Embed Size (px)
Citation preview

1
Screening for impaired visual acuity and vision-related
functional limitations in adults 65 years and older in primary
health care: Systematic review
November 2017
University of Alberta Evidence Review Synthesis Centre
ERSC Project Lead Investigator: Lisa Hartling
ERSC Project Staff: Jennifer Pillay, Tara MacGregor, Robin Featherstone (Research
librarian), Ben Vandermeer (Statistician)
ERSC Experts: Ellen Freeman PhD, and William Hodge MD, PhD, FRCSC
Suggested citation: Pillay J, Freeman EE, Hodge W, MacGregor T, Featherstone R, Vandermeer
B, and Hartling L. Screening for impaired visual acuity and vision-related functional limitations
in adults 65 years and older in primary health care: systematic review. Edmonton, AB; Evidence
Review Synthesis Centre. Available at: http://canadiantaskforce.ca/ctfphc-guidelines/overview/
Author contributions:
JP, LH, EF, WH, RF, and BV contributed to protocol development. RF designed and
implemented the database search strategy and conducted grey literature searches. TM led the
screening and quality assessments and contributed to data extraction and GRADE assessments.
JP contributed to study selection, quality assessments, and GRADE assessments, and verified all
data extraction. EF, WH, LH and BV provided methodological expertise for data analysis and
interpretation of findings. JP, EF, and LH contributed to discussions with the CTFPHC and
PHAC who provided feedback on the draft report and interpretations of the findings. JP and TM
drafted and EF, WH, RF, BV, and LH critically reviewed the report.
Acknowledgements:
We would like to acknowledge Kassi Shave and Annabritt Chisholm from the Edmonton ERSC
who assisted with screening and selection of studies. We also thank Tara Landry, MLIS, for peer
reviewing the search strategy.
Members of the Canadian Task Force on Preventive Health Care (CTFPHC) and staff within the
Global Health & Guidance Division (GHGD) of PHAC participated in development of the

2
protocol and approved the final report. The ERSC is responsible for study selection, data
collection, analysis and preparation of the manuscript of the review while the CTFPHC and
GHGD provided input into the interpretations of the findings. The ERSC takes final
responsibility for the content of the review.
CTFPHC Working Group: Brenda Wilson (Chair), and the following members: Brett
Thombs, James Dickinson, Scott Klarenbach, Maria Bacchus
PHAC GHGD Staff: Susan Courage, Alejandra Jaramillo Garcia, Nicki Sims-Jones
The following individuals represent content experts and stakeholders that reviewed a draft
version of this report during March 2017. The ERSC considered all input when finalizing the
report and responses to comments were sent to all reviewers. The conclusions and synthesis of
the scientific literature presented in this report does not necessarily represent the views of
individual reviewers.
Mathieu Carignan
Canadian Occupational Therapy Low Vision Rehabilitation Network
Walter T. Delpero, MD, FRCSC
Assistant Professor
Department of Ophthalmology
University of Ottawa
Natasha Kuran
Manager, Senior Policy Unit
Public Health Agency of Canada
Matthieu Lafontaine-Godbout, MD
Assistant Professor at the Faculty of Medicine and Health Sciences
University of Sherbrooke
Susan J. Leat, PhD, FCOptom, FAAO
Professor, School of Optometry and Vision Science,
University of Waterloo
Professor Stephen Lord
Senior Principal Research Fellow
Falls, Balance and Injury Research Centre
Neuroscience Research Australia
Karen McCormac, BN
Canadian Nurses Association
Director, Quality and Patient Safety
Misericordia Health Centre

3
Linda S. Petty, BSc(OT), OT Reg (Ont)
Assistive Technology Consultant
Accessibility Services, University of Toronto Scarborough
Dr. Gilles Plourde
Senior Clinical Evaluator, Health Canada
Dallas Seitz, MD, FRCPC
Assistant Professor
Queen's University
Kimberley Simmonds, BSc, MMSc, PhD
Alberta Health
Enitan Sogbesan
Assistant Professor, Ophthalmology – Glaucoma
McMaster University
Benoît Tousignant OD, MSc, MPH, FAAO
Assistant Professor, School of Optometry
University of Montréal
Declaration of funding
The Evidence Review and Synthesis Centre conducted this review for the Public Health Agency
of Canada [PHAC], however, it does not necessarily represent the views of the Government of
Canada.
4
Summary Background: In developed countries, impaired visual acuity typically affects about 10% of people aged
65 to 75 and 20% over 75. Although uncorrected refractive error is the most frequent cause of impaired
visual acuity throughout adult life, other conditions such as cataract, macular degeneration, diabetic
retinopathy, and glaucoma also become frequent causes in older ages. This review focuses on screening
by primary care professionals (but not eye care professionals) for visual acuity or vision-related functional
limitations in order to help identify refractive errors, cataracts, and macular degeneration; glaucoma
assessment requires equipment (e.g., for visual field testing and viewing the optic nerve) and expertise
only infrequently available in a primary care setting, and testing for diabetic retinopathy is considered
case finding (rather than screening) by specialist practitioners within a group of people with a high risk of
acquiring the condition. While treatment for refractive errors and cataracts is effective without great
concern about major harms, 11% to 51% of older people appear to have unrecognized, correctable
impaired visual acuity (<20/40) and may benefit from screening in primary care in order to coordinate
care with eye professionals or other services and programs.
Purpose: This review was produced for the Canadian Task Force on Preventive Health Care (CTFPHC)
to help inform their recommendations on screening for impaired visual acuity or vision-related functional
limitations in older (≥65 years), community-dwelling adults in primary health care settings.
Review Approach: Following CTFPHC methods, a staged approach was used, applying Grading of
Recommendations Assessment, Development and Evaluation (GRADE) methods. The quality of the
evidence was determined for outcomes rated by the CTFPHC, using input from consultations with older
adult Canadians, as important or critical for decision making: benefits included reduced mortality,
fractures, loss of independence, vision-related functional limitations/quality of life, impaired visual
acuity; harms included serious or major adverse effects from treatment, and anxiety/burden from
diagnosis if limited or inaccessible treatment options for the condition. Evidence was first sought on the
clinical effectiveness of screening in primary health care; these studies would compare outcomes over
time between a control group of no screening/usual care, and an intervention group for which there is an
intent to screen all people and, if indicated, encourage them through referrals or otherwise to seek further
assessment by eye professionals and possibly treatment or other services to improve their vision and/or
other patient-important outcomes related to vision. A hierarchy of evidence was used with randomized
controlled trials (RCTs) reviewed first if available. If screening was found to have a favorable benefit-
harm ratio from a body of high-quality evidence, we would have examined its cost-effectiveness; we
would have examined patient valuation of benefits and harms if the evidence on clinical effectiveness left
considerable uncertainty about the balance of benefits and harms. Additionally, if insufficient (e.g., very
low-quality) evidence on clinical effectiveness existed, we would have sought evidence on screening test
accuracy to provide indirect evidence about screening programs. The body of evidence from RCTs on the
clinical effectiveness of screening older adults in primary health care settings is reported in this report; no
other systematically reviewed evidence is determined necessary at this time for the CTFPHC to make a
recommendation.
Data Sources and Study Selection: Four high-quality systematic reviews on vision screening, home
visits, and preventive health care were identified, and we largely relied upon these for identifying studies
reported before 2012. To update the evidence, we searched MEDLINE; Embase; Cochrane Library;
CINAHL; and PubMed to October 2017 using terms highly sensitive for screening for vision, alone or
within multicomponent assessments. Supplementary searches for grey literature were conducted (internet-
based searches, electronic libraries, trial registries, and references supplied by stakeholders), and
reference lists of other systematic reviews (n=25) and included studies were reviewed. Two reviewers
independently screened titles and abstracts of citations. Full texts of studies that were classified as
“include/unsure” by either reviewer were retrieved and screened independently by two reviewers using a
standard form with explicit inclusion and exclusion criteria. Disagreements were resolved through
consensus or consultation with a third reviewer. The flow of literature and reasons for exclusion after full-
5
text review are documented. Authors of papers, where vision screening was not explicitly stated (but
indicated in some manner) or outcomes were not reported, were contacted to obtain information and data
on our outcomes of interest.
Data Extraction, Analysis, and Interpretation: One reviewer independently extracted data, and another
reviewer verified all data from each included study. Two reviewers independently assessed the risk of
bias of each included study. We performed random-effects meta-analyses where appropriate, and
performed sensitivity and subgroup analysis based on a priori variables for patient and intervention
characteristics. Data on within-study analysis on our subgroups of interest were also collected. For
calculating the absolute effects for dichotomous outcomes, we used the relative risk and the median
baseline risk for the control group in the included trials. We examined funnel plots and conducted Egger’s
test to detect small-study bias when there were at least eight studies in a meta-analysis. When data could
not be pooled, we provide a narrative summary of findings. Two reviewers independently assessed the
quality of the body of evidence using the GRADE methodology, with consensus based on discussion and
third-reviewer input. The evidence is summarized in GRADE Evidence Profiles and Summary of
Findings tables. We chose to use standard wording to communicate our interpretations of the quality of
evidence, which reflects the degree of certainty we have in the effects. For findings supported by high,
moderate, low, and very low quality evidence we use “will”, “probably/likely”, “may/appears to”, and
“not known/very uncertain”, respectively, in our textual descriptions of the results.
Results: Our database searches from 2012 to October 2017 identified 14,995 citations after duplicates
were removed; an additional 146 records were eligible for full text review from other searches. After all
full text review (n=452) including author contacts when information was needed for determining
eligibility, we included 15 RCTs reporting on 17,400 participants. Trials were conducted in a variety of
settings although mostly in physician offices or participants’ homes. None of the trials exclusively
enrolled participants not having regular eye care providers. Only two of the 15 RCTs had an isolated
vision screening intervention, whereas all others incorporated vision screening within a multicomponent
assessment of health and functioning. Screening involved the use of questions on one or more presenting
vision problems in 10 trials and objective tests measuring presenting visual acuity with or without other
visual function testing in the other five. The number of healthcare interactions after screening ranged
between 1 and 12. Follow-up ranged from 2.5 to 47 months (mean 18.6 months); studies with longer
follow-up usually had more interactions. Only four trials reported specific screening criteria/thresholds
for referring participants to eye professionals. Most only provided referrals or follow-up when
participants reported that they did not have a regular eye care provider. For subjective outcomes from 11
RCTs, the overall risk of bias was considered high mostly due to lack of blinding of participants (n=8) or
outcome assessors (n=11). Four of five RCTs reporting on objective outcomes were at unclear risk of
bias; one had high risk of bias due to incomplete outcome data (>30% attrition of those alive at follow up
and/or large differential between groups). As would be expected for trials in this age group, attrition was
moderately high in several studies.
Benefits and Harms. Because the outcomes of mortality, fractures, and loss of independence could not
usually be attributed to the vision component of the multicomponent interventions, the trials provided no
or scarce evidence for these outcomes. Two trials (n=1,180) reported on a surrogate outcome for fractures
(falls and falls requiring medical treatment) that were attributed to vision screening (i.e., via isolated
vision intervention or other attribution by study authors) over follow-up durations of 12 to 18 months.
The quality of evidence for fractures was assessed by GRADE methods as very low, and therefore we are
very uncertain about the effects of screening with multiple vision tests on fractures over medium-term
follow-up. Low-quality evidence from one RCT (n=1,807; median 3.9 years follow up) showed that
screening with objective tools (logMAR chart with pinhole correction) of visual acuity may make little or
no difference in vision-related functioning over long-term follow-up (NEI-VFQ-25, range 0-100;
minimally important difference 4-6 points; mean difference, 0.4 units higher for screening; 95% CI, -1.25
to 2.05 units). Screening with multiple objective vision tests probably makes little to no difference in
high-contrast, distance visual acuity for older adults over medium-term follow-up (minimally important

6
difference 0.1 logMAR; 4 RCTs; n=1,236; mean difference, -0.01 logMAR; 95% CI, -0.05 to 0.03).
Quality assessment (1 RCT; n=519) found that screening with multiple objective vision tests may reduce
worsening (RR 0.55, 95% CI 0.39 to 0.78; absolute effect, 126 fewer per 1000; 95% CI, 62 to 171 fewer)
and/or improve (RR, 1.82; 95% CI, 1.08 to 3.08; absolute effect, 73 more per 1000; 95% CI, 7 more to
185 more) high-contrast, distance visual acuity by at least 0.1 logMAR (minimally important difference)
for a proportion of older adults over medium-term follow up. We are very uncertain about the effects of
screening using tests of visual acuity on the proportion of people no longer having impaired visual acuity
(worse than 20/60) in both eyes or in either eye over long-term follow-up (1 RCT; n=1,807). Screening
with objective tools may make little to no difference in the proportion of people having bilateral impaired
visual acuity worse than 20/40 over medium-to-long term follow-up (2 RCTs; n=1,967; RR, 0.82; 95%
CI, 0.66 to 1.02; absolute effects, 67 fewer per 1,000; 95% CI, 7 more to 127 fewer). It may make little to
no difference in the proportion having impaired visual acuity worse than 20/40 in either eye over long-
term follow up (1 RCT; n=1,807; RR, 0.98; 95% CI, 0.82 to 1.17; absolute effect, 15 less per 1000; 95%
CI, 108 less to 102 more). Ten RCTs reported on the outcome of self-reported vision problems using non-
validated questions. Moderate quality evidence from 10 RCTs (n=8,683) comparing screening using self-
reported vision with no screening or usual care found no significant difference for self-reported vision
problems (RR, 0.97; 95% CI, 0.90 to 1.05; absolute effect, 9 fewer per 1,000; 95% CI, 16 more to 31
fewer) over a median follow-up period of 20 months. Most of our planned subgroup analyses—follow-up
duration, screening personnel, setting, and type of screening tool—did not appear to explain the
heterogeneity in the effects for this outcome. One subgroup analysis with some credibility compared
studies of relatively younger patients (mean age <75 years) who were completely independent in
activities of daily living (ADLs) (3 RCTs; n=5,269) with those of older patients (e.g., 75 and older) with
some reliance on others for ADLs (7 RCTs; n=3,414) (self-reported vision problems: RR, 0.85; 95% CI,
0.76 to 0.96 vs. RR, 1.03; 95% CI, 0.96 to 1.11, respectively; p=0.008 between groups; I2=0% for each).
No trial reported on any of harm of interest.
Implementation Factors. From data of seven RCTs, about a third (median 35%) of patients screening
positive for vision problems were referred to eye professionals, although the range of 29 to 95% was
large. In total for these seven trials, there were 574 referrals provided to 3,225 screened patients (18% of
those screened). Reasons for not referring provided by several trial authors were mostly related to patients
reporting care by eye professionals. The uptake of referrals (5 RCTs reporting) was moderate (median
68%; range 18-96%). One additional trial reported similar compliance (68%) to any of multiple
recommendations (visit eye professional, wear hat/sunglasses in high-glare situations, turn light on at
night). Over the five trials reporting on referral uptake (n = 3,063 screened), 231 patients (7.5%) likely
received further assessment for their vision via referrals. This number may not represent those getting
treatment; for example, in one RCT, 26 of 101 complying with referrals (5% of screened population)
received treatment (20 new glasses and 6 surgeries). In another, only 2% of screened patients received
new glasses or cataract surgery.
Limitations: There should be some consideration that the trials did not focus only on patients with
unrecognized vision problems (e.g., many reported current care by an eye professional), and that the
absolute effects may have been different if the study investigators had excluded these patients, thus
changing the baseline rates of impaired vision. The results, though, may best represent a typical primary
care setting where a vision screen may be given to all patients. Further, in 10 of the trials the control
group patients had some form of vision assessment (for outcome comparison), and in at least one trial
some patients received referrals to eye professionals; results across many outcomes may underestimate
what may occur should a practitioner newly initiate screening and referrals into practice. Although several
trials included assessment of factors that could theoretically affect vision if treated (e.g., medication
review, nutrition assessment) we are making the assumption that the vision screening and subsequent care
by eye professionals, would have been the largest contributor to any beneficial effect on vision. Although
we report on differential effects for an a priori-defined subgroup for the outcome of self-reported vision
problems, between-study analyses based on study-level patient variables are observational in nature with
the potential for an ecological fallacy and confounding by other between-study differences. The

7
credibility of this subgroup effect is not considered high, and the magnitude of the difference between
sub-groups is considered low quality evidence. Further research is warranted to determine if these effects
are valid.
Conclusions: Evidence was either not found or of low quality for most outcomes considered most critical
for decision making by the CTFPHC for screening for impaired visual acuity or vision-related functional
limitations for older, community-dwelling adults in primary health care settings. No evidence was found
for mortality, loss of independence, or critical harms; the quality of evidence available for the outcome of
fractures was very low such that we cannot make any conclusions on the effects. Screening probably
makes little to no difference for mean visual acuity over medium-term follow-up across populations of
older adults. It may also make little or no difference for vision-related functional limitations and we have
no certainty about effects on the number of patients with impaired visual acuity meeting clinically
relevant thresholds (e.g. worse than 20/60). Low quality evidence suggested that there may be some
benefit in the numbers of patients having their vision worsen or improve by a marginal degree (0.1
logMAR=5 letters). For an added outcome of self-reported vision problems, screening probably makes
little to no difference; studies where the average patient age was relatively younger (< 75 years) and all
patients were independent in ADLs at baseline showed a greater effect for this outcome than those of
older patients with at least some requiring assistance with ADLs, although other confounding factors may
exist between these groups of studies and the findings are considered exploratory and in need of more
research. The results of largely no effect across outcomes could relate in part to a fairly low referral rate
by clinicians for those patients screening positive (due to reports of regular eye professional care),
moderate uptake of referrals by patients, and low numbers of patients receiving treatments. Findings are
most applicable to screening all older adults in primary care, and not for those seeking and receiving care
by eye professionals or other providers working in visual rehabilitation settings where comprehensive
assessments and treatment/services would be directly provided.
PROSPERO Registration #: CRD42016053088
8
Section I. Purpose and Background
The purpose of this review was to examine the evidence on vision screening of community-
dwelling older adults (ages ≥65 and not under the care of an eye professional) within primary
health care. The findings will be used by the Canadian Task Force on Preventive Health Care
(CTFPHC)―supplemented by consultations with patients and stakeholder on issues of
feasibility, acceptability, costs/resources, and equity―to inform recommendations to support
primary care providers in delivering preventive health care.
Background
The prevalence of impaired visual acuity and vision-related functional limitations in the world is
high. In World Health Survey data from 70 countries (not including Canada), 21% of adults
overall reported difficulty in “recognizing a person you know across the road”; this proportion
varied by country income status with high-income countries having a prevalence of 13%.1 In
2007, the total financial cost of vision loss in Canada was estimated at $15.8 billion, and its
prevalence was projected to double by the year 2032 due to changing population demographics.2
Prevalence of impaired visual acuity increases with age. Impaired visual acuity and other
problems within the visual system negatively impact vision-related functioning, quality of life
(QoL), and likely mental health;3,4
in older adults this manifests through various effects such as
decreased participation in social and leisure activities, difficulty in family relationships, and
injuries from accidents including falls.5-15
They also affect instrumental activities of daily living
(IADLs), or ability to work, drive safely, or maintain a driver’s license, therefore limiting
independence.
Terms, Definitions, and Scope of Screening in Primary Care
Visual acuity refers to the sharpness or clarity of vision. Impairment in visual acuity may be
caused by problems with the sharpness of the image reaching the retina (e.g. refractive error,
media opacities such as cataract), by retinal disease, or by the central processing or interpretation
of visual neural signals. The World Health Organization (WHO)16
uses presenting distance
visual acuity to classify individuals into categories of mild or none [≥20/60], moderate [<20/60
to ≥20/200], severe [<20/200 to ≥20/400] visual impairment, with blindness defined as a visual
acuity worse than 20/400; the term low vision (replaced by moderate and severe impairment) is
not used within the WHO classification any longer, to avoid confusion with the need for low

9
vision care which often occurs at a less severe threshold of visual acuity and is often not specific
to visual acuity.17,18
The WHO classification is not always used, particularly in studies from
North America which define visual impairment at worse than 20/40, when some form of vision-
related functional limitation often begins, and legal blindness at 20/200 or worse.19-22
Depending
on the jurisdiction, in Canada poorer than 20/40 or 20/50 serves as the acuity required for an
unrestricted driving license.
Although visual impairment is typically defined by degree of impaired visual acuity, this term
may also be used to refer to other problems with visual function (e.g., visual field loss―areas in
the field of view/peripheral vision in which objects cannot be seen, lowlight vision, colour
vision, contrast sensitivity, binocularity).18
Likewise, findings related to visual acuity (e.g.,
severe inability to see, blindness) may be interpreted in terms of vision disability23
which more
often refers to activity or functional limitations resulting from one or more problems in the visual
system. For this review, we will use the term impaired visual acuity when referring to loss of
visual function measured in terms of visual acuity and meeting WHO or North American
thresholds (<20/60 or <20/40); we will use vision-related functional limitations when referring to
functional deficits such as inability to drive or perform IADLs (e.g., handle finances, take
medication) directly resulting from impaired visual acuity and/or other functional or structural
problems within the visual system. Other outcomes, to which vision loss may contribute, are
defined as potential adverse consequences of vision loss, such as falls, fractures, depression,
cognitive decline, loss of independence.
These terms (impaired visual acuity, vision-related functional limitations, potential
consequences of vision loss) align with a focus on screening tests used most often within primary
care, including visual acuity charts and structured screening questions or tasks focusing on
vision-related function (e.g., problems with reading, driving); they also align with the outcomes
chosen for this review. When tests or outcomes (e.g., contrast sensitivity) are used that do not fall
into these categories we will use the terminology reported by the authors.
The CTFPHC uses the Institute of Medicine’s definition of primary care as, “the provision
of integrated, accessible health care services by clinicians who are accountable for addressing a
large majority of personal health care needs, developing a sustained partnership with patients,
10
and practicing in the context of family and community.”24
The main clinicians involved are
individuals who use a recognized scientific knowledge base and have the authority to direct the
delivery of personal health services to patients. The CTFPHC’s main audience is primary care
physicians and nurses, although the Task Force recognizes the importance and relevancy of their
recommendations to community and public health professionals (public health nurses,
nutritionists), physician specialists, other health care and allied health professionals. This view
also aligns with Health Canada’s functional definition of primary health care: (i) to direct
provision of first-contact services (by providers such as family physicians, nurse practitioners,
pharmacists, and telephone advice lines); (ii) to coordinate care to ensure continuity and ease of
movement across the system, so that care remains integrated when Canadians require more
specialized services (with specialists or in hospitals, for example); and to include other care
models such as community health centres, public health nurses, well baby clinics, and the
inclusion of non-medical health care providers with a focus on health promotion.25,26
For this guideline, we acknowledge that optometrists regularly provide first-contact services and
are considered primary health care practitioners of the eye and visual system, but they are
considered to be outside the scope of this review which is focusing on whether practitioners
without considerable eye training or specialized equipment should routinely conduct limited
screening for potential vision problems. Rather, we are considering that assessment by an
optometrist could be advised or arranged by other primary health care providers should screening
indicate the need for further testing and/or treatment. For clarity, throughout this document we
use the term primary care consistent with the Institute of Medicine’s definition with focus on
professionals covering a wide range of personal health care needs. We use the term eye
professional to indicate optometrists or ophthalmologists.
Prevalence and Incidence of Impaired Visual Acuity in an Aging Population
Several studies in Canada and other developed countries have documented the prevalence of
impaired visual acuity in older populations. In 2006, 13.4% of Canadians aged 75 years and
older reported having a “seeing limitation”; more older (aged 75 and older) than young people
(aged 15 to 24) with limitations said they were severe (30.5% vs. 16.7%).27,28
A more recent
study found prevalences of habitual/presenting (with current spectacles) impaired visual acuity
(<20/40) of 3.9% (95% confidence interval [CI], 1.9 to 8.1; 60-69 years) and 7.5% (95% CI, 3.1
to 16.9; >80 years) and an overall reduced visual acuity (<20/25) prevalence of 15.2% (95% CI

11
12.8 to 18.0); an odds ratio (OR) of 3.56 (95% CI, 1.22 to 10.35) was found for impaired
distance visual acuity in older (≥65 years) versus younger (39 to 64 years) people.21
Apart from
increasing age, the only demographic variable significantly associated with distance and near
visual acuity in this study was increased time since last eye examination. In general, reports from
developed countries including the United States (U.S.) and United Kingdom (U.K.) suggest that
impaired visual acuity typically affects about 10% of people aged 65 to 75 and 20% over 75.29-32
Large studies the U.S., Australia, and Europe have found the prevalence of impaired visual
acuity to increase dramatically (up to three-fold) over the age of 60;33-35
one in the U.S. found
that 75 year olds were 12.8 times more likely (95% CI, 9.6 to 17.1) to develop impaired visual
acuity over 15 years than those younger than 75 years.36
Residents of nursing homes are reported
to have at least three times higher levels of impaired visual acuity than community-dwelling
older adults of similar ages.37-39
Etiology and Treatment for Conditions Causing Visual Impairment
Although uncorrected refractive error is the most frequent cause of impaired visual acuity,21,40,41
cataract, macular degeneration, diabetic retinopathy, and glaucoma are the next most frequent
causes and predominate as causes of visual impairment in older ages.40
For example, a large
study in the U.S. found that, until age 60, impaired visual acuity was due to uncorrected
refractive errors in 85–90% of individuals while, after age 60, at least 40% of impairment was
caused by ocular disease.41
Glaucoma can cause vision loss (mainly from visual field loss) and
diabetic retinopathy can cause impaired visual acuity, but screening for these conditions is not
the focus of this review on screening in primary care settings. Glaucoma screening requires
equipment (e.g., for visual field testing and viewing the optic nerve) and expertise only
infrequently available in a primary care setting, and testing for diabetic retinopathy is considered
case finding (rather than screening) by specialist practitioners within a group of people with a
high risk of acquiring the condition.
Refractive Errors. Refractive errors comprise myopia (nearsightedness), hyperopia
(farsightedness), astigmatism (difference in refractive error between two meridia), and
presbyopia. They occur when the eye is unable to focus light on the fovea. Presbyopia, which
occurs due to the eye’s natural aging (e.g., loss of flexibility in the lens at about age 45), is the
loss of the eye’s ability to change its focus to see near objects. Impaired visual acuity may exist
with or without refractive correction; for the purposes of this report we focus on presenting, or
habitual, visual acuity and not best-corrected. Refractive errors can be treated with spectacles,

12
contact lenses, or reading glasses. Refractive errors may also be corrected with refractive surgery
(e.g. laser in situ keratomileusis [LASIK] or epithelial keratomileusis [LASEK]), although this
option is more often selected in younger adults.42
Rates of complications are generally low; a
review found corneal ectasia rates ranging from 0 to 0.87% for LASIK and keratitis rates from 0
to 3.4% for LASIK and LASEK.43
Improvement in vision-related QoL of older persons has been
demonstrated when uncorrected refractive error is corrected.44,45
Both refractive lenses and
surgery are considered effective for correcting refractive errors and improving vision-related
function in older adults with little harm.43
For some, though, impaired visual acuity may be too
severe for adequate correction.
Age-Related Macular Degeneration (AMD). Age-related macular degeneration (AMD) is the
most common cause of legal blindness in individuals over the age of 65 in North America.40
It
has been estimated that AMD causes about 50% of all cases of blindness in old age in developed
countries.46
AMD affects the central part of the retina—the macula, leading to progressive loss of
central vision (i.e., blurring vision) and, if severe, to scotomas (complete loss of central vision).
Macular degeneration can be “dry” (deterioration and loss of photoreceptors without new blood
vessel formation) or “wet” (presence of blood vessels that leak); wet AMD is less common but
results in faster vision loss. Antioxidants and zinc are effective for managing dry AMD; they
have been shown (10-year follow-up of the Age Related Eye Disease Studies [AREDS]) to
reduce conversion of dry to wet AMD (OR, 0.66; 95% CI, 0.53 to 0.83) and moderate vision loss
(OR, 0.71; 95% CI, 0.57 to 0.88),47,48
without association with increased risk of most adverse
events.43
Treatments available for wet AMD include thermal laser, photodynamic therapy, and
antiangiogenic (anti-VEGF) drugs administered into the vitreous cavity.49
Today anti-VEGF
therapy dominates treatment for wet AMD. Studies between VEGF inhibitors and sham have
reported no significant differences in incidence of serious ocular harms, including ocular
hemorrhage, retinal detachment, or endophthalmitis, although results across studies were found
to be imprecise in one review because of low event rates.43
There is some high quality evidence
that some anti-VEGF agents injected into the vitreous may increase systemic vaso-occlusive
events though the number needed to harm is very high. Tobacco smoking is the principal
modifiable risk factor for development and progression of AMD,50-53
such that smoking
cessation interventions are speculated, but not proven, to offer considerable benefit. Another
modifiable risk factor is sun exposure (≥ 8 hours daily) during working years.54
For both dry and
wet AMD, aims are early identification and prevention of progression and permanent vision loss;

13
rehabilitation strategies are also available to reduce associated harms (see Additional Therapy
and Services below).
Cataracts. Cataract occurs when denaturation of lens proteins in aging eyes cause the normally
transparent lens to opacify, leading to blurring of vision, increased sensitivity to glare, and loss
of contrast sensitivity. Cataracts represent the second most common cause of correctable
impaired visual acuity after the correction of refractive error.34,55
Worldwide, cataracts are the
most common cause of blindness. Advancing age remains the most common risk factor, with
progression typically extending over a long period of time. Other common risk factors include
diabetes mellitus, smoking, alcohol, history of ocular trauma, ultraviolet light, and previous
intraocular inflammation or surgery (e.g., for glaucoma).56,57
The most common treatment is
surgical cataract extraction and intraocular lens implantation. Phacoemulsification, involving
ultrasound energy with small corneal incisions and soft artificial lens insertion, is the most
commonly used method for removing the lens in developed countries.58,59
Based on a large
number of observational studies and widespread clinical consensus, cataract surgery is believed
to be highly effective in improving visual acuity with a low complication rate (e.g., 0.13 percent
endophthalmitis), in patients with mild to advanced cataracts.43
Cataract surgery is the most
common surgical procedure performed in health services in high income countries, leading to
great public health implications.
Additional Therapy and Services
Vision Rehabilitation Therapy and Treatment. When other treatments do not adequately correct
impaired visual acuity or improve vision-related function, are contraindicated or otherwise not
used, vision rehabilitation therapy and treatment should be considered.17,60
This can include
training (e.g., eccentric viewing in AMD) and/or devices to improve vision-related tasks such as
reading and mobility. Home modifications may be undertaken to improve visibility using
contrast and lighting modifications. Optical devices are also often used, including optical
magnifiers and video magnifiers. These services can include multidisciplinary assessment and
training by optometrists, ophthalmologists, and others including social workers, occupational
therapists, and orientation and mobility professionals; multidisciplinary clinics are located in
some Canadian provinces including Ontario (n=10), Quebec (n=14), Alberta (n=2), and
Manitoba (n=2), but in others, optometrists work independently to provide assessment and
devices, with referral to the Canadian National Institute for the Blind (CNIB) for other aspects of
rehabilitation.17
There is also heterogeneity in the availability and extent of government funding

14
for these services. A model has been proposed recently for integrated low-vision rehabilitation
services in Canada.17
Organizations Serving People with Impaired Visual Function and Blindness. In Canada, the
largest agency serving people with impaired visual acuity and blindness is CNIB which has nine
geographic service divisions and over 60 regional offices; there is also a CNIB Library for the
Blind which serves all areas of Canada. CNIB operates a variety of rehabilitative, low-vision and
social service programs, as well as prevention of blindness and public education programs.
Several other organizations exist within the country to provide services, with a few examples
being the Canadian Council of the Blind (an organization of consumers), the Institut Nazareth et
Louis-Braille (the largest provider in Quebec), and MAB-Mackay.
Social Programs. Other supports exist for people with severe vision loss that meets certain
criteria. According to the Canadian Ophthalmologic Society40
“identification can lead to access
to financial resources, through disability pensions or social programs geared to the visually
impaired, that may enhance quality of life despite poor visual status.” Although the national
disability pension benefit program (Canadian Pension Plan Disability Benefits) is only offered to
those under 65, disability tax credits and savings plans are available and provincial social
assistance and support programs exist (e.g., Alberta’s Cross Disability Support Services and
Adult Health Benefit Program, British Columbia’s Disability Assistance Program, the Ontario
Disability Support Program, PEI’s Disability Support Program). In view of the possible impact
of vision-related functional impairment on social roles and relationships, some Canadian experts
have called for the creation of more community and other targeted interventions for allowing
people to maintain active social participation.14
Screening Tests in Primary Care
Screening for impaired visual acuity or vision-related functional limitations in primary care does
not imply replication of the comprehensive eye examinations used in offices of eye
professionals. Although eye professional organizations consider a comprehensive eye
examination a form of screening (in terms of primary prevention in asymptomatic people),40
such
an examination within this review would be considered diagnostic in nature and would not be
feasibly conducted in primary care. The intent of screening in primary care would be to use one
or more simple tests (with sufficient accuracy) to attempt to identify individuals with impaired
visual acuity or other problems causing functional limitations, but who have not sought eye
assessments or care themselves, for referral to, or care coordination with, eye or other

15
professionals. Screening tests that would likely be feasible for application by a primary care
provider without specialized equipment or extra training can be categorized into three groups:
direct tests of near or far visual function (e.g., acuity tests with reading or describing text or
symbols on charts or pages), direct clinical examination of the eye and its structures (e.g.,
fundoscopy), and structured enquiry about visual acuity or vision-related functional
limitations/problems. Screening tests may be used alone, or in combination with other tests
evaluated within multicomponent assessment strategies (e.g., comprehensive geriatric
assessments). As such, screening may be situated within prevention programs or interventions.
Eye Function Screening Tests. Most tests of eye function used in primary care practice will
focus on testing visual acuity. The Snellen chart (widely used in primary care) assesses high
contrast distance visual acuity, using letters of different sizes arranged from largest at the top to
smallest at the bottom, read one eye at a time or with both eyes usually from 6 meters (20 feet).
A person with 20/100 vision would need to be 20 feet away to read the smallest letters that
someone with “normal” (20/20) vision could read at 100 feet. The fraction can also be given using
the metric system (6/6 in meters = 20/20 in feet; 6/12 = 20/40, and 6/18 = 20/60) or using the
decimal or the logarithm of the minimum angle of resolution (logMAR) conversion. In logMAR
units, lower scores represent better vision. A more standardized test available and considered the
gold standard for clinical trials is the ETDRS chart.61
The frequency of its use in primary care in
Canada is not known but it appears to be feasible and practical for this setting. This chart has
letters with equal legibility, rows with an equal number of letters, a true log progression in letter
sizes down the chart, and consistent spacing between letters and rows (i.e., controlled crowding).
This and other “logMAR” charts were developed to improve accuracy and repeatability, thus
improving accuracy of longitudinal follow-up measurements. For example, the test-retest
reliability of the ETDRS charts (about ±0.10 to 0.15 logMAR [1 to 1.5 lines] in normal vision)62-
65 has been shown to be significantly better than with Snellen charts (up to ±0.33 logMAR
66).
The variability of both charts increases in poor vision situations,67-69
and may be higher in typical
use than in research settings.62
For statistical analysis, acuity scores from any chart can be
converted into logMAR units for comparison, although this is not very meaningful with the older
Snellen charts.
Other Tests. Other visual acuity testing can also be assessed using a handheld card or other
screening tools; a common threshold of reduced visual acuity is an inability to read a newspaper
at a normal reading distance of 40 cm with best refractive correction.70
Tools exist (e.g.,
16
Tumbling Es, Landolt C, Lea test) that incorporate symbols/optotypes that do not require
familiarity with the Roman alphabet. Pinhole testing may detect some, but not all, cases where
refractive correction may improve visual acuity; it will not correct reduced acuity due to non-
refractive causes such as cataract or AMD. Pinhole acuity therefore has value in distinguishing
between decreased vision from refractive errors and from medical eye problems. Low or mixed
contrast sensitivity cards or charts, such as the Pelli-Robinson Contrast Sensitivity Chart,71
Smith
Kettlewell Institute Low Luminance (SKILL card),72
and Mixed Contrast Reading Card73
are not
widely used yet. The Amsler grid, evenly spaced horizontal and vertical lines on paper, is used to
detect retinal defects affecting central vision, including AMD (associated with distortion in the
boxes on the grid or blank areas in the grid), although its sensitivity and specificity have been
reported as poor.74
Clinical Examination of Eye and Its Structures. Clinically significant cataracts can be
visualized via physical examination as change of colour or opacities in the lens. Early signs of
retinal defects can be observed using fundoscopic examination. This testing for the most part is
considered to apply within comprehensive eye examination by eye professionals.
Vision-Related Functional Limitations. Because vision-related function does not correlate
highly with visual acuity, and vice versa, it may be useful to assess patients’ perception of the
effect of their vision (and any interventions) on their functional ability.75
Structured screening
questions may be used (administered by personnel or patients) to elicit perceived problems in
function (e.g., reading, driving) due to vision, but not specific to visual acuity. Questions may be
used alone or within an interview schedule or assessment of various health domains (e.g.,
comprehensive geriatric assessment). Use of a validated questionnaire such as the National Eye
Institute Visual Function Questionnaire (NEI-VFQ-25) may also allow interpretation on their
vision-related quality-of-life.76,77
Rationale for Review of Vision Screening in Primary Care
Although regular eye examinations for older adults (≥65 years of age) within professional vision
settings (e.g., optometrist offices, ophthalmologist offices) are promoted, readily available (over
4,500 optometrists in Canada), and widely-funded in Canada, it is unclear whether primary care
professionals should routinely screen for impaired visual acuity or other vision problems in this
population. Decisions on whether or not to recommend screening in primary care depend on the
17
degree to which identifying problems in this setting leads eventually to benefits that would not
otherwise be achieved, and that any benefits achieved would be sufficient to justify any harms.
Such benefits would include improvements, or prevention of decline, in visual acuity and/or
vision-related functioning, and reductions in potential consequences of poor vision such as
fractures or loss of independence. One factor that may influence whether primary care screening
would be effective is the degree to which most older adults are routinely visiting eye care
professionals (regardless of whether they have symptoms), or if there is a significant number not
seeking this care who therefore may have unrecognized vision problems and may benefit from
screening in primary care.
Self-reported data by seniors in the Canadian Community Health Surveys in 2005 suggested that
59% consulted with optometrists or ophthalmologists (in-person or via the telephone) during the
previous year.78
The survey also found that 86% of those with glaucoma, 76% of those with
cataract, and 63% of those with diabetes had used an eye care provider in the last year. Despite
these data, it is unclear what proportion of people who are not seeking eye professional care—
because of complexities related to symptoms (e.g., vision changes can be relatively subtle,
progress slowly over time, or occur in persons with cognitive dysfunction or other comorbid
conditions) or other barriers to care such as geography or lack of access to resources—would
benefit from either doing so, or receiving screening in primary care. Relatively high attendance
at eye professional offices by older adults within Canada might be expected due to the widely
available public funding for periodic eye examinations for this demographic; beyond assessment,
though, funding for spectacles, low vision services, and equipment is quite variable.17,78,79
Moreover, findings that over 40% of older adults in Canada have not sought a vision assessment
over the previous year78
and that between 11-51% of older adults in developed countries have
undetected, but highly correctable, impaired visual acuity (<20/40; based on pinhole correction)
suggest that there could be benefit from primary care screening.30
Relevant Guidelines
There exist no Canadian recommendations on vision screening for adults at or above 65 years of
age targeting primary health care providers apart from eye professionals.
Primary Care Physician Settings

18
The United States Preventive Services Task Force (USPSTF) has, to-date, offered the most
relevant guideline in terms of targeting primary care providers (not eye professionals), on visual
acuity screening in primary care for adults 65 years and older and not presenting with vision
problems.80
Their 2016 recommendation was “no recommendation” because of “insufficient
evidence to assess the balance of benefits and harms of screening for impaired visual acuity in
older adults.” Of note, the most direct evidence on screening program effectiveness used for this
guideline was from three trials undertaken mainly in primary care physician offices. Evidence
from screening in homes or other primary-healthcare-relevant settings was not examined.43
The American Academy of Family Physicians recommendation on screening for visual acuity in
older adults is in agreement with this USPSTF recommendation (insufficient evidence).81
In 1995, the Canadian Task Force on the Periodic Health Exam, the earlier iteration of the
CTFPHC, recommended performing visual acuity testing using the Snellen chart and fundoscopy
or retinal photography as part of periodic health examination of elderly patients with diagnosis
with diabetes for at least 5 years (B recommendation).82
No recommendation was made for the
general population 65 years of age or older.
Eye Professional Organizations
Most guidelines for vision screening are developed within the context of eye professional
settings; the term “screening” in such guidelines refers to asymptomatic patients but usually
involves tests which go well beyond what is possible in primary care. Because of this, the below
guidelines are acknowledged although are not directly related to this review focusing on vision
screening by other primary care providers using simple screening tests.
The Canadian Ophthalmological Society’s 2007 recommendations on periodic eye examinations
(i.e., by an eye professional) specify comprehensive eye tests for: (i) asymptomatic, low-risk
older adults (>65 years) at least every two years (Level 1 evidence), (ii) high-risk (e.g., those
with diabetes, cataract, macular degeneration, or glaucoma [and glaucoma suspects], and patients
with a family history of these conditions) adults over 60 annually (Consensus), and (iii)
19
symptomatic adults of all ages noting changes in visual acuity, visual field, colour vision, or
physical changes to the eye as soon as possible (Consensus).40
The Canadian Association of Optometrists recommends adults aged 65 years or older should
undergo an eye examination annually (Level 1 evidence using 2001 USPSTF criteria).83,84
The American Academy of Ophthalmology recommends comprehensive medical eye
examinations (i.e., by an optometrist or ophthalmologist) every 1-2 years for asymptomatic
patients 65 years and older without risk factors; recommendations for those with risk factors are
limited to glaucoma.85
The American Optometric Association recommends comprehensive adult eye and vision
examinations annually for those over 60 and asymptomatic or risk free, and annually or as
recommended for those over 60 and at risk.86

20
Section II. Review Scope and Approach
This review was completed by the Evidence Review and Synthesis Centre (ERSC) at the
University of Alberta. The review was developed, conducted, and prepared according to the
CTFPHC methods (http://canadiantaskforce.ca/methods/methods-manual/). A working group of
CTFPHC members was formed for development of the topic, refinement of the key questions
and scope, and rating of patient-important outcomes considered most important for creating a
recommendation. Perspectives of patients, and members of the public were incorporated
regarding prioritization of outcomes (benefits and harms), and will be engaged once again during
guideline development. The protocol was registered with the International Prospective Registry
of Systematic Reviews (PROSPERO) database (CRD42016053088).
Analytical Framework
Figure 1 is an analytical framework that depicts the structure used to address the relevant Key
Questions (KQs) for evaluating the benefits and harms of primary care screening for community-
dwelling older adults (≥ 65 years) with unrecognized impaired visual acuity or vision-related
functional limitations.
Figure 1. Analytical framework
AE = adverse effect; KQ = key question; QoL = quality of life
Key Questions*

21
Stage 1a
KQ1: What are the benefits and harms of screening compared with no
screening for unrecognized** impaired visual acuity or vision-related
functional limitations in community-dwelling adults ≥65 years of age?
Stage 1b
KQ2: (a) How do community-dwelling adults ≥65 years of age weigh the
benefits and harms of screening for impaired visual acuity or vision-
related functional limitations, and (b) how do these values inform their
acceptance or decisions to undergo screening?
KQ3: What is the cost-effectiveness of screening for unrecognized impaired
visual acuity or vision-related functional limitations in community-
dwelling adults ≥65 years of age?
Stage 2
KQ4: What is the accuracy of screening tests commonly used in primary care
settings for impaired visual acuity or vision-related functional limitations?
*Decision process for staging outlined in section on Staged Approach, e.g., stage 2 was sequential to stage 1 and would have only
been conducted if inadequate quality of the evidence was identified from stage 1a. Stage 1b was not conducted because of little
uncertainty by the CTFPHC in the balanace of benefits/harms (KQ2) and lack of effectiveness (KQ3).
**By unrecognized we include people that may have symptoms but have not brought them to medical attention, or do not
recognize they have a vision-related dysfunction; they will typically not have actively sought eye assessment or care.
Staged Approach
We took a staged approach to this review based on the quality of the body of evidence for each
KQ, assessed using methods developed by the Grading of Recommendations Assessment,
Development and Evaluation (GRADE) Working Group (http://www.gradeworkinggroup.org/).
The GRADE methods for assessing the quality of evidence (classified as high, moderate, low,
very low) are described in more depth later, but, essentially, for each outcome rated as critical by
the CTFPHC and sample of patients, a rating of high quality evidence relies on precise and
consistent effect estimates from studies having few limitations on internal validity (i.e., not high
risk of bias) and examining directly relevant populations, interventions, comparators, and

22
outcomes (i.e., PICOs). Decisions made during the evidence review (to proceed through KQs)
are based on the information needs of the CTFPHC for making a recommendation based on the
balance of critical benefits and harms, as defined by transparent rating processes.
Evidence with the potential to provide the most internal validity and direct evidence for the
effectiveness of screening programs was prioritized; that is, we started by examining evidence
from randomized controlled trials (RCTs) of screening programs reporting on clinically
important outcomes (most directly related to PICOs and analytical framework) for KQ1. These
studies would compare outcomes over time between a control group of no screening/usual care,
and an intervention group for which there is an intent to screen all people and, if indicated,
encourage them through referrals or otherwise to seek further assessment by eye professionals
and possibly treatment or other services to improve their vision and/or other patient-important
outcomes related to vision. Further staging beyond this point (observational evidence for KQ1 or
review of KQ4) would require careful deliberation with documentation of rationale. In cases
where evidence on test accuracy and treatment effects may be used to provide indirect evidence
on screening program effectiveness, limitations would be recognized that this evidence may not
account for several factors (e.g., differences in absolute, and possibly relative, effects when
comparing studies in general screening populations vs. those requiring treatment; follow-up on
referrals for diagnosis and/or treatment; adherence to screening and treatment; types of screening
protocols) that would be captured by direct evidence. Only the study designs with the highest
possibility of internal validity (RCTs for treatment and exclusion of case-controls for accuracy)
would be examined. Answering KQ 2 is important when the evidence suggests that an
intervention may be effective or that there may be important harms, but there is some degree of
uncertainty, or when there is evidence of effectiveness, but there are also important harms to
consider and the balance between these could reflect personal preferences. Examining cost-
effectiveness (KQ3) relies on having enough moderate-to-high quality evidence on KQ1 with
demonstration of a positive benefit-harm ratio. We report here only on KQ1 because the
CTFPHC determined that at this time examination of the other KQs was not required for their
decision making.
Section III. Review Methods
Integration of Existing Systematic Reviews

23
To build in efficiencies and capitalize on other work conducted, we followed, as suitable, the
CTFPHC’s approach to integrating existing systematic reviews (see Appendix A). For this
review, our approach focused on examining existing reviews to identify studies meeting our
criteria, with the addition of an update of the evidence to present date using a unique,
comprehensive search. We had no plans to use data extraction or other findings from the
reviews. During protocol development, we identified four good quality systematic reviews to
integrate into this review; reviewing their searches, scope, inclusion criteria and
included/excluded studies lists indicated they would together capture studies for KQ1 to 2012
and KQ4 to 2015.43,87-89
Additonal systematic reviews identified during our search update from
2012 were also examined closely for studies.
Literature Search
For KQ1, we conducted searches to update the literature from that identified by existing reviews
to 2012. Our planned searches for KQs 2-4 are included in our protocol (available at
http://canadiantaskforce.ca/guidelines/upcoming-guidelines/visual-acuity/) but not here because
of the focus on KQ1.
The literature search strategy for KQ1 was developed and implemented by a research librarian.
The search strategy consisted of both controlled vocabulary, such as the National Library of
Medicine's MeSH (Medical Subject Headings), and keywords, and was peer-reviewed using the
PRESS checklist. Terms used were intended to generate a highly sensitive search to capture
studies that may employ vision screening as a (even unreported) portion of a multicomponent
assessment (e.g., geriatric assessment, risk assessment) as well as interventions to reduce risk for
older adults. Methodological filters were applied to limit retrieval to RCTs. The search was
restricted by language to include full texts published in English or French, and was limited to a
publication date on or after 2012.
On August 30, 2016, we searched MEDLINE (1946-) via Ovid; Embase (1974-) via Ovid;
Cochrane Library; CINAHL (1937-present) via EBSCOhost; and PubMed via NCBI Entrez. The
searches were updated in October 2017. The search strategies for all databases are reported in
Appendix B.

24
Supplementary searches were conducted and documented according to CTFPHC methods for
grey literature searching, primarily through internet-based searches (via adapted Canadian
Agency for Drugs and Therapeutics in Health [CADTH] grey literature checklists;
https://www.cadth.ca/resources/finding-evidence/grey-matters) and trial registries
(ClinicalTrials.gov, World Health Organization International Clinical Trials Registry Platform).
Websites of relevant Canadian stakeholder organizations were also searched. We reviewed the
bibliographies of all included papers and relevant systematic reviews. We contacted authors (by
email with three attempts over 30 days) of relevant protocols, trial registries, and abstracts that
identified studies not located in the searches to obtain any reports or publications of completed
studies.
All results of the database searches were imported into an EndNote® database (Thomson Reuters,
New York, NY) for reference citation, and into DistillerSR (Evidence Partners Inc., Ottawa,
Canada) for screening and selection procedures. Our grey literature search process was
documented, with literature eligible for full text screening identified in the PRISMA flow
diagram.
Eligibility Criteria
Table 1 outlines the study eligibility criteria for KQ1 based on the population, intervention,
comparator, outcomes, timing, setting, and study design (PICOTS-D). Following the table, we
provide details on outcome rating and additional criteria. For this review, the term unrecognized
was used to represent people who may have symptoms but have not brought them to medical
attention, or who do not recognize they have a vision-related dysfunction; they are people who
have not recently sought eye assessment or care. Trials including younger participants were
included if the mean age minus one standard deviation (SD) was more than 65 years.
Table 1. Eligibility criteria using PICOTS-D for KQ1: Benefits and harms of vision screening
Criteria Include Exclude

25
Populations Community-dwelling adults age 65 years and older with
unrecognized* impaired visual acuity or vision-related
functional limitations
Population subgroups of interest: age (65-74 vs 75-84
vs 85+), socioeconomic status (i.e., education, income),
ethnicity (i.e., percent non-Hispanic white versus others),
geographical region (rural vs. urban)
Significant portion of participants (>25%) with visual
acuity worse than 20/200 (i.e. severe or profound
visual impairment)
Focus on older adults having characteristics placing
them at high risk for vision problems or when
screening test application by primary care providers
would be considered significantly challenging. This
would exclude studies where most patients have a
history of falls, residency in nursing homes, diabetes,
dementia (including Alzheimer's), other disorders of
the vision system such as glaucoma as well as stroke,
Parkinson's or other conditions making it difficult to
participate in vision screening.
Interventions Vision screening tests, alone or within multicomponent
screening/assessment, performed by primary health care
professionals (may include home- or online-based tools
interpreted by primary care professionals) or their
designates
Screening may be followed by interventions including
referral and structured treatment or therapy provided by
eye care professionals, occupational therapists, or social
workers for screen positive participants in intervention
arm.
Intervention subgroups: type of screening test (i.e. self-
report vs. charts or other more objective tests; visual
acuity vs. vision-related function), active treatment vs.
referrals vs. no referrals; health care provider interpreting
the tests (physician vs nurse vs other); setting of program
(physician office vs. community/home)
Tests or assessments that only evaluate reading speed
or visual field
Tests performed by eye professionals
Comparator No vision screening, delayed screening, attention control
(e.g. educational session without tests),
screening/assessments involving all components as
intervention except vision component; usual care (may
include targeted screening/case finding)
Different vision screening test
Outcomes Benefits:
Mortality
When vision screening is within a multicomponent
screening intervention, the study will only be included

26
Potential adverse consequence of poor vision:
fractures (risk or rate of incidence; will accept falls
as surrogate)
Potential consequence of poor vision: loss of
independence
Vision-related QoL or functioning:
(i) using composite/index scores from validated
scales (e.g., Activities of Daily Vision,
National Eye Institute Visual Function
Questionnaire, Visual Function Index)
(ii) non-validated tools involving self-report of
functional limitations related to vision (e.g.,
reading, IADLs)
Presenting (habitual with or without glasses) visual
acuity:
(i) mean change in acuity in logMAR units
(ii) proportion with minimally important
difference, i.e., change of 0.10 logMAR (5
letters, 1 line)
(iii) proportion at follow up with acuity equal to or
better than 6/18, 3/10 (0.3), 20/60, logMAR
0.5 (i.e., no or mild impairment using WHO
classification)
(iv) proportion at follow up with acuity equal to or
better than 6/12, logMAR 0.3, 20/40 (i.e.,
impaired visual acuity using North American
convention)
(v) self-report of visual disturbances (e.g., blurred
vision)
Harms
Serious or major AEs from associated vision/eye
treatment (requiring hospital admission, urgent
intervention, causing disability, permanently
limiting self-care or activities of daily living or as
defined by authors)
Anxiety or stress if true positive/diagnosed but
treatment options are limited or inaccessible (e.g.,
because of real or perceived costs) for condition
(e.g., AMD, contraindications)
Implementation Factors**
in assessment of vision-related outcomes, i.e. not for
mortality, falls etc., unless the outcome is attributed
directly to a reduced or improved vision by the
authors.

27
Uptake of referrals (proportion of intervention
group)
Eye care professional visits (difference between
groups)
Timing 1980 to present (approximate onset of policy and
research on vision screening in primary care)
Any follow-up duration
Subgroups: short-term (0-<6 months), medium-term (6-
<24 months), long-term (24+ months) follow-up
Design Health outcomes & implementation factors: RCTs only
Harms: staged to RCTs, then controlled experimental,
then controlled observational
Language English and French
Setting Generalizable to primary health care, including but not
limited to physician offices, primary care clinics,
community health centres, participant’s home, prisons,
remote stations
Eye specialist setting
Any setting where it could not be reasonably
generalizable to a Canadian primary care
* By unrecognized we include people that may have symptoms but have not brought them to medical attention, or do not
recognize they have a vision-related dysfunction; they will typically not have actively sought eye assessment or care.
**Secondary outcome in studies reporting on other outcomes.
Outcome Rating
The primary outcomes of interest for this review are listed in Table 1. The outcomes considered
most patient-important, thus critical for making recommendations on screening for impaired
visual acuity and vision-related functional limitations were selected based on ratings by members
of the CTFPHC and on the basis of the findings of an engagement exercise with a sample of
older adults in Canada, conducted by an independent group with expertise in knowledge
translation from St. Michael's Hospital in Toronto, Ontario. All patient-important outcomes rated
as critical (7 to 9 out of 9) were included, with the possibility to also include those rated as
important (4 to 6 out of 9) if there were fewer than eight critical outcomes; this rule of thumb for
the number of outcomes is based on guidance based on cognitive limits when guideline panels
are considering net balance of benefits and harms. Outcomes in the category of Implementation

28
Factors were considered secondary outcomes, therefore were only considered when studies also
reported on one or more critical outcomes. All outcome ratings were conducted prior to final
study selection and data extraction; that is, the CTFPHC was blinded to the studies and their
results.
Additional Eligibility Considerations
We did not have a minimum sample size for inclusion, nor did we have a minimum threshold for
extent of incomplete follow-up or participant attrition; these factors were considered during
assessment of the quality of the body of evidence (e.g., using GRADE methods the precision
domain accounts for sample size across studies and the study limitations/risk of bias domain
considers high and/or differential attrition).
Case reports and case series (i.e., group of patients selected based on particular outcome) were
excluded as were papers not reporting primary research (e.g. editorials, commentaries, opinion
pieces). Conference abstracts and systematic reviews were not eligible for inclusion, but were
examined and served to help identify full study reports.
Screening and Selecting Studies for Inclusion
For the database searches, two reviewers independently screened the titles and abstracts (when
available) using broad inclusion/exclusion criteria. Citations were classified as “include/unsure,”
“exclude,” or “reference” (i.e., conference abstracts, protocols, and systematic reviews). One
reviewer examined the “reference” group further, and this reviewer and the librarian conducted
all grey literature searches. The full text of all studies classified as “include/unsure” or identified
after reviewing the reference citations or grey literature were independently reviewed by two
reviewers using a standard form outlining the inclusion and exclusion criteria. Disagreements on
final inclusion of all studies were resolved through consensus or consultation with a third
reviewer. The title/abstract screening and full-text selection processes were conducted and
documented in DistillerSR. The flow of literature and reasons for full text exclusions were
recorded in a PRISMA Flow Chart.
At any stage of screening, we screened as “include/unsure” studies evaluating multicomponent
screening or assessments, where it was not clear if a vision test was incorporated and/or if vision

29
outcomes were collected or analyzed. For this to occur in cases of missing test information at full
text review, there must have been enough description of the screening/assessment to suggest a
vision component may have been included (e.g., mention of physical or medical function, or
safety/risk assessment), or mention of referral to a range of specialists. Studies with a clear focus
on one or more interventions (e.g., exercise therapy, cognitive therapy) unrelated to vision were
excluded. For those we screened in with insufficient data for inclusion/exclusion, we contacted
the first or corresponding author by email (via published report or limited internet searching), up
to three times over four weeks to obtain further clarification on the intervention and/or whether
data for vision outcomes were available. We accepted individual patient data (raw data) on
outcomes provided it was delivered in an easily accessible and analyzable format.
Data Extraction & Reporting
One reviewer independently extracted data from each included study; a second reviewer verified
all data. Disagreements were resolved through discussion or consultation with a third reviewer
until consensus was reached.
Study characteristics tables were created for each study and a narrative summary was written to
summarize all studies by design, country of origin, sample sizes, population(s) (including
subgroups), intervention(s) (including data on screening criteria and for subgroup questions),
comparator(s), setting, and outcome measures, as reported by studies.
When there were multiple publications associated with a study we considered the earliest report
of the main (primary) outcome data to be the primary data source, so long as this was a full paper
and not an abstract. We extracted data from the primary source first and then added outcome data
reported in the secondary/associated publications and data sources. We reference the primary
source throughout the evidence report; where applicable we also cite an associated publication.
For continuous outcomes measures, we extracted (by study arm) the mean baseline and endpoint
or change scores, standard deviations (SD) or other measure of variability, and number analyzed.
We did not include outcome data from studies that did not provide a follow up change or
endpoint scores, or data that could be used to calculate follow up scores. When necessary, we

30
approximated means by medians. If standard deviations were not given, they were computed
from p-values, 95% confidence intervals (95% CIs), standard errors, z-statistics, or t-statistics. If
computation was not possible they were estimated from upper bound p-values, ranges, inter-
quartile ranges, or (as a last resort) by imputation using the largest reported SD from the other
studies in the same meta-analysis. For dichotomous outcomes, we extracted counts or
proportions, and sample size, by study arm. Details on our methods for extracting data for harms
are included in our protocol but were not used in this review which included no studies reporting
on the harms of interest.
Data on within-study analyses on our subgroups of interest was collected, including: subgroups
(independent variables), the type of analysis (e.g., subgroup/stratified or regression analysis), the
outcomes assessed (dependent variables), and the authors’ conclusions. We collected data
suitable for patient and intervention subgroups (see Table 1) for performing our own subgroup
analyses based on study-level data.
Units of Analysis Issues. Unit of analysis errors can occur in studies that employ a cluster design
(i.e., a clinical practice) and yet are analyzed at the individual level (i.e., patients), potentially
leading to overly precise results and contributing greater weight in a meta-analysis. For trials
which were cluster-randomized, for example by medical practice but not individual homes, we
performed adjustments for clustering if this was not done in the published report. We used an
intra-class correlation coefficient (ICC) of 0.01 reported in Smeeth 2002.90
Risk of Bias Assessment
Two reviewers independently assessed the risk of bias (ROB) of each included study, with
disagreements resolved through discussion to reach consensus. The results for each study and
across studies are reported by each domain and for the overall ROB score. The ROB for each
study was assessed on an outcome basis where needed, particularly when different outcomes
were assumed to have different susceptibilities to bias; for example, subjective outcomes and

31
expected harms are more prone to bias from non-blinding than objective outcomes and
unexpected/rare harms.
The RCTs were appraised using the Cochrane Risk of Bias tool.86
This tool consists of six
domains (sequence generation, allocation concealment, blinding, incomplete outcome data,
selective outcome reporting, and “other” sources of bias) and a categorization of the overall
ROB. For each domain a rating of low, unclear, or high ROB is determined. Blinding and
incomplete outcome data were assessed separately for patients/providers and outcome
assessment, and also by outcome (e.g., subjective vs. objective). To assist with outcome
reporting bias assessments, we sought study protocols and studies/data from registries; our
contact with authors to obtain outcome data also helped to minimize this bias. The overall
assessment was based on the responses to individual domains. If one or more individual domains
were assessed as having a high ROB, the overall score was rated as high ROB. The overall ROB
was low only if all components are rated as having a low ROB, and was unclear for all other
studies.
Data Analysis & Synthesis
For pairwise meta-analysis, we employed a random effects model using Review Manager
Version 5.0 (The Cochrane Collaboration, Copenhagen, Denmark). For continuous outcomes, we
report a pooled mean difference (MD); if multiple tools were used we would have used one of a
variety of options that exist for communicating results when combining two or more outcome
scales measuring similar constructs (based on clinical input).91,92
For dichotomous outcomes, we
reported relative risks (RR) or rate ratios, and absolute effects between groups with
corresponding 95% CIs. For calculating the absolute effects, we used the relative risk and
median baseline risk for the control group in the included studies. If event rates were less than
1%, the Peto odds ratio method was planned, unless control groups were of unequal sizes or
when there was a large magnitude of effect; when events became more frequent (5%–10%), the
Mantel-Haenszel method without correction factor was used for quantitative synthesis.93
The decision to pool studies was not based solely on the statistical heterogeneity (I2
statistic was
reported), but rather on interpretation of the clinical and methodological differences between
32
studies. When substantial heterogeneity was suspected, we conducted sensitivity analyses for
methodological differences, as appropriate (e.g., for studies rated as high risk of bias, parallel
versus cross-over designs), or subgroup analysis when heterogeneity was thought to arise from
differing effects based on our planned population or intervention subgroups of interest (see Table
1 and section below). Where there were at least eight studies in a meta-analysis, we analyzed
small study bias (which includes publication bias) both visually using the funnel plot and
quantitatively using Egger’s test.94
We would not have combined results from RCTs with other
study designs, if applicable. When a meta-analysis was not appropriate or feasible (based on
reporting) the results of each study are described.
Subgroup Analyses
Our primary approach for evaluating differential effect for subgroups (see Table 1) was to record
any within-study subgroup analyses performed by study investigators using individual patient
data; these results preserve the within-study randomization. Because these results are often based
on diverse methodology and may be difficult to interpret across the body of evidence, we also
performed our own subgroup analyses using study-level data, as possible, using either meta-
regressions (usually for continuous variables to enable some quantification of the effect) or by
stratifying the results of the pairwise meta-analyses by categories based on subgroup variables.
Stratified analyses were considered when at least two studies made up any group in a meta-
analysis (e.g., short vs. medium vs. long duration follow up; mean age for study was 65-74 years
vs. ≥75 years of age). Some support for the findings occurs when variables are limited in number
and defined a priori, the magnitude of the difference is practically important (supporting different
recommendations for each group), and the difference in the effects between subgroups are
statistically significant (e.g., Chi2 test for subgroup effects).
95 Nevertheless, these analyses rely
on study-level data and are observational (i.e., studies are not randomized), therefore are
interpreted as exploratory.
Assessment of the Overall Quality of the Evidence using GRADE
Two reviewers independently assessed the quality of the body of evidence, or confidence in the
effect estimates, for each outcome of interest using the GRADE methodology.96-100
Discrepancies were resolved through discussion and third-party consultation to reach consensus.
Assessments were entered into GRADEPro software and summarized in GRADE Evidence
Profiles and Summary of Findings tables. Within the GRADE Evidence to Decision (EtD)

33
Framework, the CTFPHC will use this evidence on each outcome, to assess the net benefits and
harms of each service across all outcomes (considering the relative importance of each), and also
consider patient preferences and values in addition to other elements including feasibility,
acceptability, costs, and equity (using stakeholder input), to develop the recommendations on
screening for impaired visual acuity or vision-related functional limitations in primary care.
The general approach is outlined here although methods align with GRADE guidance. For
evidence on the benefits and harms of screening, as a starting point the quality was assigned as
high for evidence from RCTs (low if using observational studies). Thereafter, we examined and
potentially downgraded the quality based on the five core domains: study limitations/ROB,
inconsistency, indirectness, imprecision, and reporting bias. We also considered the additional
domains of dose-response association, plausible confounding, and strength of association (i.e.,
large magnitude of effect [i.e., large ≤ 0.5 or ≥ 2.0 or very large RR ≤ 0.2 or ≥ 5.0]), to
potentially upgrade the quality when no other serious concerns existed.101
For the study limitations domain supported by evidence from RCTs, we downgraded the quality
by one or two levels depending on the proportion of trials (e.g., one very large trial may
outweigh two very small trials) assessed as having high ROB for the particular outcome under
consideration. For inconsistency we downgraded when 95% CIs did not overlap each other in
most studies; when the body of evidence for an outcome consisted of a single study, although
there is no evidence of inconsistency we usually downgrade for this domain because of lack of
demonstrated consistency. Indirectness of the evidence was based on evaluating the relevance of
the body of evidence’s PICOs compared with ours; for instance, we downgraded when falls
(surrogate to critical outcome) were used for the outcome of fractures. A precise estimate is one
that allows for a clinically useful conclusion. We assessed the findings as imprecise when the
total sample size for the outcome (using total events for dichotomous outcomes) did not meet the
Optimal Information Size, or (if OIS sufficient), when the 95% CI crossed no effect but also
included values that would represent important benefit or harm to many patients; in terms of
these values, for dichotomous outcomes we used a general rule-of-thumb of crossing a RR of
0.75 or 1.2596
and for continuous outcomes we would use a minimally important difference
(MID) for each tool if literature was available for this. We had defined a priori MIDs for some
continuous outcomes: NEI-VFQ-25 (4-6 point change),75
and (via clinical input and data on test
34
reliability) change in visual acuity (≥ 0.1 logMAR = 5 letters = 1 line). Other thresholds would
have been determined, as necessary depending on the measurement scale used, based on
available literature or clinical input. Thresholds may also be determined by the CTFPHC in a
post hoc manner (thus may change the ratings for precision) after considering what magnitude of
effect would be clinically meaningful in view of balancing benefits and harms and other
considerations such as cost and patient preferences. Reporting bias was evaluated with respect to
publication (small study) bias.
Interpretations
In efforts to enhance communication about how our interpretations of the quality of evidence
reflect varying levels of certainty about the effects, we chose to use standard wording to describe
each level of GRADE findings. For findings of high, moderate, low, and very low quality
evidence we use “will”, “probably/likely”, “may/appears to”, and “not known/very uncertain”,
respectively, in our textual descriptions when discussing the results.

35
Section IV. Results
Key Question 1. Benefits and harms of screening
Literature Search and Selection
Our database searches from 2012 identified 14,995 citations after duplicates were removed; 452
of these were eligible for full text review after screening titles and abstracts. An additional 146
records were eligible for full text review, based on review of all titles and/or abstracts from (i)
the included and excluded study lists from the four systematic reviews43,88,89,102
selected a priori
for review (n=138), (ii) other unique records (n=4) from reference lists of 21 other relevant
systematic reviews (one on vision103
and others on geriatric or falls risk assessment etc.)
identified in our database search (Appendix C), (iii) our grey literature searches of trial
registries, dissertation abstracts (n=0), and (iv) stakeholder websites or suggestions during peer
review (n=4). After complete full text review (n=452), including author contacts when
information was needed for determining eligibility (i.e., inclusion of a vision component to the
intervention and vision-related outcomes in cases of multicomponent interventions), we excluded
437 articles for reasons identified in Figure 2 and Appendix D, and included 15104-118
RCTs
reporting on 17,400 participants. Fourteen of these were identified by our database search and
the four primary systematic reviews; one118
was found from the reference list of another
systematic review.103
Description of the Included Studies
All 15 trials we included examined older adults regardless of whether or not they had recognized
vision problems. Although this deviated from our inclusion criteria, as stated a priori, it was
decided that while the main population anticipated to potentially benefit from screening in
primary care would be those people not having regular eye care provision, in reality screening in
primary care would not necessarily use this selective (possibly considered case finding) approach
and the benefits at a population level are suitable to examine in terms of screening programs.
Appendix E includes detailed study characteristics tables.
The number of enrolled participants across the 15 trials ranged from 93 to 4,340. The average
age of participants in the 11 trials that reported age was 78.5 years,104-106,110,112-118
with the other
four trials recruiting participants aged 70 and over109,111
, having inclusion criteria of age 75 to

36
84,108
or only recruiting participants aged 75 or older107
. The mean age was below 75 years in
three trials,112,115,116
and 85 years or older in one.104
A slight majority (62.8%) of participants was
female in the 11 trials reporting on sex104-106,108,111-118
(with one reporting >80% females)104
, two
studies reporting on ethnicity included predominately White participants (86.5%)114,115
, and six
reporting on the proportion living alone reported that nearly half of participants lived alone
(46.8%).104,106,108,112,113,117
Figure 2. Flow of literature through screening and selection process
a Reports of these trials provided information strongly suggesting no vision outcome data was collected (e.g., only
used hospital records) (n=4), or the study authors did not respond to our attempts at contact (n=8). b Authors confirmed that there was no collection of data for an outcome relevant to the vision component of the
intervention (n=27; report of another systematic review89
relied on for 4 of these responses) or that this data was no
longer available (n=2).
37
Only three studies reported on the education level of participants, without any indication that the
study population predominantly represented a low or high level of education.104,112,115
Trials were
conducted in Norway,104
Germany,112
the U.K.,106,107,109,111,116
Australia,110,113,117,118
the
Netherlands,105,108
and the U.S.114,115
One study noted that 51.5%109
of participants were from an
urban geographical region, another selected from 4 rural and 1 borough municipalities104
; while
others commented that their respondents were from a metropolitan area112
, urban community113
,
urban residential area107
, or suburb.110
Recruitment was from general practice lists for 10
studies;105-107,109-112,114-116
two trials108,113
recruited from the population/community, and three
from an aged care assessment list,117
a home care list,104
or an insurance company registry.118
Most studies excluded patients living in residential care facilities and/or with dementia, and as
per protocol we excluded studies where recent falls or severe cognitive impairment was an
inclusion criteria. Only three of the studies required participants to be completely dependent in
ADLs,112,115,116
and in two trials patients were either receiving some form of home care104
or
being assessed for home care provision.117
For those studies reporting on any falls at baseline
(n=7),106,110,111,113,115,117,118
rates over the previous 12 months were generally 23% to
33%111,115,117,118
but as high as 55% (receiving aged care assessments),117
over the last 6 months
was 20%,106
and over the last month was 6.3%.113
None of the trials exclusively enrolled
participants not having regular eye care providers.
Only two113,117
of the 15 RCTs had an isolated vision screening intervention arm; both trials used
a multifactorial design where one or more of four arms did not receive vision screening for
comparison. All other trials incorporated vision screening within a multicomponent assessment
of health and functioning. Ten 105,107-112,114-116
of the trials relied on self-reports on general
presenting vision (e.g., fair or worse vision indicating a positive screen)108,109,111
or on having
one or more difficulties with vision (e.g., reading newspaper or one of several vision-related
activities);105,107,110,112,114-116
in two of these trials,105,114
participants having responded positively
to having difficulties were to also have their vision screened using a Snellen chart. Five
trials104,106,113,117,118
relied only on objective tests of presenting, distance visual acuity, with or
without additional tests for other vision functions such as near vision,117
contrast sensitivity118
or
visual field.113,117,118
Apart from the Snellen chart screening in those trials also using self-
reported vision difficulties, the charts used for measuring distance visual acuity included the
Verbaken chart113
(low and high contrast), Bailey-Lovie logMAR104
, Glasgow acuity chart106
,

38
VectorVision logMAR chart,117
and a letter chart with high and low contrast letters reported by
the authors.118,119
The vision screening was performed at home in seven trials104,107-111,113
, at a physician’s office or
the home in four,105,106,112,116
and at a day hospital,117
falls clinic,118
physician office,114
and
through telephone calls along with visits to the nurse at a physician office115
in the other four
trials. Screening was performed by nurses in seven of the trials,104,106-111
by the researchers in
two trials,117,118
a trained assessor113
or office staff member114
in two, and through self-reported
mailed questionnaires in three.112,115,116
Only one trial used a physician to complete the
screening.105
Trials reported one screening visit, but also had between 1 and 12 health care
interactions after screening where results could have been assessed and treatment referrals made.
Follow-up ranged from 2.5 to 47 months (mean 18.6 months); studies with longer follow-up
usually had more interactions. All trials included some action based on the screening results,
such as providing results to physicians,110,112,114-116
referrals to eye professionals,104,108,117,118
one
or both of the former.105-107,109,111,113
For those providing results to the physicians and no direct
referrals to eye professionals, three provided physicians with training and manuals and either
clinically pertinent articles,114
or easy access to clinical practice guidelines and screening results
within electronic patient records.112,116
Although it is difficult to predict to what extent other
(non-vision specific) features of the multicomponent interventions may theoretically lead to
changes in visual acuity or vision-related function, three trials provided co-interventions that
were considered more likely to contribute to vision changes beyond what would be expected
from referral to eye professionals; these included advice on improving vision (e.g., wearing hats
and avoiding multifocal lenses when outside),118
and home lighting condition
improvements.104,111
Ten studies reported that the control group also received some form of vision assessment at
baseline,104,106,107,109,111,113-115,117,118
although this information was used for outcome comparison
with the screened group and not explicitly acted upon with referrals or other intervention
components (i.e., not considered screening). One study using an objective screening method for
the intervention group allowed for referrals based on serious self-reported vision problems which
were assessed in all people in the control group;117
another trial of objective screening106
included “targeted screening” in their control group, with all patients given a basic screen
39
(including self-reported vision) and those having three or more major health or functional issues
receiving a detailed assessment including the objective vision screening (only 5.5% of control
group received detailed vision screening). We did not exclude these two studies for not having a
comparator of interest (no screening, usual care, or attention control) because there was limited
certainty for the other studies that the control group did not receive screening with referrals in
some cases (i.e., there was no prohibition from screening/testing control group participants) or
that participants’ knowledge of their results from the baseline vision assessment would not lead
them to self-seek eye professional care. Therefore, we consider the control groups in these trials
to largely represent usual care where there may be some form of screening.
Although 11105-112,115,116,118
trial authors reported on participant deaths by study group during
follow-up, and some reported in some manner on loss of independence (e.g., five105,109,112,116,117
reported on movement into long-term care), the multicomponent nature of most of the
interventions prevented us from attributing effects on these non-vision outcomes to vision
screening. The two studies113,117
(n=630) with multifactorial designs and thus reporting on results
specific to vision screening did not report on mortality of loss of independence by arm. No study
reported on fractures, although two reported on falls that were attributed to vision screening,
either because vision was an isolated intervention113
or because of other reasons for attribution
stated but not reported in detail.110
One trial 106
reported on vision-related functional limitations
using a validated questionnaire. Five104,106,113,117,118
reported on distance visual acuity measured
by charts, with variable numbers reporting on related outcomes of mean change in visual acuity
across all participants (n=4), proportion of participants with impaired visual acuity changing for
better or worse by ≥0.1 logMAR (n=1), or the proportion meeting a particular threshold (<20/60;
n=1 or <20/40; n=2). Ten trials105,107-112,114-116
reported on self-reported vision, as either (fair or
worse) general vision or having problems in one or more tasks related to vision. No trials
reported the harms of serious AEs (attributed to vision screening or its sequelae) or anxiety/stress
from a diagnosis in situations of inaccessible treatment options.
We have some confidence that the results on vision outcomes are not confounded greatly by
other components in the trials (e.g, medication review, nutritional assessment), but cannot rule
this out; where it is more obvious there may have been considerable confounding (e.g., lighting

40
modifications) we provide comment in the results section and have incorporated this into our
GRADE assessments of indirectness.
Methodological Quality of Studies
Table 2 shows a summary of the assessments by ROB domain for the trials. Sequence generation
was described and adequate (low ROB) for most (13 of 15) trials, as was allocation concealment
(10 of 15). For trials reporting subjective outcomes (n=11; i.e., self-reported vision or vision-
related functioning), ratings were high ROB for the blinding domains, except for three RCTs
having unclear ROB for participants/personnel because the control group did not receive the
vision assessment at baseline and the providers were not in contact with the control group during
the trial. For objective outcomes (i.e., measured visual acuity using charts), which are less prone
to performance and outcome ascertainment biases (n=5), trials were rated as unclear ROB for
these domains with the exception of one trial rated as low ROB for outcome assessment due to
adequate blinding of personnel. Two RCTs were at high ROB, and six were at unclear risk, for
incomplete outcome data; both RCTs at high ROB had >30% attrition in both groups for
outcomes of interest to this review even when considering attrition due to deaths (e.g.,
intervention group: 42.1% of those alive vs. control group: 32.3% of those alive106
). Both our
methods and those of Smeeth et al.89
(one of the reviews we integrated) largely guarded against
selective outcome reporting; authors of 10 of the trials were contacted and 8 provided results, or
clarified definitions, for outcomes of interest. Moreover, we had a fairly high response rate (23 of
31; 74%) for the studies we excluded for not having vision outcome data collected or as an
objective of the study. Overall, ROB for subjective outcomes was considered high105-112,114-116
and for objectives outcomes (i.e. visual acuity using standardized charts) was considered
unclear104,113,117,118
or high.106
Table 2. Risk of bias ratings for each domain
Study Sequence Generation
Allocation Concealment
Blinding of Participants and Personnel
Blinding of Outcome Assessors
Incomplete Outcome Data
Selective Outcome Reporting
Other Biases*
S O S O S O
Dapp 2011
L L H H H L U
Day 2002
L L U U L U L
Eekhof 2000
U U U H U L U
Haanes 2015
L U U U U U L
Harari L L H H U L L

41
2008
Lord 2005
L L U L U L L
McEwan 1990
L U H H U L L
Moore 1997
L U H H L L U
Newbury 2001
L L U H L L L
Smeeth 2003
L L H U H U H H L L
Tay 2006
U U U U U L L
Van Rossum 1993
L L U H U L L
Vetter 1984
L L H H U L L
Vetter 1992
L L H H U L L
Wagner 1994
L L H H L L L
ROB: risk of bias; S = subjective; O = objective; L (green) = low ROB; U (yellow) = unclear ROB; H (red) = high ROB
Blank cells indicate scoring not applicable (i.e. no subjective or objective outcomes were reported by that study).
*Other source of bias was baseline imbalances between groups.
Detailed Findings by Outcome
No trial contributed data for mortality or loss of independance because of the i) inability to
attribute any effects on these to vision screening alone when the interventions (13 trials) included
multicomponent screening/assessments incorporating multiple health and functional domains, or
ii) lack of reporting on these outcomes by group in those trials113,117
(n=630) with results specific
to a vision screen. All other outcomes were vision-related or directly attributed to vision
screening.
Fractures
No trial reported on fractures although falls were considered to provide indirect evidence for this
outcome. In a full-factorial trial randomizing patients (n=1,107) to vision improvement
(screening using multiple objective tests [visual acuity, stereopsis, field of view] with referrals),
strength and balance, home hazard management, or no intervention (8 groups in total) to reduce
falls, Day et al.113
reported no significant difference (incidence rate ratio [IRR], 0.91; 95% CI,
0.82 to 1.16) for total number of falls over 18 months between those receiving the vision
screening (97.8 per 100 person years) compared with those not receiving this intervention (107.3
per 100 person years). The main effects model results (i.e., vision vs. no vision screening across
all 8 groups) were used because of no significant interaction effect between groups, but we
cannot rule out confounding on this outcome from the other interventions received by 75% of
participants receiving vision screening. No significant difference was found in another 12-month
trial reporting on falls attributed to poor vision (intervention: 4 of 45 vs. control: 3 of 44; RR,
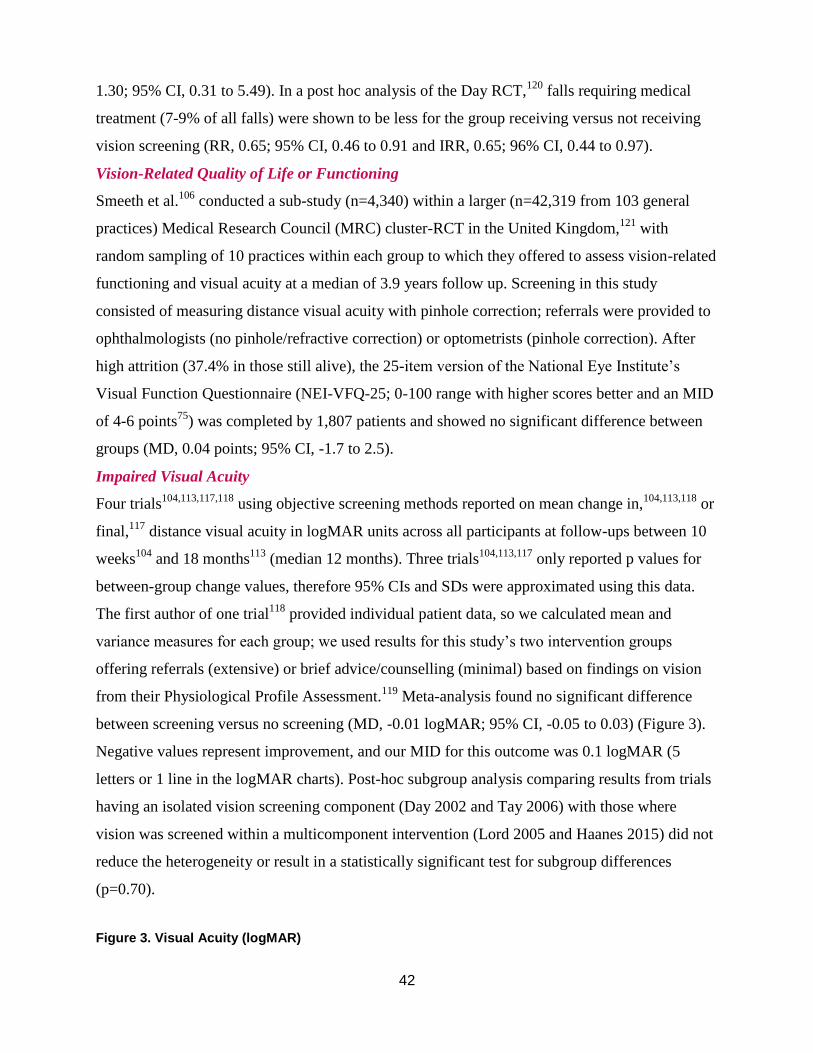
42
1.30; 95% CI, 0.31 to 5.49). In a post hoc analysis of the Day RCT,120
falls requiring medical
treatment (7-9% of all falls) were shown to be less for the group receiving versus not receiving
vision screening (RR, 0.65; 95% CI, 0.46 to 0.91 and IRR, 0.65; 96% CI, 0.44 to 0.97).
Vision-Related Quality of Life or Functioning
Smeeth et al.106
conducted a sub-study (n=4,340) within a larger (n=42,319 from 103 general
practices) Medical Research Council (MRC) cluster-RCT in the United Kingdom,121
with
random sampling of 10 practices within each group to which they offered to assess vision-related
functioning and visual acuity at a median of 3.9 years follow up. Screening in this study
consisted of measuring distance visual acuity with pinhole correction; referrals were provided to
ophthalmologists (no pinhole/refractive correction) or optometrists (pinhole correction). After
high attrition (37.4% in those still alive), the 25-item version of the National Eye Institute’s
Visual Function Questionnaire (NEI-VFQ-25; 0-100 range with higher scores better and an MID
of 4-6 points75
) was completed by 1,807 patients and showed no significant difference between
groups (MD, 0.04 points; 95% CI, -1.7 to 2.5).
Impaired Visual Acuity
Four trials104,113,117,118
using objective screening methods reported on mean change in,104,113,118
or
final,117
distance visual acuity in logMAR units across all participants at follow-ups between 10
weeks104
and 18 months113
(median 12 months). Three trials104,113,117
only reported p values for
between-group change values, therefore 95% CIs and SDs were approximated using this data.
The first author of one trial118
provided individual patient data, so we calculated mean and
variance measures for each group; we used results for this study’s two intervention groups
offering referrals (extensive) or brief advice/counselling (minimal) based on findings on vision
from their Physiological Profile Assessment.119
Meta-analysis found no significant difference
between screening versus no screening (MD, -0.01 logMAR; 95% CI, -0.05 to 0.03) (Figure 3).
Negative values represent improvement, and our MID for this outcome was 0.1 logMAR (5
letters or 1 line in the logMAR charts). Post-hoc subgroup analysis comparing results from trials
having an isolated vision screening component (Day 2002 and Tay 2006) with those where
vision was screened within a multicomponent intervention (Lord 2005 and Haanes 2015) did not
reduce the heterogeneity or result in a statistically significant test for subgroup differences
(p=0.70).
Figure 3. Visual Acuity (logMAR)
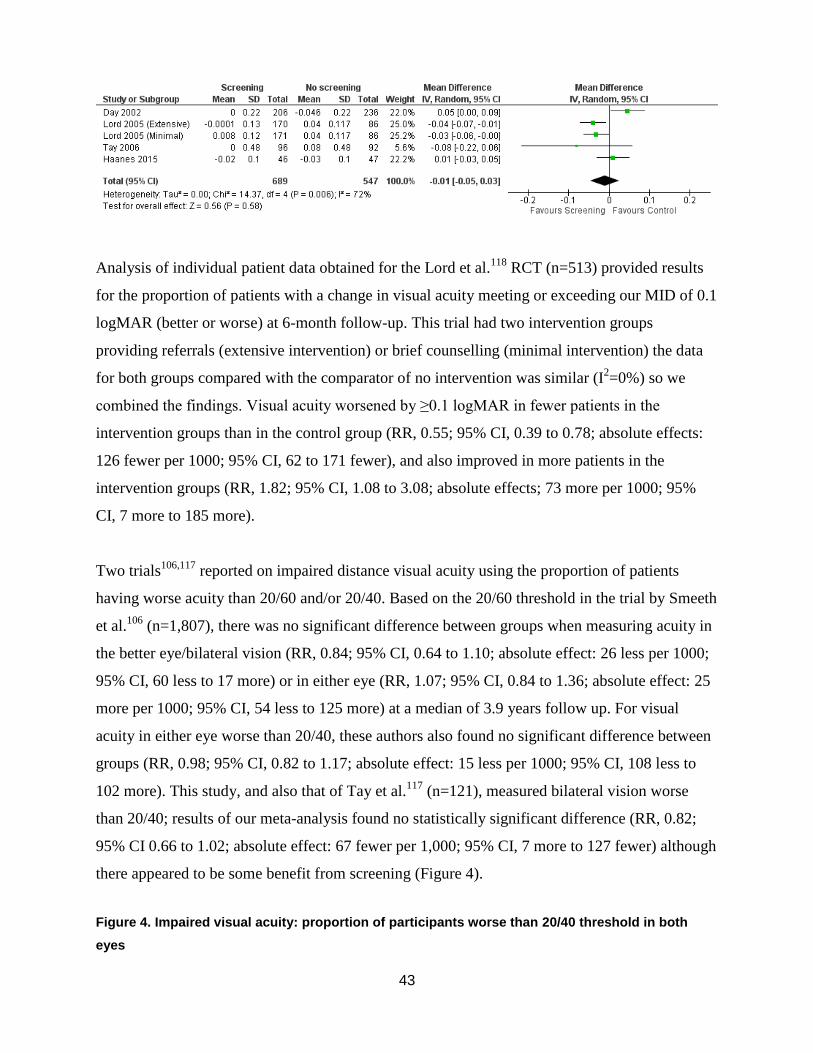
43
Analysis of individual patient data obtained for the Lord et al.118
RCT (n=513) provided results
for the proportion of patients with a change in visual acuity meeting or exceeding our MID of 0.1
logMAR (better or worse) at 6-month follow-up. This trial had two intervention groups
providing referrals (extensive intervention) or brief counselling (minimal intervention) the data
for both groups compared with the comparator of no intervention was similar (I2=0%) so we
combined the findings. Visual acuity worsened by ≥0.1 logMAR in fewer patients in the
intervention groups than in the control group (RR, 0.55; 95% CI, 0.39 to 0.78; absolute effects:
126 fewer per 1000; 95% CI, 62 to 171 fewer), and also improved in more patients in the
intervention groups (RR, 1.82; 95% CI, 1.08 to 3.08; absolute effects; 73 more per 1000; 95%
CI, 7 more to 185 more).
Two trials106,117
reported on impaired distance visual acuity using the proportion of patients
having worse acuity than 20/60 and/or 20/40. Based on the 20/60 threshold in the trial by Smeeth
et al.106
(n=1,807), there was no significant difference between groups when measuring acuity in
the better eye/bilateral vision (RR, 0.84; 95% CI, 0.64 to 1.10; absolute effect: 26 less per 1000;
95% CI, 60 less to 17 more) or in either eye (RR, 1.07; 95% CI, 0.84 to 1.36; absolute effect: 25
more per 1000; 95% CI, 54 less to 125 more) at a median of 3.9 years follow up. For visual
acuity in either eye worse than 20/40, these authors also found no significant difference between
groups (RR, 0.98; 95% CI, 0.82 to 1.17; absolute effect: 15 less per 1000; 95% CI, 108 less to
102 more). This study, and also that of Tay et al.117
(n=121), measured bilateral vision worse
than 20/40; results of our meta-analysis found no statistically significant difference (RR, 0.82;
95% CI 0.66 to 1.02; absolute effect: 67 fewer per 1,000; 95% CI, 7 more to 127 fewer) although
there appeared to be some benefit from screening (Figure 4).
Figure 4. Impaired visual acuity: proportion of participants worse than 20/40 threshold in both
eyes

44
Self-Reported Vision
The vision screening in the majority of the trials (n=10) consisted of a self-reported measure of
either general vision (e.g., very good or good vs. fair to poor or blind) or difficulties in one or
more tasks related to visual acuity (e.g., reading newspaper at 40 cm) and/or other vision
functioning (e.g., seeing objects in dim lighting); participants were instructed to answer
questions in relation to problems when wearing usual spectacles. This outcome deviates from our
planned outcomes of either self-reported vison-related functioning/quality of life, or visual
acuity. The questions covered some but not all of those validated together to reflect vision-
related functioning and quality of life (as would the VFQ-25 for an example); moreover, the
questions used have been shown to have low-to-moderate (0.19 to 0.57) correlation with
impaired visual acuity1,122
and thus fairly poor sensitivity for this outcome.30,89
We combined all
outcomes together because of uncertainty on how patients interpret these questions, what other
factors apart from visual function may contribute to the results (e.g., sociodemographic variables,
depressed mood, and impaired cognitive function),123,124
and whether there would be any reliable
way to differentiate between these different questions in terms of their impact on patients. Even
though difficult to accurately interpret, we did agree with others122,123
that self-reported vision
can complement more objective measures of visual acuity and has been used to measure the
impact of visual impairment on health and physical function.5,6,8,12
Our meta-analysis of all 10 trials (n=8,683) found no significant difference in self-reported
vision from screening using self-reported tools compared with usual care over a median duration
of 20 months (RR, 0.97; 95% CI, 0.90 to 1.05; I2=29%; absolute effect based on median control
event rate of 31%: 9 fewer per 1,000; 95% CI, 16 more to 31 fewer) (Figure 5). Examination of
the funnel plot and use of Egger’s test (p=0.35) did not suggest any small study bias.
Figure 5. Self-reported vision problems: all studies
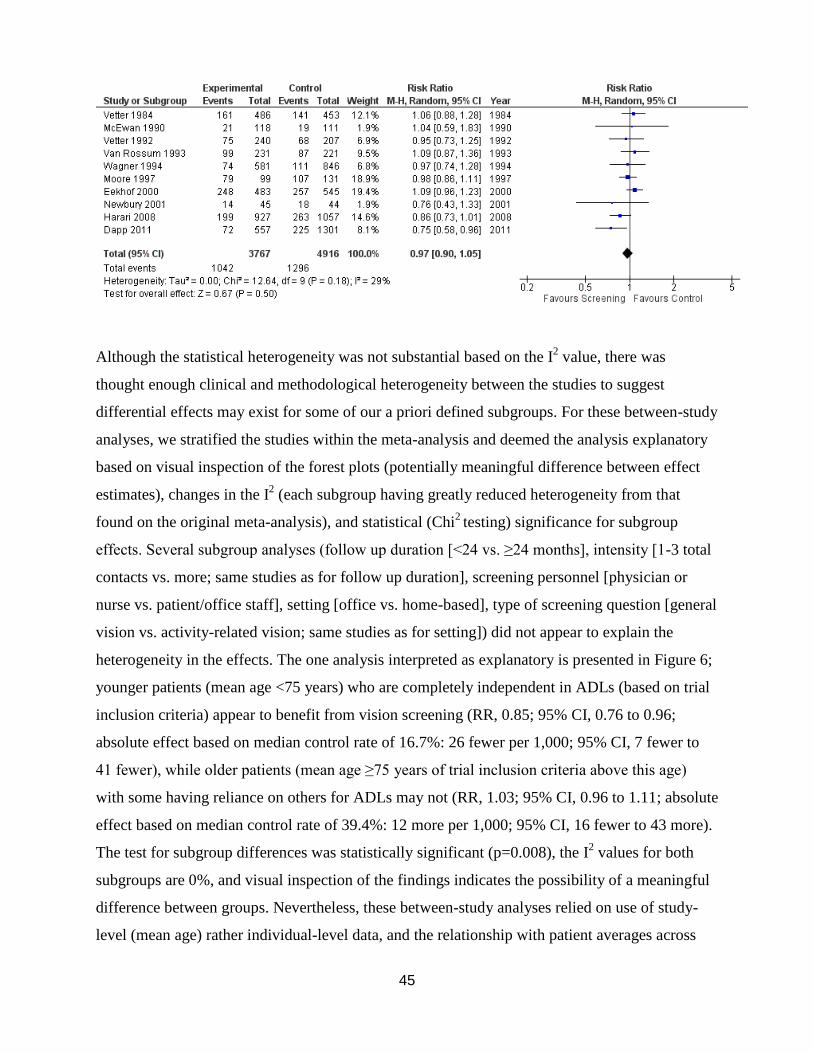
45
Although the statistical heterogeneity was not substantial based on the I2 value, there was
thought enough clinical and methodological heterogeneity between the studies to suggest
differential effects may exist for some of our a priori defined subgroups. For these between-study
analyses, we stratified the studies within the meta-analysis and deemed the analysis explanatory
based on visual inspection of the forest plots (potentially meaningful difference between effect
estimates), changes in the I2 (each subgroup having greatly reduced heterogeneity from that
found on the original meta-analysis), and statistical (Chi2 testing) significance for subgroup
effects. Several subgroup analyses (follow up duration [<24 vs. ≥24 months], intensity [1-3 total
contacts vs. more; same studies as for follow up duration], screening personnel [physician or
nurse vs. patient/office staff], setting [office vs. home-based], type of screening question [general
vision vs. activity-related vision; same studies as for setting]) did not appear to explain the
heterogeneity in the effects. The one analysis interpreted as explanatory is presented in Figure 6;
younger patients (mean age <75 years) who are completely independent in ADLs (based on trial
inclusion criteria) appear to benefit from vision screening (RR, 0.85; 95% CI, 0.76 to 0.96;
absolute effect based on median control rate of 16.7%: 26 fewer per 1,000; 95% CI, 7 fewer to
41 fewer), while older patients (mean age ≥75 years of trial inclusion criteria above this age)
with some having reliance on others for ADLs may not (RR, 1.03; 95% CI, 0.96 to 1.11; absolute
effect based on median control rate of 39.4%: 12 more per 1,000; 95% CI, 16 fewer to 43 more).
The test for subgroup differences was statistically significant (p=0.008), the I2 values for both
subgroups are 0%, and visual inspection of the findings indicates the possibility of a meaningful
difference between groups. Nevertheless, these between-study analyses relied on use of study-
level (mean age) rather individual-level data, and the relationship with patient averages across
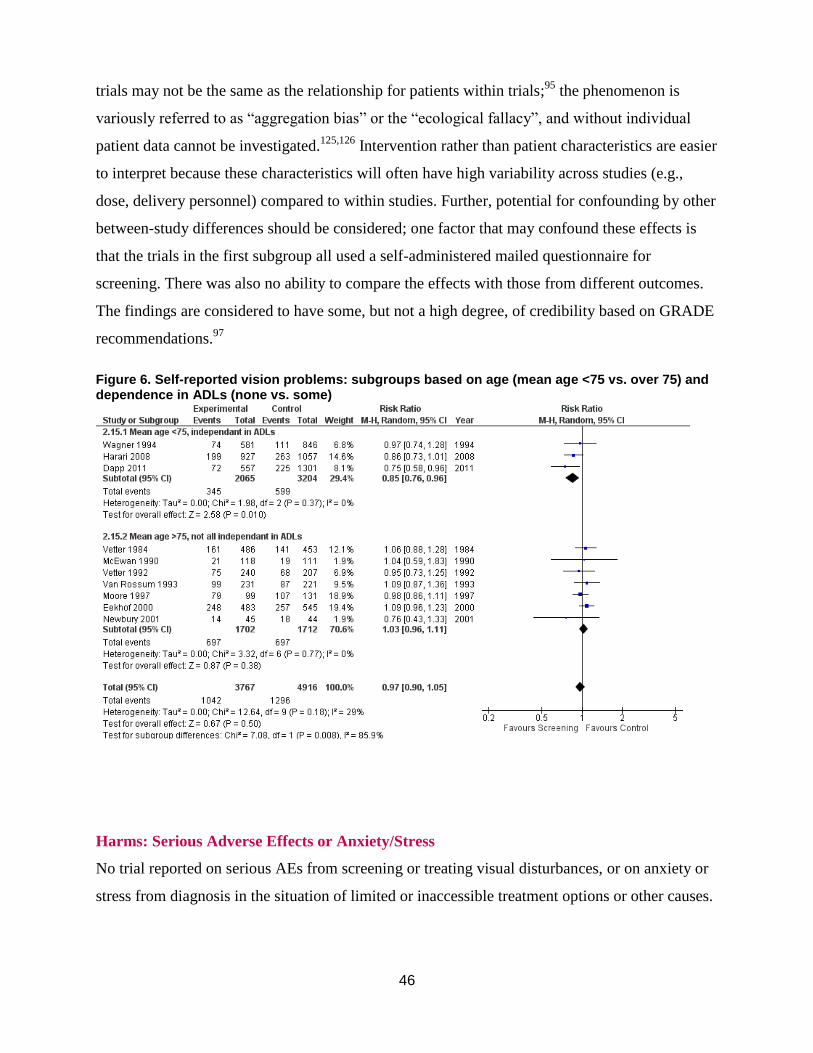
46
trials may not be the same as the relationship for patients within trials;95
the phenomenon is
variously referred to as “aggregation bias” or the “ecological fallacy”, and without individual
patient data cannot be investigated.125,126
Intervention rather than patient characteristics are easier
to interpret because these characteristics will often have high variability across studies (e.g.,
dose, delivery personnel) compared to within studies. Further, potential for confounding by other
between-study differences should be considered; one factor that may confound these effects is
that the trials in the first subgroup all used a self-administered mailed questionnaire for
screening. There was also no ability to compare the effects with those from different outcomes.
The findings are considered to have some, but not a high degree, of credibility based on GRADE
recommendations.97
Figure 6. Self-reported vision problems: subgroups based on age (mean age <75 vs. over 75) and dependence in ADLs (none vs. some)
Harms: Serious Adverse Effects or Anxiety/Stress
No trial reported on serious AEs from screening or treating visual disturbances, or on anxiety or
stress from diagnosis in the situation of limited or inaccessible treatment options or other causes.

47
Implementation Factors
Several studies reported on one or more of our outcomes related to implementation of screening
programs; these outcomes might also reflect the utility of screening for changing clinical
management and behaviors of patients. Two trials112,116
reported on eye professional visits for
both the intervention and control groups over 12 months. Our meta-analysis shown in Figure 7
for this outcome found no significant difference between groups (RR, 1.01; 95% CI, 0.95 to
1.08; RR > 1.0 favoring screening). The finding seems to contradict the one favoring screening
for self-reported vision problems found within the subgroup including these studies, of relatively
younger patients having dependence in their ADLs (Figure 6).
Figure 7. Eye professional visits over 12 months during trial
Seven104-106,110,113,114,117
other trials reported on the proportion of patients screened positive for
vision problems that actually received referrals to eye professionals and/or their physician (left
columns in Table 3). Fewer than half (median 35%) of patients were referred although the range
of 29 to 95% is large. Reflecting that many of the trials are comparing screening to usual care
which may include screening, having data on the control group would have been informative.
For example, Moore et al.114
noted that 17 of 20 eligible people in their control group received
referrals. In total for all participants receiving screening in these seven trials (n=3,225) there
were 574 referrals provided (18% of those screened). Reasons provided by several trial authors
were mostly related to these patients reporting care by eye professionals.
Five trials104-106,113,117
reported on referral uptake for those provided with referrals to see an eye
professional (right column in Table 3). The uptake was moderate (median 68%; range 18 to
96%). Not reported in Table 3, one additional trial reported moderate compliance (68%) to one
of multiple recommendations (visit eye professional, wear hat/sunglasses in high-glare situations,
turn light on at night).118
For all participants screened in these five trials (n = 3,063), 231 patients
(7.5%) likely received further assessment for their vision via referrals. This number may not,

48
though, represent those getting treatment; for example, in the Day trial113
only 26 of 101 (26%)
complying with referrals received treatment (20 new glasses and 6 surgeries); of the overall
population getting screened (n=543) only 5% received treatment. Similarly, in the Smeeth trial106
34 of 1,565 getting vision assessed (2%) received new glasses (n=18) or cataract surgery (n=16).
Table 3. Referrals provided to patients screening positive (left) uptake of referralsprovided (right)
Study Referrals Number
Screened
positive
% Study Uptake Referrals %
Moore 1997 19 20 95% Moore 1997 NR
Eekhof 2000 79 268 29% Eekhof 2000 33 79 42%
Newbury 2001 8 24 33% Newbury
2001
NR
Day 2002 101 287 35% Day 2002 97 101 96%
Smeeth 2003 299 451 66% Smeeth 2003* 68 115 59%
Tay 2006 57 96 59% Tay 2006* 31 36 86%
Haanes 2015 11 38 29% Haanes 2015 2 11 18%
Total
(N=3,225 in
intervention
groups)
574 1184 Median
35%,
Range
29-95%
Total
(N=3,063 in
intervention
groups)
231 342 Mean
68%,
Range
18-96%
*Data on uptake of referrals was not available for all patients receiving referrals.
Within-study Subgroup Analyses
We collected data from study reports on any within-study analyses conducted evaluating the
possibility of differential effects for subgroups on patient and intervention characteristics.
Smeeth et al.106
reported that the effects on impaired visual acuity (<20/60 and <20/40) or vision-
related functioning in their participants aged 75 years and older were not significantly different
after adjustment for age, sex, level of self-reported visual difficulty at baseline, and time until
follow up. Stratification by age, sex, level of self-reported visual difficulty at baseline, social
isolation, or time until follow up also produced no evidence of subgroup effects. These authors
also found that people with worse vision were more likely to be referred, and that people with
evidence of cognitive impairment at the time of screening were less likely to be referred. Our
own between-study subgroup analyses are discussed within the main findings above for self-
reported vision problems, which was the only outcome for which we examined any effects. Our
findings suggest that vision screening using self-reported, but not validated tools, tools may be
49
more beneficial for relatively younger (<75 years) and independent older adults, than for those
over 75 requiring some assistance; we interpret these with caution because this form of analysis
is exploratory and may be confounded by other variables differing between studies.
Key Questions 2-4
This review followed a staged approach based on the quality of the body of evidence (using
GRADE assessments) and the information needs of the CTFPHC for making a recommendation
on this topic. The CTFPHC has found that the evidence from KQ1 does not indicate a favorable
benefit-harm ratio across outcomes, therefore we have not examined the cost-effectiveness
(KQ3; requiring certainty in favorable benefit-harm ratio) of screening programs. Older adults’
valuation of benefit and harm outcomes (KQ2) has not been examined either because there was
not considerable uncertainty in the balance of benefits and harms as judged by the CTFPHC.
Adding findings from evidence on accuracy of screening tests (KQ4), as indirect evidence on the
clinical effects of screening for vision would not improve the certainty enough to change the
strength or direction of a recommendation.
Quality of Evidence
Our GRADE Summary of Findings and Evidence Profile tables at the end of this report include
all findings discussed in more detail above as well as our GRADE assessments on the quality of
the body of evidence for each outcome; the reasons for each GRADE decision are included in the
table footnotes. The GRADE assessments form the basis of our conclusions on the current
evidence base for each outcome, which are summarized in the discussion below.
50
Section V. Discussion
We reviewed the evidence from 15 RCTs examining the effects of screening for vision—mostly
within multicomponent screening/assessments—compared with no screening or usual care, for
community-dwelling older adults (≥65 years) within settings applicable to primary health care.
Summary of Findings and Quality of Evidence
In this section we briefly summarize the evidence for each outcome, and provide our
interpretations for each based on our GRADE assessments (ES 1 GRADE Summary of Findings
table).
Mainly because the outcomes of mortality and loss of independence could not be attributed
specifically to the vision component of multicomponent interventions, no trial provided evidence
for these outcomes. No trial reported any harm that could be attributed to vision screening. Given
the small number—5 to 10% at most suggested using the findings on implementation factors—of
patients that appear to have received any treatment by eye care professionals during follow up,
the number of serious AEs from treatment, if reported, would likely have been very small; in this
case very large screening studies would be necessary to provide precise findings for these
outcomes. Moreover, other harms relevant to screening interventions (e.g., resulting from
unnecessary interventions from false-positives) would be minimal in this situation where any
invasive procedures would be undertaken after diagnosis.
Two trials (n=1,180) reported on a surrogate outcome (falls and falls requiring medical
treatment) for fractures that were attributed to vision screening over follow-up durations of 12 to
18 months. The quality of evidence for the outcome of fractures was assessed by GRADE
methods as very low, and therefore we are very uncertain about the effects of screening with
multiple vision tests on fractures over medium-term follow-up.
With low quality evidence from one RCT (n=1,807), screening with objective tools of visual
acuity may make little to no difference in vision-related functioning over long-term follow-up
51
(NEI-VFQ-25, range 0-100; MID 4-6 points; MD, 0.4 units higher for universal screening; 95%
CI, -1.25 to 2.05 units).
Screening with multiple objective vision tests probably makes little to no difference in high-
contrast, distance visual acuity for older adults over medium-term follow-up (4 RCTs; n=1,236;
MD, -0.01 logMAR; 95% CI, -0.05 to 0.03). One RCT (n=519) found that screening with
multiple objective vision tests may reduce the proportion of patients having their high-contrast,
distance visual acuity worsen (RR 0.55, 95% CI 0.39 to 0.78; absolute effect, 126 fewer per
1000; 95% CI, 62 to 171 fewer) and/or improve (RR, 1.82; 95% CI, 1.08 to 3.08; absolute effect,
73 more per 1000; 95% CI, 7 more to 185 more) by a marginal degree (MID 0.1 logMAR) over
medium-term follow-up. We are very uncertain about the effects of screening using tests of
visual acuity on the proportion having impaired visual acuity worse than 20/60 in both eyes or in
either eye after long-term follow-up (1 RCT; n=1,807). Screening with objective tools appears to
make little to no difference for bilateral impaired visual acuity (proportion with worse than
20/40) over medium-to-long term follow-up (2 RCTs; n=1,967; RR, 0.82; 95% CI, 0.66 to 1.02;
absolute effects, 67 fewer per 1,000; 95% CI, 7 more to 127 fewer), although results indicated
benefit may occur for some. It may make little or no difference for impaired visual acuity
(proportion with worse than 20/40) in either eye over long-term follow up (1 RCT; n=1,807; RR,
0.98; 95% CI, 0.82 to 1.17; absolute effect, 15 less per 1000; 95% CI, 108 less to 102 more).
Moderate quality evidence from 10 RCTs (n=8,683) comparing self-reported screening with
usual care found no significant difference for self-reported vision problems (RR, 0.97; 95% CI,
0.90 to 1.05; absolute effect, 9 fewer per 1,000; 95% CI, 16 more to 31 fewer) over a median
follow-up of 20 months. Most of our planned subgroup analyses—follow-up duration, screening
personnel, setting, and type of screening question—did not appear to explain the heterogeneity in
the effects. Based on our criteria, the analysis deemed most explanatory compared studies of
relatively younger patients (mean age <75 years) who were completely independent in ADLs (3
RCTs; n=5,269) with those of older patients (e.g., recruitment of 75 and older) with at least some
relying on others for ADLs (7 RCTs; n=3,414) (RR, 0.85; 95% CI, 0.76 to 0.96 vs. RR, 1.03;
95% CI, 0.96 to 1.11, respectively; p=0.008 between groups, I2=0% for both; possibly
meaningful difference between effect sizes). The results are observational in nature, and the

52
potential for confounding by other between-study differences should be considered. Further
research is warranted to explore this finding.
The lack of impact found by the investigators of these trials might be attributed in part by limited
follow-up for screen-positive patients; only about a third (median 35%) of patients screening
positive were referred to eye professionals—most of the remaining (65%) screen-positives were
not provided referrals because of report of current care by eye professionals—and uptake of
referrals by patients who were provided them was moderate (median 68%) and might not
represent those receiving treatments (e.g., ≤5% of those screened in two RCTs received
treatment).
Findings in Comparison with Other Systematic Reviews
Three other systematic reviews specific to vision43,89,103
warrant comparison with ours in terms
of their scope and findings. The use of questions about visual problems as a screening tool and
the lack of clear plans of intervention for those people found to have a visual problem were
proposed as explanations for the lack of effectiveness of screening for visual impairment (within
multicomponent interventions) in community settings found in a 1998 systematic review of
RCTs107-109,111,115
by Smeeth and Iliffe.127
A 2006 update of this review, including findings from
an RCT (using objective screening tests and planned follow up for the vision component) led by
one of the review authors,106
found similar effects of no significant difference when considering
self-reported vision problems, vision-related functioning, and impaired visual acuity. The authors
comment that although an isolated vision screening intervention may produce greater effects, the
likelihood of this occurring in clinical practice is small which limits the pragmatic aspects of
such a trial. Findings of no difference from vision screening from the two RCTs113,117
we
included that isolated a vision intervention would not support this view (Figure 5). When
considering other reasons for no effect on impaired visual acuity, these authors also comment on
how among those (around half) who attended an ophthalmologist following screening but had no
improvement in visual acuity there could have possibly been benefit in terms of function and
quality of life from interventions for low vision that would not be expected to improve visual
acuity.89
However, the result for visual function (NEI-VFQ-25) in their RCT106
did not differ in
the two trial arms either.

53
A more recent systematic review by Chou and colleagues43
also found no significant difference
from screening for vision problems based on three RCTs105,106,114
where screening mainly took
place in physician offices (included the Smeeth trial where >30% of screening took place in
participant homes, but excluded [based on 2009 report] another trial undertaken in a clinic115
).
This review differs from ours in that the CTFPHC considered home and other community
settings as relevant to primary care; we considered that multiple settings could provide relevant
findings so long as eye professionals were not undertaking screening, populations met inclusion
criteria for this review, and the screening approach was considered feasible for primary care
settings. We are not sure on the reason that we included some studies (e.g., Harari and Dapp
RCTs in physician offices) not reviewed by Chou et al.; these trials are not located in their
excluded studies lists, which could indicate that their search strategy (focusing on vision
screening) was not as sensitive as ours (including multiple terms for multicomponent/falls
risk/geriatric assessments) to capture studies where vision was screened within broader health
risk assessments. Chou et al. also undertook additional reviews on the indirect evidence on
accuracy of screening tests and of benefits and harms from treatment (compared with placebo,
sham, or no treatment). The authors concluded that (i) screening questions or a questionnaire are
inaccurate compared to a visual acuity test (e.g., the Snellen eye chart) and (ii) visual acuity tests
have suboptimal (and variable) accuracy compared to a comprehensive ophthalmological
examination. Although using the Snellen chart as a reference standard may be viewed by some as
problematic, this first finding aligns well with other reports1,122
finding a moderate (at best)
correlation between self-reported vision and visual acuity; self-report may correlate better with
other visual functions or conditions, and/or be confounded by factors unspecific to vision. The
finding that a visual acuity test had less accuracy for detecting visual conditions compared with a
comprehensive eye examination was not surprising because of unclear clinical significance of
testing visual acuity for some visual conditions. Chou et al. also comment on one trial128
(n=616;
not meeting their inclusion criteria) that reported an increased risk of falls and a trend toward
increased risk of fractures (18 control events) among frail older adults who underwent vision
assessment by an optometrist versus usual care; this finding contrasts with that of a meta-analysis
including this trial by Zhang at el.103
finding a reduction in the incidence of falls (OR, 0.39; 95%
CI, 0.07 to 0.70) in four trials of vision interventions (including referrals and first cataract
surgery) versus no intervention. This review by Zhang et al focusing on vision interventions and

54
falls included two of the same studies as ours (focused on screening but not by
optomtetrists),113,118
but also others that directly provided vision treatments in high-risk
populations (residential care) or people with known vision conditions.
Limitations of Evidence Base
The evidence base did not allow for findings on mortality or loss of independence because of
either the inability to attribute causation on these health outcomes from changes in vision (within
13 multicomponent interventions), or because of lack of reporting by arm in the two trials with
an isolated vision component. Less confounding was apparent in two trials that we used for
indirect evidence on fractures. Nevertheless, although many factors will contribute to risk for
loss of independence or fractures, impaired vision is arguably an important risk factor which also
contributes to several better recognized risks.129,130
It is unclear to what extent our outcomes of
impaired visual acuity and self-reported vision problems would capture the possible benefits
from vision screening. Although impaired visual acuity correlates with visual functioning and
quality of life, other aspects of vision including visual cognition (visual attention, processing)
may be important, yet under-investigated, such that optimal screening in primary care settings
could be difficult without integrating multidisciplinary approaches.130
Self-reported vision has
been associated with health and functioning,5,6,8,12
and this outcome may complement those from
tests on visual acuity when determining the overall effects of vision interventions;122
one should
likely bear in mind, though, that there is uncertainty about the direction (or existence) of a casual
association of impaired vision with some outcomes including mental health (depression)3 and
cognitive impairment. Similar pathological mechanisms seem to exist for visual conditions (e.g.,
AMD) and cognitive impairment (indicating comorbidity), yet impaired vison may also reduce
the quality of interactive experiences of older adults and thus ultimately negatively affect
physical, mental, and psychosocial behaviours.131
The quality of evidence was limited for all outcomes by potential biases threatening internal
validity, mainly from lack of blinding patients, personnel and outcome assessors (especially for
self-reported outcomes) or by high attrition, even after deaths were considered. For most
outcomes, we considered the evidence reasonably applicable to our PICOTs so did not
downgrade the evidence for indirectness; the outcomes of fractures (using surrogate outcome of
55
falls) and visual acuity (mean change) were the only ones downgraded for this GRADE domain.
For visual acuity this downgrading was because of two studies enrolling only patients that were
considered at higher-risk than the average population in primary care,104,117
and one of these also
providing an intervention (home lighting modification) thought to possibly confound results for a
vision outcome. Although we did not downgrade other outcomes for indirectness, there is
concern about the applicability of the results to the current Canadian primary health care system
where better follow-up to screening may occur; this may particularly relate to locations where
there are active programs for integrated primary health care or linkages with multidisciplinary
vision rehabilitation for seniors, and/or situations when possible barriers such as cost of
prescription glasses or devices are minimal for the patient because of private insurance or other
assistance programs. Moreover, the positive effects on self-reported vision found in the studies
of Dapp et al.112
and Harari et al.116
resulted from a system where electronic health records and
“problem area” notifications were integrated, which is not standard practice at this time in
Canada.
Interpretation of the effects may need to consider that the subjective outcome of self-reported
vision was reported by studies using self-reported screening, and the objective outcomes where
visual acuity was measured can be attributed to screening with similar tests; similar findings of
little to no effect across most outcomes appears to allow for similar interpretations between
screening methods. For self-reported vision, although several trials included assessment of
factors that could theoretically impact vision if treated (e.g., medication review, nutrition
assessment) we are making the assumption that the vision screening would have been the largest
contributor to any beneficial effect. Any exaggeration in effect may have been offset by findings
that people may not self-report vision problems (and hence receive any follow-up) despite
having a reduced visual acuity as shown through objective means.15
Precise and consistent
findings of little or no difference for this outcome do not suggest substantial confounding existed
by either factor.
There should be some consideration that the trials in practice did not focus only on patients with
unrecognized vision problems (i.e., they recruited patients who reported having an eye care
provider as well as those who did not). It is likely that excluding patients who were already
receiving eye care would change the baseline rate of impaired vision in the group of trial
56
participants, thus probably increasing the proportion of participants in a position to benefit from
screening. Conversely, patients who do not already have an eye care provider may be less likely,
on average, to follow through with referral recommendations following a positive screening test.
These factors could mean that the absolute (and possibly relative) effects of the same screening
intervention, in patients with unrecognized vision problems, might be different from that
observed in the more mixed group of participants. Moreover, the results as they are reported
here, though, may best represent a typical primary care setting where a vision screen may be
given to all patients. In 10 of the trials the control group patients received some form of vision
assessment, and may have also received referrals to eye professionals as part of usual care;
results across many outcomes may underestimate what may occur should a practitioner newly
initiate screening and referrals into practice. There is a possibility that the findings would have
been different should we have received data for two trials without records available as per author
contact, or if authors of some trials had data from vision outcomes despite no indication of this in
the reporting (and therefore excluded based on insufficient reporting to prompt author contact).
Limitations in Evidence Synthesis
This review followed rigorous methodological standards, which were detailed a priori in a
protocol. Nevertheless, several limitations are inherent within systematic reviews in general.
There is a possibility of selective reporting bias (e.g., researchers only reporting positive
outcomes) and small study bias (including publication bias), whereby small trials are only
published when unexpectedly strong results are found. In terms of selective outcome reporting,
the findings of no effect reported by many studies of differing sizes, and our successful contacts
with several authors to confirm or obtain data helped minimize this effect. Our pre-specified tests
for publication bias (small study effects) indicated no bias for the outcome of self-reported
vision, the only outcome reported by eight or more studies. Moreover, vision outcomes were not
the primary outcomes reported by studies, which would reduce their likelihood of leading to
publication bias. We focused on studies published in English or French, and trials published in
other languages may have differing results; effect sizes in language restricted reviews have
shown to not differ significantly (overestimating effect sizes by 2%) from those not having
restrictions.132
We based our assessments of the risk of bias on study publications and did not
contact authors to verify the methods used. Some studies may have been adequately conducted,

57
but the methods were poorly reported. Our findings for the planned subgroup variables are based
on study-level data (e.g., average patient age) and should be considered observational in nature
and thus of low quality especially for the magnitude of difference in effect. Discussion on
interpreting subgroup analyses with caution is included in the results section; further research
would be required to further examine this finding. Systematic reviews may become outdated, at
least in part, if new studies are published that change some or all of their conclusions. This
review should be revisited should new studies become available that appear to indicate a
different quality of evidence particularly with respect to harms or the outcomes of fractures or
loss of independence.
Conclusions
Evidence was either not found or of low quality for most outcomes considered most critical for
decision making by the CTFPHC for screening for impaired visual acuity or vision-related
functional limitations for older, community-dwelling adults in primary health care settings. No
study contributed findings for mortality, loss of independence, or harms specific to vision
screening; the quality of evidence available for the outcome of fractures was very low such that
we cannot make any conclusions on the effects. Screening probably makes little to no difference
for mean distance visual acuity over medium-term follow-up across populations of older adults.
It also may make little to no difference for vision-related functional limitations and we are not
certain about the effects on the number of patients with impaired visual acuity meeting clinically
relevant thresholds (e.g., worse than 20/60). Low quality evidence found that there may be some
benefit in the number of patients having their vision worsen or improve by a marginal degree
(0.1 logMAR=5 letters). For an added outcome of self-reported vision problems, screening
probably makes little to no difference; studies where the average patient age was relatively
younger (< 75 years) and all patients were independent in ADLs at baseline showed a greater
effect for this outcome than those of older patients with at least some requiring assistance with
ADLs, although other confounding factors may exist between these groups of studies and the
findings are considered exploratory and in need of further research. The results of largely no
effect across outcomes could relate in part to a fairly low referral rate by clinicians for those
patients screening positive (due to reports of regular eye care), moderate uptake of referrals by
patients, and low numbers of patients receiving treatments. Findings are most applicable to

58
screening all older adults in primary care, and not for those seeking and receiving care by eye
professionals or other providers working in visual rehabilitation settings where comprehensive
assessments and treatment/services would be directly provided.

59
ES 1. Grade Summary of Findings Table and Evidence Profile for KQ1
Vision screening compared to no vision screening/usual care in adults ≥65 in primary care
Patient or population: adults ≥ 65 years of age, with undetected impaired visual acuity or vision-related functional limitations
Setting: primary care
Intervention: vision screening
Comparison: no vision screening or usual care
Outcomes Anticipated absolute effects* (95% CI) Relative effect (95% CI)
№ of participants (studies)
Quality of the evidence (GRADE)
Comments
Risk with no vision screening/usual care
Risk with vision screening
Mortality
- - 0 studies reported on this
outcome in a manner that
was attributable to vision
screening.
Potential adverse
consequences of
poor vision
(fractures)
Assessed with self-
report logs with
follow up
Follow up range 12
months to 18
months
Day 2002:
Falls requiring medical treatment:
IG 49/547 vs CG 75/543
48 fewer per 1000 (12 to 75 fewer)
Any fall:
IG 691/547 vs CG 757/543;
163 fewer per 1000 (28 to 292 fewer)
Newberry 2001:
Any fall:
IG 4/45 vs. CG 3/44 20 more per 1000 (48 less to 305 more)
Day 2002:
Requiring medical treatment RR 0.65 (0.46 to
0.91); IRR 0.65;
95% CI 0.44 to
0.97
Any fall RR, 0.88; 95%
CI, 0.79 to 0.98);
IRR, 0.91; 95%
CI, 0.82 to 1.16
Newberry 2001:
Any fall RR 1.30 (0.31 to 5.49)
1180
(2 RCTs)110,113 ⨁◯◯◯
VERY LOW
We are very uncertain about the effects of screening with multiple vision tests on fractures over medium-term
follow-up.a
Potential adverse
consequences of
poor vision (loss
of independence)
- - 0 studies reported on this
outcome in a manner that
was attributable to vision
screening.

60
Vision screening compared to no vision screening/usual care in adults ≥65 in primary care
Patient or population: adults ≥ 65 years of age, with undetected impaired visual acuity or vision-related functional limitations
Setting: primary care
Intervention: vision screening
Comparison: no vision screening or usual care
Outcomes Anticipated absolute effects* (95% CI) Relative effect (95% CI)
№ of participants (studies)
Quality of the evidence (GRADE)
Comments
Risk with no vision screening/usual care
Risk with vision screening
Vision-related
functional
limitations/quality
of life
Assessed with
NEI-VFQ-25
scale from 0 to 100
(higher scores
better)
Follow up median
3.9 years
The mean vision-
related
functioning/quality
of life was 0 Units
The mean vision-related
functioning/quality of life in
the intervention group was
0.4 Units higher (1.25 lower
to 2.05 higher)
- 1807
(1 RCT)106 ⨁⨁◯◯
LOW
Screening with objective
tools of visual acuity may
make little or no difference in
vision-related functioning
over long-term follow-up.b
Impaired visual
acuity (mean change
in high contrast
distance visual
acuity)
Screening with
objective screening;
threshold for
minimally important
difference was 0.1
logMAR, or 5 letters.
Follow up median 12
months.
The mean change in
visual acuity was 0
logMAR
The mean visual
acuity in the
intervention group
was 0.01 logMAR
lower (0.05 lower to
0.03 higher)
1343
(4 RCTs)104,113,117,118
⨁⨁⨁◯
MODERATE
Screening with multiple
objective vision tests
probably makes little to no
difference in high-contrast,
distance visual acuity over
medium-term follow-up.c

61
Vision screening compared to no vision screening/usual care in adults ≥65 in primary care
Patient or population: adults ≥ 65 years of age, with undetected impaired visual acuity or vision-related functional limitations
Setting: primary care
Intervention: vision screening
Comparison: no vision screening or usual care
Outcomes Anticipated absolute effects* (95% CI) Relative effect (95% CI)
№ of participants (studies)
Quality of the evidence (GRADE)
Comments
Risk with no vision screening/usual care
Risk with vision screening
Impaired visual
acuity (≥0.1
logMAR change for
worse or better)
Screening with
objective tools.
Follow up 6
months
Lord 2005:
Worse VA (≥0.1 logMAR):
Lord 2005 (n=519): IG 53/341 vs. CG 50/178
126 fewer per 1000 (62 to 171 fewer)
Better VA (≤ -0.1logMAR):
Lord 2005 (n=519): IG 56/341 vs CG 16/178
73 more per 1000 (7 more to 185 more)
Worse VA:
RR 0.55, 95% CI
0.39 to 0.78
Better VA:
RR 1.82, 95% CI
1.08 to 3.08
519
(1 RCT)118 ⨁⨁◯◯
LOW
Screening with multiple
objective vision tests may
reduce worsening and/or
improve high-contrast,
distance visual acuity over
medium-term follow-up.d
Impaired visual
acuity (<20/60
distance visual
acuity: bilateral or
either eye)
Screening with
objective
screening.
Follow up median
3.9 years.
Smeeth 2003:
Bilateral: IG 114/817 vs. CG 160/962
26 less per 1000 (60 less to 17 more)
Either eye: IG 307/829 vs. CG 339/978
25 more per 1000 (54 less to 125 more)
Bilateral: RR,
0.84 (0.64 to
1.10)
Either eye: RR,
1.07 (0.84 to
1.36)
1807
(1 RCT)106 ⨁◯◯◯
VERY LOW
We are very uncertain about
the effects of screening
using tests of visual acuity
on impaired visual acuity
(worse than 20/60) in both
eyes or in either eye over
long-term follow-up.e
Impaired visual
acuity (<20/40
distance visual
acuity; bilateral)
Screening with
objective
screening.
Follow up range 12
months to 46
months.
374 per 1,000
307 per 1,000
(247 to 381)
RR 0.82
(0.66 to
1.02)
1967
(2 RCTs)106,117 ⨁⨁◯◯
LOW
Screening with objective
tools may make little to no
difference for bilateral
impaired visual acuity (worse
than 20/40) over medium-to-
long term follow-up.f
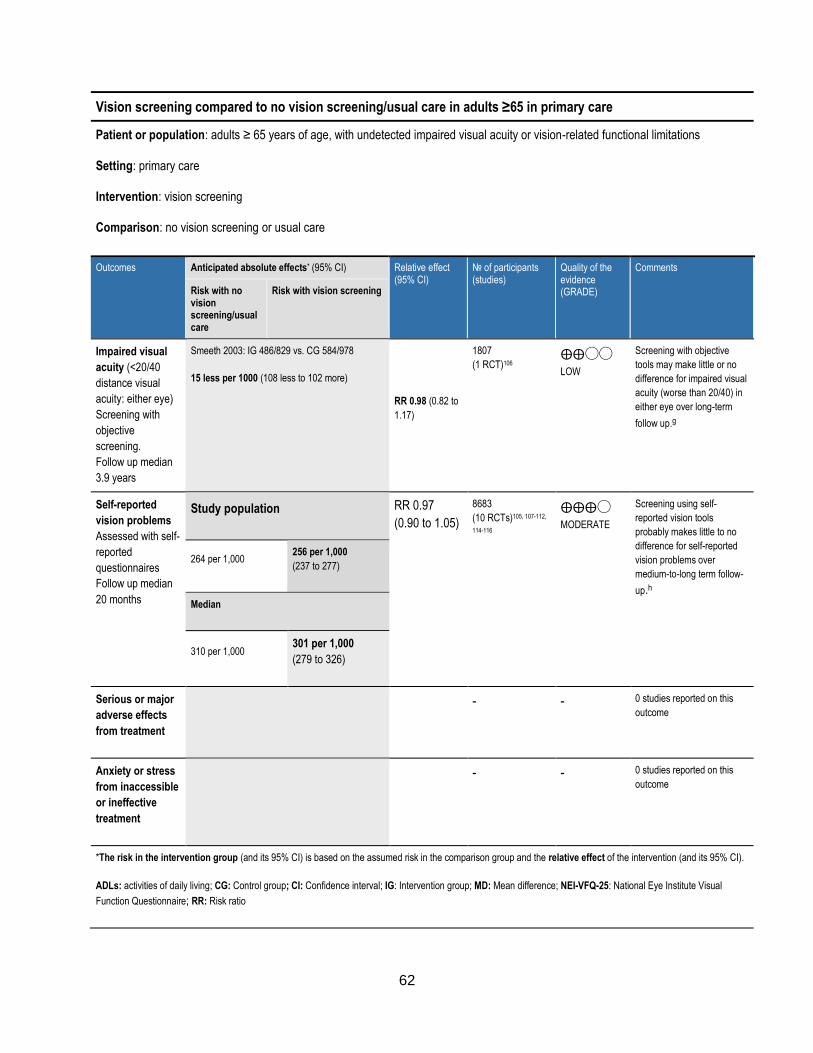
62
Vision screening compared to no vision screening/usual care in adults ≥65 in primary care
Patient or population: adults ≥ 65 years of age, with undetected impaired visual acuity or vision-related functional limitations
Setting: primary care
Intervention: vision screening
Comparison: no vision screening or usual care
Outcomes Anticipated absolute effects* (95% CI) Relative effect (95% CI)
№ of participants (studies)
Quality of the evidence (GRADE)
Comments
Risk with no vision screening/usual care
Risk with vision screening
Impaired visual
acuity (<20/40
distance visual
acuity: either eye)
Screening with
objective
screening.
Follow up median
3.9 years
Smeeth 2003: IG 486/829 vs. CG 584/978
15 less per 1000 (108 less to 102 more)
RR 0.98 (0.82 to
1.17)
1807
(1 RCT)106 ⨁⨁◯◯
LOW
Screening with objective
tools may make little or no
difference for impaired visual
acuity (worse than 20/40) in
either eye over long-term
follow up.g
Self-reported
vision problems
Assessed with self-
reported
questionnaires
Follow up median
20 months
Study population RR 0.97
(0.90 to 1.05)
8683
(10 RCTs)105, 107-112,
114-116
⨁⨁⨁◯
MODERATE
Screening using self-
reported vision tools
probably makes little to no
difference for self-reported
vision problems over
medium-to-long term follow-
up.h
264 per 1,000 256 per 1,000
(237 to 277)
Median
310 per 1,000 301 per 1,000
(279 to 326)
Serious or major
adverse effects
from treatment
- - 0 studies reported on this
outcome
Anxiety or stress
from inaccessible
or ineffective
treatment
- - 0 studies reported on this
outcome
*The risk in the intervention group (and its 95% CI) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI).
ADLs: activities of daily living; CG: Control group; CI: Confidence interval; IG: Intervention group; MD: Mean difference; NEI-VFQ-25: National Eye Institute Visual
Function Questionnaire; RR: Risk ratio
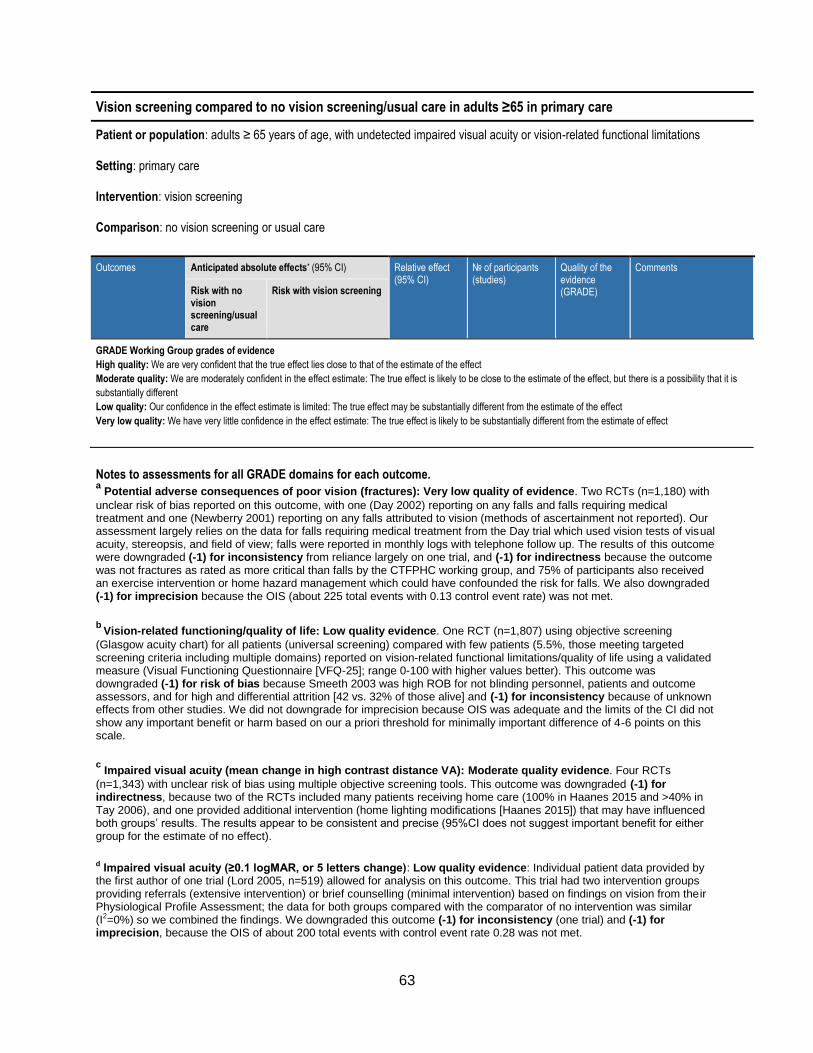
63
Vision screening compared to no vision screening/usual care in adults ≥65 in primary care
Patient or population: adults ≥ 65 years of age, with undetected impaired visual acuity or vision-related functional limitations
Setting: primary care
Intervention: vision screening
Comparison: no vision screening or usual care
Outcomes Anticipated absolute effects* (95% CI) Relative effect (95% CI)
№ of participants (studies)
Quality of the evidence (GRADE)
Comments
Risk with no vision screening/usual care
Risk with vision screening
GRADE Working Group grades of evidence
High quality: We are very confident that the true effect lies close to that of the estimate of the effect
Moderate quality: We are moderately confident in the effect estimate: The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is
substantially different
Low quality: Our confidence in the effect estimate is limited: The true effect may be substantially different from the estimate of the effect
Very low quality: We have very little confidence in the effect estimate: The true effect is likely to be substantially different from the estimate of effect
Notes to assessments for all GRADE domains for each outcome. a Potential adverse consequences of poor vision (fractures): Very low quality of evidence. Two RCTs (n=1,180) with
unclear risk of bias reported on this outcome, with one (Day 2002) reporting on any falls and falls requiring medical treatment and one (Newberry 2001) reporting on any falls attributed to vision (methods of ascertainment not reported). Our assessment largely relies on the data for falls requiring medical treatment from the Day trial which used vision tests of visual acuity, stereopsis, and field of view; falls were reported in monthly logs with telephone follow up. The results of this outcome were downgraded (-1) for inconsistency from reliance largely on one trial, and (-1) for indirectness because the outcome was not fractures as rated as more critical than falls by the CTFPHC working group, and 75% of participants also received an exercise intervention or home hazard management which could have confounded the risk for falls. We also downgraded (-1) for imprecision because the OIS (about 225 total events with 0.13 control event rate) was not met.
b Vision-related functioning/quality of life: Low quality evidence. One RCT (n=1,807) using objective screening
(Glasgow acuity chart) for all patients (universal screening) compared with few patients (5.5%, those meeting targeted screening criteria including multiple domains) reported on vision-related functional limitations/quality of life using a validated measure (Visual Functioning Questionnaire [VFQ-25]; range 0-100 with higher values better). This outcome was downgraded (-1) for risk of bias because Smeeth 2003 was high ROB for not blinding personnel, patients and outcome assessors, and for high and differential attrition [42 vs. 32% of those alive] and (-1) for inconsistency because of unknown effects from other studies. We did not downgrade for imprecision because OIS was adequate and the limits of the CI did not show any important benefit or harm based on our a priori threshold for minimally important difference of 4-6 points on this scale.
c Impaired visual acuity (mean change in high contrast distance VA): Moderate quality evidence. Four RCTs
(n=1,343) with unclear risk of bias using multiple objective screening tools. This outcome was downgraded (-1) for indirectness, because two of the RCTs included many patients receiving home care (100% in Haanes 2015 and >40% in Tay 2006), and one provided additional intervention (home lighting modifications [Haanes 2015]) that may have influenced both groups’ results. The results appear to be consistent and precise (95%CI does not suggest important benefit for either group for the estimate of no effect).
d Impaired visual acuity (≥0.1 logMAR, or 5 letters change): Low quality evidence: Individual patient data provided by the first author of one trial (Lord 2005, n=519) allowed for analysis on this outcome. This trial had two intervention groups providing referrals (extensive intervention) or brief counselling (minimal intervention) based on findings on vision from their Physiological Profile Assessment; the data for both groups compared with the comparator of no intervention was similar (I2=0%) so we combined the findings. We downgraded this outcome (-1) for inconsistency (one trial) and (-1) for imprecision, because the OIS of about 200 total events with control event rate 0.28 was not met.

64
e Impaired visual acuity (<20/60 distance visual acuity: bilateral or either eye): Very low quality evidence. One RCT
(n=1,807) using objective screening for visual acuity (Glasgow acuity logMAR chart) in all (universal group) versus few (5.5%, targeted for multiple risk factors) patients reported on impaired visual acuity (<20/60; <6/18) in both or either eye. We downgraded this outcome (-1) for risk of bias (Smeeth 2003 had no blinding and high and differential attrition), (-1) for inconsistency (one study), and (-1) for imprecision (both estimates met OIS but lower [bilateral] and upper [either eye] boundaries of the CI cross our threshold of RR 0.75 to 1.25).
f Impaired visual acuity (<20/40 distance visual acuity: bilateral): Low quality evidence. Two RCTs (n=1,967) reported
on bilateral impaired visual acuity (worse than 20/40). This outcome was downgraded (-1) for risk of bias (Smeeth 2003 unclear risk for no blinding and high risk for and differential attrition; Tay unclear ROB for all domains except selective outcome reporting) and (-1) for imprecision with OIS met but lower limit of CI (RR 0.66) indicating possible benefit despite estimate of little or no effect. Results are most applicable when screening using one or more objective tests of visual acuity.
g Impaired visual acuity (<20/40 distance visual acuity: either eye): Low quality evidence. One RCT (n=1,807)
reported on impaired visual acuity in either eye (worse than 20/40). This outcome was downgraded (-1) for risk of bias (Smeeth 2003 unclear risk for no blinding and high risk for and differential attrition) and (-1) for inconsistency (one trial). The estimate of little to no difference is precise without indication of important benefit or harm based on our threshold limits of RR 0.75 or 1.25.
h Self-reported vision problems (all studies): Moderate quality evidence. Ten RCTs (n=8,683) using variety of self-reported screening tools, primarily with a question(s) on general vision (4 with single question) but some including multiple questions (4 asking on vision-related activities, and 2 including visual acuity measurement after positive self-report responses). Patients of a variety of ages and risk factors for frailty and/or falls were included but all met our inclusion criteria. Most sensitivity analyses (e.g. setting, screening personnel, duration of follow up) did not alter our overall quality assessment. This outcome was downgraded (-1) for risk of bias (i.e., no blinding of participants or providers in any study, high ROB from attrition in one study [Dapp 2011], and unclear ROB for allocation concealment in Eekhof 2000, McEwan 1990, and Moore 1997). Although there was some inconsistency (2 CIs not overlapping; I2=29%) we did not have serious concerns for this domain. We did not downgrade for imprecision because the OIS was met and limits of the CI were within a RR of 0.75 and 1.25 when the estimates effect was of little or no difference. Overall, the results are generally applicable to the overall screening population of interest, for screening testing using self-report tools compared with usual care where some screening may take place.
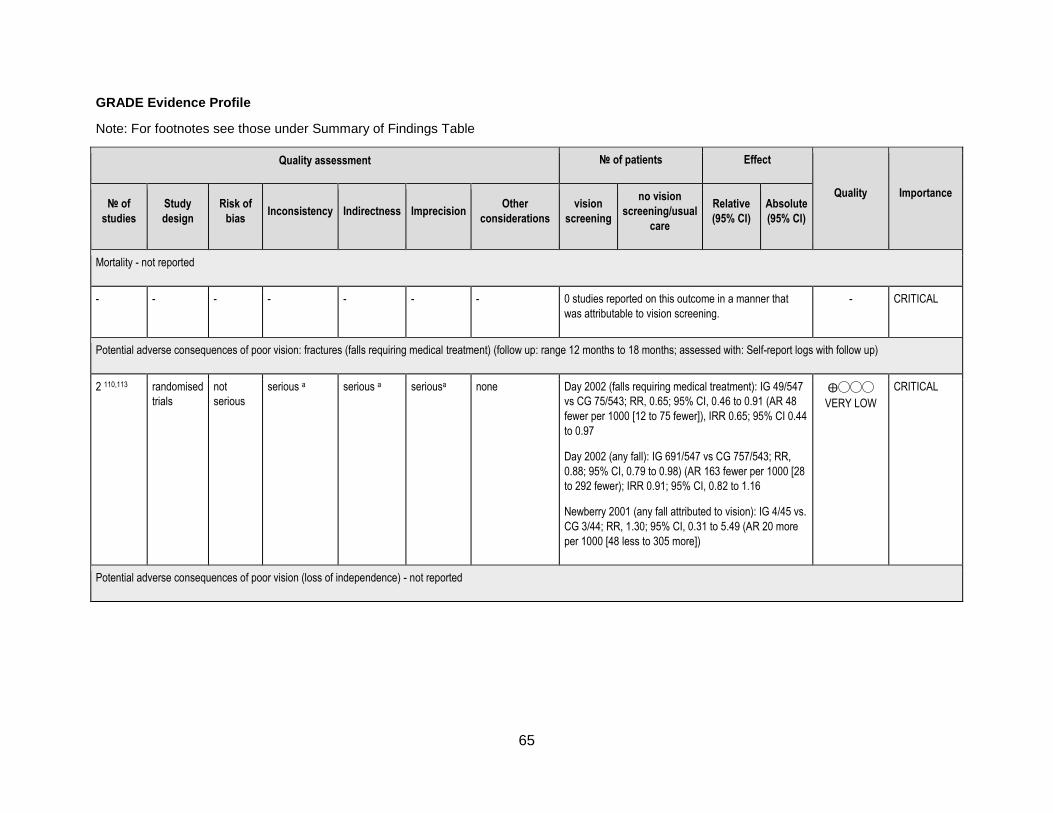
65
GRADE Evidence Profile
Note: For footnotes see those under Summary of Findings Table
Quality assessment № of patients Effect
Quality Importance № of
studies
Study
design
Risk of
bias Inconsistency Indirectness Imprecision
Other
considerations
vision
screening
no vision
screening/usual
care
Relative
(95% CI)
Absolute
(95% CI)
Mortality - not reported
- - - - - - - 0 studies reported on this outcome in a manner that
was attributable to vision screening.
- CRITICAL
Potential adverse consequences of poor vision: fractures (falls requiring medical treatment) (follow up: range 12 months to 18 months; assessed with: Self-report logs with follow up)
2 110,113 randomised
trials
not
serious
serious a serious a seriousa none Day 2002 (falls requiring medical treatment): IG 49/547
vs CG 75/543; RR, 0.65; 95% CI, 0.46 to 0.91 (AR 48
fewer per 1000 [12 to 75 fewer]), IRR 0.65; 95% CI 0.44
to 0.97
Day 2002 (any fall): IG 691/547 vs CG 757/543; RR,
0.88; 95% CI, 0.79 to 0.98) (AR 163 fewer per 1000 [28
to 292 fewer); IRR 0.91; 95% CI, 0.82 to 1.16
Newberry 2001 (any fall attributed to vision): IG 4/45 vs.
CG 3/44; RR, 1.30; 95% CI, 0.31 to 5.49 (AR 20 more
per 1000 [48 less to 305 more])
⨁◯◯◯
VERY LOW
CRITICAL
Potential adverse consequences of poor vision (loss of independence) - not reported
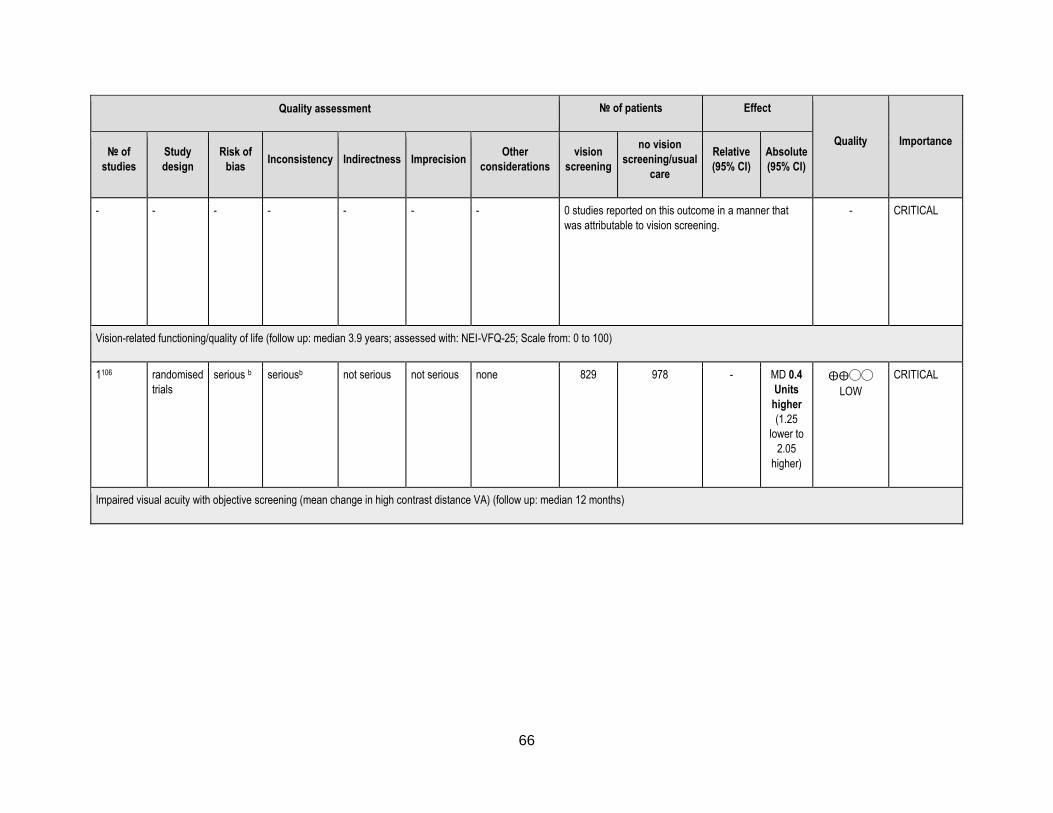
66
Quality assessment № of patients Effect
Quality Importance № of
studies
Study
design
Risk of
bias Inconsistency Indirectness Imprecision
Other
considerations
vision
screening
no vision
screening/usual
care
Relative
(95% CI)
Absolute
(95% CI)
- - - - - - - 0 studies reported on this outcome in a manner that
was attributable to vision screening.
- CRITICAL
Vision-related functioning/quality of life (follow up: median 3.9 years; assessed with: NEI-VFQ-25; Scale from: 0 to 100)
1106 randomised
trials
serious b seriousb not serious not serious none 829 978 - MD 0.4
Units
higher
(1.25
lower to
2.05
higher)
⨁⨁◯◯
LOW
CRITICAL
Impaired visual acuity with objective screening (mean change in high contrast distance VA) (follow up: median 12 months)
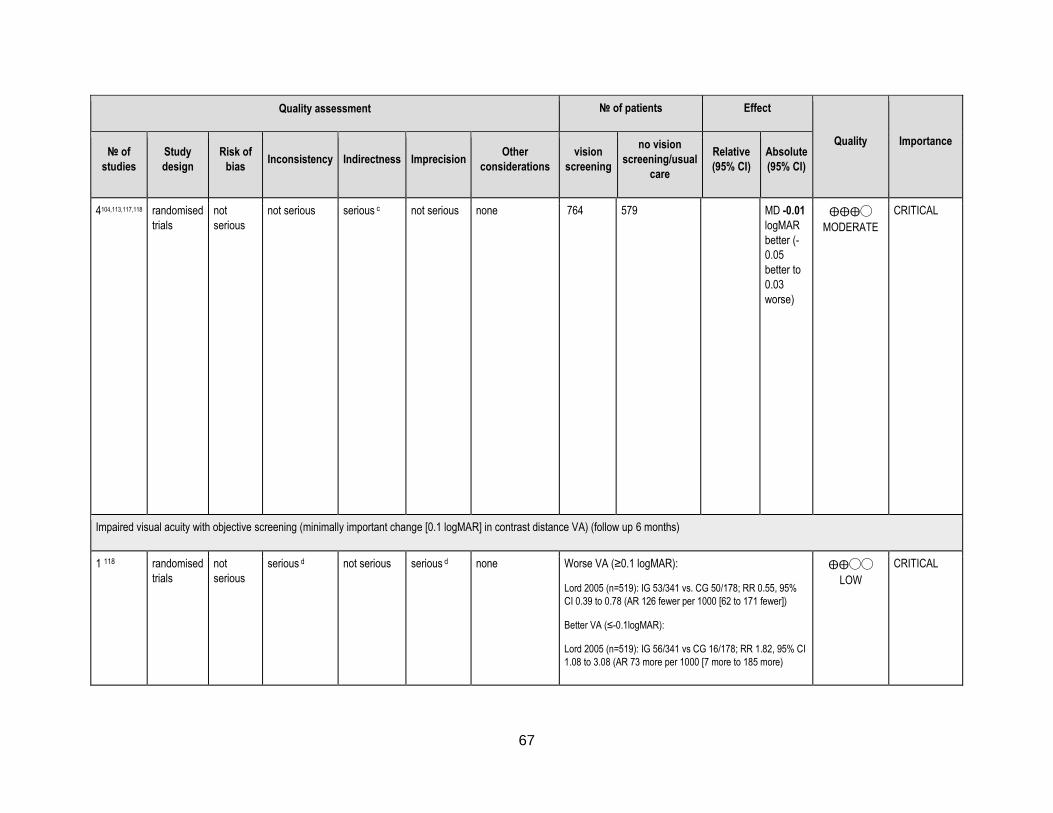
67
Quality assessment № of patients Effect
Quality Importance № of
studies
Study
design
Risk of
bias Inconsistency Indirectness Imprecision
Other
considerations
vision
screening
no vision
screening/usual
care
Relative
(95% CI)
Absolute
(95% CI)
4104,113,117,118 randomised
trials
not
serious
not serious serious c not serious none
764 579 MD -0.01
logMAR
better (-
0.05
better to
0.03
worse)
⨁⨁⨁◯
MODERATE
CRITICAL
Impaired visual acuity with objective screening (minimally important change [0.1 logMAR] in contrast distance VA) (follow up 6 months)
1 118 randomised
trials
not
serious
serious d not serious serious d none Worse VA (≥0.1 logMAR):
Lord 2005 (n=519): IG 53/341 vs. CG 50/178; RR 0.55, 95%
CI 0.39 to 0.78 (AR 126 fewer per 1000 [62 to 171 fewer])
Better VA (≤-0.1logMAR):
Lord 2005 (n=519): IG 56/341 vs CG 16/178; RR 1.82, 95% CI
1.08 to 3.08 (AR 73 more per 1000 [7 more to 185 more)
⨁⨁◯◯
LOW
CRITICAL

68
Quality assessment № of patients Effect
Quality Importance № of
studies
Study
design
Risk of
bias Inconsistency Indirectness Imprecision
Other
considerations
vision
screening
no vision
screening/usual
care
Relative
(95% CI)
Absolute
(95% CI)
Impaired visual acuity with objective screening (<20/60 distance visual acuity: bilateral or either eye) (follow up: median 47 months)
1106 randomised
trials
serious e serious e not serious serious e none Smeeth 2003: Bilateral: IG 114/817 vs. CG 160/962;
RR, 0.84; 95% CI, 0.64 to 1.10 (AR 26 less per 1000
[60 less to 17 more]); Either eye: IG 307/829 vs. CG
339/978; RR, 1.07; 95% CI, 0.84 to 1.36 (AR 25 more
per 1000 [54 less to 125 more])
⨁◯◯◯
VERY LOW
CRITICAL
Impaired visual acuity with objective screening (<20/40 distance visual acuity; bilateral) (follow up: range 12 months to 47 months)
2 106,117 randomised
trials
serious f not serious not serious serious f none 290/913
(31.8%)
394/1054
(37.4%)
RR 0.82
(0.66 to
1.02)
67 fewer
per
1,000
(from 7
more to
127
fewer)
⨁⨁◯◯
LOW
Impaired visual acuity with objective screening (<20/40 distance visual acuity: either eye) (follow up: range 12 months to 47 months; assessed with: Visual acuity charts (logMAR))
1 106 randomised
trials
serious g serious g not serious not serious none Smeeth 2003: IG 486/829 vs. CG 584/978; RR, 0.98;
95% CI, 0.82 to 1.17) (AR 15 less per 1000 [108 less to
102 more])
⨁⨁◯◯
LOW
CRITICAL
Self-reported vision problems (primarily self-report screening tools) (follow up: median 20 months; assessed with self-reported questionnaires)

69
Quality assessment № of patients Effect
Quality Importance № of
studies
Study
design
Risk of
bias Inconsistency Indirectness Imprecision
Other
considerations
vision
screening
no vision
screening/usual
care
Relative
(95% CI)
Absolute
(95% CI)
10105,107-
112,114-116 randomised
trials
serious h not serious not serious not serious none 1042/3767
(27.7%)
1296/4916
(26.4%)
RR 0.97
(0.90 to
1.05)
8 fewer
per
1,000
(from 13
more to
26 fewer)
⨁⨁⨁◯
MODERATE
CRITICAL
31.0% 9 fewer
per
1,000
(from 16
more to
31 fewer)
Serious or major adverse effects from treatment - not reported
- - - - - - - 0 studies reported on this outcome - CRITICAL
Anxiety or stress from inaccessible or ineffective treatment - not reported
- - - - - - - 0 studies reported on this outcome - CRITICAL
ADLs: activities of daily living; CG: Control group; CI: Confidence interval; IG: Intervention group; MD: Mean difference; NEI-VFQ-25: National Eye Institute Visual Function Questionnaire; RR: Risk ratio

70
References
1. Freeman EE, Roy-Gagnon MH, Samson E, et al. The global burden of visual difficulty in low,
middle, and high income countries. PLoS ONE. 2013;8(5):e63315.
2. Cruess AF, Gordon KD, Bellan L, et al. The cost of vision loss in Canada. 2. Results. Can J
Ophthalmol. 2011;46(4):315-318.
3. Ribeiro MV, Hasten-Reiter Junior HN, Ribeiro EA, et al. Association between visual impairment
and depression in the elderly: a systematic review. Arq Bras Oftalmol. 2015;78(3):197-201.
4. Renaud J, Bedard E. Depression in the elderly with visual impairment and its association with
quality of life. Clin Interv Aging. 2013;8:931-943.
5. Chou KL. Combined effect of vision and hearing impairment on depression in older adults:
evidence from the English Longitudinal Study of Ageing. J Affect Disord. 2008;106(1-2):191-
196.
6. Crews JE, Campbell VA. Vision impairment and hearing loss among community-dwelling older
Americans: implications for health and functioning. Am J Public Health. 2004;94(5):823-829.
7. Griffith LE, Raina P, Levasseur M, et al. Functional disability and social participation restriction
associated with chronic conditions in middle-aged and older adults. J Epidemiol Community
Health. 2017;71(4):381-89.
8. Jin YP, Wong DT. Self-reported visual impairment in elderly Canadians and its impact on healthy
living. Can J Ophthalmol. 2008;43(4):407-413.
9. Klein BE, Klein R, Lee KE, Cruickshanks KJ. Performance-based and self-assessed measures of
visual function as related to history of falls, hip fractures, and measured gait time. The Beaver
Dam Eye Study. Ophthalmology. 1998;105(1):160-164.
10. Public Health Agency of Canada. Seniors' Falls in Canada: Second Report. Ottawa, ON2014.
11. Rovner BW, Zisselman PM, Shmuely-Dulitzki Y. Depression and disability in older people with
impaired vision: a follow-up study. J Am Geriatr Soc. 1996;44(2):181-184.
12. Theis KA, Furner SE. Shut-In? Impact of Chronic Conditions on Community Participation
Restriction among Older Adults. J Aging Res. 2011;2011:759158.
13. Tinetti ME, Kumar C. The patient who falls: "It's always a trade-off". JAMA. 20
2010;303(3):258-266.
14. Yang Y, Trope GE, Buys YM, et al. Glaucoma severity and participation in diverse social roles:
does visual field loss matter? J Glaucoma. Jul 2016;25(7):e697-703.
15. Perlmutter MS, Bhorade A, Gordon M, et al. Cognitive, visual, auditory, and emotional factors
that affect participation in older adults. Am J Occup Ther. 2010;64:570-9.
16. World Health Organization. Visual disturbances and blindness (H53-H54), in Chapter 7. Diseases
of the eye and adnexa. International Statistical Classification of Diseases and Related Health
Problems 10th Revision (ICD-10) Version for 2010.
17. Leat SJ. A proposed model for integrated low-vision rehabilitation services in Canada. Optom Vis
Sci. 2016;93(1):77-84.
18. Leat SJ, Legge GE, Bullimore MA. What is low vision? A re-evaluation of definitions. Optom
Vis Sci. 1999;76(4):198-211.
19. Klein R, Klein BE, Linton KL, De Mets DL. The Beaver Dam Eye Study: visual acuity.
Ophthalmology. 1991;98(8):1310-1315.
20. Maberley DA, Hollands H, Chuo J, et al. The prevalence of low vision and blindness in Canada.
Eye (Lond). 2006;20(3):341-346.
21. Robinson B, Feng Y, Woods CA, et al. Prevalence of visual impairment and uncorrected
refractive error - report from a Canadian urban population-based study. Ophthalmic Epidemiol.
2013;20(3):123-130.
71
22. West SK, Munoz B, Rubin GS, et al. Function and visual impairment in a population-based study
of older adults. The SEE project. Salisbury Eye Evaluation. Invest Ophthalmol Vis Sci.
1997;38(1):72-82.
23. Courtney-Long EA, Carroll DD, Zhang QC, et al. Prevalence of Disability and Disability Type
Among Adults--United States, 2013. MMWR. Morbidity and mortality weekly report.
2015;64(29):777-783.
24. Committee on the Future of Primary Care, Divisions of Health Care Services, Institute of
Medicine. Primary Care: America’s Health in a New Era. Washington, D.C.: National Academy
Press; 1996.
25. Health Canada. About Primary Health Care. 2012. Available at https://www.canada.ca/en/health-
canada/services/primary-health-care/about-primary-health-care.html Accessed February 2, 2017.
26. Health Council of Canada. Health Care Renewal in Canada: Accelerating Change 2005.
http://healthcouncilcanada.ca/rpt_det.php?id=170.
27. Statistics Canada. Facts on Seeing Limitations. Ottawa, Ontario: Statistics Canada; 2009.
Available at http://www.statcan.gc.ca/pub/89-628-x/2009013/fs-fi/fs-fi-eng.htm
28. Statistics Canada. The 2006 Participation and Activity Limitation Survey: Disability in Canada
(89-628-X). Ottawa, Ontario: Statistics Canada; 2010.
29. Evans BJ, Rowlands G. Correctable visual impairment in older people: a major unmet need.
Ophthalmic Physiol Opt. 2004;24(3):161-180.
30. Kahn, HA, Leibowitz, HM, Ganley, JP et al. The Framingham Eye Study. I. Outline and major
prevalence findings. Am J Epidemiol. 1977;106:17-32.
31. Schiller JS LJ, Peregoy JA. Summary Health Statistics for U.S. Adults: National Health Interview
Survey, 2011. Vital Health Stat. 2012;10(256).
32. Evans JR, Fletcher AE, Wormald RP, et al. Prevalence of visual impairment in people aged 75
years and older in Britain: results from the MRC trial of assessment and management of older
people in the community. Br J Ophthalmol. 2002;86(7):795-800.
33. Attebo K, Mitchell P, Smith W. Visual acuity and the causes of visual loss in Australia. The Blue
Mountains Eye Study. Ophthalmology. 1996;103(3):357-364.
34. Klaver CC, Wolfs RC, Vingerling JR, et al. Age-specific prevalence and causes of blindness and
visual impairment in an older population: the Rotterdam Study. Arch Ophthalmol.
1998;116(5):653-658.
35. Weih LM, VanNewkirk MR, McCarty CA, Taylor HR. Age-specific causes of bilateral visual
impairment. Arch Ophthalmol. 2000;118(2):264-269.
36. Klein R, Klein BE, Lee KE, et al. Changes in visual acuity in a population over a 15-year period:
the Beaver Dam Eye Study. Am J Ophthalmol. 2006;142(4):539-549.
37. Mitchell P, Hayes P, Wang JJ. Visual impairment in nursing home residents: the Blue Mountains
Eye Study. Med J Aust. 1997;166(2):73-76.
38. Owsley C, McGwin G, Scilley K, et al. The visual status of older persons residing in nursing
homes. Arch Ophthalmol. 2007;125(7):925-930.
39. West SK, Friedman D, Munoz B, et al. A randomized trial of visual impairment interventions for
nursing home residents: study design, baseline characteristics and visual loss. Ophthalmic
Epidemiol. 2003;10(3):193-209.
40. Delpero W et al. and the Canadian Ophthalmological Society Clinical Practice Guideline Expert
Committee. Canadian Ophthalmological Society evidence-based clinical practice guidelines for
the periodic eye examination in adults in Canada. Can J Ophthalmol. 2007;42(1):39-45, 158-163.
41. Vitale S, Cotch MF, Sperduto RD. Prevalence of visual impairment in the United States. JAMA
2006;295(18):2158-2163.
42. Ghanem RC, de la Cruz J, Tobaigy FM, et al. LASIK in the presbyopic age group: safety,
efficacy, and predictability in 40- to 69-year-old patients. Ophthalmology. 2007;114(7):1303-
1310.

72
43. Chou R, Dana T, Bougatsos C, et al. Screening for Impaired Visual Acuity in Older Adults: A
Systematic Review to Update the 2009 U.S. Preventive Services Task Force Recommendation.
Report no. 14-05209-EF-1. Agency for Healthcare Research and Quality, Rockville MD; 2016.
44. Coleman AL, Yu F, Keeler E, Mangione CM. Treatment of uncorrected refractive error improves
vision-specific quality of life. J Am Geriatr Soc. 2006;54(6):883-890.
45. Owsley C, McGwin G, Jr., Scilley K, et al. Effect of refractive error correction on health-related
quality of life and depression in older nursing home residents. Arch Ophthalmol.
2007;125(11):1471-1477.
46. Trautner C, Haastert B, Richter B, et al. Incidence of blindness in southern Germany due to
glaucoma and degenerative conditions. Invest Ophthalmol Vis Sci. 2003;44(3):1031-1034.
47. Chew EY, Clemons TE, Agron E, et al. Long-term effects of vitamins C and E, beta-carotene,
and zinc on age-related macular degeneration: AREDS report no. 35. Ophthalmology.
2013;120(8):1604-1611 e1604.
48. Evans JR, Lawrenson JG. Antioxidant vitamin and mineral supplements for slowing the
progression of age-related macular degeneration. Cochrane Database Syst Rev.
2012;11:CD000254.
49. Eter N, Krohne TU, Holz FG. New pharmacologic approaches to therapy for age-related macular
degeneration. BioDrugs. 2006;20(3):167-179.
50. Chakravarthy U, Wong TY, Fletcher A, et al. Clinical risk factors for age-related macular
degeneration: a systematic review and meta-analysis. BMC ophthalmol. 2010;10:31.
51. Klein R, Knudtson MD, Cruickshanks KJ, Klein BE. Further observations on the association
between smoking and the long-term incidence and progression of age-related macular
degeneration: the Beaver Dam Eye Study. Arch Ophthalmol. 2008;126(1):115-121.
52. Smith W, Assink J, Klein R, et al. Risk factors for age-related macular degeneration: pooled
findings from three continents. Ophthalmology. 2001;108(4):697-704.
53. Velilla S, Garcia-Medina JJ, Garcia-Layana A, et al. Smoking and age-related macular
degeneration: review and update. J Ophthalmol. 2013;2013:895147.
54. Schick T, Ersoy L, Lechanteur YT, et al. History of sunlight exposure is a risk factor for age-
related macular degeneration. Retina. 2016;36(4):787-790.
55. Congdon N, O'Colmain B, Klaver CC, et al. Causes and prevalence of visual impairment among
adults in the United States. Arch Ophthalmol. 2004;122(4):477-485.
56. Chang JR, Koo E, Agron E, et al. Risk factors associated with incident cataracts and cataract
surgery in the Age-related Eye Disease Study (AREDS): AREDS report number 32.
Ophthalmology. 2011;118(11):2113-2119.
57. West SK, Valmadrid CT. Epidemiology of risk factors for age-related cataract. Survey of
Ophthalmology. 1995;39(4):323-334.
58. de Silva SR, Riaz Y, Evans JR. Phacoemulsification with posterior chamber intraocular lens
versus extracapsular cataract extraction (ECCE) with posterior chamber intraocular lens for age-
related cataract. Cochrane Database Syst Rev. 2014(1):CD008812.
59. Riaz Y, Mehta JS, Wormald R, et al. Surgical interventions for age-related cataract. Cochrane
Database Syst Rev. 2006(4):CD001323.
60. Markowitz SN. Principles of modern low vision rehabilitation. Can J Ophthalmol.
2006;41(3):289-312.
61. Ferris FL, 3rd, Bailey I. Standardizing the measurement of visual acuity for clinical research
studies: guidelines from the Eye Care Technology Forum. Ophthalmology. 1996;103(1):181-182.
62. Arditi A, Cagenello R. On the statistical reliability of letter-chart visual acuity measurements.
Invest Ophthalmol Vis Sci. 1993;34(1):120-129.
63. Lovie-Kitchin JE. Validity and reliability of visual acuity measurements. Ophthalmic Physiol
Opt. 1988;8(4):363-370.
64. Lovie-Kitchin JE, Brown B. Repeatability and intercorrelations of standard vision tests as a
function of age. Optom Vis Sci. 2000;77(8):412-420.
73
65. Siderov J, Tiu AL. Variability of measurements of visual acuity in a large eye clinic. Acta
Ophthalmologica Scandinavica. 1999;77(6):673-676.
66. Rosser DA, Laidlaw DA, Murdoch IE. The development of a "reduced logMAR" visual acuity
chart for use in routine clinical practice. Br J Ophthalmol. 2001;85(4):432-436.
67. Blackhurst DW, Maguire MG. Reproducibility of refraction and visual acuity measurement under
a standard protocol. The Macular Photocoagulation Study Group. Retina. 1989;9(3):163-169.
68. Kiser AK, Mladenovich D, Eshraghi F, et al. Reliability and consistency of visual acuity and
contrast sensitivity measures in advanced eye disease. Optom Vis Sci. 2005;82(11):946-954.
69. Leinonen J, Laakkonen E, Laatikainen L. Random measurement error in visual acuity
measurement in clinical settings. Acta Ophthalmologica Scandinavica. 2005;83(3):328-332.
70. Legge GE. Glenn A. Fry Award Lecture 1990: three perspectives on low vision reading. Optom
Vis Sci. 1991;68(10):763-769.
71. Pelli DG RJ, Wilkins AJ,. The design of a new letter chart for measuring contrast sensitivity. Clin
Vis Sci 1988;2:187-199.
72. Haegerstrom-Portnoy G, Brabyn J, Schneck ME, Jampolsky A. The SKILL Card. An acuity test
of reduced luminance and contrast. Smith-Kettlewell Institute Low Luminance. Invest
Ophthalmol Vis Sci. 1997;38(1):207-218.
73. Colenbrander A FD. The Mixed Contrast Reading card, a new screening test for contrast
sensitivity. In: Jones S RG, Hamlin D, ed. Vision 2005. International Congress Series London:
Elsevier; 2006.
74. Schuchard RA. Validity and interpretation of Amsler grid reports. Arch Ophthalmol.
1993;111(6):776-780.
75. Suner IJ, Kokame GT, Yu E, et al. Responsiveness of NEI VFQ-25 to changes in visual acuity in
neovascular AMD: validation studies from two phase 3 clinical trials. Invest Ophthalmol Vis Sci.
2009;50(8):3629-3635.
76. Mangione CM, Lee PP, Gutierrez PR, et al. Development of the 25-item National Eye Institute
Visual Function Questionnaire. Arch Ophthalmol. 2001;119(7):1050-1058.
77. Mangione CM, Lee PP, Pitts J, et al. Psychometric properties of the National Eye Institute Visual
Function Questionnaire (NEI-VFQ). NEI-VFQ Field Test Investigators. Arch Ophthalmol.
1998;116(11):1496-1504.
78. Jin YP, Trope GE. Eye care utilization in Canada: disparity in the publicly funded health care
system. Can J Ophthalmol. 2011;46(2):133-138.
79. Hong CJ, Trope GE, Buys YM, et al. Does government assistance improve utilization of eye care
services by low-income individuals? Can J Ophthalmol. 2014;49(4):320-325.
80. Siu AL, Bibbins-Domingo K, Grossman DC, et al. Screening for Impaired Visual Acuity in Older
Adults: US Preventive Services Task Force Recommendation Statement. JAMA.
2016;315(9):908-914.
81. American Academy of Family Physicians. Clinical Preventive Service Recommendations: Visual
Difficulties and Impairment, 2016. Available at http://www.aafp.org/patient-care/clinical-
recommendations/all/visual.html
82. Canadian Task Force on the Periodic Health Examination. Periodic health examination, 1995
update: 3. Screening for visual problems among elderly patients. CMAJ. 1995;152(8):1211-1222.
83. Canadian Association of Optometrists. Frequency of Eye Examinations, 2013. Available at:
https://opto.ca/position-statements
84. Robinson BS MK, Glenny C, Stolee P. An evidence-based guideline for the frequency of
optometric eye examinations. Primary Health Care: Open Access. 2012;2(4).
85. Feder RS OT, Prum BE, and the American Academy of Ophthalmology Preferred Practice
Pattern Committee. Comprehensive Adult Medical Eye Evaluation. American Academy of
Ophthalmology, 2015. Available at http://www.aao.org/preferred-practice-
pattern/comprehensive-adult-medical-eye-evaluation-2015

74
86. American Optometric Association Evidence-based Optometry Guideline Development Group.
Comprehensive Adult Eye and Vision Examination. St. Louis, MO: American Optometric
Association; 2015. Available at: http://aoa.uberflip.com/i/578152-aoa-clinical-practice-
guidelines-adult-eye-exam
87. Mayo-Wilson E, Grant S, Burton J, et al. Preventive home visits for mortality, morbidity, and
institutionalization in older adults: a systematic review and meta-analysis. PLoS ONE.
2014;9(3):e89257.
88. Ploeg J, Feightner J, Hutchison B, et al. Effectiveness of preventive primary care outreach
interventions aimed at older people: meta-analysis of randomized controlled trials. Can Fam
Physician. 2005;51:1244-1245.
89. Smeeth L, Iliffe S. Community screening for visual impairment in the elderly. Cochrane
Database Syst Rev. 2006(3):CD001054.
90. Smeeth L, Ng ES. Intraclass correlation coefficients for cluster randomized trials in primary care:
data from the MRC Trial of the Assessment and Management of Older People in the Community.
Controlled Clinical Trials. 2002;23(4):409-421.
91. Guyatt GH, Thorlund K, Oxman AD, et al. GRADE guidelines: 13. Preparing summary of
findings tables and evidence profiles-continuous outcomes. J Clin Epidemiol. 2013;66(2):173-
183.
92. Johnston BC, Patrick DL, Thorlund K, et al. Patient-reported outcomes in meta-analyses-part 2:
methods for improving interpretability for decision-makers. Health Qual Life Outcomes.
2013;11:211.
93. Fu R, Gartlehner G, Grant M, et al. Conducting quantitative synthesis when comparing medical
interventions: AHRQ and the Effective Health Care Program. J Clin Epidemiol.
2011;64(11):1187-1197.
94. Egger M, Davey Smith G, Schneider M, Minder C. Bias in meta-analysis detected by a simple,
graphical test. BMJ. 1997;315(7109):629-634.
95. Higgins JP Green S. Section 9.6.6 Interpretation of subgroup analyses and meta-regressions.
Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0. Online, 2011.
Available at: http://handbook.cochrane.org/
96. Guyatt GH, Oxman AD, Kunz R, et al. GRADE guidelines: 6. Rating the quality of evidence--
imprecision. J Clin Epidemiol. 2011;64(12):1283-1293.
97. Guyatt GH, Oxman AD, Kunz R, et al. GRADE guidelines: 8. Rating the quality of evidence--
indirectness. J Clin Epidemiol. 2011;64(12):1303-1310.
98. Guyatt GH, Oxman AD, Kunz R, et al. GRADE guidelines: 7. Rating the quality of evidence--
inconsistency. J Clin Epidemiol. 2011;64(12):1294-1302.
99. Guyatt GH, Oxman AD, Schunemann HJ, et al. GRADE guidelines: a new series of articles in the
Journal of Clinical Epidemiology. J Clin Epidemiol. 2011;64(4):380-382.
100. Guyatt GH, Oxman AD, Vist G, et al. GRADE guidelines: 4. Rating the quality of evidence--
study limitations (risk of bias). J Clin Epidemiol. 2011;64(4):407-415.
101. Guyatt GH, Oxman AD, Sultan S, et al. GRADE guidelines: 9. Rating up the quality of evidence.
J Clin Epidemiol. 2011;64(12):1311-1316.
102. Mayo-Wilson E, Grant S, Burton J, et al. Preventive home visits for mortality, morbidity, and
institutionalization in older adults: a systematic review and meta-analysis. PLoS ONE.
2014;9(3):e89257.
103. Zhang XY, Shuai J, Li LP. Vision and relevant risk factor interventions for preventing falls
among older people: a network meta-analysis. Sci. 2015;5:10559.
104. Haanes GG, Kirkevold M, Hofoss D, et al. An intervention designed to improve sensory
impairments in the elderly and indoor lighting in their homes: an exploratory randomized
controlled trial. J Multidiscip Healthc. 2015;8:11-20.
105. Eekhof J, De Bock G, Schaapveld K, Springer M. Effects of screening for disorders among the
elderly: an intervention study in general practice. Fam Pract. 2000;17(4):329-333.

75
106. Smeeth L, Fletcher AE, Hanciles S, et al. Screening older people for impaired vision in primary
care: cluster randomised trial. BMJ. 2003;327(7422):1027.
107. McEwan RT, Davison N, Forster DP, et al. Screening elderly people in primary care: a
randomized controlled trial. Br J Gen Pract. 1990;40(332):94-97.
108. van Rossum E, Frederiks CM, Philipsen H, et al. Effects of preventive home visits to elderly
people. BMJ. 1993;307(6895):27-32.
109. Vetter NJ, Jones DA, Victor CR. Effect of health visitors working with elderly patients in general
practice: a randomised controlled trial. BMJ (Clinical Research Ed.). 1984;288(6414):369-372.
110. Newbury JW, Marley JE, Beilby JJ. A randomised controlled trial of the outcome of health
assessment of people aged 75 years and over. Med J Aust. 2001;175(2):104-107.
111. Vetter NJ, Lewis PA, Ford D. Can health visitors prevent fractures in elderly people? BMJ.
1992;304(6831):888-890.
112. Dapp U, Anders JA, von Renteln-Kruse W, et al. A randomized trial of effects of health risk
appraisal combined with group sessions or home visits on preventive behaviors in older adults. J
Gerontol A Biol Sci Med Sci. 2011;66(5):591-598.
113. Day L, Fildes B, Gordon I, et al. Randomised factorial trial of falls prevention among older
people living in their own homes. BMJ. 2002;325(7356):128.
114. Moore AA, Siu A, Partridge JM, et al. A randomized trial of office-based screening for common
problems in older persons. Am J Med. 1997;102(4):371-378.
115. Wagner EH, LaCroix AZ, Grothaus L, et al. Preventing disability and falls in older adults: a
population-based randomized trial. Am J Public Health. 1994;84(11):1800-1806.
116. Harari D, Iliffe S, Kharicha K, et al. Promotion of health in older people: a randomised controlled
trial of health risk appraisal in British general practice. Age Ageing. 2008;37(5):656-71.
117. Tay T, Rochtchina E, Mitchell P, et al. Eye care service utilization in older people seeking aged
care. Clin Exp Ophthalmol. 2006;34(2):141-145.
118. Lord SR, Tiedemann A, Chapman K, et al. The effect of an individualized fall prevention
program on fall risk and falls in older people: a randomized, controlled trial. J Am Geriatr Soc.
2005;53(8):1296-1304.
119. Lord SR, Menz HB, Tiedemann A. A physiological profile approach to falls risk assessment and
prevention. Phys Ther. 2003;83(3):237-252.
120. Fitzharris MP, Day L, Lord SR, et al. The Whitehorse NoFalls trial: effects on fall rates and
injurious fall rates. Age Ageing. 2010;0:1-6.
121. Fletcher AE, Price GM, Ng ES, et al. Population-based multidimensional assessment of older
people in UK general practice: a cluster-randomised factorial trial. Lancet.
2004;364(9446):1667-1677.
122. Klein BE, Klein R, Lee KE, Cruickshanks KJ. Associations of performance-based and self-
reported measures of visual function. The Beaver Dam Eye Study. Ophthalmic Epidemiol.
1999;6(1):49-60.
123. Kempen GI, van Heuvelen MJ, van den Brink RH, et al. Factors affecting contrasting results
between self-reported and performance-based levels of physical limitation. Age Ageing.
1996;25(6):458-464.
124. Iliffe S, Kharicha K, Harari D, et al. Self-reported visual function in healthy older people in
Britain: an exploratory study of associations with age, sex, depression, education and income.
Fam Pract. 2005;22(6):585-590.
125. Morgenstern H. Uses of ecological analysis in epidemiologic research. Am J Public Health.
1982;72:1336-1344.
126. Thompson SG, Higgins JP. How should meta-regression analyses be undertaken and interpreted?
Stat Med. 15 2002;21(11):1559-1573.
127. Smeeth L, Iliffe S. Community screening for visual impairment in the elderly. Cochrane
Database Syst Rev. 2000(2):CD001054.

76
128. Cumming RG, Ivers R, Clemson L, et al. Improving vision to prevent falls in frail older people: a
randomized trial. J Am Geriatr Soc. 2007;55:175–181.
129. Coleman AL, Stone K, Ewing SK, et al. Higher risk of multiple falls among elderly women who
lose visual acuity. Ophthalmology. 2004;111(5):857-862.
130. Reed-Jones RJ, Solis GR, Lawson KA, et al. Vision and falls: a multidisciplinary review of the
contributions of visual impairment to falls among older adults. Maturitas. 2013;75(1):22-28.
131. Clemons TE, Rankin MW, McBee WL. Cognitive impairment in the Age-Related Eye Disease
Study: AREDS report no. 16. Arch Ophthalmol. 2006;124(4):537-543.
132. Moher D, Pham B, Klassen TP, et al. What contributions do languages other than English make
on the results of meta-analyses? J Clin Epidemiol. 2000;53(9):964-972.
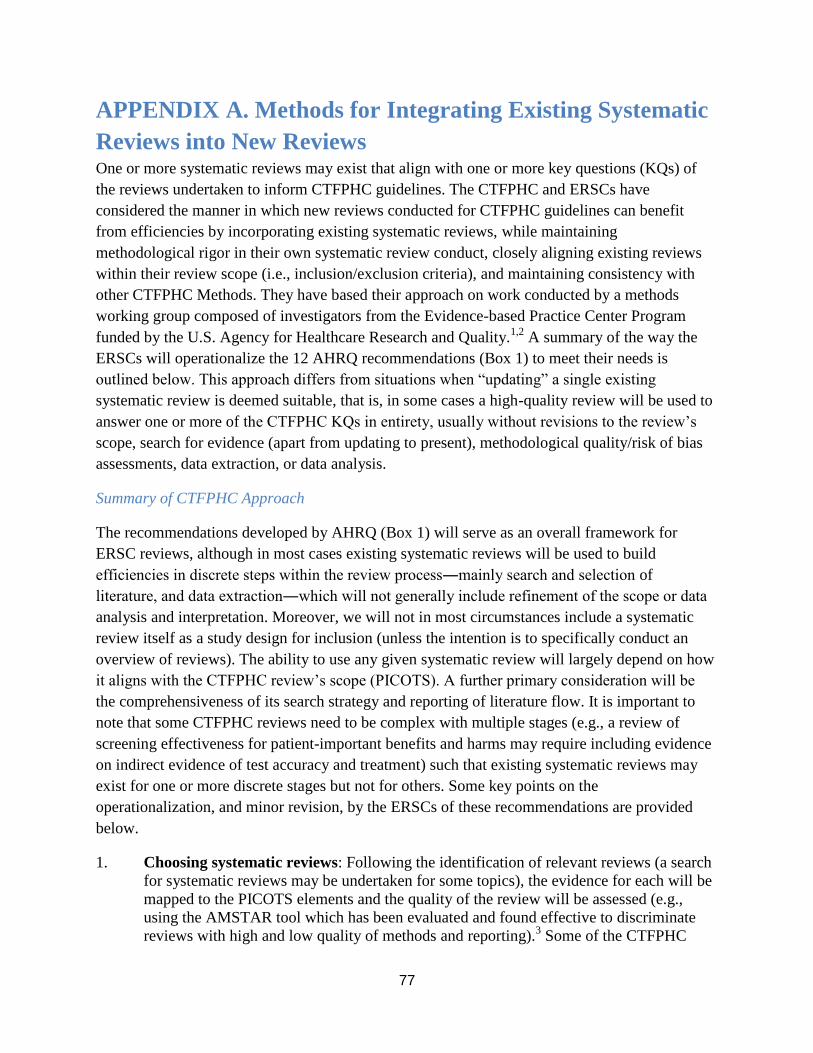
77
APPENDIX A. Methods for Integrating Existing Systematic
Reviews into New Reviews One or more systematic reviews may exist that align with one or more key questions (KQs) of
the reviews undertaken to inform CTFPHC guidelines. The CTFPHC and ERSCs have
considered the manner in which new reviews conducted for CTFPHC guidelines can benefit
from efficiencies by incorporating existing systematic reviews, while maintaining
methodological rigor in their own systematic review conduct, closely aligning existing reviews
within their review scope (i.e., inclusion/exclusion criteria), and maintaining consistency with
other CTFPHC Methods. They have based their approach on work conducted by a methods
working group composed of investigators from the Evidence-based Practice Center Program
funded by the U.S. Agency for Healthcare Research and Quality.1,2
A summary of the way the
ERSCs will operationalize the 12 AHRQ recommendations (Box 1) to meet their needs is
outlined below. This approach differs from situations when “updating” a single existing
systematic review is deemed suitable, that is, in some cases a high-quality review will be used to
answer one or more of the CTFPHC KQs in entirety, usually without revisions to the review’s
scope, search for evidence (apart from updating to present), methodological quality/risk of bias
assessments, data extraction, or data analysis.
Summary of CTFPHC Approach
The recommendations developed by AHRQ (Box 1) will serve as an overall framework for
ERSC reviews, although in most cases existing systematic reviews will be used to build
efficiencies in discrete steps within the review process―mainly search and selection of
literature, and data extraction―which will not generally include refinement of the scope or data
analysis and interpretation. Moreover, we will not in most circumstances include a systematic
review itself as a study design for inclusion (unless the intention is to specifically conduct an
overview of reviews). The ability to use any given systematic review will largely depend on how
it aligns with the CTFPHC review’s scope (PICOTS). A further primary consideration will be
the comprehensiveness of its search strategy and reporting of literature flow. It is important to
note that some CTFPHC reviews need to be complex with multiple stages (e.g., a review of
screening effectiveness for patient-important benefits and harms may require including evidence
on indirect evidence of test accuracy and treatment) such that existing systematic reviews may
exist for one or more discrete stages but not for others. Some key points on the
operationalization, and minor revision, by the ERSCs of these recommendations are provided
below.
1. Choosing systematic reviews: Following the identification of relevant reviews (a search
for systematic reviews may be undertaken for some topics), the evidence for each will be
mapped to the PICOTS elements and the quality of the review will be assessed (e.g.,
using the AMSTAR tool which has been evaluated and found effective to discriminate
reviews with high and low quality of methods and reporting).3 Some of the CTFPHC

78
KQs may only have a single existing systematic review for possible incorporation, while
others may have more than one; if suitable, a decision between systematic reviews will be
based on methodological quality, comprehensiveness and quality of its literature search
and reporting (e.g., assessed using PRESS checklist), comprehensiveness of reporting on
included studies, and the best fit within the CTFPHC scope and methods. In some cases
two or more reviews may be integrated because, together, they capture the full scope of
the CTFPHC KQ(s). Rationale will be provided for choices made.
Note: If no review is deemed a good fit for purpose for integration (i.e., de novo process
all together appears to be best option) we will at minimum examine available reviews for
their search strategies (to ensure that our search strategies are comprehensive) and review
their reference lists for identification of studies.
2. Searching: Various strategies will be considered. If one or more reviews are fit for
purpose (but do not meet criteria for classification as a systematic review update) and
cover a scope that is very similar or broader than the CTFPHC topic, we may update the
search(es) if the last search date was prior to 6 months before commencing our review.
When there are multiple reviews being considered, updating the literature to present may
involve a new comprehensive search strategy to identify studies published after the date
of the earliest existing review; this may reduce complexities when trying to implement,
document, and remove duplicates from multiple searches. Alternatively, if the scope of
the existing review(s) is narrower (e.g., missing an element in PICOTS) or the search
deemed sub-optimal in some manner (e.g., missing key terms, additional database viewed
as highly relevant) we may re-run the existing review’s search concurrent with an
original (e.g., broader) search and remove the citations previously screened for the other
review. If more appropriate, we may update the other review’s search and use a new
search for the missing PICO element(s) (e.g., one additional intervention) for a longer
time period to meet our timeframe. In cases where we feel screening excluded studies
lists is appropriate we will also undertake this. Careful consideration will be used to
ensure a comprehensive search is conducted regardless of approach taken; moreover, the
ERSC librarians will help determine on a case-by-case basis what approach would be
feasible for implementation to ensure aims of building efficiencies are possible.
3. Screening and selection: We will assess articles included in all relevant reviews (based
on full text if necessary) to determine if they meet our inclusion criteria.
4. Data extraction and methodological quality assessments: We will consider
incorporating the data on study and participant characteristics rather than extracting these
data anew; we may also use the review author’s risk of bias assessments if the
tools/methods are consistent with CTFPHC methods. These steps will create efficiencies
but because they are dependent on the quality of the systematic review and extent of
reporting, the ERSC staff will verify the data on at least 5 to 10% of studies.1
5. Data analysis: We will consider using quantitative outcome data from reviews (with
verification), but will not typically use meta-analyses or quality (GRADE) assessments of
existing reviews.
6. Reporting: Transparent reporting of all integration steps used will be included in the
evidence review report.

79
1. Existing reviews should be confirmed as systematic reviews through the application of a minimum set of eligibility criteria. We propose that the minimum eligibility criteria for systematic reviews include an explicit and adequate search, application of predefined eligibility criteria to select studies, risk of bias assessment for included studies, and synthesis of results.
2. Criteria to assess the relevance, in terms of question elements and currency, and quality of existing systematic reviews under consideration for inclusion in reviews should be predefined.
3. The quality of relevant existing systematic reviews should be assessed in an explicit manner with a minimum set of quality criteria that include search of multiple sources, use of a generally accepted tool for risk of bias assessment, and sufficient information to assess the strength of the body of evidence that includes the major domains of risk of bias, directness, consistency, precision, and reporting bias.
4. The risk of bias assessments from the existing systematic review may be used when the review described an explicit process, including the use of a tool or method that is compatible with the approach of the current review and that assessed the key sources of potential bias.
5. We suggest that risk of bias assessment be repeated in a sample of studies from an existing review under consideration for inclusion in a new review to confirm concordance with current review team approach.
6. We recommend that at a minimum, reviews should narratively describe findings of the prior review(s), including the number and types of studies included, and the overall findings.
7. We recommend that newly identified studies be clearly distinguished from studies in the existing review(s) when presented in the narrative and any tables (eg, separate tables).
8. Summary tables should include sufficient information to support ratings for overall strength of evidence, including ratings for individual strength of evidence domains (study limitations, consistency, precision, directness, reporting bias). The strength of evidence ratings should be based on the underlying primary evidence, not the number or quality of existing systematic reviews.
9. Using strength of evidence domains as a framework (study limitations, consistency, precision, directness, and reporting bias), review authors should consider how new evidence would change estimates of effect or ratings for strength of evidence. A new quantitative synthesis (ie, pooled estimate) is needed if new studies would change conclusions or strength of evidence judgements, or to obtain a more precise or more up-to-date estimate.
10. In cases where the existing systematic review(s) did not complete strength of evidence grading for a comparison and outcome of interest, the strength of evidence should be assessed for the body of evidence, considering primary studies from prior review(s) and any new studies identified.
11. In cases where no new studies are added to the body of evidence, the strength of evidence assessment from the existing systematic review may be used if conducted using an acceptable grading approach consistent with current review context. In these cases, we suggest that the overall strength of evidence assessment be reviewed, considering the strength of evidence domains, to confirm consistency with current review team assessments.
12. In cases where new studies are added to the body of evidence, the strength of evidence may need to be reassessed on the basis of all studies/evidence.
Box 1. AHRQ recommendations on integrating existing systematic reviews for new systematic reviews.
1Robinson KA, Chou R, Berkman ND, et al. Integrating bodies of evidence: existing systematic reviews and primary studies.
Methods Guide for Effectiveness and Comparative Effectiveness Reviews [Internet]. Rockville (MD): Agency for Healthcare
Research and Quality (US); 2015 Feb.
2Robinson KA, Chou R, Berkman ND, et al. Twelve recommendations for integrating existing systematic reviews into new
reviews: EPC guidance. J Clin Epidemiol. 2016 Feb;70:38-44. PMID: 26261004.

80
APPENDIX B. Database Search Strategies
MEDLINE: Epub Ahead of Print, In-Process & Other Non-Indexed Citations,
Ovid MEDLINE(R) Daily and Ovid MEDLINE(R) 1946 to Present
1. *Accidental Falls/pc
2. *Cataract/di, pc
3. *Eye Diseases/di, pc
4. *Macular Degeneration/di, pc
5. *Vision Disorders/di, pc
6. Vision Screening/
7. Vision Tests/
8. exp Visual Acuity/ and (assess* or detect* or diagnos* or evaluat* or exam* or prevent* or
screen* or test*).tw,kf.
9. Amsler.tw,kf.
10. ((AMD or ARMD or cataract* or eye or eyes or macular degeneration or ocular or
ophthalm* or visual or vision) adj3 (assess* or detect* or diagnos* or evaluat* or exam* or
prevent* or screen* or test*)).tw,kf.
11. (E chart* or E test*).tw,kf.
12. ((evaluat* or exam* or test*) adj3 (pin hole or pinhole)).tw,kf.
13. (fall* adj2 prevent*).ti.
14. funduscop*.tw,kf.
15. Jaeger.tw,kf.
16. Landolt*.tw,kf.
17. (Log-Mar* or LogMAR*).tw,kf.
18. Snellen*.tw,kf.
19. or/1-18 [Combined MeSH & text words for vision screening - narrow]
20. Community Health Services/
21. Community Health Workers/
22. Early Diagnosis/
23. Family Practice/
24. Geriatric Assessment/
25. Health Promotion/
26. Health Status/
27. Home Care Services/
28. Home Health Nursing/
29. House Calls/
30. Mass Screening/
31. Nurses, Community Health/
32. Nursing Assessment/
33. Office Visits/
34. Primary Health Care/
35. Preventive Health Services/
36. ((assess* or detect* or diagnostic* or evaluat* or exam* or prevent* screen* or test*) adj5
(family doctor* or family practi* or family physician* or general practic* or GP or primary
care or primary health care)).tw,kf.

81
37. ((assessment* or education or promotion*) adj1 health*).tw,kf.
38. ((care* or service* or support* or visit*) adj2 (communit* or domicil* or home* or out-
reach* or outreach*)).tw,kf.
39. (communit* adj3 (out-reach* or outreach* or practice* or program*)).tw,kf.
40. ((clinician* or health or doctor* or nurse* or physician* or volunteer*) adj2 visit*).tw,kf.
41. (early and detect*).ti.
42. geriatric assessment*.tw,kf.
43. (pre-dispos* or predispos*).ti.
44. or/20-43 [Combined MeSH & text words for screening - broad]
45. (assess* or detect* or diagnostic* or evaluat* or exam* or prevent* or screen* or
test*).tw,kf.
46. and/44-45 [text word filter on broad screening results]
47. or/19,46 [Combined screening sets]
48. exp Aged/
49. Geriatrics/
50. Health Services for the Aged/
51. (aged or ageing or aging or elder* or geriatric* or octogenarian* or septuagenarian* or
senior*).tw,kf.
52. ((adult* or citizen? or client? or consumer? or female? or male? or men or patient? or
people or person* or wom#n) adj3 older*).tw,kf.
53. or/48-52 [Combined MeSH & text words for older adults]
54. and/47,53 [Combined concepts for screening and older adults]
55. "Clinical Trials as Topic"/
56. controlled clinical trial.pt.
57. randomized controlled trial.pt.
58. placebo.ab.
59. random*.ab.
60. trial.ti.
61. or/55-60 [Modified Cochrane highly sensitive RCT filter: sensitivity and precision
maximizing version]
62. exp Animals/ not Humans/
63. (animal or animal-model* or animals or canine* or cat or cats or dog or dogs or feline or
felines or hamster or hamsters or mice or monkey or monkeys or mouse or pig or piglet or
piglets or pigs or porcine or primate* or rabbit or rabbits or rat or rats or rodent or rodents or
sheep or swine or swines).ti.
64. 61 not (62 or 63)
65. 54 and 64 [RCT & animal filter applied]
66. (Adolescent/ or exp Child/ or exp Infant/) not exp Adult/
67. Adolescent Medicine/
68. exp Pediatrics/
69. (paediatr* or pediatr*).jw.
70. (adolesc* or babies or baby or boy* or child* or fetal or fetus or foet* or girl* or infan* or
juvenile* or kid or kids or neo-nat* or neonat* or new-born* or newborn* or paediatr* or
pediatr* or preadolesc* or prepubesc* or preteen* or pubescen* or teen* or toddler* or
youth*).tw,kf.
71. or/66-70 [Combined MeSH & textwords for pediatric studies]
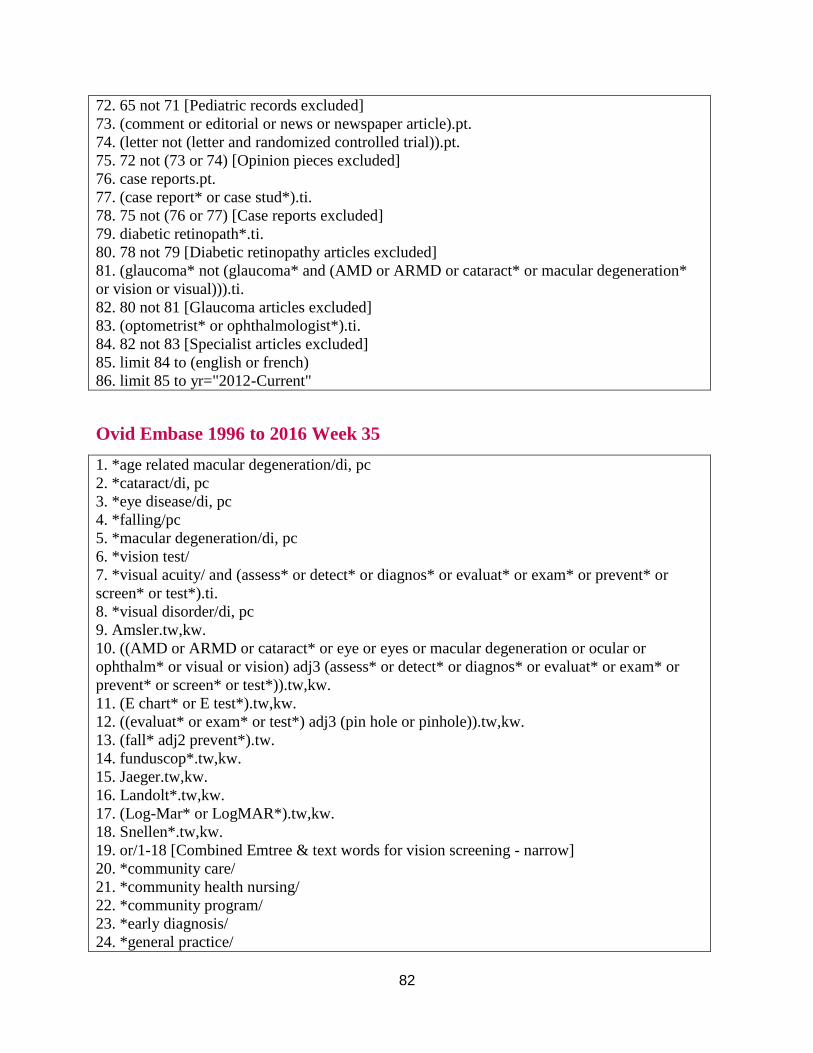
82
72. 65 not 71 [Pediatric records excluded]
73. (comment or editorial or news or newspaper article).pt.
74. (letter not (letter and randomized controlled trial)).pt.
75. 72 not (73 or 74) [Opinion pieces excluded]
76. case reports.pt.
77. (case report* or case stud*).ti.
78. 75 not (76 or 77) [Case reports excluded]
79. diabetic retinopath*.ti.
80. 78 not 79 [Diabetic retinopathy articles excluded]
81. (glaucoma* not (glaucoma* and (AMD or ARMD or cataract* or macular degeneration*
or vision or visual))).ti.
82. 80 not 81 [Glaucoma articles excluded]
83. (optometrist* or ophthalmologist*).ti.
84. 82 not 83 [Specialist articles excluded]
85. limit 84 to (english or french)
86. limit 85 to yr="2012-Current"
Ovid Embase 1996 to 2016 Week 35
1. *age related macular degeneration/di, pc
2. *cataract/di, pc
3. *eye disease/di, pc
4. *falling/pc
5. *macular degeneration/di, pc
6. *vision test/
7. *visual acuity/ and (assess* or detect* or diagnos* or evaluat* or exam* or prevent* or
screen* or test*).ti.
8. *visual disorder/di, pc
9. Amsler.tw,kw.
10. ((AMD or ARMD or cataract* or eye or eyes or macular degeneration or ocular or
ophthalm* or visual or vision) adj3 (assess* or detect* or diagnos* or evaluat* or exam* or
prevent* or screen* or test*)).tw,kw.
11. (E chart* or E test*).tw,kw.
12. ((evaluat* or exam* or test*) adj3 (pin hole or pinhole)).tw,kw.
13. (fall* adj2 prevent*).tw.
14. funduscop*.tw,kw.
15. Jaeger.tw,kw.
16. Landolt*.tw,kw.
17. (Log-Mar* or LogMAR*).tw,kw.
18. Snellen*.tw,kw.
19. or/1-18 [Combined Emtree & text words for vision screening - narrow]
20. *community care/
21. *community health nursing/
22. *community program/
23. *early diagnosis/
24. *general practice/
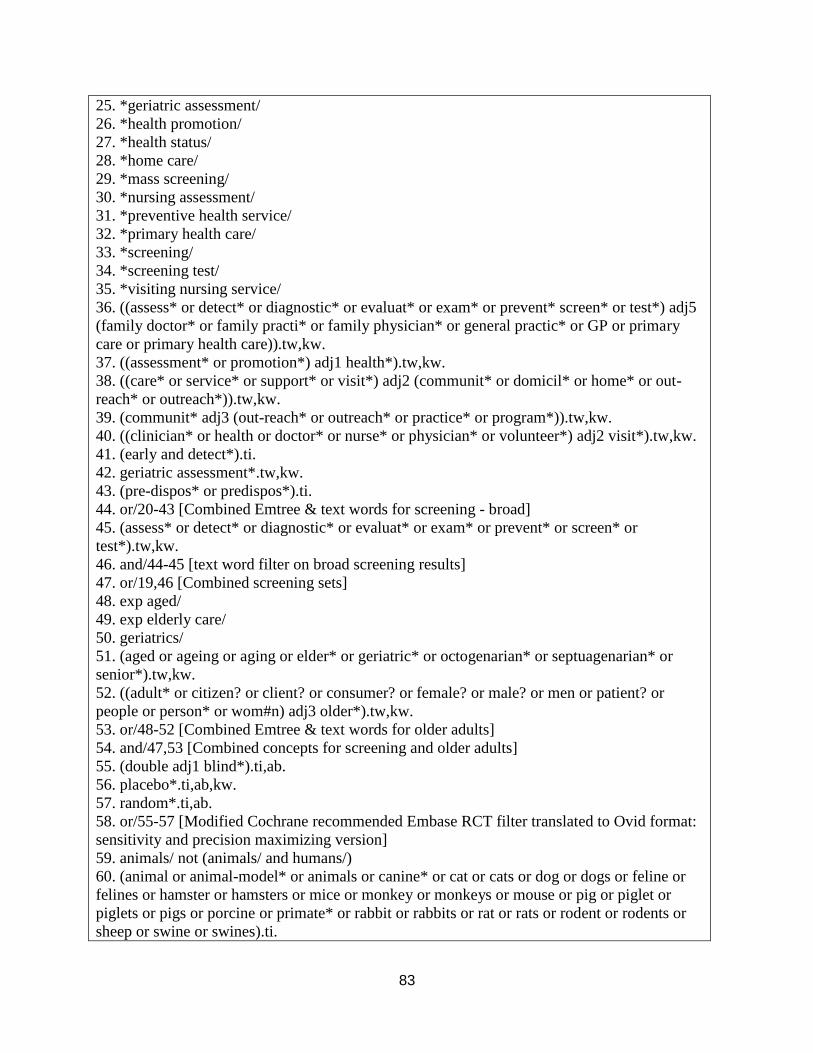
83
25. *geriatric assessment/
26. *health promotion/
27. *health status/
28. *home care/
29. *mass screening/
30. *nursing assessment/
31. *preventive health service/
32. *primary health care/
33. *screening/
34. *screening test/
35. *visiting nursing service/
36. ((assess* or detect* or diagnostic* or evaluat* or exam* or prevent* screen* or test*) adj5
(family doctor* or family practi* or family physician* or general practic* or GP or primary
care or primary health care)).tw,kw.
37. ((assessment* or promotion*) adj1 health*).tw,kw.
38. ((care* or service* or support* or visit*) adj2 (communit* or domicil* or home* or out-
reach* or outreach*)).tw,kw.
39. (communit* adj3 (out-reach* or outreach* or practice* or program*)).tw,kw.
40. ((clinician* or health or doctor* or nurse* or physician* or volunteer*) adj2 visit*).tw,kw.
41. (early and detect*).ti.
42. geriatric assessment*.tw,kw.
43. (pre-dispos* or predispos*).ti.
44. or/20-43 [Combined Emtree & text words for screening - broad]
45. (assess* or detect* or diagnostic* or evaluat* or exam* or prevent* or screen* or
test*).tw,kw.
46. and/44-45 [text word filter on broad screening results]
47. or/19,46 [Combined screening sets]
48. exp aged/
49. exp elderly care/
50. geriatrics/
51. (aged or ageing or aging or elder* or geriatric* or octogenarian* or septuagenarian* or
senior*).tw,kw.
52. ((adult* or citizen? or client? or consumer? or female? or male? or men or patient? or
people or person* or wom#n) adj3 older*).tw,kw.
53. or/48-52 [Combined Emtree & text words for older adults]
54. and/47,53 [Combined concepts for screening and older adults]
55. (double adj1 blind*).ti,ab.
56. placebo*.ti,ab,kw.
57. random*.ti,ab.
58. or/55-57 [Modified Cochrane recommended Embase RCT filter translated to Ovid format:
sensitivity and precision maximizing version]
59. animals/ not (animals/ and humans/)
60. (animal or animal-model* or animals or canine* or cat or cats or dog or dogs or feline or
felines or hamster or hamsters or mice or monkey or monkeys or mouse or pig or piglet or
piglets or pigs or porcine or primate* or rabbit or rabbits or rat or rats or rodent or rodents or
sheep or swine or swines).ti.

84
61. 58 not (59 or 60)
62. and/54,61 [RCT & animal filter applied]
63. exp juvenile/ not exp adult/
64. exp pediatrics/
65. (paediatr* or pediatr*).jx.
66. (adolesc* or babies or baby or boy* or child* or fetal or fetus or foet* or girl* or infan* or
juvenile* or kid or kids or neo-nat* or neonat* or new-born* or newborn* or paediatr* or
pediatr* or preadolesc* or prepubesc* or preteen* or pubescen* or teen* or toddler* or
youth*).tw,kw.
67. or/63-66 [Combined Emtree & textwords for pediatric records]
68. 62 not 67 [Pediatric records excluded]
69. (conference* or editorial or letter).pt.
70. 68 not 69 [Publication types excluded]
71. case report/
72. (case report* or case stud*).ti.
73. 70 not (71 or 72) [Case reports excluded]
74. diabetic retinopath*.ti.
75. 73 not 74 [Diabetic retinopathy articles excluded]
76. (glaucoma* not (glaucoma* and (AMD or ARMD or cataract* or macular degeneration*
or vision or visual))).ti.
77. 75 not 76 [Glaucoma articles excluded]
78. (optometrist* or ophthalmologist*).ti.
79. 77 not 78 [Specialist articles excluded]
80. limit 79 to (english or french)
81. limit 80 to yr="2012-Current"
82. remove duplicates from 81
Cochrane Library via Wiley
ID Search
#1 [mh "Accidental Falls"/PC]
#2 [mh ^Cataract] and (assess* or detect* or diagnos* or evaluat* or exam* or prevent* or
screen* or test*):ti,ab,kw
#3 [mh ^"Eye Diseases"/DI,PC]
#4 [mh "Macular Degeneration"/DI,PC]
#5 [mh "Vision Disorders" [mj]/DI,PC]
#6 [mh ^"Vision, Screening"]
#7 [mh ^"Vision Tests"]
#8 [mh "Visual Acuity"] and (assess* or detect* or diagnos* or evaluat* or exam* or
prevent* or screen* or test*):ti,ab,kw
#9 Amsler:ti,ab,kw
#10 ((AMD or ARMD or cataract* or eye or eyes or "macular degeneration" or ocular or
ophthalm* or visual or vision) near/3 (assess* or detect* or diagnos* or evaluat* or exam* or
prevent* or screen* or test*)):ti,ab,kw
#11 ("E chart*" or "E test*"):ti,ab,kw
#12 ((evaluat* or exam* or test*) near/3 ("pin hole" or pinhole)):ti,ab,kw

85
#13 (fall* near/2 prevent*):ti
#14 funduscop*:ti,ab,kw
#15 Jaeger:ti,ab,kw
#16 Landolt*:ti,ab,kw
#17 (Log-Mar* or LogMAR*):ti,ab,kw
#18 Snellen*:ti,ab,kw
#19 133-#18
#20 [mh ^"Community Health Services"]
#21 [mh ^"Community Health Workers"]
#22 [mh ^"Early Diagnosis"]
#23 [mh ^"Family Practice"]
#24 [mh ^"Geriatric Assessment"]
#25 [mh ^"Health Promotion"]
#26 [mh ^"Health Status"]
#27 [mh ^"Home Care Services"]
#28 [mh ^"Home Health Nursing"]
#29 [mh ^"House Calls"]
#30 [mh ^"Mass Screening"]
#31 [mh ^"Nurses, Community Health"]
#32 [mh ^"Nursing Assessment"]
#33 [mh ^"Office Visits"]
#34 [mh ^"Primary Health Care"]
#35 [mh ^"Preventive Health Services"]
#36 ((assess* or detect* or diagnos* or evaluat* or exam* or screen* or surveill* or test*)
near/5 (family doctor* or "family practi*" or "family physician*" or "general practic*" or GP or
"primary care" or "primary health care")):ti,ab,kw
#37 ((assessment* or education or promotion*) near/1 health*):ti,ab,kw
#38 ((care* or service* or support* or visit*) near/2 (communit* or domicil* or home* or out-
reach* or outreach*)):ti,ab,kw
#39 (communit* near/3 (out-reach* or outreach* or practice* or program*)):ti,ab,kw
#40 ((clinician* or health or doctor* or nurse* or physician* or volunteer*) near/2
visit*):ti,ab,kw
#41 (early and detect*):ti
#42 "geriatric assessment*":ti,ab,kw
#43 (pre-dispos* or predispos*):ti,ab,kw
#44 {or #20-#43}
#45 (assess* or detect* or diagnostic* or evaluat* or exam* or prevent* or screen* or
test*):ti,ab
#46 #44 and #45
#47 #19 or #46
#48 [mh Aged]
#49 [mh ^Geriatrics]
#50 [mh ^"Health Services for the Aged"]
#51 (aged or ageing or aging or elder* or geriatric* or octogenarian* or septuagenarian* or
senior*):ti,ab,kw
#52 ((adult* or citizen* or client* or consumer* or female* or male* or men or patient* or
86
people or person* or wom?n) near/3 older*):ti,ab,kw
#53 134-#52
#54 {and #47, #53}
#55 ([mh Adolescent] or [mh Child] or [mh Infant]) not [mh Adult]
#56 [mh ^"Adolescent Medicine"]
#57 [mh Pediatrics]
#58 (paediatr* or pediatr*):so
#59 (adolesc* or babies or baby or boy* or child* or fetal or fetus or foet* or girl* or infan*
or juvenile* or kid or kids or neo-nat* or neonat* or new-born* or newborn* or paediatr* or
pediatr* or preadolesc* or prepubesc* or preteen* or pubescen* or teen* or toddler* or
youth*):ti,ab,kw
#60 135-#59
#61 #54 not #60
#62 "diabetic retinopath*":ti
#63 #61 not #62
#64 (glaucoma* not (glaucoma* and (AMD or ARMD or cataract* or "macular
degeneration*" or vision or visual))):ti
#65 #63 not #64
#66 (optometrist* or ophthalmologist*):ti
#67 #65 not #66
#68 #65 not #66 Publication Year from 2012 to 2016, in Trials
CINAHL Plus with Full Text via EBSCOhost (1937 to the present)
S1. (MM "Accidental Falls/PC")
S2. (MM "Cataract/DI/PC")
S3. (MM "Eye Diseases/DI/PC")
S4. (MM "Macular Degeneration/DI/PC")
S5. (MM "Vision Disorders/DI/PC")
S6. (MH "Vision Screening")
S7. (MH "Vision Tests")
S8. (MH "Visual Acuity/EV")
S9. Amsler
S10. ((AMD or ARMD or cataract* or eye or eyes or "macular degeneration" or ocular or
ophthalm* or visual or vision) N3 (assess* or detect* or diagnos* or evaluat* or exam* or
prevent* or screen* or test*))
S11. ("E chart*" or "E test*")
S12. ((evaluat* or exam* or test*) N3 ("pin hole" or pinhole))
S13. TI (fall* N2 prevent*)
S14. Jaeger
S15. Landolt*
S16. (Log-Mar* or LogMAR*)
S17. Snellen*
S18. S1 OR S2 OR S3 OR S4 OR S5 OR S6 OR S7 OR S8 OR S9 OR S10 OR S11 OR S12 OR
S13 OR S14 OR S15 OR S16 OR S17

87
S19. (MH "Community Health Nursing")
S20. (MH "Community Health Services")
S21. (MH "Community Health Workers")
S22. (MH "Early Diagnosis")
S23. (MH "Family Practice")
S24. (MH "Geriatric Assessment+")
S25. (MH "Health Promotion")
S26. (MH "Health Screening")
S27. (MH "Health Status")
S28. (MH "Home Health Care")
S29. (MH "Home Nursing, Professional")
S30. (MH "Home Visits")
S31. (MH "Nursing Assessment")
S32. (MH "Office Visits")
S33. (MH "Primary Health Care")
S34. (MH "Preventive Health Care")
S35. ((assess* or detect* or diagnos* or evaluat* or exam* or screen* or surveill* or test*) N5
("family doctor*" or "family practi*" or "family physician*" or "general practic*" or GP or
"primary care" or "primary health care"))
S36. ((assessment* or education or promotion*) N1 health*)
S37. ((care* or service* or support* or visit*) N2 (communit* or domicil* or home* or out-
reach* or outreach*))
S38. (communit* N3 (out-reach* or outreach* or practice* or program*))
S39. ((clinician* or health or doctor* or nurse* or physician* or volunteer*) N2 visit*)
S40. TI (early and detect*)
S41. "geriatric assessment*"
S42. TI (pre-dispos* or predispos*)
S43. S19 OR S20 OR S21 OR S22 OR S23 OR S24 OR S25 OR S26 OR S27 OR S28 OR S29
OR S30 OR S31 OR S32 OR S33 OR S34 OR S35 OR S36 OR S37 OR S38 OR S39 OR S40
OR S41 OR S42
S44. TI (assess* or detect* or diagnostic* or evaluat* or exam* or prevent* or screen* or test*)
S45. S43 AND S44
S46. S18 OR S45
S47. (MH "Aged+")
S48. (MH "Geriatrics")
S49. (MH "Health Services for the Aged")
S50. (aged or ageing or aging or elder* or geriatric* or octogenarian* or septuagenarian* or
senior*)
S51. ((adult* or citizen* or client* or consumer* or female* or male* or men or patient* or
people or person* or wom?n) N3 older*)
S52. S47 OR S48 OR S49 OR S50 OR S51
S53. S46 AND S52
S54. (MH "Clinical Trials+")
S55. (MH "Random Assignment")
S56. PT Clinical trial
S57. TX (doubl* N1 (blind* or mask*))
88
S58. TX (clinic* N1 trial*)
S59. TX (singl* N1 (blind* or mask*))
S60. TX (trebl* N1 (blind* or mask*))
S61. TX (tripl* N1 (blind* or mask*))
S62. TX ("random* allocat*")
S63. TX ("randomi* control* trial*")
S64. S54 OR S55 OR S56 OR S57 OR S58 OR S59 OR S60 OR S61 OR S62 OR S63 [Modified
SIGN RCT filter: http://www.sign.ac.uk/methodology/filters.html#random]
S65. ((MH "Vertebrates+") NOT MH Human)
S66. TI (animal or animal-model* or animals or canine* or cat or cats or dog or dogs or feline or
felines or hamster or hamsters or mice or monkey or monkeys or mouse or pig or piglet or piglets
or pigs or porcine or primate* or rabbit or rabbits or rat or rats or rodent or rodents or sheep or
swine or swines)
S67. S64 NOT (S65 OR S66)
S68. S53 AND S67
S69. (((MH "Adolescents+") OR (MH "Child+") OR (MH "Infant+")) NOT (MH "Adult+")
S70. (MH "Adolescent Medicine")
S71. (MH "Pediatrics+")
S72. SO (paediatr* or pediatr*)
S73. (adolesc* or babies or baby or boy* or child* or fetal or fetus or foet* or girl* or infan* or
juvenile* or kid or kids or neo-nat* or neonat* or new-born* or newborn* or paediatr* or
pediatr* or preadolesc* or prepubesc* or preteen* or pubescen* or teen* or toddler* or youth*)
S74. S69 OR S70 OR S71 OR S72 OR S73
S75. S68 NOT S74
S76. TI (comment * or editor* or letter*)
S77. PT (Commentary or Editorial or Letter)
S78. S75 NOT (S76 OR S77)
S79. PT "Case Study"
S80. TI ("case report*" or "case stud*")
S81. S78 NOT (S79 OR S80)
S82. TI "diabetic retinopath*"
S83. S81 NOT S82
S84. TI (glaucoma* NOT (glaucoma* and (AMD or ARMD or cataract* or macular
degeneration* or vision or visual)))
S85. S83 NOT S84
S86. TI (optometrist* or ophthalmologist*)
S87. S85 NOT S86
S88. S85 NOT S86 – Published Date: 20120101-20161231; Language: English, French
Epub Ahead of Print, In-Process & Other Non-Indexed Citations, Ovid
MEDLINE(R) Daily and Ovid MEDLINE(R) 1946 to Present SET 1: Vision Screening – Narrow
"Accidental Falls/prevention and control"[mj:noexp] OR "Eye Diseases/diagnosis"[mj:noexp]
OR "Eye Diseases/prevention and control"[mj:noexp] OR "Vision
Disorders/diagnosis"[mj:noexp] OR "cataract/diagnosis"[mj:noexp] OR "cataract/prevention and
control"[mj:noexp] OR "Eye Diseases/diagnosis"[mj:noexp] OR "Eye Diseases/prevention and
89
control"[mj:noexp] OR "Macular Degeneration/diagnosis"[mj:noexp] OR "Macular
Degeneration/prevention and control"[mj:noexp] OR "Vision Disorders/diagnosis"[mj:noexp]
OR "Vision Disorders/prevention and control"[mj:noexp] OR "Vision Screening"[mh:noexp] OR
"Vision Tests"[mh:noexp] OR ("Visual Acuity"[mh] AND (assess[tiab] OR assessed[tiab] OR
assesses[tiab] OR assessing[tiab] OR assessment[tiab] OR assessments[tiab] OR detect[tiab] OR
detected[tiab] OR detection[tiab] OR detecting[tiab] OR detects[tiab] OR diagnose[tiab] OR
diagnosed[tiab] OR diagnoses[tiab] OR diagnosing[tiab] OR diagnosis[tiab] OR evaluate[tiab]
OR evaluated[tiab] OR evaluation[tiab] OR evaluations[tiab] OR evaluating[tiab] OR exam[tiab]
OR examinate[tiab] OR examinated[tiab] OR examination[tiab] OR examinations[tiab] OR
exams[tiab] OR prevent[tiab] OR prevented[tiab] OR prevents[tiab] OR preventing[tiab] OR
prevention[tiab] OR screen[tiab] OR screened[tiab] OR screening[tiab] OR screens[tiab] OR
test[tiab] OR tested[tiab] OR testing[tiab] OR tests[tiab])) OR Amsler[tiab] OR ((AMD[tiab] OR
ARMD[tiab] OR cataract[tiab] OR cataracts[tiab] OR eye[tiab] OR eyes[tiab] OR "macular
degeneration"[tiab] OR ocular[tiab] OR ophthalmic[tiab] OR ophthalmologic[tiab] OR
ophthalmological[tiab] OR visual[tiab] OR vision[tiab]) AND (assess[tiab] OR assessed[tiab]
OR assesses[tiab] OR assessing[tiab] OR assessment[tiab] OR assessments[tiab] OR detect[tiab]
OR detected[tiab] OR detection[tiab] OR detecting[tiab] OR detects[tiab] OR diagnose[tiab] OR
diagnosed[tiab] OR diagnoses[tiab] OR diagnosing[tiab] OR diagnosis[tiab] OR evaluate[tiab]
OR evaluated[tiab] OR evaluation[tiab] OR evaluations[tiab] OR evaluating[tiab] OR exam[tiab]
OR examinate[tiab] OR examinated[tiab] OR examination[tiab] OR examinations[tiab] OR
exams[tiab] OR prevent[tiab] OR prevented[tiab] OR prevents[tiab] OR preventing[tiab] OR
prevention[tiab] OR screen[tiab] OR screened[tiab] OR screening[tiab] OR screens[tiab] OR
test[tiab] OR tested[tiab] OR testing[tiab] OR tests[tiab])) OR "E chart"[tiab] OR "E
charts"[tiab] OR "E test"[tiab] OR "E tests"[tiab] OR ((evaluate[tiab] OR evaluates[tiab] OR
evaluated[tiab] OR evaluation[tiab] OR evaluations[tiab] OR evaluating[tiab] OR exam[tiab] OR
exams[tiab] OR examinate[tiab] OR examinated[tiab] OR examination[tiab] OR
examinations[tiab] OR exams[tiab] OR test[tiab] OR tested[tiab] OR testing[tiab] OR tests[tiab])
AND ("pin hole"[tiab] OR pinhole[tiab])) OR ((fall[tiab] OR falls[tiab]) AND (prevent[tiab] OR
prevented[tiab] OR prevents[tiab] OR preventing[tiab] OR prevention[tiab])) OR
funduscopic[tiab] OR funduscopy[tiab] OR Jaeger[tiab] OR Landolt[tiab] OR "Log Mar"[tiab]
OR LogMAR[tiab] OR Snellen[tiab]
SET 2: Community Screening – Broad
"Community Health Services"[mh:noexp] OR "Community Health Workers"[mh:noexp] OR
"Early Diagnosis"[mh:noexp] OR "Family Practice"[mh:noexp] OR "Geriatric
Assessment"[mh:noexp] OR "Health Promotion"[mh:noexp] OR "Health Status"[mh:noexp] OR
"Home Care Services"[mh:noexp] OR "Home Health Nursing"[mh:noexp] OR "House
Calls"[mh:noexp] OR "Mass Screening"[mh:noexp] OR "Nurses, Community
Health"[mh:noexp] OR "Nursing Assessment"[mh:noexp] OR "Office Visits"[mh:noexp] OR
"Primary Health Care"[mh:noexp] OR "Preventive Health Services"[mh:noexp] OR
((assess[tiab] OR assessed[tiab] OR assesses[tiab] OR assessing[tiab] OR assessment[tiab] OR
assessments[tiab] OR detect[tiab] OR detected[tiab] OR detection[tiab] OR detecting[tiab] OR
detects[tiab] OR diagnostic[tiab] OR evaluate[tiab] OR evaluated[tiab] OR evaluation[tiab] OR
evaluations[tiab] OR evaluating[tiab] OR exam[tiab] OR examinate[tiab] OR examinated[tiab]
OR examination[tiab] OR examinations[tiab] OR exams[tiab] OR prevent[tiab] OR
prevented[tiab] OR preventing[tiab] OR prevention[tiab] OR screen[tiab] OR screened[tiab] OR

90
screening[tiab] OR screens[tiab] OR test[tiab] OR tested[tiab] OR testing[tiab] OR tests[tiab])
AND ("family doctor"[tiab] OR "family doctors"[tiab] OR "family practice"[tiab] OR "family
physician"[tiab] OR "family physicians"[tiab] OR "general practice"[tiab] OR "general
practitioner"[tiab] OR "general practitioners"[tiab] OR GP[tiab] OR "primary care"[tiab] OR
"primary health care"[tiab] OR "primary healthcare"[tiab])) OR "community care"[tiab] OR
"community out reach"[tiab] OR "community outreach"[tiab] OR "community practice"[tiab]
OR "community program"[tiab] OR "community programs"[tiab] OR "community
services"[tiab] OR "community support"[tiab] OR (early[ti] AND (detect[ti] OR detected[ti] OR
detecting[ti] OR detection[ti] OR detects[ti])) OR "geriatric assessment"[tiab] OR "geriatric
assessments"[tiab] OR "health assessment"[tiab] OR "health assessments"[tiab] OR "health
education"[tiab] OR "health promotion"[tiab] OR "home care"[tiab] OR "home support"[tiab]
OR "home visit"[tiab] OR "home visits"[tiab] OR "pre disposed"[ti] OR "pre disposition"[ti] OR
predisposed[ti] OR predisposition[ti]
SET 3: Text words to narrow broad screening set
assess[tiab] OR assessed[tiab] OR assesses[tiab] OR assessing[tiab] OR assessment[tiab] OR
assessments[tiab] OR detect[tiab] OR detected[tiab] OR detection[tiab] OR detecting[tiab] OR
detects[tiab] OR diagnostic[tiab] OR evaluate[tiab] OR evaluated[tiab] OR evaluation[tiab] OR
evaluations[tiab] OR evaluating[tiab] OR exam[tiab] OR examinate[tiab] OR examinated[tiab]
OR examination[tiab] OR examinations[tiab] OR exams[tiab] OR prevent[tiab] OR
prevented[tiab] OR preventing[tiab] OR prevention[tiab] or prevents[tiab] OR screen[tiab] OR
screened[tiab] OR screening[tiab] OR screens[tiab] OR test[tiab] OR tested[tiab] OR
testing[tiab] OR tests[tiab]
SET 4: Text word filter on broad screening results
#2 AND #3
SET 5: Combined concepts for vision and community-based screening
#1 OR #4
SET 6: Older adults
"aged"[MeSH Terms] OR "geriatrics"[MeSH Terms:noexp] OR "Health Services for the
Aged"[mh:noexp] OR aged[tiab] OR ageing[tiab] OR aging[tiab] OR elder[tiab] OR elders[tiab]
OR geriatric[tiab] OR geriatrics[tiab] OR octogenarian[tiab] OR octogenarians[tiab] OR "older
adult"[tiab] OR "older adults"[tiab] OR "older clients"[tiab] OR "older consumers"[tiab] OR
"older females"[tiab] OR "older males"[tiab] OR "older patients"[tiab] OR "older persons"[tiab]
OR "older people"[tiab] OR septuagenarian[tiab] OR septuagenarians[tiab] OR senior[tiab] OR
seniors[tiab]
Set 7: Combined concepts for screening and older adults
#5 AND #6
SET 8: Modified Cochrane highly sensitive RCT filter: sensitivity and precision maximizing
version
"clinical trials as topic"[mh:noexp] OR "controlled clinical trial"[pt] OR "randomized controlled
trial"[pt] OR placebo[tiab] OR randomised[tiab] OR randomized[tiab] OR randomly[tiab] OR
91
trial[ti]
Set 9: RCT filter appled to screening and older adults
#7 AND #8
Set 10: Animal filter
("animals"[MeSH Terms] NOT "humans"[MeSH Terms]) OR animal[ti] OR animals[ti] OR
canine[ti] OR cat[ti] OR cats[ti] OR dog[ti] OR dogs[ti] OR feline[ti] OR felines[ti] OR
hamster[ti] OR hamsters[ti] OR mice[ti] OR monkey[ti] OR monkeys[ti] OR mouse[ti] OR
pig[ti] OR piglet[ti] OR piglets[ti] OR pigs[ti] OR porcine[ti] OR primate[ti] OR primates[ti] OR
rabbit[ti] OR rabbits[ti] OR rat[ti] OR rats[ti] OR rodent[ti] OR rodents[ti] OR sheep[ti] OR
swine[ti] OR swines[ti]
Set 11: Animal filter applied to combined results
#9 NOT #10
SET 12: Child filter
(("adolescent"[MeSH Terms] OR "child"[MeSH Terms] OR "infant"[MeSH Terms]) NOT
"adult"[MeSH Terms]) OR "Adolescent Medicine"[mh] OR "pediatrics"[MeSH Terms] OR
adolescence[tiab] OR adolescent[tiab] OR adolescents[tiab] OR baby[tiab] OR babies[tiab] OR
child[tiab] OR childhood[tiab] OR children[tiab] OR childrens[tiab] OR childs[tiab] OR
infancy[tiab] OR infant[tiab] OR infants[tiab] OR neonatal[tiab] OR neonatology[tiab] OR
neonate[tiab] OR neonates[tiab] OR "new born"[tiab] OR "new borns"[tiab] OR newborn[tiab]
OR newborns[tiab] OR paediatric[tiab] OR paediatrician[tiab] OR paediatricians[tiab] OR
peadiatric[tiab] OR peadiatricians[tiab] OR pediatric[tiab] OR pediatrician[tiab] OR
pediatricians[tiab] OR "pre mature"[tiab] OR premature[tiab] OR "pre term"[tiab] OR
preterm[tiab] OR preschool[tiab] OR preschooler[tiab] OR preschoolers[tiab] OR
prepubescence[tiab] OR prepubescent[tiab] OR prepubescents[tiab] OR teen[tiab] OR
teenaged[tiab] OR teenager[tiab] OR teenagers[tiab] OR teens[tiab] OR toddler[tiab] OR
toddlers[tiab] OR youth[tiab] OR youths[tiab]
SET 13: Child filter applied to combined results
#11 NOT #12
SET 14: Opinion piece filter
comment[pt] OR editorial[pt] OR (letter[pt] NOT (letter[pt] AND "randomized controlled
trial"[pt])) OR news[pt] OR "newspaper article"[pt]
SET 15: Opinion piece filter applied to combined results
#13 NOT #14
SET 16: Case reports filter
"case reports"[pt] OR "case report"[ti] OR "case reports"[ti] OR "case study"[ti] OR "case
studies"[ti]
SET 17: Case reports filters applied to combined results

92
#15 NOT #16
SET 18: Diabetic retinopathy filter
"diabetic retinopathies"[ti] OR "diabetic retinopathy"[ti]
SET 19: Diabetic retinopathy filter applied to combined results
#17 NOT #18
SET 20: Glaucoma filter
(glaucoma[ti] OR glaucomas[ti]) NOT ((glaucoma[ti] OR glaucomas[ti]) AND (AMD[ti] OR
ARMD[ti] OR cataract[ti] OR cataracts[ti] OR "macular degeneration"[ti] OR vision[ti] OR
visual[ti]))
SET 21: Glaucoma filter applied to combined results
#19 NOT #20
SET 22: Specialist filter
optometrist[ti] or optometrists[ti] or ophthalmologist[ti] or ophthalmologists[ti]
SET 23: Specialist filter applied to combined results
#21 NOT #22
SET 24: Language limits
#21 NOT #22 Filters: English; French
SET 25: Electronic Publications filter
(publisher[sb] NOT pubstatusnihms NOT pubstatuspmcsd NOT pmcbook) OR
(pubstatusaheadofprint)
SET 26: Electronic Publications filter applied to final results
#24 AND #25
PubMed search on one line:
((((((((((("Accidental Falls/prevention and control"[mj:noexp] OR "Eye
Diseases/diagnosis"[mj:noexp] OR "Eye Diseases/prevention and control"[mj:noexp] OR
"Vision Disorders/diagnosis"[mj:noexp] OR "cataract/diagnosis"[mj:noexp] OR
"cataract/prevention and control"[mj:noexp] OR "Eye Diseases/diagnosis"[mj:noexp] OR "Eye
Diseases/prevention and control"[mj:noexp] OR "Macular Degeneration/diagnosis"[mj:noexp]
OR "Macular Degeneration/prevention and control"[mj:noexp] OR "Vision
Disorders/diagnosis"[mj:noexp] OR "Vision Disorders/prevention and control"[mj:noexp] OR
"Vision Screening"[mh:noexp] OR "Vision Tests"[mh:noexp] OR ("Visual Acuity"[mh] AND
(assess[tiab] OR assessed[tiab] OR assesses[tiab] OR assessing[tiab] OR assessment[tiab] OR
assessments[tiab] OR detect[tiab] OR detected[tiab] OR detection[tiab] OR detecting[tiab] OR
detects[tiab] OR diagnose[tiab] OR diagnosed[tiab] OR diagnoses[tiab] OR diagnosing[tiab] OR
diagnosis[tiab] OR evaluate[tiab] OR evaluated[tiab] OR evaluation[tiab] OR evaluations[tiab]
OR evaluating[tiab] OR exam[tiab] OR examinate[tiab] OR examinated[tiab] OR

93
examination[tiab] OR examinations[tiab] OR exams[tiab] OR prevent[tiab] OR prevented[tiab]
OR prevents[tiab] OR preventing[tiab] OR prevention[tiab] OR screen[tiab] OR screened[tiab]
OR screening[tiab] OR screens[tiab] OR test[tiab] OR tested[tiab] OR testing[tiab] OR
tests[tiab])) OR Amsler[tiab] OR ((AMD[tiab] OR ARMD[tiab] OR cataract[tiab] OR
cataracts[tiab] OR eye[tiab] OR eyes[tiab] OR "macular degeneration"[tiab] OR ocular[tiab] OR
ophthalmic[tiab] OR ophthalmologic[tiab] OR ophthalmological[tiab] OR visual[tiab] OR
vision[tiab]) AND (assess[tiab] OR assessed[tiab] OR assesses[tiab] OR assessing[tiab] OR
assessment[tiab] OR assessments[tiab] OR detect[tiab] OR detected[tiab] OR detection[tiab] OR
detecting[tiab] OR detects[tiab] OR diagnose[tiab] OR diagnosed[tiab] OR diagnoses[tiab] OR
diagnosing[tiab] OR diagnosis[tiab] OR evaluate[tiab] OR evaluated[tiab] OR evaluation[tiab]
OR evaluations[tiab] OR evaluating[tiab] OR exam[tiab] OR examinate[tiab] OR
examinated[tiab] OR examination[tiab] OR examinations[tiab] OR exams[tiab] OR prevent[tiab]
OR prevented[tiab] OR prevents[tiab] OR preventing[tiab] OR prevention[tiab] OR screen[tiab]
OR screened[tiab] OR screening[tiab] OR screens[tiab] OR test[tiab] OR tested[tiab] OR
testing[tiab] OR tests[tiab])) OR "E chart"[tiab] OR "E charts"[tiab] OR "E test"[tiab] OR "E
tests"[tiab] OR ((evaluate[tiab] OR evaluates[tiab] OR evaluated[tiab] OR evaluation[tiab] OR
evaluations[tiab] OR evaluating[tiab] OR exam[tiab] OR exams[tiab] OR examinate[tiab] OR
examinated[tiab] OR examination[tiab] OR examinations[tiab] OR exams[tiab] OR test[tiab] OR
tested[tiab] OR testing[tiab] OR tests[tiab]) AND ("pin hole"[tiab] OR pinhole[tiab])) OR
((fall[tiab] OR falls[tiab]) AND (prevent[tiab] OR prevented[tiab] OR prevents[tiab] OR
preventing[tiab] OR prevention[tiab])) OR funduscopic[tiab] OR funduscopy[tiab] OR
Jaeger[tiab] OR Landolt[tiab] OR "Log Mar"[tiab] OR LogMAR[tiab] OR Snellen[tiab]) OR
(("Community Health Services"[mh:noexp] OR "Community Health Workers"[mh:noexp] OR
"Early Diagnosis"[mh:noexp] OR "Family Practice"[mh:noexp] OR "Geriatric
Assessment"[mh:noexp] OR "Health Promotion"[mh:noexp] OR "Health Status"[mh:noexp] OR
"Home Care Services"[mh:noexp] OR "Home Health Nursing"[mh:noexp] OR "House
Calls"[mh:noexp] OR "Mass Screening"[mh:noexp] OR "Nurses, Community
Health"[mh:noexp] OR "Nursing Assessment"[mh:noexp] OR "Office Visits"[mh:noexp] OR
"Primary Health Care"[mh:noexp] OR "Preventive Health Services"[mh:noexp] OR
((assess[tiab] OR assessed[tiab] OR assesses[tiab] OR assessing[tiab] OR assessment[tiab] OR
assessments[tiab] OR detect[tiab] OR detected[tiab] OR detection[tiab] OR detecting[tiab] OR
detects[tiab] OR diagnostic[tiab] OR evaluate[tiab] OR evaluated[tiab] OR evaluation[tiab] OR
evaluations[tiab] OR evaluating[tiab] OR exam[tiab] OR examinate[tiab] OR examinated[tiab]
OR examination[tiab] OR examinations[tiab] OR exams[tiab] OR prevent[tiab] OR
prevented[tiab] OR preventing[tiab] OR prevention[tiab] OR screen[tiab] OR screened[tiab] OR
screening[tiab] OR screens[tiab] OR test[tiab] OR tested[tiab] OR testing[tiab] OR tests[tiab])
AND ("family doctor"[tiab] OR "family doctors"[tiab] OR "family practice"[tiab] OR "family
physician"[tiab] OR "family physicians"[tiab] OR "general practice"[tiab] OR "general
practitioner"[tiab] OR "general practitioners"[tiab] OR GP[tiab] OR "primary care"[tiab] OR
"primary health care"[tiab] OR "primary healthcare"[tiab])) OR "community care"[tiab] OR
"community out reach"[tiab] OR "community outreach"[tiab] OR "community practice"[tiab]
OR "community program"[tiab] OR "community programs"[tiab] OR "community
services"[tiab] OR "community support"[tiab] OR (early[ti] AND (detect[ti] OR detected[ti] OR
detecting[ti] OR detection[ti] OR detects[ti])) OR "geriatric assessment"[tiab] OR "geriatric
assessments"[tiab] OR "health assessment"[tiab] OR "health assessments"[tiab] OR "health
education"[tiab] OR "health promotion"[tiab] OR "home care"[tiab] OR "home support"[tiab]

94
OR "home visit"[tiab] OR "home visits"[tiab] OR "pre disposed"[ti] OR "pre disposition"[ti] OR
predisposed[ti] OR predisposition[ti]) AND (assess[tiab] OR assessed[tiab] OR assesses[tiab]
OR assessing[tiab] OR assessment[tiab] OR assessments[tiab] OR detect[tiab] OR detected[tiab]
OR detection[tiab] OR detecting[tiab] OR detects[tiab] OR diagnostic[tiab] OR evaluate[tiab]
OR evaluated[tiab] OR evaluation[tiab] OR evaluations[tiab] OR evaluating[tiab] OR exam[tiab]
OR examinate[tiab] OR examinated[tiab] OR examination[tiab] OR examinations[tiab] OR
exams[tiab] OR prevent[tiab] OR prevented[tiab] OR preventing[tiab] OR prevention[tiab] OR
prevents[tiab] OR screen[tiab] OR screened[tiab] OR screening[tiab] OR screens[tiab] OR
test[tiab] OR tested[tiab] OR testing[tiab] OR tests[tiab]))) AND ("aged"[MeSH Terms] OR
"geriatrics"[MeSH Terms:noexp] OR "Health Services for the Aged"[mh:noexp] OR aged[tiab]
OR ageing[tiab] OR aging[tiab] OR elder[tiab] OR elders[tiab] OR geriatric[tiab] OR
geriatrics[tiab] OR octogenarian[tiab] OR octogenarians[tiab] OR "older adult"[tiab] OR "older
adults"[tiab] OR "older clients"[tiab] OR "older consumers"[tiab] OR "older females"[tiab] OR
"older males"[tiab] OR "older patients"[tiab] OR "older persons"[tiab] OR "older people"[tiab]
OR septuagenarian[tiab] OR septuagenarians[tiab] OR senior[tiab] OR seniors[tiab])) AND
("clinical trials as topic"[mh:noexp] OR "controlled clinical trial"[pt] OR "randomized controlled
trial"[pt] OR placebo[tiab] OR randomised[tiab] OR randomized[tiab] OR randomly[tiab] OR
trial[ti])) NOT (("animals"[MeSH Terms] NOT "humans"[MeSH Terms]) OR animal[ti] OR
animals[ti] OR canine[ti] OR cat[ti] OR cats[ti] OR dog[ti] OR dogs[ti] OR feline[ti] OR
felines[ti] OR hamster[ti] OR hamsters[ti] OR mice[ti] OR monkey[ti] OR monkeys[ti] OR
mouse[ti] OR pig[ti] OR piglet[ti] OR piglets[ti] OR pigs[ti] OR porcine[ti] OR primate[ti] OR
primates[ti] OR rabbit[ti] OR rabbits[ti] OR rat[ti] OR rats[ti] OR rodent[ti] OR rodents[ti] OR
sheep[ti] OR swine[ti] OR swines[ti])) NOT ((("adolescent"[MeSH Terms] OR "child"[MeSH
Terms] OR "infant"[MeSH Terms]) NOT "adult"[MeSH Terms]) OR "Adolescent
Medicine"[mh] OR "pediatrics"[MeSH Terms] OR adolescence[tiab] OR adolescent[tiab] OR
adolescents[tiab] OR baby[tiab] OR babies[tiab] OR child[tiab] OR childhood[tiab] OR
children[tiab] OR childrens[tiab] OR childs[tiab] OR infancy[tiab] OR infant[tiab] OR
infants[tiab] OR neonatal[tiab] OR neonatology[tiab] OR neonate[tiab] OR neonates[tiab] OR
"new born"[tiab] OR "new borns"[tiab] OR newborn[tiab] OR newborns[tiab] OR
paediatric[tiab] OR paediatrician[tiab] OR paediatricians[tiab] OR peadiatric[tiab] OR
peadiatricians[tiab] OR pediatric[tiab] OR pediatrician[tiab] OR pediatricians[tiab] OR "pre
mature"[tiab] OR premature[tiab] OR "pre term"[tiab] OR preterm[tiab] OR preschool[tiab] OR
preschooler[tiab] OR preschoolers[tiab] OR prepubescence[tiab] OR prepubescent[tiab] OR
prepubescents[tiab] OR teen[tiab] OR teenaged[tiab] OR teenager[tiab] OR teenagers[tiab] OR
teens[tiab] OR toddler[tiab] OR toddlers[tiab] OR youth[tiab] OR youths[tiab])) NOT
(comment[pt] OR editorial[pt] OR (letter[pt] NOT (letter[pt] AND "randomized controlled
trial"[pt])) OR news[pt] OR "newspaper article"[pt])) NOT ("case reports"[pt] OR "case
report"[ti] OR "case reports"[ti] OR "case study"[ti] OR "case studies"[ti])) NOT ("diabetic
retinopathies"[ti] OR "diabetic retinopathy"[ti])) NOT ((glaucoma[ti] OR glaucomas[ti]) NOT
((glaucoma[ti] OR glaucomas[ti]) AND (AMD[ti] OR ARMD[ti] OR cataract[ti] OR cataracts[ti]
OR "macular degeneration"[ti] OR vision[ti] OR visual[ti])))) NOT (optometrist[ti] OR
optometrists[ti] OR ophthalmologist[ti] OR ophthalmologists[ti]) AND ((English[lang] OR
French[lang]))) AND ((publisher[sb] NOT pubstatusnihms NOT pubstatuspmcsd NOT
pmcbook) OR (pubstatusaheadofprint))
95
APPENDIX C: Systematic Reviews Examined for Studies
1. Balzer K, Bremer M, Schramm S, et al. Falls prevention for the elderly. GMS Health Technology
Assessment. 2012;8:Doc01. doi: http://dx.doi.org/10.3205/hta000099. 2. Choi M, Hector M. Effectiveness of intervention programs in preventing falls: a systematic review of
recent 10 years and meta-analysis. J Am Med Dir Assoc. 2012 Feb;13(2):188.e13-21. doi:
http://dx.doi.org/10.1016/j.jamda.2011.04.022. PMID: 21680249. 3. Chou R, Dana T, Bougatsos C, et al. Screening for Impaired Visual Acuity in Older Adults: A Systematic
Review to Update the 2009 U.S. Preventive Services Task Force Recommendation. Rockville MD; 2016. 4. Deschodt M, Flamaing J, Haentjens P, et al. Impact of geriatric consultation teams on clinical outcome in
acute hospitals: a systematic review and meta-analysis. BMC Medicine. 2013;11:48. doi:
http://dx.doi.org/10.1186/1741-7015-11-48. PMID: 23433471. 5. Ekdahl AW, Sjostrand F, Ehrenberg A, et al. Frailty and comprehensive geriatric assessment organized as
CGA-ward or CGA-consult for older adult patients in the acute care setting: a systematic review and meta-
analysis. European Geriatric Medicine. 2015;6(6):523-40. doi:
http://dx.doi.org/10.1016/j.eurger.2015.10.007. 6. Gagnon C, Lafrance M. Prévention des chutes auprès des personnes âgées vivant à domicile: analyse des
données scientifiques et recommandations préliminaires à l'élaboration d'un guide de pratique clinique:
Institut national de santé publique du Québec; 2011. 7. Gillespie LD, Robertson MC, Gillespie WJ, et al. Interventions for preventing falls in older people living in
the community. Cochrane Database of Systematic Reviews. 2012;9:CD007146. doi:
http://dx.doi.org/10.1002/14651858.CD007146.pub3. 8. Goodwin VA, Abbott RA, Whear R, et al. Multiple component interventions for preventing falls and fall-
related injuries among older people: systematic review and meta-analysis. BMC Geriatrics. 2014;14:15.
doi: http://dx.doi.org/10.1186/1471-2318-14-15. PMID: 24495705. 9. Karlsson MK, Magnusson H, von Schewelov T, et al. Prevention of falls in the elderly--a review.
Osteoporos Int. 2013 Mar;24(3):747-62. doi: http://dx.doi.org/10.1007/s00198-012-2256-7. PMID:
23296743 10. Karlsson MK, Vonschewelov T, Karlsson C, et al. Prevention of falls in the elderly: a review. Scand J
Public Health. 2013 Jul;41(5):442-54. doi: http://dx.doi.org/10.1177/1403494813483215. PMID:
23554390. 11. Krogsboll LT, Jorgensen KJ, Gronhoj Larsen C, et al. General health checks in adults for reducing
morbidity and mortality from disease: Cochrane systematic review and meta-analysis. BMJ.
2012;345:e7191. doi: http://dx.doi.org/10.1136/bmj.e7191. PMID: 23169868. 12. Krogsboll LT, Jorgensen KJ, Gronhoj Larsen C, et al. General health checks in adults for reducing
morbidity and mortality from disease. Cochrane Database of Systematic Reviews. 2012;10:CD009009. doi:
http://dx.doi.org/10.1002/14651858.CD009009.pub2. 13. Lood Q, Haggblom-Kronlof G, Dahlin-Ivanoff S. Health promotion programme design and efficacy in
relation to ageing persons with culturally and linguistically diverse backgrounds: a systematic literature
review and meta-analysis. BMC Health Services Research. 2015;15:560. doi:
http://dx.doi.org/10.1186/s12913-015-1222-4. PMID: 26674647.
96
14. Mayo-Wilson E, Grant S, Burton J, et al. Preventive home visits for mortality, morbidity, and
institutionalization in older adults: a systematic review and meta-analysis. PLoS ONE. 2014;9(3):e89257.
doi: http://dx.doi.org/10.1371/journal.pone.0089257. PMID: 24622676. 15. Nyman SR, Victor CR. Older people's participation in and engagement with falls prevention interventions
in community settings: an augment to the Cochrane systematic review. Age & Ageing. 2012 Jan;41(1):16-
23. doi: http://dx.doi.org/10.1093/ageing/afr103. PMID: 21875865. 16. Ploeg J, Feightner J, Hutchison B, et al. Effectiveness of preventive primary care outreach interventions
aimed at older people: meta-analysis of randomized controlled trials. Can Fam Physician. 2005
Sep;51:1244-5. PMID: 16926937. 17. Si S, Moss JR, Sullivan TR, et al. Effectiveness of general practice-based health checks: a systematic
review and meta-analysis. British Journal of General Practice. 2014 Jan;64(618):e47-53. doi:
http://dx.doi.org/10.3399/bjgp14X676456. PMID: 24567582. 18. Skelton DA, Howe TE, Ballinger C, et al. Environmental and behavioural interventions for reducing
physical activity limitation in community-dwelling visually impaired older people. Cochrane Database of
Systematic Reviews. 2013(6):CD009233. 19. Smeeth L, Iliffe S. Community screening for visual impairment in the elderly. Cochrane Database Syst
Rev. 2006 Jul 19(3):CD001054. doi: 10.1002/14651858.CD001054.pub2. PMID: 16855956. 20. Stubbs B, Brefka S, Denkinger MD. What works to prevent falls in community-dwelling older adults?
umbrella review of meta-analyses of randomized controlled trials. Physical Therapy. 2015 Aug;95(8):1095-
110. doi: http://dx.doi.org/10.2522/ptj.20140461. 21. Tappenden P, Campbell F, Rawdin A, et al. The clinical effectiveness and cost-effectiveness of home-
based, nurse-led health promotion for older people: a systematic review. Health Technology Assessment
(Winchester, England). 2012;16(20):1-72. doi: http://dx.doi.org/10.3310/hta16200. 22. Tourigny A, Bedard A, Laurin D, et al. Preventive home visits for older people: a systematic review. Can J
Aging. 2015 Dec;34(4):506-23. doi: http://dx.doi.org/10.1017/S0714980815000446. PMID: 26526379. 23. Tricco AC, Cogo E, Holroyd-Leduc J, et al. Efficacy of falls prevention interventions: protocol for a
systematic review and network meta-analysis. Syst Rev. 2013;2:38. doi: http://dx.doi.org/10.1186/2046-
4053-2-38. PMID: 23738619 24. You EC, Dunt D, Doyle C, et al. Effects of case management in community aged care on client and carer
outcomes: a systematic review of randomized trials and comparative observational studies. BMC Health
Services Research. 2012;12:395. doi: http://dx.doi.org/10.1186/1472-6963-12-395. 25. Zhang XY, Shuai J, Li LP. Vision and relevant risk factor interventions for preventing falls among older
people: a network meta-analysis. Scientific Reports. 2015;5:10559. doi:
http://dx.doi.org/10.1038/srep10559.
97
APPENDIX D: List of Excluded Studies
Language
1. Dam VH, Bleijenberg N, Numans ME, et al. [Proactive and structured care for the elderly in primary care].
Tijdschrift voor gerontologie en geriatrie; 2013. p. 81-9.
2. Inaba Y, Obuchi S, Arai T, et al. [Effects of exercise intervention on exercise behavior in community-dwelling
elderly subjects: a randomized controlled trial]. Nihon Ronen Igakkai zasshi. Japanese journal of geriatrics;
2013. p. 788-96.
3. Józefowski P, Borowska A, Szafraniec R, et al. [The impact of group therapeutic exercises on postural stability
and the risk of falls of postmenopausal women]. Wiadomo?ci lekarskie (Warsaw, Poland : 1960); 2015. p.
132-8.
4. Metzelthin SF, Rossum E, Witte LP, et al. Frail elderly people living at home; effects of an interdisciplinary
primary care programme. [Dutch]. Nederlands tijdschrift voor geneeskunde; 2014.
5. Pröfener F, Anders J, Dapp U, et al. Acceptance of preventive home visits among frail elderly persons.
Participants an non-participants in a Follow-up after 2 and 4 years within the LUCAS longitudinal study.
Zeitschrift fur gerontologie und geriatrie. 2016;49(7):596-605.
6. Wolter A, Stolle C, Roth G, et al. [Does the resident care assessment instrument improve long-term home
care? - results of a nation-wide study in Germany]. Gesundheitswesen (Bundesverband der Ärzte des
Öffentlichen Gesundheitsdienstes (Germany)); 2013. p. 29-32.
Study Design
7. Preventing falls through conversation. GM: Midlife & Beyond. 2017;2(47):7-7
8. Aartolahti E, Hakkinen A, Lonnroos E, et al. Relationship between functional vision and balance and mobility
performance in community-dwelling older adults. Aging-Clinical & Experimental Research. 2013
Oct;25(5):545-52. doi: http://dx.doi.org/10.1007/s40520-013-0120-z.
9. Agarwal G, McDonough B, Angeles R, et al. Rationale and methods of a multicentre randomised controlled
trial of the effectiveness of a Community Health Assessment Programme with Emergency Medical Services
(CHAP-EMS) implemented on residents aged 55 years and older in subsidised seniors' housing buildings in
Ontario, Canada. BMJ Open. 2015;5(6):e008110. doi: http://dx.doi.org/10.1136/bmjopen-2015-008110.
10. Albert SM, Edelstein O, King J, et al. Assessing the quality of a non-randomized pragmatic trial for primary
prevention of falls among older adults. Prevention Science. 2015 Jan;16(1):31-40. doi:
http://dx.doi.org/10.1007/s11121-014-0466-2.
11. Alessi CA, Stuck AE, Aronow HU, et al. The process of care in preventive in-home comprehensive geriatric
assessment. J Am Geriatr Soc. 1997 Sep;45(9):1044-50. PMID: 9288009.
12. Alexander S, Hunter A. Challenges in the Prevention of Falls and Fall-Related Injuries in Older Adults.
Clinical Nurse Specialist: The Journal for Advanced Nursing Practice. 2017;31(1):20-22
13. Almeida ST, Soldera CL, Carli GA, et al. Analysis of extrinsic and intrinsic factors that predispose elderly
individuals to fall. Revista Da Associacao Medica Brasileira. 2012 Jul-Aug;58(4):427-33.

98
14. Anonymous. Exercise programme aims to cut number of falls across Europe. Nursing Older People.
2014;26(9):7-. doi: 10.7748/nop.26.9.7.s5.
15. Anonymous. Preventing falls in older people. Nursing Standard. 2015;29(34):19-. doi:
10.7748/ns.29.34.19.s25.
16. Anonymous. NICE launches new standards to reduce falls. GM: Midlife & Beyond. 2015;45(4):12-.
17. Arnold AL, Goujon N, Busija L, et al. Near-vision impairment and unresolved vision problems in Indigenous
Australian adults. Clinical & Experimental Ophthalmology. 2013 Apr;41(3):223-30. doi:
http://dx.doi.org/10.1111/j.1442-9071.2012.02846.x.
18. Arora KS, Chang DS, Supakontanasan W, et al. Assessment of a rapid method to determine approximate
visual acuity in large surveys and other such settings. American Journal of Ophthalmology. 2014
Jun;157(6):1315-21.e1. doi: http://dx.doi.org/10.1016/j.ajo.2014.02.031.
19. Bleijenberg N, ten Dam VH, Drubbel I, et al. Development of a proactive care program (U-CARE) to preserve
physical functioning of frail older people in primary care. Journal of Nursing Scholarship. 2013 Sep;45(3):230-
7. doi: http://dx.doi.org/10.1111/jnu.12023.
20. Bleijenberg N, Ten Dam VH, Steunenberg B, et al. Exploring the expectations, needs and experiences of
general practitioners and nurses towards a proactive and structured care programme for frail older patients: a
mixed-methods study. Journal of Advanced Nursing. 2013 Oct;69(10):2262-73. doi:
http://dx.doi.org/10.1111/jan.12110.
21. Bleijenberg N, Drubbel I, Neslo REJ, et al. Cost-Effectiveness of a Proactive Primary Care Program for Frail
Older People: A Cluster-Randomized Controlled Trial. Journal of the American Medical Directors
Association. 2017.
22. Bouman A, van Rossum E, Evers S, et al. Effects on health care use and associated cost of a home visiting
program for older people with poor health status: a randomized clinical trial in the Netherlands. J Gerontol A
Biol Sci Med Sci. 2008;63(3):291-7. PMID: 18375878.
23. Bruce J, Ralhan S, Sheridan R, et al. The design and development of a complex multifactorial falls assessment
intervention for falls prevention: The Prevention of Falls Injury Trial (PreFIT). BMC Geriatrics.
2017;17(1):116.
24. Bula CJ, Alessi CA, Aronow HU, et al. Community physicians' cooperation with a program of in-home
comprehensive geriatric assessment. J Am Geriatr Soc. 1995 Sep;43(9):1016-20. PMID: 7657917.
25. Burton E, Lewin G, Clemson L, et al. Physical activity programs for older people receiving a restorative home
care service, which is more effective? Journal of Science and Medicine in Sport; 2012. p. S304.
26. Cattelani L, Palumbo P, Palmerini L, et al. FRAT-up, a Web-based Fall-Risk Assessment Tool for Elderly
People Living in the Community. Journal of Medical Internet Research. 2015;17(2):e41-e. doi:
10.2196/jmir.4064.
27. Chandler JM, Duncan PW, Kochersberger G, et al. Is lower extremity strength gain associated with
improvement in physical performance and disability in frail, community-dwelling elders? Arch Phys Med
Rehabil. 1998 Jan;79(1):24-30. PMID: 9440412.

99
28. Chou R, Dana T, Bougatsos C, et al. Screening for impaired visual acuity in older adults: updated evidence
report and systematic review for the US Preventive Services Task Force. JAMA. 2016 Mar 1;315(9):915-33.
doi: http://dx.doi.org/10.1001/jama.2016.0783.
29. Ciaschini PM, Straus SE, Dolovich LR, et al. Community-based randomised controlled trial evaluating falls
and osteoporosis risk management strategies. Trials. 2008;9:62. doi: 10.1186/1745-6215-9-62. PMID:
18983670.
30. Clark DO, Stump TE, Tu W, et al. Improving the validity of activity of daily living dependency risk
assessment. Journal of Applied Gerontology. 2015 Apr;34(3):329-42. doi:
http://dx.doi.org/10.1177/0733464812471894.
31. Clarke S, Bradley R, Simmonds B, et al. Can paramedics use FRAX (the WHO Fracture Risk Assessment
Tool) to help GPs improve future fracture risk in patients who fall? Protocol for a randomised controlled
feasibility study. BMJ Open. 2014;4(9):e005744. doi: http://dx.doi.org/10.1136/bmjopen-2014-005744.
32. Clemson L, Mackenzie L, Roberts C, et al. Integrated solutions for sustainable fall prevention in primary care,
the iSOLVE project: a type 2 hybrid effectiveness-implementation design. Implement Sci. 2017;12(1):12
33. Close JC, Wesson J, Sherrington C, et al. Can a tailored exercise and home hazard reduction program reduce
the rate of falls in community dwelling older people with cognitive impairment: protocol paper for the i-
FOCIS randomised controlled trial. BMC Geriatrics. 2014;14:89. doi: http://dx.doi.org/10.1186/1471-2318-14-
89.
34. Cohen D, Morrison A. Interventions for Preventing Falls Among Older Adults Living in the Community.
American Family Physician. 2017;95(3):152-153
35. Colon-Emeric CS. A team approach: comprehensive evaluation for functional decline in older patients.
American Family Physician. 2013;88(6):397-.
36. Counsell SR, Callahan CM, Buttar AB, et al. Geriatric Resources for Assessment and Care of Elders
(GRACE): a new model of primary care for low-income seniors. J Am Geriatr Soc. 2006 Jul;54(7):1136-41.
doi: 10.1111/j.1532-5415.2006.00791.x. PMID: 16866688.
37. Currin ML, Comans TA, Heathcote K, et al. Staying safe at home. Home environmental audit
recommendations and uptake in an older population at high risk of falling. Australasian Journal on Ageing.
2012 Jun;31(2):90-5. doi: http://dx.doi.org/10.1111/j.1741-6612.2011.00545.x.
38. Dahlin-Ivanoff S, Gosman-Hedstrom G, Edberg AK, et al. Elderly persons in the risk zone. Design of a
multidimensional, health-promoting, randomised three-armed controlled trial for "prefrail" people of 80+ years
living at home. BMC Geriatr. 2010;10:27. doi: 10.1186/1471-2318-10-27. PMID: 20504358.
39. Dahlin-Ivanoff S, Eklund K, Wilhelmson K, et al. For whom is a health-promoting intervention effective?
Predictive factors for performing activities of daily living independently. BMC Geriatrics. 2016;16(1):171.
40. Darby J, Williamson T, Logan P, et al. Comprehensive geriatric assessment on an acute medical unit: A
qualitative study of older people's and informal carer's perspectives of the care and treatment received. Clinical
Rehabilitation. 2016 Jan 22;22:22. doi: http://dx.doi.org/10.1177/0269215515624134.
41. de Negreiros Cabral K, Perracini MR, Soares AT, et al. Effectiveness of a multifactorial falls prevention
program in community-dwelling older people when compared to usual care: study protocol for a randomised
controlled trial (Prevquedas Brazil). BMC Geriatrics. 2013;13:27. doi: http://dx.doi.org/10.1186/1471-2318-
13-27.

100
42. Demons JL, Chenna S, Callahan KE, et al. Utilizing a Meals on Wheels Program to Teach Falls Risk
Assessment to Medical Students. Gerontology & Geriatrics Education. 2014;35(4):409-20. doi:
10.1080/02701960.2014.930033.
43. Doba N, Tokuda Y, Goldstein NE, et al. A pilot trial to predict frailty syndrome: the Japanese Health Research
Volunteer Study. Experimental Gerontology. 2012 Aug;47(8):638-43. doi:
http://dx.doi.org/10.1016/j.exger.2012.05.016.
44. Dolovich L, Oliver D, Lamarche L, et al. A protocol for a pragmatic randomized controlled trial using the
Health Teams Advancing Patient Experience: Strengthening Quality (Health TAPESTRY) platform approach
to promote person-focused primary healthcare for older adults. Implementation Science. 2016;11:49. doi:
http://dx.doi.org/10.1186/s13012-016-0407-5.
45. Donate-Martinez A, Rodenas F, Garces J. Impact of a primary-based telemonitoring programme in HRQOL,
satisfaction and usefulness in a sample of older adults with chronic diseases in Valencia (Spain). Archives of
Gerontology & Geriatrics. 2016 Jan-Feb;62:169-75. doi: http://dx.doi.org/10.1016/j.archger.2015.09.008.
46. Dorresteijn TAC, Rixt Zijlstra GA, Van Haastregt JCM, et al. Feasibility of a nurse-led in-home cognitive
behavioral program to manage concerns about falls in frail older people: A process evaluation. Research in
Nursing & Health. 2013;36(3):257-70. doi: 10.1002/nur.21534.
47. Downey PA, Perry SB, Anderson JM. Screening Postmenopausal Women for Fall and Fracture Prevention.
Journal of Geriatric Physical Therapy. 2013;36(3):138-45. doi: 10.1519/JPT.0b013e31827bc497.
48. Duerksen R, Limburg H, Lansingh VC, et al. Review of blindness and visual impairment in Paraguay: changes
between 1999 and 2011. Ophthalmic Epidemiology. 2013 Oct;20(5):301-7. doi:
http://dx.doi.org/10.3109/09286586.2013.821497.
49. Duffin C. Exercise scheme reduces risk of falls. Nursing Standard. 2012;27(5):8-.
50. Duffy A. The development of evidenced-based falls assessment in Ireland. Nursing & Residential Care.
2013;15(6):421-5.
51. El-Khoury F, Cassou B, Charles M-A, et al. The effect of fall prevention exercise programmes on fall induced
injuries in community dwelling older adults. British Journal of Sports Medicine. 2015;49(20):1348-. doi:
10.1136/bmj.f6234.
52. Fairhall N, Aggar C, Kurrle SE, et al. Frailty intervention trial (FIT). BMC Geriatr. 2008;8(1):27.
53. Fairhall N, Kurrle SE, Sherrington C, et al. Effectiveness of a multifactorial intervention on preventing
development of frailty in pre-frail older people: study protocol for a randomised controlled trial. BMJ Open.
2015;5(2):e007091. doi: http://dx.doi.org/10.1136/bmjopen-2014-007091.
54. Fairhall N, Sherrington C, Kurrle SE, et al. Economic evaluation of a multifactorial, interdisciplinary
intervention versus usual care to reduce frailty in frail older people. Journal of the American Medical Directors
Association. 2015 Jan;16(1):41-8. doi: http://dx.doi.org/10.1016/j.jamda.2014.07.006.
55. Fairhall N, Sherrington C, Lord S, et al. A multifactorial interdisciplinary intervention reduces frailty,
increases function and is cost-effective in older adults who are frail: Randomised controlled trial.
Physiotherapy (United Kingdom); 2015. p. eS371-eS2.

101
56. Fletcher AE, Jones DA, Bulpitt CJ, et al. The MRC trial of assessment and management of older people in the
community: objectives, design and interventions [ISRCTN23494848]. BMC Health Serv Res. 2002 Oct
25;2(1):21. PMID: 12398790.
57. Frese T, Hein S, Sandholzer H. Feasibility, understandability, and usefulness of the STEP self-rating
questionnaire: results of a cross-sectional study. Clinical Interventions In Aging. 2013;8:515-21. doi:
http://dx.doi.org/10.2147/CIA.S41826.
58. Fuzhong L, Harmer P, Fitzgerald K. Implementing an Evidence-Based Fall Prevention Intervention in
Community Senior Centers. American Journal of Public Health. 2016;106(11):2026-2031.
59. Ganz DA, Kim SB, Zingmond DS, et al. Effect of a falls quality improvement program on serious fall-related
injuries. Journal of the American Geriatrics Society. 2015 Jan;63(1):63-70. doi:
http://dx.doi.org/10.1111/jgs.13154.
60. Ghasemi M, RezaeiDehaghani A, Mehrabi T. Investigating the effect of education based on need to prevent
falling during activities of daily living among the elderlies referring to health centers of Isfahan. Iranian
Journal of Nursing and Midwifery Research. 2016 Jul-Aug;21(4):430-5. doi: http://dx.doi.org/10.4103/1735-
9066.185599.
61. Gladman J, Edmans J. Acute Medical Unit Comprehensive Geriatric Assessment Intervention Study
(AMIGOS). UK Clinical Research Network (UKCRN) (available At: Http://public.ukcrn.org.uk); 2012.
62. Grapton X, Lemesle P, Strotz V. Falls: risk and prevention in private rheumatology practice. Osteoporosis
international. Conference: world congress on osteoporosis, osteoarthritis and musculoskeletal diseases, WCO-
IOF-ESCEO 2017. Italy. 2017;28:S211-s212.
http://onlinelibrary.wiley.com/o/cochrane/clcentral/articles/674/CN-
01409674/frame.htmlhttps://link.springer.com/content/pdf/10.1007%2Fs00198-017-3950-2.pdf.
63. Gunner-Svensson F, Ipsen J, Olsen J, et al. Prevention of relocation of the aged in nursing homes. Scand J
Prim Health Care. 1984 May;2(2):49-56. PMID: 6544449.
64. Gustafson DH, Sr., McTavish F, Gustafson DH, Jr., et al. The effect of an information and communication
technology (ICT) on older adults' quality of life: study protocol for a randomized control trial. Trials
[Electronic Resource]. 2015;16:191. doi: http://dx.doi.org/10.1186/s13063-015-0713-2.
65. Gustafsson S, Lood Q, Wilhelmson K, et al. A person-centred approach to health promotion for persons 70+
who have migrated to Sweden: promoting aging migrants' capabilities implementation and RCT study
protocol. BMC Geriatrics. 2015;15:10. doi: http://dx.doi.org/10.1186/s12877-015-0005-4.
66. Haanes GG, Kirkevold M, Hofoss D, Eilertsen G. Discrepancy between self-assessments and standardised
tests of vision and hearing abilities in older people living at home: an ROC curve analysis. Journal of Clinical
Nursing. 2015;24(23-24):3380-3388.
67. Hanger HC, Sainsbury R. Screening the elderly: a Christchurch study. N Z Med J. 1990 Oct 10;103(899):473-
5. PMID: 2216130.
68. Harper KJ, Barton AD, Arendts G, Edwards DG, Petta AC, Celenza A. Controlled clinical trial exploring the
impact of a brief intervention for prevention of falls in an emergency department. Emerg Med Australas.
2017;29(5):524-530.
102
69. Hay WI, van Ineveld C Fau - Browne G, Browne G Fau - Roberts J, et al. Prospective care of elderly patients
in family practice. Is screening effective? 19990120 DCOM- 19990120(0008-350X (Print))doi: D - NLM:
PMC2277795 EDAT- 1998/12/31 MHDA- 1998/12/31 00:01 CRDT- 1998/12/31 00:00 PST - ppublish.
70. Hill E, Fauerbach LA. Falls and Fall Prevention in Older Adults. Journal of Legal Nurse Consulting. 2014
Summer2014;25(2):24-9.
71. Hookway LA, Frazier M, Rivera N, et al. Population-based study of presbyopia in Nicaragua. Clinical &
Experimental Optometry. 2016 Jul 10;10:10. doi: http://dx.doi.org/10.1111/cxo.12402.
72. Jamous KF, Jalbert I, Kalloniatis M, et al. Australian general medical practitioner referral pathways for people
with different ocular conditions. Clinical & Experimental Optometry. 2014 Mar;97(2):152-9. doi:
http://dx.doi.org/10.1111/cxo.12102.
73. Jansen S, Schoe J, van Rijn M, et al. Factors associated with recognition and prioritization for falling, and the
effect on fall incidence in community dwelling older adults. BMC Geriatrics. 2015;15:169. doi:
http://dx.doi.org/10.1186/s12877-015-0165-2.
74. Johnson M, Kelly L, Siric K, et al. Improving falls risk screening and prevention using an e-learning approach.
Journal of Nursing Management. 2015;23(7):910-9. doi: 10.1111/jonm.12234.
75. Kallstrand-Eriksson J, Baigi A, Buer N, et al. Perceived vision-related quality of life and risk of falling among
community living elderly people. Scandinavian Journal of Caring Sciences. 2013 Jun;27(2):433-9. doi:
http://dx.doi.org/10.1111/j.1471-6712.2012.01053.x.
76. Kallstrand-Eriksson J, Hildingh C, Bengtsson B. History of falling and visual ability among independently
living elderly in Sweden. Clinical Ophthalmology. 2016;10:1265-73. doi:
http://dx.doi.org/10.2147/OPTH.S101060.
77. Katahira N, Tsukasaki K. Nursing care in multifunctional small group homes providing day, visiting and
overnight services for older people living at home. International Journal of Nursing Practice. 2016;22(6):605-
615.
78. Kim E, Park YK, Byun YH, et al. Influence of aging on visual perception and visual motor integration in
Korean adults. Journal of Exercise Rehabilitation. 2014 Aug;10(4):245-50. doi:
http://dx.doi.org/10.12965/jer.140147.
79. King A, Boyd M, Dagley L. Use of a screening tool and primary health care gerontology nurse specialist for
high-needs older people. Contemporary Nurse: A Journal for the Australian Nursing Profession.
2017;53(1):23-35.
80. Kono A, Izumi K, Kanaya Y, et al. Assessing the quality and effectiveness of an updated preventive home visit
programme for ambulatory frail older Japanese people: research protocol for a randomized controlled trial.
Journal of Advanced Nursing. 2014 Oct;70(10):2363-72. doi: http://dx.doi.org/10.1111/jan.12390.
81. Kopplin LJ, Mansberger SL. Predictive value of screening tests for visually significant eye disease. American
Journal of Ophthalmology. 2015 Sep;160(3):538-46.e3. doi: http://dx.doi.org/10.1016/j.ajo.2015.05.033.
82. Kwan MMS, LinS.I, Close JCT, et al. Depressive symptoms in addition to visual impairment, reduced strength
and poor balance predict falls in older Taiwanese people. Age and Ageing. 2012 September;41(5):606-12. doi:
http://dx.doi.org/10.1093/ageing/afs065.

103
83. Lam BL, Christ SL, Zheng DD, et al. Longitudinal relationships among visual acuity and tasks of everyday
life: the Salisbury Eye Evaluation study. Investigative Ophthalmology & Visual Science. 2013 Jan;54(1):193-
200. doi: http://dx.doi.org/10.1167/iovs.12-10542.
84. Langdon R, Johnson M, Carroll V, et al. Assessment of the elderly: it's worth covering the risks. Journal of
Nursing Management. 2013;21(1):94-105. doi: 10.1111/j.1365-2834.2012.01421.x.
85. Langeland E, Tuntland H, Forland O, et al. Study protocol for a multicenter investigation of reablement in
Norway.[Erratum appears in BMC Geriatr. 2015;15:120 Note: Langland, Eva [corrected to Langeland, Eva];
PMID: 26453340]. BMC Geriatrics. 2015;15:111. doi: http://dx.doi.org/10.1186/s12877-015-0108-y.
86. Legg L, Gladman J, Drummond A, et al. A systematic review of the evidence on home care reablement
services. Clinical Rehabilitation. 2016 Aug;30(8):741-9. doi: http://dx.doi.org/10.1177/0269215515603220.
87. Li Z, Changshui W, Yao H. Effects of different interventions on falls and falls-related functional factors in
veteran elderly: A pilot randomized controlled trial. Annals of physical and rehabilitation medicine; 2014. p.
e153.
88. Li CM, Chang CI, Yu WR, Yang W, Hsu CC, Chen CY. Enhancing elderly health examination effectiveness
by adding physical function evaluations and interventions. Arch Gerontol Geriatr. 2017;70:38-43.
89. Liimatta H, Lampela P, Laitinen-Parkkonen P, Pitkala KH. Preventive home visits to promote the health-
related quality of life of home-dwelling older people: Baseline findings and feasibility of a randomized,
controlled trial. European Geriatric Medicine. 2017.
90. Lindfield R, Griffiths U, Bozzani F, et al. A rapid assessment of avoidable blindness in Southern Zambia.
PLoS ONE [Electronic Resource]. 2012;7(6):e38483. doi: http://dx.doi.org/10.1371/journal.pone.0038483.
91. Locatelli I, Monod S, Cornuz J, Bula CJ, Senn N. A prospective study assessing agreement and reliability of a
geriatric evaluation. BMC Geriatrics. 2017;17(1):153.
92. Lorig K, Ritter PL, Plant K, et al. The South Australia health chronic disease self-management Internet trial.
Health Education & Behavior. 2013 Feb;40(1):67-77. doi: http://dx.doi.org/10.1177/1090198112436969.
93. Ludwig C, Busnel C. Derivation of a frailty index from the resident assessment instrument - home care
adapted for Switzerland: a study based on retrospective data analysis. BMC Geriatrics. 2017;17:1-10.
94. Markle-Reid M, Browne G, Gafni A. Nurse-led health promotion interventions improve quality of life in frail
older home care clients: lessons learned from three randomized trials in Ontario, Canada. Journal of Evaluation
in Clinical Practice. 2013 Feb;19(1):118-31. doi: http://dx.doi.org/10.1111/j.1365-2753.2011.01782.x.
95. Marsden J. Preserving vision and promoting visual health in older people. Nursing Older People.
2017;29(6):22-26.
96. McGill N. Public Health Prevention: Vision Health Gains Attention as Nation's Population Ages. American
Journal of Public Health. 2016;106(7):1159-. doi: 10.2105/ajph.2016.303267.
97. McKenzie G, Lasater K, Delander GE, Neal MB, Morgove M, Eckstrom E. Falls prevention education:
Interprofessional training to enhance collaborative practice. Gerontology & Geriatrics Education.
2017;38(2):232-243

104
98. McWilliam CL, Vingilis E, Ward-Griffin C, et al. An evaluation of the effectiveness of engaging Canadian
clients as partners in in-home care. Health & Social Care in the Community. 2014 Mar;22(2):210-24. doi:
http://dx.doi.org/10.1111/hsc.12082.
99. Mehrotra A, An R, Patel DN, et al. Impact of a patient incentive program on receipt of preventive care.
American Journal of Managed Care. 2014 Jun;20(6):494-501.
100. Melillo P, Orrico A, Attanasio M, et al. A pilot study for development of a novel tool for clinical decision
making to identify fallers among ophthalmic patients. BMC Medical Informatics & Decision Making. 2015;15
Suppl 3:S6. doi: http://dx.doi.org/10.1186/1472-6947-15-S3-S6.
101. Melillo P, Orrico A, Chirico F, et al. Identifying fallers among ophthalmic patients using classification tree
methodology. PLoS ONE [Electronic Resource]. 2017;12(3):e0174083.
102. Metzelthin SF, Bleijenberg N, Blom JW, et al. Primary care strategies to maintain independence of frail older
people: Looking for evidence across borders. European Geriatric Medicine; 2014. p. S31-s2.
103. Mikolaizak AS, Simpson PM, Tiedemann A, et al. Intervention to prevent further falls in older people who call
an ambulance as a result of a fall: a protocol for the iPREFER randomised controlled trial. BMC Health
Services Research. 2013;13:360. doi: http://dx.doi.org/10.1186/1472-6963-13-360.
104. Miller DK, Lewis LM, Nork MJ, et al. Controlled trial of a geriatric case-finding and liaison service in an
emergency department. J Am Geriatr Soc. 1996 May;44(5):513-20. PMID: 8617898.
105. Monaghan EG. Fall Prevention Intervention And The Triple Aim Goals. Vol 107. Washington, District of
Columbia: American Journal of Public Health 2017:e22-e22
106. Moniz-Pereira V, Carnide F, Machado M, et al. Falls in Portuguese older people: procedures and preliminary
results of the study Biomechanics of Locomotion in the Elderly. Acta Reumatologica Portuguesa. 2012 Oct-
Dec;37(4):324-32.
107. Morris R, Brand C, Hill KD, et al. RESPOND-a patient-centred program to prevent secondary falls in older
people presenting to the emergency department with a fall: Protocol for a program evaluation. EMA -
Emergency Medicine Australasia; 2015. p. 43.
108. Morris RL, Brand CA, Hill KD, et al. RESPOND: a patient-centred programme to prevent secondary falls in
older people presenting to the emergency department with a fall-protocol for a mixed methods programme
evaluation. Injury Prevention. 2016 Apr;22(2):153-60. doi: http://dx.doi.org/10.1136/injuryprev-2014-041453.
109. Muntinga ME, Hoogendijk EO, van Leeuwen KM, et al. Implementing the chronic care model for frail older
adults in the Netherlands: study protocol of ACT (frail older adults: care in transition). BMC Geriatrics.
2012;12:19. doi: http://dx.doi.org/10.1186/1471-2318-12-19.
110. Murphy K, Lowe S. Improving Fall Risk Assessment in Home Care. Home Healthcare Nurse. 2013;31(7):389-
96. doi: 10.1097/NHH.0b013e3182977cdc.
111. Narirat J, Sirirat C, Thanomkwan T, et al. Action Research Development of a Fall Prevention Program for
Thai Community-dwelling Older Persons. Pacific Rim International Journal of Nursing Research.
2015;19(1):69-78.
112. Nicolaides-Bouman A, van Rossum E, Habets H, et al. Home visiting programme for older people with health
problems: process evaluation. J Adv Nurs. 2007 Jun;58(5):425-35. doi: 10.1111/j.1365-2648.2007.04235.x.
PMID: 17442032.
105
113. Nicolaides-Bouman A, van Rossum E, Kempen GI, et al. Effects of home visits by home nurses to elderly
people with health problems: design of a randomised clinical trial in the Netherlands [ISRCTN92017183].
BMC Health Serv Res. 2004 Dec 15;4(1):35. doi: 10.1186/1472-6963-4-35. PMID: 15601473.
114. Nykanen I, Rissanen TH, Sulkava R, et al. Effects of individual dietary counseling as part of a comprehensive
geriatric assessment (CGA) on nutritional status: a population-based intervention study. Journal of Nutrition,
Health & Aging. 2014 Jan;18(1):54-8. doi: http://dx.doi.org/10.1007/s12603-013-0342-y.
115. okayTaiwo OA, Beki-bele CO, Adeoye AO, et al. Prevalence and pattern of eye disorders among commercial
motorcycle riders in Ile-Ife, Osun state. Nigerian Postgraduate Medical Journal. 2014 Sep;21(3):255-61.
116. Owsley C, McGwin G, Jr., Searcey K. A population-based examination of the visual and ophthalmological
characteristics of licensed drivers aged 70 and older. Journals of Gerontology Series A-Biological Sciences &
Medical Sciences. 2013 May;68(5):567-73. doi: http://dx.doi.org/10.1093/gerona/gls185.
117. Pacini M, Smith RD, Wilson EC, et al. Home-based medication review in older people: is it cost effective?
Pharmacoeconomics. 2007;25(2):171-80. PMID: 17249858.
118. Palvanen M, Kannus P, Piirtola M, et al. The chaos falls clinic in preventing falls and injuries among home-
dwelling older adults: A randomised controlled trial. Osteoporosis International; 2012. p. S140.
119. Parry SW, Hill H, Lawson J, et al. A Novel Approach to Proactive Primary Care-Based Case Finding and
Multidisciplinary Management of Falls, Syncope, and Dizziness in a One-Stop Service: Preliminary Results.
Journal of the American Geriatrics Society. 2016;64(11):2368-2373.
120. Parsons M, Senior H, Mei-Hu Chen X, et al. Assessment without action; a randomised evaluation of the
interRAI home care compared to a national assessment tool on identification of needs and service provision for
older people in New Zealand. Health & Social Care in the Community. 2013 Sep;21(5):536-44. doi:
http://dx.doi.org/10.1111/hsc.12045.
121. Parsons M, Senior HE, Kerse N, et al. The Assessment of Services Promoting Independence and Recovery in
Elders Trial (ASPIRE): a pre-planned meta-analysis of three independent randomised controlled trial
evaluations of ageing in place initiatives in New Zealand. Age & Ageing. 2012 Nov;41(6):722-8. doi:
http://dx.doi.org/10.1093/ageing/afs113.
122. Peeters GM, de Vries OJ, Elders PJ, et al. Prevention of fall incidents in patients with a high risk of falling:
design of a randomised controlled trial with an economic evaluation of the effect of multidisciplinary
transmural care. BMC Geriatr. 2007;7:15. doi: 10.1186/1471-2318-7-15. PMID: 17605771.
123. Perry M. Ageing and the eyes: preventing vision loss. Practice Nursing. 2014;25(8):387-90.
124. Pighills A, Ballinger C, Pickering R, et al. A critical review of the effectiveness of environmental assessment
and modification in the prevention of falls amongst community dwelling older people. British Journal of
Occupational Therapy. 2016;79(3):133-43. doi: 10.1177/0308022615600181.
125. Quinn T. Review: Evidence is insufficient to determine the risk-benefit ratio for vision acuity screening in
older adults. ACP Journal Club. 2016;164(12):1-.
126. Rabiu MM, Jenf M, Fituri S, et al. Prevalence and causes of visual impairment and blindness, cataract surgical
coverage and outcomes of cataract surgery in Libya. Ophthalmic Epidemiology. 2013;20(1):26-32. doi:
http://dx.doi.org/10.3109/09286586.2012.746994.

106
127. Ramani L, Furmedge DS, Reddy SPH. Comprehensive geriatric assessment. British Journal of Hospital
Medicine (17508460). 2014:C122-5.
128. Reider NC, Naylor P-J, Gaul C. Sensitivity and Specificity of the Minimal Chair Height Standing Ability Test:
A Simple and Affordable Fall-Risk Screening Instrument. Journal of Geriatric Physical Therapy.
2015;38(2):90-5. doi: 10.1519/jpt.0000000000000025.
129. Reuben DB, Ganz DA, Roth CP, et al. Effect of nurse practitioner comanagement on the care of geriatric
conditions. Journal of the American Geriatrics Society. 2013 Jun;61(6):857-67. doi:
http://dx.doi.org/10.1111/jgs.12268.
130. Ribeiro de Paula G, Nogueira de Souza B, Ferreira Santos L, et al. Quality of life assessment for health
promotion groups. Revista Brasileira de Enfermagem. 2016;69(2):222-9. doi: 10.1590/0034-
7167.2016690206i.
131. Rim TH, Nam JS, Choi M, et al. Prevalence and risk factors of visual impairment and blindness in Korea: the
Fourth Korea National Health and Nutrition Examination Survey in 2008-2010. Acta Opthalmologica. 2014
Jun;92(4):e317-25. doi: http://dx.doi.org/10.1111/aos.12355.
132. Robichaud L, Hebert R, Roy PM, et al. A preventive program for community-dwelling elderly at risk of
functional decline: a pilot study. Arch Gerontol Geriatr. 2000 Jan-Feb;30(1):73-84. PMID: 15374051.
133. Robinson B, Feng Y, Woods CA, et al. Prevalence of visual impairment and uncorrected refractive error -
report from a Canadian urban population-based study. Ophthalmic Epidemiology. 2013 Jun;20(3):123-30. doi:
http://dx.doi.org/10.3109/09286586.2013.789915.
134. Rokicki W, Drozdzowska B, Czekajlo A, et al. Common ophthalmic problems of urban and rural
postmenopausal women in a population sample of Raciborz district, a RAC-OST-POL Study. Annals of
Agricultural & Environmental Medicine. 2014;21(1):70-4.
135. Romera L, Orfila F, Segura JM, et al. Effectiveness of a primary care based multifactorial intervention to
improve frailty parameters in the elderly: a randomised clinical trial: rationale and study design. BMC
Geriatrics. 2014;14:125. doi: http://dx.doi.org/10.1186/1471-2318-14-125.
136. Rubenstein LZ, Josephson KR, Nichol-Seamons M, et al. Comprehensive health screening of well elderly
adults: an analysis of a community program. J Gerontol. 1986 May;41(3):342-52. PMID: 3700984.
137. Ruikes FG, Meys AR, van de Wetering G, et al. The CareWell-primary care program: design of a cluster
controlled trial and process evaluation of a complex intervention targeting community-dwelling frail elderly.
BMC Family Practice. 2012;13:115. doi: http://dx.doi.org/10.1186/1471-2296-13-115.
138. Ruikes FG, Zuidema SU, Akkermans RP, et al. Multicomponent Program to Reduce Functional Decline in
Frail Elderly People: A Cluster Controlled Trial. Journal of the American Board of Family Medicine: JABFM.
2016 Mar-Apr;29(2):209-17. doi: http://dx.doi.org/10.3122/jabfm.2016.02.150214.
139. Russo A, Bowen D. Visual impairment: setting sights on an independent life. Nursing & Residential Care.
2013;15(1):38-40.
140. Saccomano SJ, Ferrara LR. Fall prevention in older adults. Nurse Practitioner. 2015;40(6):40-7. doi:
10.1097/01.NPR.0000465117.19783.ee.
107
141. Schrodt LA, Garbe KC, Shubert TE. Trained Community Providers Conduct Fall Risk Screenings With
Fidelity: An Effective Model for Expanding Reach. Health Promotion Practice. 2014;15(4):599-607. doi:
10.1177/1524839913514752.
142. Schubert CC, Myers LJ, Allen K, et al. Implementing Geriatric Resources for Assessment and Care of Elders
Team Care in a Veterans Affairs Medical Center: Lessons Learned and Effects Observed. Journal of the
American Geriatrics Society. 2016 Jul;64(7):1503-9. doi: http://dx.doi.org/10.1111/jgs.14179.
143. Sheerin L. Screening for falls. Emergency Nurse. 2015;23(3):11-. doi: 10.7748/en.23.3.11.s12.
144. Sherrington C, Fairhall N, Kirkham C, et al. Exercise and fall prevention self-management to reduce mobility-
related disability and falls after fall-related lower limb fracture in older people: protocol for the RESTORE
(Recovery Exercises and STepping On afteR fracturE) randomised controlled trial. BMC Geriatrics.
2016;16:34. doi: http://dx.doi.org/10.1186/s12877-016-0206-5.
145. Snooks H, Anthony R, Chatters R, et al. Support and assessment for fall emergency referrals (SAFER 2)
research protocol: cluster randomised trial of the clinical and cost effectiveness of new protocols for
emergency ambulance paramedics to assess and refer to appropriate community-based care. BMJ Open.
2012;2(6)doi: http://dx.doi.org/10.1136/bmjopen-2012-002169.
146. Snooks HA, Anthony R, Chatters R, et al. Paramedic Assessment of Older Adults After Falls, Including
Community Care Referral Pathway: Cluster Randomized Trial. Annals of Emergency Medicine.
2017;70(4):495-505.e428.
147. Snooks HA, Anthony R, Chatters R, et al. Support and Assessment for Fall Emergency Referrals (SAFER) 2: a
cluster randomised trial and systematic review of clinical effectiveness and cost-effectiveness of new protocols
for emergency ambulance paramedics to assess older people following a fall with referral to community-based
care when appropriate. Health Technology Assessment (Winchester, England). 2017;21(13):1-218.
148. Sommers LS, Marton KI, Barbaccia JC, et al. Physician, nurse, and social worker collaboration in primary care
for chronically ill seniors. Arch Intern Med. 2000 Jun 26;160(12):1825-33. PMID: 10871977.
149. Sorensen KH, Sivertsen J. Follow-up three years after intervention to relieve unmet medical and social needs
of old people. Compr Gerontol B. 1988 Aug;2(2):85-91. PMID: 3228801.
150. Sprange K, Mountain GA, Brazier J, et al. Lifestyle Matters for maintenance of health and wellbeing in people
aged 65 years and over: study protocol for a randomised controlled trial. Trials [Electronic Resource].
2013;14:302. doi: http://dx.doi.org/10.1186/1745-6215-14-302.
151. Stenhagen M, Ekstrom H, Nordell E, et al. Falls in the general elderly population: a 3- and 6- year prospective
study of risk factors using data from the longitudinal population study 'Good ageing in Skane'. BMC
Geriatrics. 2013;13:81. doi: http://dx.doi.org/10.1186/1471-2318-13-81.
152. Stijnen MM, Duimel-Peeters IG, Jansen MW, et al. Early detection of health problems in potentially frail
community-dwelling older people by general practices--project [G]OLD: design of a longitudinal, quasi-
experimental study. BMC Geriatrics. 2013;13:7. doi: http://dx.doi.org/10.1186/1471-2318-13-7.
153. Stuck AE, Kharicha K, Dapp U, et al. The PRO-AGE study: an international randomised controlled study of
health risk appraisal for older persons based in general practice. BMC medical research methodology.
2007;7(1):1.
154. Suijker JJ, Buurman BM, ter Riet G, et al. Comprehensive geriatric assessment, multifactorial interventions
and nurse-led care coordination to prevent functional decline in community-dwelling older persons: protocol

108
of a cluster randomized trial. BMC Health Services Research. 2012;12:85. doi: http://dx.doi.org/10.1186/1472-
6963-12-85.
155. Suijker JJ, MacNeil-Vroomen JL, van Rijn M, et al. Cost-effectiveness of nurse-led multifactorial care to
prevent or postpone new disabilities in community-living older people: Results of a cluster randomized trial.
PLoS ONE [Electronic Resource]. 2017;12(4):e0175272.
156. Szanton SL, Wolff JW, Leff B, et al. CAPABLE trial: a randomized controlled trial of nurse, occupational
therapist and handyman to reduce disability among older adults: rationale and design. Contemporary Clinical
Trials. 2014 May;38(1):102-12. doi: http://dx.doi.org/10.1016/j.cct.2014.03.005.
157. Taing D, McKay K. Better Strength, Better Balance! Partnering to deliver a fall prevention program for older
adults. Canadian Journal of Public Health. 2017;108(3):e314-e319.
158. Tan PJ, Khoo EM, Saedon NI, et al. 105 A Randomised Controlled Study On Individually-Tailored
Multifactorial Falls Intervention In Older Fallers In Malaysia. Age & Ageing. 2014;43(suppl_1):i29-i.
159. Tatsuya H, Shigeru I, Nobuou M, et al. A Modified Fall Risk Assessment Tool That Is Specific to Physical
Function Predicts Falls in Community-Dwelling Elderly People. Journal of Geriatric Physical Therapy.
2014;37(4):159-65. doi: 10.1519/JPT.0b013e3182abe7cb.
160. Teeranut H, Borwarnluck T, Parinya R. The Effects of a Physical Activity Program for Fall Prevention among
Thai Older Adults. Pacific Rim International Journal of Nursing Research. 2015;19(1):4-18.
161. Theander E, Edberg AK. Preventive home visits to older people in Southern Sweden. Scand J Public Health.
2005;33(5):392-400. PMID: 16267888.
162. Tiedemann A, Paul S, Ramsay E, et al. What is the effect of a combined physical activity and fall prevention
intervention enhanced with health coaching and pedometers on older adults' physical activity levels and
mobility-related goals? Study protocol for a randomised controlled trial. BMC Public Health. 2015;15:477.
doi: http://dx.doi.org/10.1186/s12889-015-1380-7.
163. Tinetti ME, Baker DI, Garrett PA, et al. Yale FICSIT: risk factor abatement strategy for fall prevention. J Am
Geriatr Soc. 1993 Mar;41(3):315-20. PMID: 8440856.
164. Tuunainen E, Jantti P, Pyykko I, et al. Intervention to prevent falls in elderly adults living in a residential
home. Journal of the American Geriatrics Society. 2013 Aug;61(8):1426-7. doi:
http://dx.doi.org/10.1111/jgs.12395.
165. U.S. Preventive Services Task Force. Screening for Impaired Visual Acuity in Older Adults: Recommendation
Statement. Skokie, Illinois: American Academy of Family Physicians; 2016. p. 1024A-C.
166. van Hout HP, Nijpels G Fau - van Marwijk HWJ, van Marwijk Hw Fau - Jansen APD, et al. Design and pilot
results of a single blind randomized controlled trial of systematic demand-led home visits by nurses to frail
elderly persons in primary care [ISRCTN05358495]. 2003 20051006 DCOM- 20060614(1471-2318
(Electronic))doi: D - NLM: PMC1242228 - epublish.
167. van Rijn M, Suijker JJ, Bol W, et al. Comprehensive geriatric assessment: recognition of identified geriatric
conditions by community-dwelling older persons. Age & Ageing. 2016;45(6):894-899.
168. Van Voast Moncada L, Mire LG. Preventing Falls in Older Persons. American Family Physician.
2017;96(4):240-247.

109
169. Walters K, Kharicha K, Goodman C, et al. Promoting independence, health and well-being for older people: a
feasibility study of computer-aided health and social risk appraisal system in primary care. BMC Family
Practice. 2017;18(1):47.
170. Wells M, Wade M. Physical performance measures: An important component of the comprehensive geriatric
assessment. Nurse Practitioner. 2013;38(6):48-53. doi: 10.1097/01 .NPR.0000429895.41373.7e.
171. Whitney SL, Marchetti GF, Ellis JL, et al. Improvements in Balance in Older Adults Engaged in a Specialized
Home Care Falls Prevention Program. Journal of Geriatric Physical Therapy. 2013;36(1):3-12. doi:
10.1519/JPT.0b013e3182550ea5.
172. Wilkinson-Meyers L, Brown P, McLean C, et al. Met and unmet need for personal assistance among
community-dwelling New Zealanders 75 years and over. Health & Social Care in the Community. 2014
May;22(3):317-27. doi: http://dx.doi.org/10.1111/hsc.12087.
173. Wilson N, Kvizhinadze G, Pega F, Nair N, Blakely T. Home modification to reduce falls at a health district
level: Modeling health gain, health inequalities and health costs. PLoS ONE. 2017;12 (9) (no
pagination)(e0184538).
174. Windsor J, Dix A. A bedside tool to assess eyesight in hospital patients at risk of falls. Nursing Times.
2017;113(5):1-7.
175. Withey MB, Breault A. A Home Healthcare and School of Pharmacy Partnership to Reduce Falls. Home
Healthcare Nurse. 2013;31(6):295-302. doi: 10.1097/NHH.0b013e318294787c.
176. Wittich W, Barstow EA, Jarry J, et al. Screening for sensory impairment in older adults: Training and practice
of occupational therapists in Quebec. Canadian Journal of Occupational Therapy. 2015;82(5):283-93. doi:
10.1177/0008417415573076.
177. Wong KC, Wong FK, Chang KK. Health-social partnership intervention programme for community-dwelling
older adults: a research protocol for a randomized controlled trial. Journal of Advanced Nursing. 2015
Nov;71(11):2673-85. doi: http://dx.doi.org/10.1111/jan.12700.
178. Wrede J, Voigt I, Bleidorn J, et al. Complex health care decisions with older patients in general practice:
patient-centeredness and prioritization in consultations following a geriatric assessment. Patient Education &
Counseling. 2013 Jan;90(1):54-60. doi: http://dx.doi.org/10.1016/j.pec.2012.07.015.
179. Wu TY, Chie WC, Yang RS, et al. Risk factors for single and recurrent falls: a prospective study of falls in
community dwelling seniors without cognitive impairment. Preventive Medicine. 2013 Nov;57(5):511-7. doi:
http://dx.doi.org/10.1016/j.ypmed.2013.07.012.
180. Wyman JF, Croghan CF, Nachreiner NM, et al. Effectiveness of education and individualized counseling in
reducing environmental hazards in the homes of community-dwelling older women. J Am Geriatr Soc. 2007
Oct;55(10):1548-56. doi: 10.1111/j.1532-5415.2007.01315.x. PMID: 17908058.
181. Yao Y, Shao J, Sun W, et al. Prevalence of blindness and causes of visual impairment among adults aged 50
years or above in southern. Jiangsu Province of China. Pakistan Journal of Medical Sciences. 2013
Sep;29(5):1203-7.
182. Zhu RR, Shi J, Yang M, et al. Prevalences and causes of vision impairment in elderly Chinese: a
socioeconomic perspective of a comparative report nested in Jiangsu Eye Study. International Journal of
Ophthalmology. 2016;9(7):1051-6. doi: http://dx.doi.org/10.18240/ijo.2016.07.19.
110
183. Zijlstra GA, van Haastregt JC, Du Moulin MF, et al. Effects of the implementation of an evidence-based
program to manage concerns about falls in older adults. Gerontologist. 2013 Oct;53(5):839-49. doi:
http://dx.doi.org/10.1093/geront/gns142.
184. Zozula A, Carpenter CR, Lipsey K, et al. Prehospital emergency services screening and referral to reduce falls
in community-dwelling older adults: a systematic review. Emergency Medicine Journal. 2016 May;33(5):345-
50. doi: http://dx.doi.org/10.1136/emermed-2015-204815.
185. Kono A, Fujita T, Tsumura C, et al. Preventive home visit model targeted to specific care needs of ambulatory
frail elders: preliminary report of a randomized trial design. Aging Clin Exp Res. 2009 Apr;21(2):167-73.
PMID: 19448389.
186. Newbury JW. 75+ Health assessments: a randomised controlled trial; 2001.
187. Hawranik P. Testing the Effectiveness of a Vision Care Program on Falls, Fractures and Quality of Life.
Misericordia Health Centre.
188. McGraw C, Déry L, Wittich W. Falls prevention through the visual impairment detection program. Insight:
Research and Practice in Visual Impairment and Blindness. 2011;4(2):74-82.
189. Quebec Gd. La prevention des chutes dans un continuum de services pour les anise vivant a domicile: Cadre
de reference. . http://publications.msss.gouv.qc.ca/acrobat/f/documentation/2004/04-232-01.pdf. 2004.
Population
190. Scientific Research -- Falls, Fractures and Trauma. Age & Ageing. 2017;46:ii14-ii14.
191. Acton JH, Molik B, Court H, Margrain TH. Effect of a Home Visit-Based Low Vision Rehabilitation
Intervention on Visual Function Outcomes: An Exploratory Randomized Controlled Trial. Investigative
Ophthalmology & Visual Science. 2016;57(15):6662-6667.
192. Aveiro MC, Driusso P, Santos JG, et al. Effects of a physical therapy program on quality of life among
community-dwelling elderly women: randomized-controlled trial. Fisioterapia em Movimento; 2013.
193. Blom J, Elzen WD, Houwelingen Anne HV, et al. Effectiveness and cost-effectiveness of a proactive, goal-
oriented, integrated care model in general practice for older people. A cluster randomised controlled trial:
Integrated systematic care for older people-the ISCOPE study. Age and Ageing. 2016 01 Jan;45(1):30-41. doi:
http://dx.doi.org/10.1093/ageing/afv174.
194. Campbell AJ, Robertson MC, La Grow SJ, et al. Randomised controlled trial of prevention of falls in people
aged > or =75 with severe visual impairment: the VIP trial. BMJ. 2005 Oct 8;331(7520):817. doi:
10.1136/bmj.38601.447731.55. PMID: 16183652.
195. Caplan GA, Williams AJ, Daly B, et al. A randomized, controlled trial of comprehensive geriatric assessment
and multidisciplinary intervention after discharge of elderly from the emergency department--the DEED II
study. J Am Geriatr Soc. 2004 Sep;52(9):1417-23. doi: 10.1111/j.1532-5415.2004.52401.x. PMID: 15341540.
196. Chu MM, Fong KN, Lit AC, et al. An Occupational Therapy Fall Reduction Home Visit Program for
Community-Dwelling Older Adults in Hong Kong After an Emergency Department Visit for a Fall. Journal of
the American Geriatrics Society. 2017;65(2):364-372
111
197. Church JL, Haas MR, Goodall S. Cost Effectiveness of Falls and Injury Prevention Strategies for Older Adults
Living in Residential Aged Care Facilities. Pharmacoeconomics. 2015 Dec;33(12):1301-10. doi:
http://dx.doi.org/10.1007/s40273-015-0313-8.
198. Ciaschini PM, Straus SE, Dolovich LR, et al. Community-based intervention to optimise falls risk
management: a randomised controlled trial. Age Ageing. 2009 Nov;38(6):724-30. doi: 10.1093/ageing/afp176.
PMID: 19767629.
199. Clemson L, Cumming Rg Fau - Kendig H, Kendig H Fau - Swann M, et al. The effectiveness of a community-
based program for reducing the incidence of falls in the elderly: a randomized trial. 20040902 DCOM-
20041007(0002-8614 (Print)).
200. Close J, Ellis M, Hooper R, et al. Prevention of falls in the elderly trial (PROFET): a randomised controlled
trial. Lancet. 1999 Jan 9;353(9147):93-7. doi: 10.1016/s0140-6736(98)06119-4. PMID: 10023893.
201. Dan A, Raubvogel G, Chen T, et al. The Impact of Multimedia Education on Uptake of Comprehensive Eye
Examinations in Rural China: A Randomized, Controlled Trial. Ophthalmic Epidemiology. 2015;22(4):283-
90. doi: http://dx.doi.org/10.3109/09286586.2015.1056812.
202. Davison J, Bond J, Dawson P, et al. Patients with recurrent falls attending Accident & Emergency benefit from
multifactorial intervention--a randomised controlled trial. Age Ageing. 2005 Mar;34(2):162-8. doi:
10.1093/ageing/afi053. PMID: 15716246.
203. de Vries OJ, Elders PJ, Muller M, et al. Multifactorial intervention to reduce falls in older people at high risk
of recurrent falls: a randomized controlled trial. Arch Intern Med. 2010;170(13):1110-7.
204. Dickson G, Chesser A, Woods NK, et al. Time required for screening for visual impairment in primary care: a
randomized comparison of 3 common visual tests. Journal of Primary Care & Community Health. 2012 Jul
1;3(3):174-9. doi: http://dx.doi.org/10.1177/2150131911429824.
205. Ekerstad N, Karlson BW, Dahlin Ivanoff S, et al. Is the acute care of frail elderly patients in a comprehensive
geriatric assessment unit superior to conventional acute medical care? Clinical Interventions In Aging.
2017;12:1-9
206. Ekerstad N, Ivanoff S, Landahl S, et al. Acute care of severely frail elderly patients in a CGA-unit is associated
with less functional decline than conventional acute care. Clinical interventions in aging. 2017;12:1239-1249.
http://onlinelibrary.wiley.com/o/cochrane/clcentral/articles/102/CN-01405102/frame.html
https://www.dovepress.com/getfile.php?fileID=37852.
207. Elley CR, Robertson MC, Garrett S, et al. Effectiveness of a falls-and-fracture nurse coordinator to reduce
falls: a randomized, controlled trial of at-risk older adults. J Am Geriatr Soc. 2008 Aug;56(8):1383-9. doi:
10.1111/j.1532-5415.2008.01802.x. PMID: 18808597.
208. Elley CR, Robertson MC, Kerse NM, et al. Falls Assessment Clinical Trial (FACT): design, interventions,
recruitment strategies and participant characteristics. BMC Public Health. 2007;7:185. doi: 10.1186/1471-
2458-7-185. PMID: 17662156.
209. Enguidanos S, Gibbs N, Jamison P. From hospital to home: a brief nurse practitioner intervention for
vulnerable older adults. Journal of Gerontological Nursing. 2012 Mar;38(3):40-50. doi:
http://dx.doi.org/10.3928/00989134-20120116-01.
112
210. Foo CL, Siu VW, Ang H, et al. Risk stratification and rapid geriatric screening in an emergency department - a
quasi-randomised controlled trial. BMC Geriatrics. 2014;14:98. doi: http://dx.doi.org/10.1186/1471-2318-14-
98.
211. Freiberger E, Blank WA, Salb J, et al. Effects of a complex intervention on fall risk in the general practitioner
setting: a cluster randomized controlled trial. Clinical Interventions In Aging. 2013;8:1079-88. doi:
http://dx.doi.org/10.2147/CIA.S46218.
212. Gallagher EM, Brunt H. Head over heels: Impact of a health promotion program to reduce falls in the elderly.
Canadian Journal on Aging/La Revue canadienne du vieillissement. 1996;15(01):84-96.
213. Gitlin LN, Hauck WW, Dennis MP, et al. Long-term effect on mortality of a home intervention that reduces
functional difficulties in older adults: results from a randomized trial. J Am Geriatr Soc. 2009 Mar;57(3):476-
81. doi: 10.1111/j.1532-5415.2008.02147.x. PMID: 19187417.
214. Gitlin LN, Hauck WW, Winter L, et al. Effect of an in-home occupational and physical therapy intervention on
reducing mortality in functionally vulnerable older people: preliminary findings. J Am Geriatr Soc. 2006
Jun;54(6):950-5. doi: 10.1111/j.1532-5415.2006.00733.x. PMID: 16776791.
215. Green J, Forster A, Bogle S, et al. Physiotherapy for patients with mobility problems more than 1 year after
stroke: a randomised controlled trial. Lancet. 2002 Jan 19;359(9302):199-203. doi: 10.1016/s0140-
6736(02)07443-3. PMID: 11812553.
216. Group AHSR, Chew EY, Clemons TE, et al. Randomized trial of a home monitoring system for early
detection of choroidal neovascularization home monitoring of the Eye (HOME) study. Ophthalmology. 2014
Feb;121(2):535-44. doi: http://dx.doi.org/10.1016/j.ophtha.2013.10.027.
217. Hendriks MR, Bleijlevens MH, van Haastregt JC, et al. Lack of effectiveness of a multidisciplinary fall-
prevention program in elderly people at risk: a randomized, controlled trial. J Am Geriatr Soc. 2008
Aug;56(8):1390-7. doi: 10.1111/j.1532-5415.2008.01803.x. PMID: 18662214.
218. Hogan DB, MacDonald FA, Betts J, et al. A randomized controlled trial of a community-based consultation
service to prevent falls. CMAJ. 2001 Sep 4;165(5):537-43. PMID: 11563205.
219. Holland R, Lenaghan E, Harvey I, et al. Does home based medication review keep older people out of
hospital? The HOMER randomised controlled trial. BMJ. 2005 Feb 5;330(7486):293. doi:
10.1136/bmj.38338.674583.AE. PMID: 15665005.
220. Holland R, Lenaghan E, Smith R, et al. Delivering a home‐based medication review, process measures from
the HOMER randomised controlled trial. International journal of pharmacy practice. 2006;14(1):71-9.
221. Junius-Walker U, Wrede J, Voigt I, et al. Impact of a priority-setting consultation on doctor-patient agreement
after a geriatric assessment: cluster randomised controlled trial in German general practices. Quality in
Primary Care. 2012;20(5):321-34.
222. Kingston P, Jones M, Lally F, et al. Older people and falls: A randomized controlled trial of a health visitor
(HV) intervention. Reviews in Clinical Gerontology. 2001;11(03):209-14.
223. La Grow SJ, Robertson MC, Campbell AJ, et al. Reducing hazard related falls in people 75 years and older
with significant visual impairment: how did a successful program work? Inj Prev. 2006 Oct;12(5):296-301.
doi: 10.1136/ip.2006.012252. PMID: 17018669.

113
224. Lee HC, Chang KC, Tsauo JY, et al. Effects of a multifactorial fall prevention program on fall incidence and
physical function in community-dwelling older adults with risk of falls. Archives of Physical Medicine &
Rehabilitation. 2013 Apr;94(4):606-15, 15.e1. doi: http://dx.doi.org/10.1016/j.apmr.2012.11.037.
225. Lenaghan E, Holland R, Brooks A. Home-based medication review in a high risk elderly population in primary
care--the POLYMED randomised controlled trial. Age Ageing. 2007 May;36(3):292-7. doi:
10.1093/ageing/afm036. PMID: 17387123.
226. Li Y, Liebel DV, Friedman B. An investigation into which individual instrumental activities of daily living are
affected by a home visiting nurse intervention. Age & Ageing. 2013 Jan;42(1):27-33. doi:
http://dx.doi.org/10.1093/ageing/afs151.
227. Lightbody E, Watkins C, Leathley M, et al. Evaluation of a nurse-led falls prevention programme versus usual
care: a randomized controlled trial. Age Ageing. 2002 May;31(3):203-10. PMID: 12006310.
228. Lin MR, Wolf SL, Hwang HF, et al. A randomized, controlled trial of fall prevention programs and quality of
life in older fallers. J Am Geriatr Soc. 2007 Apr;55(4):499-506. doi: 10.1111/j.1532-5415.2007.01146.x.
PMID: 17397426.
229. Liu T, Congdon N, Yan X, et al. A randomized, controlled trial of an intervention promoting cataract surgery
acceptance in rural China: the Guangzhou Uptake of Surgery Trial (GUSTO). Investigative Ophthalmology &
Visual Science. 2012;53(9):5271-8. doi: http://dx.doi.org/10.1167/iovs.12-9798.
230. Liu-Ambrose T, Donaldson MG, Ahamed Y, et al. Otago home-based strength and balance retraining
improves executive functioning in older fallers: a randomized controlled trial. J Am Geriatr Soc. 2008
Oct;56(10):1821-30. doi: 10.1111/j.1532-5415.2008.01931.x. PMID: 18795987.
231. Luukinen H, Lehtola S, Jokelainen J, et al. Prevention of disability by exercise among the elderly: a
population-based, randomized, controlled trial. Scand J Prim Health Care. 2006 Dec;24(4):199-205. doi:
10.1080/02813430600958476. PMID: 17118858.
232. Luukinen H, Lehtola S, Jokelainen J, et al. Pragmatic exercise-oriented prevention of falls among the elderly: a
population-based, randomized, controlled trial. Prev Med. 2007 Mar;44(3):265-71. doi:
10.1016/j.ypmed.2006.09.011. PMID: 17174387.
233. Mahoney JE, Shea TA, Przybelski R, et al. Kenosha County falls prevention study: a randomized, controlled
trial of an intermediate-intensity, community-based multifactorial falls intervention. J Am Geriatr Soc. 2007
Apr;55(4):489-98. doi: 10.1111/j.1532-5415.2007.01144.x. PMID: 17397425.
234. Markle-Reid M, Weir R, Browne G, et al. Health promotion for frail older home care clients. J Adv Nurs. 2006
May;54(3):381-95. doi: 10.1111/j.1365-2648.2006.03817.x. PMID: 16629922.
235. Matchar DB, Duncan PW, Lien CT, et al. Randomized Controlled Trial of Screening, Risk Modification, and
Physical Therapy to Prevent Falls Among the Elderly Recently Discharged From the Emergency Department
to the Community: The Steps to Avoid Falls in the Elderly Study Archives of Physical Medicine &
Rehabilitation. 2017;98(6):1086-1096..
236. Mikolaizak AS, Lord SR, Tiedemann A, et al. A multidisciplinary intervention to prevent subsequent falls and
health service use following fall-related paramedic care: a randomised controlled trial. Age & Ageing.
2017;46(2):200-207.
114
237. Noble N, Paul C, Carey M, et al. A randomised trial assessing the acceptability and effectiveness of providing
generic versus tailored feedback about health risks for a high need primary care sample. BMC Family Practice.
2015;16:95. doi: http://dx.doi.org/10.1186/s12875-015-0309-7.
238. Owsley C, McGwin G, Jr., Searcey K, et al. Effect of an eye health education program on older African
Americans' eye care utilization and attitudes about eye care. Journal of the National Medical Association.
2013;105(1):69-76.
239. Patil R, Uusi-Rasi K, Kannus P, et al. Concern about falling in older women with a history of falls:
associations with health, functional ability, physical activity and quality of life. Gerontology. 2014;60(1):22-
30. doi: http://dx.doi.org/10.1159/000354335.
240. Pighills AC, Torgerson DJ, Sheldon TA, et al. Environmental assessment and modification to prevent falls in
older people. J Am Geriatr Soc. 2011 Jan;59(1):26-33. doi: 10.1111/j.1532-5415.2010.03221.x. PMID:
21226674.
241. Radwany SM, Hazelett SE, Allen KR, et al. Results of the promoting effective advance care planning for
elders (PEACE) randomized pilot study. Population Health Management. 2014 Apr;17(2):106-11. doi:
http://dx.doi.org/10.1089/pop.2013.0017.
242. Rahimi Foroushani A, Estebsari F, Mostafaei D, et al. The effect of health promoting intervention on healthy
lifestyle and social support in elders: a clinical trial study. Iranian Red Crescent Medical Journal. 2014
Aug;16(8):e18399. doi: http://dx.doi.org/10.5812/ircmj.18399.
243. Sach TH, Logan PA, Coupland CA, et al. Community falls prevention for people who call an emergency
ambulance after a fall: an economic evaluation alongside a randomised controlled trial. Age & Ageing. 2012
Sep;41(5):635-41. doi: http://dx.doi.org/10.1093/ageing/afs071.
244. Salem BE, Ma-Pham J, Chen S, Brecht ML, Antonio AL, Ames M. Impact of a Community-Based Frailty
Intervention Among Middle-Aged and Older Prefrail and Frail Homeless Women: A Pilot Randomized
Controlled Trial. Community Mental Health Journal. 2017;53(6):688-694.
245. Salminen M, Vahlberg T, Sihvonen S, et al. Effects of risk-based multifactorial fall prevention program on
maximal isometric muscle strength in community-dwelling aged: a randomized controlled trial. Aging Clin
Exp Res. 2008 Oct;20(5):487-93. PMID: 19039292.
246. Salminen MJ, Vahlberg TJ, Salonoja MT, et al. Effect of a risk-based multifactorial fall prevention program on
the incidence of falls. J Am Geriatr Soc. 2009 Apr;57(4):612-9. doi: 10.1111/j.1532-5415.2009.02176.x.
PMID: 19392952.
247. Shyu YI, Liang J, Tseng MY, et al. Comprehensive care improves health outcomes among elderly Taiwanese
patients with hip fracture. Journals of Gerontology Series A-Biological Sciences & Medical Sciences. 2013
Feb;68(2):188-97. doi: http://dx.doi.org/10.1093/gerona/gls164.
248. Sjosten NM, Salonoja M, Piirtola M, et al. A multifactorial fall prevention programme in home-dwelling
elderly people: a randomized-controlled trial. Public Health. 2007 Apr;121(4):308-18. doi:
10.1016/j.puhe.2006.09.018. PMID: 17320125.
249. Sjosten NM, Vahlberg TJ, Kivela SL. The effects of multifactorial fall prevention on depressive symptoms
among the aged at increased risk of falling. Int J Geriatr Psychiatry. 2008 May;23(5):504-10. doi:
10.1002/gps.1927. PMID: 17932996.
115
250. Souied EH, Delcourt C, Querques G, et al. Oral docosahexaenoic acid in the prevention of exudative age-
related macular degeneration: the Nutritional AMD Treatment 2 study. Ophthalmology. 2013
Aug;120(8):1619-31. doi: 10.1016/j.ophtha.2013.01.005. PMID: 23395546.
251. Spice CL, Morotti W, George S, et al. The Winchester falls project: a randomised controlled trial of secondary
prevention of falls in older people. Age and ageing. 2009;38(1):33-40.
252. Steinberg M, Cartwright C Fau - Peel N, Peel N Fau - Williams G, et al. A sustainable programme to prevent
falls and near falls in community dwelling older people: results of a randomised trial. 20000420 DCOM-
20000420(0143-005X (Print))doi: D - NLM: PMC1731645 EDAT- 2000/04/04 09:00 MHDA- 2000/04/25
09:00 CRDT- 2000/04/04 09:00 PST - ppublish.
253. Stevens JA, Mahoney JE, Ehrenreich H. Circumstances and outcomes of falls among high risk community-
dwelling older adults. Injury Epidemiology. 2014;1(1)doi: http://dx.doi.org/10.1186/2197-1714-1-5.
254. Tan PJ, Khoo EM, Chinna K, et al. An individually-tailored multifactorial intervention program for older
fallers in a middle-income developing country: Malaysian Falls Assessment and Intervention Trial (MyFAIT).
BMC Geriatrics. 2014;14:78. doi: http://dx.doi.org/10.1186/1471-2318-14-78.
255. Tanajewski L, Franklin M, Gkountouras G, et al. Cost-Effectiveness of a Specialist Geriatric Medical
Intervention for Frail Older People Discharged from Acute Medical Units: Economic Evaluation in a Two-
Centre Randomised Controlled Trial (AMIGOS). PLoS ONE [Electronic Resource]. 2015;10(5):e0121340.
doi: http://dx.doi.org/10.1371/journal.pone.0121340.
256. Thingstad P, Taraldsen K, Saltvedt I, et al. The long-term effect of comprehensive geriatric care on gait after
hip fracture: the Trondheim Hip Fracture Trial-a randomised controlled trial. Osteoporosis International.
2016;27(3):933-942.
257. Thygesen LC, Fokdal S, Gjorup T, et al. Can municipality-based post-discharge follow-up visits including a
general practitioner reduce early readmission among the fragile elderly (65+ years old)? A randomized
controlled trial. Scandinavian Journal of Primary Health Care. 2015 Jun;33(2):65-73. doi:
http://dx.doi.org/10.3109/02813432.2015.1041831.
258. Tiedemann A, O'Rourke S, Sesto R, et al. A 12-week Iyengar yoga program improved balance and mobility in
older community-dwelling people: a pilot randomized controlled trial. The journals of gerontology. 2013
Sep;Series A, Biological sciences and medical sciences. 68(9):1068-75. doi:
http://dx.doi.org/10.1093/gerona/glt087.
259. Vaapio S, Salminen M, Vahlberg T, et al. Effects of risk-based multifactorial fall prevention on health-related
quality of life among the community-dwelling aged: a randomized controlled trial. Health Qual Life
Outcomes. 2007;5:20. doi: 10.1186/1477-7525-5-20. PMID: 17462083.
260. van Haastregt JC, Diederiks JP, van Rossum E, et al. Effects of a programme of multifactorial home visits on
falls and mobility impairments in elderly people at risk: randomised controlled trial. BMJ. 2000 Oct
21;321(7267):994-8. PMID: 11039967.
261. Waterman H, Ballinger C, Brundle C, et al. A feasibility study to prevent falls in older people who are sight
impaired: the VIP2UK randomised controlled trial. Trials [Electronic Resource]. 2016;17(1):464.
262. Wesson J, Clemson L, Brodaty H, et al. A feasibility study and pilot randomised trial of a tailored prevention
program to reduce falls in older people with mild dementia. BMC Geriatrics. 2013;13:89. doi:
http://dx.doi.org/10.1186/1471-2318-13-89.

116
263. Wong FK, Chow SK, Chan TM, et al. Comparison of effects between home visits with telephone calls and
telephone calls only for transitional discharge support: a randomised controlled trial. Age & Ageing. 2014
Jan;43(1):91-7. doi: http://dx.doi.org/10.1093/ageing/aft123.
264. Yıldırım P, Ofluoglu D, Aydogan S, et al. Tai Chi vs. combined exercise prescription: A comparison of their
effects on factors related to falls. Journal of Back & Musculoskeletal Rehabilitation. 2016;29(3):493-501. doi:
10.3233/bmr-150645.
265. Yu DS. Effects of a Health and Social Collaborative Case Management Model on Health Outcomes of Family
Caregivers of Frail Older Adults: Preliminary Data from a Pilot Randomized Controlled Trial. Journal of the
American Geriatrics Society. 2016;64(10):2144-2148
Intervention
266. Althomali M, Vallis L, Leat S. Does visual attention training improve balance and mobility in older adults?
Investigative ophthalmology and visual science. Conference: 2016 annual meeting of the association for
research in vision and ophthalmology, ARVO 2016. United states. 2016;57(12):1495.
http://onlinelibrary.wiley.com/o/cochrane/clcentral/articles/300/CN-01377300/frame.html.
267. Arkkukangas M, Soderlund A, Eriksson S, Johansson AC. Fall Preventive Exercise With or Without Behavior
Change Support for Community-Dwelling Older Adults: A Randomized Controlled Trial With Short-Term
Follow-up. Journal of Geriatric Physical Therapy. 2017;27:27.
268. Arundel C, Jefferson L, Bailey M, et al. A randomized, embedded trial of pre-notification of trial participation
did not increase recruitment rates to a falls prevention trial. Journal of Evaluation in Clinical Practice.
2017;23(1):73-78.
269. Badrasawi M, Shahar S, Zahara A, Nor FR, Singh D. Efficacy of L-carnitine supplementation on frailty status
and its biomarkers,nutritional status,and physical and cognitive function among prefrail older adults: a double-
blind,randomized,placebo-controlled clinical trial. Clinical interventions in aging. 2016;11:1675-1686.
http://onlinelibrary.wiley.com/o/cochrane/clcentral/articles/746/CN-
01288746/frame.htmlhttps://www.dovepress.com/getfile.php?fileID=33636.
270. Balaban DJ, Goldfarb NI, Perkel RL, et al. Follow-up study of an urban family medicine home visit program. J
Fam Pract. 1988 Mar;26(3):307-12. PMID: 3346634.
271. Barban F, Annicchiarico R, Melideo M, et al. Reducing fall risk with combined motor and cognitive training in
elderly fallers. Brain Sciences. 2017;7 (2) (no pagination)(19).
272. Berglund H, Hasson H, Kjellgren K, et al. Effects of a continuum of care intervention on frail older persons'
life satisfaction: a randomized controlled study. Journal of Clinical Nursing. 2015 Apr;24(7-8):1079-90. doi:
http://dx.doi.org/10.1111/jocn.12699.
273. Bernabei R, Landi F, Gambassi G, et al. Randomised trial of impact of model of integrated care and case
management for older people living in the community. BMJ. 1998 May 2;316(7141):1348-51. PMID:
9563983.
274. Bianchetti L, Squazzoni F, Casnici N, et al. Social networks and health status in the elderly: the 'ANZIANI IN-
RETE' population-based study. Aging Clinical & Experimental Research. 2017;16:16.
275. Bleijenberg N, Drubbel I, Schuurmans MJ, et al. Effectiveness of a Proactive Primary Care Program on
Preserving Daily Functioning of Older People: A Cluster Randomized Controlled Trial. Journal of the
American Geriatrics Society. 2016 Jul 26;26:26. doi: http://dx.doi.org/10.1111/jgs.14325.
117
276. Blom J, den Elzen W, van Houwelingen AH, et al. Effectiveness and cost-effectiveness of a proactive, goal-
oriented, integrated care model in general practice for older people. A cluster randomised controlled trial:
Integrated Systematic Care for older People--the ISCOPE study. Age & Ageing. 2016;45(1):30-41.
277. Boult C, Leff B, Boyd CM, et al. A matched-pair cluster-randomized trial of guided care for high-risk older
patients. Journal of General Internal Medicine. 2013 May;28(5):612-21. doi: http://dx.doi.org/10.1007/s11606-
012-2287-y.
278. Callahan K, Miller M, Kritchevsky S, Houston D, Williamson J, Rejeski W. Promoting active aging in primary
care. Journal of the american geriatrics society. Conference: 2017 annual scientific meeting of the american
geriatrics society. United states. 2017;65:S36.
http://onlinelibrary.wiley.com/o/cochrane/clcentral/articles/980/CN-01376980/frame.html.
279. Campbell AJ, Robertson MC, Gardner MM, et al. Falls prevention over 2 years: a randomized controlled trial
in women 80 years and older. Age Ageing. 1999 Oct;28(6):513-8. PMID: 10604501.
280. Campbell AJ, Robertson MC, Gardner MM, et al. Randomised controlled trial of a general practice
programme of home based exercise to prevent falls in elderly women. BMJ. 1997 Oct 25;315(7115):1065-9.
PMID: 9366737.
281. Carpenter GI, Demopoulos GR. Screening the elderly in the community: controlled trial of dependency
surveillance using a questionnaire administered by volunteers. 1990 19900726 DCOM- 19900726(0959-8138
(Print))doi: D - NLM: PMC1662856 EDAT- 1990/05/12 MHDA- 1990/05/12 00:01 CRDT- 1990/05/12 00:00
PST - ppublish.
282. Chan A, Matchar DB, Tsao MA, et al. Self-Care for Older People (SCOPE): a cluster randomized controlled
trial of self-care training and health outcomes in low-income elderly in Singapore. Contemporary Clinical
Trials; 2015. p. 313-24.
283. Chao J, Wang Y, Xu H, et al. The effect of community-based health management on the health of the elderly:
a randomized controlled trial from China. BMC Health Services Research. 2012;12:449. doi:
http://dx.doi.org/10.1186/1472-6963-12-449.
284. Cheong, A, Lam H, Tsang W, Leat S, Li R. Slow-pace videogames are more effective than fast-pace
videogames in enhancing visual attention in older adults. Investigative ophthalmology and visual science.
Conference: 2016 annual meeting of the association for research in vision and ophthalmology, ARVO 2016.
United States. 2016;57(12):1510
285. Ciechanowski P, Wagner E, Schmaling K, et al. Community-integrated home-based depression treatment in
older adults: a randomized controlled trial. JAMA. 2004 Apr 7;291(13):1569-77. doi:
10.1001/jama.291.13.1569. PMID: 15069044.
286. Clarke M, Clarke Sj Fau - Jagger C, Jagger C. Social intervention and the elderly: a randomized controlled
trial. 1992 19930316 DCOM- 19930316(0002-9262 (Print)).
287. Clemson L, Lannin NA, Wales K, et al. Occupational Therapy Predischarge Home Visits in Acute Hospital
Care: A Randomized Trial. Journal of the American Geriatrics Society. 2016;64(10):2019-2026.
288. Cockayne S, Rodgers S, Green L, et al. Clinical effectiveness and cost-effectiveness of a multifaceted podiatry
intervention for falls prevention in older people: a multicentre cohort randomised controlled trial (the
REducing Falls with ORthoses and a Multifaceted podiatry intervention trial). Health Technology Assessment
(Winchester, England). 2017;21(24):1-198.
118
289. Cockayne S, Adamson J, Clarke A, et al. Cohort Randomised Controlled Trial of a Multifaceted Podiatry
Intervention for the Prevention of Falls in Older People (The REFORM Trial). PLoS ONE [Electronic
Resource]. 2017;12(1):e0168712.
290. Cockayne S, Fairhurst C, Adamson J, et al. An optimised patient information sheet did not significantly
increase recruitment or retention in a falls prevention study: An embedded randomised recruitment trial. Trials.
2017;18 (1) (no pagination)(144).
291. Cohen MA, Miller J, Shi X, et al. Prevention program lowered the risk of falls and decreased claims for long-
term services among elder participants. Health Affairs. 2015;34(6):971-7. doi:
http://dx.doi.org/10.1377/hlthaff.2014.1172.
292. Cohen MA, Miller J, Xiaomei S, et al. IMPROVING CARE. Prevention Program Lowered The Risk Of Falls
And Decreased Claims For Long-Term Services Among Elder Participants. Health Affairs. 2015;34(6):971-7.
doi: 10.1377/hlthaff.2014.1172.
293. Counsell SR, Callahan CM, Tu W, et al. Cost analysis of the Geriatric Resources for Assessment and Care of
Elders care management intervention. J Am Geriatr Soc. 2009 Aug;57(8):1420-6. PMID: 19691149.
294. Crawford Shearer NB, Fleury JD, Belyea M. Randomized control trial of the Health Empowerment
Intervention: feasibility and impact. Nurs Res. 2010 May-Jun;59(3):203-11. doi:
10.1097/NNR.0b013e3181dbbd4a. PMID: 20404773.
295. Dalby DM, Sellors JW, Fraser FD, et al. Effect of preventive home visits by a nurse on the outcomes of frail
elderly people in the community: a randomized controlled trial. CMAJ. 2000 Feb 22;162(4):497-500. PMID:
10701382.
296. Dapp U, Neumann L, Golgert S, et al. Long-term effects of the intervention "active health promotion in old
age" over a 13 year period-results from the LUCAS cohort study (prolong health). European journal of
epidemiology. Conference: health - exploring complexity: an interdisciplinary systems approach, HEC 2016.
Germany. Conference start: 20160828. Conference end: 20160902. 2016;31:S39.
http://onlinelibrary.wiley.com/o/cochrane/clcentral/articles/794/CN-
01267794/frame.htmlhttps://link.springer.com/content/pdf/10.1007%2Fs10654-016-0183-1.pdf.
297. Daragjati J, Musacchio C, Polidori M, et al. Multidimensional prognostic index in hospitalized elderly patients
across Europe and Australia: a prospective multicenter study of the European MPI-AGE project. European
geriatric medicine. Conference: 12th international congress of the european union geriatric medicine society,
EUGMS 2016. Portugal. Conference start: 20161005. Conference end: 20161007. 2016;7:S16.
http://onlinelibrary.wiley.com/o/cochrane/clcentral/articles/726/CN-01252726/frame.html
298. De Vriendt P, Peersman W, Florus A, et al. Improving Health Related Quality of Life and Independence in
Community Dwelling Frail Older Adults through a Client-Centred and Activity-Oriented Program. A
Pragmatic Randomized Controlled Trial. Journal of Nutrition, Health & Aging. 2016 Jan;20(1):35-40. doi:
http://dx.doi.org/10.1007/s12603-015-0581-1.
299. Di Pollina L, Guessous I, Petoud V, et al. Integrated care at home reduces unnecessary hospitalizations of
community-dwelling frail older adults: a prospective controlled trial. BMC Geriatrics. 2017;17(1):53.
300. Eckerblad J, Theander K, Ekdahl AW, et al. Symptom trajectory and symptom burden in older people with
multimorbidity, secondary outcome from the RCT AGe-FIT study. Journal of Advanced Nursing. 2016 May
25;25:25. doi: http://dx.doi.org/10.1111/jan.13032.

119
301. Ekdahl AW, Alwin J, Eckerblad J, et al. Long-Term Evaluation of the Ambulatory Geriatric Assessment: A
Frailty Intervention Trial (AGe-FIT): Clinical Outcomes and Total Costs After 36 Months. Journal of the
American Medical Directors Association. 2016 Mar 1;17(3):263-8. doi:
http://dx.doi.org/10.1016/j.jamda.2015.12.008.
302. Elbar O, Tzedek I, Vered E, et al. A water-based training program that includes perturbation exercises
improves speed of voluntary stepping in older adults: A randomized controlled cross-over trial. Archives of
Gerontology and Geriatrics. 2013 January;56(1):134-40. doi: http://dx.doi.org/10.1016/j.archger.2012.08.003.
303. El-Khoury F, Cassou B, Latouche A, et al. Effectiveness of two year balance training programme on
prevention of fall induced injuries in at risk women aged 75-85 living in community: Ossébo randomised
controlled trial. BMJ: British Medical Journal. 2015;351(8019):10-.
304. Epstein AM, Hall JA, Fretwell M, et al. Consultative geriatric assessment for ambulatory patients. A
randomized trial in a health maintenance organization. JAMA. 1990 Jan 26;263(4):538-44. PMID: 2294326.
305. Evans C, Bone A, Morgan M, et al. Feasibility of delivering a model of short-term integrated palliative and
supportive care for the frail elderly with non-cancer conditions in community settings: a phase II randomised
trial (optcare elderly study). Palliative medicine. Conference: 9th world research congress of the european
association for palliative care, EAPC 2016. Ireland. Conference start: 20160609. Conference end: 20160611.
2016;30(6):Np21. http://onlinelibrary.wiley.com/o/cochrane/clcentral/articles/402/CN-
01304402/frame.htmlhttp://journals.sagepub.com/doi/pdf/10.1177/0269216316646056.
306. Ferreira A, Chaves P, Simoes D. The effect of a fall prevention exercise programme on fear of falling in the
elderly. European geriatric medicine. Conference: 12th international congress of the european union geriatric
medicine society, EUGMS 2016. Portugal. Conference start: 20161005. Conference end: 20161007.
2016;7:S189. http://onlinelibrary.wiley.com/o/cochrane/clcentral/articles/674/CN-01252674/frame.html
307. Ford JH, 2nd, Abramson B, Wise M, Dattalo M, Mahoney JE. Bringing Healthy Aging to Scale: A
Randomized Trial of a Quality Improvement Intervention to Increase Adoption of Evidence-Based Health
Promotion Programs by Community Partners. J Public Health Manag Pract. 2017;23(5):e17-e24.
308. Fox PJ, Vazquez L, Tonner C, et al. A randomized trial of a multifaceted intervention to reduce falls among
community-dwelling adults. Health Educ Behav. 2010 Dec;37(6):831-48. doi: 10.1177/1090198110366003.
PMID: 21051772.
309. Frese T, Deutsch T, Keyser M, et al. In-home preventive comprehensive geriatric assessment (CGA) reduces
mortality--a randomized controlled trial. Archives of Gerontology & Geriatrics. 2012 Nov-Dec;55(3):639-44.
doi: http://dx.doi.org/10.1016/j.archger.2012.06.012.
310. Gawler S, Skelton DA, Dinan-Young S, et al. Reducing falls among older people in general practice: The
ProAct65+ exercise intervention trial. Archives of Gerontology and Geriatrics. 2016 01 Nov;67:46-54. doi:
http://dx.doi.org/10.1016/j.archger.2016.06.019.
311. Gill TM, Pahor, M., Gurlnik, J.M., McDermott, M.M., King, A., Buford, T.W.,. Effect of structured physical
activity on prevention of serious fall injuries in adults aged 70-89. BMJ: British Medical Journal.
2016;352(8043):i245-i. doi: 10.1136/bmj.i245.
312. Gitlin LN, Winter L, Dennis MP, et al. A randomized trial of a multicomponent home intervention to reduce
functional difficulties in older adults. J Am Geriatr Soc. 2006 May;54(5):809-16. doi: 10.1111/j.1532-
5415.2006.00703.x. PMID: 16696748.
120
313. Gouveia BR, Jardim HG, Martins MM, et al. An evaluation of a nurse-led rehabilitation programme (the
ProBalance Programme) to improve balance and reduce fall risk of community-dwelling older people: A
randomised controlled trial. International Journal of Nursing Studies. 2016;56:1-8. doi:
10.1016/j.ijnurstu.2015.12.004.
314. Granbom M, Kristensson J, Sandberg M. Effects on leisure activities and social participation of a case
management intervention for frail older people living at home: a randomised controlled trial. Health & Social
Care in the Community. 2017;25(4):1416-1429.
315. Gschwind YJ, Eichberg S, Ejupi A, et al. ICT-based system to predict and prevent falls (iStoppFalls): results
from an international multicenter randomized controlled trial. European Reviews of Aging & Physical
Activity. 2015;12:10. doi: http://dx.doi.org/10.1186/s11556-015-0155-6.
316. Guse CE, Peterson DJ, Christiansen AL, et al. Translating a Fall Prevention Intervention Into Practice: A
Randomized Community Trial. American Journal of Public Health. 2015 Jul;105(7):1475-81. doi:
http://dx.doi.org/10.2105/AJPH.2014.302315.
317. Gustafsson S, Eklund K, Wilhelmson K, et al. Long-term outcome for ADL following the health-promoting
RCT--elderly persons in the risk zone. Gerontologist. 2013 Aug;53(4):654-63. doi:
http://dx.doi.org/10.1093/geront/gns121.
318. Gustafsson S, Wilhelmson K, Eklund K, et al. Health-promoting interventions for persons aged 80 and older
are successful in the short term--results from the randomized and three-armed Elderly Persons in the Risk Zone
study. Journal of the American Geriatrics Society. 2012 Mar;60(3):447-54. doi:
http://dx.doi.org/10.1111/j.1532-5415.2011.03861.x.
319. Gustafsson S, Wilhelmson K, Eklund K, et al. Health-promoting interventions for persons aged 80 and older
are successful in the short term--results from the randomized and three-armed Elderly Persons in the Risk Zone
study. J Am Geriatr Soc. 2012 Mar;60(3):447-54. doi: 10.1111/j.1532-5415.2011.03861.x. PMID: 22409735.
320. Hall N, De Beck P, Johnson D, et al. Randomized trial of a health promotion program for frail elders.
Canadian Journal on Aging/La Revue canadienne du vieillissement. 1992;11(01):72-91.
321. Headley CM, Payne L. Examination of a fall prevention program on leisure and leisure-based fear of falling of
older adults. International Journal on Disability and Human Development. 2014 01 Feb;13(1):149-54. doi:
http://dx.doi.org/10.1515/ijdhd-2013-0023.
322. Hendriksen C Fau - Lund E, Lund E Fau - Stromgard E, Stromgard E. Consequences of assessment and
intervention among elderly people: a three year randomised controlled trial. 1984 19850128 DCOM-
19850128(0267-0623 (Print))doi: D - NLM: PMC1443760 EDAT- 1984/12/01 MHDA- 1984/12/01 00:01
CRDT- 1984/12/01 00:00 PST - ppublish.
323. Huang HC, Liu Cy Fau - Huang Y-T, Huang Yt Fau - Kernohan WG, et al. Community-based interventions to
reduce falls among older adults in Taiwan - long time follow-up randomised controlled study. 20100524
DCOM- 20100826(1365-2702 (Electronic)).
324. Huang TT, Acton GJ. Effectiveness of home visit falls prevention strategy for Taiwanese community-dwelling
elders: randomized trial. Public Health Nurs. 2004 May-Jun;21(3):247-56. doi: 10.1111/j.0737-
1209.2004.21307.x. PMID: 15144369.
325. Jeon MY, Jeong H, Petrofsky J, et al. Effects of a randomized controlled recurrent fall prevention program on
risk factors for falls in frail elderly living at home in rural communities. Medical Science Monitor.
2014;20:2283-91. doi: http://dx.doi.org/10.12659/MSM.890611.
121
326. Johansson E, Dahlberg R, Jonsson H, et al. Does a Falls Prevention Program Impact Perceived Participation in
Everyday Occupations? A Pilot Randomized Controlled Trial. OTJR: Occupation, Participation, & Health.
2015 Oct;35(4):204-12. doi: http://dx.doi.org/10.1177/1539449215589728.
327. Kamei T, Kajii F, Yamamoto Y, et al. Effectiveness of a home hazard modification program for reducing falls
in urban community-dwelling older adults: A randomized controlled trial. Japan Journal of Nursing Science:
JJNS. 2015 Jul;12(3):184-97. doi: http://dx.doi.org/10.1111/jjns.12059.
328. Kapan A, Winzer E, Haider S, et al. Impact of a lay-led home-based intervention programme on quality of life
in community-dwelling pre-frail and frail older adults: a randomized controlled trial. BMC Geriatrics.
2017;17(1):154.
329. Kapan A, Luger E, Haider S, et al. Fear of falling reduced by a lay led home-based program in frail
community-dwelling older adults: A randomised controlled trial. Arch Gerontol Geriatr. 2017;68:25-32.
330. Kerse N, McLean C, Moyes SA, et al. The cluster-randomized BRIGHT trial: Proactive case finding for
community-dwelling older adults. Annals of Family Medicine. 2014 Nov-Dec;12(6):514-24. doi:
http://dx.doi.org/10.1370/afm.1696.
331. King AI, Parsons M, Robinson E, et al. Assessing the impact of a restorative home care service in New
Zealand: a cluster randomised controlled trial. Health & Social Care in the Community. 2012 Jul;20(4):365-74.
doi: http://dx.doi.org/10.1111/j.1365-2524.2011.01039.x.
332. Kono A, Izumi K, Yoshiyuki N, et al. Effects of an Updated Preventive Home Visit Program Based on a
Systematic Structured Assessment of Care Needs for Ambulatory Frail Older Adults in Japan: A Randomized
Controlled Trial. Journals of Gerontology Series A Biological Sciences & Medical Sciences. 2016 Apr
13;13:13. doi: http://dx.doi.org/10.1093/gerona/glw068.
333. Kono A, Kai I, Sakato C, et al. Effect of preventive home visits for ambulatory housebound elders in Japan: a
pilot study. Aging Clin Exp Res. 2004 Aug;16(4):293-9. PMID: 15575123.
334. Kono A, Kanaya Y, Fujita T, et al. Effects of a preventive home visit program in ambulatory frail older people:
a randomized controlled trial. Journals of Gerontology Series A-Biological Sciences & Medical Sciences. 2012
Mar;67(3):302-9. doi: http://dx.doi.org/10.1093/gerona/glr176.
335. Kono A, Kanaya Y, Tsumura C, et al. Effects of preventive home visits on health care costs for ambulatory
frail elders: a randomized controlled trial. Aging-Clinical & Experimental Research. 2013 Oct;25(5):575-81.
doi: http://dx.doi.org/10.1007/s40520-013-0128-4.
336. Krebs DE, Jette AM, Assmann SF. Moderate exercise improves gait stability in disabled elders. Arch Phys
Med Rehabil. 1998 Dec;79(12):1489-95. PMID: 9862288.
337. Lampela P, Lavikainen P, Huupponen R, et al. Comprehensive geriatric assessment decreases prevalence of
orthostatic hypotension in older persons. Scandinavian Journal of Public Health. 2013 Jun;41(4):351-8. doi:
http://dx.doi.org/10.1177/1403494813475533.
338. Leung KS, Li CY, Tse YK, et al. Effects of 18-month low-magnitude high-frequency vibration on fall rate and
fracture risks in 710 community elderly - A cluster-randomized controlled trial. Osteoporosis International.
2014 June;25(6):1785-95. doi: http://dx.doi.org/10.1007/s00198-014-2693-6.

122
339. Leveille SG, Wagner Eh Fau - Davis C, Davis C Fau - Grothaus L, et al. Preventing disability and managing
chronic illness in frail older adults: a randomized trial of a community-based partnership with primary care.
19981106 DCOM- 19981106(0002-8614 (Print)).
340. Levine S, Steinman BA, Attaway K, et al. Home care program for patients at high risk of hospitalization.
American Journal of Managed Care. 2012 Aug;18(8):e269-76.
341. Lewin G, De San Miguel K, Knuiman M, et al. A randomised controlled trial of the Home Independence
Program, an Australian restorative home-care programme for older adults. Health & Social Care in the
Community. 2013 Jan;21(1):69-78. doi: http://dx.doi.org/10.1111/j.1365-2524.2012.01088.x.
342. Luker KA. Health visiting and the elderly. Midwife Health Visit Community Nurse. 1979 Nov;15(11):457-9.
PMID: 259890.
343. Mazya A, Garvin P, Unosson M, Ekdahl A. Outpatient comprehensive geriatric assessment: effects on frailty.
European geriatric medicine. Conference: 12th international congress of the european union geriatric medicine
society, EUGMS 2016. Portugal. Conference start: 20161005. Conference end: 20161007. 2016;7:S16.
http://onlinelibrary.wiley.com/o/cochrane/clcentral/articles/727/CN-01252727/frame.html.
344. Merom D, Mathieu E, Cerin E, et al. Social Dancing and Incidence of Falls in Older Adults: A Cluster
Randomised Controlled Trial. PLoS Med. 2016;13(8):e1002112.
345. Metzelthin SF, van Rossum E, Hendriks MR, et al. Reducing disability in community-dwelling frail older
people: cost-effectiveness study alongside a cluster randomised controlled trial. Age & Ageing. 2015
May;44(3):390-6. doi: http://dx.doi.org/10.1093/ageing/afu200.
346. Muntinga ME, Van Leeuwen KM, Schellevis FG, Nijpels G, Jansen AP. From concept to content: assessing
the implementation fidelity of a chronic care model for frail, older people who live at home. BMC Health
Services Research. 2015;15:18.
347. Nelson ME, Layne JE, Bernstein MJ, et al. The effects of multidimensional home-based exercise on functional
performance in elderly people. J Gerontol A Biol Sci Med Sci. 2004 Feb;59(2):154-60. PMID: 14999030.
348. Ng TP, Feng L, Nyunt MS, et al. Nutritional, Physical, Cognitive, and Combination Interventions and Frailty
Reversal Among Older Adults: A Randomized Controlled Trial. American Journal of Medicine. 2015
Nov;128(11):1225-36.e1. doi: http://dx.doi.org/10.1016/j.amjmed.2015.06.017.
349. Ng T-P, Nyunt M, Feng L, et al. Multi-domains lifestyle interventions reduces depressive symptoms among
frail and pre-frail older persons: randomized controlled trial. Journal of nutrition, health & aging. 2016:1-9.
http://onlinelibrary.wiley.com/o/cochrane/clcentral/articles/455/CN-
01287455/frame.htmlhttps://link.springer.com/content/pdf/10.1007%2Fs12603-016-0867-y.pdf.
350. Otaka Y, Morita M, Mimura T, Uzawa M, Liu M. Establishment of an appropriate fall prevention program: a
community-based study. Geriatrics & gerontology international. 2017;17(7):1081-1089.
http://onlinelibrary.wiley.com/o/cochrane/clcentral/articles/502/CN-01394502/frame.html.
351. Park JH. The effects of eyeball exercise on balance ability and falls efficacy of the elderly who have
experienced a fall: A single-blind, randomized controlled trial. Arch Gerontol Geriatr. 2017;68:181-185.
352. Parsons J, Rouse P, Robinson EM, et al. Goal setting as a feature of homecare services for older people: does it
make a difference? Age & Ageing. 2012 Jan;41(1):24-9. doi: http://dx.doi.org/10.1093/ageing/afr118.
123
353. Parsons JG, Sheridan N, Rouse P, et al. A randomized controlled trial to determine the effect of a model of
restorative home care on physical function and social support among older people. Archives of Physical
Medicine & Rehabilitation. 2013 Jun;94(6):1015-22. doi: http://dx.doi.org/10.1016/j.apmr.2013.02.003.
354. Parsons M, Senior H, Kerse N, Chen MH, Jacobs S, Anderson C. Randomised trial of restorative home care
for frail older people in New Zealand. Nursing Older People. 2017;29(7):27-33.
355. Perula LA, Varas-Fabra F, Rodriguez V, et al. Effectiveness of a multifactorial intervention program to reduce
falls incidence among community-living older adults: a randomized controlled trial. Archives of Physical
Medicine & Rehabilitation. 2012 Oct;93(10):1677-84. doi: http://dx.doi.org/10.1016/j.apmr.2012.03.035.
356. Pirouzi S, Motealleh AR, Fallahzadeh F, et al. Effectiveness of treadmill training on balance control in elderly
people: A randomized controlled clinical trial. Iranian Journal of Medical Sciences. 2014;39(6):565-70.
357. Ran L, Jiang X, Li B, et al. Association among activities of daily living, instrumental activities of daily living
and health-related quality of life in elderly Yi ethnic minority. BMC Geriatrics. 2017;17(1):74.
358. Robertson MC, Devlin N, Scuffham P, et al. Economic evaluation of a community based exercise programme
to prevent falls. J Epidemiol Community Health. 2001 Aug;55(8):600-6. PMID: 11449021.
359. Robertson MC, Gardner MM, Devlin N, et al. Effectiveness and economic evaluation of a nurse delivered
home exercise programme to prevent falls. 2: Controlled trial in multiple centres. BMJ. 2001 Mar
24;322(7288):701-4. PMID: 11264207.
360. Rosstad T, Salvesen O, Steinsbekk A, Grimsmo A, Sletvold O, Garasen H. Generic care pathway for elderly
patients in need of home care services after discharge from hospital: a cluster randomised controlled trial.
BMC Health Services Research. 2017;17(1):275.
361. Rubin KH, Holmberg T, Rothmann MJ, et al. The Risk-Stratified Osteoporosis Strategy Evaluation study
(ROSE): A Randomized Prospective Population-Based Study. Design and Baseline Characteristics. Calcified
Tissue International. 2015;96(2):167-79. doi: http://dx.doi.org/10.1007/s00223-014-9950-8.
362. Ryan JW, Spellbring AM. Implementing strategies to decrease risk of falls in older women. Journal of
Gerontological Nursing. 1996 19970403 DCOM- 19970403;22(12):25-31.
363. Sahlen KG, Dahlgren L, Hellner BM, et al. Preventive home visits postpone mortality--a controlled trial with
time-limited results. BMC Public Health. 2006;6:220. doi: 10.1186/1471-2458-6-220. PMID: 16945128.
364. Samuel SE, Nayak A, Kotian MS. Effects of functional and balance training on quality of life among
community dwelling older adults. Biomedicine (India). 2013 July-September;33(3):369-74.
365. Schraeder C, Shelton P Fau - Sager M, Sager M. The effects of a collaborative model of primary care on the
mortality and hospital use of community-dwelling older adults. 2001 20010212 DCOM- 20010301(1079-5006
(Print)).
366. Serra-Prat M, Sist X, Domenich R, et al. Effectiveness of an intervention to prevent frailty in pre-frail
community-dwelling older people consulting in primary care: A randomised controlled trial. Age and Ageing.
2017;46(3):401-407.
367. Shapiro A, Taylor M. Effects of a community-based early intervention program on the subjective well-being,
institutionalization, and mortality of low-income elders. Gerontologist. 2002 Jun;42(3):334-41. PMID:
12040135.
124
368. Sheffield C, Smith CA, Becker M. Evaluation of an agency-based occupational therapy intervention to
facilitate aging in place. Gerontologist. 2013 Dec;53(6):907-18. doi: http://dx.doi.org/10.1093/geront/gns145.
369. Smee DJ, Berry HL, Waddington GS, et al. A balance-specific exercise intervention improves falls risk but not
total physical functionality in community-dwelling older adults. Physical & Occupational Therapy in
Geriatrics. 2014;32(4):310-20. doi: 10.3109/02703181.2014.934945.
370. Stevens M, Holman CD, Bennett N. Preventing falls in older people: impact of an intervention to reduce
environmental hazards in the home. J Am Geriatr Soc. 2001 Nov;49(11):1442-7. PMID: 11890581.
371. Stevens M, Holman CD, Bennett N, et al. Preventing falls in older people: outcome evaluation of a
randomized controlled trial. J Am Geriatr Soc. 2001 Nov;49(11):1448-55. PMID: 11890582.
372. Stolle C, Wolter A, Roth G, Rothgang H. Improving health status and reduction of institutionalization in long-
term care--Effects of the Resident Assessment Instrument-Home Care by degree of implementation.
International Journal of Nursing Practice. 2015;21(5):612-621.
373. Sundsli K, Soderhamn U, Espnes GA, et al. Self-care telephone talks as a health-promotion intervention in
urban home-living persons 75+ years of age: a randomized controlled study. Clinical Interventions In Aging.
2014;9:95-103. doi: http://dx.doi.org/10.2147/CIA.S55925.
374. Taylor SF, Coogle CL, Cotter JJ, Welleford EA, Copolillo A. Community-Dwelling Older Adults' Adherence
to Environmental Fall Prevention Recommendations. Journal of Applied Gerontology.
2017:733464817723087.
375. Toye C, Parsons R, Slatyer S, et al. Outcomes for family carers of a nurse-delivered hospital discharge
intervention for older people (the Further Enabling Care at Home Program): Single blind randomised
controlled trial. International Journal of Nursing Studies. 2016;64:32-41.
376. Tuntland H, Aaslund MK, Espehaug B, et al. Reablement in community-dwelling older adults: a randomised
controlled trial. BMC Geriatrics. 2015;15:145. doi: http://dx.doi.org/10.1186/s12877-015-0142-9.
377. Ueda T, Higuchi Y, Imaoka M, Todo E, Kitagawa T, Ando S. Tailored education program using home floor
plans for falls prevention in discharged older patients: A pilot randomized controlled trial. Arch Gerontol
Geriatr. 2017;71:9-13.
378. Uittenbroek RJ, Kremer HP, Spoorenberg SL, et al. Integrated care for older adults improves perceived quality
of care: results of a randomized controlled trial of Embrace. Journal of General Internal Medicine. 2016 Jun
6;6:6. doi: http://dx.doi.org/10.1007/s11606-016-3742-y.
379. Ukawa S, Satoh H, Yuasa M, et al. A randomized controlled trial of a Functioning Improvement Tool home-
visit program and its effect on cognitive function in older persons. International Journal of Geriatric
Psychiatry. 2012 Jun;27(6):557-64. doi: http://dx.doi.org/10.1002/gps.2753.
380. Ukawa S, Yuasa M, Ikeno T, et al. Randomised controlled pilot study in Japan comparing a home visit
program using a Functioning Improvement Tool with a home visit with conversation alone. Australasian
Journal on Ageing. 2012 Sep;31(3):187-9. doi: http://dx.doi.org/10.1111/j.1741-6612.2012.00589.x.
381. van Dijk DJA, M RC, van Empelen P, W JA, B JM. Favourable outcomes of a preventive screening and
counselling programme for older people in underprivileged areas in the Netherlands: The PRIMUS project.
Preventive Medicine Reports. 2017;6:258-264.
125
382. Vass M, Avlund K, Lauridsen J, et al. Feasible model for prevention of functional decline in older people:
municipality-randomized, controlled trial. J Am Geriatr Soc. 2005 Apr;53(4):563-8. doi: 10.1111/j.1532-
5415.2005.53201.x. PMID: 15816999.
383. Voukelatos A, Merom D, Sherrington C, et al. The impact of a home-based walking programme on falls in
older people: The easy steps randomised controlled trial. Age and Ageing. 2015 01 May;44(3):377-83. doi:
http://dx.doi.org/10.1093/ageing/afu186.
384. Wasson J, Gaudette C Fau - Whaley F, Whaley F Fau - Sauvigne A, et al. Telephone care as a substitute for
routine clinic follow-up. 19920414 DCOM- 19920414(0098-7484 (Print)).
385. Weed HG. 2017 - Preoperative geriatric assessment reduced hospital stay and complications in patients ≥65 y
having vascular surgery. ACP Journal Club. 2017;167(2):1-1
386. Wilhelmson K, Eklund K. Positive Effects on Life Satisfaction Following Health-Promoting Interventions for
Frail Older Adults: A Randomized Controlled Study. Health Psychology Research. 2013 Jan 2;1(1):e12. doi:
http://dx.doi.org/10.4081/hpr.2013.e12.
387. Williams ME, Williams TF, Zimmer JG, et al. How does the team approach to outpatient geriatric evaluation
compare with traditional care: a report of a randomized controlled trial. J Am Geriatr Soc. 1987
Dec;35(12):1071-8. PMID: 3119693.
388. Yates SM, Dunnagan TA. Evaluating the effectiveness of a home-based fall risk reduction program for rural
community-dwelling older adults. J Gerontol A Biol Sci Med Sci. 2001 Apr;56(4):M226-30. PMID:
11283195.
389. Ziden L, Haggblom-Kronlof G, Gustafsson S, et al. Physical function and fear of falling 2 years after the
health-promoting randomized controlled trial: elderly persons in the risk zone. Gerontologist. 2014
Jun;54(3):387-97. doi: http://dx.doi.org/10.1093/geront/gnt078.
No outcomes (as reported; indication of no vision outcome)
390. Fordyce M, Bardole D, Romer L, et al. Senior team assessment and referral program—STAR. The Journal of
the American Board of Family Practice. 1997;10(6):398-406.
391. Robson E, Edwards J, Gallagher E, et al. Steady As You Go (SAYGO): A Falls-Prevention Program for
Seniors Living in the Community. Canadian Journal on Aging/La Revue canadienne du vieillissement.
2003;22(02):207-16.
392. Burton LC, Steinwachs DM, German PS, et al. Preventive services for the elderly: would coverage affect
utilization and costs under Medicare? Anm J Public health 1995;85(3)387-391.
393. Burton LC, German Ps Fau - Shapiro S, Shapiro S. A preventive services demonstration. Health status, health
behaviors, and cost outcomes 2 years after intervention. The Johns Hopkins Medicare Preventive Services
Demonstration Team. 19971201 DCOM- 19971201(0025-7079 (Print)).
394. Fabacher D, Josephson K, Pietruszka F, et al. An in-home preventive assessment program for independent
older adults: a randomized controlled trial. J Am Geriatr Soc. 1994 Jun;42(6):630-8. PMID: 8201149.
395. Pathy MS, Bayer A, Harding K, et al. Randomised trial of case finding and surveillance of elderly people at
home. Lancet. 1992 Oct 10;340(8824):890-3. PMID: 1357306.
126
396. Stuck AE, Aronow HU, Steiner A, et al. A trial of annual in-home comprehensive geriatric assessments for
elderly people living in the community. N Engl J Med. 1995 Nov 2;333(18):1184-9. doi:
10.1056/nejm199511023331805. PMID: 7565974.
397. Suijker J, MacNeil-Vroomen J, Rijn M, et al. Economic evaluation of nurse-led multifactorial care to prevent
or postpone new disabilities in community-living older people: results of a cluster randomized trial. European
geriatric medicine. Conference: 12th international congress of the european union geriatric medicine society,
EUGMS 2016. Portugal. Conference start: 20161005. Conference end: 20161007. 2016;7:S103.
http://onlinelibrary.wiley.com/o/cochrane/clcentral/articles/699/CN-01252699/frame.html.
398. Tinetti ME, Baker DI, McAvay G, et al. A multifactorial intervention to reduce the risk of falling among
elderly people living in the community. N Engl J Med. 1994 Sep 29;331(13):821-7. doi:
10.1056/nejm199409293311301. PMID: 8078528.
399. Tulloch AJ, Moore V. A randomized controlled trial of geriatric screening and surveillance in general practice.
J R Coll Gen Pract 1979;29(209): 733-742.
400. Yeo G, Ingram L, Skurnick J, et al. Effects of a geriatric clinic on functional health and well-being of elders. J
Gerontol. 1987 May;42(3):252-8. PMID: 3571860.
No outcomes (as per author response)
401. Behm L, Eklund K, Wilhelmson K, et al. Health Promotion Can Postpone Frailty: Results from the RCT
Elderly Persons in the Risk Zone. 2015 20160718(1525-1446 (Electronic)).
402. Behm L, Wilhelmson K, Falk K, et al. Positive health outcomes following health-promoting and disease-
preventive interventions for independent very old persons: long-term results of the three-armed RCT Elderly
Persons in the Risk Zone. Archives of Gerontology & Geriatrics. 2014 May-Jun;58(3):376-83. doi:
http://dx.doi.org/10.1016/j.archger.2013.12.010.
403. Behm L, Eklund K, Wilhelmson K, et al. Health Promotion Can Postpone Frailty: Results from the RCT
Elderly Persons in the Risk Zone. Public Health Nursing. 2016;33(4):303-315
404. Bouman AI, van Rossum E, Ambergen TW, et al. [Effects of a home visiting program for older people with
poor health status: a randomized, clinical trial in the Netherlands]. Ned Tijdschr Geneeskd. 2009 Apr
4;153(14):644-50. PMID: 19425321.
405. Counsell SR, Callahan CM, Clark DO, et al. Geriatric care management for low-income seniors: a randomized
controlled trial. JAMA. 2007 Dec 12;298(22):2623-33. doi: 10.1001/jama.298.22.2623. PMID: 18073358.
406. Eklund K, Wilhelmson K, Gustafsson H, et al. One-year outcome of frailty indicators and activities of daily
living following the randomised controlled trial: "Continuum of care for frail older people". BMC Geriatrics.
2013;13:76. doi: http://dx.doi.org/10.1186/1471-2318-13-76.
407. Fairhall N, Sherrington C, Lord SR, et al. Effect of a multifactorial, interdisciplinary intervention on risk
factors for falls and fall rate in frail older people: a randomised controlled trial. Age & Ageing. 2014
Sep;43(5):616-22. doi: http://dx.doi.org/10.1093/ageing/aft204.
408. Fletcher AE, Price GM, Ng ES, et al. Population-based multidimensional assessment of older people in UK
general practice: a cluster-randomised factorial trial. Lancet. 2004 Nov 6-12;364(9446):1667-77. doi:
10.1016/s0140-6736(04)17353-4. PMID: 15530627.

127
409. Godwin M, Gadag V, Pike A, et al. A randomized controlled trial of the effect of an intensive 1-year care
management program on measures of health status in independent, community-living old elderly: the Eldercare
project. Family Practice. 2016 Feb;33(1):37-41. doi: http://dx.doi.org/10.1093/fampra/cmv089.
410. Hoogendijk EO, van der Horst HE, van de Ven PM, et al. Effectiveness of a Geriatric Care Model for frail
older adults in primary care: Results from a stepped wedge cluster randomized trial. European Journal of
Internal Medicine. 2016 Mar;28:43-51. doi: http://dx.doi.org/10.1016/j.ejim.2015.10.023
411. Markle-Reid M, Browne G, Gafni A, et al. The effects and costs of a multifactorial and interdisciplinary team
approach to falls prevention for older home care clients 'at risk' for falling: a randomized controlled trial. Can J
Aging. 2010 Mar;29(1):139-61. doi: 10.1017/s0714980809990377. PMID: 20202271.
412. Metzelthin SF, van Rossum E, de Witte LP, et al. Effectiveness of interdisciplinary primary care approach to
reduce disability in community dwelling frail older people: cluster randomised controlled trial. BMJ.
2013;347:f5264. doi: http://dx.doi.org/10.1136/bmj.f5264.
413. Ploeg J, Brazil K, Hutchison B, et al. Effect of preventive primary care outreach on health related quality of
life among older adults at risk of functional decline: randomised controlled trial. BMJ. 2010;340:c1480. doi:
10.1136/bmj.c1480. PMID: 20400483.
414. Sherman H, Soderhielm-Blid S, Forsberg C, et al. Effects of preventive home visits by district nurses on self-
reported health of 75-year-olds. Primary Health Care Research & Development. 2016 Jan;17(1):56-71. doi:
http://dx.doi.org/10.1017/S1463423614000565.
415. Shumway-Cook A, Silver IF, LeMier M, et al. Effectiveness of a community-based multifactorial intervention
on falls and fall risk factors in community-living older adults: a randomized, controlled trial. The Journals of
Gerontology Series A: Biological Sciences and Medical Sciences. 2007;62(12):1420-7.
416. Stuck AE, Moser A, Morf U, et al. Effect of health risk assessment and counselling on health behaviour and
survival in older people: a pragmatic randomised trial. PLoS Medicine / Public Library of Science. 2015
Oct;12(10):e1001889. doi: http://dx.doi.org/10.1371/journal.pmed.1001889.
417. van Hout HP, Jansen AP, van Marwijk HW, et al. Prevention of adverse health trajectories in a vulnerable
elderly population through nurse home visits: a randomized controlled trial [ISRCTN05358495]. J Gerontol A
Biol Sci Med Sci. 2010 Jul;65(7):734-42. doi: 10.1093/gerona/glq037. PMID: 20457579.
418. Yamada Y, Ikegami N. Preventive home visits for community‐dwelling frail elderly people based on
Minimum Data Set‐Home Care: Randomized controlled trial. Geriatrics & Gerontology International.
2003;3(4):236-42.
419. Rubenstein LZ, Aronow HU, Schloe M, et al. A home-based geriatric assessment, follow-up and health
promotion program: design, methods, and baseline findings from a 3-year randomized clinical trial. Aging
(Milano). 1994 Apr;6(2):105-20. PMID: 7918729.
420. Byles JE, Tavener M, O'Connell RL, et al. Randomised controlled trial of health assessments for older
Australian veterans and war widows. Med J Aust. 2004 Aug 16;181(4):186-90. PMID: 15310251.
421. Hebert R, Robichaud L, Roy PM, et al. Efficacy of a nurse-led multidimensional preventive programme for
older people at risk of functional decline. A randomized controlled trial. Age Ageing. 2001 Mar;30(2):147-53.
PMID: 11395345.
128
422. Kono A, Kanaya Y, Fujita T, et al. Effects of a preventive home visit program in ambulatory frail older people:
a randomized controlled trial. J Gerontol A Biol Sci Med Sci. 2012 Mar;67(3):302-9. doi:
10.1093/gerona/glr176. PMID: 22016361.
423. Parsons M, Senior H, Kerse N, et al. Should care managers for older adults be located in primary care? A
randomized controlled trial. Journal of the American Geriatrics Society. 2012 Jan;60(1):86-92. doi:
http://dx.doi.org/10.1111/j.1532-5415.2011.03763.x.
424. Stuck AE, Minder CE, Peter-Wuest I, et al. A randomized trial of in-home visits for disability prevention in
community-dwelling older people at low and high risk for nursing home admission. Arch Intern Med. 2000
Apr 10;160(7):977-86. PMID: 10761963.
No outcome data available (as per author) 425. Thomas R, Worrall G, Elgar F, et al. Can they keep going on their own? A four-year randomized trial of
functional assessments of community residents. Canadian Journal on Aging/La Revue canadienne du
vieillissement. 2007;26(04):379-89.
426. Moller UO, Kristensson J, Midlov P, et al. Effects of a one-year home-based case management intervention on
falls in older people: a randomized controlled trial. Journal of Aging & Physical Activity. 2014 Oct;22(4):457-
64. doi: http://dx.doi.org/10.1123/japa.2013-0101.
No outcome (no response from author after 3 email contacts)
427. Cornillon E, Blanchon Ma Fau - Ramboatsisetraina P, Ramboatsisetraina P Fau - Braize C, et al.
[Effectiveness of falls prevention strategies for elderly subjects who live in the community with performance
assessment of physical activities (before-after)]. 20021223 DCOM- 20030221(0168-6054 (Print)).
428. Ferrer A, Formiga F, Sanz H, et al. Multifactorial assessment and targeted intervention to reduce falls among
the oldest-old: a randomized controlled trial. Clinical Interventions In Aging. 2014;9:383-93. doi:
http://dx.doi.org/10.2147/CIA.S57580.
429. Imhof L, Naef R, Wallhagen MI, et al. Effects of an advanced practice nurse in-home health consultation
program for community-dwelling persons aged 80 and older. Journal of the American Geriatrics Society. 2012
Dec;60(12):2223-31. doi: http://dx.doi.org/10.1111/jgs.12026.
430. Lihavainen K, Sipila S, Rantanen T, et al. Effects of comprehensive geriatric assessment and targeted
intervention on mobility in persons aged 75 years and over: a randomized controlled trial. Clinical
Rehabilitation. 2012 Apr;26(4):314-26. doi: http://dx.doi.org/10.1177/0269215511423269.
431. Luck T, Motzek T, Luppa M, et al. Effectiveness of preventive home visits in reducing the risk of falls in old
age: a randomized controlled trial. Clinical Interventions In Aging. 2013;8:697-702. doi:
http://dx.doi.org/10.2147/CIA.S43284.
432. Palvanen M, Kannus P, Piirtola M, et al. Effectiveness of the Chaos Falls Clinic in preventing falls and injuries
of home-dwelling older adults: a randomised controlled trial. Injury. 2014 Jan;45(1):265-71. doi:
http://dx.doi.org/10.1016/j.injury.2013.03.010.
433. Stolle C, Wolter A, Roth G, et al. Effects of the Resident Assessment Instrument in home care settings: results
of a cluster randomized controlled trial. Zeitschrift fur Gerontologie und Geriatrie. 2012 Jun;45(4):315-22. doi:
http://dx.doi.org/10.1007/s00391-011-0221-2.
129
434. Suijker JJ, van Rijn M, Buurman BM, et al. Effects of nurse-led multifactorial care to prevent disability in
community-living older people: cluster randomized trial. PLoS ONE [Electronic Resource].
2016;11(7):e0158714. doi: http://dx.doi.org/10.1371/journal.pone.0158714.
Setting
435. Lihavainen K, Sipila S, Rantanen T, et al. Effects of comprehensive geriatric intervention on physical
performance among people aged 75 years and over. Aging Clinical and Experimental Research; 2012. 331-8.
436. Zintchouk D, Lauritzen T, Damsgaard E. Comprehensive geriatric care in elderly referred to a rehabilitation
unit-a randomized trial. European geriatric medicine. Conference: 12th international congress of the european
union geriatric medicine society, EUGMS 2016. Portugal. Conference start: 20161005. Conference end:
20161007. 2016;7:S104. http://onlinelibrary.wiley.com/o/cochrane/clcentral/articles/694/CN-
01252694/frame.html.
Other
437. Neumann L, Dapp U, von Renteln-Kruse W, Minder CE. Health promotion and preventive care intervention
for older community-dwelling people: Long-term effects of a randomised controlled trial (RCT) within the
LUCAS cohort. Journal of Nutrition, Health and Aging. 2017:1-8.
APPENDIX E: Study Characteristics
Haanes 20151
Objective
To evaluate the changes in vision, hearing, and lighting conditions at home following
a clinical intervention.
Methods
Design: RCT
Country: Norway
Study period: September 2011-February 2012
Inclusion criteria: 80 yrs and over, receiving home care, able to speak Norwegian
Exclusion criteria: dementia, cognitive impairment, very serious illness
Participants
Recruitment: home care lists
Sample: Intervention (n=46); Control (n=47)
Mean age (SD): Intervention=88 (NR); Control=88 (NR)
Race/ethnicity: NR
Females (%): Intervention=83; Controls=72
Falls (%): NR
Lives alone (%): Intervention=72; Controls=70
Education (%): Intervention= 72; Controls=64 (Elementary only)
Income (%): Intervention=26; Controls=30 (Difficult financial status)
Urban (%): NR, 4 rural and 1 borough municipalities (all maximum 1hr drive to
specialist)
Diabetes (%): NR
Dementia (%): exclusion criteria

130
Residing in nursing homes (%): Intervention= 0; Controls=0 (receiving home care)
Baseline vision loss (%): 95% logMAR ≤0.8 (at least slight VI); 39.8% logMAR <0.4
(<20/50); 17% had difficulties ADLs/IALDs because of hearing or vision, 21% could
not read regular newsprint (all participants)
Other disorders of vision (%): NR
Length of follow-up: 2.5 mo; loss to follow-up: Intervention= 5 (11%), Control= 8
(17%)
Interventions
Intervention:
Vision screening: 1) measured visual acuity and 2) self-reported vision problems
Tool & administration of screening test: 1) Bailey-Lovie LogMAR distance VA chart
at 6m presenting with spectacles and 2) KAS-Screen instrument with 16 questions
on hearing and vision and 1 global question “Do you consider your vision to be good,
not so good, poor or very poor/deaf/blind?”; trained home care nurses
Care in response to screening test: Home care nurses gave advice and referred to
specialists if VA ≤0.7 logMAR and not currently treated.
Setting of program: home
Number of interactions after screening & duration of intervention: 9; 2.5 mo
Other components of screening/assessment: hearing tests and assessment of home
lighting conditions with interventions for both
Other components of care potentially impacting vision: assessment and correction of
lighting condition in homes; assistance with booking medical appointments
Control: Usual care from home care nurses; same vision assessment at baseline
Outcomes
Benefits:
Mean change in acuity: Bailey-Lovie LogMAR distance VA chart
Harms: NR
Implementation factors:
Referrals/recommendations provided to those eligible
Uptake of referrals
Notes Data sources: Published paper and dissertation provided by author.
Most participants wore ready-made spectacles; only 6% daily.
Dapp 20112
Objective
To evaluate the feasibility and acceptance of the Health Risk Assessment for Older
Persons (HRA-O) instrument combined with physician training and with group
sessions or preventive home visits, and to determine the short-term effects of this
multifaceted intervention on preventive care use and health behavior in older
persons.
Methods
Design: RCT
Country: Germany
Study period: 2000-2002

131
Inclusion criteria: 60 years and older (country’s age for elderly care)
Exclusion criteria: those with need for human help in basic ADLs and/or receiving
nursing care, cognitive impairment, terminal disease and/or inability to understand
German
Participants
Recruitment: 14 GP offices in metropolitan area of Hamburg (7 additional used for
concurrent comparison group); practitioners matched for age, gender, qualifications
Sample: Intervention (n=878); Control (n=1702)
Mean age (SD): Intervention=71.9 (7.7); Control=71.8 (7.6)
Race/ethnicity: NR
Females (%): Intervention=61.5; Control=63.3
Falls (%): NR
Lives alone (%): Intervention=35; Control=37.4
Education (%): Intervention=18.8; Control=23.5 (low level)
Income (%): NR
Urban (%): metropolitan region
Diabetes (%): Intervention=9.4; Control=10.7
Dementia (%): exclusion criteria
Residing in nursing homes (%): exclusion criteria
Baseline vision loss: NR
Other disorders of vision (%): NR
Length of follow-up: 12 mo for vision outcomes; loss to follow-up:
Intervention=29.4%, Control=16.2% at 12 mo (37% and 24% for vision outcome;
35% and 21% for vision check-ups) (1.5% deaths)
Interventions
Intervention:
Vision screening: 1) self-reported vision problems
Tool & administration of screening test: 1) 11 self-reported vision questions (e.g.
near and far vision, contrast sensitivity) selected from VFQ-25 including overall
question “At the present time, would you say your eyesight using both eyes (with
your glasses or contact lenses, if you wear them) is excellent/good/fair/poor/very
poor/completely blind?” (if excellent no further questioning); self-administered via
mailed by participants
Care in response to screening test: participants received personalized feedback
report and GPs received summary report (both computer-generated); includes
individually tailored information and recommendations based on the older persons'
responses to the questionnaire (including vision check-ups), general health
information on each domain addressed in the HRA-O questionnaire, and sources of
further information in the community; GPs provided manual with evidence-based
guidelines; other healthcare professionals involved in reinforcement sessions
Setting of program: Home (self-administered screening & 2 home visits providing
reinforcement for some [n=77]), GP offices (routine visits for all), and geriatric
centres for an interdisciplinary group visit for reinforcement (n=503)
Number of interactions after screening & duration of intervention: routine visits with
GPs + 1-2 reinforcements sessions; up to 1 year

132
Other components of screening/assessment: HRA-O is multidimensional
Other components of care potentially impacting vision: one 4-hr group,
empowerment-based structured interdisciplinary session (n=503) or two preventive
home visits from nurse with additional vision assessment (n=77); all GPs for both
groups received training at baseline and bimonthly in risk assessment and health
promotion
Control: Usual care by same trained GPs; vision assessed via HRA-O only at 1-year
followup
Outcomes
Benefits:
Self-reported vision problems: based on 9 HRA-O select vision questions from
VHQ-25 (proportion with ≥1 sub-domain having moderate or greater difficulty)
Harms: NR
Implementation factors:
Eye care professional visits: self-reported vision check-up in previous year
Notes
Data from study publication, published protocol, and author contact (clarifying
definition of outcome).
This study also incorporated a comparison group (not randomized) which was not
considered for this systematic review.
Harari 20083
Objective
To evaluate the effect of using the Health Risk Appraisal for Older Persons (HRA-O)
on health behavior and preventative-care uptake in older, functionally independent,
people in NHS primary care.
Methods
Design: RCT
Country: London, UK
Study period: April 2001-April 2002
Inclusion criteria: 65 yrs and over
Exclusion criteria: nursing home resident, needing help in basic ADLs, dementia,
terminal disease, and non-English speaking
Participants
Recruitment: registered patients of 18 GPs
Sample: Intervention (n=1240); Control (n=1263)
Mean age (SD): Intervention= 74.7(6.4); Control= 74.4(6.2)
Race/ethnicity: NR (all English-speaking)
Females (%): Intervention= 55.3; Controls= 54.6
Falls (%): NR
Lives alone (%): NR
Education (%): NR
Income (%): wide diversity of social classes
Urban (%): urban residential areas
Diabetes (%): Intervention= 7.7; Controls=7.2

133
Dementia (%): exclusion criteria
Residing in nursing homes (%): exclusion criteria
Baseline vision loss: Intervention: 21.4% (Fair, poor or very poor vision); Control: Not
collected
Other disorders of vision (%): NR
Length of follow-up:12 months; loss to follow-up (return of HRA-O questionnaire at 1
yr): Intervention=300 (24%), Control=197 (16%)
Interventions
Intervention:
Vision screening: 1) self-reported vision problems
Tool & administration of screening test: 1) 11 self-reported vision questions (e.g.
near and far vision, contrast sensitivity) selected from VFQ-25 including overall
question “At the present time, would you say your eyesight using both eyes (with
your glasses or contact lenses, if you wear them) is excellent/good/fair/poor/very
poor/completely blind?” (if excellent overall vision no other questions asked); self-
administered via mailed by participants
Care in response to screening test: Patients given feedback (20-35 page report)
about their results, information on each domain assessed in HRA-O and on other
services in community, and a personalized preventative health checklist. They were
given a letter encouraging followup with their GP or practice nurse and a reminder at
6 mo. GPs provided with 1-page summary report (scanned into IT system) and
chose which items to integrate into the electronic patient record with prompts; GPs
also provided manual with evidence-based guidance for preventive practices. No
reinforcement or dedicated professional time.
Setting of program: home (computer-generated feedback) and GP offices during
routine visits
Number of interactions after screening & duration of intervention: variable based on
routine visits; reminders sent after 6 mo to patients not contacting GPs
Other components of screening: HRA-O questionnaire measures 21 domains,
including medical history, health measurements, medications, pain, oral health,
hearing, nutrition, injury prevention, tobacco and alcohol use and social network.
Other components of care potentially impacting vision: All GPs and practice nurses
for both groups received training at baseline and bimonthly in risk assessment and
health promotion.
Control: Usual care by same trained GPs; vision assessed via HRA-O only at 1-year
followup
Outcomes
Benefits:
Self-reported vision problems: based on 9 HRA-O select vision questions from
VHQ-25 (proportion with ≥1 sub-domain having moderate or greater difficulty)

134
Harms: NR
Implementation factors:
Eye professional visits: self-reported vision check-ups in previous yr
Notes
Data from study publication, published protocol, and author contact.
Results are from analysis of individual patient data provided by authors.
This study also incorporated a comparison group (not randomized) which was not
considered for this systematic review.
Tay 20064
Objective
To assess the need for, and the use of eye care services in older people seeking
aged care.
Methods
Design: RCT
Country: Australia
Study period: 2003-2004
Inclusion criteria: 65 years or older, English speaking, living at home, being
assessed for aged care provision
Exclusion criteria: profound dementia
Participants
Recruitment: approached clients attending aged care assessment services at
Westmead Hospital, Sydney, serving residents living in three local government areas
with an estimated population of almost 400 000
Sample: Intervention (n=96); Control (n=92)
Mean age (SD): 82 (6) in final sample (15% ≤74 yrs; 34% ≥85 yrs)
Race/ethnicity: NR
Females (%): 64 (in final sample)
Falls (%): 55 (last 12 months)
Lives alone (%): 34 (in final sample)
Education (%): NR
Income (%): NR
Urban (%): NR
Diabetes (%): NR
Dementia (%): NR
Residing in nursing homes (%): exclusion criteria (all being assessed for aged care)
but 41% receiving health services such as home care
Baseline vision loss: Intervention: 31% bilateral & 29% unilateral visual impairment
Other disorders of vision (%): NR
Length of follow-up: 12 mos; loss to follow-up: 67 (36%; 30% in survivor group); NR
by group
Interventions Factorial 2x2 with vision, hearing, vision and hearing, no testing (self-report
135
screening only groups
Intervention:
Vision screening: measured distance and near visual acuity (with pinhole correction)
and visual field; self-reported vision problems
Tool & administration of screening test: presenting distance visual acuity
(VectorVision logMAR chart), binocular near vision and visual field using
confrontation method, pinhole testing if presenting acuity <6/6; Are you able to
recognize a friend across the street?; Can you read ordinary print in the newspaper
reasonably well, with your glasses?
Care in response to screening test: Only vision tests (not self-report) led to referrals.
People with under-corrected refractive error (pinhole VA improved at least 10
letters/2 lines in those with presenting VA <6/6), bilateral visual impairment (better
eye VA <6/12), or having suspected visual field defects were recommended to have
further assessment by eye care professionals.
Setting of program: home visits or day hospital
Number of interactions after screening: 0
Other components of screening/assessment: hearing for half, multicomponent aged
care assessments
Other components of intervention potentially impacting vision: no obvious
Control: No vision testing/measurement; self-reported vision assessed during
routine aged care assessment and interview using a standardized questionnaire
(10% referred to eye care professionals)
Outcomes
Benefits:
Impaired visual acuity: distance high contrast VA (numbers of letters)
Impaired visual acuity: proportion with bilateral visual impairment (presenting
acuity <6/12 in the better eye)
Harms: NR
Implementation factors:
Referrals provided
Uptake of referrals
Notes Data from published paper with confirmation of interventions and results by author.
Lord 20055
Objective
To determine whether an individualized falls prevention program comprising
exercise, visual, and counseling interventions can reduce physiological falls risk and
falls in older people at some risk for falls.
Methods
Design: RCT
Country: Australia
Study period: NR
Inclusion criteria: community-dwelling people aged 75 and older, living in northern
Sydney, Australia, at some risk for falls via physiological profile assessment (PPA;
136
9% consenting people excluded for this).
Exclusion criteria: minimal English language skills, blind, Parkinson’s disease, or a
Short Portable Mental Status Questionnaire score less than 7.
Participants
Recruitment: drawn from a health insurance company membership database.
Sample: Extensive Intervention (n=210); Minimal Intervention Group (n=206);
Control (n=204)
Mean age (SD): Extensive Intervention=80.3 (4.3); Minimal Intervention Group=80.7
(4.6); Control= 80.2 (4.6)
Race/ethnicity: NR
Females (%): Extensive Intervention=66.7; Minimal Intervention Group=62.1;
Controls= 69.1
Falls (%): Extensive Intervention=33.3; Minimal Intervention Group=26.2;
Controls=29.4 (fall in last year; difference between groups for fear of falling)
Lives alone (%): NR
Education (%): NR
Income (%): NR
Urban (%): NR
Diabetes (%): Extensive Intervention= 7.6; Minimal Intervention Group=5.8;
Controls=7.8
Dementia (%): exclusion criteria
Residing in nursing homes (%): exclusion criteria
Baseline vision loss: (to come after analysis)
Other disorders of vision (%): NR
Length of follow-up: 6 months for vision outcomes; loss to follow-up: Extensive
Intervention=41 (19.5%), Minimal Intervention Group=35 (17%); Control=26 (12.7%)
Interventions
Extensive Intervention:
Vision screening: measured visual acuity and other vision loss
Tool & administration of screening test: presenting high and low contrast visual
acuity assessed with logMAR chart at 3m, edge-contrast sensitivity was assessed
with the Melbourne Edge Test and depth perception with the Howard-Dohlman
apparatus; administered by investigators
Care in response to screening test: Participants received risk assessment report
including written recommendations. If subjects had one or more PPA vision
standardized test scores less than -1 they received interventions for maximizing
vision, including referral to an eye specialist, change in spectacles and cataract
surgery. Referral also if no eye examination in 6mos. Advice regarding wearing
multifocal glasses at home only.
Setting of program: falls assessment clinic
Number of interactions after screening & duration of intervention: counselling
session after the assessment (may have also received twice weekly exercise
classes)
Other components of screening/assessment: Physiological Profile Assessment
which includes lower limb sensation, strength of muscles, reaction time, and body

137
sway; Short-Form 12 Health Status Questionnaire
Other components of care potentially impacting vision: counselling regarding
medications and other medical conditions.
Minimal Intervention: Same screening tool and setting. Received a report outlining
their falls risk, a profile of their test results and specific recommendations for
preventing falls. They received brief advice about how to maximize their vision. No
referrals or counselling session.
Control: No intervention; baseline vision assessment. At the end of 12 months they
received a report outlining their falls risk, a profile of test results and
recommendations for preventing falls.
Outcomes
Benefits:
Impaired visual acuity: mean change in visual acuity: high contrast distance visual
acuity, proportion with minimally important difference (0.1 logMAR change for
worse and better) in visual acuity
Harms: NR
Implementation factors: NR
Notes
Data from published report and author contact. Results based on analysis of
individual patient data provided by author. Each intervention group is compared with
the control group for analysis, with adjustment for sample size in the control group.
Smeeth 20036
Objective
To determine the effectiveness of screening for visual impairment in people aged 75
or over as part of a multidimensional screening programme.
Methods
Design: RCT cluster, 2x2 factorial for 1) universal vs targeted assessment, and 2)
multidisciplinary geriatric vs. usual primary care management
Country: United Kingdom
Study period: 1995 to 1999
Inclusion criteria: 75 years or over, registered with participating general practices
Exclusion criteria: resident in a long stay hospital, nursing home, terminally ill
Participants
Recruitment: random sample of 4340 participants from 20 general practices; part of
larger RCT of 106 general practices
Sample: Universal screening (n=2140); Targeted screening (n=2200)
Mean age (SD): Universal =80.3 (NR); Targeted =79.9 (NR)
Race/ethnicity: NR
Females (%): Universal =60.2; Targeted =63.2
Falls (%): Universal =20.4; Targeted =17.7 (at home over past 6 mo)
Lives alone (%): NR (45% in larger trial sample)
Education (%): NR
Income (%): NR (clusters stratified for Jarman index of underprivileged areas)
Urban (%): NR
Diabetes (%): NR

138
Dementia (%): NR
Residing in nursing homes (%): exclusion criteria
Baseline vision loss (%): Universal: 28.8; Targeted: 43 (visual acuity <6/18 in either
eye); targeted participants only had testing if meeting detailed screening criteria (see
below description of control intervention)
Other disorders of vision (%): Universal 3; targeted 1 (Blind)
Length of follow-up: 36 to 60 mos (median 3.9 yr); loss to follow-up: Universal=1311
(61% [42.1% of those alive]), Targeted=1222 (66% [32.3% of those alive])
Interventions
Intervention (universal screening):
Vision screening: measured visual acuity
Tool & administration of screening test: visual acuity (logMAR scale using a Glasgow
acuity chart) Snellen equivalent acuity, people with VA less than 6/18 in either eye
had measurements repeated using a pinhole occlude; administered by trained nurse
Care in response to screening test: Referred to ophthalmologist if pinhole vision was
less (worse) than 6/18, unless they were registered as blind or had seen an
ophthalmologist in the previous year. Participants whose presenting VA was worse
than 6/18 but with pinhole testing improved to better than 6/18 (refractive error) were
advised to see an optician.
Setting of program: GP offices or at home (33.5%)
Number of interactions after screening: none
Other components of screening/assessment: detailed assessment comprehensive
for multiple clinical domains; also received brief assessment that includes vision
component
Other components of intervention potentially impacting vision: none obvious
Control (targeted screening): Brief screening assessment (all participants) that
included a question about difficulty seeing newsprint; administered by nurse, office
staff or mail. Only people found to have a pre-specified range and level of problems
during the brief assessment (3 or more problems or any one of 4 “serious”
symptoms; no referral for just vision) were invited to have the detailed assessment
including visual acuity and offered referrals as suitable (overall 5.5% had detailed
assessments).
Outcomes
Benefits:
Vision-related functional limitations: mean composite score of VFQ-25 (range:
100 points; higher scores better)
Impaired visual acuity: 1) Proportion with impaired visual acuity (worse than 6/18
in either and both eyes; WHO standards), 2) Proportion with impaired visual
acuity (worse than 6/12 in either and both eyes; North American standards)
Harms: NR
Implementation factors:
Referrals/recommendations to those eligible based on screen
Uptake of referrals
Notes Data from publication.
139
Day 20027
Objective
To test the effectiveness of, and explore interactions between, three interventions to
prevent falls among older people.
Methods
Design: RCT (full factorial 2x2x2 design with 8 groups based on vision, strength and
balance, home modifications, and control)
Country: Australia
Study Period: NR
Inclusion criteria: 70 years and older, living in their own home/accommodation
Exclusion criteria: participated in moderate physical activity with balance component
in last 2 mo; could not walk 10-20 meters without rest, angina, or help; severe
respiratory or cardiac disease; psychiatric illness prohibiting participation; dysphasia;
recent major home modifications; education or language score > 4 on short portable
mental status questionnaire; no approval from GP
Participants
Recruitment: registered on Australian electoral roll (96% eligible voters registered)
Sample:
For vision outcomes (n=442 randomly selected for vision assessment of 971
completing from 1090 enrolled): vision alone (n=51); all those receiving vision
intervention (n=206); no intervention (n=47); all receiving no vision intervention
(n=236)
For falls outcomes (n=1090): vision alone (n=139); all those receiving vision
intervention (n=547); no intervention (n=137); all receiving no vision intervention
(n=543)
Mean age (SD): 76.1 (5.0): 46% 70-74, 7.3% over 85 (all participants)
Race/ethnicity (%) White: NR
Females (%): 59.8
Falls (%): 6.3 in past month
Lives alone (%): 54%
Education (%): NR
Income (%): NR
Urban (%): urban community of Melbourne
Diabetes (%): NR
Dementia (%): NR
Residing in nursing homes (%): exclusion criteria
Baseline vision: high contrast VA in best eye: 0.08 (0.19) logMAR; low contrast in
best eye 0.38 (0.19) logMAR
Other disorders of vision (%): NR
Length of follow-up: up to 18 mo; loss to follow-up: for vision, only those completing
[89%] with baseline variables similar to all participants; for falls 11% overall withdrew
but similar total person-years across groups (range: 167-188 person yrs)
Interventions Factorial design of 3 possible interventions with vision: vision, vision + strength and
balance (1-hour class for 15 weeks), vision + home hazards (removal or modification

140
of hazards), and 3 without (no intervention, strength and balance, home hazards)
Intervention (vision intervention):
Vision screening: structured measurement of visual acuity and other vision problems
Tool & administration of screening test: dual (high and low contrast) visual acuity
(Verbaken chart; with glasses 2m from chart), stereopsis (random dot stereo
butterfly test and crossed disparity circles), and field of view (OKP glaucoma
screening test); administered by trained assessor
Care in response to screening test: If a participant's vision tested below
predetermined criteria and if he or she was not already receiving treatment for the
problem identified, the participant was referred to his or her usual eye care provider,
GP, or local optometrist, to whom the vision assessment results were given.
Setting of program: home
Number of interactions after screening: vision only group: none except for those
referred to eye professional or GP; other groups receiving vision (up to 15 if in
strength and balance)
Other components of screening/assessment: vision only group: none; other groups
receiving vision: strength and balance and home hazards
Control: No intervention until after study; vision assessment at baseline; all 4 groups
not allocated to vision screening received Australian Optometrist Association's
brochure on eye care for those aged over 40.
Outcomes
Benefits:
Falls: risk of falls requiring medical attention (sought medical care or attended
hospital); reported using monthly calendar system to record daily falls, with follow
up if not submitting or if reporting fall. Results using main effects factorial model
for all 3 groups receiving vision (no interaction effects found); further analysis
using negative binomial regression for singular and additive average effects of
intervention vs. not receiving intervention.
Impaired visual acuity: mean change in logMAR for high contrast visual acuity
Harms: NR
Implementation factors:
Referrals for those eligible
Uptake of referrals
Notes Data from original (via online version) and subsequent published paper, and author
contact for additional information on results (no additional vision results available)
and screening tool.
Newbury 20018
Objective
To measure the outcomes of a health assessment, conducted by a nurse, of people
aged 75 years and older (75+HA) living independently in their own homes.
Methods
Design: RCT
Country: Australia
Study Period: August 1998 – February 1999
141
Inclusion criteria: 75 years and older, living independently in the community
Exclusion criteria: residing in a nursing home, suffering from dementia, unable to
consent to the study
Participants
Recruitment: 6 general practices in a suburban area, with random sample of every
20th patient in register assessed for eligibility and invited via letter and follow-up
telephone call
Sample: Intervention (n=50); Control (n=50)
Mean age (SD): Intervention=78.96 (3.49); Control=80.76 (3.76)
Race/ethnicity: NR
Females (%): Intervention=60; Control=66
Falls (%): Intervention= 45; Control= 38.6
Lives alone (%): NR
Education (%): NR
Income (%): NR
Urban (%): suburb of Adelaide
Diabetes (%): NR
Dementia (%): exclusion criteria
Residing in nursing homes (%): exclusion criteria
Other disorders of vision (%): Intervention= Glaucoma 14%, cataract 32%, macular
degeneration 2%, other 14% (but all at year 2 reduced so thought error); Control=
Glaucoma 10%, cataract 16%, macular degeneration 2%, other 2%
Length of follow-up: 12 months; loss to follow-up: Intervention=5 (10%); Control=6
(8.5%)
Interventions
Intervention:
Vision screening: 2 self-report questions within 75+HA tool
Tool & administration of screening test: “Do you have any difficulty in seeing
newsprint, even when you are wearing your glasses?”; self-assessed vision as very
good, good, fair, poor or blind; self-reporting of visual pathology (Cataracts, macular
degeneration, diabetic retinopathy etc) and driving; administered by nurse
Care in response to screening test: Results sent to nominated GP right after
assessment.
Setting of program: home visit for screening and GP encounters for follow up
Number of interactions after screening: only routine visits to GP
Other components of screening/assessment: 75+HA assesses 13 domains including
hearing, physical condition, medication, compliance, cognition, mood AGL, mobility,
nutrition, social and housing and SF-36. Geriatric Depression Scale also
administered.
Other components of intervention potentially impacting vision: none other than
conditions screened
Control: Usual care (no home visits and GP blinded); vision assessment via 75+HA
at 1 year follow-up.
Outcomes Benefits:
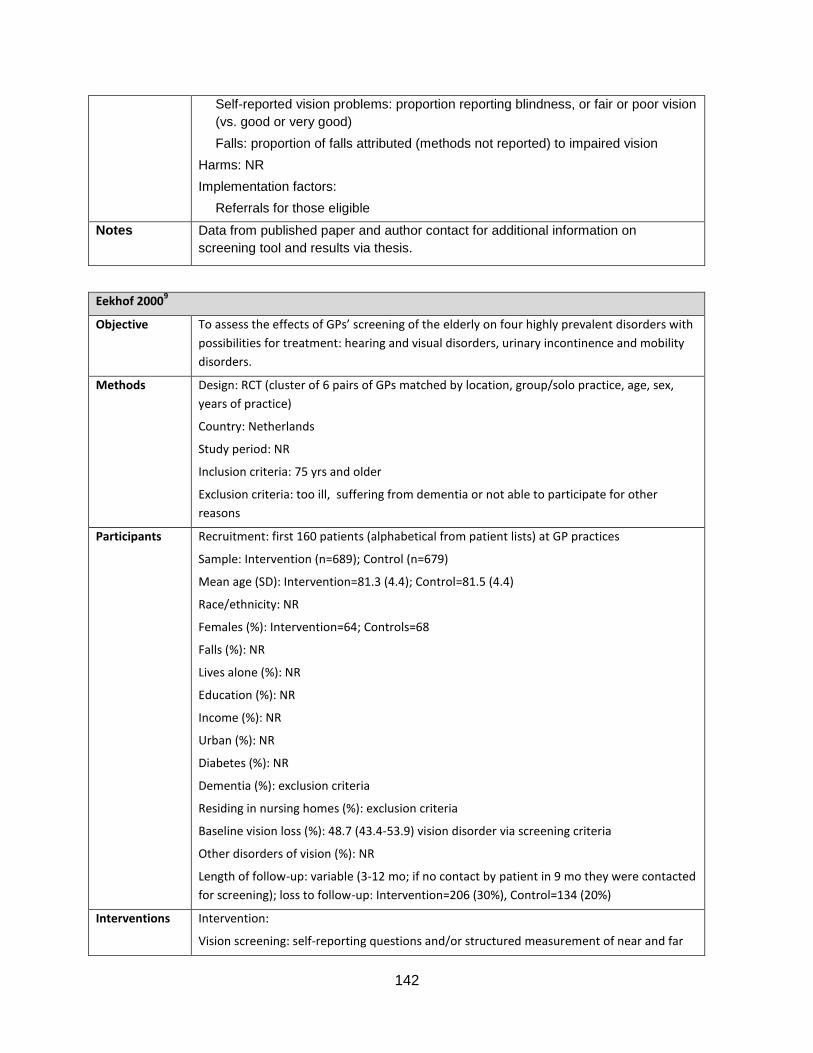
142
Self-reported vision problems: proportion reporting blindness, or fair or poor vision
(vs. good or very good)
Falls: proportion of falls attributed (methods not reported) to impaired vision
Harms: NR
Implementation factors:
Referrals for those eligible
Notes
Data from published paper and author contact for additional information on
screening tool and results via thesis.
Eekhof 20009
Objective
To assess the effects of GPs’ screening of the elderly on four highly prevalent disorders with
possibilities for treatment: hearing and visual disorders, urinary incontinence and mobility
disorders.
Methods
Design: RCT (cluster of 6 pairs of GPs matched by location, group/solo practice, age, sex,
years of practice)
Country: Netherlands
Study period: NR
Inclusion criteria: 75 yrs and older
Exclusion criteria: too ill, suffering from dementia or not able to participate for other
reasons
Participants
Recruitment: first 160 patients (alphabetical from patient lists) at GP practices
Sample: Intervention (n=689); Control (n=679)
Mean age (SD): Intervention=81.3 (4.4); Control=81.5 (4.4)
Race/ethnicity: NR
Females (%): Intervention=64; Controls=68
Falls (%): NR
Lives alone (%): NR
Education (%): NR
Income (%): NR
Urban (%): NR
Diabetes (%): NR
Dementia (%): exclusion criteria
Residing in nursing homes (%): exclusion criteria
Baseline vision loss (%): 48.7 (43.4-53.9) vision disorder via screening criteria
Other disorders of vision (%): NR
Length of follow-up: variable (3-12 mo; if no contact by patient in 9 mo they were contacted
for screening); loss to follow-up: Intervention=206 (30%), Control=134 (20%)
Interventions
Intervention:
Vision screening: self-reporting questions and/or structured measurement of near and far

143
visual acuity under usual functioning (e.g. with spectacles if worn)
Tool & administration of screening test: having difficulty in recognizing a face at 4 m, and/or
reading the normal letters in a newspaper, and/or impaired vision with both eyes (Snellen
chart ˂0.3 [20/40]), or not being able to read normal newspaper letters at 25 cm distance;
administered by GPs
Care in response to screening test: GP discussed results with the patient; followed new
findings with treatment or referrals to specialists (usual care of GPs)
Setting of program: GP offices and/or homes
Number of interactions after screening & duration of intervention: not specified except
frequent visits for some
Other components of screening/assessment: screening for hearing, urinary incontinence,
mobility disorders
Other components of intervention potentially impacting vision outcomes: none
Control: Not selected or screened in the first year; screened along with intervention group
in the second year.
Outcomes
Benefits:
Self-reported vision problems: proportion with disorder in vision via difficulty in
recognizing a face at 4 m, and/or reading the normal letters in a newspaper, and/or
impaired vision with both eyes (Snellen chart ˂0.3), or not being able to read normal
newspaper letters at 25 cm distance
Harms: NR
Implementation factors:
Referrals/recommendations for those eligible
Uptake of referrals (referrals to ophthalmologist or other interventions provided by GP)
Notes
Data from published paper.
GPs in Netherlands have mean 6 contacts per year with people 75+ years old, with many
contacts taking place at homes.
Moore 199710
Objective
To test the effectiveness of a 10-minute office-staff administered screen to evaluate
malnutrition/weight loss, visual impairment, hearing loss, cognitive impairment,
urinary incontinence, depression, physical limitation, and reduced leg mobility among
older persons seen in office practice.
Methods
Design: RCT cluster (13 pairs of physicians matched by specialty [17 community-
based internists, 9 family physicians])
Country: Los Angeles, USA
Study Period: NR
Inclusion criteria: 70 yrs or older, English speaking, not acutely or terminally ill, and
able to answer questions; new visit or physical examination
Exclusion criteria: NR
Participants Recruitment: 8-12 from each practice; no specific protocol except inclusion criteria
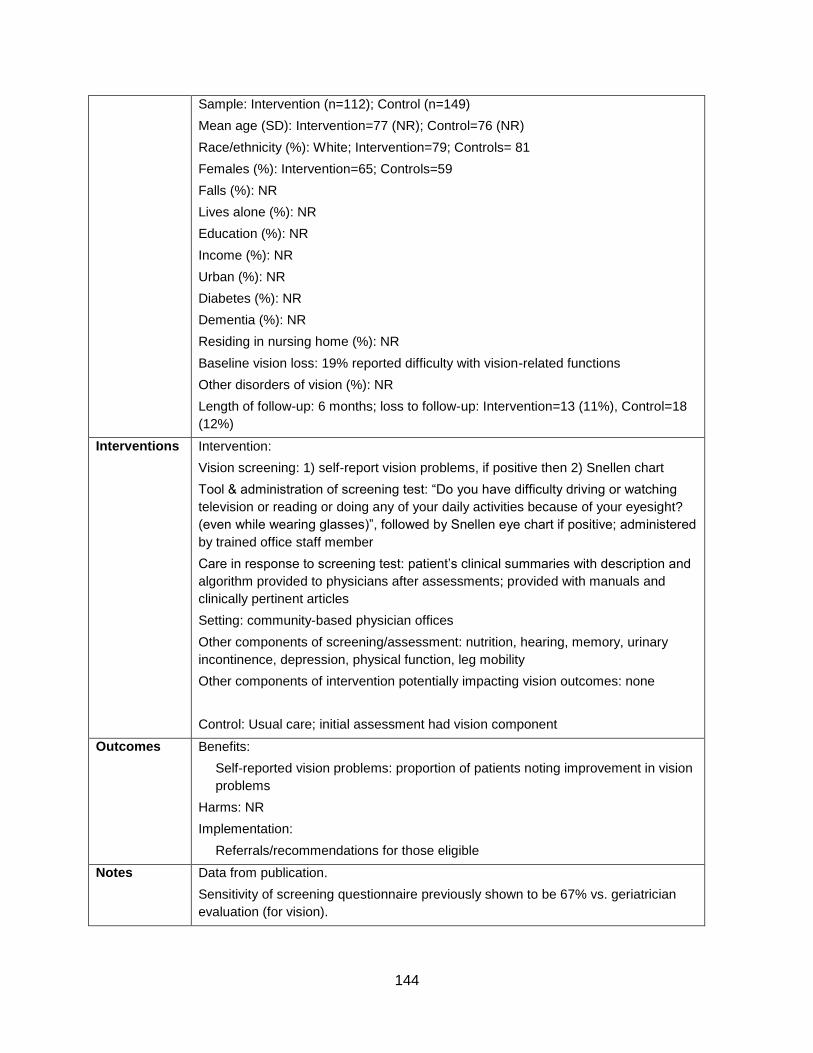
144
Sample: Intervention (n=112); Control (n=149)
Mean age (SD): Intervention=77 (NR); Control=76 (NR)
Race/ethnicity (%): White; Intervention=79; Controls= 81
Females (%): Intervention=65; Controls=59
Falls (%): NR
Lives alone (%): NR
Education (%): NR
Income (%): NR
Urban (%): NR
Diabetes (%): NR
Dementia (%): NR
Residing in nursing home (%): NR
Baseline vision loss: 19% reported difficulty with vision-related functions
Other disorders of vision (%): NR
Length of follow-up: 6 months; loss to follow-up: Intervention=13 (11%), Control=18
(12%)
Interventions
Intervention:
Vision screening: 1) self-report vision problems, if positive then 2) Snellen chart
Tool & administration of screening test: “Do you have difficulty driving or watching
television or reading or doing any of your daily activities because of your eyesight?
(even while wearing glasses)”, followed by Snellen eye chart if positive; administered
by trained office staff member
Care in response to screening test: patient’s clinical summaries with description and
algorithm provided to physicians after assessments; provided with manuals and
clinically pertinent articles
Setting: community-based physician offices
Other components of screening/assessment: nutrition, hearing, memory, urinary
incontinence, depression, physical function, leg mobility
Other components of intervention potentially impacting vision outcomes: none
Control: Usual care; initial assessment had vision component
Outcomes
Benefits:
Self-reported vision problems: proportion of patients noting improvement in vision
problems
Harms: NR
Implementation:
Referrals/recommendations for those eligible
Notes
Data from publication.
Sensitivity of screening questionnaire previously shown to be 67% vs. geriatrician
evaluation (for vision).
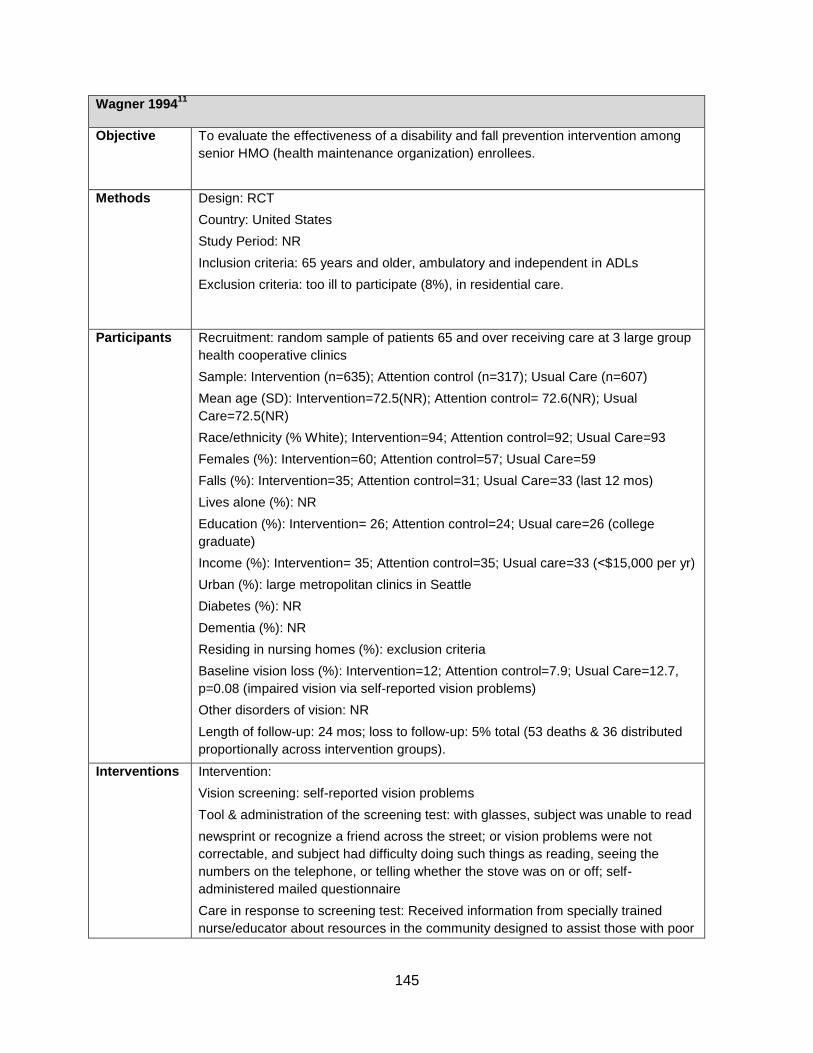
145
Wagner 199411
Objective
To evaluate the effectiveness of a disability and fall prevention intervention among
senior HMO (health maintenance organization) enrollees.
Methods
Design: RCT
Country: United States
Study Period: NR
Inclusion criteria: 65 years and older, ambulatory and independent in ADLs
Exclusion criteria: too ill to participate (8%), in residential care.
Participants
Recruitment: random sample of patients 65 and over receiving care at 3 large group
health cooperative clinics
Sample: Intervention (n=635); Attention control (n=317); Usual Care (n=607)
Mean age (SD): Intervention=72.5(NR); Attention control= 72.6(NR); Usual
Care=72.5(NR)
Race/ethnicity (% White); Intervention=94; Attention control=92; Usual Care=93
Females (%): Intervention=60; Attention control=57; Usual Care=59
Falls (%): Intervention=35; Attention control=31; Usual Care=33 (last 12 mos)
Lives alone (%): NR
Education (%): Intervention= 26; Attention control=24; Usual care=26 (college
graduate)
Income (%): Intervention= 35; Attention control=35; Usual care=33 (˂$15,000 per yr)
Urban (%): large metropolitan clinics in Seattle
Diabetes (%): NR
Dementia (%): NR
Residing in nursing homes (%): exclusion criteria
Baseline vision loss (%): Intervention=12; Attention control=7.9; Usual Care=12.7,
p=0.08 (impaired vision via self-reported vision problems)
Other disorders of vision: NR
Length of follow-up: 24 mos; loss to follow-up: 5% total (53 deaths & 36 distributed
proportionally across intervention groups).
Interventions
Intervention:
Vision screening: self-reported vision problems
Tool & administration of the screening test: with glasses, subject was unable to read
newsprint or recognize a friend across the street; or vision problems were not
correctable, and subject had difficulty doing such things as reading, seeing the
numbers on the telephone, or telling whether the stove was on or off; self-
administered mailed questionnaire
Care in response to screening test: Received information from specially trained
nurse/educator about resources in the community designed to assist those with poor
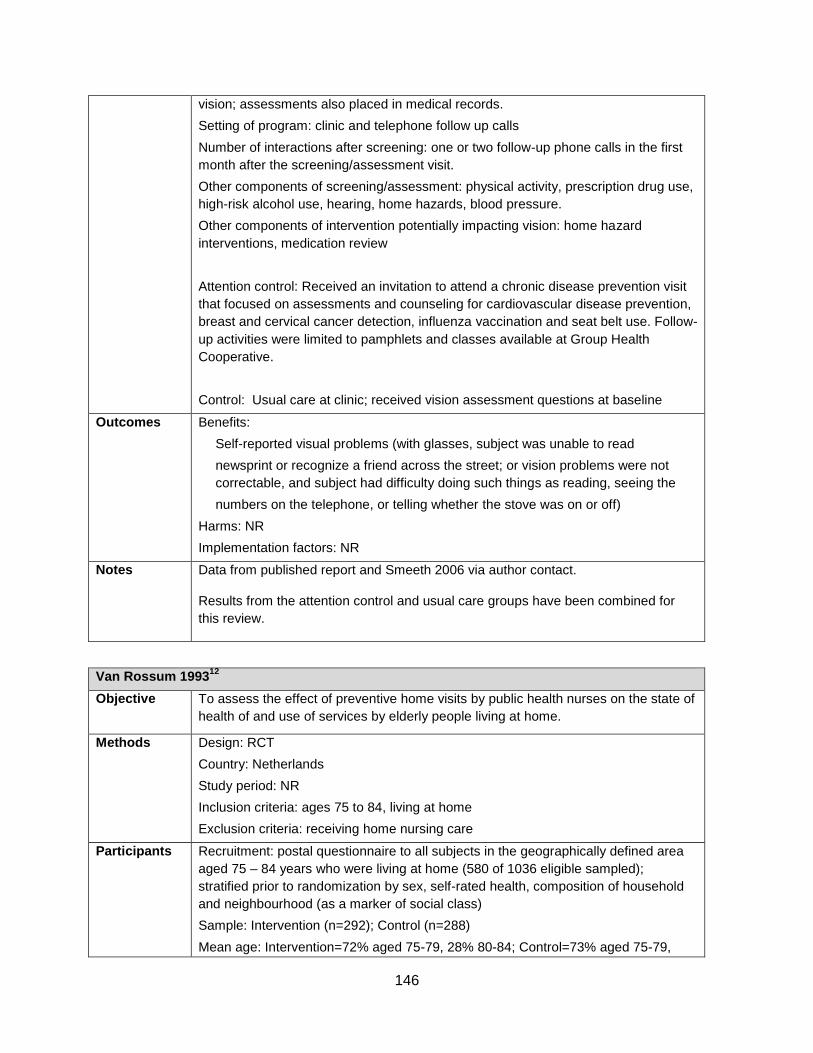
146
vision; assessments also placed in medical records.
Setting of program: clinic and telephone follow up calls
Number of interactions after screening: one or two follow-up phone calls in the first
month after the screening/assessment visit.
Other components of screening/assessment: physical activity, prescription drug use,
high-risk alcohol use, hearing, home hazards, blood pressure.
Other components of intervention potentially impacting vision: home hazard
interventions, medication review
Attention control: Received an invitation to attend a chronic disease prevention visit
that focused on assessments and counseling for cardiovascular disease prevention,
breast and cervical cancer detection, influenza vaccination and seat belt use. Follow-
up activities were limited to pamphlets and classes available at Group Health
Cooperative.
Control: Usual care at clinic; received vision assessment questions at baseline
Outcomes
Benefits:
Self-reported visual problems (with glasses, subject was unable to read
newsprint or recognize a friend across the street; or vision problems were not
correctable, and subject had difficulty doing such things as reading, seeing the
numbers on the telephone, or telling whether the stove was on or off)
Harms: NR
Implementation factors: NR
Notes Data from published report and Smeeth 2006 via author contact.
Results from the attention control and usual care groups have been combined for
this review.
Van Rossum 199312
Objective
To assess the effect of preventive home visits by public health nurses on the state of
health of and use of services by elderly people living at home.
Methods
Design: RCT
Country: Netherlands
Study period: NR
Inclusion criteria: ages 75 to 84, living at home
Exclusion criteria: receiving home nursing care
Participants
Recruitment: postal questionnaire to all subjects in the geographically defined area
aged 75 – 84 years who were living at home (580 of 1036 eligible sampled);
stratified prior to randomization by sex, self-rated health, composition of household
and neighbourhood (as a marker of social class)
Sample: Intervention (n=292); Control (n=288)
Mean age: Intervention=72% aged 75-79, 28% 80-84; Control=73% aged 75-79,

147
27% 80-84.
Race/ethnicity: NR
Females (%): Intervention=58; Controls=57
Falls (%): NR
Lives alone (%): Intervention=39; Controls=39
Education (%): NR
Income (%): NR
Urban (%): conducted in Weert (60 000 inhabitants)
Diabetes (%): NR
Dementia (%): NR
Residing in nursing homes (%): exclusion criteria
Baseline vision loss: NR
Other disorders of vision (%): NR
Length of follow-up: 36 mos; loss to follow-up: Intervention=61 (20%; 42 deaths),
Control=67 (23%; 50 deaths)
Interventions
Intervention:
Vision screening: self-reported vision problems
Tool & administration of screening test: “How do you assess your vision at present?”;
administered by trained nurse
Care in response to screening test: Those answering ‘fair’, ‘not so good’ or bad’ to
the screening question advised by nurse to contact an optometrist.
Setting of program: home visit
Number of interactions after screening: 4 visits per year for 3 years, extra visits were
done if necessary, telephone contact with the nurse was available
Other components of screening/assessment: functional state, medication, social
contacts and housing conditions
Other components of intervention potentially impacting vision: regular home visits (4
visits per year over 3 years) and telephone calls as needed; no physical
examinations but discussions, information, and advice provided based on checklist
Control: No home visits; no vision assessment at baseline
Outcomes
Benefits:
Self-reported vision problems: proportion answering fair, not so good or bad
Harms: NR
Implementation factors: NR
Notes Data from published paper and Smeeth 2006 after their author contact.
Vetter 199213
Objective
To assess whether intervention by a health visitor could reduce the number of
fractures, over a four year period, in those aged 70 and over.

148
Methods
Design: RCT
Country: United Kingdom
Study period: NR
Inclusion criteria: registered with a general practice.
Exclusion criteria: likely to refuse trial entry
Participants
Recruitment: patient lists of 5 GP offices of patients 70 years and older
Sample: Intervention (n=350); Control (n=324)
Mean age (SD): NR; all aged 70 and over (similar between groups)
Race/ethnicity: NR
Females (%): NR; similar distribution between groups
Falls (%): 23% each group; fractures 3% annual prevalence each group
Lives alone (%): NR
Education (%): NR
Income (%): NR
Urban (%): NR
Diabetes (%): NR
Dementia (%): NR
Residing in nursing homes (%): exclusion criteria
Baseline vision: NR
Other disorders of vision (%): NR
Length of follow-up: 48 mos; loss to follow-up: Intervention=110 (31.4% [25% died]);
Control=114 (35.2% [33% died])
Interventions
Intervention:
Vision screening: self-reported vision problems
Tool & administration of screening test: two questions about glasses and difficulty
seeing and third question about recent eye exam; administered by research
assistant
Care in response to screening test: Those reporting difficulties seeing were referred
by a health visitor to an optometrist or to their GP, and were offered advice from the
health visitor.
Setting of program: home visit within GP practices
Number of interactions after screening: at least annually; as often as was thought
necessary by the health visitor
Other components of screening/assessment: annual assessment on nutrition,
medical conditions, environment and improvement to general muscle tone and
fitness aimed at reducing falls and fractures
Control: Usual care; vision assessment at baseline
Outcomes
Benefits:
Self-reported vision problems: proportion with a positive response to the question
“Do you have any difficulty seeing (even when wearing your glasses)?”
149
Harms: NR
Implementation factors: NR
Notes
Data from published paper; definition of outcome measurement and results reported
by Smeeth 2006 after their author contact.
McEwan 199014
Objective
To evaluate the effectiveness of a primary care linked screening programme to
resolve health and related problems and to improve the quality of life of elderly
people.
Methods
Design: RCT
Country: United Kingdom
Study period: 1986-1988
Inclusion criteria: 75 years and over who were registered with a Newcastle practice
in 1986
Exclusion criteria: too ill for assessment, in hospital
Participants
Recruitment: registered patients of a general practice in Newcastle
Sample: Intervention (n=151); Control (n=145)
Mean age (SD): NR, ≥75
Race/ethnicity: NR
Females (%): NR
Falls (%): NR
Lives alone (%): NR (no difference between groups)
Education (%): NR
Income (%): NR, wide diversity of social classes
Urban (%): NR, urban residential area
Diabetes (%): NR
Dementia (%): NR
Residing in nursing homes (%): NR (some, but no difference between groups)
Baseline vision loss: 23% difficulty reading newspaper
Other disorders of vision (%): NR
Length of follow-up:20 months; loss to follow-up: Intervention=33 (22%); Control=34
(23%)
Interventions
Intervention:
Vision screening: self-reported vision problems
Tool & administration of screening test: question about vision (difficulty reading
ordinary newsprint) in initial interview with community nurse interviewer; additional
screening by care planning nurse
Care in response to screening test: Care planning nurse gave advice and or referred
to an optometrist those reporting “always” OR “quite often” problems; primary care
team consultation.

150
Setting of program: home visit
Number of interactions after screening & duration of intervention: 1 visit
Other components of screening/assessment: multicomponent home nurse
assessment and care plan: ADLs, social functioning, current medical problems,
compliance with medication
Other components of care potentially impacting vision: Care plan activities related to
medication, social function etc. Provision of a booklet describing health, social and
voluntary services.
Control: Usual care from primary care team; received screening assessment
Outcomes
Benefits:
Self-reported vision problems: proportion who “always” or “quite often” had
difficulty reading ordinary newsprint (with glasses worn)
Harms: NR
Implementation factors: NR
Notes Published and unpublished data. Data on outcome measurement and results
reported by Smeeth 2006 after their author contact.
Vetter 198415
Objective
To test the effectiveness of health visitors’ visiting and monitoring of a caseload of
elderly people in their respective general practices.
Methods
Design: RCT
Country: United Kingdom
Study period: NR
Inclusion criteria: born in 1909 or before (70 years old or over), living at home,
patient at one of two general practices
Exclusion criteria: permanent residential care
Participants
Recruitment: age-sex register of 2 general practices (10 GPs in total) of all patients
born in 1909 or before, living at home
Sample: Intervention (n=577); Control (n=571)
Mean age (SD): NR; all over age 70
Race/ethnicity: NR
Females (%): NR
Falls (%): NR
Lives alone (%): NR
Education (%): NR
Income (%): NR, higher socioeconomic status in rural area
Urban (%): Intervention= 51; Controls=52
Diabetes (%): NR
Dementia (%): NR
151
Residing in nursing homes (%): exclusion criteria
Baseline vision loss: NR
Other disorders of vision (%): NR
Length of follow-up: 24 mos; loss to follow-up: Intervention=89 (15.4%; 80 deaths),
Control=115 (20%; 105 deaths)
Interventions
Intervention:
Vision screening: self-report vision problems
Tool & administration of screening test: two questions about glasses and difficulty
seeing; health visitor
Care in response to screening test: Those reporting difficulties seeing were referred
by the health visitor to an optometrist or to their GP and were offered advice from the
health visitor.
Setting of program: home visits within GP practices
Number of interactions after screening: one unsolicited visit a year plus extras as
needed
Other components of screening/assessment: semi-structured questions about
physical, mental and social characteristics
Other components of intervention potentially impacting vision: annual home visits
with assessments and advice including information on services, benefits and
allowances
Control: Usual care; no home visits but received initial interview with screening
question
Outcomes
Benefits:
Self-reported vision problems: proportion with a positive response to the question
“Do you have any difficulty seeing (even when wearing your glasses)”
Harms: NR
Implementation factors: NR
Notes Data from published paper and systematic review with author contact for results.
References
1. Haanes GG, Kirkevold M, Hofoss D, et al. An intervention designed to improve sensory impairments in the
elderly and indoor lighting in their homes: an exploratory randomized controlled trial. J Multidiscip
Healthc. 2015(8):11-20. doi: http://dx.doi.org/10.2147/JMDH.S71718. PMID: 25678795. 2. Dapp U, Anders JA, von Renteln-Kruse W, et al. A randomized trial of effects of health risk appraisal
combined with group sessions or home visits on preventive behaviors in older adults. J Gerontol A Biol Sci
Med Sci. 2011:66(5):591-8. PMID: 21350242. 3. Harari D, Iliffe S, Kharicha K, et al. Promotion of health in older people: a randomised controlled trial of
health risk appraisal in British general practice. Age Ageing. 2008;37(5):656-71. PMID: 18755784. 4. Tay T, Rochtchina E, Mitchell P, et al. Eye care service utilization in older people seeking aged care. Clin
Exp Ophthalmol. 2006:34(2):141-5. doi: 10.1111/j.1442-9071.2006.01139.x. PMID: 16626428.
152
5. Lord SR, Tiedemann A, Chapman K, et al. The effect of an individualized fall prevention program on fall
risk and falls in older people: a randomized, controlled trial. J Am Geriatr Soc. 2005;53(8):1296-304.
PMID: 16078954. 6. Smeeth L, Fletcher AE, Hanciles S, et al. Screening older people for impaired vision in primary care:
cluster randomised trial. BMJ. 2003:1;327(7422):1027. doi: 10.1136/bmj.327.7422.1027. PMID:
14593039. 7. Day L, Fildes B, Gordon I, et al. Randomised factorial trial of falls prevention among older people living in
their own homes. BMJ. 2002;325(7356):128. PMID: 12130606. 8. Newbury JW, Marley JE, Beilby JJ. A randomised controlled trial of the outcome of health assessment of
people aged 75 years and over. Med J Aust. 2001:16;175(2):104-7. PMID: 11556409. 9. Eekhof J, De Bock G, Schaapveld K, et al. Effects of screening for disorders among the elderly: an
intervention study in general practice. Fam Pract. 2000:17(4):329-33. PMID: 10934182. 10. Moore AA, Siu A, Partridge JM, et al. A randomized trial of office-based screening for common problems
in older persons. Am J Med. 1997:102(4):371-8. PMID: 9217619. 11. Wagner EH, LaCroix AZ, Grothaus L, et al. Preventing disability and falls in older adults: a population-
based randomized trial. Am J Public Health. 1994:84(11):1800-6. PMID: 7977921. 12. van Rossum E, Frederiks CM, Philipsen H, et al. Effects of preventive home visits to elderly people. BMJ.
1993:307(6895):27-32. PMID: 8343668. 13. Vetter NJ, Lewis PA, Ford D. Can health visitors prevent fractures in elderly people? BMJ.
1992:304(6831):888-90. PMID: 1392755. 14. McEwan RT, Davison N, Forster DP, et al. Screening elderly people in primary care: a randomized
controlled trial. Br J Gen Pract. 1990:40(332):94-7. PMID: 2112022. 15. Vetter NJ, Jones DA, Victor CR. Effect of health visitors working with elderly patients in general practice:
a randomised controlled trial. Br Med J (Clin Res Ed). 1984:288(6414):369-72. PMID: 6229314.