Embed Size (px)
Citation preview

http://jiv.sagepub.com/Violence
Journal of Interpersonal
http://jiv.sagepub.com/content/early/2013/12/03/0886260513507133The online version of this article can be found at:
DOI: 10.1177/0886260513507133
published online 5 December 2013J Interpers ViolenceSandra Flynn, Cathryn Rodway, Louis Appleby and Jenny Shaw
SurveySerious Violence by People With Mental Illness: National Clinical
- Mar 25, 2014version of this article was published on more recent A
Published by:
http://www.sagepublications.com
On behalf of:
American Professional Society on the Abuse of Children
can be found at:Journal of Interpersonal ViolenceAdditional services and information for
http://jiv.sagepub.com/cgi/alertsEmail Alerts:
http://jiv.sagepub.com/subscriptionsSubscriptions:
http://www.sagepub.com/journalsReprints.navReprints:
http://www.sagepub.com/journalsPermissions.navPermissions:
What is This?
- Dec 5, 2013OnlineFirst Version of Record >>
- Mar 25, 2014Version of Record
at NORTHERN ILLINOIS UNIV on September 9, 2014jiv.sagepub.comDownloaded from at NORTHERN ILLINOIS UNIV on September 9, 2014jiv.sagepub.comDownloaded from

Journal of Interpersonal Violence201X, Vol XX(X) 1 –21© The Author(s) 2013
Reprints and permissions:sagepub.com/journalsPermissions.nav
DOI: 10.1177/0886260513507133jiv.sagepub.com
Article
Serious Violence by People With Mental Illness: National Clinical Survey
Sandra Flynn, PhD,1 Cathryn Rodway, MA,1 Louis Appleby, MD, FRCPsych,1 and Jenny Shaw, PhD, FRCPsych1
AbstractThis study aimed to estimate the prevalence of mental disorder in offenders convicted of serious violence, examine their social and clinical characteristics, and compare them with patients convicted of homicide. We examined a national clinical survey of all people convicted of serious violence in England and Wales in 2004. Mental disorder was measured by contact with mental health services within 12 months of the offense. Of the 5,966 serious violent offenders, 293 (5%) had been in recent contact with mental health services. Personality disorder (63, 22%) and schizophrenia (55, 19%) were the most common diagnoses. Most had previous convictions for violence (168, 61%). Seventy-two (25%) patients were at high risk of violence and 34 (49%) were not subject to the Care Programme Approach. Compared with serious violence offenders, homicide offenders were more likely to have been patients (293, 5% vs. 65, 10%; p < .01). We conclude that patients were responsible for a small proportion of serious violent offenses; however, high-risk patients require closer supervision, and regular inquiry about changing delusional beliefs, thoughts of violence, and weapon carriage.
1University of Manchester, UK
Corresponding Author:Sandra Flynn, National Confidential Inquiry Into Suicide and Homicide by People With Mental Illness, Centre for Mental Health and Risk, University of Manchester, Jean McFarlane Building, Oxford Road, Manchester, M13 9PL, UK. Email: [email protected]
507133 JIVXXX10.1177/0886260513507133Journal of Interpersonal ViolenceFlynn et al.research-article2013
at NORTHERN ILLINOIS UNIV on September 9, 2014jiv.sagepub.comDownloaded from

2 Journal of Interpersonal Violence XX(X)
Keywordsviolent offenders, homicide, mental health and violence
Introduction
There were an estimated 1.9 million acts of violence reported in the Crime Survey for England and Wales in 2012 (Office for National Statistics, 2013). The U.K. Government’s action plan for reducing serious violent crime identi-fied key targets: the reduction of gun crime and gang-related violence, knife crime, and sexual and domestic violence. The government also identified individual risk factors associated with violent behavior such as alcohol abuse and exposure to violence at an early age, for example, through domestic vio-lence (Home Office, 2008). The link between criminal offending and mental illness has long been established. Previous research has shown that people with a major mental disorder have a small but increased risk of being violent (Arseneault, Moffitt, Caspi, Taylor, & Silva, 2000; Brennan, Grekin, & Vanman, 2000; Kooyman, Dean, Harvey, & Walsh, 2007; Lindqvist & Allebeck, 1990; Link & Stueve, 1994; Tiihonen, Isohanni, Rasanen, Koiranen, & Moring, 1997; Wessely, Castle, Douglas, & Taylor, 1994). The risk of vio-lence has also been shown to increase with comorbid substance abuse (Fazel, Langstrom, Hjern, Grann, & Lichtenstein, 2009). Numerous studies have reported violence within a patient sample (Link, Andrews, & Cullen, 1992; Monahan & Applebaum, 2000; Steadman et al., 1998) or mental illness in violent prisoners (Eronen, Hakola, & Tiihonen, 1996; Taylor & Gunn, 1984; Teplin, 1990).
In the few studies that have investigated the prevalence of violence by peo-ple with mental disorder, attributable risk was shown to be between 3% and 5% (Swanson, 1994). It is important to accurately establish the prevalence of mental illness in a community sample of violent offenders to reliably inform public perception and reduce stigma. Previous research has highlighted the importance of managing patients considered at high risk of violent offending through the use of the Care Programme Approach (CPA; Appleby et al., 2006; Swinson, Flynn, Kapur, Appleby, & Shaw, 2010). CPA was introduced by the Department of Health in 1991 to provide specialist mental health services with an effective structure to care for patients with complex needs, such as risk of harm to self or others, increased disengagement, comorbidity, and those requiring multi-agency support. It involves (a) assessment of need, (b) the formation of a care plan, (c) the appointment of a care coordinator, and (d) regular multidisciplinary review (Department of Health, 1999).
The definition of a mental disorder in the literature can be limiting, with several studies reporting either a combined group of mental disorders, or
at NORTHERN ILLINOIS UNIV on September 9, 2014jiv.sagepub.comDownloaded from

Flynn et al. 3
specific diagnosis, particularly schizophrenia/psychosis (Elbogen, Van Dorn, Swanson, Swartz, & Monahan, 2006; Fazel et al., 2009; Kooyman et al., 2007; Silver, Felson, & Vaneseltine, 2008). A further limitation as highlighted by Vinkers, de Beurs, Barendregt, Rinnie, and Hoek (2011) has been the defi-nition of “violent offending,” which is often over inclusive (i.e., any physical assault) or too specific (i.e., just homicide).
The theory suggesting that mental illness is a more significant feature in homicide than serious violence (Silver et al., 2008) has also been considered in this study. Based on attribution theory, it is hypothesized that the more deviant and abhorrent the act, the stronger the association with mental illness. Silver et al. (2008) tested the hypotheses by examining mental illness in those committing homicide and sexual offenses, compared with other physical assaults. They found homicide was more common than physical assault in those with minor mental health problems, but no relationship was found with severe mental illness. In light of this evidence, the early identification of mental health patients at risk of offending is essential to prevent behaviors escalating into serious violence.
The study has been undertaken as part of the National Confidential Inquiry Into Suicide and Homicide by People With Mental Illness (NCISH). The NCISH is a large-scale epidemiological study that provides a rich source of clinical data using a unique national database (Shaw et al., 1999). The meth-odology used by the NCISH was applied to a cohort of serious violent offend-ers. The aims of this study were to estimate the prevalence of mental disorder in offenders convicted of serious violence; to undertake an examination of the social, offense, and clinical characteristics of patients who committed serious violence, particularly those considered high risk; and to compare patients who committed serious violence with patients who were known to have committed homicide. The rational for these aims was to update the lit-erature by reporting the prevalence of serious violence committed by people with mental illness in a current national population sample. We also wanted to present the diagnosis, clinical care, management, and treatment received by violent patients under the care of mental health services, and to determine whether patients committing serious violence were clinically different from those who committed a homicide.
Method
Design
The NCISH was established by the U.K. Department of Health in 1992 fol-lowing a number of high-profile homicides by mental health patients, and
at NORTHERN ILLINOIS UNIV on September 9, 2014jiv.sagepub.comDownloaded from

4 Journal of Interpersonal Violence XX(X)
criticism of the provision of community care for patients with severe mental illness. The main aims of the NCISH are to establish the rate of mental disor-der in patients in contact with mental health services who died by suicide or had been convicted of homicide, and to recommend measures to reduce the risk of suicide and homicide by people under the care of mental health ser-vices. In this study, the NCISH methodology was applied to a national popu-lation of offenders convicted of serious violent offenses in England and Wales, and as such, this study was an extension of the NCISH’s ongoing core research into suicide and homicide. Our data collection process is outlined in Figure 1.
Sample
Comprehensive national sample of serious violent offenders. We were notified by the Home Office Offender Index of all convictions for serious violent offenses in England and Wales between January 1, 2004, and December 31, 2004, with a total of 6,474 offenses committed by 5,966 individuals. Demographic information and details of the offender and offense were available for all
Obtain nationalsample of serious
violent offender data
Identification ofmental health service
contact
No previous contactwith
mental health services
Previous contact withmental health services
Send questionnaire toconsultant psychiatrist
for completion
Figure 1. Data collection process.
at NORTHERN ILLINOIS UNIV on September 9, 2014jiv.sagepub.comDownloaded from

Flynn et al. 5
perpetrators. The authors selected four offenses defined as “specified violent offenses” under Schedule 15 (section 244) of the Criminal Justice Act 2003, chapter 44 (HMSO, 2003). We specifically focused on Offenses Against the Person, which are considered to represent a potential “near miss homicide”; these were attempted murder, malicious wounding “and other like offenses” (Section 20), wounding or other act endangering life (Section 18), and threats or conspiracy to murder. Our contacts within the Police Service advised the inclusion of “threats to kill,” as this offense has long been considered an indicator of future violence, and this has also been previously reported in the literature (MacDonald, 1963; Planansky & Jihnson, 1977). Vinkers et al. (2011) in a Dutch study of over 20,000 pre-trial forensic psychiatric reports between 2000 and 2007 found threats of homicide and homicide attempts to be significantly associated with mental disorders such as personality disor-ders and psychotic disorders. It has been observed in an Australian study of adult forensic patients who had threatened to kill another person that of the 144 patients in their sample, over 20% had committed an assault including 1 homicide within 12 months of making the threat (Warren, Mullen, & Ogloff, 2011).
Greater Manchester Police provided a detailed history of previous offend-ing on all the serious violence perpetrators in the study. The data were extracted from the Police National Computer.
Identification of mental health service contact. Identifiable information on the 5,966 perpetrators who had been convicted of a serious violent offense in 2004 was sent to all hospitals and mental health service providers in England and Wales, within the perpetrators’ district of residence and adjacent districts. We were notified by our contacts within the hospital of the date of the per-son’s last contact with mental health services (if any), and the name of the supervising clinician. The cases with mental health contacts will be hence-forth referred to as “patients.”
Collection of clinical data. Following the confirmation of contact with mental health services, a questionnaire was sent to the supervising clinician. The questionnaire consisted of 10 sections containing questions on priority patients, demographic information, psychiatric and forensic history, details of the index incident, details of other violence incidents, psychiatric in-patient violence, outpatient community patients, treatment and compliance, last con-tact with mental health services, clinicians’ views on prevention, and a final section for additional information. This questionnaire required clinicians to extract factual information from case notes, and is not based on opinion. The questionnaire was completed by the supervising clinician at the time of the
at NORTHERN ILLINOIS UNIV on September 9, 2014jiv.sagepub.comDownloaded from

6 Journal of Interpersonal Violence XX(X)
incident in conjunction with the multidisciplinary team, based on their per-sonal knowledge of the patient and from a review of the patients’ case notes. We consider this to be the most reliable source of information regarding patient care and diagnoses. Diagnoses were made by the clinicians who treated the patients in accordance with the International Classification of Disease–10th Revision (World Health Organization, 1992). The question-naire used in this study was a variant of the NCISH’s homicide questionnaire. A sample is available on the NCISH website (www.bbmh.manchester.ac.uk/cmhr/research/centreforsuicideprevention/nci/FAQs/Inquirymethodology/Coresuihomimethod/).
An audit of the NCISH’s case ascertainment method and inter-rater reli-ability of the questionnaire was previously undertaken across 16 hospitals. The identification of a mental health contact ranged from 98% to 100%. Agreement on the validity of key questions (including diagnoses) ranged from 90% to 100% (Windfuhr et al., 2008).
Serious Violence Sample
Between January 1, 2004, and December 31, 2004, in England and Wales, 307 offenders were known to have been in contact with mental health ser-vices 12 months prior to the offense. This figure of 307 is probably an under-estimation as it is likely that some service contacts were not identified, particularly for those individuals who had been under services in one locality and moved areas without making contact with services in their new district of residence. Of the 307 patients, data were not obtained on four cases due to missing case notes. Participation was not mandatory and a further 10 clini-cians did not wish to be involved; therefore, we had a response rate of 95%.
NCISH Homicide Sample
The NCISH focuses on two core areas of research: suicide and homicide. To date, the NCISH has collated data on 95,000 suicides and 10,000 homicides over 17 years. A sample of homicide cases from the NCISH’s national clini-cal survey was used as a comparator with people convicted of serious vio-lence for the same time period. The data were extracted from the NCISH homicide database on all homicide perpetrators convicted between January 1, 2004, and December 31, 2004, in England and Wales. Of the 655 convicted homicide perpetrators, 65 were confirmed as having been in contact with mental health services (i.e., mental health patients) within 12 months of the offense. Clinical data were available on all of these patients, with a question-naire response rate of 100%.
at NORTHERN ILLINOIS UNIV on September 9, 2014jiv.sagepub.comDownloaded from

Flynn et al. 7
The NCISH clinical survey method of data collection was used for both the serious violence sample and the comparison homicide group. These 65 homicide patients were used as a comparison group only and were not included in the main “serious violence” analysis.
Measures
Previous Violence
We defined a history of previous violence as convictions for homicide, attempted murder, grievous bodily harm, actual bodily harm, threats to kill, and other violent acts such as common assault. These are listed as violent offenses under the Offenses Against the Person Act 1861.
High Risk
The study distinguishes a group of patients who posed a significant risk to others, referred to as “high-risk patients.” The definition is based on the Department of Health’s white paper “Reforming the Mental Health Act—Summary” (Department of Health, 2000) that refers to high-risk patients with mental illness who had been “detained under civil powers, and others who are remanded or convicted offenders.” Our definition of high-risk patients included those with severe mental illness, a history of violence, or previous detention under mental health legislation, but does not include patients with severe personality disorder. Information on previous detention was extracted from the clinical questionnaire and convictions for previous violence from antecedent data via the Police National Computer. The rationale for the defi-nition of high risk was based on potential dangerousness of patients based on illness, previous violence, and involuntary detention.
Severe Mental Illness
Severe mental illness is an accepted clinical term. In this study, we have adopted a broad definition based on diagnoses of schizophrenia and other delusional disorders and affective disorders. We have not assessed the dura-tion of illness or level of dysfunction in this definition.
Data Analysis
To address the first aim of the study, general population and patient rates were calculated using mid-year population estimates (aged 10 and over) as a
at NORTHERN ILLINOIS UNIV on September 9, 2014jiv.sagepub.comDownloaded from

8 Journal of Interpersonal Violence XX(X)
denominator. These data were obtained from the Office for National Statistics. In addition, descriptive statistics were used to describe the proportion of seri-ous violence in England and Wales committed by mental health patients. The second aim was addressed by using descriptive statistics to examine the demographic, behavioral, offending, and clinical characteristics of these patients. For the third aim, inferential statistics were used to test for differ-ences between patients convicted of serious violence and patients who had been convicted of homicide. The findings are presented in tables as propor-tions with 95% confidence intervals (CIs). Chi-square was used to test asso-ciations between the independent variables (demographic, behavioral, offending, and clinical characteristics) and the dependent variable (serious violence or homicide outcome). Logistic regression analyses were also con-ducted to test for association. Odds ratios (ORs) were calculated and the pro-portions are presented with 95% CIs.
As this study mostly reported descriptive statistical analysis, we did not undertake sensitivity analysis to measure the effect of missing data on these findings. However, we found the proportion of missing data to be acceptable. Analysis showed a median of 2% missing data for demographic/behavioral and offense variables and 6% for clinical data. If an item of information was not available or not known for a particular case, the case was removed from the analysis of that item; the denominator in all estimates was the number of valid cases. Data were analyzed using STATA Version 11 (StataCorp, 2009).
Ethical Approval
We sought permission to extend the NCISH methodology to include serious violence from the Patient Information Advisory Group (now the National Information Governance Board for Health and Social Care). Authorization was obtained under Section 251 of the National Health Service Act 2006 (HMSO, 2006). This was granted in the interest of improving patient care, permitting confidential and identifiable information to be obtained without informed consent from a large cohort. Ethical approval was obtained on September 9, 2003. The study is also registered under the Data Protection Act 1998 (Parliament, UK, 1998).
Results
Serious Violence in the General Population
A total of 6,474 offenses were committed by 5,966 individuals, with a rate of 12.7 offenders per 100,000 population. The most common offense
at NORTHERN ILLINOIS UNIV on September 9, 2014jiv.sagepub.comDownloaded from

Flynn et al. 9
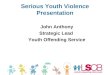
was malicious wounding (see Figure 2). The majority of perpetrators were male (5,480, 92%). The median age of offenders was 26 (range = 17-88), with nearly half unemployed at the time of the offense (2,749, 47%). Most of the perpetrators were born in the United Kingdom (5,264, 90%).
Serious Violence Among Mental Health Patients
Prevalence of patients committing serious violence. Three-hundred and seven offenders were known to have been in contact with mental health services 12 months prior to the offense, with a 1-year rate of 0.66 per 100,000 population. The main findings were based on the 293 patients for whom clinical data were received. Patients committed a total of 354 offenses, the most common being malicious wounding (see Figure 2).
Demographic and behavioral characteristics. The demographic and behavioral characteristics of patients are presented in Table 1. Patients were predomi-nantly male, unmarried, and unemployed, with a median age of 30. Both alcohol misuse and drug misuse were frequently reported. The majority had previous convictions, and the number of court appearances ranged from 1 to 213 (with a median of 8). Nearly two thirds had convictions for previous violence, including four patients who had previously been convicted of homi-cide. Half had previously received a custodial sentence.
Seriousviolent offences
N=6474
Malicious wounding(Section 20)
N=3904
PatientsMalicious wounding
(Section 20)N=156 (4%)
Wounding(Section 18)
N=1640
PatientsWounding
(Section 18)N=74 (5%)
Threats to killN=825
PatientsThreats to killN=120 (15%)
Attempted murderN=105
PatientsAttempted murder
N=4 (1%)
Figure 2. Number of serious violent offenses in England and Wales, 2004, by general population and patients.
at NORTHERN ILLINOIS UNIV on September 9, 2014jiv.sagepub.comDownloaded from

10 Journal of Interpersonal Violence XX(X)
Offense characteristics. Figure 3 shows the number of offenses by primary diagnosis. Attempted murder was the least common violent offense commit-ted by patients; all four of the patients convicted of this offense had severe mental illness.
Clinical characteristics. The clinical characteristics of offenders are presented in Table 2. The most common diagnosis was personality disorder. Severe mental illness (schizophrenia or affective disorder) was diagnosed in 98 cases (34.5%), in 23 (23%) of these patients, the onset of illness had been in the previous year. Of the 55 patients with schizophrenia (0.9% of all serious vio-lent offenders), 47 (85%) had dual diagnosis (severe mental illness and drug
Table 1. Demographic, Behavioral, and Offense Characteristics of Patients Committing Serious Violence and Homicide in England and Wales, 2004.
Serious Violence in 2004 (n = 293)
Homicide in 2004 (n = 65)
n % 95% CI n % 95% CI p value
Demographic characteristics Age: Median (range) 30 (17-82) 31 (15-62) .46 Male 245 84 [79, 88] 53 82 [70, 90] .69 Black and minority
ethnic groups35 13 [9, 17] 10 16 [8, 27] .48
Not currently married 218 80 [75, 85] 53 84 [73, 92] .47 Unemployed/long-term
sickness leave233 86 [82, 90] 48 80 [68, 89] .22
Living alone 114 44 [38, 50] 23 40 [27, 53] .56Behavioral characteristics History of self-harm 147 53 [47, 59] 37 60 [46, 72] .33 History of alcohol
misuse199 71 [65, 76] 37 61 [47, 73] .12
History of drug misuse 199 72 [67, 78] 42 67 [54, 78] .37History of offending Any previous
convictions232 84 [79, 88] 47 84 [72, 92] .98
Any previous convictions for violence
168 61 [55, 67] 31 48 [35, 60] .05
Previously sentenced to prison
133 50 [44, 57] 25 41 [29, 55] .22
Note. CI = confidence interval.
at NORTHERN ILLINOIS UNIV on September 9, 2014jiv.sagepub.comDownloaded from

Flynn et al. 11
and/or alcohol misuse and/or dependence). The 55 patients with schizophre-nia committed 71 offenses, the most common being malicious wounding (29, 41%). Patients with personality disorders were most frequently convicted of threats to kill (52, 59% of 88 offenses), and malicious wounding was the most common violent offense committed by patients with affective disorders (21, 46% of 46 offenses; see Figure 3). A total of 78 (27%) patients had dual diagnosis.
Most patients had their last contact with general psychiatry services (209, 72%); 7 (2%) were last seen by forensic services. Over a quarter of patients missed their last appointment with mental health services. A fifth refused treatment with medication within a month of the offense. The majority of patients (231, 80%) were not receiving care under the CPA at a level requir-ing regular multidisciplinary reviews. Clinicians stated that 34 (16%) of the violent assaults were preventable. Factors that could have made the violence significantly less likely included better patient compliance with medication (75, 32%), closer patient supervision (45, 19%), availability of dual diagnosis services (44, 18%), and better liaison between services (44, 18%).
High-risk patients. Our definition of high-risk patients included those with severe mental illness (schizophrenia or affective disorder) and a history of violence or previous detention under mental health legislation. Of the 72 (25%) high-risk patients, 13 (18%) were in-patients at the time of the offense,
31 0 0 0 0
29
21
29
24
15
33
52
1616
1114
811
8
21
77
18
0
10
20
30
40
50
60
Schizophrenia Affectivedisorder
Personalitydisorder
Alcoholdependence
Drugdependence
Otherdiagnosis*
Frequency
Attempted murderMalicious woundingThreats to killWounding
*Other diagnosis: adjustment disorder, organic disorder, alcohol misuse, drug misuse, anxiety/phobia/panic/obsessive compulsive disorder, dementia.
Figure 3. Patients: Number of serious violent offenses by primary diagnosis.
at NORTHERN ILLINOIS UNIV on September 9, 2014jiv.sagepub.comDownloaded from

12 Journal of Interpersonal Violence XX(X)
Table 2. Comparison of Clinical Characteristics of Patients Committing Serious Violence and Homicide in England and Wales, 2004.
Serious Violence in 2004 (n = 293)
Homicide in 2004 (n = 65)
n % 95% CI n % 95% CI p value
In-patient 16 6 [3, 9] 0 0 [0, 0] .05Post-discharge patient 32 12 [8, 16] 6 9 [3, 19] .59Subject to enhanced CPA 56 20 [15, 25] 12 19 [10, 31] .98Missed last contact 82 31 [26, 37] 28 45 [32, 58] .04Follow-up action taken
after missed appointment66 81 [71, 89] 12 63 [38, 74] .08
Non-compliance in the last month
48 19 [14, 24] 11 21 [11, 34] .74
Attempts to encourage adherence with medication
23 49 [34, 64] 2 18 [2, 52] .09
Primary diagnosis Schizophrenia and other
delusional disorders55 19 [15, 24] 16 25 [15, 38] .28
Affective disorder (bipolar and depression)
43 15 [11, 20] 10 16 [8, 27] .89
Alcohol dependence 39 14 [1, 18] 4 6 [2, 15] .14 Drug dependence 33 12 [8, 16] 9 14 [7, 25] .56 Personality disorder 63 22 [17, 27] 14 22 [13, 34] .99Any secondary diagnosis 182 62 [56, 68] 39 60 [47, 72] .75Duration of history (under
12 months)90 33 [28, 39] 18 30 [19, 43] .63
Previous admissions as an in-patient
160 55 [49, 61] 43 67 [54, 78] .08
Previously detained under the MH Act
77 27 [22, 32] 9 14 [7, 25] .04
Last contact within 7 days of offense
57 21 [16, 25] 10 16 [8, 27] .38
Symptoms at last contact 162 59 [53, 65] 30 48 [35, 61] .09Estimate of immediate risk:
low or none180 88 [83, 92] 54 95 [85, 99] .15
Estimate of long-term risk: low or none
119 59 [52, 66] 44 79 [66, 88] <0.01
Offense thought to be preventable
34 16 [11, 21] 6 11 [4, 22] .36
Note. CPA = care programme approach; MH Act = Mental Health Act.
at NORTHERN ILLINOIS UNIV on September 9, 2014jiv.sagepub.comDownloaded from

Flynn et al. 13
and 7 (10%) had been discharged from in-patient care within 3 months before the offense. Twenty (29%) had disengaged with services, and 22 (34%) were non-adherent with medication. A total of 57 (83%) had a history of alcohol and/or drug misuse, and 34 (49%) were not subject to enhanced CPA. Of those high-risk patients not under the CPA, 11 (32%) missed their last appointment, and 6 (21%) were non-adherent with their medication in the month before the offense. Most were under the care of general adult services (89%).
Serious Violent Patients Versus NCISH Homicide Patients
We compared the 293 patients convicted of serious violence with 65 patients convicted of homicide (see Tables 1 and 2). Schizophrenia was shown to be 3 times more likely in patients who committed homicide than in patients who committed serious violence (16, 2% vs. 55, 0.9%; ORs = 2.7). Patients also committed proportionally more homicides than serious violence (65, 10% vs. 293, 5%; p < .01). Patients who committed homicide were more likely to have missed their last appointment with mental health services, and their long-term risk of violence was more commonly estimated to be low or none by the clinicians responsible for their care. Serious violence patients were more frequently detained under the Mental Health Act. Serious violence patients with severe mental illness were also more likely to have dual diagno-sis compared with homicide offenders with severe mental illness (78, 80%, vs. 14, 54%; p > .01). There were no significant differences in the proportion of patients with previous convictions for sexual offenses, criminal damage, or carrying offensive weapons. We found a borderline significant difference in the proportion of patients with previous violent convictions (p = .05), which was more common in patients who committed serious violence.
Discussion
Main Findings
We reported findings from a large population-based study examining perpe-trators convicted of serious violence in England and Wales. We found that 5% of offenders were patients who had been in recent contact with mental health services. Most of the violence by mental health patients was committed by young males, who had a history of violence, alcohol abuse, and drug misuse, and had previously been imprisoned. Personality disorders and schizophrenia were the most common diagnoses. The commonest offense among those with personality disorder was threats to kill, whereas malicious wounding was more common in patients with severe mental illness.
at NORTHERN ILLINOIS UNIV on September 9, 2014jiv.sagepub.comDownloaded from

14 Journal of Interpersonal Violence XX(X)
It has previously been suggested that offenders who commit serious vio-lence had an increased relative risk of committing homicide (Soothill, Francis, & Liu, 2008), and that there is a similarity in the etiology of people who commit serious violence and homicide (Gottfredson & Hirschi, 1990). If the criminological theories are carried, one would assume that the character-istics of serious violence offenders and homicide offenders would be similar, including rates of contact with mental health services. We found there to be comparable demographic and behavioral characteristics; however, there were some interesting differences. Strikingly, the proportion of patients in contact with mental health services was significantly lower in the serious violence sample. However, serious violence patients were more likely to have a his-tory of previous violence and previous detention under the Mental Health Act compared with homicide patients, suggesting that a higher proportion had previously presented as a danger to themselves or others. Serious violence patients with severe mental illness were also significantly more likely to have comorbid substance misuse than homicide patients. Substance abuse comor-bidity has been found to increase risk of violence in patients with schizophre-nia (Fazel et al., 2009), and Volavka and Swanson (2011) suggested substance abuse treatment be incorporated into risk management plans of patients with severe mental illness.
How Do We Explain Higher Rates of Mental Disorder in Those Convicted of Homicide?
It has been asserted that perpetrators of homicide and those who commit seri-ous acts of violence are exhibiting the same behavioral characteristics, the only difference being the “legal label” applied to a fatal or non-fatal outcome (Harries, 1990). Proponents of this theory suggest the reason why some acts of violence result in the loss of life could be associated with the lethality of the method used, the response of the police, and the timely receipt of medical attention for the victim. Conversely, an alternative hypothesis suggests that these offenses can be distinguished by the perpetrators’ motivation, whether they had the intent to kill or to injure (Kleck, 1991). Silver et al. (2008) tested the hypothesis that the more serious or heinous the crime, the more likely the perpetrator will have severe mental illness, but an association was only observed in those with minor mental disorder. Therefore, it could be argued that the higher proportion of mental disorder in homicide compared with other violence may be linked to the severity of symptoms in some perpetra-tors, which leads them to kill rather than injure, but this would only account for a minority of cases.
at NORTHERN ILLINOIS UNIV on September 9, 2014jiv.sagepub.comDownloaded from

Flynn et al. 15
To put our findings in context, the prevalence of psychotic disorders in the general population of men aged 25 to 35 years in England was 0.6% in 2007 (National Centre for Social Research, 2009). Although not directly comparable, we found a higher proportion of serious violent and homicide offenders with schizophrenia in our general population sample (0.9% and 2%, respectively). Contact with mental health services before the offense was also more common among perpetrators of homicide than serious violence. The difference could be explained by a psychotic mental state at the time of the offense. In a study of homicide perpetrated by men with schizophrenia, Joyal, Putkonen, Paavola, and Tiihonen (2004) found that 60% were motivated by psychotic symptoms. Meehan et al. (2006) also observed that in homicides committed by people with schizophrenia (59% were experiencing delusions at the time of the offense), psychotic symptoms may place some patients at risk of committing violent acts due to a sense of personal threat and loss of control. Therefore, it is possible that there is a group of people with psychosis who when violent are more likely to have a lethal outcome, and this is related to specific delusions, intent, and the carriage of lethal weapons (Rodway et al., 2009). Evidence has shown that esca-lating psychotic symptomology (paranoia and command hallucinations) increases homicidal ideation and intent (Kaplan & Sadock, 1995; Schwartz, Petersen, & Skaggs, 2001). In addition, physical assaults motivated by psycho-sis and manifesting extreme violence are more likely to have a fatal outcome.
Limitations
The study describes a large national consecutive case series of offenders con-victed of violence against the person who had been in recent contact with mental health services prior to the offense. The NCISH’s established method-ology has proven validity and representativeness, with mental health contact identified in 98% to 100% of cases. The comprehensive clinical data set enabled an in-depth analysis of the care and treatment received by patients prior to the incident. The findings should be considered in the context of the methodological shortcomings. Reporting data on convicted offenders rather than those suspected or charged with an offense ensured that the individuals were found guilty; however, this may have led to an underestimation of vio-lence by people with mental illness, as not all incidents are reported or pros-ecuted. Contact with mental health services as a measure of mental illness may also underestimate the extent of violent offenders who had a mental ill-ness at the time of offense. This definition does not include patients whose care was managed by a general practitioner or primary care teams in the com-munity. Unlike the NCISH homicide study, we did not obtain reports from
at NORTHERN ILLINOIS UNIV on September 9, 2014jiv.sagepub.comDownloaded from

16 Journal of Interpersonal Violence XX(X)
psychiatric assessment used in court; therefore, a comparison of symptoms of mental illness at the time of the offense between serious violence and the NCISH homicide patients was not possible. Furthermore, we were unable to provide a detailed examination of personality disorder types, which would have been a valuable addition to the results. Finally, as this was largely a descriptive study, we were unable to test hypotheses or establish causal fac-tors that may have led to the violent incident.
Implications for Service Provision
Our findings have shown that mental health patients were responsible for a small proportion of serious violence committed nationally. This is a key mes-sage that can be used to reduce stigma and challenge the public perception that people with mental illness are dangerous. Of the patient group who com-mitted serious violent acts, our study highlights implications for mental health service management. We reported that over a third of patients who committed a serious act of violence had severe mental illness, a quarter were defined as high-risk, having severe mental illness and previous convictions for violence or detention under the Mental Health Act. However, our findings show that despite the high-risk status of these patients, CPA was under-used and disengagement from treatment and non-adherence with medication was not uncommon, a finding consistent with a study of homicide patients by Swinson et al. (2010). To reduce the risk of adverse incidents, care plans should be in place to manage risk and specify action if a crisis does occur. New guidance for the use of CPA was published by the Department of Health in 2008 (Department of Health, 2008). Whether this has led to fewer high-risk patients disengaging with services is unknown, but the evidence from this study suggests that better risk management for these patients is required.
The majority of the patients in this study had their last contact with general adult services rather than the forensic service. Future research into the use of risk assessment tools such as the Historical, Clinical, Risk Management–20 (HCR-20) in this setting may help to identify patients most at risk of commit-ting serious acts of violence and inform future management plans. Staff need to ensure that high-risk patients maintain contact with services and that staff regularly inquire about changing delusional beliefs, thoughts of violence, and weapon carriage.
Acknowledgments
The study was carried out as part of the National Confidential Inquiry Into Suicide and Homicide by People With Mental Illness. We acknowledge the help of district directors of public health, health authority and trust contacts, and consultant
at NORTHERN ILLINOIS UNIV on September 9, 2014jiv.sagepub.comDownloaded from

Flynn et al. 17
psychiatrists for completing the questionnaires. We acknowledge the contribution made by members of the National Confidential Inquiry: Kelly Hadfield, James Burns, Professor Navneet Kapur, Dr. Kirsten Windfuhr, Dr. Alyson Williams, Dr. Isabelle. M. Hunt, Dr. David While, Alison Roscoe, Saied Ibrahim, Rebecca Lowe, Phil Stones, Julie Hall, and Huma Daud.
Declaration of Conflicting Interest
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Louis Appleby is the National Clinical Director for Health and Criminal Justice for England.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Healthcare Quality Improvement Partnership (HQIP), Department of Health, UK.
References
Appleby, L., Shaw, J., Kapur, N., Windfuhr, K., Ashton, A., Swinson, N., . . .Stones, P. (2006). Avoidable deaths: Five year report of the National Confidential Inquiry Into Suicide and Homicide by People With Mental Illness. Retrieved from http://www.bbmh.manchester.ac.uk/cmhr/research/centreforsuicidepreven-tion/nci/reports/avoidable_deaths_full_report_december_2006.pdf
Arseneault, L., Moffitt, T. E., Caspi, A., Taylor, P., & Silva, P. A. (2000). Mental disorders and violence in a total birth cohort: Results from the Dunedin Study. Archives of General Psychiatry, 57, 979-986.
Brennan, P. A., Grekin, E. R., & Vanman, E. J. (2000). Violence among the mentally ill: Effective treatments and management strategies. In S. Hodgins (Ed.), Major mental disorders and crime in the community: A focus on patient populations and cohort investigations (pp. 3-18). Dordrecht, The Netherlands: Kluwer Academic Publishers.
Department of Health. (1999). Effective care co-ordination in mental health ser-vices: Modernising the care programme approach (A policy booklet). London, England.
Department of Health. (2000). Reforming the Mental Health Act. London, England. Retrieved from http://webarchive.nationalarchives.gov.uk/+/www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsLegislation/DH_4006263
Department of Health. (2008). Refocusing the care programme approach: Policy and positive practice guidance. London, England. Retrieved from http://webarchive.nationalarchives.gov.uk/20130107105354/http:/dh.gov.uk/prod_consum_dh/groups/dh_digitalassets/@dh/@en/documents/digitalasset/dh_083649.pdf
Elbogen, E. B., Van Dorn, R., Swanson, J. W., Swartz, M. S., & Monahan, J. (2006). Treatment engagement and violence risk in mental disorders. British Journal of Psychiatry, 189, 354-360.
at NORTHERN ILLINOIS UNIV on September 9, 2014jiv.sagepub.comDownloaded from

18 Journal of Interpersonal Violence XX(X)
Eronen, M., Hakola, P., & Tiihonen, J. (1996). Mental disorders and homicidal behav-ior in Finland. Archives of General Psychiatry, 53, 497-501.
Fazel, S., Langstrom, N., Hjern, A., Grann, M., & Lichtenstein, P. (2009). Schizophrenia, substance abuse and violent crime. Journal of American Medical Association, 301, 2016-2023.
Gottfredson, M. R., & Hirschi, T. (1990). A general theory of crime. Palo Alto, CA: Stanford University Press.
Harries, K. D. (1990). Serious violence: Patterns of homicide and assault in America. Springfield, IL: Charles C. Thomas.
HMSO. (2003). Criminal Justice Act 2003. London, England: TSO (The Stationery Office). Retrieved from http://www.legislation.gov.uk/ukpga/2003/44/contents
HMSO. (2006). National Health Service Act 2006. London, England: TSO (The Stationery Office). Retrieved from http://www.legislation.gov.uk/ukpga/2006/41/pdfs/ukpga_20060041_en.pdf
Home Office. (2008). Saving lives. Reducing harm. Protecting the public: An action plan for tackling violence 2008-11. London: England. Retrieved from http://webarchive.nationalarchives.gov.uk/20100413151441/http:/www.homeoffice.gov.uk/documents/violent-crime-action-plan-08/index.html
Joyal, C. C., Putkonen, A., Paavola, P., & Tiihonen, J. (2004). Characteristics and circumstances of homicidal acts committed by offenders with schizophrenia. Psychological Medicine, 34, 433-442.
Kaplan, H. I., & Sadock, B. J. (1995). Pocket handbook of clinical psychiatry (2nd ed.). Baltimore, MD: Williams & Wilkins.
Kleck, R. (1991). Point blank: Guns and violence in America. New York, NY: Aldine de Gruyter.
Kooyman, I., Dean, K., Harvey, S., & Walsh, E. (2007). Outcomes of public concern in Schizophrenia. British Journal of Psychiatry, 191, S29-S39.
Lindqvist, P., & Allebeck, P. (1990). Schizophrenia and crime. A longitudinal follow-up of 644 Schizophrenics in Stockholm. British Journal of Psychiatry, 157, 345-350.
Link, B. G., Andrews, H., & Cullen, F. T. (1992). The violent and illegal behaviour of mental patients reconsidered. American Sociological Review, 57, 275-292.
Link, B. G., & Stueve, A. (1994). Psychotic symptoms and the violent/illegal behav-iours of mental patients compared to community controls. In J. Monahan & H. J. Steadman (Eds.), Violence and mental disorder developments in risk assessment (pp. 137-155). Chicago, IL: University of Chicago Press.
MacDonald, J. M. (1963). The threat to kill. American Journal of Psychiatry, 120, 125-130.
Meehan, J., Flynn, S., Hunt, I. M., Robinson, J., Bickley, H., Parsons, R., . . .Shaw, J. (2006). Perpetrators of homicide with schizophrenia: A national clinical survey in England and Wales. Psychiatric Services, 57, 1648-1651.
Monahan, J, & Appelbaum, P. S. (2000). Reducing violence risk: Diagnostically based clues from the MacArthur Violence Risk Assessment Study. In S. Hodgins (Ed.), Effective prevention of crime and violence among the mentally ill (pp. 19-34). Dordrecht, The Netherlands: Kluwer Academic Publishers.
at NORTHERN ILLINOIS UNIV on September 9, 2014jiv.sagepub.comDownloaded from

Flynn et al. 19
National Centre for Social Research. (2009). Adult psychiatric morbidity in England 2007: Results of a household study. Leicester, UK: University of Leicester. Retrieved from https://catalogue.ic.nhs.uk/publications/mental-health/surveys/adul-psyc-morb-res-hou-sur-eng-2007/adul-psyc-morb-res-hou-sur-eng-2007-rep.pdf
Office for National Statistics. (2013). Statistical bulletin: Crime in England and Wales, year ending September 2012. Retrieved from http://www.ons.gov.uk/ons/rel/crime-stats/crime-statistics/period-ending-sept-2012/stb-crime-in-england-and-wales–year-ending-sept-2012.html
Parliament, UK. (1998) Data Protection Act 1998. Retrieved from http://www.data-protection.manchester.ac.uk/whatisdataprotection/thedataprotectionact/
Planansky, K., & Jihnson, R. (1977). Homicidal aggression in schizophrenic men. Acta Psychiatrica Scandinavica, 55, 65-73.
Rodway, C., Flynn, S., Swinson, N., Roscoe, A., Hunt, I. M., Windfuhr, K., . . .Shaw, J. (2009). Methods of homicide in England and Wales: A comparison by diagnos-tic group. Journal of Forensic Psychiatry & Psychology, 20, 268-305.
Schwartz, R. C., Petersen, S., & Skaggs, J. L. (2001). Predictors of homicidal ide-ation and intent in schizophrenia: An empirical study. American Journal of Orthopsychiatry, 71, 379-384.
Shaw, J., Appleby, J., Amos, T., McDonnell, R., Harris, C., McCann, K., . . .Parsons, R. (1999). Mental disorder and clinical care in people convicted of homicide: National clinical survey. British Medical Journal, 318, 1240-1244.
Silver, E., Felson, R. B., & Vaneseltine, M. (2008). The relationship between mental health problems and violence among criminal offenders. Criminal Justice and Behaviour, 35, 405-426.
Soothill, K., Francis, B., & Liu, J. (2008). Does serious offending lead to homicide? Exploring the interrelationship and sequencing of serious crime. British Journal of Criminology, 48, 522-537.
StataCorp. (2009). Version 11 for Windows. College Station, TX.Steadman, H. J., Mulvey, E. P., Monahan, J., Robbins, P. C., Appelbaum, P. S.,
Grisso, T., . . .Silver, E. (1998). Violence by people discharged from acute psy-chiatric inpatient facilities and by others in the same neighborhoods. Archives of General Psychiatry, 55, 1-9.
Swanson, J. W. (1994). Mental disorder, substance abuse, and community violence: An epidemiologic approach. In J. Monahan & H. J. Steadman (Eds.), Violence and mental disorder: Developments in risk assessment (pp. 101-136). Chicago, IL: University of Chicago Press.
Swinson, N., Flynn, S., Kapur, N., Appleby, L., & Shaw, J. (2010). The use of the Care Programme Approach in perpetrators of homicide. Journal of Forensic Psychiatry and Psychology, 21, 649-659.
Taylor, & Gunn, J. (1984). Violence and psychosis: I. Risk of violence among psy-chotic men. British Medical Journal, 288, 1945-1949.
Teplin, L. A. (1990). The prevalence of severe mental disorder among urban jail detainees: Comparison with the epidemiologic catchment area program. American Journal of Public Health, 80, 663-669.
at NORTHERN ILLINOIS UNIV on September 9, 2014jiv.sagepub.comDownloaded from

20 Journal of Interpersonal Violence XX(X)
Tiihonen, J., Isohanni, M., Rasanen, P., Koiranen, M., & Moring, J. (1997). Specific major mental disorders and criminality: A 26-year prospective study of the 1966 northern Finland birth cohort. American Journal of Psychiatry, 154, 840-845.
Vinkers, D. J., de Beurs, E., Barendregt, M., Rinnie, T., & Hoek, H. W. (2011). The relationship between mental disorders and different types of crime. Criminal Behaviour and Mental Health, 21, 307-320.
Volavka, J., & Swanson, J. (2011). Violent behavior in mental illness: The role of substance abuse. Journal of American Medical Association, 304, 563-564.
Warren, L., Mullen, P. E., & Ogloff, J. R. (2011). A clinical study of those who utter threats to kill. Behavioural Sciences & the Law, 29, 141-154.
Wessely, S. C., Castle, D., Douglas, A. J., & Taylor, P. J. (1994). The criminal careers of incident cases of schizophrenia. Psychological Medicine, 24, 483-502.
Windfuhr, K., While, D., Hunt, I., Turnbull, P., Lowe, R., & Burns, J. . . . National Confidential Inquiry Into Suicide and Homicide by People With Mental Illness. (2008). Suicide in juveniles and adolescents in the United Kingdom. Journal of Child Psychology and Psychiatry, 49, 1155-1165.
World Health Organization. (1992). The ICD 10 classification of mental and behav-ioural disorders: Diagnostic criteria for research. Geneva, Switzerland.
Author Biographies
Sandra Flynn, PhD, is a research fellow currently working for the National Confidential Inquiry Into Suicide and Homicide by People With Mental Illness, Manchester, UK. She has a PhD from the University of Manchester on examining mental illness in perpetrators of homicide followed by suicide. Her research interests include homicide and serious violence by people with mental illness.
Cathryn Rodway, MA, is a research assistant at the National Confidential Inquiry Into Suicide and Homicide by People With Mental Illness, Manchester, UK. Her research interests include homicide, serious violence, and mental health. She has an MA in applied social research from the University of Manchester.
Louis Appleby, MD, FRCPsych, graduated in medicine in Edinburgh and subse-quently trained in both hospital medicine and psychiatry, the latter at the Institute of Psychiatry, London. He has an MD from Edinburgh and is a fellow of the Royal College of Physicians and Royal College of Psychiatrists. He has held research grants totaling £15.5 million from the Wellcome Trust, Medical Research Council, Department of Health, and other National Health Service sources. He leads a group of over 30 researchers in two research centers. The Centre for Suicide Prevention is the largest suicide research unit internationally. Its findings have been the basis of Government policy on suicide prevention. The Centre for Women’s Mental Health Research is one of the leading research centers on maternal mental health, both con-tributing to and evaluating national policy. In 2000, he was seconded (part-time) as the Government’s National Director for Mental Health to lead a national program of reform in mental health care, and in 2010, National Clinical Director for Health and Criminal Justice. He leads the National Suicide Prevention Strategy for England.
at NORTHERN ILLINOIS UNIV on September 9, 2014jiv.sagepub.comDownloaded from

Flynn et al. 21
Jenny Shaw, PhD, FRCPsych, is a professor of forensic psychiatry at the University of Manchester, and a consultant forensic psychiatrist at Guild Lodge Medium Secure Unit, Preston, UK. She is the assistant director of the National Confidential Inquiry Into Suicide and Homicide by People With Mental Illness. Her research interests include homicide, suicide, prison health research, and the criminal justice system.
at NORTHERN ILLINOIS UNIV on September 9, 2014jiv.sagepub.comDownloaded from