified as either “convinc-ingly supports,” “favors acceptance,”“inadequate to accept or reject,” or“favors rejection” of a causal associa-tion. They also included mechanisticstudies and individual case reports toassess the biological plausibility of AEand considered this in addition to anystatistical association. For each vaccinediscussed in the IOM report, we startedwith the IOM findings andmodified them,if needed, on the basis of any additionalevidence we identified.
RESULTS
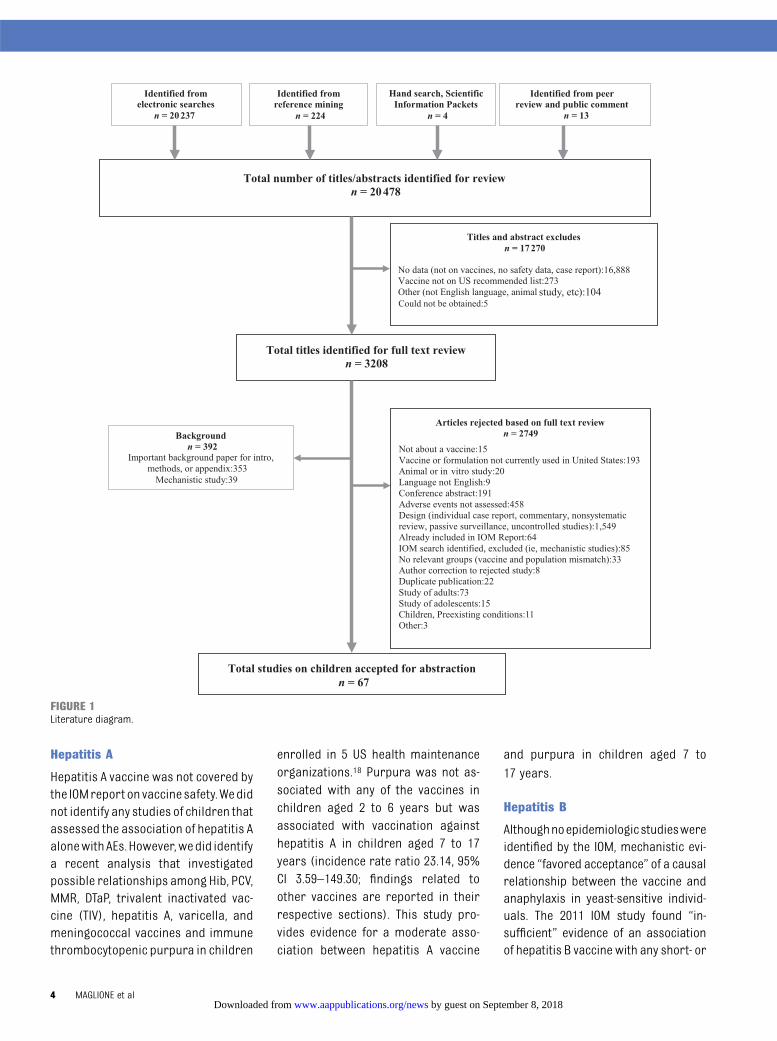
As presented in Fig 1, 20 478 titles wereidentified through electronic literaturesearches; review of product inserts;review of Food and Drug Administra-tion, Advisory Committee on Immuni-zation Practices, and other Web sites;reference mining; and requests forScientific Information Packets fromdrug manufacturers. Of those, 17 270were excluded on review of abstract ortitle for reasons such as “not abouta vaccine,” “vaccine not within thescope of this project” (formulationsnever available in the United States,recommended only for travel), or be-cause they were animal studies. Uponfull text review of the remaining 3208articles, 392 were identified as relevantbackground/theoretical materials andset aside as potential references forthe Introduction; 2749 other articleswere excluded. The most commonreason for exclusion was lack of suit-able study design (1549): individualcase reports, nonsystematic reviews,and studies using passive surveillancewere excluded. Many publications(458) discussed vaccines on the rec-ommended schedule but did not reportor assess AEs. Eighty-eight studies onadults or adolescents were excludedfor this article, as were 11 studies of
children with preexisting conditionssuch as HIV, juvenile arthritis, orcancer, which left 67 studies. Thesestudies are in addition to those in-cluded in the 2011 IOM consensusreport Adverse Effects of Vaccines:Evidence and Causality, which werenot abstracted.
We present the results for each vaccinein alphabetical order. Results aresummarized in Table 1.
DTaP
The IOM studied diphtheria toxoid,tetanus toxoid, and acellular pertussis-containing vaccines alone and in com-bination inbothchildrenandadults. TheIOM committee did not find evidencethat “favors acceptance” of causalrelationships for any conditions. Theyfound the evidence “favors rejection” ofa causal relationship between type 1diabetes and vaccines containingdiphtheria toxoid, tetanus toxoid, andacellular pertussis antigens.10–14 Wefound no additional studies in childrenpublished after the IOM search date;our review of their assessment sup-ports their conclusions.
Hib Vaccine
The IOM did not study the safety of Hibvaccine.We identified 3 controlled trialsof the Hib vaccine in children15–17; 1 wasset in the United States, the other 2 inAsia. Results of the US trial (N = 5190)indicated that Hib vaccination was as-sociated with redness (odds ratio [OR]2.71, 95% confidence interval [CI] 1.57–4.67) and swelling (OR 9.44, 95% CI4.90–18.19) but not with hospital-izations. Vaccination was not associ-ated with high fever in either the UStrial or a trial in the Philippines. A trialin Vietnam15 found the vaccine was notassociated with any serious AEs, in-cluding convulsion, diarrhea, fungalinfection, or gastroesophageal refluxdisease. No other AEs were associatedwith the Hib vaccination.
REVIEW ARTICLE
PEDIATRICS Volume 134, Number 2, August 2014 3 by guest on September 8, 2018www.aappublications.org/newsDownloaded from
Hepatitis A
Hepatitis A vaccine was not covered bythe IOMreport on vaccine safety.Wedidnot identify any studies of children thatassessed the association of hepatitis AalonewithAEs.However,wedid identifya recent analysis that investigatedpossible relationships among Hib, PCV,MMR, DTaP, trivalent inactivated vac-cine (TIV), hepatitis A, varicella, andmeningococcal vaccines and immunethrombocytopenic purpura in children
enrolled in 5 US health maintenanceorganizations.18 Purpura was not as-sociated with any of the vaccines inchildren aged 2 to 6 years but wasassociated with vaccination againsthepatitis A in children aged 7 to 17years (incidence rate ratio 23.14, 95%CI 3.59–149.30; findings related toother vaccines are reported in theirrespective sections). This study pro-vides evidence for a moderate asso-ciation between hepatitis A vaccine
and purpura in children aged 7 to
17 years.
Hepatitis B
Althoughnoepidemiologicstudieswereidentified by the IOM, mechanistic evi-dence “favored acceptance” of a causalrelationship between the vaccine andanaphylaxis in yeast-sensitive individ-uals. The 2011 IOM study found “in-sufficient” evidence of an associationof hepatitis B vaccine with any short- or
FIGURE 1Literature diagram.
4 MAGLIONE et al by guest on September 8, 2018www.aappublications.org/newsDownloaded from
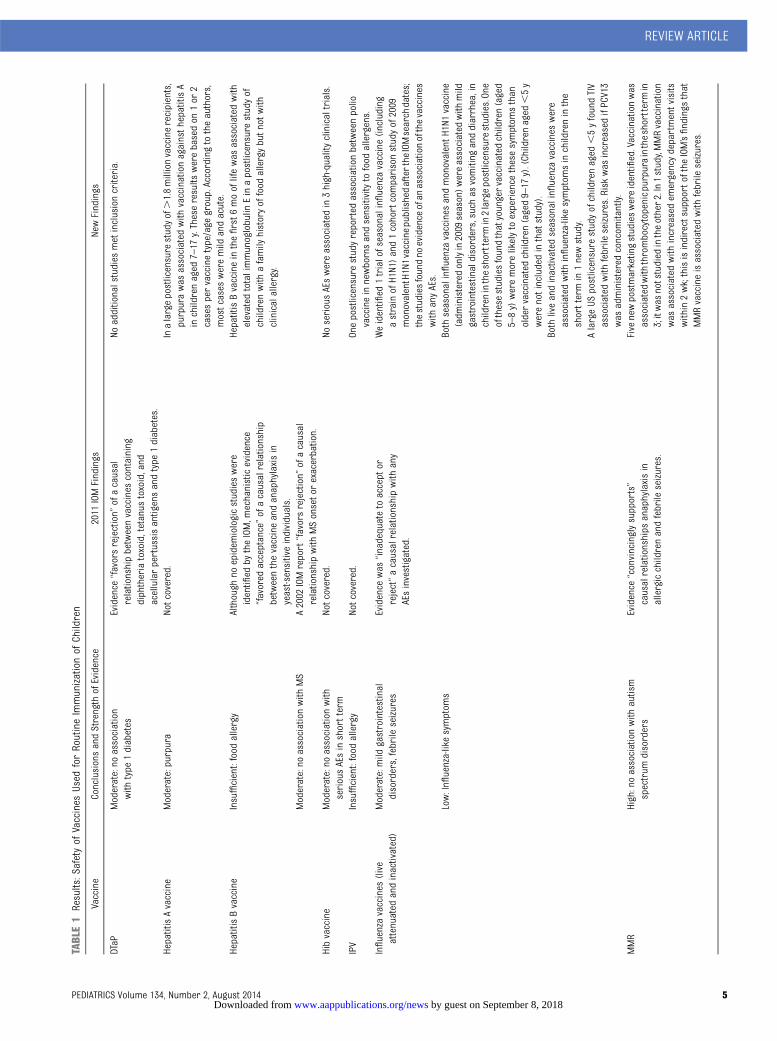
TABLE1
Results:S
afetyof
Vaccines
Used
forRoutineImmunizationof
Children
Vaccine
ConclusionsandStrength
ofEvidence
2011
IOMFindings
NewFindings
DTaP
Moderate:no
association
with
type
1diabetes
Evidence
“favorsrejection”
ofacausal
relationshipbetweenvaccines
containing
diphtheriatoxoid,tetanus
toxoid,and
acellularpertussisantigensandtype
1diabetes.
Noadditionalstudies
metinclusioncriteria.
HepatitisAvaccine
Moderate:purpura
Notcovered.
Inalargepostlicensure
studyof.1.8millionvaccinerecipients,
purpurawas
associated
with
vaccinationagainsth
epatitisA
inchildrenaged
7–17
y.Theseresults
werebasedon
1or
2casespervaccinetype/age
group.Accordingtotheauthors,
mostcases
weremild
andacute.
HepatitisBvaccine
Insufficient:food
allergy
Although
noepidem
iologicstudieswere
identified
bytheIOM,m
echanisticevidence
“favored
acceptance”ofacausalrelationship
betweenthevaccineandanaphylaxisin
yeast-sensitiveindividuals.
HepatitisBvaccineinthefirst6
mooflifewas
associated
with
elevated
totalimmunoglobulin
Einapostlicensure
studyof
childrenwith
afamily
historyoffood
allergybutn
otwith
clinicalallergy.
Moderate:no
associationwith
MS
A2002
IOMreport“favorsrejection”
ofacausal
relationshipwith
MSonsetorexacerbation.
Hibvaccine
Moderate:no
associationwith
seriousAEsinshortterm
Notcovered.
NoseriousAEswereassociated
in3high-qualityclinicaltrials.
IPV
Insufficient:food
allergy
Notcovered.
Onepostlicensure
studyreported
associationbetweenpolio
vaccineinnewbornsandsensitivityto
food
allergens.
Influenzavaccines
(live
attenuated
andinactivated)
Moderate:mild
gastrointestinal
disorders,febrile
seizures
Evidence
was
“inadequatetoaccept
orreject”acausalrelationshipwith
any
AEsinvestigated.
Weidentified
1trialofseasonalinfluenzavaccine(including
astrainofH1N1)and1cohortcomparisonstudyof2009
monovalentH1N1vaccinepublishedafterthe
IOMsearch
dates;
thestudiesfoundno
evidence
ofan
associationofthevaccines
with
anyAEs.
Low:Influenza-likesymptom
sBoth
seasonalinfluenzavaccines
andmonovalentH
1N1vaccine
(adm
inisteredonlyin2009
season)w
ereassociated
with
mild
gastrointestinaldisorders,such
asvomiting
anddiarrhea,in
childrenintheshorttermin2largepostlicensurestudies.One
ofthesestudiesfoundthatyoungervaccinated
children(aged
5–8y)weremorelikelyto
experience
thesesymptom
sthan
oldervaccinated
children(aged9–17
y).(Childrenaged
,5y
werenotincludedinthatstudy).
Both
liveandinactivated
seasonalinfluenzavaccines
were
associated
with
influenza-likesymptom
sinchildreninthe
shorttermin1newstudy.
AlargeUS
postlicensure
studyofchildrenaged
,5yfoundTIV
associated
with
febrile
seizures.Riskwas
increasedifPCV13
was
administeredconcom
itantly.
MMR
High:noassociationwith
autism
spectrum
disorders
Evidence
“convincinglysupports”
causalrelationships
anaphylaxisin
allergicchildrenandfebrile
seizures.
Five
newpostmarketingstudieswereidentified.Vaccinationwas
associated
with
thrombocytopenicp
urpuraintheshorttermin
3;itwas
notstudied
intheother2.In1study,MMRvaccination
was
associated
with
increasedem
ergencydepartmentvisits
within2wk;thisisindirectsupportofthe
IOM’sfindings
that
MMRvaccineisassociated
with
febrile
seizures.
REVIEW ARTICLE
PEDIATRICS Volume 134, Number 2, August 2014 5 by guest on September 8, 2018www.aappublications.org/newsDownloaded from
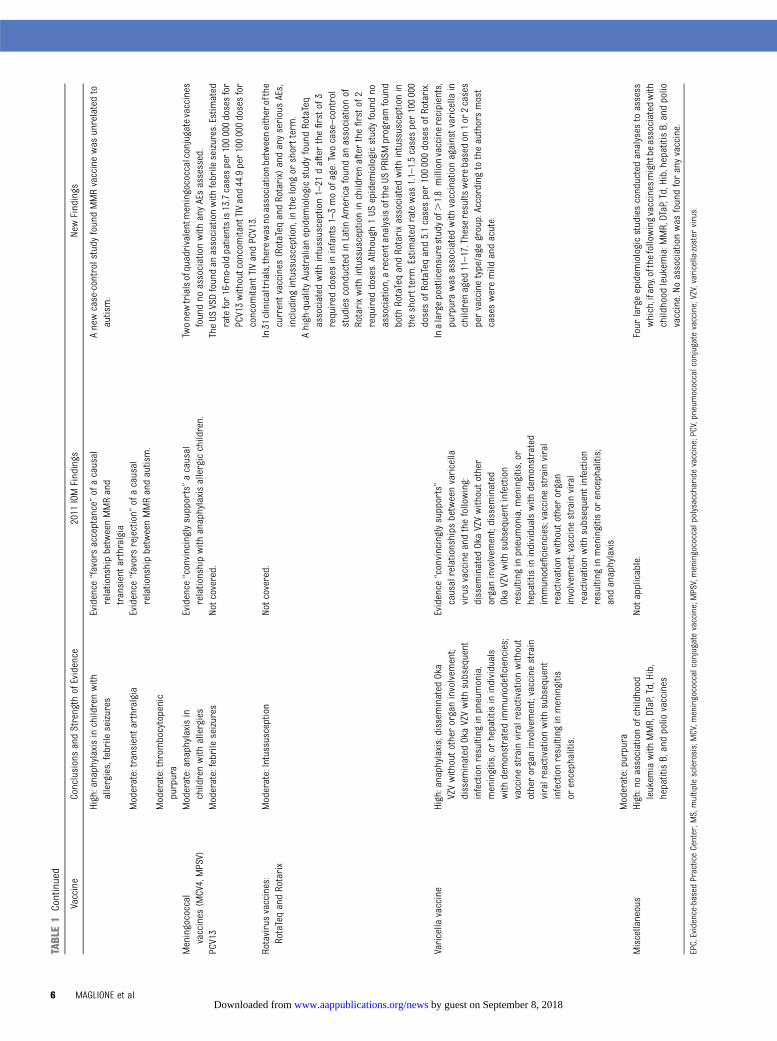
TABLE1
Continued
Vaccine
ConclusionsandStrength
ofEvidence
2011
IOMFindings
NewFindings
High:anaphylaxisinchildrenwith
allergies,febrile
seizures
Evidence
“favorsacceptance”ofacausal
relationshipbetweenMMRand
transientarthralgia
Anewcase-controlstudyfoundMMRvaccinewas
unrelatedto
autism.
Moderate:transientarthralgia
Evidence
“favorsrejection”
ofacausal
relationshipbetweenMMRandautism.
Moderate:thrombocytopenic
purpura
Meningococcal
vaccines
(MCV4,MPSV)
Moderate:anaphylaxisin
childrenwith
allergies
Evidence
“convincinglysupports”acausal
relationshipwith
anaphylaxisallergicchildren.
Twonewtrialsofquadrivalentmeningococcalconjugatevaccines
foundno
associationwith
anyAEsassessed.
PCV13
Moderate:febrile
seizures
Notcovered.
TheUS
VSDfoundan
associationwith
febrile
seizures.Estimated
ratefor16-mo-oldpatientsis13.7casesper100000dosesfor
PCV13withoutconcomitantTIVand44.9per100000dosesfor
concom
itant
TIVandPCV13.
Rotavirusvaccines:
RotaTeqandRotarix
Moderate:Intussusception
Notcovered.
In31
clinicaltrials,therewas
noassociationbetweeneitherofthe
currentvaccines
(RotaTeq
andRotarix)andanyseriousAEs,
includingintussusception,inthelong
orshortterm.
Ahigh-qualityAustralianepidem
iologicstudyfoundRotaTeq
associated
with
intussusception1–21
dafterthefirstof3
required
dosesininfants1–3moofage.Twocase–control
studiesconductedinLatin
Americafoundan
associationof
Rotarixwith
intussusceptioninchildrenafterthefirstof2
required
doses.Although
1US
epidem
iologicstudyfoundno
association,arecentanalysisoftheUS
PRISMprogramfound
both
RotaTeqandRotarixassociated
with
intussusceptionin
theshortterm.Estimated
ratewas
1.1–1.5casesper100000
dosesofRotaTeqand5.1casesper100000dosesofRotarix.
Varicella
vaccine
High:anaphylaxis;disseminated
Oka
VZVwithoutother
organinvolvem
ent;
dissem
inated
OkaVZVwith
subsequent
infectionresulting
inpneumonia,
meningitis,orhepatitisinindividuals
with
demonstratedimmunodeficiencies;
vaccinestrainviralreactivationwithout
otherorganinvolvem
ent;vaccinestrain
viralreactivationwith
subsequent
infectionresulting
inmeningitis
orencephalitis.
Evidence
“convincinglysupports”
causalrelationships
betweenvaricella
virusvaccineandthefollowing:
dissem
inated
OkaVZVwithoutother
organinvolvem
ent;dissem
inated
OkaVZVwith
subsequent
infection
resulting
inpneumonia,m
eningitis,or
hepatitisinindividualswith
demonstrated
immunodeficiencies;vaccine
strainviral
reactivationwithoutother
organ
involvem
ent;vaccinestrainviral
reactivationwith
subsequent
infection
resulting
inmeningitis
orencephalitis;
andanaphylaxis.
Inalargepostlicensurestudyof.1.8millionvaccinerecipients,
purpurawas
associated
with
vaccinationagainstvaricellain
childrenaged
11–17.These
results
werebasedon
1or
2cases
pervaccinetype/age
group.Accordingtotheauthorsmost
casesweremild
andacute.
Moderate:purpura
Miscellaneous
High:noassociationofchildhood
leukem
iawith
MMR,DTaP,Td,Hib,
hepatitisB,andpolio
vaccines
Notapplicable.
Four
largeepidem
iologicstudiesconductedanalyses
toassess
which,ifany,ofthe
followingvaccinesmightbe
associated
with
childhood
leukem
ia:M
MR,DTaP,Td,Hib,hepatitisB,andpolio
vaccine.No
associationwas
foundforanyvaccine.
EPC,Evidence-based
PracticeCenter;M
S,multiplesclerosis;MCV,m
eningococcalconjugatevaccine;MPSV,meningococcalpolysaccharide
vaccine;PCV,pneumococcalconjugatevaccine;VZV,varicella-zostervirus.
6 MAGLIONE et al by guest on September 8, 2018www.aappublications.org/newsDownloaded from

long-term AEs in children. A 2002 IOMreview on hepatitis B vaccine anddemyelinating neurologic disordersconcluded that the evidence “favorsrejection” of a causal relationshipwith incident multiple sclerosis ormultiple sclerosis relapse.19 We iden-tified 1 study published after the IOM2011 search: Gallagher and Goodman(2010)20 conducted a secondary anal-ysis of National Health Interview Surveydata on 7074 boys born before 1999.Vaccination status and health out-comes were reported by parents.Results were significant for the risk ofautism in children who received theirfirst dose of hepatitis B vaccine duringthe first month of life (OR 3.00, 95% CI1.11–8.13), compared with those whoreceived the vaccination after thefirst month of life or not at all. Signifi-cant protective factors included non-Hispanic white ethnicity (OR 0.36,95% CI 0.15–0.88) and belonging to ahousehold with 2 parents (OR 0.30, 95%CI 0.12–0.75). It is unclear why theauthors selected “first month of life” asthe only vaccination time period stud-ied, without presenting analyses forother time periods or comparing “evervaccinated” with “never vaccinated.”Because of high risk of bias and lowquality, this study presents insufficientevidence that hepatitis B vaccine isassociated with autism.
IPV: Inactivated Polio Virus
The IOM did not study IPV vaccine. Oursearch identified a case–control studyof .2000 children with atopic derma-titis and a family history of allergy in 12Western countries,21 which found thatnewborns immunized against poliohad higher odds (OR 2.60, 95% CI 1.08–6.25) of sensitivity to food allergens.This relationship did not hold for thoseimmunized against polio later in life. Aself-controlled case series of pre-mature infants born in the UnitedStates22 found no increased risk of
wheezing and lower respiratory syn-drome associated with DTaP, IPV, Hib,varicella, PCV7, MMR, or TIV vaccina-tion. In sum, the strength of evidence isinsufficient to determine an associa-tion between polio vaccine in new-borns and sensitivity to food allergens.
Influenza Vaccines
Influenza vaccine is administered in 2forms: live attenuated vaccine (LAIV),administered intranasally, and TIV, ad-ministered intramuscularly. The IOMfound no evidence that “convincinglysupports” causal relationships in thepediatric population for any AEs. Weidentified 1 trial of seasonal influenzavaccine (which included a strain ofH1N1 [swine flu])23 and 1 cohort com-parison study of 2009monovalent H1N1vaccine24 published after the IOMsearch dates; the studies found no ev-idence of an association of the vaccineswith AEs.
Six observational studies also met ourinclusion criteria.25–30 A 2011 UK studyof 2336 children25 found no associationbetween flu vaccines and febrile seizures;however, a recent study using theUS Vaccine Safety Datalink (VSD)26
found an association of flu vaccine withfebrile seizures, which increased withconcomitant administration of pneu-mococcal vaccine (PCV13). In thehighest risk age group (16 months),estimated rate was 12.5 per 100 000doses for TIV without concomitantPCV13, 13.7 per 100 000 doses forPCV13 without concomitant TIV, and44.9 per 100 000 doses for concomitantTIV and PCV13. In large, high-qualitypostlicensure studies, both LAIV andTIV were associated with mild gastro-intestinal disorders,27,28 such as short-term vomiting and diarrhea in children.Strength of evidence is moderatefor these AEs. One of these studiesfound that younger vaccinated children(aged 5–8 years) were more likely toexperience these symptoms than older
vaccinated children (aged 9–17 years).(Children ,5 years of age were notincluded in that study). Finally, an Ital-ian study31 of children hospitalized forinfluenza-like illness (ILI) found thosevaccinated with seasonal vaccine (OR2.1, 95% CI 1.1–4.1) were significantlymore likely to show symptoms of ILIthan unvaccinated children, whereasthose vaccinated for H1N1 were not athigher risk (OR 1.3, 95% CI 0.6–3.1).Strength of evidence is moderate formild gastrointestinal events and fe-brile seizures and low for ILI.
MMR
The IOM committee found that mecha-nistic evidence “convincingly supports”causal relationships betweenMMR andmeasles inclusion body encephalitis inimmunocompromised children andanaphylaxis in allergic patients. Theyalso found epidemiologic evidence that“convincingly supports” a causal re-lationship between MMR vaccine andfebrile seizures.32–38 The IOM committeefound the evidence “favors acceptance”of a causal relationship between MMRand transient arthralgia in the pediatricpopulation.39–45 They found the evidence“favors rejection” of a causal relation-ship between MMR and autism.46–50 Inaddition, a causal relationship betweenthe Urabe strain of mumps and asepticmeningitis has been shown; there isno evidence to link Jeryl Lynn strain,commonly used in the United States, tothis AE.
We identified 5 postlicensure studies ofchildhood MMR vaccination publishedafter the IOM searches. In a case–control study of 189 young adults withautism spectrum disorder and 224controls, Uno et al51 found that child-hood receipt of MMR vaccine was notassociated with an increased rate ofnew-onset autism (OR 1.10, 95% CI0.64–1.90). In 3 studies,18,52,53 MMRvaccination was associated with throm-bocytopenic purpura in children in the
REVIEW ARTICLE
PEDIATRICS Volume 134, Number 2, August 2014 7 by guest on September 8, 2018www.aappublications.org/newsDownloaded from
short term after vaccination. Strength ofevidence is moderate because findingswere consistent and ORs similar in 3European countries, Canada, and theUnited States. Finally, 1 Canadian studyfound MMR vaccination was associatedwith increased emergency departmentvisits within 2 weeks. This finding isconsistent with the IOM’s findings thatMMR vaccine is associated with febrileseizures.
Meningococcal
The IOM found the evidence “convinc-ingly supports” a causal relationshipwith anaphylaxis in children who maybe allergic to ingredients. The IOMconclusion does not differentiate be-tween meningococcal conjugate ormeningococcal polysaccharide vac-cines. We found 2 studies of quadriva-lent meningococcal conjugate vaccinein children54,55 published after the IOMreport. A trial in Saudi Arabia found nostatistical association with grade 2 or 3fever, malaise, myalgia, or headache inthe short term.54 A trial in the UnitedStates and South America55 foundvaccination was not associated withsevere change in eating habits, severeirritability, severe persistent crying,severe sleepiness, or urticaria in theyear after vaccination.
Thus, the strength of evidence is mod-erate that meningococcal vaccine maycause anaphylaxis in children who areallergic to ingredients. Strength of ev-idence is insufficient to determine anassociation with less serious eventssuch as headache, irritability, and ur-ticaria.
PCV13
The IOM did not study the safety ofPCV13. As noted earlier, the VSD26 an-alyzed data on .200 000 US childrenaged,5 years and found that vaccineagainst pneumonia (PCV13) was asso-ciatedwith febrile seizures; importantly,administration of influenza vaccine at
the same visit was associated with in-creased risk. For example, in the high-est risk group, which was 16-month-oldchildren, the estimated rate was 13.7per 100 000 doses for PCV13 withoutconcomitant TIV and 44.9 per 100 000doses for concomitant TIV and PCV13.Risk difference estimates varied by agedue to the varying baseline risk forseizures in young children. Thus thestrength of evidence for an associationbetween PCV13 and febrile seizures ismoderate, and the risk is particularlyhigh when coadministered with in-fluenza vaccine.
Rotavirus Vaccines: RotaTeq andRotarix
The IOMreportdidnotaddressvaccinesagainst rotavirus. Thirty-one trials ofrotavirus vaccine56–85 met our inclusioncriteria. Participants in the acceptedstudies received 2 or 3 oral-administereddoses of Rotarix (18 studies) or RotaTeq(13 studies). Neither Rotarix nor RotaTeqwas associated with increased risk ofAEs other than cough, runny nose, orirritability.
We identified 5 postlicensure studieson intussusception risk86–90; an earlierbrand of rotavirus vaccine (Rotashield)was withdrawn from the market in1999 due to concerns about risk forthis condition. A high-quality epidemi-ologic study (N = 296 023) conducted inAustralia86 found RotaTeq associatedwith intussusception in children 1 to 21days after the first of 3 required dosesbut found no association with Rotarix.Two postlicensure studies were re-cently conducted in the United States.Shui et al89 analyzed VSD data on786 725 doses of RotaTeq and foundno association with intussusception atany time after vaccination. However,a recent analysis of data from the USPost-Licensure Rapid ImmunizationSafety Monitoring (PRISM) program90
found that intussusception risk wasincreased after Dose 1 of RotaTeq and
Dose 2 of Rotarix. The RotaTeq analysishad higher statistical power becausethat vaccine was administered toorders of magnitude more childrenthan Rotarix. Estimated rate of in-tussusception was 1.1 to 1.5 cases per100 000 doses of RotaTeq and 5.1 casesper 100 000 doses of Rotarix.
In addition, 2 case–control studiesconducted in Latin America found anassociation with intussusception inchildren after the first of 2 requireddoses of Rotarix. One study estimatedRotarix increased risk by 3.7 additionalcases per 100 000 person years inMexico.87 The other Latin Americanstudy estimated risk as 1 case per51 000 vaccinations in Mexico and 1 caseper 68 000 vaccinations in Brazil.88 Insum, there is moderate strength evi-dence that vaccination against rotavi-rus is associated with intussusception,but the occurrence is extremely rare,and risk factors have not been in-vestigated.
Varicella
The IOM committee found evidence“convincingly supports” causal rela-tionships in children between varicellavirus vaccine and the following: dis-seminated Oka strain varicella zostervirus (Oka VZV) without other organinvolvement; disseminated Oka VZVwith subsequent infection resulting inpneumonia,91 meningitis, or hepatitisin individuals with demonstrated immu-nodeficiencies; vaccine strain viralreactivation without other organ in-volvement; vaccine strain viral reac-tivation with subsequent infectionresulting in meningitis or encephali-tis92; and anaphylaxis.91
We identified 1 study that investigatedpossible relationships among Hib, PCV,MMR,DTaP, TIV, hepatitis A, varicella, andmeningococcal vaccines and immunethrombocytopenic purpura in chil-dren enrolled in 5 US health mainte-nance organizations.18 Purpura was not
8 MAGLIONE et al by guest on September 8, 2018www.aappublications.org/newsDownloaded from

associated with any of the vaccinesin children aged 2 to 6 years but wasassociated with vaccination againstvaricella in children aged 11 to 17years (incidence rate ratio R 12.14, 95%CI 1.10–133.96; findings related to othervaccines are reported in their re-spective sections). This study providesevidence for a moderate associationbetween varicella vaccine and purpurain children aged 11 to 17 years.
Studies Controlling for MultipleVaccinations During Childhood
Four high-quality epidemiologic studiesinvestigated the potential relationshipbetween vaccinations and onset ofchildhood leukemia. Groves and col-leagues93 included 439 US childrenwith lymphoblastic leukemia in acase–control analysis to investigateany possible relationship with oralor injected polio vaccine, diphtheria-tetanus pertussis vaccine, MMR, Hib,or hepatitis B vaccine. Controls wereselected using random-digit dialing,which resulted in controls of highersocioeconomic status then the 439cases. None of the vaccines were as-sociated with leukemia. The relation-ship between vaccination and leukemiawas also assessed in a case–controlstudy of children in Northern California.94
Cases were matched on date of birth,gender, and race/ethnicity. Analysis alsocontrolled for maternal education andfamily income. None of the vaccinesinvestigated (DPT, polio vaccine, MMR,Hib, hepatitis B vaccine) were associ-ated with increased risk of leukemia.Similarly, the Cross-Canada Child-hood Leukemia Study95 found no as-sociation between vaccines againstmumps, measles, rubella, diphtheria,tetanus, pertussis, polio, or hepatitis Band leukemia. Finally, a large case–control study of children born inTexas96 found that several vaccinesmay have a protective effect againstacute lymphoblastic leukemia.
DISCUSSION
This study updated the evidence pre-sented in the 2011 IOM report and ex-panded the scope of that study byincluding additional vaccines such asthose against Hib, hepatitis A, PCV13,rotavirus, and IPV. Findings related tothese vaccines indicate that the Hibvaccine is associated with local dis-comfort such as redness and swellingbut isnotassociatedwithseriousAEsorhospitalization. Strength of evidence ismoderate for the following associa-tions:HepatitisAvaccineandpurpura inchildren aged 7 to 17 years, PCV13 andfebrile seizures with an escalation ofrisk when coadministered with TIV, androtavirus vaccine and intussusception.None of the vaccines studied here wereassociated with childhood-onset leu-kemia.
Our findings support the following IOMresults: vaccine against hepatitis B isnot associated with any long- or short-termAEs; theMMRvaccine isassociatedwith febrile seizures; MMR vaccine isnot associated with autism. In addition,our study found moderate evidencelinking both LAIV and TIV forms of theinfluenza vaccines with mild gastroin-testinal events; TIV was associated withfebrile seizures. We also found mod-erate (but consistent) strength evi-dence of an association between theMMR vaccine and thrombocytopenicpurpura in children; therewasasimilarassociation between the varicella vac-cine and thrombocytopenic purpura inchildren aged 11 to 17 years.
Literature search procedures for thisreview were extensive; however, someunpublished trial results may not havebeen identified. An independent Scien-tific Resource Center under contractwith AHRQ requested Scientific In-formation Packets from the vaccinemanufacturers. (The research teamwas prohibited from contacting man-ufacturers directly.) Only 2 companiesresponded.
Our findings are based on only themostrigorous study designs to assess po-tential statistical associations; how-ever, thesedesignshave limitations thatmust be considered. Controlled trialsoften have insufficient sample size toidentify rare AEs and do not have ex-tended follow-up to identify long-termsequelae. In addition, trials may pur-posely exclude subjects who could bemore susceptible to AEs. For this rea-son, any comprehensive review ofvaccine safety must include post-licensure studies, but these also havelimitations. Large epidemiologic stud-ies sometimes include any availableformulation of vaccines against a par-ticular disease and may not stratifyresults by dosage or formulation. Forexample, the relationship between the“seasonal influenza vaccine” and an AEcould be studied over several years ofdata without considering the changesin formulation over the seasons ordifferentiating between live or inactivevaccine. In addition, people who avoidvaccinations (whether purposely ornot) may differ from those who receivevaccinations in terms of race, gender,age, socioeconomic status, and preex-isting medical conditions, and thesedifferences may be associated withhealth outcomes. Observational stud-ies may attempt to control for suchpotential confounders by usingmatched cohorts or multivariate re-gression analysis; still, some factorssuch as environmental exposuresmay be unmeasured or challenging toadequately control for.
The self-controlled case series wasdeveloped specifically to assess thesafety of vaccines; this method eli-minates confounding by all time-independent variables by usingcases as their own controls and pre-defined “time windows” before andafter vaccination. This design hasbeen used to study purpura, febrileseizures, intussusception, and autism
REVIEW ARTICLE
PEDIATRICS Volume 134, Number 2, August 2014 9 by guest on September 8, 2018www.aappublications.org/newsDownloaded from

in children. However, the assumptionof no temporal shifts in this model isdifficult to justify in very young chil-dren because any patient character-istics that change with time will notbe adequately controlled for.
Importantly, some AE signals thatwarrant future research may not havebeen identified by this project. Passivesurveillance systems such as the USVaccine Adverse Event Reporting Sys-tem97 are crucial in identifying signalsregarding AEs post licensure, but theyare not designed to assess a statisticalassociation, so they were excluded assources of data.
CONCLUSIONS
Our findings may allay some patient,caregiver, and health care providerconcerns. Strength of evidence is highthatMMR vaccine is not associatedwiththe onset of autism in children; thisconclusion supports findings of allprevious reviews on the topic. There isalso high-strength evidence that MMR,DTaP, Td, Hib, and hepatitis B vaccinesare not associated with childhood leu-kemia.
Evidence was found for an associationof several serious AEs with vaccines;
however, these events were extremelyrare: absolute risk is low. For example,strength of evidence is moderate forassociation of vaccines against rotavi-rus with intussusception. Although 1large US epidemiologic study foundno association, a recent analysis ofthe US PRISM program90 found bothRotaTeq and Rotarix associated withintussusception in the short term. Esti-mated rates were 1.1 to 1.5 cases per100 000 doses of RotaTeq and 5.1 casesper 100 000 doses of Rotarix.
Few studies were powered to detectpatient characteristics associated withincreased risk of rare AEs. Advancedhealth information technology systemsthat contain both vaccination andhealth outcome recordsmay be used toconduct such investigations. In theUnited States, the VSD contains datafrom such systems at 9 large managedcare organizations. In addition, thePRISM program also conducts activesurveillance using electronic healthcare databases from managed careorganizations. Nations with single-payer health care systems often haveelectronic registries that allow largeepidemiologic studies of entire pop-ulations. Future analyses should be
stratified by formulation and brand ofvaccine whenever possible.
ACKNOWLEDGMENTSThe authors thank Aneesa Motala, BA,for compiling the many peer reviewcomments and formatting the final re-port. We thank Susanne Hempel, PhD,for her advice on study design, PaulShekelle, MD, PhD, for his advice and re-viewof thedraft andfinal versionsof theevidence report, Kim Wittenberg, MA,for serving as the AHRQ Task Order Of-ficer and Steve Bende, PhD, for repre-senting the Office of the AssistantSecretary for Health. We thank the fol-lowing individuals for serving on theTechnical Expert Panel for the project:Meghan Baker, MD ScD; Richard Beigi,MD, MSc; Kathryn Edwards, MD; KristenFeemster, MD, MSPH; Bruce Fireman,MA; David Martin, MD; and ClaudiaVellozzi, MD, MPH. Finally, we would liketo thank the following Peer Reviewers:Janet D. Cragan, MD, MPH; FrancescaCunningham, PharmD; Frank Destefano,MD, MPH; and Laura Elizabeth Riley, MD.Please note that service as a PeerReviewer or Expert Panel memberdoes not imply endorsement of thestudy findings.
REFERENCES
1. Centers for Disease Control and Pre-vention (CDC). Ten great public healthachievements—United States, 1900–1999.MMWR Morb Mortal Wkly Rep. 1999;48(12):241–243
2. Sugerman DE, Barskey AE, Delea MG, et al.Measles outbreak in a highly vaccinatedpopulation, San Diego, 2008: role of theintentionally undervaccinated. Pediatrics.2010;125(4):747–755
3. Atwell JE, Van Otterloo J, Zipprich J, et al.Nonmedical vaccine exemptions and per-tussis in California, 2010. Pediatrics. 2013;132(4):624–630
4. Institute of Medicine. Adverse Effectsof Vaccines: Evidence and Causality.Washington, DC: The National AcademyPress; 2011
5. Castro M, Dozor A, Fish J, et al. The safetyof inactivated influenza vaccine in adultsand children with asthma. N Engl J Med.2001;345(21):1529–1536
6. US Department of Health and HumanServices. Common Terminology Criteria forAdverse Events (CTCAE). Version 4.0. May28, 2009 (v4.03: June 14, 2010)
7. Santaguida PL, Raina P. The Development ofthe McHarm Quality Assessment Scale foradverse events: Delphi Consensus on im-portant criteria for evaluating harms.2008. Available at: http://hiru.mcmaster.ca/epc/mcharm.pdf. Accessed May 5, 2012
8. Owens DK, Lohr KN, Atkins D, et al. AHRQ se-ries paper 5: grading the strength of a bodyof evidence when comparing medical inter-ventions—agency for healthcare research
and quality and the effective health-careprogram. J Clin Epidemiol. 2010;63(5):513–523
9. Balshem H, Helfand M, Schünemann HJ,et al. GRADE guidelines: 3. Rating thequality of evidence. J Clin Epidemiol. 2011;64(4):401–406
10. Blom L, Nyström L, Dahlquist G. The Swedishchildhood diabetes study. Vaccinations andinfections as risk determinants for diabe-tes in childhood. Diabetologia. 1991;34(3):176–181
11. DeStefano F, Mullooly JP, Okoro CA, et al; Vac-cine Safety Datalink Team. Childhood vacci-nations, vaccination timing, and risk of type 1diabetes mellitus. Pediatrics. 2001;108(6):E112
12. Hviid A, Stellfeld M, Wohlfahrt J, Melbye M.Childhood vaccination and type 1 diabetes.N Engl J Med. 2004;350(14):1398–1404
10 MAGLIONE et al by guest on September 8, 2018www.aappublications.org/newsDownloaded from

13. Klein NP, Hansen J, Lewis E, et al. Post-marketing safety evaluation of a tetanustoxoid, reduced diphtheria toxoid and 3-component acellular pertussis vaccine ad-ministered to a cohort of adolescents ina United States health maintenance orga-nization. Pediatr Infect Dis J. 2010;29(7):613–617
14. Infections and vaccinations as risk factorsfor childhood type I (insulin-dependent)diabetes mellitus: a multicentre case–control investigation. EURODIAB Substudy 2Study Group. Diabetologia. 2000;43(1):47–53
15. Huu TN, Toan NT, Tuan HM, et al. Safety andreactogenicity of primary vaccination withthe 10-valent pneumococcal non-typeableHaemophilus influenzae protein D con-jugate vaccine in Vietnamese infants:a randomised, controlled trial. BMC InfectDis. 2013;13:95
16. Santosham M, Wolff M, Reid R, et al. Theefficacy in Navajo infants of a conjugatevaccine consisting of Haemophilus influ-enzae type b polysaccharide and Neisseriameningitidis outer-membrane proteincomplex. N Engl J Med. 1991;324(25):1767–1772
17. Capeding MRZ, Nohynek H, Pascual LG, et al.The immunogenicity of three Haemophilusinfluenzae type B conjugate vaccines aftera primary vaccination series in Philippineinfants. Am J Trop Med Hygiene. 1996;55(5):516–520
18. O’Leary ST, Glanz JM, McClure DL, et al. Therisk of immune thrombocytopenic purpuraafter vaccination in children and adoles-cents. Pediatrics. 2012;129(2):248–255
19. Institute of Medicine. Immunization SafetyReview: Multiple Immunizations and Im-mune Dysfunction. Washington, DC: TheNational Academies Press; 2002
20. Gallagher CM, Goodman MS. Hepatitis Bvaccination of male neonates and autismdiagnosis, NHIS 1997–2002. J Toxicol Envi-ron Health A. 2010;73(24):1665–1677
21. Grüber C, Warner J, Hill D, Bauchau V;EPAAC Study Group. Early atopic diseaseand early childhood immunization—isthere a link? Allergy. 2008;63(11):1464–1472
22. Mullooly JP, Schuler R, Barrett M, Maher JE.Vaccines, antibiotics, and atopy. Pharma-coepidemiol Drug Saf. 2007;16(3):275–288
23. Englund JA, Walter E, Black S, et al; GRC28Study Team. Safety and immunogenicity oftrivalent inactivated influenza vaccine ininfants: a randomized double-blind placebo-controlled study. Pediatr Infect Dis J. 2010;29(2):105–110
24. Mallory RM, Malkin E, Ambrose CS, et al.Safety and immunogenicity following ad-
ministration of a live, attenuated mono-valent 2009 H1N1 influenza vaccine tochildren and adults in two randomizedcontrolled trials. PLoS ONE. 2010;5(10):e13755
25. Stowe J, Andrews N, Bryan P, Seabroke S,Miller E. Risk of convulsions in childrenafter monovalent H1N1 (2009) and trivalentinfluenza vaccines: a database study. Vac-cine. 2011;29(51):9467–9472
26. Tse A, Tseng HF, Greene SK, Vellozzi C, LeeGM; VSD Rapid Cycle Analysis InfluenzaWorking Group. Signal identification andevaluation for risk of febrile seizures inchildren following trivalent inactivated in-fluenza vaccine in the Vaccine SafetyDatalink Project, 2010–2011. Vaccine. 2012;30(11):2024–2031
27. Baxter R, Toback SL, Sifakis F, et al. Apostmarketing evaluation of the safety ofAnn Arbor strain live attenuated influenzavaccine in children 5 through 17 years ofage. Vaccine. 2012;30(19):2989–2998
28. Glanz JM, Newcomer SR, Hambidge SJ,et al. Safety of trivalent inactivated in-fluenza vaccine in children aged 24 to 59months in the vaccine safety datalink. ArchPediatr Adolesc Med. 2011;165(8):749–755
29. Morgan TM, Schlegel C, Edwards KM, et al;Urea Cycle Disorders Consortium. Vaccinesare not associated with metabolic events inchildren with urea cycle disorders. Pedi-atrics. 2011;127(5). Available at: www.pedi-atrics.org/cgi/content/full/127/5/e1147
30. Hambidge SJ, Ross C, McClure D, Glanz J;VSD team. Trivalent inactivated influenzavaccine is not associated with sickle cellhospitalizations in adults from a large co-hort. Vaccine. 2011;29(46):8179–8181
31. Italian Multicenter Study Group for Drugand Vaccine Safety in Children. Effective-ness and safety of the A-H1N1 vaccine inchildren: a hospital-based case–controlstudy. BMJ Open. 2011;1(2):e000167
32. Barlow WE, Davis RL, Glasser JW, et al;Centers for Disease Control and PreventionVaccine Safety Datalink Working Group. Therisk of seizures after receipt of whole-cellpertussis or measles, mumps, and rubellavaccine. N Engl J Med. 2001;345(9):656–661
33. Chen RT, Glasser JW, Rhodes PH, et al; TheVaccine Safety Datalink Team. VaccineSafety Datalink project: a new tool for im-proving vaccine safety monitoring in theUnited States. Pediatrics. 1997;99(6):765–773
34. Farrington P, Pugh S, Colville A, et al. A newmethod for active surveillance of adverseevents from diphtheria/tetanus/pertussisand measles/mumps/rubella vaccines. Lancet.1995;345(8949):567–569
35. Griffin MR, Ray WA, Mortimer EA, FenichelGM, Schaffner W. Risk of seizures aftermeasles-mumps-rubella immunization. Pe-diatrics. 1991;88(5):881–885
36. Miller E, Andrews N, Stowe J, Grant A,Waight P, Taylor B. Risks of convulsion andaseptic meningitis following measles-mumps-rubella vaccination in the UnitedKingdom. Am J Epidemiol. 2007;165(6):704–709
37. Vestergaard M, Hviid A, Madsen KM, et al.MMR vaccination and febrile seizures:evaluation of susceptible subgroups andlong-term prognosis. JAMA. 2004;292(3):351–357
38. Ward KN, Bryant NJ, Andrews NJ, et al. Riskof serious neurologic disease after immu-nization of young children in Britain andIreland. Pediatrics. 2007;120(2):314–321
39. Benjamin CM, Chew GC, Silman AJ. Jointand limb symptoms in children afterimmunisation with measles, mumps, andrubella vaccine. BMJ. 1992;304(6834):1075–1078
40. Davis RL, Marcuse E, Black S, et al; TheVaccine Safety Datalink Team. MMR2 im-munization at 4 to 5 years and 10 to 12years of age: a comparison of adverseclinical events after immunization in theVaccine Safety Datalink project. Pediatrics.1997;100(5):767–771
41. Dos Santos BA, Ranieri TS, Bercini M, et al.An evaluation of the adverse reaction po-tential of three measles-mumps-rubellacombination vaccines. Rev Panam SaludPublica. 2002;12(4):240–246
42. Heijstek MW, Pileggi GC, Zonneveld-Huijssoon E,et al. Safety of measles, mumps and ru-bella vaccination in juvenile idiopathicarthritis. Ann Rheum Dis. 2007;66(10):1384–1387
43. LeBaron CW, Bi D, Sullivan BJ, Beck C,Gargiullo P. Evaluation of potentially com-mon adverse events associated with thefirst and second doses of measles-mumps-rubella vaccine. Pediatrics. 2006;118(4):1422–1430
44. Peltola H, Heinonen OP. Frequency of trueadverse reactions to measles-mumps-rubella vaccine. A double-blind placebo-controlled trial in twins. Lancet. 1986;1(8487):939–942
45. Virtanen M, Peltola H, Paunio M, HeinonenOP. Day-to-day reactogenicity and thehealthy vaccinee effect of measles-mumps-rubella vaccination. Pediatrics. 2000;106(5).Available at: www.pediatrics.org/cgi/content/full/106/5/e62
46. Farrington CP, Miller E, Taylor B. MMR andautism: further evidence against a causalassociation. Vaccine. 2001;19(27):3632–3635
REVIEW ARTICLE
PEDIATRICS Volume 134, Number 2, August 2014 11 by guest on September 8, 2018www.aappublications.org/newsDownloaded from

47. Madsen KM, Hviid A, Vestergaard M, et al. Apopulation-based study of measles, mumps,and rubella vaccination and autism. N EnglJ Med. 2002;347(19):1477–1482
48. Mrozek-Budzyn D, Kie1tyka A, Majewska R.Lack of association between measles-mumps-rubella vaccination and autism inchildren: a case-control study. Pediatr In-fect Dis J. 2010;29(5):397–400
49. Smeeth L, Cook C, Fombonne E, et al. MMRvaccination and pervasive developmentaldisorders: a case-control study. Lancet.2004;364(9438):963–969
50. Taylor B, Miller E, Farrington CP, et al. Au-tism and measles, mumps, and rubellavaccine: no epidemiological evidence fora causal association. Lancet. 1999;353(9169):2026–2029
51. Uno Y, Uchiyama T, Kurosawa M, Aleksic B,Ozaki N. The combined measles, mumps,and rubella vaccines and the total numberof vaccines are not associated with de-velopment of autism spectrum disorder:the first case–control study in Asia. Vac-cine. 2012;30(28):4292–4298
52. Andrews N, Stowe J, Miller E, et al; VAESCOconsortium. A collaborative approach toinvestigating the risk of thrombocytopenicpurpura after measles-mumps-rubellavaccination in England and Denmark. Vac-cine. 2012;30(19):3042–3046
53. Bertuola F, Morando C, Menniti-Ippolito F,et al. Association between drug and vac-cine use and acute immune thrombocyto-penia in childhood: a case–control study inItaly. Drug Saf. 2010;33(1):65–72
54. Khalil M, Al-Mazrou Y, Findlow H, et al.Safety and immunogenicity of a meningo-coccal quadrivalent conjugate vaccine infive- to eight-year-old Saudi Arabian chil-dren previously vaccinated with two dosesof a meningococcal quadrivalent poly-saccharide vaccine. Clin Vaccine Immunol.2012;19(10):1561–1566
55. Klein NP, Reisinger KS, Johnston W, et al.Safety and immunogenicity of a novelquadrivalent meningococcal CRM-conjugatevaccine given concomitantly with routinevaccinations in infants [published correctionappears in Pediatr Infect Dis J. 2012;31(10):1105]. Pediatr Infect Dis J. 2012;31(1):64–71
56. Block SL, Vesikari T, Goveia MG, et al; Pen-tavalent Rotavirus Vaccine Dose Confirma-tion Efficacy Study Group. Efficacy,immunogenicity, and safety of a pentava-lent human-bovine (WC3) reassortant ro-tavirus vaccine at the end of shelf life.Pediatrics. 2007;119(1):11–18
57. Chang C-C, Chang M-H, Lin T-Y, Lee H-C,Hsieh W-S, Lee P-I. Experience of pentava-lent human-bovine reassortant rotavirus
vaccine among healthy infants in Taiwan.J Formos Med Assoc. 2009;108(4):280–285
58. Christie CDC, Duncan ND, Thame KA, et al.Pentavalent rotavirus vaccine in developingcountries: safety and health care resourceutilization. Pediatrics. 2010;126(6). Availableat: www.pediatrics.org/cgi/content/full/126/6/e1499
59. Dennehy PH, Brady RC, Halperin SA, et al;North American Human Rotavirus VaccineStudy Group. Comparative evaluation ofsafety and immunogenicity of two dosagesof an oral live attenuated human rotavirusvaccine. Pediatr Infect Dis J. 2005;24(6):481–488
60. Goveia MG, Rodriguez ZM, Dallas MJ, et al;REST Study Team. Safety and efficacy of thepentavalent human-bovine (WC3) reassor-tant rotavirus vaccine in healthy prematureinfants. Pediatr Infect Dis J. 2007;26(12):1099–1104
61. Grant LR, Watt JP, Weatherholtz RC, et al.Efficacy of a pentavalent human-bovinereassortant rotavirus vaccine against ro-tavirus gastroenteritis among AmericanIndian children. Pediatr Infect Dis J. 2012;31(2):184–188
62. Kawamura N, Tokoeda Y, Oshima M, et al.Efficacy, safety and immunogenicity ofRIX4414 in Japanese infants during the firsttwo years of life. Vaccine. 2011;29(37):6335–6341
63. Kerdpanich A, Chokephaibulkit K, Watana-veeradej V, et al. Immunogenicity of a live-attenuated human rotavirus RIX4414 vaccinewith or without buffering agent. Hum Vaccin.2010;6(3):254–262
64. Kim DS, Lee TJ, Kang JH, et al. Immunoge-nicity and safety of a pentavalent human-bovine (WC3) reassortant rotavirus vaccinein healthy infants in Korea. Pediatr InfectDis J. 2008;27(2):177–178
65. Kim JS, Bae CW, Lee KY, et al. Immunoge-nicity, reactogenicity and safety of a humanrotavirus vaccine (RIX4414) in Koreaninfants: a randomized, double-blind, placebo-controlled, phase IV study. Hum VaccinImmunother. 2012;8(6):806–812
66. Madhi SA, Cunliffe NA, Steele D, et al. Effectof human rotavirus vaccine on severe di-arrhea in African infants. N Engl J Med.2010;362(4):289–298
67. Narang A, Bose A, Pandit AN, et al. Immu-nogenicity, reactogenicity and safety ofhuman rotavirus vaccine (RIX4414) in In-dian infants. Hum Vaccin. 2009;5(6):414–419
68. Omenaca F, Sarlangue J, Szenborn L, et al;ROTA-054 Study Group. Safety, reactogenicityand immunogenicity of the human rotavirusvaccine in preterm European Infants: a ran-
domized phase IIIb study. Pediatr Infect Dis J.2012;31(5):487–493
69. Phua KB, Quak SH, Lee BW, et al. Evaluationof RIX4414, a live, attenuated rotavirusvaccine, in a randomized, double-blind,placebo-controlled phase 2 trial involving2464 Singaporean infants. J Infect Dis.2005;192(suppl 1):S6–S16
70. Phua KB, Lim FS, Lau YL, et al. Safety andefficacy of human rotavirus vaccine duringthe first 2 years of life in Asian infants:randomised, double-blind, controlled study.Vaccine. 2009;27(43):5936–5941
71. Phua KB, Lim FS, Lau YL, et al. Rotavirusvaccine RIX4414 efficacy sustained duringthe third year of life: A randomized clinicaltrial in an Asian population. Vaccine. 2012;30(30):4552–4557
72. Rodriguez ZM, Goveia MG, Stek JE, et al.Concomitant use of an oral live pentavalenthuman-bovine reassortant rotavirus vac-cine with licensed parenteral pediatricvaccines in the United States. Pediatr InfectDis J. 2007;26(3):221–227
73. Ruiz-Palacios GM, Pérez-Schael I, VelázquezFR, et al; Human Rotavirus Vaccine StudyGroup. Safety and efficacy of an attenuatedvaccine against severe rotavirus gastro-enteritis. N Engl J Med. 2006;354(1):11–22
74. Sow SO, Tapia M, Haidara FC, et al. Efficacyof the oral pentavalent rotavirus vaccine inMali. Vaccine. 2012;30(suppl 1):A71–A78
75. Steele AD, Reynders J, Scholtz F, et al.Comparison of 2 different regimens forreactogenicity, safety, and immunogenicityof the live attenuated oral rotavirus vaccineRIX4414 coadministered with oral poliovaccine in South African infants. J InfectDis. 2010;202(suppl):S93–S100
76. Steele AD, Madhi SA, Louw CE, et al. Safety,reactogenicity, and immunogenicity of humanrotavirus vaccine RIX4414 in human immu-nodeficiency virus-positive infants in SouthAfrica. Pediatr Infect Dis J. 2011;30(2):125–130
77. Tregnaghi MW, Abate HJ, Valencia A, et al;Rota-024 Study Group. Human rotavirusvaccine is highly efficacious when coad-ministered with routine expanded programof immunization vaccines including oralpoliovirus vaccine in Latin America. PediatrInfect Dis J. 2011;30(6):e103–e108
78. Vesikari T, Karvonen A, Puustinen L, et al.Efficacy of RIX4414 live attenuated humanrotavirus vaccine in Finnish infants. PediatrInfect Dis J. 2004;23(10):937–943
79. Vesikari T, Clark HF, Offit PA, et al. Effects ofthe potency and composition of the multi-valent human-bovine (WC3) reassortantrotavirus vaccine on efficacy, safety andimmunogenicity in healthy infants. Vaccine.2006;24(22):4821–4829
12 MAGLIONE et al by guest on September 8, 2018www.aappublications.org/newsDownloaded from

80. Vesikari T, Matson DO, Dennehy P, et al;Rotavirus Efficacy and Safety Trial (REST)Study Team. Safety and efficacy of a penta-valent human-bovine (WC3) reassortantrotavirus vaccine. N Engl J Med. 2006;354(1):23–33
81. Vesikari T, Karvonen A, Bouckenooghe A,Suryakiran PV, Smolenov I, Han HH. Immu-nogenicity, reactogenicity and safety of thehuman rotavirus vaccine RIX4414 oralsuspension (liquid formulation) in Finnishinfants. Vaccine. 2011;29(11):2079–2084
82. Vesikari T, Karvonen A, Korhonen T, et al.Safety and immunogenicity of RIX4414 liveattenuated human rotavirus vaccine inadults, toddlers and previously unin-fected infants. Vaccine. 2004;22(21-22):2836–2842
83. Zaman K, Sack DA, Yunus M, et al. Suc-cessful co-administration of a human ro-tavirus and oral poliovirus vaccines inBangladeshi infants in a 2-dose schedule at12 and 16 weeks of age. Vaccine. 2009;27(9):1333–1339
84. Zaman K, Dang DA, Victor JC, et al. Efficacyof pentavalent rotavirus vaccine againstsevere rotavirus gastroenteritis in infantsin developing countries in Asia: a rando-mised, double-blind, placebo-controlledtrial. Lancet. 2010;376(9741):615–623
85. Zaman K, Yunus M, El Arifeen S, et al.Methodology and lessons-learned from theefficacy clinical trial of the pentavalent
rotavirus vaccine in Bangladesh. Vaccine.2012;30(suppl 1):A94–A100
86. Buttery JP, Danchin MH, Lee KJ, et al;PAEDS/APSU Study Group. Intussusceptionfollowing rotavirus vaccine administration:post-marketing surveillance in the NationalImmunization Program in Australia. Vac-cine. 2011;29(16):3061–3066
87. Velázquez FR, Colindres RE, Grajales C,et al. Postmarketing surveillance of in-tussusception following mass introduc-tion of the attenuated human rotavirusvaccine in Mexico. Pediatr Infect Dis J.2012;31(7):736–744
88. Patel MM, López-Collada VR, Bulhões MM,et al. Intussusception risk and health ben-efits of rotavirus vaccination in Mexico andBrazil. N Engl J Med. 2011;364(24):2283–2292
89. Shui IM, Baggs J, Patel M, et al. Risk ofintussusception following administration ofa pentavalent rotavirus vaccine in USinfants. JAMA. 2012;307(6):598–604
90. Yih K, Lieu T, Kulldorff M, et al. In-tussusception risk after rotavirus vac-cination in U.S. infants. Mini-SentinelCoordinating Center; June 2013. Availableat: www.mini-sentinel.org/work_products/PRISM/Mini-Sentinel_PRISM_Rotavirus-and-intussusception-Report.pdf. Accessed June30, 2013
91. Black S, Shinefield H, Ray P, et al. Post-marketing evaluation of the safety and ef-
fectiveness of varicella vaccine. PediatrInfect Dis J. 1999;18(12):1041–1046
92. Donahue JG, Kieke BA, Yih WK, et al; VaccineSafety DataLink Team. Varicella vaccinationand ischemic stroke in children: is there anassociation? Pediatrics. 2009;123(2). Avail-able at: www.pediatrics.org/cgi/content/full/123/2/e228
93. Groves FD, Gridley G, Wacholder S, et al.Infant vaccinations and risk of childhoodacute lymphoblastic leukaemia in the USA.Br J Cancer. 1999;81(1):175–178
94. Ma X, Does MB, Metayer C, Russo C, Wong A,Buffler PA. Vaccination history and risk ofchildhood leukaemia. Int J Epidemiol. 2005;34(5):1100–1109
95. MacArthur AC, McBride ML, Spinelli JJ,Tamaro S, Gallagher RP, Theriault GP. Riskof childhood leukemia associated withvaccination, infection, and medication usein childhood: the Cross-Canada ChildhoodLeukemia Study. Am J Epidemiol. 2008;167(5):598–606
96. Pagaoa MA, Okcu MF, Bondy ML, ScheurerME. Associations between vaccination andchildhood cancers in Texas regions. JPediatr. 2011;158(6):996–1002
97. Haber P, Iskander J, Walton K, Campbell SR,Kohl KS. Internet-based reporting to thevaccine adverse event reporting system:a more timely and complete way for pro-viders to support vaccine safety. Pediatrics.2011;127(suppl 1):S39–S44
(Continued from first page)
The authors of this report are responsible for its content. Statements in the report should not be construed as endorsement by the Agency for HealthcareResearch and Quality or the US Department of Health and Human Services.
www.pediatrics.org/cgi/doi/10.1542/peds.2014-1079
doi:10.1542/peds.2014-1079
Accepted for publication May 7, 2014
Address correspondence to Margaret A. Maglione, MPP, RAND Corporation, 1776 Main St Mailstop 4W, Santa Monica, CA 90407. E-mail: [email protected]
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2014 by the American Academy of Pediatrics
FINANCIAL DISCLOSURE: The authors have indicated they have no financial relationships relevant to this article to disclose.
FUNDING: Supported under Contract No. HHSA290200710062I from the Agency for Healthcare Research and Quality, US Department of Health and Human Services.
POTENTIAL CONFLICT OF INTEREST: The authors have indicated they have no potential conflicts of interest to disclose.
COMPANION PAPER: A companion to this article can be found on page XXX, and online at www.pediatrics.org/cgi/doi/10.1542/peds.2014-1494.
REVIEW ARTICLE
PEDIATRICS Volume 134, Number 2, August 2014 13 by guest on September 8, 2018www.aappublications.org/newsDownloaded from

originally published online July 1, 2014; Pediatrics Courtney Gidengil
Chari, Sydne Newberry, Roberta Shanman, Tanja Perry, Matthew Bidwell Goetz and Margaret A. Maglione, Lopamudra Das, Laura Raaen, Alexandria Smith, Ramya
ReviewSafety of Vaccines Used for Routine Immunization of US Children: A Systematic
ServicesUpdated Information &
014-1079http://pediatrics.aappublications.org/content/early/2014/06/26/peds.2including high resolution figures, can be found at:
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtmlin its entirety can be found online at: Information about reproducing this article in parts (figures, tables) or
Reprintshttp://www.aappublications.org/site/misc/reprints.xhtmlInformation about ordering reprints can be found online:
by guest on September 8, 2018www.aappublications.org/newsDownloaded from
originally published online July 1, 2014; Pediatrics Courtney Gidengil
Chari, Sydne Newberry, Roberta Shanman, Tanja Perry, Matthew Bidwell Goetz and Margaret A. Maglione, Lopamudra Das, Laura Raaen, Alexandria Smith, Ramya
ReviewSafety of Vaccines Used for Routine Immunization of US Children: A Systematic
http://pediatrics.aappublications.org/content/early/2014/06/26/peds.2014-1079located on the World Wide Web at:
The online version of this article, along with updated information and services, is
ISSN: 1073-0397. 60007. Copyright © 2014 by the American Academy of Pediatrics. All rights reserved. Print the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elk Grove Village, Illinois,has been published continuously since 1948. Pediatrics is owned, published, and trademarked by Pediatrics is the official journal of the American Academy of Pediatrics. A monthly publication, it
by guest on September 8, 2018www.aappublications.org/newsDownloaded from





























