Embed Size (px)
Citation preview
1
2014 SPR PG Course
2014 SPR Postgraduate Course
Washington DC
Module 1: Body Imaging Techniques
Moderators: Taylor Chung, MD and Shreyas Vasanawala, MD/PhD
2014 SPR PG Course
SAM 1: The half value thickness of human tissue is approximately:
• A. 3.5 cm• B. 7 cm• C. 10.5 cm• D. 14 cm
2014 SPR PG Course
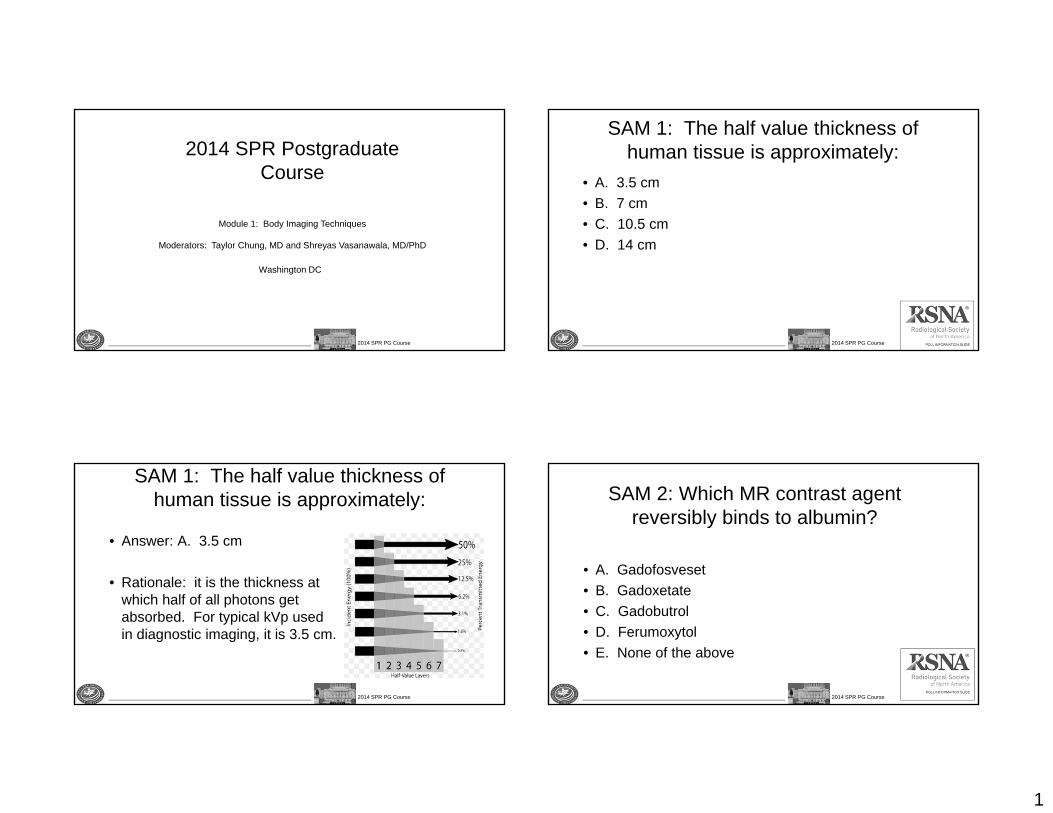
SAM 1: The half value thickness of human tissue is approximately:
• Answer: A. 3.5 cm
• Rationale: it is the thickness at which half of all photons get absorbed. For typical kVp used in diagnostic imaging, it is 3.5 cm.
2014 SPR PG Course
SAM 2: Which MR contrast agent reversibly binds to albumin?
• A. Gadofosveset• B. Gadoxetate• C. Gadobutrol• D. Ferumoxytol• E. None of the above
2
2014 SPR PG Course
Which MR contrast agent reversibly binds to albumin?
• Answer: A. Gadofosveset (Ablavar) is a blood pool agent that reversibly binds to serum albumin, thus prolonging half life in the vessels. PMID 21709565
• B. Gadoxetate (Eovist) is a hepatobiliary agent that has approximately 50% biliary excretion in healthy individuals. In patients with elevated serum bilirubin, less biliary excretion is seen. In patients with liver failure, serum bilirubin above 2 mg/dL is a indicator that hepatobiliary excretion will be diminished to the point of decreased diagnostic utility. PMID 21997981
• C. Gadobutrol is a macrocyclic extracellular agent. PMID 12042967• D. Ferumoxytol is an iron oxide that can be bolus injected and produces both T1 and
T2* shortening. It has FDA approval not as a diagnostic imaging agent, but rather for iron replacement therapy. It has a reported anaphylaxic reaction rate that is higher than that of gadolinium agents. PMID 22045905
• E. None of the above is not correct since choice A is correct.
2014 SPR PG Course
SAM 3: What is NOT a potential disadvantage of using gadoxetate?
• A. Less reliable vascular imaging• B. Pseudo-washout of a hemangioma• C. Prolonged MR exam time• D. Failure of hepatic update• E. Inconclusive evaluation of focal nodular
hyperplasia
2014 SPR PG Course
What is NOT a potential disadvantage of using gadoxetate?
• A. Less reliable vascular imaging• B. Pseudo-washout of a hemangioma• C. Prolonged MR exam time• D. Failure of hepatic update• Answer: E. Inconclusive evaluation of focal
nodular hyperplasia
2014 SPR PG Course
SAM 4: Touch the higher resolutionimage
3
2014 SPR PG Course
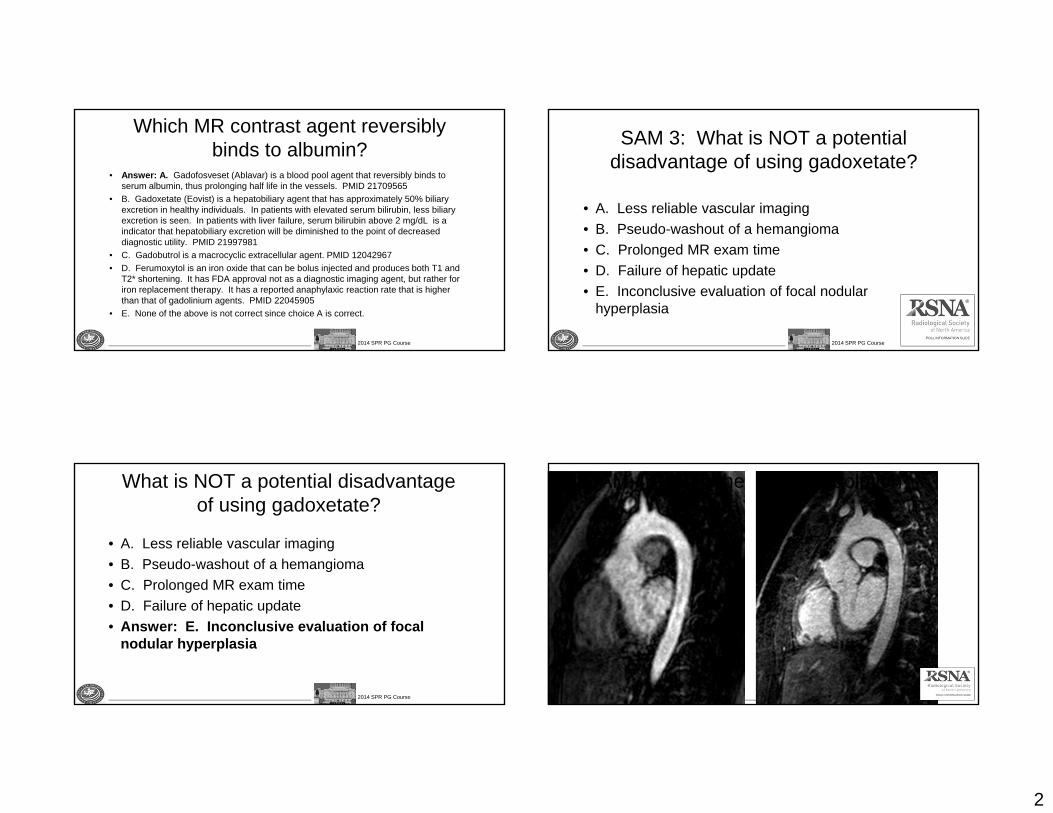
Touch the higher resolution image
• Answer: the right image
• Rationale: Note crisp delineation of descending aorta.
• Reference: Congenital heart disease: cardiovascular MR imaging by using a blood pool contrast agent. Radiology 2011, 260(3):680-8.
2014 SPR PG Course
SAM 5: Why do the aortic root and proximal ascending aorta lack motion
artifact?• A. High spatial resolution
technique• B. Time-resolved
technique• C. ECG triggering• D. ECG triggering and
respiratory synchronization• E. Good breath-holding
2014 SPR PG Course
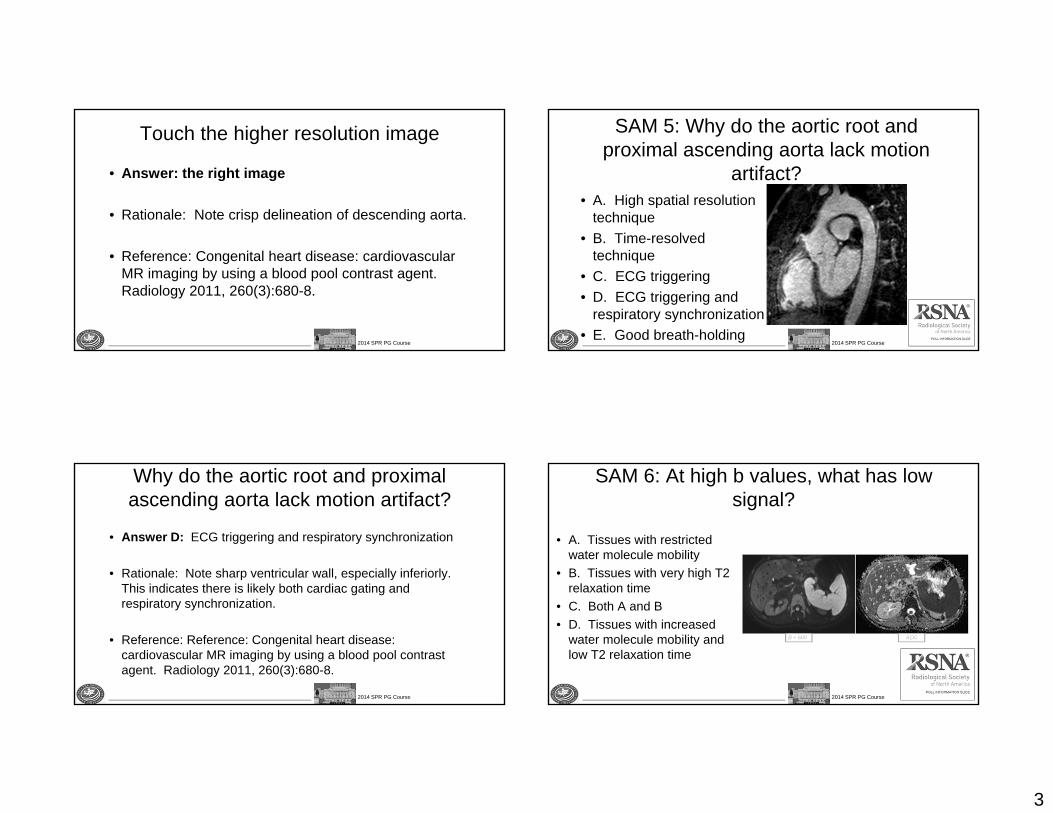
Why do the aortic root and proximal ascending aorta lack motion artifact?
• Answer D: ECG triggering and respiratory synchronization
• Rationale: Note sharp ventricular wall, especially inferiorly. This indicates there is likely both cardiac gating and respiratory synchronization.
• Reference: Reference: Congenital heart disease: cardiovascular MR imaging by using a blood pool contrast agent. Radiology 2011, 260(3):680-8.
2014 SPR PG Course
SAM 6: At high b values, what has low signal?
• A. Tissues with restricted water molecule mobility
• B. Tissues with very high T2 relaxation time
• C. Both A and B• D. Tissues with increased
water molecule mobility and low T2 relaxation time
4
2014 SPR PG Course
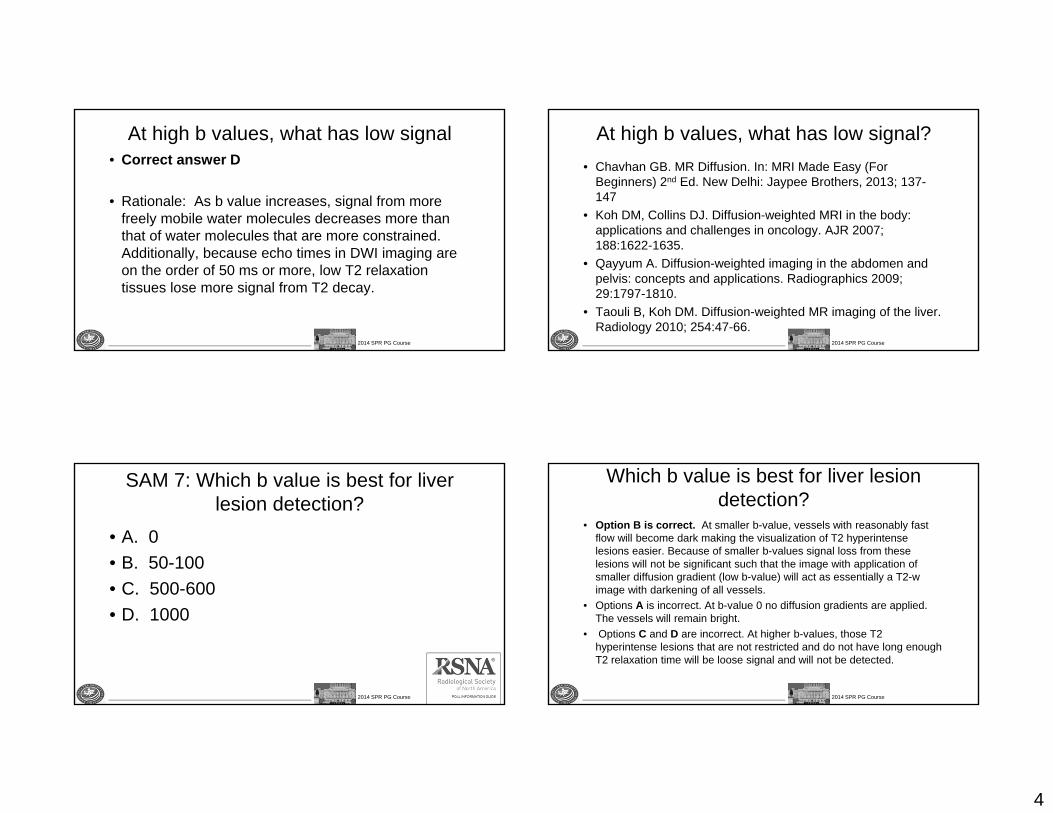
At high b values, what has low signal• Correct answer D
• Rationale: As b value increases, signal from more freely mobile water molecules decreases more than that of water molecules that are more constrained. Additionally, because echo times in DWI imaging are on the order of 50 ms or more, low T2 relaxation tissues lose more signal from T2 decay.
2014 SPR PG Course
At high b values, what has low signal?• Chavhan GB. MR Diffusion. In: MRI Made Easy (For
Beginners) 2nd Ed. New Delhi: Jaypee Brothers, 2013; 137-147
• Koh DM, Collins DJ. Diffusion-weighted MRI in the body: applications and challenges in oncology. AJR 2007; 188:1622-1635.
• Qayyum A. Diffusion-weighted imaging in the abdomen and pelvis: concepts and applications. Radiographics 2009; 29:1797-1810.
• Taouli B, Koh DM. Diffusion-weighted MR imaging of the liver. Radiology 2010; 254:47-66.
2014 SPR PG Course
SAM 7: Which b value is best for liver lesion detection?
• A. 0• B. 50-100• C. 500-600• D. 1000
2014 SPR PG Course
Which b value is best for liver lesion detection?
• Option B is correct. At smaller b-value, vessels with reasonably fast flow will become dark making the visualization of T2 hyperintenselesions easier. Because of smaller b-values signal loss from these lesions will not be significant such that the image with application of smaller diffusion gradient (low b-value) will act as essentially a T2-w image with darkening of all vessels.
• Options A is incorrect. At b-value 0 no diffusion gradients are applied. The vessels will remain bright.
• Options C and D are incorrect. At higher b-values, those T2 hyperintense lesions that are not restricted and do not have long enough T2 relaxation time will be loose signal and will not be detected.
5
2014 SPR PG Course
Which b value is best for liver lesion detection?
• Soyer P, Boudiaf M, Place V, at al. Preoperative detection of hepatic metastases: comparison of diffusion-weighted, T2-weighted fast spin echo and gadolinium-enhanced MR imaging using surgical and histopathologic findings as standard of reference. Eur J Radiol 2011; 80:245-252.
• Yang DM, Jahng GH, Kim HC, et al. The detection and discrimination of malignant and benign focal hepatic lesions: T2 weighted vs diffusion-weighted MRI. Br J Radiol 2011; 84:319-326.
• Parikh T, Drew SJ, Lee VS, et al. Focal liver lesion detection and characterization with diffusion-weighted MR imaging: comparison with standard breath-hold T2-weighted imaging. Radiology 2008; 246:812-822.
2014 SPR PG Course
SAM 8: Size-specific dose estimate (SSDE) is calculated from the patient’s
size and what other parameter?• A. Effective dose• B. CTDIvol
• C. DLP• D. Skin entrance dose
2014 SPR PG Course
SAM: Size-specific dose estimate (SSDE) is calculated from the patient’s
size and what other parameter?
• Answer: CTDIvol•
Rationale: this is by definition of SSDE.
2014 SPR PG Course
SAM 9: Which of the following is NOT important for slow flow detection?
• A. Increasing transducer frequency• B. Lowering filters• C. Lowering the Pulse Repetition Frequency• D. Raising the baseline
6
2014 SPR PG Course
Which of the following is NOT important for slow flow detection?
• Incorrect A. Increasing transducer frequency. Since according to the Doppler equation, the Doppler shift that is produced by the slow flow is directly proportional to the insonating frequency, increasing the insonating frequency will increase the Doppler shift produced by low velocity scatterers, and enhance detection of slow flow.
• Incorrect B. Lowering filters. The filters eliminate low velocity shifts, which often arise from motion of large objects, such as respiratory motion, and which are often of high amplitude and may obscure the pertinent information. However, this must be done carefully when attempting to detect low velocity flow, because such frequency shifts may also be eliminated. Therefore, careful lowering of the filters is important in the ability to detect slow flow
2014 SPR PG Course
Which of the following is NOT important for slow flow detection?
• Incorrect C. Lowering the Pulse Repetition Frequency. This is important to detect and characterize the signal arising from slow-moving structures. If an inappropriately high PRF is used, the signal from the slow flow may be so small as to be largely undetected, and in spectral mode, the waveform will be difficult to analyze.
• Correct answer D: Raising the baseline will change where on the screen the signal is visualized, but will not change the character of the signal itself.
2014 SPR PG Course
Which of the following is NOT important for slow flow detection?
• 1. Hernanz-Schulman, M., Applications of Doppler sonography to diagnosis of extracranial pediatric disease. Radiology, 1993. 189(1): p. 1-14.
• 2. Mitchell, D.G., Color Doppler imaging: principles, limitations, and artifacts.Radiology, 1990. 177(1): p. 1-10.
• 3. Pozniak, M.A., J.A. Zagzebski, and K.A. Scanlan, Spectral and color Doppler artifacts. Radiographics, 1992. 12(1): p. 35-44.
• 4. Scoutt, L.M., M.L. Zawin, and K.J. Taylor, Doppler US. Part II. Clinical applications. Radiology, 1990. 174(2): p. 309-19.
• 5. Taylor, K.J. and S. Holland, Doppler US. Part I. Basic principles, instrumentation, and pitfalls. Radiology, 1990. 174(2): p. 297-307.
• 6. Winkler, P. and K. Helmke, Major pitfalls in Doppler investigations with particular reference to the cerebral vascular system. Part I. Sources of error, resulting pitfalls and measures to prevent errors. Pediatr Radiol, 1990. 20(4): p. 219-28.
• 7. Winkler, P., K. Helmke, and M. Mahl, Major pitfalls in Doppler investigations. Part II. Low flow velocities and colour Doppler applications. Pediatr Radiol, 1990. 20(5): p. 304-10.
2014 SPR PG Course
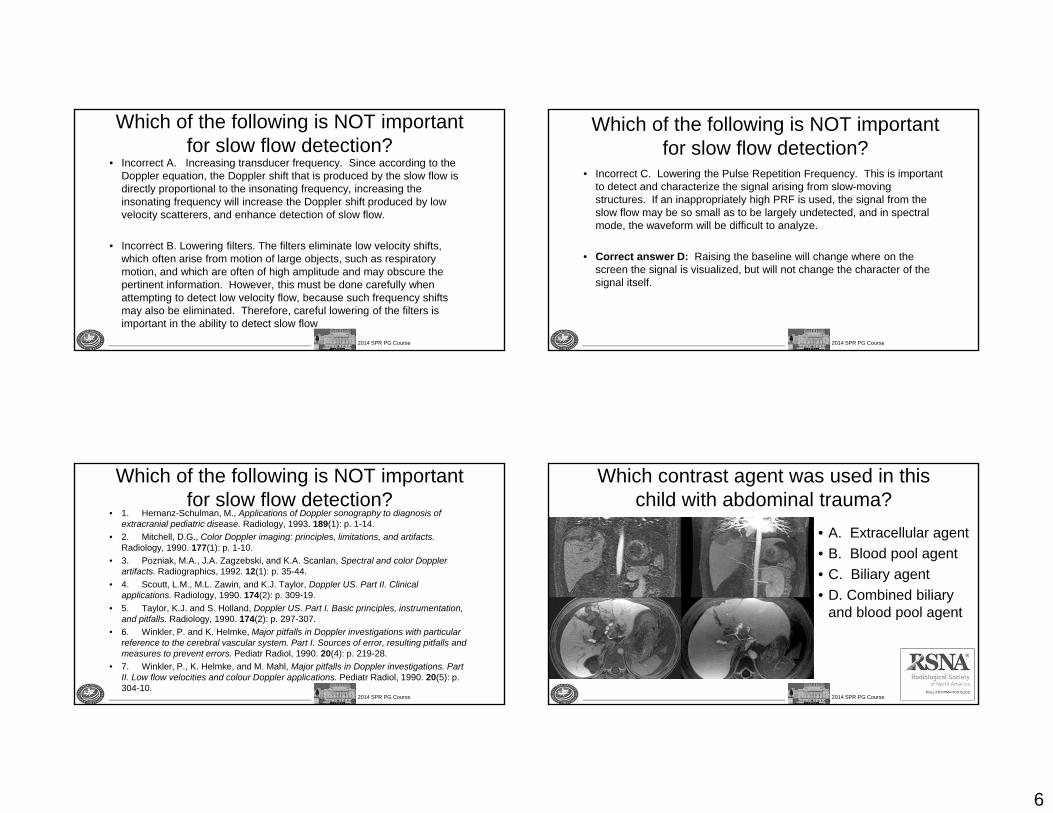
Which contrast agent was used in this child with abdominal trauma?
• A. Extracellular agent• B. Blood pool agent• C. Biliary agent• D. Combined biliary
and blood pool agent
7
2014 SPR PG Course
Which contrast agent was used in this child with abdominal trauma?
• Answer: E. both gadoxetate (Eovist) for biliary evaluation and gadofosveset (Ablavar) for vascular evaluation
• Rationale: Note that vascular structures, the liver, and the bile ducts are all bright, indicative of two contrast agents.
2014 SPR PG Course
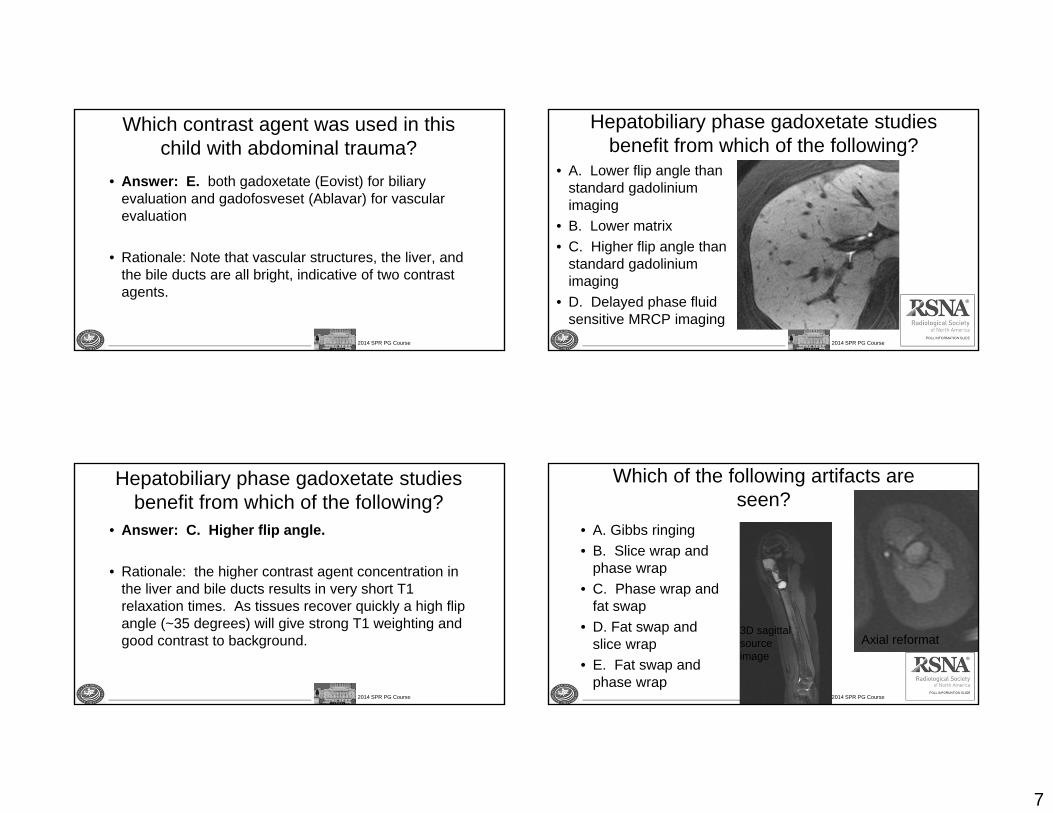
Hepatobiliary phase gadoxetate studies benefit from which of the following?
• A. Lower flip angle than standard gadolinium imaging
• B. Lower matrix• C. Higher flip angle than
standard gadolinium imaging
• D. Delayed phase fluid sensitive MRCP imaging
2014 SPR PG Course
Hepatobiliary phase gadoxetate studies benefit from which of the following?
• Answer: C. Higher flip angle.
• Rationale: the higher contrast agent concentration in the liver and bile ducts results in very short T1 relaxation times. As tissues recover quickly a high flip angle (~35 degrees) will give strong T1 weighting and good contrast to background.
2014 SPR PG Course
Which of the following artifacts are seen?
• A. Gibbs ringing• B. Slice wrap and
phase wrap• C. Phase wrap and
fat swap• D. Fat swap and
slice wrap• E. Fat swap and
phase wrap
Axial reformat3D sagittal sourceimage
8
2014 SPR PG Course
Which artifacts are seen?
Answer: D. Fat swap and slice wrap.
Rationale: Two point dixon imaging isperformed here, which usually giveshomogeneous fat suppression. However,occassionally components of what shouldbe in a fat image get improperly allocatedto the water image, and vice versa,i.e. a fat-water swap. Also, when 3Dimaging is performed, as in this case, theslab excitation profile is not perfect, soexcited tissue that is beyond the nominalslab may wrap in the slice direction.
2014 SPR PG Course
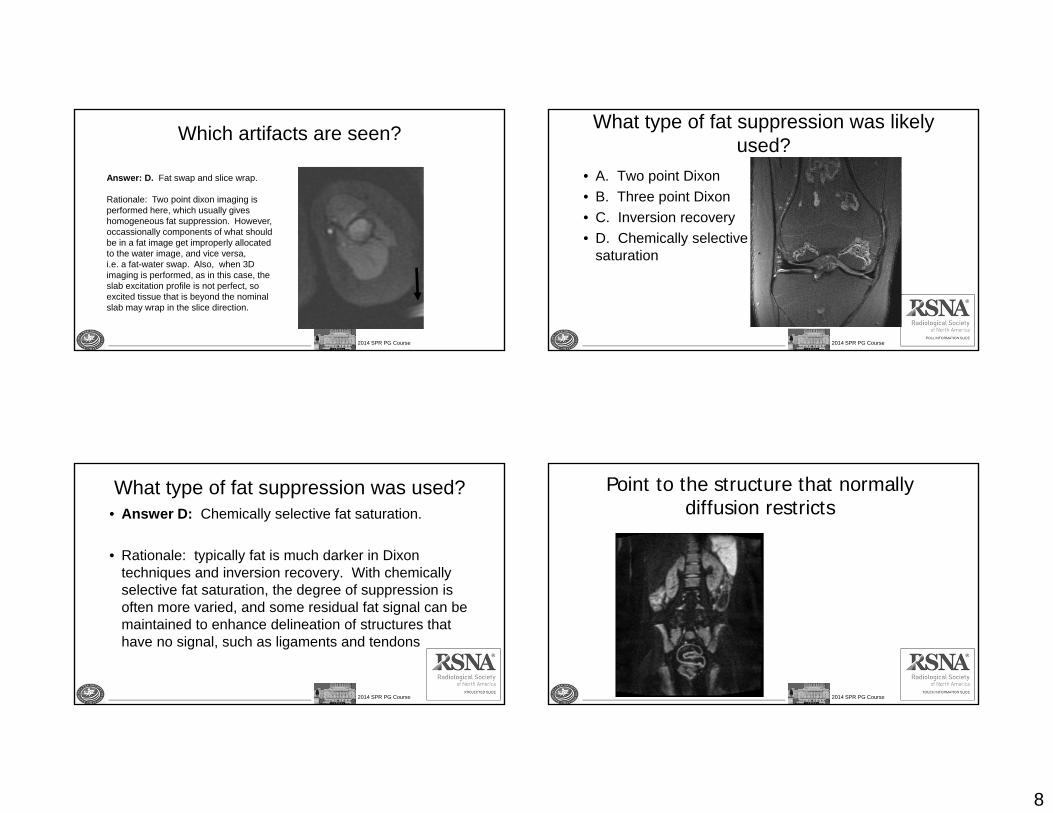
What type of fat suppression was likely used?
• A. Two point Dixon• B. Three point Dixon• C. Inversion recovery• D. Chemically selective
saturation
2014 SPR PG Course
What type of fat suppression was used?• Answer D: Chemically selective fat saturation.
• Rationale: typically fat is much darker in Dixon techniques and inversion recovery. With chemically selective fat saturation, the degree of suppression is often more varied, and some residual fat signal can be maintained to enhance delineation of structures that have no signal, such as ligaments and tendons
2014 SPR PG Course
Point to the structure that normally diffusion restricts
9
2014 SPR PG Course
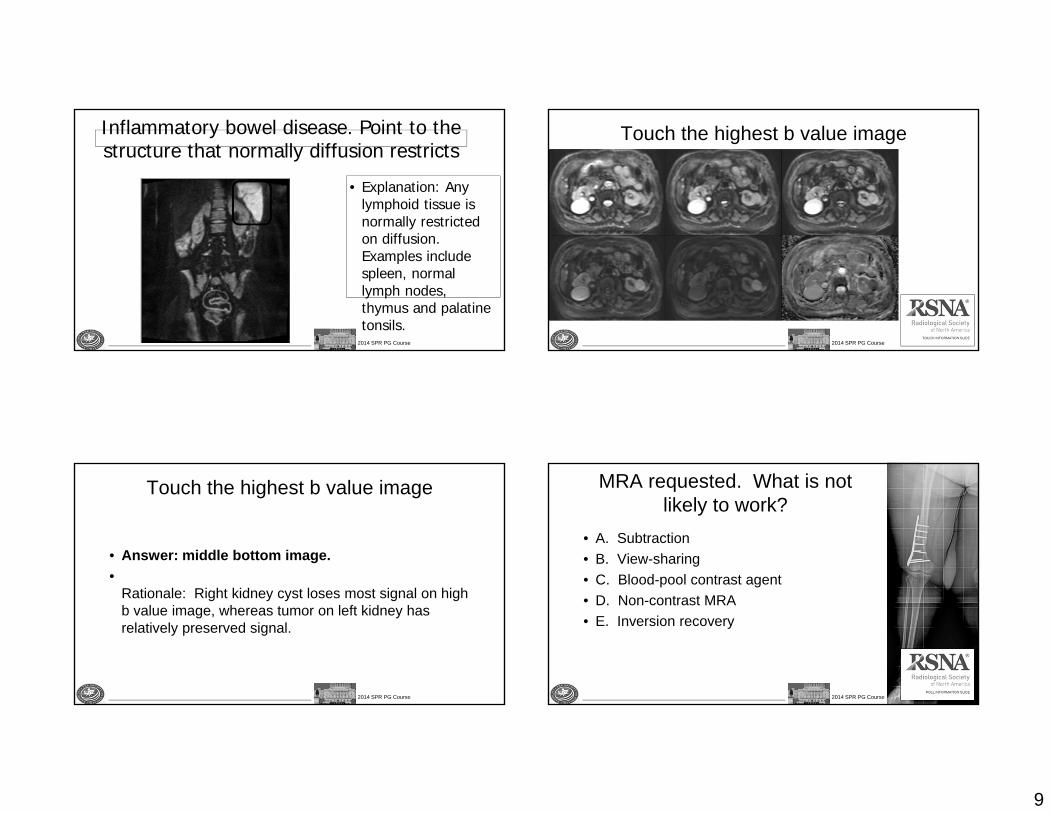
Inflammatory bowel disease. Point to the structure that normally diffusion restricts
• Explanation: Any lymphoid tissue is normally restricted on diffusion. Examples include spleen, normal lymph nodes, thymus and palatine tonsils.
2014 SPR PG Course
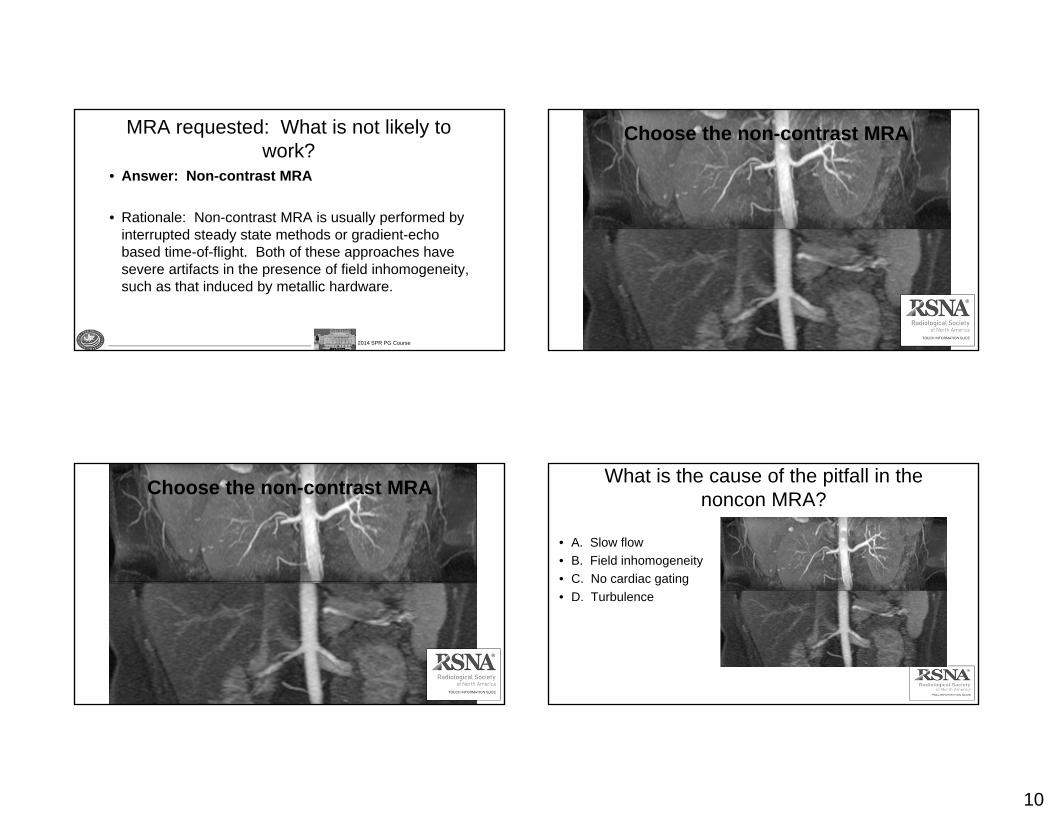
Touch the highest b value image
2014 SPR PG Course
Touch the highest b value image
• Answer: middle bottom image.•
Rationale: Right kidney cyst loses most signal on high b value image, whereas tumor on left kidney has relatively preserved signal.
2014 SPR PG Course
MRA requested. What is not likely to work?
• A. Subtraction• B. View-sharing• C. Blood-pool contrast agent• D. Non-contrast MRA• E. Inversion recovery
10
2014 SPR PG Course
MRA requested: What is not likely to work?
• Answer: Non-contrast MRA
• Rationale: Non-contrast MRA is usually performed by interrupted steady state methods or gradient-echo based time-of-flight. Both of these approaches have severe artifacts in the presence of field inhomogeneity, such as that induced by metallic hardware.
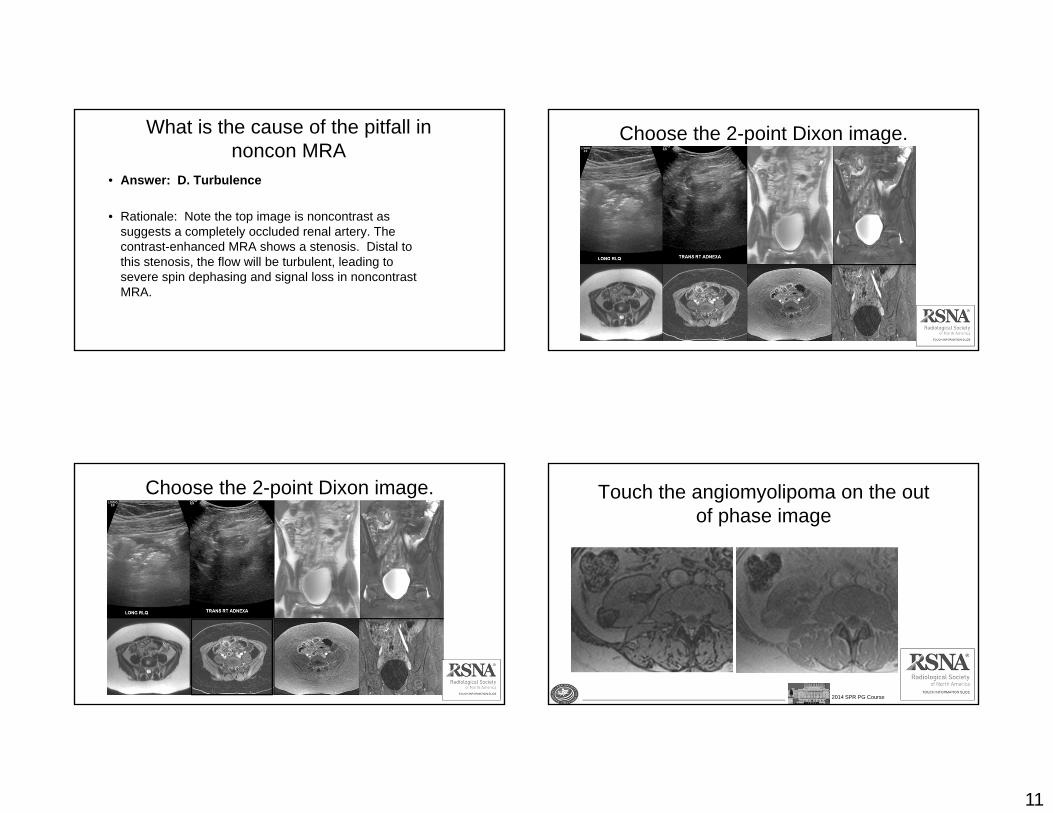
Choose the non-contrast MRA
Choose the non-contrast MRA What is the cause of the pitfall in the noncon MRA?
• A. Slow flow• B. Field inhomogeneity• C. No cardiac gating• D. Turbulence
11
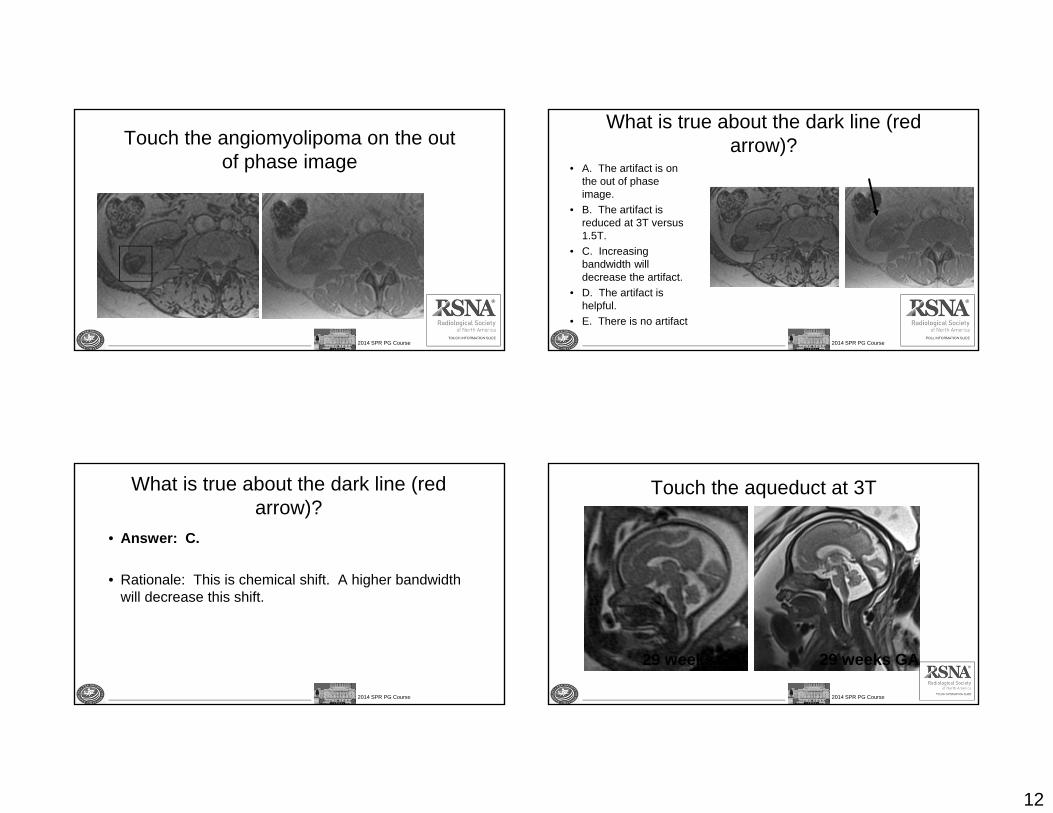
What is the cause of the pitfall in noncon MRA
• Answer: D. Turbulence
• Rationale: Note the top image is noncontrast as suggests a completely occluded renal artery. The contrast-enhanced MRA shows a stenosis. Distal to this stenosis, the flow will be turbulent, leading to severe spin dephasing and signal loss in noncontrastMRA.
Choose the 2-point Dixon image.
Choose the 2-point Dixon image.
2014 SPR PG Course
Touch the angiomyolipoma on the out of phase image
12
2014 SPR PG Course
Touch the angiomyolipoma on the out of phase image
2014 SPR PG Course
What is true about the dark line (red arrow)?
• A. The artifact is on the out of phase image.
• B. The artifact is reduced at 3T versus 1.5T.
• C. Increasing bandwidth will decrease the artifact.
• D. The artifact is helpful.
• E. There is no artifact
2014 SPR PG Course
What is true about the dark line (red arrow)?
• Answer: C.
• Rationale: This is chemical shift. A higher bandwidth will decrease this shift.
2014 SPR PG Course
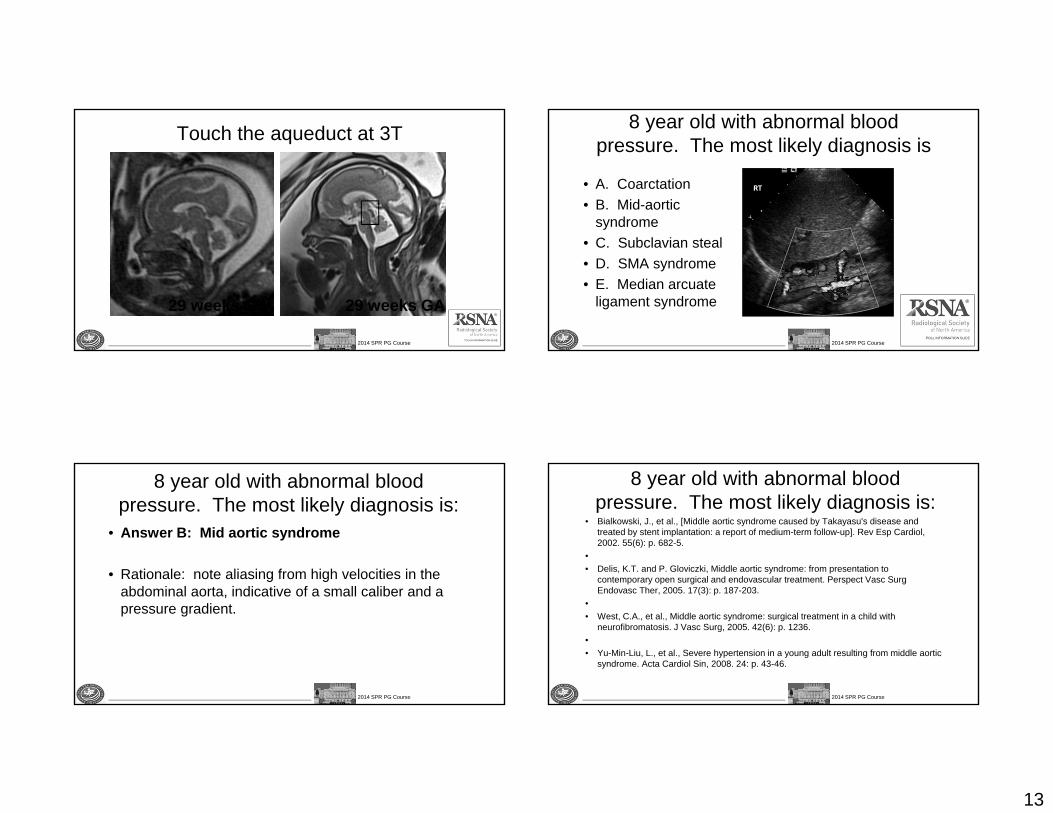
Touch the aqueduct at 3T
29 weeks GA 29 weeks GA
13
2014 SPR PG Course
Touch the aqueduct at 3T
29 weeks GA 29 weeks GA
2014 SPR PG Course
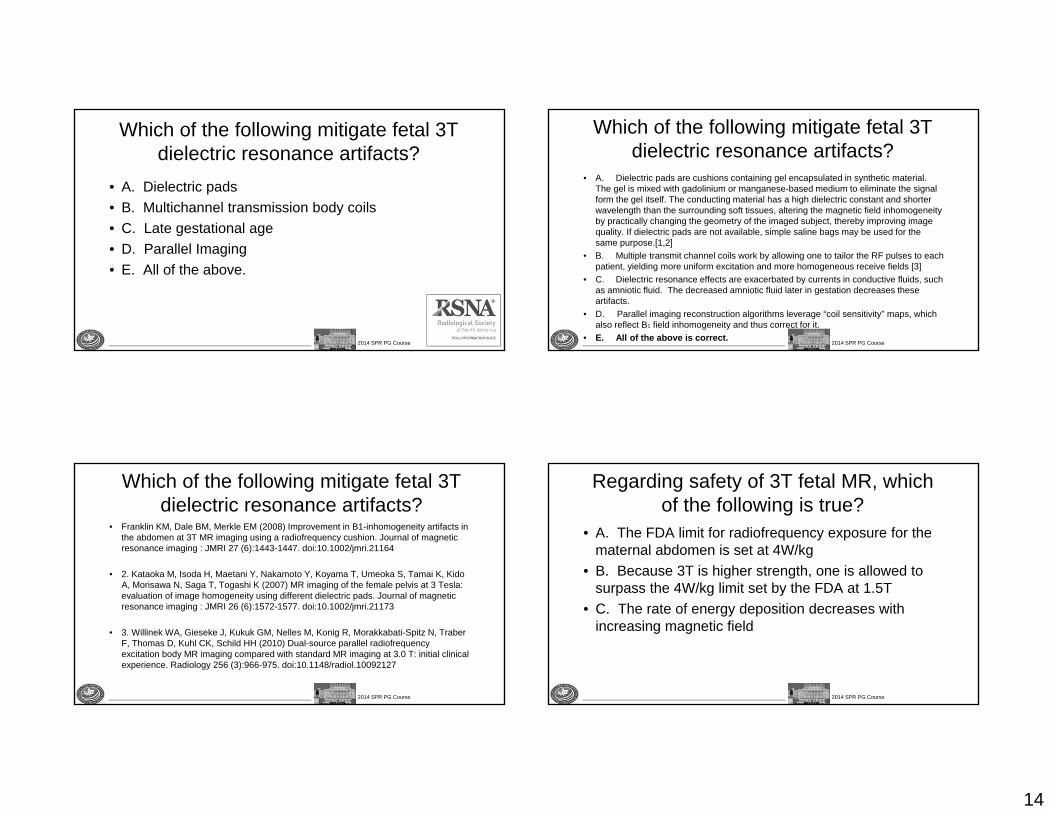
8 year old with abnormal blood pressure. The most likely diagnosis is
• A. Coarctation• B. Mid-aortic
syndrome• C. Subclavian steal• D. SMA syndrome• E. Median arcuate
ligament syndrome
2014 SPR PG Course
8 year old with abnormal blood pressure. The most likely diagnosis is:
• Answer B: Mid aortic syndrome
• Rationale: note aliasing from high velocities in the abdominal aorta, indicative of a small caliber and a pressure gradient.
2014 SPR PG Course
8 year old with abnormal blood pressure. The most likely diagnosis is:
• Bialkowski, J., et al., [Middle aortic syndrome caused by Takayasu's disease and treated by stent implantation: a report of medium-term follow-up]. Rev Esp Cardiol, 2002. 55(6): p. 682-5.
•• Delis, K.T. and P. Gloviczki, Middle aortic syndrome: from presentation to
contemporary open surgical and endovascular treatment. Perspect Vasc SurgEndovasc Ther, 2005. 17(3): p. 187-203.
•• West, C.A., et al., Middle aortic syndrome: surgical treatment in a child with
neurofibromatosis. J Vasc Surg, 2005. 42(6): p. 1236.•• Yu-Min-Liu, L., et al., Severe hypertension in a young adult resulting from middle aortic
syndrome. Acta Cardiol Sin, 2008. 24: p. 43-46.
14
2014 SPR PG Course
Which of the following mitigate fetal 3T dielectric resonance artifacts?
• A. Dielectric pads• B. Multichannel transmission body coils• C. Late gestational age• D. Parallel Imaging• E. All of the above.
2014 SPR PG Course
Which of the following mitigate fetal 3T dielectric resonance artifacts?
• A. Dielectric pads are cushions containing gel encapsulated in synthetic material. The gel is mixed with gadolinium or manganese-based medium to eliminate the signal form the gel itself. The conducting material has a high dielectric constant and shorter wavelength than the surrounding soft tissues, altering the magnetic field inhomogeneity by practically changing the geometry of the imaged subject, thereby improving image quality. If dielectric pads are not available, simple saline bags may be used for the same purpose.[1,2]
• B. Multiple transmit channel coils work by allowing one to tailor the RF pulses to each patient, yielding more uniform excitation and more homogeneous receive fields [3]
• C. Dielectric resonance effects are exacerbated by currents in conductive fluids, such as amniotic fluid. The decreased amniotic fluid later in gestation decreases these artifacts.
• D. Parallel imaging reconstruction algorithms leverage “coil sensitivity” maps, which also reflect B1 field inhomogeneity and thus correct for it.
• E. All of the above is correct.
2014 SPR PG Course
Which of the following mitigate fetal 3T dielectric resonance artifacts?
• Franklin KM, Dale BM, Merkle EM (2008) Improvement in B1-inhomogeneity artifacts in the abdomen at 3T MR imaging using a radiofrequency cushion. Journal of magnetic resonance imaging : JMRI 27 (6):1443-1447. doi:10.1002/jmri.21164
• 2. Kataoka M, Isoda H, Maetani Y, Nakamoto Y, Koyama T, Umeoka S, Tamai K, Kido A, Morisawa N, Saga T, Togashi K (2007) MR imaging of the female pelvis at 3 Tesla: evaluation of image homogeneity using different dielectric pads. Journal of magnetic resonance imaging : JMRI 26 (6):1572-1577. doi:10.1002/jmri.21173
• 3. Willinek WA, Gieseke J, Kukuk GM, Nelles M, Konig R, Morakkabati-Spitz N, TraberF, Thomas D, Kuhl CK, Schild HH (2010) Dual-source parallel radiofrequency excitation body MR imaging compared with standard MR imaging at 3.0 T: initial clinical experience. Radiology 256 (3):966-975. doi:10.1148/radiol.10092127
2014 SPR PG Course
Regarding safety of 3T fetal MR, which of the following is true?
• A. The FDA limit for radiofrequency exposure for the maternal abdomen is set at 4W/kg
• B. Because 3T is higher strength, one is allowed to surpass the 4W/kg limit set by the FDA at 1.5T
• C. The rate of energy deposition decreases with increasing magnetic field
15
2014 SPR PG Course
Regarding safety of 3T fetal MR, which of the following is true?
• Correct answer: A. The FDA limits of exposure to changing magnetic fields are independent of magnetic field strength, remaining at 4W/kg to the maternal abdomen at 1.5 and 3T imaging. B is thus wrong. C is also wrong, as the rate of energy deposition will in fact increase with increasing magnetic fields. Optimizing protocol is necessary to decrease SAR while scanning at 3T (utilizing, for example, decreasing number of slices, lowering flip angles, or increasing repetition time)
• Shellock FG, Crues JV (2004) MR procedures: biologic effects, safety, and patient care. Radiology 232 (3):635-652. doi:10.1148/radiol.2323030830
2014 SPR PG Course
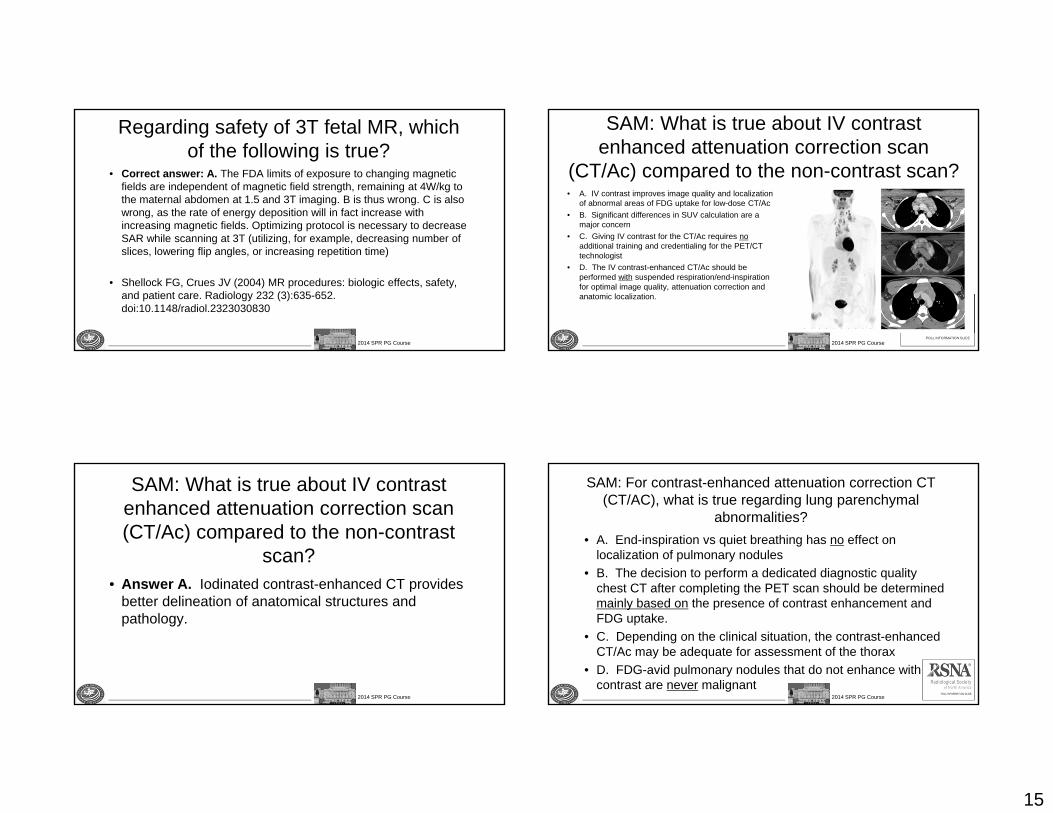
SAM: What is true about IV contrast enhanced attenuation correction scan
(CT/Ac) compared to the non-contrast scan?• A. IV contrast improves image quality and localization
of abnormal areas of FDG uptake for low-dose CT/Ac• B. Significant differences in SUV calculation are a
major concern• C. Giving IV contrast for the CT/Ac requires no
additional training and credentialing for the PET/CT technologist
• D. The IV contrast-enhanced CT/Ac should be performed with suspended respiration/end-inspiration for optimal image quality, attenuation correction and anatomic localization.
2014 SPR PG Course
SAM: What is true about IV contrast enhanced attenuation correction scan (CT/Ac) compared to the non-contrast
scan?• Answer A. Iodinated contrast-enhanced CT provides
better delineation of anatomical structures and pathology.
2014 SPR PG Course
SAM: For contrast-enhanced attenuation correction CT (CT/AC), what is true regarding lung parenchymal
abnormalities?• A. End-inspiration vs quiet breathing has no effect on
localization of pulmonary nodules• B. The decision to perform a dedicated diagnostic quality
chest CT after completing the PET scan should be determined mainly based on the presence of contrast enhancement and FDG uptake.
• C. Depending on the clinical situation, the contrast-enhanced CT/Ac may be adequate for assessment of the thorax
• D. FDG-avid pulmonary nodules that do not enhance with IV contrast are never malignant
16
2014 SPR PG Course
For contrast-enhanced attenuation correction CT (CT/AC), which is true regarding lung parenchymal
abnormalities?
• Answer is C.
2014 SPR PG Course
SAM: In Doppler US, which will NOT decrease aliasing?
• A. Increasing the pulse repetition frequency• B. Decreasing the insonating frequency• C. Increasing the angle of insonation• D. Lowering the baseline • E. Decreasing the level of the filters
2014 SPR PG Course
In Doppler US, which will NOT decrease aliasing?
• A. Increasing the Pulse Repetition Frequency . Aliasing occurs as a result of sampling frequencies above the Nyquist frequency, which is defined as ½ of the Pulse Repetition Frequency. Therefore, increasing the Pulse Repetition Frequency is one of the best ways to decrease or eliminate aliasing.
• B. Decreasing the insonating frequency. The Doppler shift that occurs secondary to motion of the interrogated object is defined by the following equation: fD = (2f0vcos)/c, where fD = the frequency of the detected Doppler shift, f0 = the insonating frequency, v = the velocity of the moving object, and c = the speed of sound in tissue. Therefore, decreasing the insonating frequency will decrease the frequency of the detected Doppler shift, and decrease aliasing.
• C. Increasing the angle of insonation. The detected Doppler frequency shift, fD , also depends on the cosine of . Since the cosine of 0o is 1, and this decreases to 0 90o , increasing the angle of insonation will decrease the magnitude of the frequency shift, and reduce aliasing.
2014 SPR PG Course
In Doppler US, which will NOT decrease aliasing?
• D. Lowering the baseline. Lowering the baseline does not decrease the frequency shift. However lowering the baseline changes how the Doppler shift is depicted, so that wrapping is decreased and possibly eliminated without necessarily changing the parameters that will reduce the Doppler frequency shift.
•• Correct answer E. Decreasing the level of the filters. The filters
eliminate low frequency shifts, which often have very high amplitude, but emanate from motion of solid tissues, such as that which arises from respiratory motion, or from the vessel walls (also known as “wall thump”). These very low velocity “noise” shifts have nothing to do with the high velocities that generate aliasing, and therefore this is the correct answer.

17
2014 SPR PG Course
In Doppler US, which will NOT decrease aliasing?
• 1. Hernanz-Schulman, M., Applications of Doppler sonography to diagnosis of extracranial pediatric disease. Radiology, 1993. 189(1): p. 1-14.
• 2. Mitchell, D.G., Color Doppler imaging: principles, limitations, and artifacts. Radiology, 1990. 177(1): p. 1-10.
• 3. Pozniak, M.A., J.A. Zagzebski, and K.A. Scanlan, Spectral and color Doppler artifacts. Radiographics, 1992. 12(1): p. 35-44.
• 4. Scoutt, L.M., M.L. Zawin, and K.J. Taylor, Doppler US. Part II. Clinical applications. Radiology, 1990. 174(2): p. 309-19.
• 5. Taylor, K.J. and S. Holland, Doppler US. Part I. Basic principles, instrumentation, and pitfalls. Radiology, 1990. 174(2): p. 297-307.
• 6. Winkler, P. and K. Helmke, Major pitfalls in Doppler investigations with particular reference to the cerebral vascular system. Part I. Sources of error, resulting pitfalls and measures to prevent errors. Pediatr Radiol, 1990. 20(4): p. 219-28.
• 7. Winkler, P., K. Helmke, and M. Mahl, Major pitfalls in Doppler investigations. Part II. Low flow velocities and colour Doppler applications. Pediatr Radiol, 1990. 20(5): p. 304-10.