Embed Size (px)
Citation preview
This article was downloaded by: [Western Kentucky University]On: 29 October 2014, At: 02:27Publisher: RoutledgeInforma Ltd Registered in England and Wales Registered Number: 1072954Registered office: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK
Residential Treatment for Children &YouthPublication details, including instructions for authors andsubscription information:http://www.tandfonline.com/loi/wrtc20
Self, Peer, and Staff RatingsHenry F. Kaplan PhD a & James D. Kloss PhD ba Mendota Mental Health Institute, Madison, WI, 53704b Executive Director, Mississippi River Human Services Center,IncPublished online: 26 Oct 2008.
To cite this article: Henry F. Kaplan PhD & James D. Kloss PhD (1988) Self, Peer, and StaffRatings, Residential Treatment for Children & Youth, 6:1, 27-41, DOI: 10.1300/J007v06n01_04
To link to this article: http://dx.doi.org/10.1300/J007v06n01_04
PLEASE SCROLL DOWN FOR ARTICLE
Taylor & Francis makes every effort to ensure the accuracy of all the information (the“Content”) contained in the publications on our platform. However, Taylor & Francis,our agents, and our licensors make no representations or warranties whatsoeveras to the accuracy, completeness, or suitability for any purpose of the Content. Anyopinions and views expressed in this publication are the opinions and views of theauthors, and are not the views of or endorsed by Taylor & Francis. The accuracyof the Content should not be relied upon and should be independently verifiedwith primary sources of information. Taylor and Francis shall not be liable for anylosses, actions, claims, proceedings, demands, costs, expenses, damages, and otherliabilities whatsoever or howsoever caused arising directly or indirectly in connectionwith, in relation to or arising out of the use of the Content.
This article may be used for research, teaching, and private study purposes. Anysubstantial or systematic reproduction, redistribution, reselling, loan, sub-licensing,systematic supply, or distribution in any form to anyone is expressly forbidden. Terms
& Conditions of access and use can be found at http://www.tandfonline.com/page/terms-and-conditions
Dow
nloa
ded
by [
Wes
tern
Ken
tuck
y U
nive
rsity
] at
02:
27 2
9 O
ctob
er 2
014
Self, Peer, and Staff Ratings Henry F. Kaplan, PhD James D. Kloss, PhD
ABSTRACT. The authors' experience using a 20-item sociometric scale with groups of 9 to 13 inpatient behaviorally disturbed preado- lescents is described. Evidence of validity of the method is dernon- strated via agreement with staff assessments, and application of the method for monitoring residents' progress is presented. Inasmuch as the technique provides for self-naming as well as the nomination of others, the second section deals with 11s application as a self-assess- ment tool with a built-in accuracy measure (discrepancy from pooled peers' evaluations). A parallel measure of accuracy regarding others was also developed. Positive correlations were found between sev- eral accuracy measures and level of functioning.
Psychological assessment using sociometric approaches has come to be increasingly useful for clinical purposes. The earlier Like-Dislike or Popular-Unpopular dichotomy has given way to the consideration of a variety of subgroups that are identifiable by these methods (Walder, Abelson, Eron, Banta, & Laulicht, 1961; Wig- gins & Winder, 1961). Differentiation between rejected and ne- glected (Cantrell & Prinz, 1985; Dodge, Coie, & Brakke, 1982), and between aggressive and aggressivelwithdrawn children (Millich & Landau, 1983) are examples of such refinement in focus.
Much of the research deals with children in normal classrooms. The two studies described here were carried out with disturbed chil- dren in a residential setting. They deal with establishing the validity of the interpersonal perceptions within their group and with the use of sociometric data to investigate individuals' self-perceptions.
Henry F. Kaplan may be written at the Mendota Mental Health Institute, 301 Troy Drive, Madison, WI 53704.
Residential Treatment for Children & Youth, Vol. 6(1) 1988 O 1988 by The Haworth Press, Inc. All rights resewed. 27
Dow
nloa
ded
by [
Wes
tern
Ken
tuck
y U
nive
rsity
] at
02:
27 2
9 O
ctob
er 2
014
Pekarik, Prinz, LieberP, Weintraub and Neale (1976) designed a 35-item scale for classroom-based assessment, the Pupil Evaluation Inventory. This instrument taps a broad span of behaviors relevant Po a wide age range of children of both sexes. The authors found three homogeneous factors: aggression, withdrawal, and likability. They discovered impressive inter-rater agreement between teachers and peers for the three factors. SeUf-peer conenations were Bower than teacher-peer correlations, consistent with previous research findings (Eron, Walder B Lefkowitz, 11971; Himelstein & Lubin, 1965). The inference drawn is that there is some degree of distor- tion or inaccuracy by individuals in assessing themselves, and a response set Po endorse socially desirable items has been proposed as an explanation. Self-concept studies have anso described the phe- nomenon of distortion in self-appraisal or self-presentation (Wylie, 19791, and social desirability is usually given as an explanation for this type of inaccuracy since the distortion is usually of a self-en- hancing nature.
Ledingham, Younger, Schwartaman and Bergerow (1982), using a French translation of the Pupil Evaluation Inventory, also found inter-rater agreement between peer and teacher ratings to be greater than between self-ratings and both peer and teacher ratings. Fur- ther, they explored the purported social desirability factor in self- ratings, finding self-ratings of "'8ikability" to be significantly higher thaw peer ratings within groups identified as being extremely aggressive, withdrawn or aggressive-withdrawn. Furthermore, self- ratings provided lower estimates of deviant behavior thaw did peer or teacher ratings for these extreme groups. Similar explorations using sociometric assessment with a markedny disturbed group have not yet been reported.
The grouped data reported in most studies might lead one to con- clude that such self-aggrandizing inaccuracy is a pervasive phenom- enon. But, even assuming that such enhancement is indeed normal one might ask, what are its desirable h i t s ? Where does healthy self-esteem end and denian and grandiosity begin? Then there are questions about the roots of inaccuracy. How much is conscious rnanipunation of self-image; how much is poor perspective-taking, i.e., honest but inaccurate by external standards? And, under what conditions does a child feel free to disclose negative information?
Dow
nloa
ded
by [
Wes
tern
Ken
tuck
y U
nive
rsity
] at
02:
27 2
9 O
ctob
er 2
014
Henry F. Kaplan and James D. Kloss 29
Finally, how pewasive, in fact, is the phenomenon of accentuating the positive and eliminating the negative?
Considering the importance imputed to self-concept in clinical work with children, it is noteworthy that existing standardized self- esteem measures for children do not consider these kinds of distor- tion. This paper describes a sociometric approach which includes the opportunity for nominating oneself and can be thought of as a type of self-concept measure that assesses those distortions.
The investigation described here is presented in two sections. The first parallels the works of Pekarik et al. (1976), and of Leding- ham et al. (1982), but the subjects in this section were severely behaviorally disordered children in residential treatment. The basic question was whether these children at one extreme of the behavior continuum and reflecting a limited range of behaviors can agree regarding characteristics of their peers, and to what extent do self- appraisals agree with the appraisals by peers and adults. Further, is there agreement between peers and staff members in their assess- ments of these children?
The second section deals with an approach to measuring "accu- racy" and bias of individuals' assessments of themselves and of others in their living group. The instrument for study used in both sections employed a 20-question sociometric format. This, then, was an exploration of the use of a sociometric approach to obtain clinically relevant information about disturbed children's self-con- cepts and their assessments of others. The relationship between ac- curacy and other variables will be reported here in a preliminary validation effort.
SECTION I
Method
The 20-question method grew out of the use of routine sociome- tric evaluations at the Children's Treatment Unit (CTU), a residen- tial center for behaviorally disturbed children. CTU is part of a large state-operated psychiatric facility. Like and dislike status were investigated at 2-112 to 4 month intervals. An inquiry followed the questions pertaining to like and dislike choices. Each child was
Dow
nloa
ded
by [
Wes
tern
Ken
tuck
y U
nive
rsity
] at
02:
27 2
9 O
ctob
er 2
014
30 RESIDENTIAL TREATMENT FOR CHILDREN & YOUTH
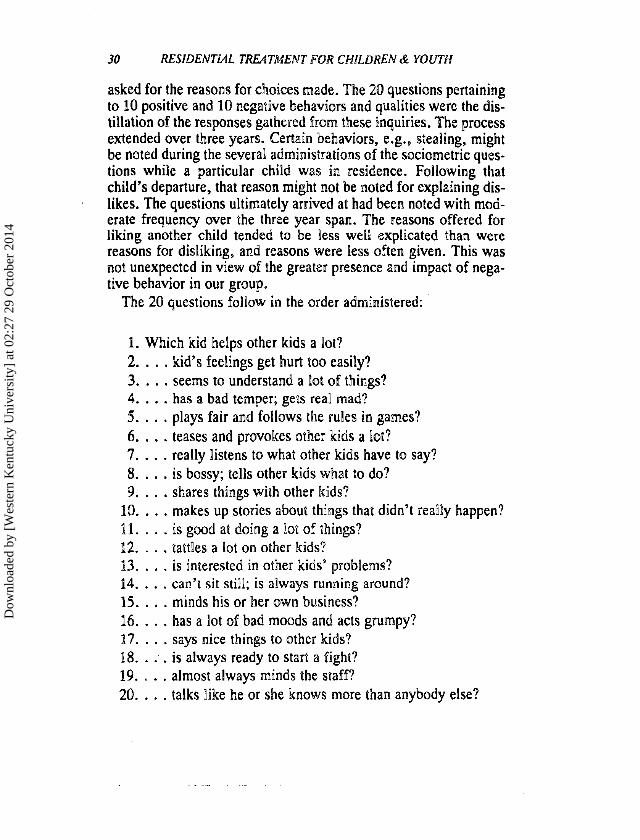
asked for the reasons for choices made. The 20 questions pertaining to 10 positive and 10 negative behaviors and qualities were the dis- tillation of the responses gathered from these inquiries. The process extended over three years. Certain behaviors, e.g., stealing, might be noted during the several administrations of the sociometric ques- tions while a particular child was in residence. Following that child's departure, that reason might not be noted for explaining dis- likes. The questions ultimately arrived at had been noted with mod- erate frequency over the three year span. The reasons offered for liking another child tended to be less well explicated than were reasons for disliking, and reasons were less often given. This was not unexpected in view of the greater presence and impact of nega- tive behavior in our group.
The 20 questions folPow in the order administered:
1. Which kid helps other kids a ha? 2. . . . kid's feelings get hurt too easily? 3. . . . seems to understand a lot of things? 4. . . . has a bad temper; gets real mad? 5. . . . plays fair and follows the rules in games? 6 . . . . teases and provokes other kids a lot? 7. . . . really Pistens to what other kids have to say? 8. . . . is bossy; tells other kids what to do? 9. . . . shares things with other kids?
10. . . . makes up stories about things that didn't really happen? Id. . . . is good at doing a lot of things? 12. . . . tattles a lot on other kids? 63. . . . is interested in other kids9 probPems? 14. . . . can't sit still; is always running around? 15. . . . minds his or her own business? 66. . . . has a lot of bad moods and acts grumpy? 17. . . . says nice things to other kids? 18. . . . is always ready to start a fight? 89. . . . almost always minds the staff? 20. . . . talks like he or she knows more than anybody else?
Dow
nloa
ded
by [
Wes
tern
Ken
tuck
y U
nive
rsity
] at
02:
27 2
9 O
ctob
er 2
014
Henry F. Kaplan and James D. Kloss
Procedure for Use of 20 Questions
Each child in residence was seen privately and was asked to name those children, including oneself, who displayed the behavior or quality noted in the question. For example, "Which kid(s) helps other kids a lot?" The subject was given a list of the children in residence that could be consulted while responding. The format was one of free choice; respondents could name any number of peers and/or themselves. Generally less than 10 minutes were needed to collect information from each child. The subjects were assured of the confidentiality of their responses. The data reported in'this sec- tion were collected in the five administrations during which nursing staff members also responded using the procedure. The population on the living unit varied from 9 to 13 over the five administrations. The five administrations covered a time span of 33 months. All children were interviewed within a period of three days for each administration. All children had been in residence at least two weeks.
The nurses and psychiatric aides responding to the same ques- tionnaire had daily responsibility for the care of the children. The number of staff members responding varied from 8 to 12.
Subjects
There were 39 children ages 6 through 13 included in the five administrations, 35 boys and 4 girls. Although three children were in residence for three administrations, nine for two administrations and 27 for a single administration, only data from the first adminis- trations are included in these analyses.
All the children had been placed in inpatient treatment because of difficult-to-manage behavior: aggression and other interpersonal conflicts with children and/or adults, destructiveness, impulsivity, hyperactivity and attention deficit problems. Subjects' mean IQ score was 96.5, standard deviation 15.6. Some children were clearly limited intellectually, four had diagnoses of pervasive devel- opmental disorder and one child had been diagnosed as schizo- phrenic. Some degree of academic retardation was present in the majority of cases.
Dow
nloa
ded
by [
Wes
tern
Ken
tuck
y U
nive
rsity
] at
02:
27 2
9 O
ctob
er 2
014
32 RESIDENTUL TREATMENT FOR CHILDREN & YOUTH
Treatment of data
Each child's total self-nominations, mentions by peers, and by staff members, were computed for the positive and the negative items. The total number of nominations by peers was divided by the number of peers and the same was done with staff nominations. This permitted direct comparison of the number of self-nominations with the average number of nominations received from peers and from staff.
Results
Table P shows the means and standard deviations of self, peers and staff nominations.
The data bear some resemblance to previous findings with nor- mal subjects: significantly more self-nominations for the positive than for the negative behaviors, significantly greater endorsement by self for positive items than endorsement by peers or staff (p < .001). There appeared to be a trend toward fewer mentions by self for negative items than by peers or staff and also for peers Po be more charitable in their assessments than are staff members.
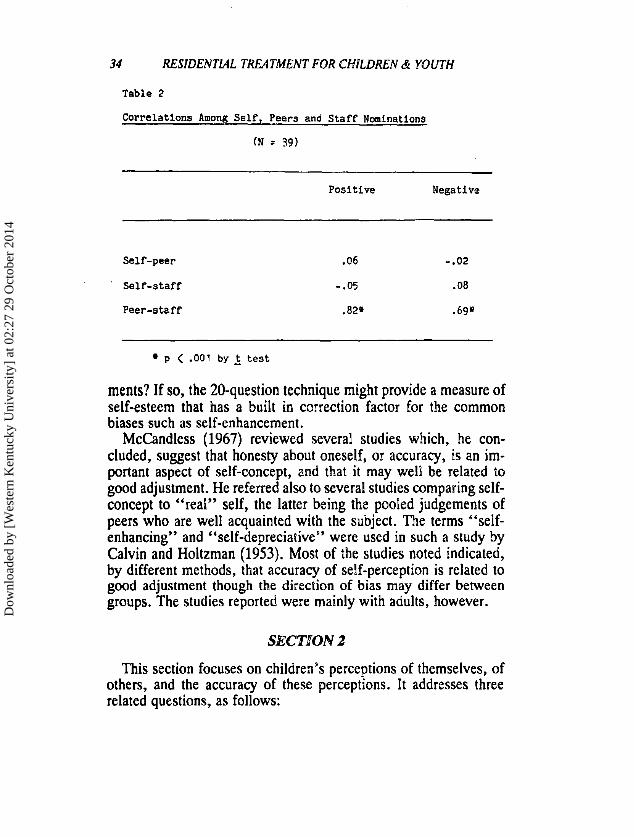
Table 2 depicts Pearson product-moment correlations among self, peer and staff nominations.
Whereas Ledingham et al. (1982) found low but generally signif- icant correlations between self and peers and self and teachers, the present findings show essentially no agreement between self and others in spite of strong agreement betweern peers and staff.
Discussion
The findings make it evident that while our hospitalized disturbed group show less accuracy in their self-assessment than do normal children, i.e., self-peer and self-staff correlations are nil, there is a high level of agreement between peers and staff. The oft-reported tendency toward self-aggrandizement is evident: over twice as many mean self-mentions (5.85) for positive items as nominations by peers or staff, and over twice as many self-mentions for positive than for negative items. Such endorsement of positives in a severely
\ \
Dow
nloa
ded
by [
Wes
tern
Ken
tuck
y U
nive
rsity
] at
02:
27 2
9 O
ctob
er 2
014
Henry F. Kaplan and James D. KIoss 33
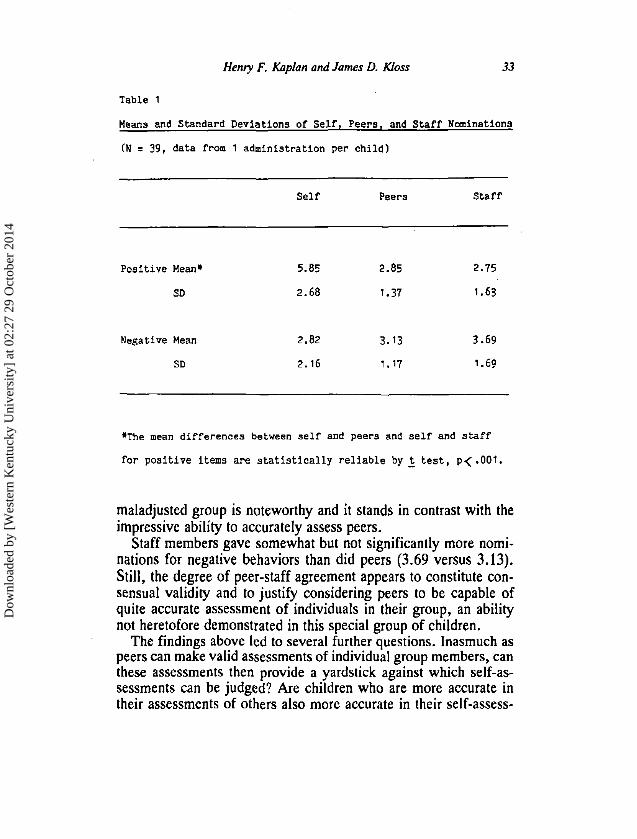
Table 1
Means and Standard Deviations of Self, Peers, and Staff Nominations
(N = 39, data from 1 administration per child)
Self Peers Staff
Positive Mean* 5.85 2.85 2.75
SD 2.68 1.37 1.63
Negative Mean
SD
*The mean differences between self and peers and self and staff
for positive items are statistically reliable by _t test, p< .001.
maladjusted group is noteworthy and it stands in contrast with the impressive ability to accurately assess peers.
Staff members gave somewhat but not significantly more nomi- nations for negative behaviors than did peers (3.69 versus 3.13). Still, the degree of peer-staff agreement appears to constitute con- sensual validity and to justify considering peers to be capable of quite accurate assessment of individuals in their group, an ability not heretofore demonstrated in this special group of children.
The findings above led to several further questions. Inasmuch as peers can make valid assessments of individual group members, can these assessments then provide a yardstick against which self-as- sessments can be judged? Are children who are more accurate in their assessments of others also more accurate in their self-assess-
Dow
nloa
ded
by [
Wes
tern
Ken
tuck
y U
nive
rsity
] at
02:
27 2
9 O
ctob
er 2
014
34 RESIDENTML TREATMENT FClR CtdlLDREN & YOUTH
Table 2
Correlations Among Se l f , Peers and Staff Nominations
(N = 39)
Positive Negative
Self-peer .06 -.02
Self-staff -.05 .08
p < .001 by t test
ments? If so, the 20-question technique might provide a measure of self-esteem that has a built in correction factor for the common biases such as self-enhancement.
McCandless (1967) reviewed several studies which, he con- cluded, suggest that honesty about oneself, or accuracy, is an im- portant aspect of self-concept, and that it may well be related to good adjustment. He referred also to several studies comparing self- concept to "real" self, the latter being the pooled judgements of peers who are well acquainted with the subject. The terns "self- enhancing" and "self-depreciative" were used in such a study by Calvin and Holtzman (1953). Most of the studies noted indicated, by different methods, that accuracy of self-perception is related to good adjustment though the direction of bias may differ between groups. The studies reported were mainly with adults, however.
This section focuses on children's perceptions of themselves, of others, and the accuracy of these perceptions. It addresses three related questions, as follows:
Dow
nloa
ded
by [
Wes
tern
Ken
tuck
y U
nive
rsity
] at
02:
27 2
9 O
ctob
er 2
014
Henry F. Kaplan and James D. KIoss 35
1. How many subjects do,,in fact, demonstrate greater accuracy in assessing others than themselves?
2. Is the inaccuracy essentially a matter of self-enhancement through endorsement of socially desirable items or might self- inaccuracy be otherwise conceptualized?
3. Is accuracy regarding self related to any other variables?
Method
Subjects
Children in this section included those in Section 1 plus 38 chil- dren who participated in 11 other administrations of the 20 question method. This made a total of 77 children. The added children were similar to those described previously in regard to background, be- haviors, age, and ability. Five administrations were interspersed among the five administrations used for Section 1, and the remain- ing six followed. Twenty-three children had one administration, and 54 had two or more.
Treatment of 20 Question Data
Inaccuracy, hereinafter referred to as discrepancy regarding self, is defined as the difference between the number of self-mentions for, e.g., the 10 positive items, and the mean mentions the child received from all peers for those items. Plus discrepancy, or plus bias, indicates a greater number of self-nominations than the mean of nominations received from peers for positive or for negative be- haviors. This approach assumes all positive items to be equivalent, and likewise for all negative items. An example of the derivation of the inaccuracy score follows:
Subject A nominated himself for 7 of the 10 positive items. His 8 peers gave him 33 nominations for those items, or a mean of 4.13. His self-discrepancy score, then, was + 2.87, indicating a plus bias on positive items.
The subject's discrepancy score regarding others was the differ- ence between the number of nominations given by the subject for all peers and the number received by all peers from the subject's peers divided by the number of choosers and again divided by the number
Dow
nloa
ded
by [
Wes
tern
Ken
tuck
y U
nive
rsity
] at
02:
27 2
9 O
ctob
er 2
014
36 RESIDENTML TREATMENT FOR CHILDREN d YOUTH
of peers (peers and choosers being identical). Thus, Subject A made 37 nominations of all peers for positive behaviors. His peers re- ceived 160 nominations for those items, excacluding those given out by the subject. Dividing by 8 (the number of other choosers) yields an average of 20. A's discrepancy, then, was 17 for 8 children. This was then divided by 8 (the number of peen) so that the resultant (+2.12) would be directly comparable to A's seif-discrepancy score. In this example discrepancy regarding others reflected a plus bias, but a lesser one than discrepancy regarding self.
The relationship between self and other discrepancy was studied in two ways, by comparing mean discrepancies regardless of dioec- tion, and also by comparing the signed discrepancies, or "'bias." Each administration was studied individually, group size ranging from 9 to 14, the modal size being 13. Investigation of bias permits a consideration of social desirability and the self-enhancement phe- nomenon. The data thus derived also permit comparing positive and negative behaviors with respect to discrepancy and type of bias, and the same is possible with respect to discrepancy vis-h-vis others. Data from all administrations for each child (187 cases) were used for this analysis.
Finally, data from the first administration only of the 77 subjects were used to obtain intercorrelations of discrepansy scores, percent of nominations received from peers that were for positive behaviors (referred to in results as percent positive), age, HQ scores, and final length of stay.
Results
Eight cone8intions obtained from the first administration for each child were significant (see Table 3) and seveeaP were quite high. Self-discrepansy on positive behaviors correlated with other dis- crepancy on positives at S O (p < .001), and the former correlated with other-discrepancy on negatives at .38 (p < .001). Seld-discrep- ancy on negatives and other-discrepancy on negatives comesated at .35 (p < .001). Other-discrepancy on positive behaviors and other- discrepancy on negatives correlated at -37. All discrepancy scores included bias, i.e., direction of discrepancy. Age, HQ, and final length of stay were not highly correlated with discrepancy scores.
Dow
nloa
ded
by [
Wes
tern
Ken
tuck
y U
nive
rsity
] at
02:
27 2
9 O
ctob
er 2
014
Henry F. Kaplan and James D. Kloss
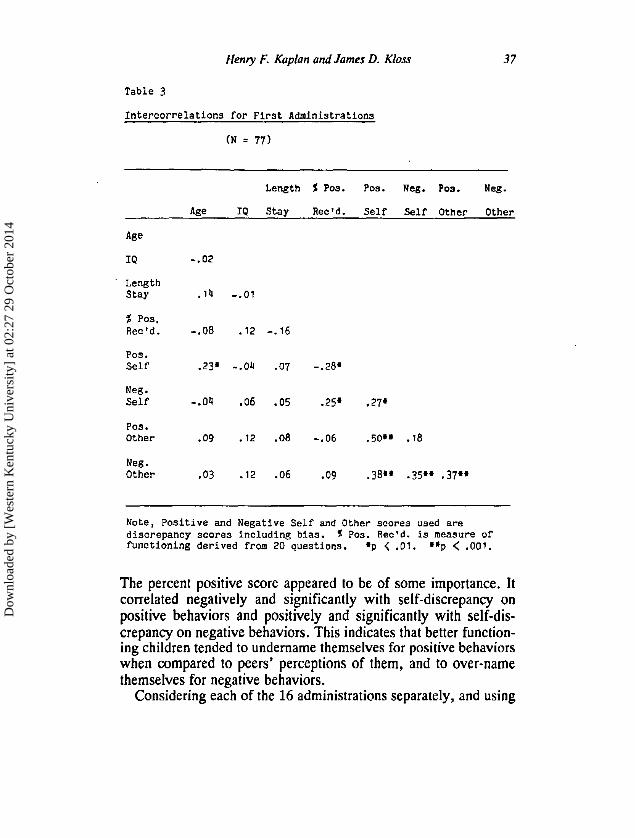
Table 3
Intercorrelations for First Administrations
(N = 77)
Length 5 Pos. Pos. Neg. Pos. Neg.
Age IQ Stay Rec'd. Self Self Other Other
Length Stay .14 -.01
% pos. Rec'd. -.08 .12 -.?6
POS. Self .23* -.04 .07 -.28*
P0S. Other .09 .?2 .08 -.06 .50** . I 8
Neg . Other -03 .12 .06 .09 .38" .35'+.37**
Note, Positive and Negative Self and Other scores used are discrepancy scores including bias. 5 Pos. Rec'd. is measure of functioning derived from 20 questions. *p < .O?. **p < .001.
The percent positive score appeared to be of some importance. It correlated negatively and significantly with self-discrepancy on positive behaviors and positively and significantly with self-dis- crepancy on negative behaviors. This indicates that better function- ing children tended to undername themselves for positive behaviors when compared to peers' perceptions of them, and to over-name themselves for negative behaviors.
Considering each of the 16 administrations separately, and using
Dow
nloa
ded
by [
Wes
tern
Ken
tuck
y U
nive
rsity
] at
02:
27 2
9 O
ctob
er 2
014
38 RESIDENTlAL TREATMENT FOR CPIILDREN & YOUTH
all data from all children, it was found that mean discrepancies regarding self were greater for positive than for negative behaviors in all 16 administrations. Discrepancies were greater for positive self-nominations than for positive other-nominations in all instances as well. Discrepancies were greater for negative self-nominations than for negative-other nominations in 93 administrations. Eight- one percent of the 187 cases showed Bower discrepancy scores for others than for self where positive behaviors were concerned. FOP negative behaviors, 60% were more accurate regarding others. Considering bias regarding self, 84% showed plus bias, or over- named on positive behaviors. For negative behaviors, 61% showed minus bias, i.e., minimized.
Further analysis indicates that, regarding positive behaviors, just over half of the cases showed plus bias regarding both self and others, i-e., are both self and other enhancing. Thirty-four percent showed plus bias for self and minus bias for others. Ian only two cases was minus bias regarding self coupled with plus bias toward others. A similar but less pronounced tendency applied to negative behaviors, i.e., for self and other biases to go together, 36% of cases showing minus bias for both self and others, i.e., under- naming.
Finally, considering combinations of biases for positive and neg- ative behaviors, in 50% of the cases the pattern was self-enhance- men1 on the former and under-naming on the Uatter. But in 32% there was over-naming for both groups of behavior. Children in this latter group might be termed "ego-centric"; they were self-anamers, A somewhat similar pattern was found regarding others, 76% erther wer-naming for both groups of behavior or under-naming for both.
DISCUSSION
The 20-question procedure combines a sociometric evaluation and a multifaceted assessment of se%f-perception. A number of mea- sures can be derived that have direct application to clinical work with children and adolescents who are well acquainted with each other, e.g,, in clubs, classrooms, or residential treatment settings. Monitoring progress in treatment is easily accotnpPished by refer- ence to the percent positive score. Level of self esteem and growth
Dow
nloa
ded
by [
Wes
tern
Ken
tuck
y U
nive
rsity
] at
02:
27 2
9 O
ctob
er 2
014
Henty F. Kaplan and James D. Kloss 39
in the ability to assess self with accuracy can also be measured over time.
The findings reported here extend the literature by documenting that even disturbed children are able to accurately assess the behav- ior of their peers. Inaccuracy about self is greater for positive be- haviors than for negative ones, perhaps because the negative behav- iors are of a more intrusive and visible nature than are positive behaviors. Ledingham et al. (1982), similarly noted higher correla- tions among self, peers and teachers on their aggressive factor than on withdrawal and likability; they described aggressive behaviors as more "perceptually compelling." But the present data also point up the tendency to self-enhancement, self-naming for positive behav- iors being in less agreement with others' perceptions than is true with neeative behaviors. "
The phenomenon of self-naming, regardless of type of behavior, seems to be noteworthy and worthy of study in more broadly repre- sentative groups. Almost a third of our children showed this pattern - .
of response. Some additional evidence of a relationship between accuracy in
assessment and overall functioning was provided by two pilot stud- ies, one involving a group of 10 gifted fourth-grade children and the other with a group of 11 hospitalized delinquent adolescents. The gifted children had a lower mean self-discrepancy score, ignoring bias, for positive and for negative behaviors than any of the 16 groups of CTU children. The average other-discrepancy was lower than 10 of the 16 CTU groups on positive items and lower than all groups on negative items. Further, accuracy regarding self was highly related to the percentage of mentions received that were for positive behaviors.
The delinquent adolescents also showed less self-discrepancy for positive behaviors than any of the CTU groups, but their self-dis- crepancy for negative behaviors fell well within the range of the CIW groups. Unlike the gifted children, accuracy regarding others was not notably greater than it was in the CTU groups. Both of these pilot groups had greater accuracy regarding others than re- garding self, and there was greater accuracy regarding self on nega- tive items than on positive items.
There is preliminary evidence offered here of the potential for
Dow
nloa
ded
by [
Wes
tern
Ken
tuck
y U
nive
rsity
] at
02:
27 2
9 O
ctob
er 2
014
40 RESIDENTLAL TREATMENT FOR CHILDREN & YOUTH
application of the '6discrepancy" and the '%asy' concepts as ap- proaches to understanding self-report and self-perception. There is a need to examine more precisely how competence, maturity, and self-esteem interact with accuracy and self-perception. Studies with more stable subjects in more stable groups with attention to sexual makeup should shed more light oh this matter.
REFERENCES
Calvin, A. D. & Holtzman, W. H. (1953). Adjustment and the discrepancy be- tween self-concept and inferred self. Journal of Consulting Psychology, 17, 39-44.
Cantrell, V. L. & Prinz, R. 9. (1985). Multiple perspectives of rejected, ne- glected, and accepted children: Relation between sociometric status and behav- ioral characteristics. Journal of Consulting and Cli~ical Psychology, 53, 884-889.
Dodge, K. A., Coie, J. D. & Brakke, N. P. (1982). Behavior patterns of socially rejected and neglected preadolescents: The roles of social approach and agpres- sion. Journal of Abnormal Child Psychology, 10, 389-410.
Eron, L. D., Walder, L. 0. & hfkowitz, M. M. (1971). Learning of aggression in children. Boston: Little, Brown & Co.
Himelstein, P. & kubin, R. (1965). Attempted validation of the self-disclosure inventory by the peer nomination technique. Journal of Psychologyi 61, 13-16. -- --.
Ledingham, J. E., Younger, A., Schwartzman, A. & Bergeron, 0. (1982). Agreement among teacher, peer, and self-ratings of children's aggression, withdrawal, and likability. Journal of Abnormal Child Psychology, 10, 363-372.
McCandless, B. R. (1967). Children: Behavior and development, 2nd edition. New York: Molt, Rinehart and Winston, Inc.
Millich, R. & Landau, S. (1984). A comparison of the social status and social behavior of aggressive and aggressivelwithdrawn boys. Journal of Abnormal Child Psychology, 12, 277-288.
Pekarik, E . G., Prinz. R. J. , Liebert, D. E., Weintraub, S. & Neale, 9. M. (1976). The pupil evaluation inventory: A sociometric technique for assessing children's social behavior. Journal of Abnormal Child Psychology, 4 , 83-97.
Walder, L. O., Abelson, R., Eron, &. D., Banta. T. 9. $r baulicht, 9. H. (1961). Development of a peer-rating measure of aggression. Psychological Repons, 9, 497-556 (monograph supplement 4-49).
Wiggins, 4. S. & Winder, C. b. (1964). The peer nomination inventory: An empirically derived sociometric measure of adjustment in preadolescent boys. Psychological Repom, 9, 643-677.
Wylie, R. C. (1979). The self-concept, Volume 2. Lincoln, NE: University of Nebraska Press.
Dow
nloa
ded
by [
Wes
tern
Ken
tuck
y U
nive
rsity
] at
02:
27 2
9 O
ctob
er 2
014
Henry F. Kaplan and James D. Kloss
BIOGRAPHICAL NOTE
Henry K. Kaplan is a psychologist w i th the Childrens Treatment Un i t o f Mendota Mental Health Institute, Madison, WI. His interests include small group dynamics and children's self-assessment and self-disclosure.
James D. Kloss is a psychologist and Executive Director of Mississi pi River Human Services Center, Ins. H i s professional interests are in !e- havioral treatment and program evaluation.
lor laculiy/prolessionals wdh journal suoscripl~on recommendalion aulhor~ly lor /her ~nsl~lul~onal Lbrary . . .
If you have read a reprinl or pholocopy 01 lhis erlicle, would you like lo make sure lhal your hbrary also subscr~bes 10 lhis journal? If you have Ihe aulhorily lo recommend sub- scriplions lo your library, we will send you a free sample copy for review wilh your librarian. Jusl fill oul the lorm below-snd make aure that you type or wrlle out clearly both the name of the journal and your own name and eddreoa.
( ) Yes, please send me a complimentary sample copy of lhis journal:
(please wrila in complele journal lille here-do not leave blank)
I will show lhis journal lo our inslilulional or agency library for a possible subscription. The name ol my inslilulional/agency library is:
CITY: STATE: ZIP:
Relurn lo: Sample Copy Deparlmenl, The Haworlh Press, Inc., 12 West 32 Streel, New York, NY 10001
Dow
nloa
ded
by [
Wes
tern
Ken
tuck
y U
nive
rsity
] at
02:
27 2
9 O
ctob
er 2
014