Embed Size (px)
Citation preview
825
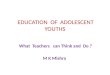
Changes in blood-lignocaine and ventricular ectopic beats withtime in 9 patients with acute myocardial infarction.
tients at least 15 min before treatment, and for 4 h thereafter
using ’Medilog’ miniature cassette recorders. The tapes werereplayed through an Oxford Instruments analyser, and dis-played on a 50 cm oscilloscope. Ventricular ectopics (V.E.B.S.)were detected by-visual inspection and printed on paper forcounting. Numbers were expressed as the total (i.e., for all
patients) for 15 min before treatment, and for each subsequent15 min period.
Results
The blood-levels are shown in the accompanyingtable. The figure shows changes in blood-levels withtime with corresponding numbers of v.E.B.s. A minimumplasma level of 2 0, µg/ml was achieved in each patient1 min after treatment, and was maintained for 60 minin all cases, and for 120 min in seven. The mean plasmalevel peaked at 1 min after injection at 6.3 µg/ml. Alater peak occurred at 10 min at 5.68 µg/ml., and themean level gradually fell thereafter to 2.5 µg/ml at 2 h,and 1.5 µg/ml at 4 h. Side-effects occurred in three pa-tients. One patient complained of dizziness and vomited15 min after treatment. One further patient complainedof dizziness, and a third patient complained of tinnitus.No adverse effect on heart-rate, blood-pressure, or atrio-ventricular conduction was noted.
The effect of lignocaine on the occurrence-rate ofV.E.B.S is also shown in the accompanying figure.Although the numbers of v.E.B.s in these patients wasrelatively low before treatment, a marked antiarryhth-mic effect was observed in the first 15 min after treat-ment. This was maintained for 90’min after which therewas a gradual return to pretreatment levels at 1 h. Thenumber of V.E.B.S present at 3 h was half that of the con-trol period.
Discussion
A rapid onset of effect after antiarrhythmic therapy isdesirable particularly in the early stage of acute myocar-dial infarction. The regimen used in the present studyprovided therapeutic plasma levels within 1 min of treat-ment, and maximum antiarrhythmic effect was observedduring the first 15 min period after it. After an initialpeak observed at 1 min after treatment, a delayed peakappeared at 10 min. This is the result of the intramuscu-lar injection, the timing of the peak being similar to thatin other studies when the injection was given into thedeltoid muscle. II 10 Intramuscular injection of lignocaineat other sites results in a longer delay before the appear-ance of peak plasma activity.9 10
The duration of maximum antiarrhythmic effect wasapproximately 90 min. Significant antiarrhythmiceffect, however, remained at 3 h. The latter was associ-ated with a mean plasma level of 1.7 µg/ml. It is impor-tant that the antiarrhythmic effect of prophylactic treat-ment should be of sufficient duration to cover a patientbefore admission to hospital. The present regimenappears to satisfy this requirement adequately. It alsoseems to us to be of potential value in the prevention ofventricular arrhythmias outside hospital. Furthermore,if combined with an oral antiarrhythmic drug such asmexiletine or disopyramide it might well form the basisof a prophylactic regimen which could be continued overthe first 2 days and would be suitable for use in generalpractice as well as in hospital.We are grateful to Mr D. B. Henderson who did the lignocaine
assays.
Requests for reprints should be addressed to D.G.J., Department ofCardiology, Newcastle General Hospital, Westgate Road, Newcastleupon Tyne NE4 6BE.
REFERENCES
1. Fulton, M., Julian, D. G., Oliver, M. F. Circulation, 1969, 40, suppl. 4, 182.2. Lown, B., Rubetman, W. Mod. Concepts cardiovasc. Dis. 1970, 39, 97.3. Mogensen, L. Acta med. Scand. 1970, 188, suppl. p. 513.4. Lie, K. I., Wellens, H. J., Van Capelle, F. J., Durrer, D. New Engl. J. Med.
1974, 291, 1324.5. Valentine, P. A., Frew, J. L., Mashford, M. L., Sloman, J. G. ibid. p. 1327.6. Scott, D. B., Jebson, P. J., Vellani, C. W., Julian, D. G. Lancet, 1968, n,
1209.7. Fehmers, M. C. O., Dunning, A. J. Am.J. Cardiol. 1972, 29, 514.8. Keenaghan, J. B. Anesthesiology, 1968, 26, 110.9. Meyer, M. B., Zelechowski, K. in Lidocaine in the Treatment of Ventricular
Arrhythmias (edited by D. B. Scott and D. G. Julian); p. 161. Edinburgh,1971.
10. Zener, J. C., Kerber, R. E., Spivack, A. P., Harrison, D. C. Circulation,1973, 47, 984.
SERUM-25-HYDROXYVITAMIN-DCONCENTRATIONS IN ADOLESCENT BOYS
GRAHAM ELLIS* J. S. WOODHEADW. T. COOKE
Nutritional and Intestinal Unit, General Hospital,Birmingham B4 6NH, and Department of Medical
Biochemistry, Welsh National School of Medicine, HeathPark, Cardiff CF4 4XN
* Present address: Department of Clinical Biochemistry, Hospital for Sick
Children, 555 University Avenue, Toronto, Ontario, Canada.
Summary In March, 1976, vitamin-D status wasinvestigated in 256 thirteen-year-old
school boys of Asian, West Indian, and European originin Birmingham. Serum-25-hydroxyvitamin-D3(25-OHD3) concentrations in 78% of the 124 Asian boysresembled those found in rickets and osteomalacia. Ser-
um-25-OHD3 concentrations were also low in a fewWest Indian and European children. Dietary intake ofvitamin D and exposure to sunlight were similar in eachgroup. Serum-parathormone concentrations were in-creased in many children with low serum-25-OHD3. Re-investigation in October, 1976, of a group of childrenwhose serum-25-OHD, concentration had been less than8 µg/l in March, 1976, showed pronounced improve-ment in all, but some still had concentrations which in-dicated a possible deficiency. It is suggested that the high
826
frequency of vitamin-D deficiency in Asian adolescentswould be much reduced if 1 mg of vitamin D3 was givenorally each school term during adolesence.
Introduction
THE incidence of rickets among immigrant schoolchildren is causing concern.1-s The continued referral ofschoolchildren with rickets to our unit over the past twoyears despite considerable local publicity about the con7dition and the means of preventing it, led us to re-ex-amine serum-25-hydroxyvitamin-D (25-OHD3) andother biochemical indices in schoolchildren.
Subjects and Methods
Schoolboys
Written consent was obtained from parents to examine andtake blood samples from boys of about thirteen years of ageattending 3 Birmingham schools (A, B and C). Schools B andC had been surveyed three years before.23 256 boys were in-vestigated, approximately 70% of those available in that agegroup in the three schools. There were 124 Asians, 67 West In-dians, and 65 Europeans, of whom 34 Asians, 65 West Indians,and 57 Europeans were born in the U.K. All were weighed andtheir heights measured. Permission was obtained to X-ray thewrists of 111 boys examined in school A. All were asked abouttheir intake of butter, margarine, cod liver oil, vitamin tablets,meat, and school meals. Dietary histories were taken from 130randomly selected boys, and vitamin D intake was estimatedby means of the tables of McCance and Widdowson. Venousblood was taken during February and March, 1976, for theestimation of serum calcium, total protein, albumin, and phos-phate by standard autoanalyser techniques, and 25-OHD3 bymethod of Ellis and Dixon. 10
Alkaline phosphatase was measured by the King-Armstrongmethod" and by an autoanalyser technique with magnesiumions as an activator.1-3 The values presented are those of themanual method. Also full blood-counts were obtained with theCoulter counter and serum folic acid (Lactobacillus casei) andvitamin B12 (Lactobacillus leischmann) were measured micro-biologically.
Serum-parathyroid-hormone (parathormone) (P.T.H.) was
measured in 119 Asian boys and in randomly selected groupsof 28 West Indian and 27 European boys by an immunoradio-metric assay’2 with a guineapig antiserum (M.R.C. 71/69)raised against bovine parathormone. Samples were assayedagainst a partially purified preparation of human P.T.H. pro-vided by Dr J. L. O’Riordan.13
Blood was taken in October, 1976, from 54 boys (34 Asians,6 Europeans, 14 West Indians) of school A whose initial ser-um-25-OHD3 concentrations had been less than 8 µg/l. Thesesamples were analysed for 25-OHD3, calcium, albumin, andalkaline phosphatase. Serum-p.T.H. was measured in samplesfrom 3 boys who had had serum concentrations above 1.0 µg/lin March.
Controls
The following groups were used as controls:Group 1.—73 English blood-donors (41 men, 32 women).
Blood-samples were taken in March, 1976.Group 2.-20 Asian professional hospital staff aged nine-
teen to forty-two of whom 1 was a vegetarian. All except 1came from India and had lived in the U.K. for twelve weeksto eight years. Blood-samples were taken between March andAugust, 1976. 5 also volunteered to take 1 mg vitamin D3orally on a single occasion and blood-samples were taken at in-tervals afterwards.
Group 3.—15 patients over sixty-five years, attending withminor orthopaedic conditions in late September and October,1976.
Group 4.-7 Asian children with rickets aged fourteen tosixteen years (6 blood-samples taken January to April) and 23adults with osteomalacia (10 Asian) aged nineteen to eighty-three (11 blood-samples taken during June to October). Thediagnoses had been established by bone biopsy or radiology.
Results
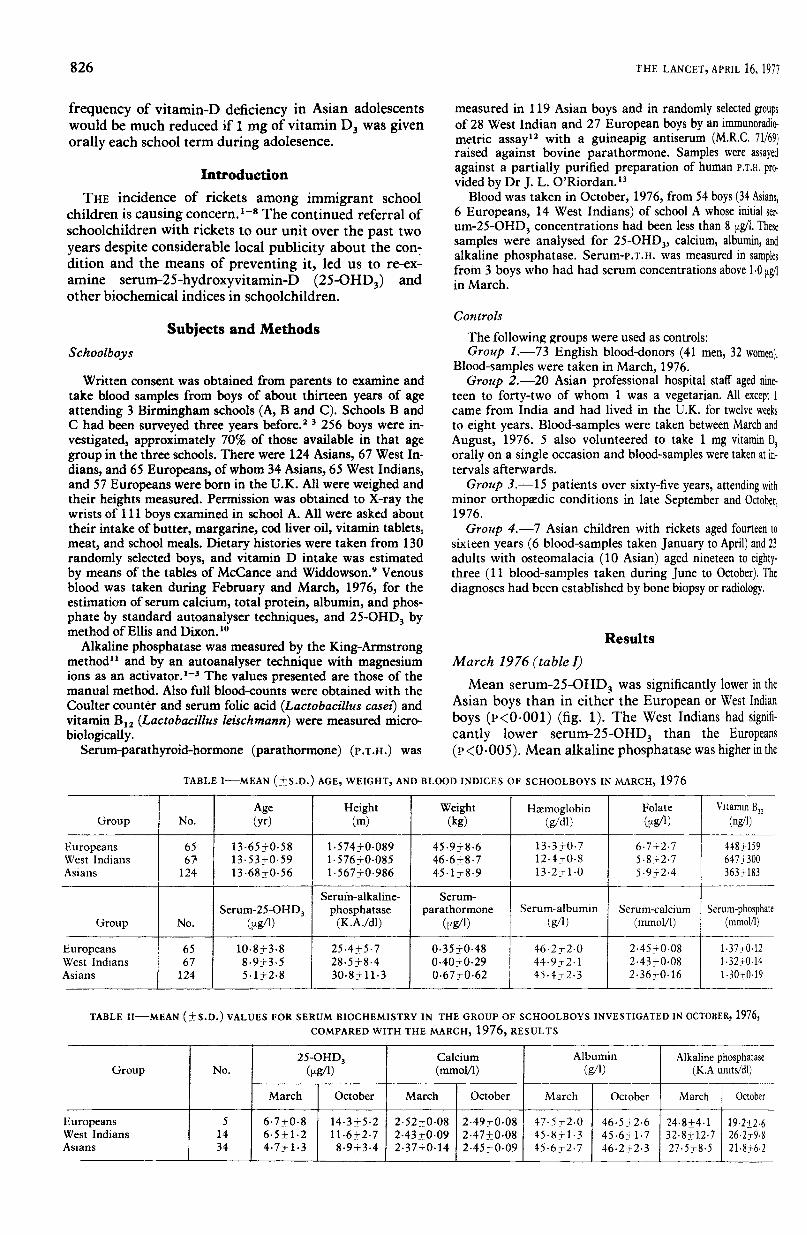
March 1976 (table I)Mean serum-25-OHD3 was significantly lower in the
Asian boys than in either the European or West Indianboys (r<0.001) (fig. 1). The West Indians had signifi-cantly lower serum-25-OHD3 than the Europeans(P<0.005). Mean alkaline phosphatase was higher in the
TABLE I—MEAN (±S.D.) AGE, WEIGHT, AND BLOOD INDICES OF SCHOOLBOYS IN MARCH, 1976
TABLE II—MEAN (±S.D.) VALUES FOR SERUM BIOCHEMISTRY IN THE GROUP OF SCHOOLBOYS INVESTIGATED IN OCTOBER, 1976,COMPARED WITH THE MARCH, 1976, RESULTS
827
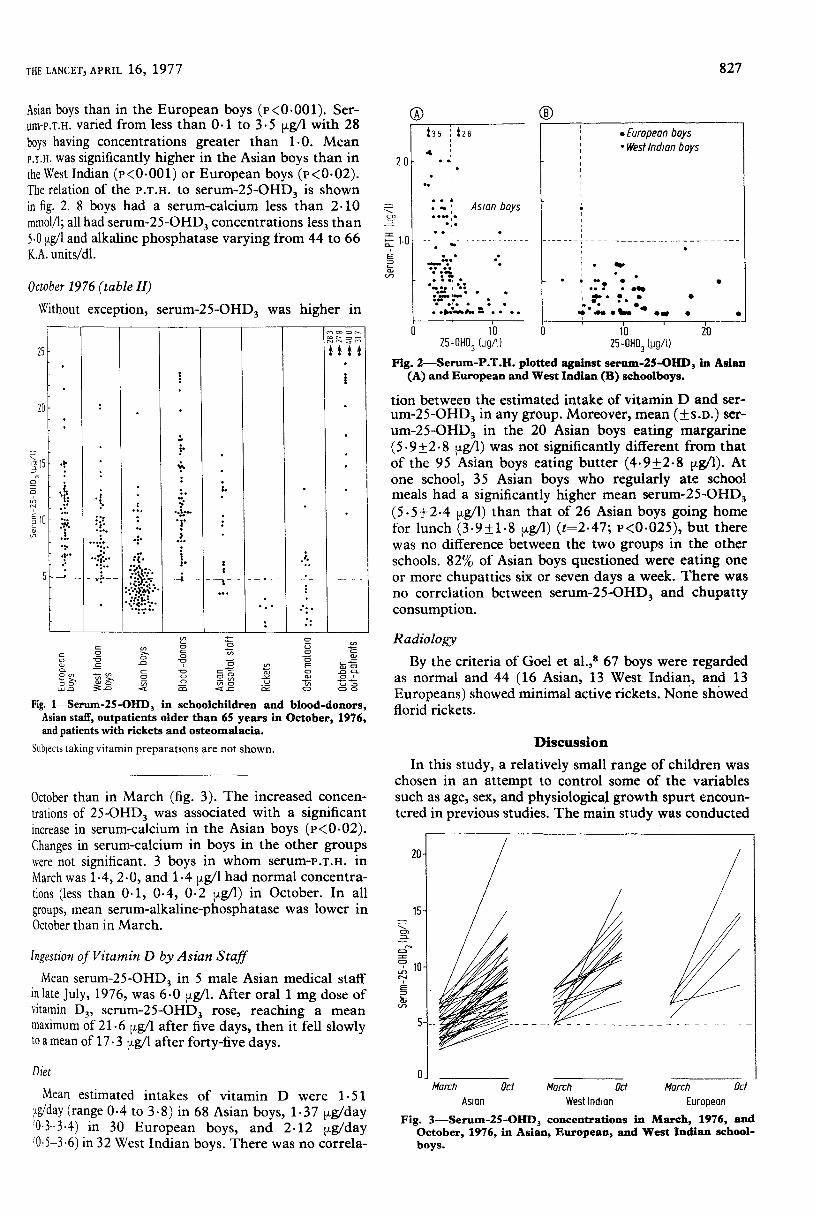
Asian boys than in the European boys (P<0-001). Ser-um-P.T.H. varied from less than 0.1 to 3.5 µg/l with 28boys having concentrations greater than 1.0. MeanP.T.H. was significantly higher in the Asian boys than inthe West Indian (P<0.001) or European boys (P<0.02).The relation of the P.T.H. to serum-25-OHD3 is shownin fig. 2. 8 boys had a serum-calcium less than 2.10mmol/l; all had serum-25-OHD3 concentrations less than5.0 µg/l and alkaline phosphatase varying from 44 to 66K.A. units/dl.
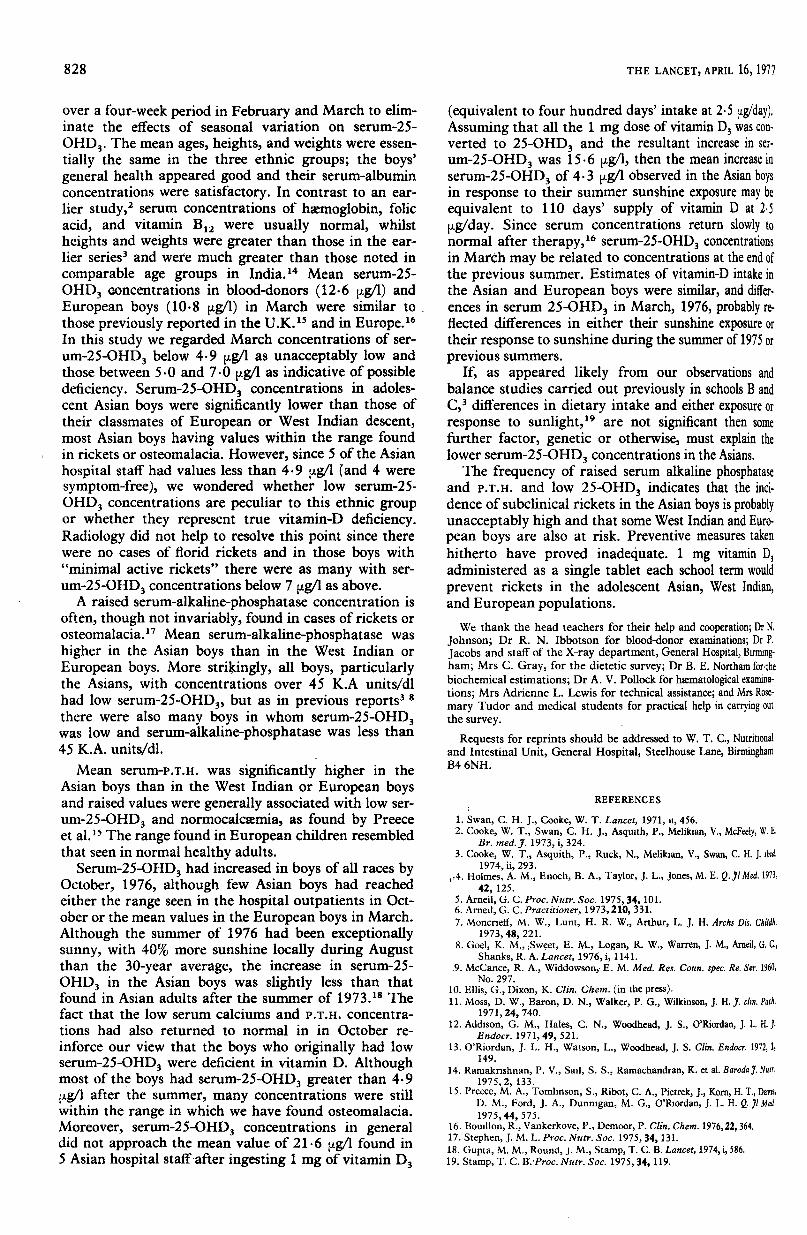
October 1976 (table II)Without exception, serum-25-OHD3 was higher in
Fig. 1—Serum-25-OHD3 in schoolchildren and blood-donors,Asian staff, outpatients older than 65 years in October, 1976,and patients with rickets and osteomalacia.
Subjects taking vitamin preparations are not shown.
October than in March (fig. 3). The increased concen-trations of 25-OHD3 was associated with a significantincrease in serum-calcium in the Asian boys (P<0.02).Changes in serum-calcium in boys in the other groupswere not significant. 3 boys in whom serum-P.T.H. inMarch was 1-4, 2-0, and 1 4 µg/l had normal concentra-tions (less than 0-1, 0.4, 0.2 µg/l) in October. In all
groups, mean serum-alkaline-phosphatase was lower inOctober than in March.
Ingestion of Vitamin D by Asian StaffMean serum-25-OHD3 in 5 male Asian medical staff
in late July, 1976, was 6-0 µg/l. After oral 1 mg dose ofvitamin D3, serum-25-OHD3 rose, reaching a mean
maximum of 21.6 µg/l after five days, then it fell slowlyto a mean of 17.3 µg/l after forty-five days.
Diet
Mean estimated intakes of vitamin D were 1-51 1
g/day (range 0.4 to 3-8) in 68 Asian boys, 1-37 µg/day(0.3-3.4) in 30 European boys, and 2.12 µg/day0.5-3.6) in 32 West Indian boys. There was no correla-
Fig. 2-Serum-P.T.H. plotted against serum-25-OHD3 in Asian(A) and European and West Indian (B) schoolboys.
tion between the estimated intake of vitamin D and ser-
um-25-OHD3 in any group. Moreover, mean (±S.D.) ser-um-25-OHD3 in the 20 Asian boys eating margarine(5.9±2.8 jjt.g/1) was not significantly different from thatof the 95 Asian boys eating butter (49±28 µg/l). Atone school, 35 Asian boys who regularly ate schoolmeals had a significantly higher mean serum-25-OHD3(3.3±2.4 µg/l) than that of 26 Asian boys going homefor lunch (39±18 µg/l) (t=2.47; P<0.025), but therewas no difference between the two groups in the otherschools. 82% of Asian boys questioned were eating oneor more chupatties six or seven days a week. There wasno correlation between serum-25-OHD3 and chupattyconsumption.
Radiology
By the criteria of Goel et al.,s 67 boys were regardedas normal and 44 (16 Asian, 13 West Indian, and 13Europeans) showed minimal active rickets. None showedflorid rickets.
Discussion
In this study, a relatively small range of children waschosen in an attempt to control some of the variablessuch as age, sex, and physiological growth spurt encoun-tered in previous studies. The main study was conducted
Fig. 3—Serum-25-OHD3 concentrations in March, 1976, andOctober, 1976, in Asian, European, and West Indian school-boys.
828
over a four-week period in February and March to elim-inate the effects of seasonal variation on serum-25-
OHD3. The mean ages, heights, and weights were essen-tially the same in the three ethnic groups; the boys’general health appeared good and their serum-albuminconcentrations were satisfactory. In contrast to an ear-lier study,2 serum concentrations of haemoglobin, folicacid, and vitamin B12 were usually normal, whilst
heights and weights were greater than those in the ear-lier series3 and were much greater than those noted incomparable age groups in India.14 Mean serum-25-
OHD3 concentrations in blood-donors (12.6 µg/l) andEuropean boys (10-8 µg/l) in March were similar to .
those previously reported in the U.K.15 and in Europe. 16In this study we regarded March concentrations of ser-um-25-OHD3 below 4-9 µg/l as unacceptably low andthose between 5.0 and 7.0 µg/l as indicative of possibledeficiency. Serum-25-OHD3 concentrations in adoles-cent Asian boys were significantly lower than those oftheir classmates of European or West Indian descent,most Asian boys having values within the range foundin rickets or osteomalacia. However, since 5 of the Asianhospital staff had values less than 4-9 µg/l (and 4 weresymptom-free), we wondered whether low serum-25-OHD3 concentrations are peculiar to this ethnic groupor whether they represent true vitamin-D deficiency.Radiology did not help to resolve this point since therewere no cases of florid rickets and in those boys with"minimal active rickets" there were as many with ser-
um-25-OHD3 concentrations below 7 µg/l as above.A raised serum-alkaline-phosphatase concentration is
often, though not invariably, found in cases of rickets orosteomalacia.17 Mean serum-alkaline-phosphatase washigher in the Asian boys than in the West Indian orEuropean boys. More strikingly, all boys, particularlythe Asians, with concentrations over 45 K.A units/dlhad low serum-25-OHD3, but as in previous reports3 8there were also many boys in whom serum-25-OHD3was low and serum-alkaline-phosphatase was less than45 K.A. units/dl.
Mean serum-P.T.H. was significantly higher in theAsian boys than in the West Indian or European boysand raised values were generally associated with low ser-um-25-OHD3 and normocalcaemia, as found by Preeceet al. 15 The range found in European children resembledthat seen in normal healthy adults.Serum-25-OHD3 had increased in boys of all races by
October, 1976, although few Asian boys had reachedeither the range seen in the hospital outpatients in Oct-ober or the mean values in the European boys in March.Although the summer of 1976 had been exceptionallysunny, with 40% more sunshine locally during Augustthan the 30-year average, the increase in serum-25-OHD3 in the Asian boys was slightly less than thatfound in Asian adults after the summer of 1973.18 Thefact that the low serum calciums and P.T.H. concentra-tions had also returned to normal in in October re-
inforce our view that the boys who originally had lowserum-25-OHD3 were deficient in vitamin D. Althoughmost of the boys had serum-25-OHD3 greater than 4-9jjt.g/1 after the summer, many concentrations were stillwithin the range in which we have found osteomalacia.Moreover, serum-25-OHD3 concentrations in generaldid not approach the mean value of 21.6 µg/l found in5 Asian hospital staff after ingesting 1 mg of vitamin D3
(equivalent to four hundred days’ intake at 2.5 µg/day).Assuming that all the 1 mg dose of vitamin D3 was con-verted to 25-OHD3 and the resultant increase in ser-
um-25-OHD3 was 15-6 µg/l, then the mean increase inserum-25-OHD3 of 4.3 µg/l observed in the Asian boysin response to their summer sunshine exposure may be
equivalent to 110 days’ supply of vitamin D at 2.5
µg/day. Since serum concentrations return slowly to
normal after therapy, 16 serum-25-OHD3 concentrationsin March may be related to concentrations at the end ofthe previous summer. Estimates of vitamin-D intake inthe Asian and European boys were similar, and differ-ences in serum 25-OHD3 in March, 1976, probably re-flected differences in either their sunshine exposure ortheir response to sunshine during the summer of 1975 orprevious summers.
If, as appeared likely from our observations andbalance studies carried out previously in schools B andC,3 differences in dietary intake and either exposure orresponse to sunlight,t9 are not significant then somefurther factor, genetic or otherwise, must explain thelower serum-25-OHD3 concentrations in the Asians.The frequency of raised serum alkaline phosphatase
and P.T.H. and low 25-OHD3 indicates that the inci-dence of subclinical rickets in the Asian boys is probablyunacceptably high and that some West Indian and Euro-pean boys are also at risk. Preventive measures takenhitherto have proved inadequate. 1 mg vitamin DJadministered as a single tablet each school term wouldprevent rickets in the adolescent Asian, West Indian,and European populations.We thank the head teachers for their help and cooperation; Dr N.
Johnson; Dr R. N. Ibbotson for blood-donor examinations; Dr P.Jacobs and staff of the X-ray department, General Hospital, Bmnmg-ham ; Mrs C. Gray, for the dietetic survey; Dr B. E. Northam for’thebiochemical estimations; Dr A. V. Pollock for htematological examina-tions ; Mrs Adrienne L. Lewis for technical assistance; and Mrs Rose-mary Tudor and medical students for practical help in carrying outthe survey. -
Requests for reprints should be addressed to W. T. C., Nutritionaland Intestinal Unit, General Hospital, Steelhouse Lane, BirminghamB4 6NH.
REFERENCES
1. Swan, C. H. J., Cooke, W. T. Lancet, 1971, ii, 456.2. Cooke, W. T., Swan, C. H. J., Asquith, P., Melikian, V., McFeely, W. E.
Br. med. J. 1973, i, 324.3. Cooke, W. T., Asquith, P., Ruck, N., Melikian, V., Swan, C. H. J. ibid.
1974, ii, 293.4. Holmes, A. M., Enoch, B. A., Taylor, J. L., Jones, M. E. Q.Jl Med. 1973,
42, 125.5. Arneil, G. C. Proc. Nutr. Soc. 1975, 34, 101.6. Arneil, G. C. Practitioner, 1973, 210, 331.7. Moncrieff, M. W., Lunt, H. R. W., Arthur, L. J. H. Archs Dis. Childh.
1973, 48, 221.8. Goel, K. M., Sweet, E. M., Logan, R. W., Warren, J. M., Arneil, G. C.,
Shanks, R. A. Lancet, 1976, i, 1141..9. McCance, R. A., Widdowson, E. M. Med. Res. Coun. spec. Re. Ser. 1960,
No. 297.10. Ellis, G., Dixon, K. Clin. Chem. (in the press).11. Moss, D. W., Baron, D. N., Walker, P. G., Wilkinson, J. H. J. clin. Path.
1971, 24, 740.12. Addison, G. M., Hales, C. N., Woodhead, J. S., O’Riordan, J. L. H. J.
Endocr. 1971, 49, 521.13. O’Riordan, J. L. H., Watson, L., Woodhead, J. S. Clin. Endocr. 1972,1,
149.14. Ramakrishnan, P. V., Sail, S. S., Ramachandran, K. et al. Baroda J. Nutr.
1975, 2, 133.15. Preece, M. A., Tomlinson, S., Ribot, C. A., Pietrek, J., Korn, H. T., Davis,
D. M., Ford, J. A., Dunnigan, M. G., O’Riordan, J. L. H. Q. Jl Med1975, 44, 575.
16. Bouillon, R., Vankerkove, P., Demoor, P. Clin. Chem. 1976, 22, 364.17. Stephen, J. M. L. Proc. Nutr. Soc. 1975, 34, 131.18. Gupta, M. M., Round, J. M., Stamp, T. C. B. Lancet, 1974, i, 586.19. Stamp, T. C. B. Proc. Nutr. Soc. 1975, 34, 119.






![eprints.whiterose.ac.ukeprints.whiterose.ac.uk/151893/9/Zhang... · Web view[9] Targher G, Bertolini L, Scala L et al. Associations between serum 25-hydroxyvitamin D3 concentrations](https://img.pdfslide.net/doc/110x75/5ec0ca15456e3f18ae1c2b9d/web-view-9-targher-g-bertolini-l-scala-l-et-al-associations-between-serum-25-hydroxyvitamin.jpg)