Embed Size (px)
Citation preview
Section 5. Health Care Facility Planning
IntroductionThe capacity to maintain essential health care services during a pandemic will begreatly reduced and rely extensively on triage, self care at home, use of alternate staffand assignment to alternate care facilities. Those individuals admitted to hospitalfacilities will be acutely ill and the health care delivery system will be overwhelmed. Toensure that the existing health care delivery system can respond to a rapid surge intransmission, collaborative planning partnerships both internally and externally arerequirements for each health care provider.
The purpose of this section is to provide overall planning guidance as well as theframework for the management of medical surge needs resulting from an incident thatoverwhelms the capacity of hospitals in Contra Costa and nearby counties in order tomeet the overall goal of minimizing mortality and morbidity. This module is to be usedwhen needed in conjunction with the Contra Costa Health Services Emergency Planand the Contra Costa County Emergency Operations Plan. (See also Sect. 6 InfectionPrevention and Control for more information on home care)
Contra Costa Health Services (CCHS) has a dual role in this plan:1) As the County Health Authority, CCHS Divisions and programs are responsible fordeveloping policies and guidance for health care providers in Contra Costa to ensurethat the local planning process for pandemic flu is comprehensive and in accordancewith State, local, and Federal requirements. CCHS has convened and oversees theprimary pandemic flu workgroups for Contra Costa.2) As a direct health care provider, Contra Costa Regional Medical Center and Clinics(CCRMC) is responsible for following all directives issued by the Health Authority toContra Costa health care providers.
Interpandemic /Pandemic Alert Period (WHO Phases 1-5)The primary Health Facility Planning objectives during the Interpandemic/PandemicAlert period are to:
1. Ensure information exchange in a timely fashion;2. Develop and streamline processes to improve facility response capacity;3. Train staff to respond to a rapidly changing disease process;4. Identify and act on areas needing further discussion and planning;5. Develop local Medical Surge Capacity.
Consistency in planning will extend local capacity to address rapidly changing healthcare needs in the community. Each Hospital should be prepared to identify and providecare to individuals with the influenza virus as part of routine operations and respond to asignificant escalation in demand for services in the event of a pandemic outbreak.
To prepare for pandemic influenza, all health care facilities in Contra Costa shoulddevelop an internal planning team with representation from infection control, materialsmanagement, vaccines and pharmaceuticals, morgue, triage, communications, nutrition,security, personnel, surveillance, and other essential health care components. Thepurpose of this internal team is to develop a functional plan to:
Prepare the facility to respond to pandemic flu; Identify and report pandemic flu progression in Contra Costa County;
Respond to county-wide health care surge needs; Maintain the fullest level of health care services possible during a changing
epidemic; Participate in Countywide workgroup efforts to increase coordination of response
and information exchange.
1. Medical Surge CapacityMedical surge capacity refers to the ability to evaluate and care for a markedlyincreased volume of patients – challenging or exceeding the normal capacity of ahospital or healthcare system. Individual hospitals plan for and routinely handle surgerequirements resulting from seasonal fluctuations in respiratory ailments,environmentally based conditions, and community incidents. In Contra Costa County,as throughout most of California, hospitals routinely operate at or near capacity.Moderately sized incidents with several to, perhaps, hundreds of patients are handled inaccordance with the County’s Multicasualty Incident Plan. Patients are transported tohospitals throughout the county and throughout the region to avoid overloading anysingle hospital. However, very large-scale incidents or widespread disease outbreaksmay overwhelm the capacity of many or all hospitals and other health care providers ina region. Responding to such incidents requires the close coordination and cooperationof hospitals, health centers and community clinics, governmental agencies, and otherhealthcare providers.
The purpose of this section is to provide a framework for the management of medicalsurge needs resulting from an incident that overwhelms the capacity of hospitals inContra Costa and nearby counties in order to meet the overall goal of minimizingmortality and morbidity. This section includes the County’s Emergency Medical ServicesAgency’s Medical Surge Capacity Plan and the response to an infectious diseaseoutbreak.
Emergency Operations and ManagementThe Medical Surge Capacity Plan is a tool to be used when needed in conjunction withthe Contra Costa Health Services Emergency Plan and the Contra Costa CountyEmergency Operations Plan. Contra Costa Health Services will be the lead agencycoordinating medical surge activities. Emergency operations shall be conducted inaccordance with the California Standardized Emergency Management System (SEMS)and the National Incident Management System (NIMS).
Surge Levels
Surge Level 0 – No External Trigger
Surge Level 0 is the normal operating level of the county’s hospitals andincludes expanded operations that hospitals can carry out on their own authorityto meet variations in demand. Under Surge Level 0, hospitals may be on CensusAlert 1 or 2 and may have been granted Staffing Program Flexibility and/orIncreased Patient Accommodation from the State Department of Health Services.Hospitals comply with all DHS requirements.
Surge Level 1 – Local Emergency and Health Officer Directive / NoAlternate Care Sites
Surge Level 1 shall be in effect when, during a duly proclaimed localemergency, a directive is issued by the County Health Officer for hospitals toexpand capacity beyond normally permitted levels. Under Surge Level 1,inpatient services are provided at facilities under hospital control. Clinics may beenlisted to provide triage, dispensing of antibiotics or other pharmaceuticals, andoutpatient treatment of patients not requiring hospitalization.
(a) The trigger for consideration of a Surge Level 1 directive shall be adetermination by the County EMS Agency that most or all hospitals inContra Costa and adjacent counties are at or near peak capacity and thatthere is a high probability that the number of patients requiring hospitaltreatment will increase.
(b) Prior to issuing a Surge Level 1 directive, the Health Officer shall confer withthe County Emergency Services Director, hospital representatives, and theState Health Officer or his representative.
(c) While a Surge Level 1 directive is in place, the County Health ServicesDepartmental Operating Center (DOC) shall be activated.
(d) While a Surge Level 1 directive is in place, hospitals shall only depart fromexisting patient capacity, staffing ratio, and other patient care standards asspecifically authorized by the Health Officer as necessary to protect thepublic health and safety. All departures from existing standards shall berecorded by the hospital and reported as soon as practical to the DOC.
(e) Hospitals shall seek to maintain or return to normal standards as conditionspermit.
Pandemic Period (WHO Phase 6)The Planning objective during this phase is:
1. Ensure supportive care for those who cannot access hospital care.
Surge Level 2 – Local Emergency and Health Officer Directive / AlternateCare Site(s)
Surge Level 2 shall be in effect when, during a duly proclaimed localemergency, a directive is issued by the County Health Officer for theestablishment of one or more Alternate Care Sites to provide supportive andother care for persons for whom hospitalization is not available due to lack ofhospital capacity under Surge Level 1 conditions. Under Surge Level 2, alldirectives and requirements set forth above under Surge Level 1 remain in effect.In addition, County Health Services shall establish one or more Alternate CareSites at facilities designated by the Health Officer. (See Alternate Care Sitessection below)
(a) The trigger for consideration of a Surge Level 2 directive shall be a findingby the Health Services DOC Director that the number of persons requiringinpatient care exceeds the capabilities of hospitals in the county operatingunder Surge Level 1.
(b) Prior to issuing a Surge Level 2 directive, the Health Officer shall confer withthe County Emergency Services Director, hospital representatives, and theState Health Officer or his representative.
(c) Upon issuance of a Surge Level 2 directive, the Health Services DOCDirector shall establish under the Operations Section, an Alternate Care SiteBranch. The Alternate Care Site Branch Director shall be responsible forsecuring and opening Alternate Care Site facilities, securing medical andancillary staff, securing logistical support including security, establishingoperating guidelines and patient care standards, and appointing a MedicalDirector and Site Administrator for each Alternate Care Site.
(d) Each Alternate Care Site shall implement a system for patient triage, patientadmission, patient care, medical record keeping, patient discharge ortransfer, and personnel record keeping.
(e) The Health Officer shall appoint one or more persons as an Ethics Advisoror Ethics Advisory Committee to advise the Health Officer on criteria fordirection of patients to Alternate Care Sites. The Ethics Advisor or chair ofthe Ethics Advisory Committee shall be a physician with training in medicalethics.
(f) The Health Officer shall appoint an Alternate Care Site Inspector withappropriate staff to regularly inspect and report to the Health Officer on thestatus of each Alternate Care Site with respect to sanitation, medical, andother conditions.
(g) The Health Services DOC Director shall endeavor to close Alternate CareSites as soon as practical upon determination that inpatient care can behandled at hospital facilities.
Planning Scenarios
The need for surge capacity may arise from a number of different scenarios rangingfrom a great earthquake to a highly toxic and widespread chemical release to pandemicinfluenza or other acutely infectious disease outbreak. The circumstances of such anincident may be natural or manmade, accidental or deliberate, time limited or continuingover an extensive period, localized in one county or region or spread over the state ornation. Each scenario presents its own set of considerations and constraints that willimpinge on how surge capacity is handled. Key variables affecting surge capacityinclude:
(1) Number of patients
(2) Acuity of patients
Decontamination required?
Treat and release or hospital admission?
Specialized or complex surgical or medical treatment needed?
Ventilator needed?
Isolation required?
(3) Duration of incident
(4) Geographic scope
Are other areas impacted so that outside assistance is not available?
(5) Impact of incident on medical personnel and facilities
Earthquake damage to hospitals?
Hospital staff impacted by illness?
While each event will present its own unique set of challenges, for planningpurposes four general scenarios have been considered.
Scenario #1 – Acute Infectious Disease
This scenario includes pandemic influenza, novel diseases such as severeacute respiratory syndrome (SARS), and infectious diseases thought to bepotentially associated with bioterrorism such as smallpox. The scenario presentsspecial challenges related to potential long duration, widespread impact, impacton health care workers, and impact on supply lines and community infrastructure.Additionally, there may be need for isolation and other protective measures.Large numbers of patients may be ventilator dependent.
Scenario #2 – Acute Botulinum or other Acute Chemical Poisoning
This scenario includes major industrial accidents (refineries, chemicalplants, tank cars), industrial sabotage, or terrorist attack. While relativelylocalized and time limited when compared to pandemic influenza, this scenariohas the potential of affecting a population over many square miles and may resultin patients seeking medical treatment over days or weeks. In 1993, an Oleum(sulfuric acid) railroad tank car release in Contra Costa County sent 22,000persons to local hospitals and clinics seeking treatment over a 10-day period.While very few persons required emergency treatment or hospitalization, thesheer volume of patients severely impacted hospital resources and required theestablishment of an alternate (non-hospital) to provide patient screening andtriage over a period of several days. Under Scenario #2, there may be need forlarge amounts of nerve agent antidotes or anti-toxin not normally available inquantity at local hospitals. There may also be a demand for ventilators.
Scenario #3 – Trauma and Burn Care
Scenario #3 includes major earthquake and large-scale attack byexplosive or incendiary device. This scenario is much more time limited and isapt to be more geographically focused. A great earthquake on the Haywardfault, however, is likely to cause widespread death and destruction throughoutthe East Bay and is likely to cripple hospitals located along the fault.
Scenario #4 – Radiation Induced Injury
This scenario includes spread of radioactive material over a largepopulation by “dirty bomb” or other means, as well as attack by nuclearexplosion. Depending on the device or material used, medical issues range fromminor to catastrophic. Psychological effects may be profound. Staff availabilitymay be impacted due to illness or safety concerns.
Resources for Medical Surge
1. Facilities
(a) Acute care hospitals
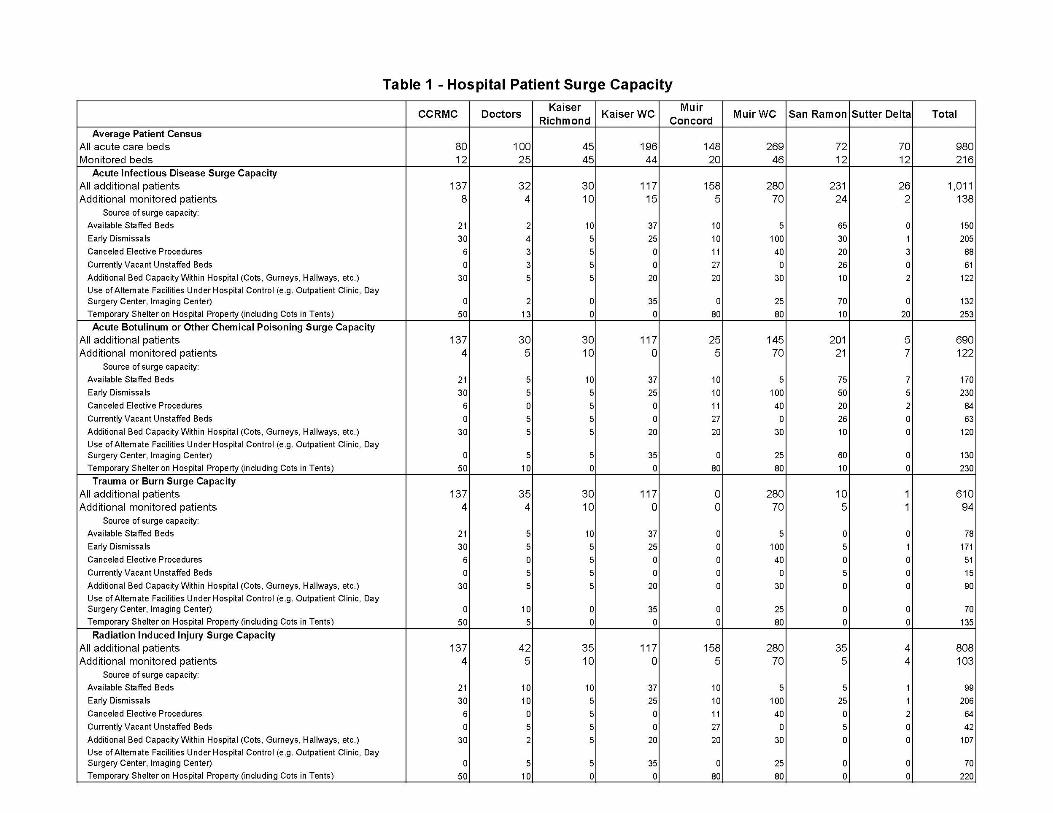
Table 1 shows the surge capacities reported by each of the county’seight acute care hospitals under each of the four planning scenarios. Surgecapacity is reported as the number of additional patients (all patients andmonitored patients) that could be handled by the hospital over and above theaverage daily census under "altered standards of care.”
“Altered standards of care” is defined by the federal Health & Human ServicesAgency for Healthcare Research and Quality:
Under normal standards of care, a provider must use the degree of skill anddiligence in the diagnosis, treatment and overall management of each patientthat a reasonable prudent provider in the same field of practice in Californiawould have used under the circumstances of the case. Altered standards ofcare represent a shift, during a mass casualty event that compromises theability of local or regional health systems to deliver services consistent withestablished standards of care, to providing care and allocation scarceequipment, supplies, and personnel in a way that saves the largest number oflives.
The numbers are reflective of physical capacity without regard to staffing.The table also shows for each hospital the sources of the reported surgecapacity; e.g., available staffed beds, early discharges, surge tents, etc.While surge capacity is reported without regard to staffing capability, a largeproportion of the surge capacity reported by each facility (varies by scenario)is from staffed vacant beds, early discharges, and cancelled electiveprocedures. Thus, a certain amount of surge can be accomplished withoutcompromising staffing levels.
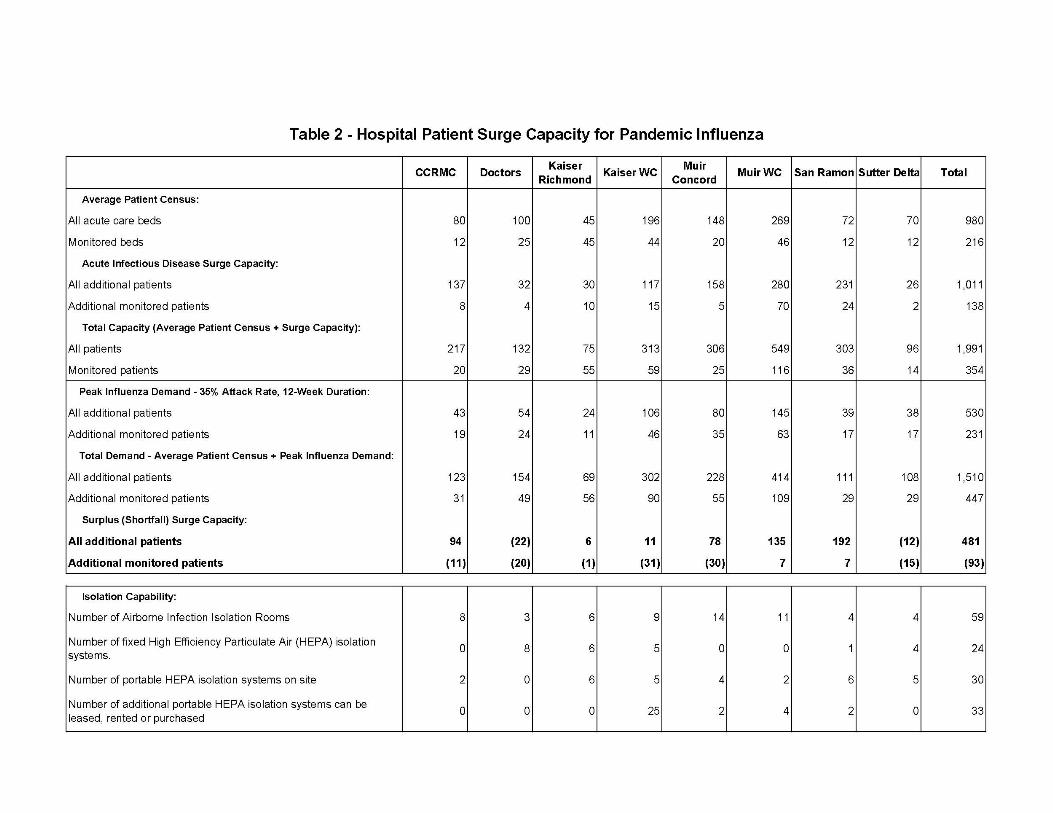
Surge capacity to handle a major influenza epidemic is shown in Table2. These figures utilize the reported surge capacities for an acute infectiousdisease scenario and the estimated increased hospital bed demandcalculated using the Centers for Disease Control and Prevention FluSurge 2.0software. Demand assumptions are for the peak week of a 12-week duration,35 percent infection rate event. Overall, Contra Costa would have sufficienthospital beds to provide medical surge for the projected 530 additionalpatients, but would be short almost one hundred monitored beds.
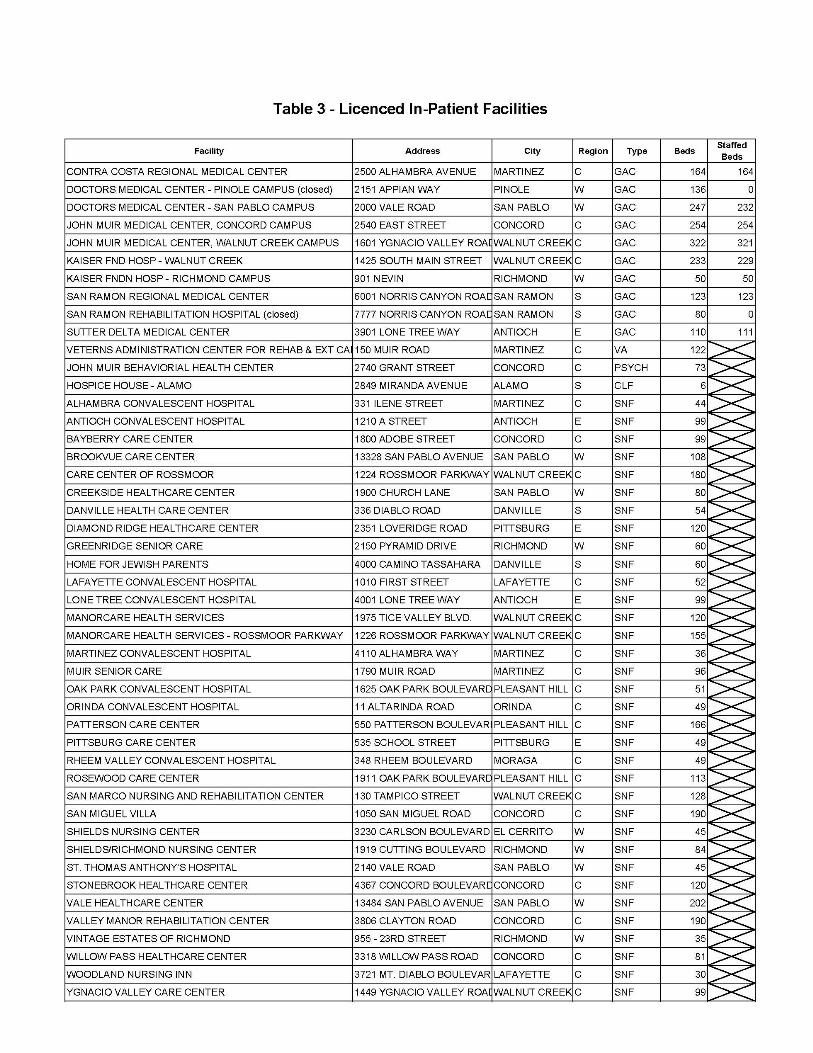
(b) Other in-patient facilities
Skilled nursing and other non-acute-care in-patient facilities represent asecondary source of surge capacity. Table 3 provides a listing of all licensedin-patient facilities in the county (including the Veterans AdministrationMartinez Rehabilitation and Long Term Care facility, which is not licensed bythe State). Not including acute care hospitals, these inpatient facilitiesaccount for a total of 3,525 beds. Assuming these facilities collectively couldhandle a surge of ten percent of licensed capacity, they could absorb some350 additional patients. Primary use for this additional capacity wouldprobably be for lower acuity patients discharged from acute care hospitals.
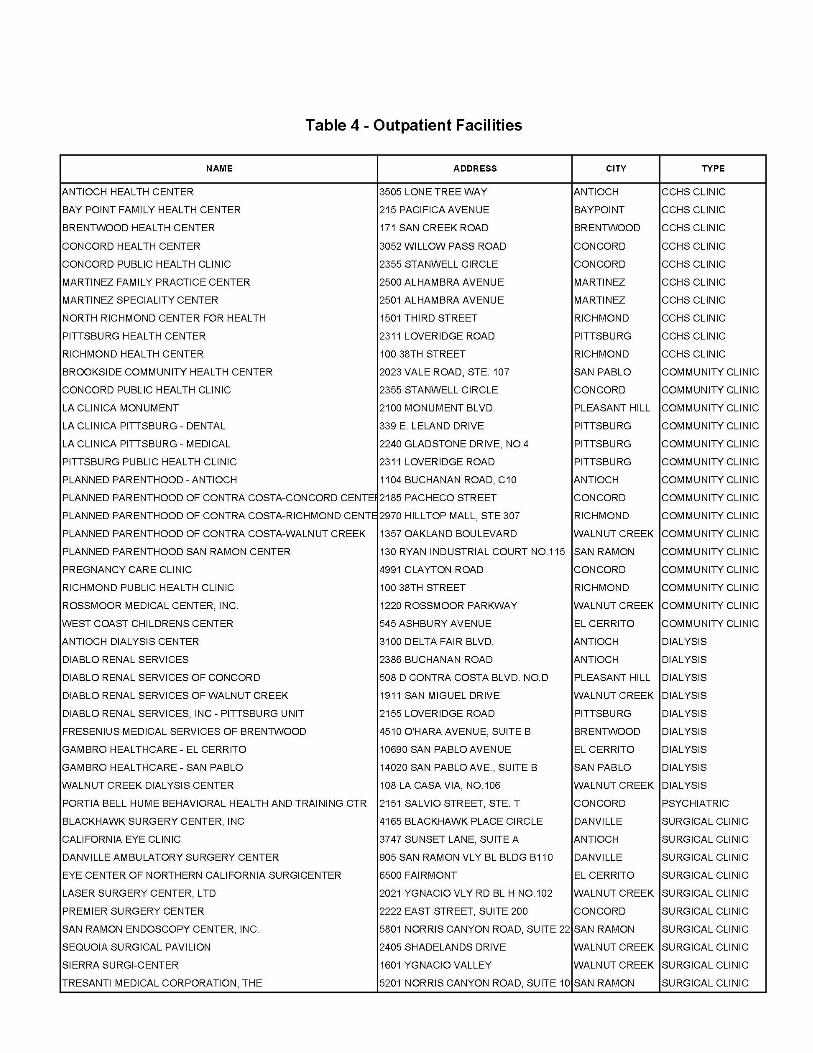
(c) Outpatient facilities
Table 4 lists Contra Costa Health Services health centers and otherlicensed outpatient facilities including community clinics, dialysis clinics,private psychiatric clinics, and surgi-centers. CCHS and community clinicscan provide important resources for dispensing, triage, and outpatient care todivert patients away from hospital emergency departments when hospital
care is not required. All community clinics are represented by the CommunityClinic Consortium of Contra Costa County. Through the Consortium,community clinics have developed disaster plans, have acquired disaster andpersonal protective equipment and supplies, and have participated withContra Costa Health Services in disaster exercises.
(d) Closed hospitals
The three closed hospitals – Los Medanos, VA Martinez, and DoctorsPinole – are accounted for under outpatient facilities.
(e) Alternate Care Sites
Schools, hotels, or other facilities may be designated as Alternate CareSites during a disaster or other large-scale emergency. The level of care will beprimarily supportive care. Alternate Care Sites will be operated under theauspices of Contra Costa Health Services with logistical support provided by theAmerican Red Cross. (See Alternate Care Sites below)
2. Personnel
Hospitals in Contra Costa and throughout most of the state operate at ornear the minimum nurse staffing level required for the number of patients in thefacility. While the number of personnel may be increased significantly on a short-term basis to handle certain surge situations, it is clear that, under any long-termscenario involving infectious disease or other conditions that may incapacitatehospital staff or present significant hazards to hospital staff, care may have to beprovided under “altered standards of care” conditions that depart significantlyfrom existing staffing ratios.
(a) Hospital and skilled nursing facility personnel can be effectively increased by50 percent through implementation of extended shifts. Accommodation willneed to be made for staff childcare.
(b) Contra Costa Health Services nursing personnel not normally assigned tohospital or health center operations may be reassigned to provide patientcare at hospitals, health centers, clinics, or Alternate Care Sites.
(c) Field paramedics and EMT’s may be enlisted to assist in patient care atAlternate Care Sites.
(d) Volunteer nurses and physicians may be recruited from the community asneeded.
3. Equipment and supplies
Contra Costa’s hospitals and clinics have obtained a wide variety of disasterequipment and supplies under the federal Health Resources and ServicesAdministration (HRSA) grants. Major categories of disaster equipment andsupplies that impact surge capacity are as follows: (Some items may have beenordered, but not yet delivered.)
(a) Decontamination units – all hospitals are equipped with decontamination unitsand related equipment and supplies.
(b) Surge shelters – all hospitals are equipped with two surge shelter tents andrelated equipment and supplies (cots, lighting, generators, heaters, etc.) tohandle up to 18 non-ambulatory patients per tent.
(c) Trauma and burn cache – John Muir Trauma Center has been equipped withan augmented trauma and burn cache designed to handle 50 traumapatients.
(d) Pharmaceuticals – All hospitals have stockpiled (or are in the process ofobtaining a stockpile) of two pharmaceutical caches and additionalDoxycycline capsules for prophylaxis of healthcare workers and familymembers. Additionally, CCRMC has stockpiled Doxycycline for prophylaxisof all first responders and family members. The County has a plan in placefor implementation of the Strategic National Stockpile.
(e) Ventilators – Hospitals report a total inventory of 123 full-scale ventilators andan average daily usage of 65, leaving an average availability of 58 full-scaleventilators to meet surge needs. Hospitals report that an additional 72 full-scale ventilators can be obtained from affiliated facilities or leased fromvendors, bring the total number of full-scale ventilators available for surge toabout 130. HRSA Year 4 funding is being used to purchase 320 disposableventilators to be stockpiled (40-each) at the county’s eight acute carehospitals.
(f) ChemPacks – Four CDC hospital ChemPacks are planned (2-each at the VAMartinez facility and at the San Ramon Regional Medical Center) containingchemical and nerve-agent antidotes to treat 1,000 persons each, or a total of4,000 persons.
(g) Protective supplies and equipment – All hospitals have obtained protectiveequipment and supplies including powered air purifying respirators (PAPR’s),protective clothing, HEPA filters, and supplies of N95 masks. Except for thePAPR’s, community clinics have obtained similar protective equipment andsupplies for disaster response.
(h) Communications and infrastructure – All hospitals and community clinics haveobtained portable satellite telephones for backup communications in the eventof a disaster. Community clinics have upgraded computer networks, installedemergency power, and obtained outside lighting to enhance operationalcapabilities.
4. Resource Tracking
Contra Costa has established a web-based Asset Logistics andResources Management System (ALARMS) developed by Ecology andEnvironment, Inc. to inventory disaster medical supplies and equipment at eachfacility and to track usage during an actual disaster. Each facility has access toreview all inventoried equipment and supplies and, when completed, will haveaccess to update its own inventory.
Alternate Care Site Planning
An Alternate Care Site as defined in Contra Costa County is a specialized County-operated emergency shelter where, under certain defined emergency conditions, sick orinjured persons may be provided temporary shelter and limited medical care for one toseveral days until discharged from care or until more appropriate care becomesavailable.
An Alternate Care Site is operated jointly by the Contra Costa County Employment andHuman Services Department, which is responsible for administration of the AlternateCare Site, and Contra Costa Health Services, which is responsible for medical care.Both County departments work in partnership with the county Office of EmergencyServices (OES) and the American Red Cross*, which will provide non-medical logisticalsupport including cots, bedding, food, and other supplies normally used in establishingand operating a shelter facility. *(Planning agreements are still being discussed with theAmerican Red Cross regarding ACSs) but tentative response roles are as follows.
America Red Cross role and response during a pandemicDuring a flu pandemic event, the Red Cross will:
Provide for feeding and bulk distribution for isolated and quarantined individuals,either directly or by convening and collaborating with others who are willing toprovide these services;
Continue to respond to disasters of all sizes; Participate in community education; and Ensure a safe and adequate blood supply.
Special Needs Shelters and Alternate Care SitesWhile the Red Cross does not operate special or medical needs shelters nor do theydeliver direct medical care, the Red Cross does anticipate receiving requests to providesignificant support to these types of facilities. This support could be in the form ofmaterial support (i.e. food, supplies) and/or human resources support (supplementalstaff or shelter management).
The Red Cross is not able to commit Red Cross workers to local public health overflowfacilities without appropriate worker protections, including liability coverage and workersafety measures. The Red Cross continues to explore the legal, risk and workerprotection considerations for a possible Red Cross support role in these facilities. Theseefforts include seeking federal assistance for a variety of protections for workers, as wellas similar assistance at the state level.
Vulnerable Populations ConsiderationsThe following issues will be taken into consideration in activating alternate care sites toserve people with special needs.
1. Consider prioritizing hospitalization versus assignment to Alternate Care Sites forsome individuals who may have extensive existing medical needs. Consideradmissions criteria to Alternate Care Site, skilled nursing facilities, licensed carefacilities or staying at home with attendants depending upon levels of careneeded.
2. Consider the assistive care needs of vulnerable populations at Alternate CareSites.
a. The assistive care needs of vulnerable populations including, but notlimited to, persons with impaired mobility, medically dependent/fragile,severe chronic disease, or developmental disabilities must be taken intoaccount at the time of the triage decision. Based upon need, someAlternate Care Sites may be designated for particular target populations.
b. Alternate Care Sites designated for vulnerable populations groups requirestaffing (for example, medical health professionals for a site catering topersons with severe chronic disease), equipment (for example, hydraulic
lifts for persons unable to assist with transfers) and other considerations(for example, wide aisles to enable wheelchair access).
c. The Alternate Care Site will provide medications or Personal ProtectiveEquipment (PPE) to caregivers or family members that accompany theperson with special needs.
3. Ensure multilingual staff capacity at Alternate Care Sites.4. Consider optimal location of care for patients who are incarcerated, registered
sex offenders, etc.
Activating Alternate Care SitesThe decision to initiate Alternate Care Site operations shall be made by the CountyHealth Officer primarily when, in accordance with the County Medical Surge Plan,hospitals and other health care facilities have implemented their own surge plans andremain overwhelmed. Under such circumstances, certain categories of patients may beadvised to receive care at home as appropriate hospital resources are simply notavailable. Persons whose condition falls within the criteria for home care, but who donot have necessary support available for home care, may be cared for at an AlternateCare Site. The Alternate Care Site is a transitional holding facility caring for patientsover a period of days to weeks until able to care for themselves, released to anappropriate caregiver, transferred to a skilled nursing facility or acute care hospital, ordiseased. An Alternate Care Site would not normally accept transfers from licensedhealth care facilities.
While primarily envisioned as a facility to be activated if needed during severe pandemicinfluenza, the Alternate Care Site could be used under any scenario in which there wasa need for the County to provide shelter and low acuity or palliative patient care. Undermost circumstances, however, it should be assumed that care can be better providedusing existing facilities even when those facilities must be operated beyond normalcapacity.
The Alternate Care Site Operations Manual has been adapted from the U.S. ArmyConcept or Operations for the Acute Care Center manual developed under theBiological Weapons Improved Response Program. The Concept of Operations for theAcute Care Center was written to assist planners, administrators, responders, medicalprofessionals, public health, and emergency management personnel in better preparingfor and providing mass casualty care. The concept of operations describes the specificcommand organization, operational execution, and the logistical and staffingrequirements associated with the Acute Care Center as envisioned in the U.S. Armydocument.
While the U.S. Army document uses the term “Acute Care Center,” the mission orpurpose of the Alternate Care Site as planned for Contra Costa County more closelyreflects that of the Alternate Care Site as described in the federal Health and HumanServices community planning guide on Mass Medical Care with Scare Resources1 thanan acute care hospital.
Major issues to be considered include:
• Physical plant: location, size, characteristics, and security needs
1 Phillips SJ, Knebel A, eds. Mass Medical Care with Scarce Resources: A Community Planning Guide. Preparedby Health Systems Research, Inc., an Altarum company, under contract No. 290-04-0010. AHRQ Publication No.07-001. Rockville, MD: United States Health and Human Services Agency for Healthcare Research and Quality2007.
• Staffing: personnel needs, volunteers, credentialing
• Level and scope of care: disaster care vs. non-disaster care, agent-specific carevs. generic care, changing standard of care in mass casualty environmentsCommand, control, and communication: Incident Command System, fail-safecommunications
• Integration with federal and state response: framework of local responsecompatible with outside resources.
(Please see Appendix XXX for Development of Standards and Guidelines forHealthcare Surge during Emergencies - Alternate Care Sites; Administrative;Declarations and Triggers; Existing Facilities)
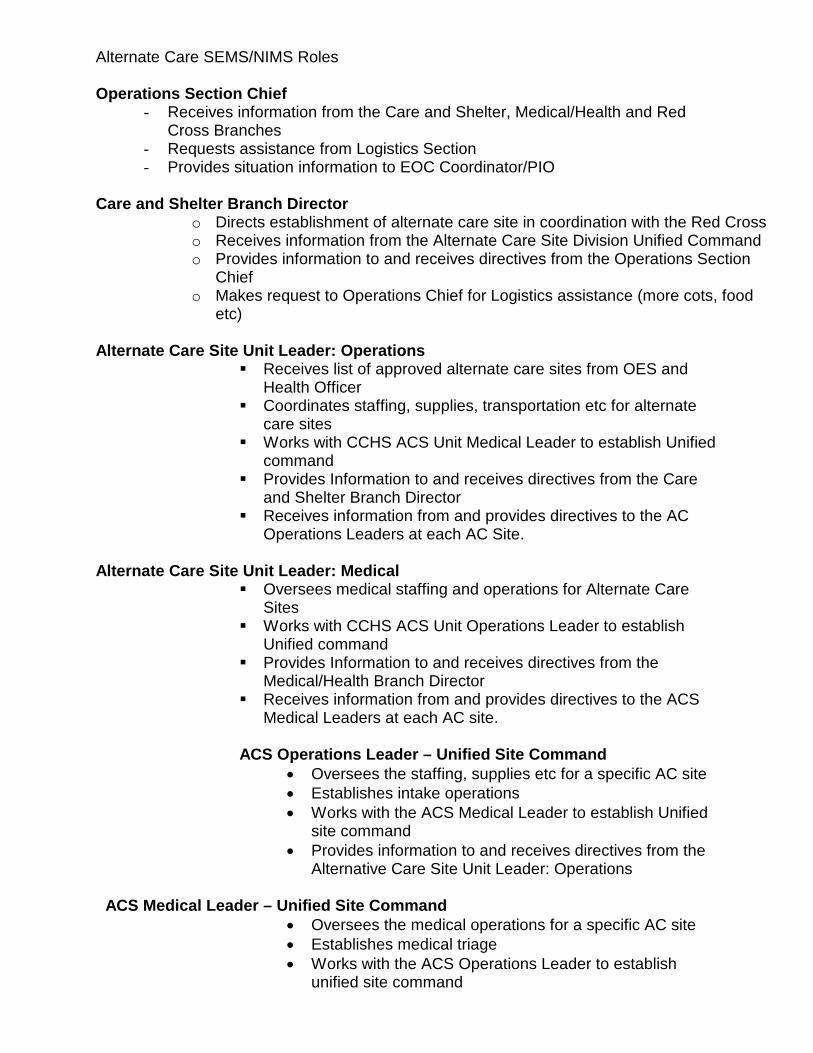
Alternate Care SEMS/NIMS Roles
Operations Section Chief- Receives information from the Care and Shelter, Medical/Health and Red
Cross Branches- Requests assistance from Logistics Section- Provides situation information to EOC Coordinator/PIO
Care and Shelter Branch Directoro Directs establishment of alternate care site in coordination with the Red Crosso Receives information from the Alternate Care Site Division Unified Commando Provides information to and receives directives from the Operations Section
Chiefo Makes request to Operations Chief for Logistics assistance (more cots, food
etc)
Alternate Care Site Unit Leader: OperationsReceives list of approved alternate care sites from OES and
Health OfficerCoordinates staffing, supplies, transportation etc for alternate
care sitesWorks with CCHS ACS Unit Medical Leader to establish Unified
commandProvides Information to and receives directives from the Care
and Shelter Branch DirectorReceives information from and provides directives to the AC
Operations Leaders at each AC Site.
Alternate Care Site Unit Leader: MedicalOversees medical staffing and operations for Alternate Care
SitesWorks with CCHS ACS Unit Operations Leader to establish
Unified commandProvides Information to and receives directives from the
Medical/Health Branch DirectorReceives information from and provides directives to the ACS
Medical Leaders at each AC site.
ACS Operations Leader – Unified Site Command Oversees the staffing, supplies etc for a specific AC site Establishes intake operations Works with the ACS Medical Leader to establish Unified
site command Provides information to and receives directives from the
Alternative Care Site Unit Leader: Operations
ACS Medical Leader – Unified Site Command Oversees the medical operations for a specific AC site Establishes medical triage Works with the ACS Operations Leader to establish
unified site command
Provides information to and receives directives from theAlternative Care Site Unit Leader: Medical
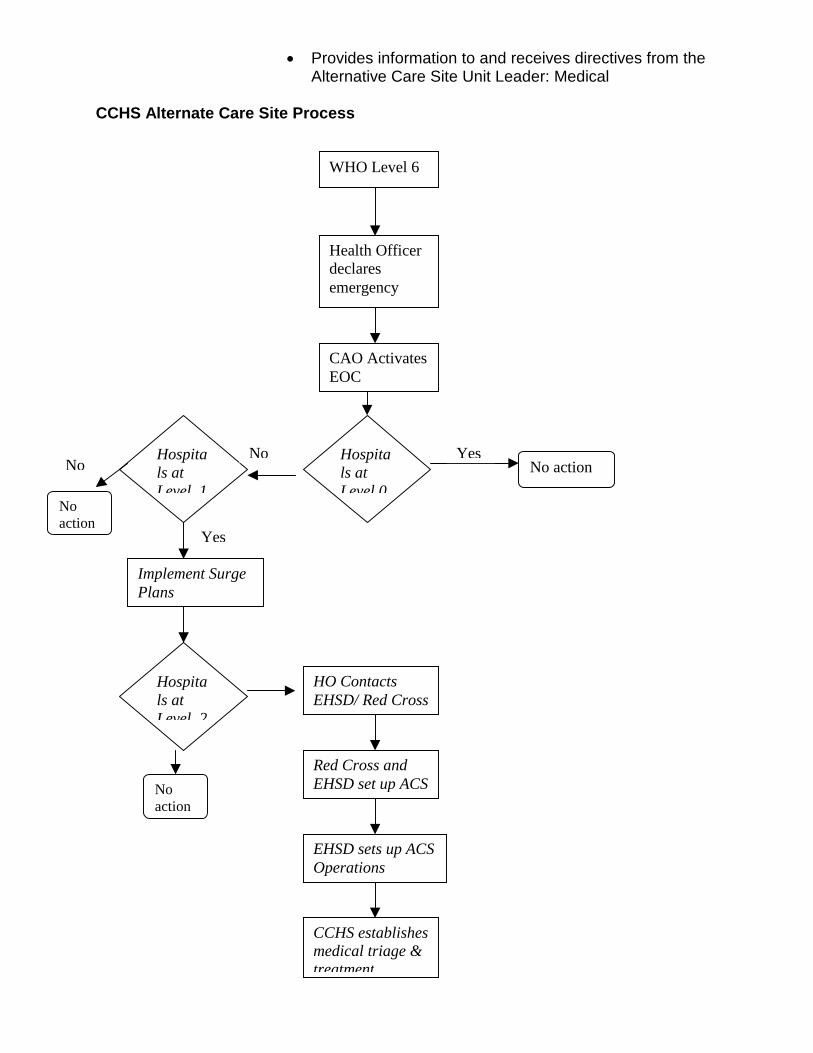
CCHS Alternate Care Site Process
WHO Level 6
Health Officerdeclaresemergency
CAO ActivatesEOC
Hospitals atLevel 0
No action
Implement SurgePlans
YesHospitals atLevel 1
No
Hospitals atLevel 2
HO ContactsEHSD/ Red Cross
Red Cross andEHSD set up ACS
EHSD sets up ACSOperations
CCHS establishesmedical triage &treatment
Yes
No
Noaction
Noaction