Embed Size (px)
Citation preview
Quality Health Care for KidsSchool-Based Health Centers
KidsHealthy Schools Begin with Healthy
2007Status Report


�
School-Based Health Center (SBHC) Fast Facts ................................1
SBHCs Today ...................................................................................... 2
Quality Health Care Projects .............................................................. 3
Access to Care .....................................................................................6
Wellness ..............................................................................................8
Mental Health ................................................................................... 10
Alcohol, Tobacco, and Other Drugs ................................................. 12
Reproductive Health and Sexual Risk Reduction ............................ 14
In their Words: What do Students Say? .......................................... 16
Certification ...................................................................................... 18
Funding and Operations .................................................................. 19
Partners ............................................................................................20
Contact information ......................................................................... 21
Additional Information .................................................................... 21
Acknowledgements ...........................................................................22
Table of Contents
“There is
no other place I can go and get medi-cine or shots. Since
my mom can’t drive, I come here to the health
center.”
- 15-year-old female

�
“We are entering an era of great oppor-tunity for Oregon. We have the ability to do more, the opportunity to do better and the responsibility to do our best. One of the ways we can do better is to ensure all kids have access to quality health care by expanding the number of school-based health centers across the state. We know that ‘healthy kids learn better’ and school-based health centers are critical to providing the quality care our kids deserve so they have their health needs met and can get back to the classroom faster.”
Governor Ted Kulongoski, December 2006
School-Based Health Center (SBHC) Fast FactsForty-four centers in 17 counties
Twenty-eight high schoolsEight middle schoolsSeven elementary schoolsOne K-12 school
Three counties received funds to plan new SBHCs
In service year 2005-2006:
There were 39,249 students with access to SBHCs at their school
Oregon SBHCs served 20,177 clients in 63,863 visits
Female clients represent 59 percent of clients and 64 percent of visits
Forty-two percent of SBHC clients were uninsured
Of SBHC clients reporting 60 percent were unlikely to receive care out-side of the SBHC
Sixty-eight percent of students reported their health was better because of the SBHC
The State of Oregon contributed $1,250,000 to SBHCs, which supported the delivery of over $2,412,000 in health care services, including over $946,000 in health care services to uninsured students.*
••••
•
•
•
•
•
•
*Estimate based on 2005-2006 utilization data.
“Excellent
service, great staff, an asset to the community.”
- 16-year-old male

�
SBHCs TodayWhat is an SBHC?School-Based Health Centers in Oregon are primary care clinics located at schools. They provide developmentally appropriate physical, emotional, behavioral and preventive health care to students regardless of their ability to pay.
What do they look like?SBHCs are staffed like a local pediatrician or family practice office
with a receptionist, nurse, clinical provider (nurse practitioner, physician assistant, or physician), and at some sites, qualified mental health professionals. At the same time they incorporate the school and student surroundings with student-made artwork on the walls, beanbag chairs in the lobby, and teen-friendly music in the lobby.
They are made to be comfortable and accessible so kids drop by when they need medical attention and/or want to learn more about
a health issue. This is validated by patient satisfaction surveys and staff reporting that students come in asking for aspirin and leave having gotten
help about abuse, depression, and dental needs.
Why have one? Healthy kids learn better
SBHCs are prevention-oriented
SBHCs see children who otherwise would not get care
Students say SBHCs get them back to the classroom faster
What’s happening today in Oregon’s SBHCs?322 students are receiving physical health care144 students without insurance are receiving health care85 students are receiving sexual risk reduction visits 43 students are receiving mental health care 30 students are receiving well/prevention visits21 students are receiving immunizations
•
•
•
•
“I am very
satisfied with the care I receive at the
health center and I am happy it is a resource here. I would not be very healthy or aware of my health deci-sions if it were not for the
health center.
– 15-year-old female

�
“I had come
to the health center and the nurse was look-ing at my back because I
had broken out in a rash. She noticed a mole and said it might be melanoma. I went to the skin
doctor the next day and he took it off right away. The health center
is important to me because it helped me prevent my prob-
lem from getting worse.”
– 16-year-old female
Quality Health Care ProjectsAfter 20 years of service and with 44 School-Based Health Centers (SBHC) in 17 counties, the Oregon SBHC model continues to evolve and strengthen to support healthy youth development. This past year proactive steps were taken to ensure our kids are receiving the quality health care they need. Cur-rently, SBHCs focus on prevention, primary care and mental health services. As these health care models progress with emerging technology and research, so must our SBHC program. In 2005-2006, SBHCs focused on the following projects to strengthen the quality of care and demonstrate the quality of services pro-vided.
Supporting Partnerships and Aligning Practice StandardsTo illustrate our commitment to high quality, age appropriate, accessible health care for school-aged youth, this past year the State SBHC Program Of-fice worked hard to align public health standards and coordinate interagency supports and technical assistance. Some partners include the Oregon Board of Pharmacy, Board of Nursing, Board of Medical Examiners, Department of Hu-man Services Immunization Program, and the State Public Health Laboratory. Not only are Oregon SBHCs partnering with other State agencies to further develop a high quality of care, we are also following national recommenda-tions for continuous quality improvement.
This past year, Oregon SBHCs have initiated a quality im-provement project targeting three key health performance measures (KPM): risk assessments, comprehensive physical exams, and body mass index (BMI) measure-ments, with a plan to include additional measures in the future. The goal of this project is to help individual sites identify areas of practice improvement and also guarantee quality care that addresses emerging child and adolescent health issues.

�
Mental Health Needs AssessmentAs we focus attention on emerging public health priorities, child and ado-lescent mental health and wellness become an essential topic. A child’s or adolescent’s mental health affects cognitive, social, and emotional growth. Creating a sustainable mental health foundation helps promote positive youth development. Currently, we know that Oregon’s SBHCs provide accessible mental health care to children and adolescents. However, the information concerning the mental health practices in our SBHCs is limited. Therefore, in order to strengthen the quality of mental health care provided, the State Program Office is assessing the current SBHC mental health system within each community. The goal of the assessment project is to provide a comprehensive understanding of the strengths and needs of the current mental health system operating in Oregon’s SBHCs. This information can guide our training, technical assistance and efforts to im-prove the overall quality of mental health services provided by our SBHCs.
Cost ModelingHow much a school-based health center costs is an elusive question due to the unique nature of the multiple community partnerships. Although focusing on health care practice is essential to quality care, determining the cost of SBHCs allows sites to maximize resources and work towards sustainability. The State SBHC Program Office is currently developing a new cost-modeling project. The goal of this project is to estimate the cost required to open a new SBHC site and also to sustain an operational SBHC. A related objective is to analyze the efficiency and cost-effectiveness of delivering healthcare services in SBHCs. Prospective centers will use the cost estimates to approximate the funds for start-up, and existing SBHCs will use the information to approximate the funds for expansion of services or hours of operation. This project will also provide centers with data and evidence necessary to engage local resources and support from their local communities.
“I have
known the health center for three years now and they really try to help you get better and I have changed
since the day I met the health clinic.”
- 13-year-old male
“A student had been seen here several times for various concerns, felt comfortable enough to come into the counseling office, and then the health center to reveal that although she had been using cutting as a cop-ing method in the past, she was considering cutting deeper to kill herself. She was able to come in and ask for help because she had developed a safe and caring relationship with the staff of the SBHC. With help from SBHC staff and county Mental Health she was admitted to the hospital for inpatient care, counseling, and support. Without the help of the SBHC she might not have been able to express her deep depression and concerns.”
– SBHC Primary Care Provider

�
What do Oregonians say about SBHCs?For the first time, the SBHC State Program Office was able to develop statewide public opinion data to evaluate the importance of various types of health care services provided in SBHCs. In 2005, the Behavioral Risk Factor Surveillance System, the largest ongoing telephone health survey system, asked Oregonians questions about the importance of providing health care services in a school-based setting.
Oregonians overwhelmingly confirmed that the 12 major health services provided by SBHCs in Oregon schools are important (“very important” or “somewhat important”).
Ninety percent or more of the public named alcohol and drug prevention, treatment for minor injuries, mental health counseling, sports exams, family planning counseling, and vaccinations as important health services provided in Oregon’s SBHCs.
“School-based health
centers are impor-tant to me because it’s an environment where I
feel safe. I like the fact that I can go in there for just about anything and they make me feel welcome.”
–15-year-old female

�
Access to CareWhat’s Happening Out ThereOregon children and families are facing many barriers to obtaining consistent and reliable access to health care. Compared to the rest of the population, families bear a disproportionate economic and social burden. An estimated 18 percent of Oregon children under 18 live in poverty (more than 150,000 children), the 23rd highest rate in the U.S. and the fifth highest in the Western U.S.1 In addition, an estimated 41 percent of Oregon children are living at or below 200 percent of the poverty level2, which is above the national average of 39 percent.3 Nationwide, parents in low-income jobs can have a more difficult time accessing health care for themselves and their children, with transporta-tion and affordability being particularly problematic.4
Health care needs are increasing for Oregon’s youth:
Rates of un-insurance are rising among children under 18, and are highest for adolescents.5
Between 2000 and 2004, the rate of youth under 18 with no health insur-ance in Oregon climbed from 8.5 percent to 12.3 percent.6
More than 62,000 uninsured children are income-eligible for public medical coverage.7
Uninsured children are 30 percent less likely to receive medical atten-tion when they are injured.8
One third of eighth and 11th grade girls report they had an unmet physi-cal or emotional need in the past year.9
1 American Community Survey2 2002 National Center on Child Poverty survey: 200% of poverty level was $37,700 for family of four.3 Ibid.4 Flores, G., Abreu, M., Olivar, MA, et al. (1998). Access barriers to health care for Latino children. Ar-chives of pediatrics and adolescent medicine, 152(11): 1119-25. 5 2003 National Survey of Children’s Health6 Oregon Population Survey, 2004� Covering Kids in Oregon. Office for Oregon Health Policy & Research, May 2005� Covering Kids: Children’s Access to Healthcare. Oregon Health Research & Evaluation Collaborative, January 2006.9 Oregon Health Teens 2006
•
•
•
•
•

�
What SBHCs are doing to helpSBHCs provide health care access to the entire student community at that school, and in some cases to the entire school district or community. Access to health care is easier and more convenient, relationships with providers are consistent, services are provided regardless of a student’s ability to pay, and SBHC providers are focused on adolescent health issues. This care includes:
Performing routine physical and sports examsDiagnosing and treating acute and chronic illnessTreating minor injuries/illnessesProviding vision, dental and blood pressure screeningsAdministering vaccinationsAlcohol and drug prevention and treatmentHealth education, counseling and wellness promotionProviding or connecting students with mental health counselingGiving classroom presentations on health and wellnessPrescribing medicationReproductive health services
See page 5 of this report for public opinion data that demonstrates Orego-nians are in support of having these types of health services in a school setting.
Patient Satisfaction Survey 2005-2006:
Sixty percent of students say they were unlikely to access health care without an SBHCNinety-seven percent rate the health care they receive at the SBHC as good or excellentSixty-seven percent say that their health has improved because of the SBHC
•
•
••
••
•
•
•••
•
•
•
Students voted with their feet — Oregon’s SBHCs served 20,177 students in 63,863 visits.

�
WellnessWhat’s Happening Out ThereBoth nationally and statewide, students are facing many challenges when it comes to wellness and healthy living. In the U.S., rates of childhood obesity are on the rise while kids are getting less and less physical activity. Portion sizes are increasing and targeted marketing of fast foods to kids and teens is problematic. All of these factors are combining to make it more difficult for kids and families to stay healthy and make good choices.
According to the 2006 Oregon Healthy Teens survey:
One in four 11th graders were either overweight or at risk for becom-ing overweight. There was a large gender gap with 31 percent of boys fitting into one of these categories as opposed to 19 percent of girls.Only one in four eighth graders reported they ate the recommended amount of fruits and vegetables over the past week. This is down from one in three in 2005.Only 36 percent of 11th graders ate breakfast every day.Twenty-two percent of eighth grade girls and 67 percent of 11th grade girls don’t attend any PE classes during an average school week.
Immunizations are the cornerstone of public health prevention. While many people identify immunizations only with early childhood, there are several important immunizations for older children and adolescents, including men-ingitis and pertussis. This is an area where school-based health centers can have a major impact.
In 2006, the FDA approved a new vaccine against HPV (Human Papilloma Virus), one of the main causes of cervical cancer. The HPV vaccine is recom-mended for girls and young women ages nine to 26. Many SBHCs will soon
have the capacity to provide this vaccine.
The National Association for Sports and Physical Education recom-mends that secondary students receive at least 225 minutes of weekly physical education. However, many schools and districts are facing financial struggles, and are cutting back PE programs for students. The importance of prevention and wellness messaging cannot be
overlooked.
“I think
that the shots I was given will pro-
tect me in the future and I’m glad I got
them.”
–14-year-old male

�
What SBHCs are doing to helpPrevention care is at the forefront of SBHC care as seen in the areas of well child/prevention check-ups, risk assessments, prevention mes-saging and immunizations. SBHCs provide well child/prevention exams on an ongoing basis. In addition, providers aggressively screen students for health and behavior risk factors that might be the first sign of a problem, and intervene. This is particularly important as health patterns established by the end of adolescence are carried through adulthood.10 Prevention messages are given routinely as part of visits, and students report high numbers of prevention messages. In fact, 85 percent of students reported receiving at least one or more of the prevention messages below during their visit.
Given the current obesity epidemic among children, it is important to note that 47 percent of students received nutrition messages and 40 percent received physical activity messages. Hearing these messages consistently in the clinic, the classroom, and at home encourages students to shape healthy lifestyles.
In 2005-2006, 7,736 immunizations were administered to 3,595 SBHC students. That doesn’t include those who were referred back to their primary care provider!
10 Muscari, M. E. (1999). Prevention are we really reaching today’s teens? American Journal of Maternal Child Nursing, 24(2), 87-91.
“I would not
have had care for my 5-year old after
a divorce, no money or health coverage. I now
prefer coming here rather than anywhere else.
- Parent of SBHC client

�0
Mental HealthWhat’s Happening Out ThereIn the United States, about one in five children and adolescents have some type of mental health disorder and one in 10 suffer from a mental health disorder severe enough to cause some level of impairment socially, aca-demically and emotionally.11 However, among these children and adolescents suffering from a mental illness with some level of impairment, only about one in five or 20 percent are receiving the treatment they need.12
In Oregon, there are 12 to 22 percent of children who need some level of men-tal health service and about seven percent of children (more than 60,000) who suffer from a serious emotional disturbance causing impairment.13 Although we do not know exactly how many of Oregon’s children receive mental health services based on insurance status, we do know that in 2005-06, more than 37,000 of Oregon’s youth were served by the public mental health system, an increase of almost 13 percent from 2004-05.
Important mental and emotional health facts from the 2006 Or-egon Healthy Teens survey of 8th and 11th graders:
Eleven percent of eighth grade girls and 18 percent of 11th grade girls reported having been diagnosed with depression, anxiety or another emotional condition. One in five 11th graders reported feeling so sad and hopeless that they stopped all normal activities for at least two weeks.Thirty-nine percent of 11th graders said they had been harassed in the last year at school.One in 10 students said they had attacked someone on school property in the last year with the intent of seriously hurting them.Seventeen percent of eighth grade boys said they had carried a hand-gun in the past year.More than half of girls who were at a normal weight said they were actively trying to lose weight.Sixteeen percent of girls seriously considered attempting suicide in the past year. Of those, about half reported they attempted suicide.
11 US Surgeon General’s Report on Mental Health, 199912 Children’s Policy Initiative, 200213 Oregon Addiction and Mental Health Division Databook, 2003

��
What SBHCs are doing to helpIn order for our SBHCs to better meet the mental health needs of children and adolescents effectively and appropriately, we need to more thoroughly under-stand the current SBHC mental health system. Therefore, the State SBHC Program Office is conducting a mental health needs assessment project. In conjunction with the needs assessment, the Program Office also developed an assessment tool capturing valuable information about mental health needs, service delivery, and barriers to providing care. The mental health assessment tool will provide specific data that will be used to provide technical assistance and training and provide information used to advocate for sustainable funding directed to-wards mental health services. During this process, the State Program Office maintains collaborations with other youth-serving mental health systems and continues to develop community partnerships to maximize local resources.
The State SBHC Program Office continues working to improve mental health services for Oregon’s children and adolescents. This year has been a year of growth for the SBHC mental health system across the state. The number of SBHCs with a mental health provider on site increased from 44 percent in 2004-2005 to about 55 percent in 2005-2006.
The top five mental health diagnoses were mood disorders, adjustment disorders, con-duct disorders, anxiety disorders, and alco-hol, tobacco and other drug disorders.14 Half of student visits for mental health conditions were seen by mental health providers and the primary care provider addressed most of the remaining mental health related visits. Among SBHCs that have a mental health pro-
vider, 25 percent of visits had a mental health component. When looking at all SBHCs, regardless of provider type, 12 percent of all SBHC visits had a mental health component, with girls making up 63 percent of these.
Where we need to goThe State SBHC Program Office is working to:
Analyze mental health needs assessment project data. This information will offer a comprehensive understanding of the complete mental health system in our SBHCs and therefore, allow the State Program Office to provide better guidance and technical assistance. Improve the quality of the mental health system in our SBHC communi-ties. The assessment tool will identify potential barriers to providing care. Once the barriers are recognized, we can work to develop plans to reduce barriers and improve mental health services and care. Continue to advocate for sustainable funding for mental health services for children.
14 Mental health data are not reported by eight SBHCs.
•
•
•
“I’ve
learned you can exercise while having
fun!”
–11-year-old female participant in SBHC-
led Nutrition and Physical Activity
Group
��
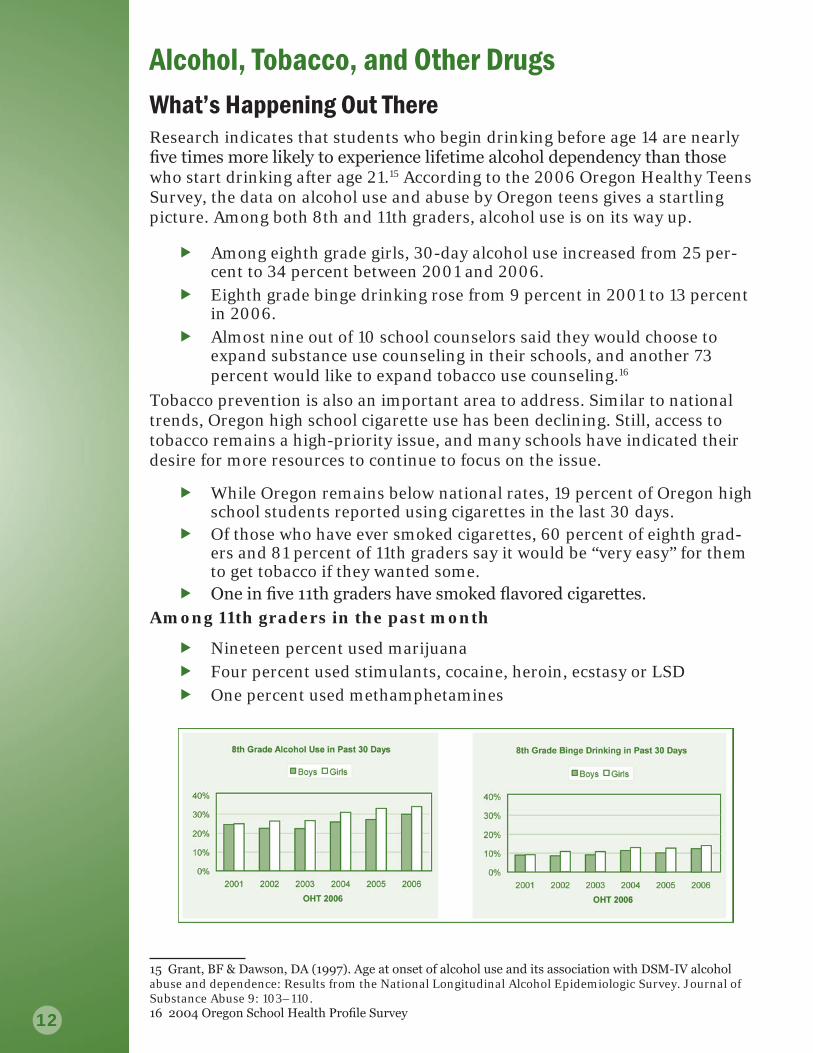
Alcohol, Tobacco, and Other DrugsWhat’s Happening Out ThereResearch indicates that students who begin drinking before age 14 are nearly five times more likely to experience lifetime alcohol dependency than those who start drinking after age 21.15 According to the 2006 Oregon Healthy Teens Survey, the data on alcohol use and abuse by Oregon teens gives a startling picture. Among both 8th and 11th graders, alcohol use is on its way up.
Among eighth grade girls, 30-day alcohol use increased from 25 per-cent to 34 percent between 2001 and 2006.Eighth grade binge drinking rose from 9 percent in 2001 to 13 percent in 2006.Almost nine out of 10 school counselors said they would choose to expand substance use counseling in their schools, and another 73 percent would like to expand tobacco use counseling.16
Tobacco prevention is also an important area to address. Similar to national trends, Oregon high school cigarette use has been declining. Still, access to tobacco remains a high-priority issue, and many schools have indicated their desire for more resources to continue to focus on the issue.
While Oregon remains below national rates, 19 percent of Oregon high school students reported using cigarettes in the last 30 days.Of those who have ever smoked cigarettes, 60 percent of eighth grad-ers and 81 percent of 11th graders say it would be “very easy” for them to get tobacco if they wanted some.One in five 11th graders have smoked flavored cigarettes.
Among 11th graders in the past month
Nineteen percent used marijuanaFour percent used stimulants, cocaine, heroin, ecstasy or LSDOne percent used methamphetamines
15 Grant, BF & Dawson, DA (199�). Age at onset of alcohol use and its association with DSM-IV alcohol abuse and dependence: Results from the National Longitudinal Alcohol Epidemiologic Survey. Journal of Substance Abuse 9: 103–110. 16 2004 Oregon School Health Profile Survey

��
What SBHCs are doing to helpSBHCs are actively screening for alcohol, tobacco and other drugs as part of their wellness and behavior risk assessment. If students are not using, they are provided prevention messages on the dangers of substance use. In fact, 32 percent of students reported receiving a prevention message about the dangers of drugs or alcohol; 28 percent about the dangers of tobacco.
If a student does show signs of using alcohol or other drugs, they are screened further to allow for proper referral to closely linked mental health services either on-site or to community providers. An actual diagnosis may be deferred until a qualified alcohol and drug counselor sees the student. Very few SBHCs have qualified alcohol and drug counselors on-site. Providers will continue to follow students by providing support, education, and prevention.
In 2005-2006, there were 733 visits occurring with an alcohol, tobacco or other drug diagnosis. Based on the anecdotal reports from SBHCs and the prevalence data previously discussed, it is unclear why the number of alcohol, tobacco and other drug related visits is low in SBHCs. Possible explanations include data tracking issues and the reality that providers are working with students very early in their use histories where a full substance use diagnosis may be premature and would cause long-term stigma. Clearly, more informa-tion is needed.
Where we need to goThe State SBHC Program Office is working with partners and local sites to:
Increase screening for alcohol, tobacco and other drugsPartner for referral sources either on-site or in the local communityImprove current data tracking systems to accommodate pre-diagnosis/early use and interventionAdvocate for fiscal policies that reimburse for early inter-vention of substance usePartner with local community for continued education and prevention, especially on underage drinking and tobacco use
••
•
•
•
“I’m chew-
ing tobacco and want to quit. My par-
ents told me to go cold turkey. I’m grateful for the help you gave me because I wouldn’t have been able
to do it without you!”
– Male SBHC student

��
Reproductive Health and Sexual Risk ReductionWhat’s Happening Out There
When SBHCs began twenty years ago, one of the main goals was to address teenage pregnancy. Happily, teen pregnancy rates in Oregon over the last several years continue to decline. Prevention and education are of high importance to SBHCs and their local communities in order to continue this trend. The release of the new HPV vac-cine (protecting against cervical cancer)
is evidence of continuing progress towards reducing health issues related to future sexual activity.
We want to continue to improve the sexual health of youth and recent data shows there is still room for improvement in prevention and education.
In 2006:
Fifteen percent of eighth graders and 41 percent of 11th graders reported hav-ing had sex at least once. Among 11th graders who have had sex, 85 percent used contraception the last time they had intercourse.
In Oregon, between 1999 and 2004:
Pregnancies for girls ages 10-17 decreased by 36 percent Teens between ages 15 and 19 were 32 percent less likely to become pregnant.17
While the rate of sexually transmitted infections (STIs) in Oregon is rising overall, the rate of teenage STIs is not seeing similar increases.
In 2005, Oregonians aged 15-19 made up:
Thirty percent of all chlamydia infectionsEighteen percent of all gonococcal infections Twenty-two percent of all reports of pelvic inflammatory disease (PID)
17 2004 Oregon Vital Statistics Report, Oregon Center for Health Statistics
��
These figures represent a substantial drop in rates in all three groups between 2001 and 2005.18 Regardless, the implications of these infections are severe. For example, chlamydia can create an infection that is asymptomatic, so patients often delay seeking treatment. The danger is that this allows the infection to progress and is one of leading causes of PID. Long-term consequences of PID include infertility, chronic pelvic pain, and future chance of ectopic pregnancies.19 Active screening for these and other STIs coupled with sexual risk reduction educa-tion is essential in keeping students healthy and safe.
What SBHCs are doing to helpSBHCs are required to provide developmentally appropriate reproductive health services to clients to ensure they maintain their reproductive health. These services include wellness exams (e.g. pelvic and testicular exams, pap smears), screening for sexually transmit-ted infections and pregnancy testing. SBHCs are encouraged to provide a wide range of services, but the decision on whether to offer family planning services on-site is a local-level decision. SBHCs that do not provide a full range of services are required to refer students to community providers.
In 2005-2006:
Twenty-three percent of all SBHC visits had a reproductive health component.Of clients ages 14-19, 82 percent of reproductive health-related visits were made by females and 18 percent by males.Abstinence counseling and safe sex prevention messages were the most frequently reported (56 percent) of all prevention messages.
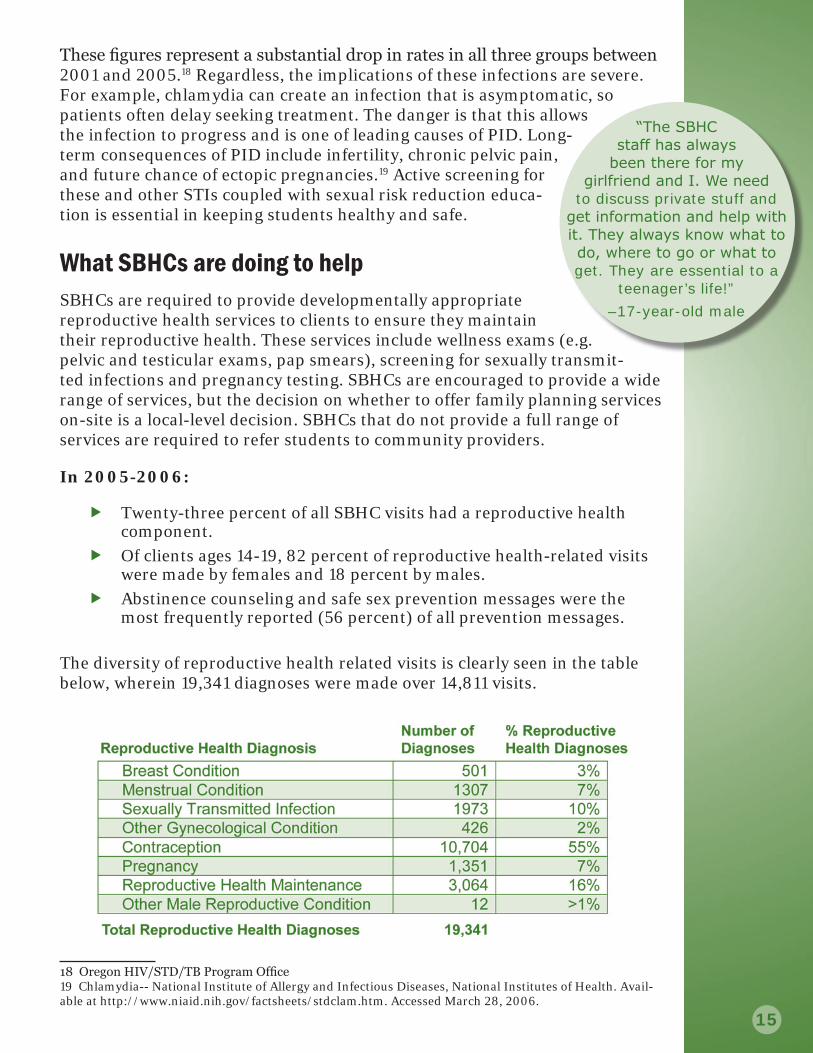
The diversity of reproductive health related visits is clearly seen in the table below, wherein 19,341 diagnoses were made over 14,811 visits.
1� Oregon HIV/STD/TB Program Office19 Chlamydia-- National Institute of Allergy and Infectious Diseases, National Institutes of Health. Avail-able at http://www.niaid.nih.gov/factsheets/stdclam.htm. Accessed March 28, 2006.
“The SBHC
staff has always been there for my
girlfriend and I. We need to discuss private stuff and
get information and help with it. They always know what to do, where to go or what to get. They are essential to a
teenager’s life!”
–17-year-old male

��
In their Words: What do Students Say? The annual Patient Satisfaction survey is an opportunity to hear the students’ voices on the health care they receive at the SBHC.
The results from the 2006 survey demonstrate how SBHCs have a positive impact on a student’s health:
Ninety-nine percent are comfortable receiving health care at the SBHC.Ninety-six percent find it easy to talk to SBHC staff.Ninety-four percent say they are likely to follow the advice given to them at the SBHC.Sixty-seven percent say their health has improved because of the SBHC.Eighty-five percent of students report-ed receiving at least one prevention message during their visit.
SBHCs see students who otherwise would not receive health care. On the 2006 Patient Satisfaction survey, 60 percent of students reported they were unlikely to receive care if there was not an SBHC at their school.
The goal of the annual Patient Satisfaction survey is to obtain a random sample of responses from 700 middle and high school clinic users. Thirty-six schools partici-pated and there was a 94 percent return rate.
The number of surveys to be completed at each SBHC was in
proportion to the percent-age of total patients
seen in the clinic during the previous school year. At the end of the multiple-choice survey, students had the opportunity to make comments and many of those quotes are used throughout this report.
“They are
so cool. They are very friendly and I like
them there. They are so awesome they just know everything you know and have good solutions for everything. Thank you health centers yeah!“
–14-year-old male

��
The SBHC model creates opportunities for health practitioners to discuss with students important prevention messages on topics ranging from the dangers of alcohol, tobacco and other drugs to the importance of eating healthy and getting exercise.
Eighty-five percent of SBHC students reported the discussion of at least one prevention message and 63 percent reported two or more prevention messages.
The most frequently reported prevention messages were mak-ing safe choices about sex (56 percent), importance of physical activity (40 percent) and feeling sad or angry (37 percent).
Students report they miss less class time when using an SBHC than if they had to access care elsewhere. It is also a likely conclusion that the presence of an SBHC helps parents miss less work since students do not have to be picked up and taken to another health care provider.
Seventy percent of students said they would miss more than one class for the care they needed that day if they had to access care elsewhere and 21 percent said they would miss the entire day.Fifty-six percent of students reported they were not missing even one class to receive health care in the SBHC that day.
“The health
center is one of the best things for
our school to have, it is confidential and it makes the kids feel safe and able to talk to someone who care. I don’t
know what I’d do if there was no health center.“
– 17-year-old female

��
CertificationOregon’s SBHC certification standards were developed through partnership with the Oregon School-Based Health Care Network, Conference of Local Health Officials, and the SBHC State Program. The goals of standardization were to increase emphasis on best practices, decrease site-to-site variability, increase ability to study clinical outcomes, and increase the potential for in-surance reimbursement. The standards are meant to represent reasonable, but high expectations. Included in the standards are guidelines for: facili-ties, operations/staffing, laboratory and clinical services, data collection and reporting, quality assurance activities and administrative proce-dures for certification.
A typical SBHC operation that offers core services is open at least three days per week during the school year and offers a total of 20 clinical hours per week of service. The average site offers 26 hours per week. Clinics are staffed by a primary care provider (i.e. nurse practitioner, physician assistant, or doctor), a registered nurse, and a health assistant. Qualified mental health professionals are also included if mental health services are being offered. The combination of these providers offer:
Performing routine physical exams, including sports physicalsDiagnosing and treating acute and chronic illnessPrescribing medicationsTreating minor injuriesProviding vision, dental, and blood pressure screeningsAdministering vaccinationsHealth education, counseling, and wellness promotionProviding or connecting students with mental health services
Giving classroom presentations on health and wellness
Certification is a voluntary process, but the State Program Office recognizes only sites that have become certified and as such their health department is eligible for funds. Certification occurs every two years at the end of legislative biennium. The next cycle will occur over the 2006-2007 school year.
For more information about the certification standards, please see: http://oregon.gov/DHS/ph/ah/sbhc/sbhc.shtml
••••••••
• “I think its
really good that the school has a health
center to go to at school because maybe without it a lot of kids wouldn’t be able
to get information that they do here.“
–16-year-old female

��
Funding and OperationsOregon’s School-Based Health Center program has benefited from 20 years of support by the Oregon Public Health Division and the Oregon Legislature. What began with an initial com-mitment of $212,000 to partially fund four SBHCs grew to a com-mitment of $3,100,000 to sup-port 47 SBHCs in the 2005-2007 biennium. Expansion dollars allocated by the Legislature for the 2005-2007 biennium led to the successful opening and certi-fication of three SBHCs in Coos, Deschutes and Jefferson counties. Currently, Marion and Wheeler counties are in the final phase of planning new SBHCs and will be certified by the end of the 2006-2007 school year.
A funding formula was revised in July 2005 to disperse state dollars to help SBHCs align with the public health delivery system. Each county that has a State certified SBHC is eligible for state dollars through their local public health authority (LPHA). The LPHA is provided funds to support their efforts based on the number of SBHCs in the county and the availability of legisla-tively approved dollars. For example, if there are one or two SBHCs the LPHA receives $50,000 a year, three to five SBHCs they receive $100,000 a year, six to nine SBHCs they receive $150,000, and over 10 centers they receive $200,000 a year. Each of these state dollars is used to leverage three to four local dollars. The funding formula requires an increasing local investment in the development of an SBHC system as the total number of centers increase. Local dollars may come through schools, school districts, county health departments, county government, hospitals, community providers, local businesses and individuals, grants, and general fundraising. Stable sources of ongoing revenue and operational funds remain a significant concern for most SBHCs as the average SBHC in Oregon costs an estimated $150,000-250,000 per year to operate.
“It’s sports physical season, and kids can go to the fast track clinic in town for $25 and get a physical exam that takes 5 minutes and clears them for sports. Or they can come see me, and get a 45-minute “physical plus”. For example, the student who just got cleared for wrestling by me, but also got an antibiotic for his asymptomatic ear infection, an application form for the low cost dental clinic, a referral to the local community health center for his medical home, and an ap-pointment to have his cholesterol checked (due to family history).”
–SBHC Staff

�0
PartnersCenters for Health and Health Care in Schools
Children First For Oregon
Community Health Centers
Department of Education
Public Health Division, DHS, Office of Family Health
Healthy Kids Learn Better Coalition
Local Health Departments
National Assembly on School-Based Health Care
Northwest Health Foundation
Oregon Addiction and Mental Health Division
Division of Medical Assistance Programs
Oregon Asthma Program
Oregon Medical Association
Oregon Nurses Association
Oregon Primary Care Association
Oregon Safety Net Advisory Council
Oregon Safety Net Policy Team
Oregon School Nurses Association
Oregon School-Based Health Care Network
State Agency Team for Youth Suicide Prevention
State and local Insurance Industries
“A 16-year-old boy without insurance and new to town came in for evaluation of painful bumps under his arm. He had been inadequately treated for a staph infection and the sores had returned and were increasing in number and size. Through the care at the school-based health center, he was treated for MRSA (resistant staph infection) and the health center’s medication funds paid for the antibiotics. Had he not received early attention for this condition, he would have likely been hospitalized or might have had to have surgical treatment for the infec-tion.”
–SBHC Staff

��
Contact informationState Program Office Staff
Robert Nystrom, BS, MA Adolescent Health Section Manager (971) 673-0252
Loretta Gallant, BA Research Analyst (971) 673-0252
Rosalyn Liu, BS, MPH Systems Development Specialist (971) 673-0252
Adriana Prata, MA, PhD Research Analyst (971) 673-0252
Additional InformationDepartment of Human Services Web site: http://www.oregon.gov/DHS/ph/ah/
Oregon School-Based Health Care Network Web site: www.osbhcn.org/
National Assembly on School-Based Health Care Web site: www.nasbhc.org/
Healthy Kids Learn Better Web site: www.hklb.org/
The Center for Health and Healthcare in Schools Web site: www.healthinschools.org/
AcknowledgementsThe SBHC State Program Office would like to extend its appreciation to all of the Oregon SBHCs and their staff who provided information used in prepara-tion of this report. Special thanks to Sarah Ramowski, Adolescent Health Policy and Assessment Specialist, for the amount of time, research, and dedi-cation she put forth during the development of this report. Design and layout of the report was done by Theresa Norman from the Web and Publication Design Team.
“A high school sophomore came to the health center to ‘talk’. After a few minutes of a superficial conversation, she revealed she had just taken an overdose of pills. The nurse intervened. Her parent was informed. The student was emotionally supported at school. She received medical care. The SBHC ar-ranged for follow-up coun-seling in the community. She is back in school and ‘hanging in there’ with sup-port. The SBHC is part of her school family, and are as committed as she is to her staying in school and graduating in two years.”
–SBHC staff

Upon request this publication can be furnished in an alternate format for individu-als with disabilities by contacting: Office of Family Health, Adolescent Health Section at (971) 673-0252. Available formats are: large print, Braille, audio tape recording, electronic format and oral presentation.