Embed Size (px)
Citation preview
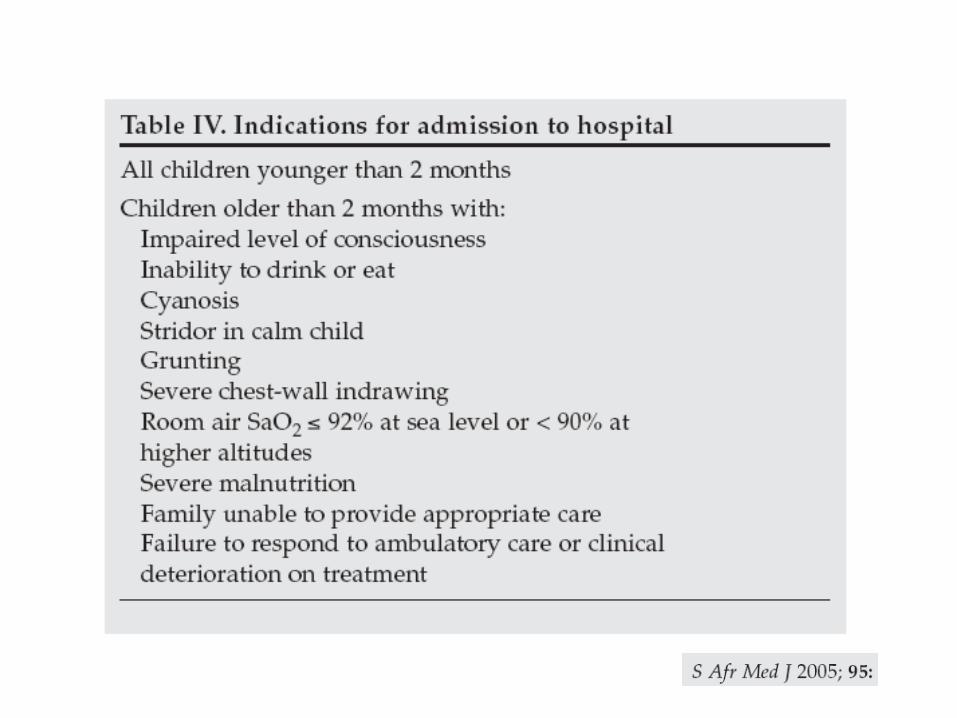
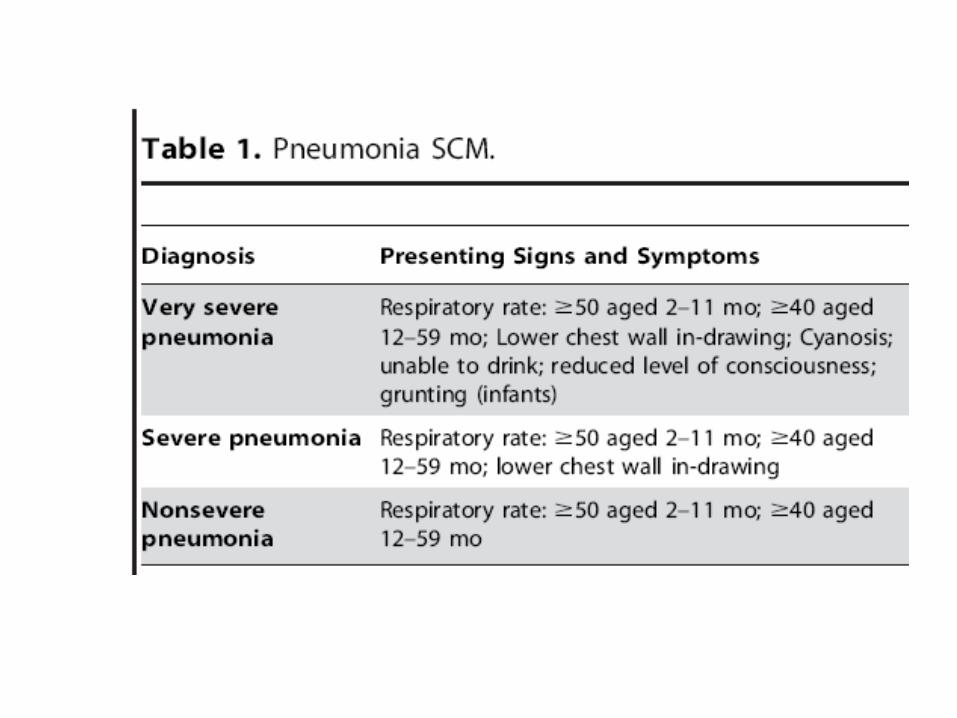
Severe pneumonia in childhood.
Robert GieDepartment Paediatrics and Child
HealthStellenbosch University.
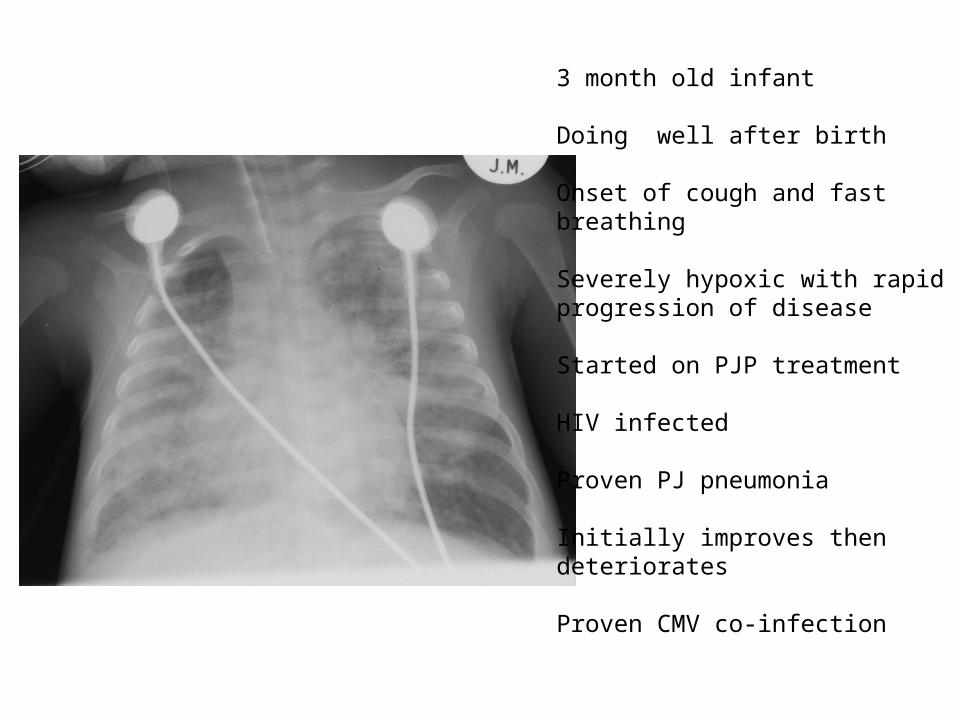
3 month old infant
Doing well after birth
Onset of cough and fast breathing
Severely hypoxic with rapid progression of disease
Started on PJP treatment
HIV infected
Proven PJ pneumonia
Initially improves then deteriorates
Proven CMV co-infection

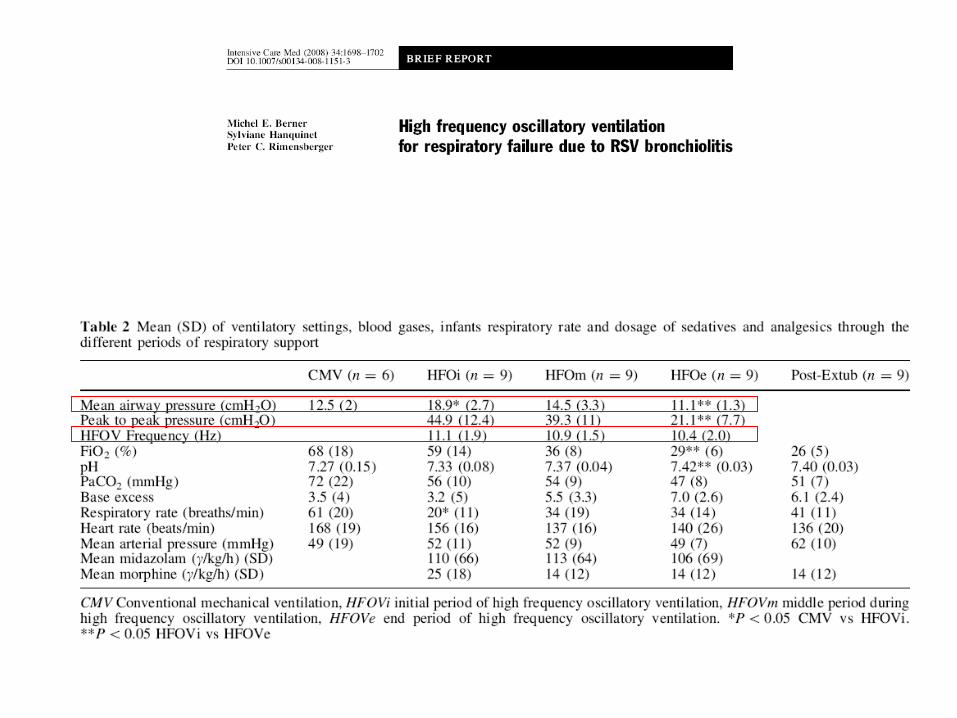
2 month old ex-premature
Presented with cough and progessive respiratory distress
Required ventilatory support Due to hypercarbia
Culture proven PTB.
Source case CXR:

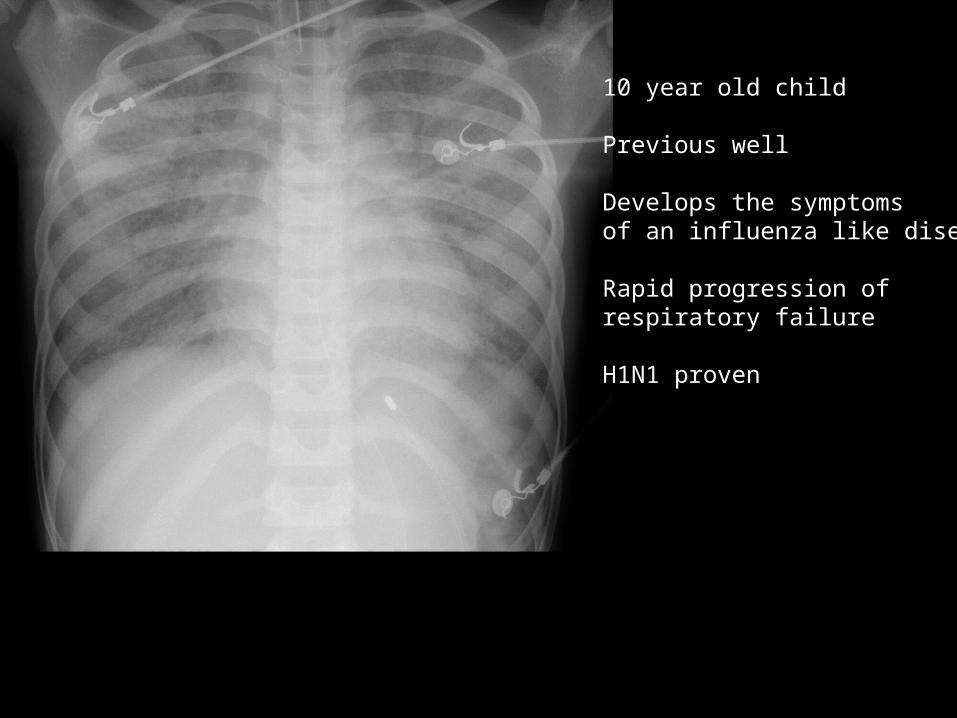
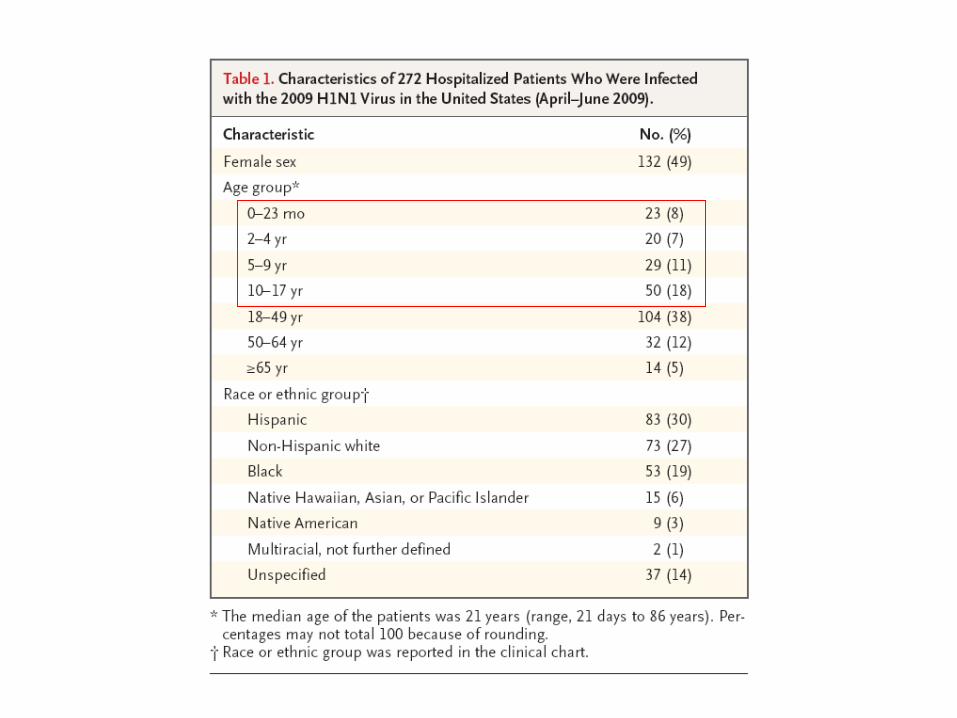
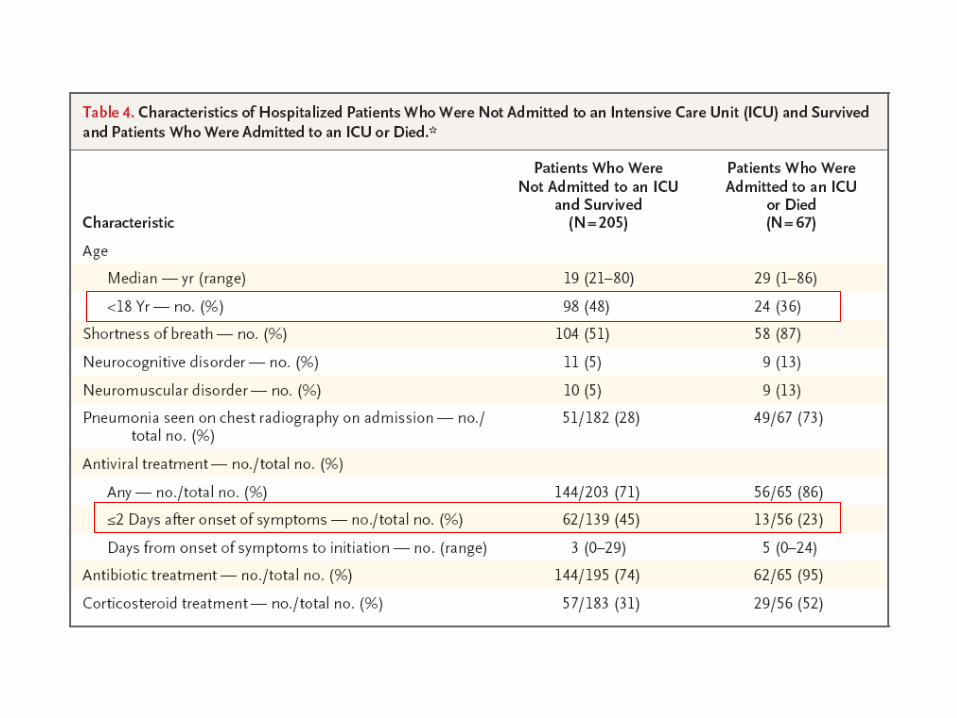
10 year old child
Previous well
Develops the symptoms of an influenza like disease
Rapid progression of respiratory failure
H1N1 proven
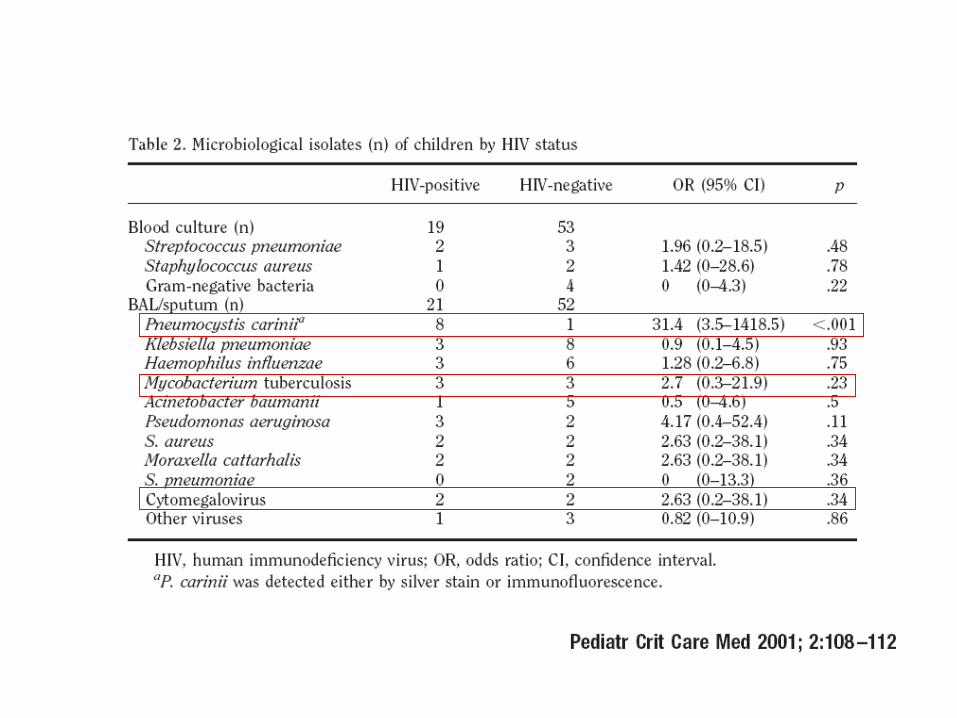
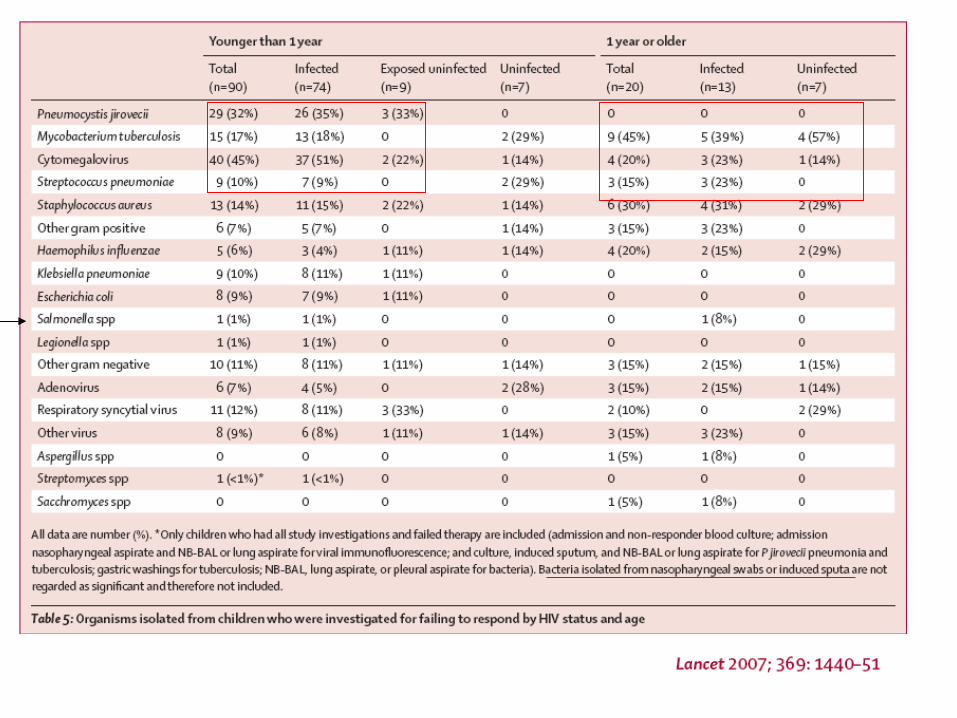
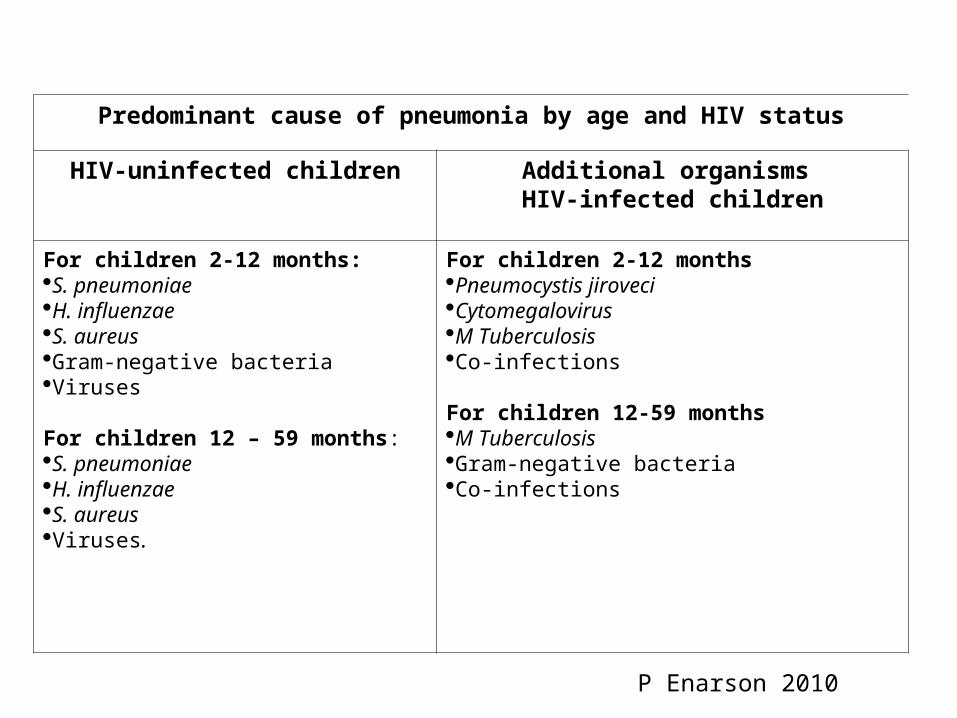
Predominant cause of pneumonia by age and HIV status
HIV-uninfected children Additional organisms HIV-infected children
For children 2-12 months: S. pneumoniae H. influenzae S. aureusGram-negative bacteria Viruses
For children 12 – 59 months: S. pneumoniae H. influenzae S. aureusViruses.
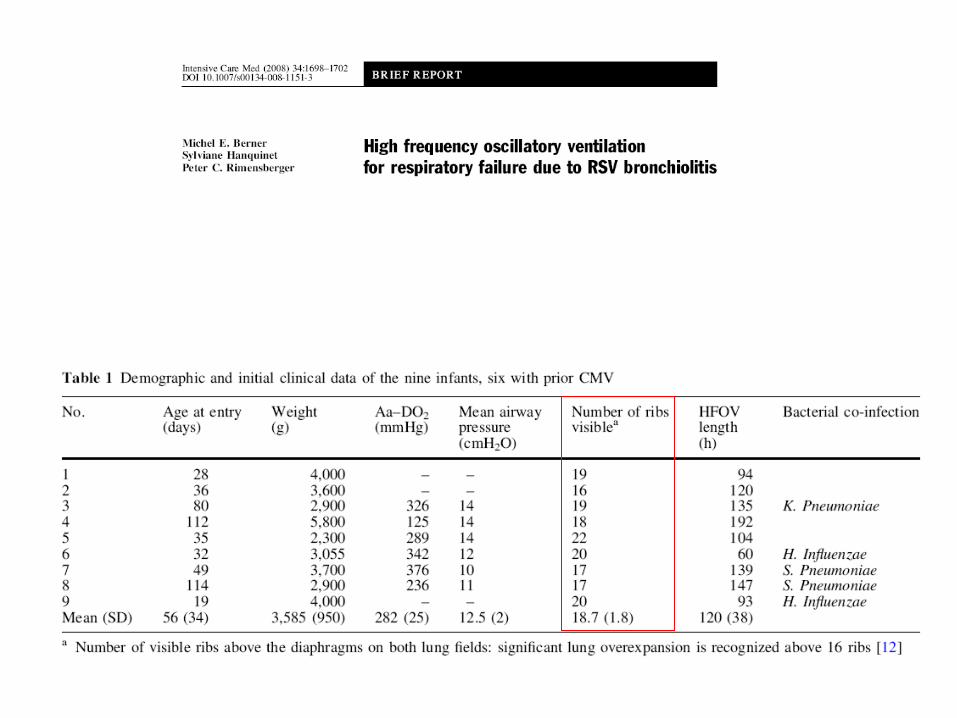
For children 2-12 monthsPneumocystis jiroveciCytomegalovirusM TuberculosisCo-infections
For children 12-59 monthsM TuberculosisGram-negative bacteria Co-infections
P Enarson 2010
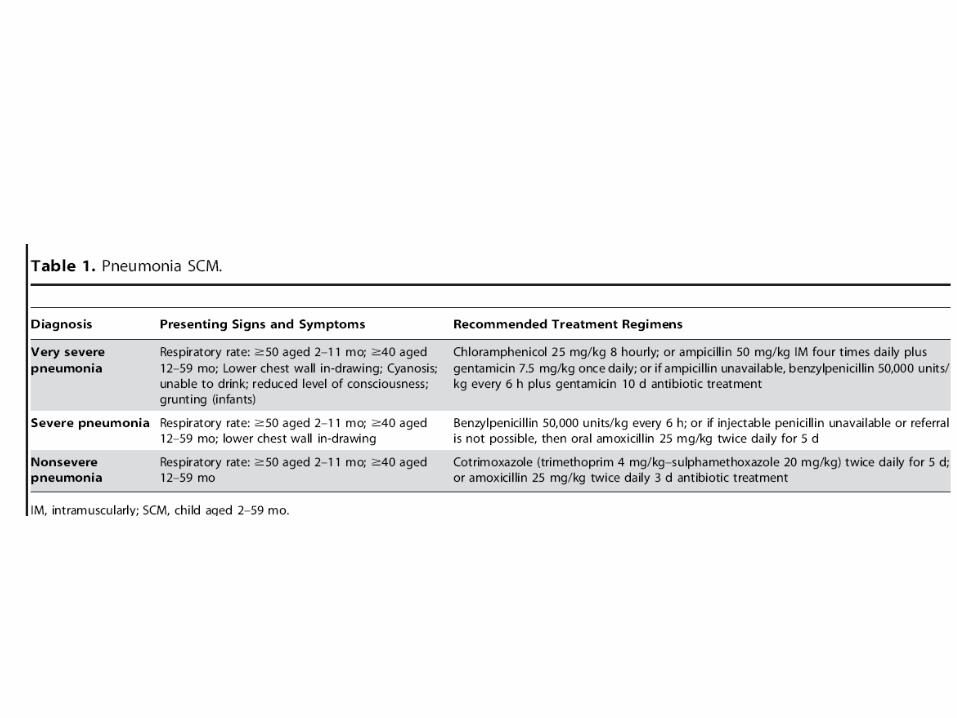
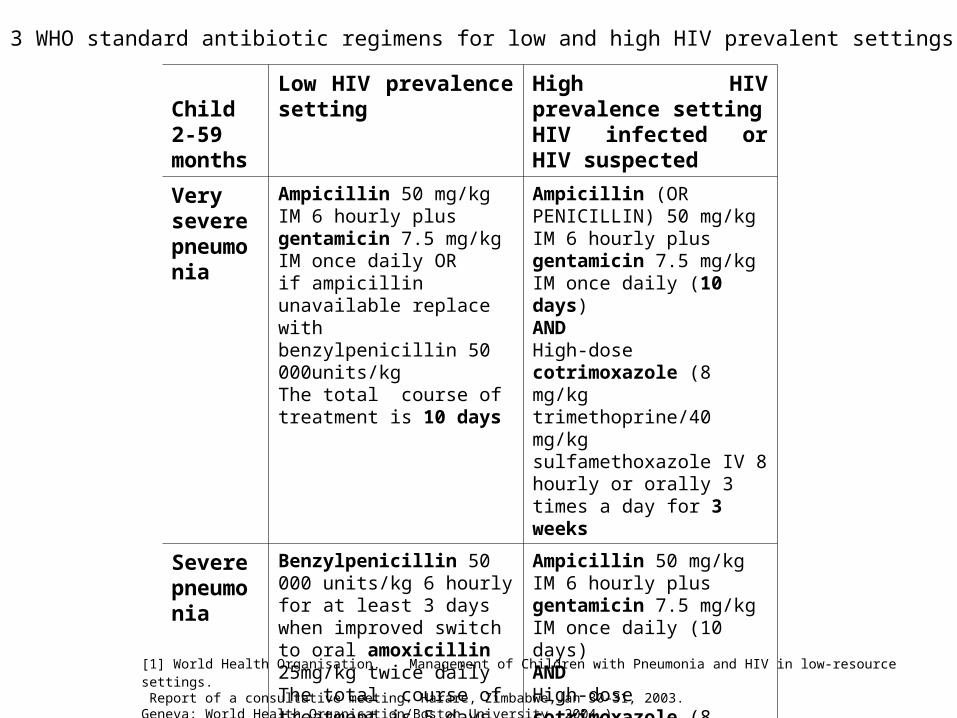
Table 3 WHO standard antibiotic regimens for low and high HIV prevalent settings
Child 2-59 months
Low HIV prevalence setting
High HIV prevalence settingHIV infected or HIV suspected
Very severe pneumonia
Ampicillin 50 mg/kg IM 6 hourly plus gentamicin 7.5 mg/kg IM once daily ORif ampicillin unavailable replace with benzylpenicillin 50 000units/kg The total course of treatment is 10 days
Ampicillin (OR PENICILLIN) 50 mg/kg IM 6 hourly plus gentamicin 7.5 mg/kg IM once daily (10 days) ANDHigh-dose cotrimoxazole (8 mg/kg trimethoprine/40 mg/kg sulfamethoxazole IV 8 hourly or orally 3 times a day for 3 weeks
Severe pneumonia
Benzylpenicillin 50 000 units/kg 6 hourly for at least 3 days when improved switch to oral amoxicillin 25mg/kg twice daily The total course of treatment is 5 days
Ampicillin 50 mg/kg IM 6 hourly plus gentamicin 7.5 mg/kg IM once daily (10 days) ANDHigh-dose cotrimoxazole (8 mg/kg trimethoprine/40 mg/kg sulfamethoxazole) IV 8 hourly or orally 3 times a day for 3 weeks
[1] World Health Organisation. Management of Children with Pneumonia and HIV in low-resource settings. Report of a consultative meeting. Harare, Zimbabwe,Jan 30–31, 2003. Geneva: World Health Organisation/Boston University, 2004.)
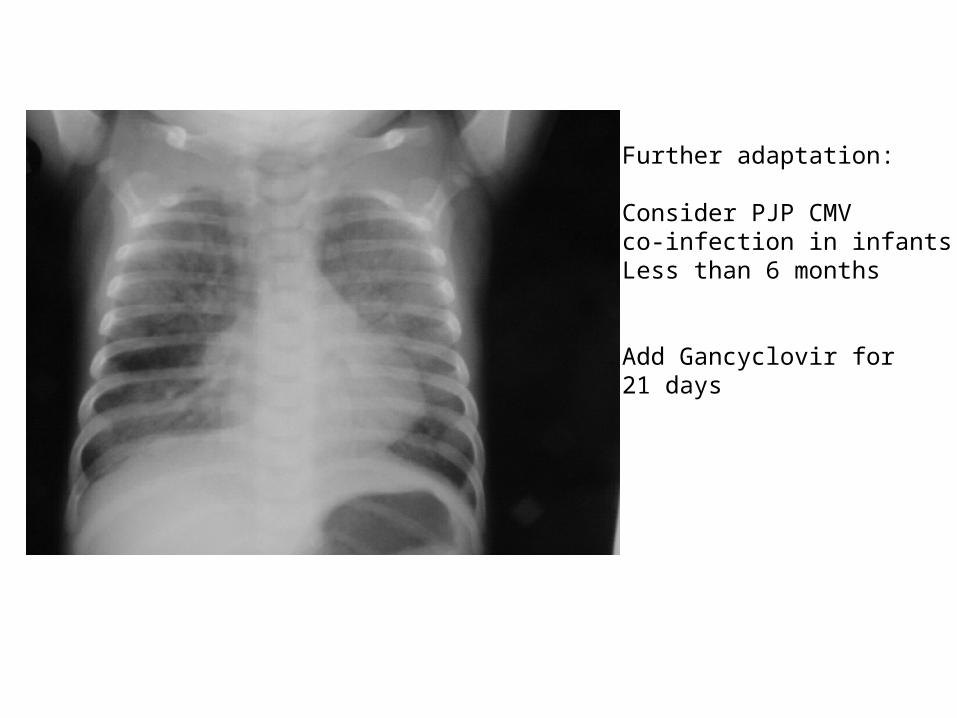
Further adaptation:
Consider PJP CMV co-infection in infantsLess than 6 months
Add Gancyclovir for 21 days
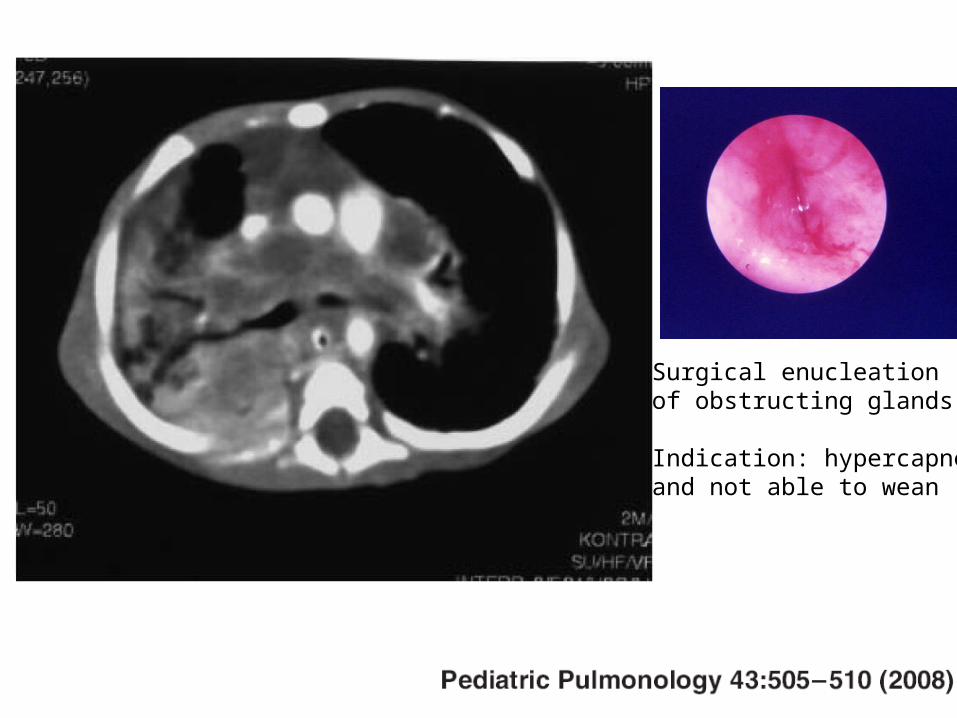
Surgical enucleation of obstructing glands.
Indication: hypercapnea and not able to wean
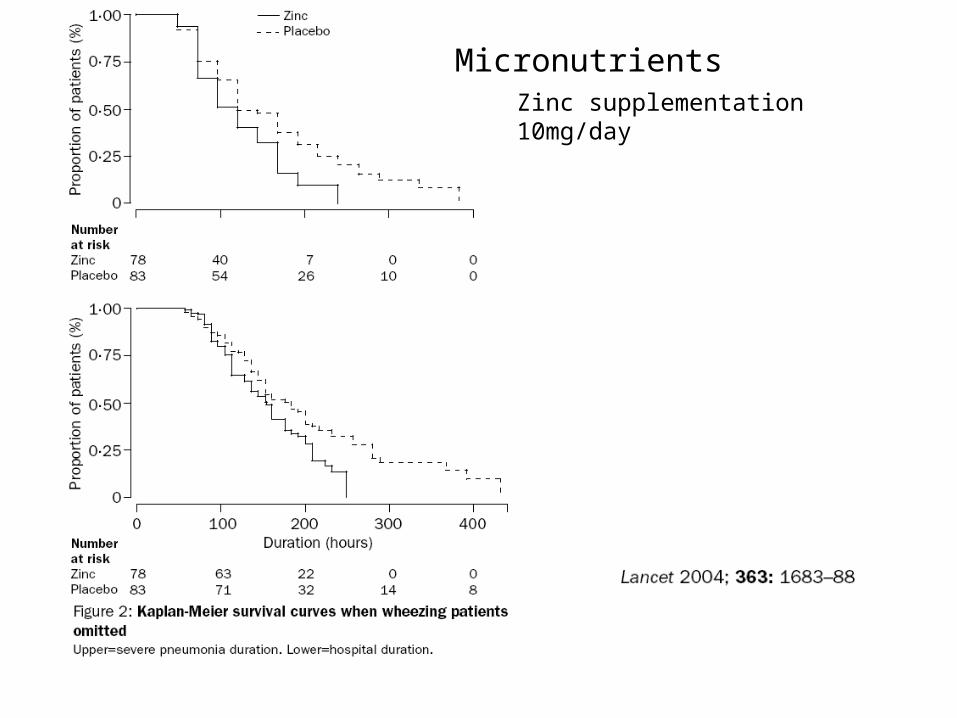
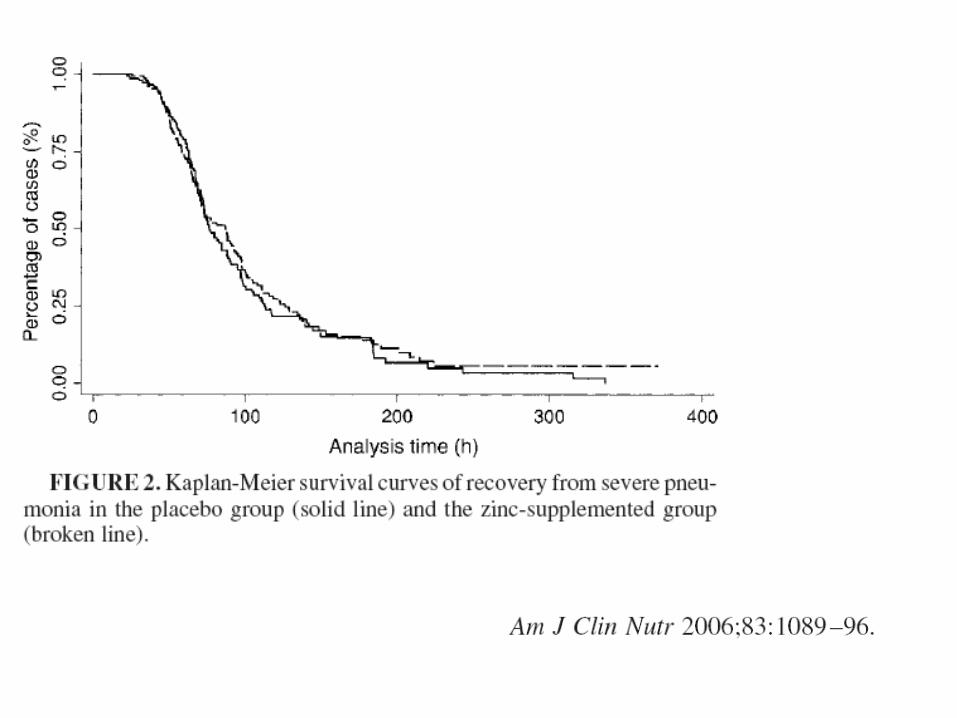
Zinc supplementation10mg/day
Micronutrients
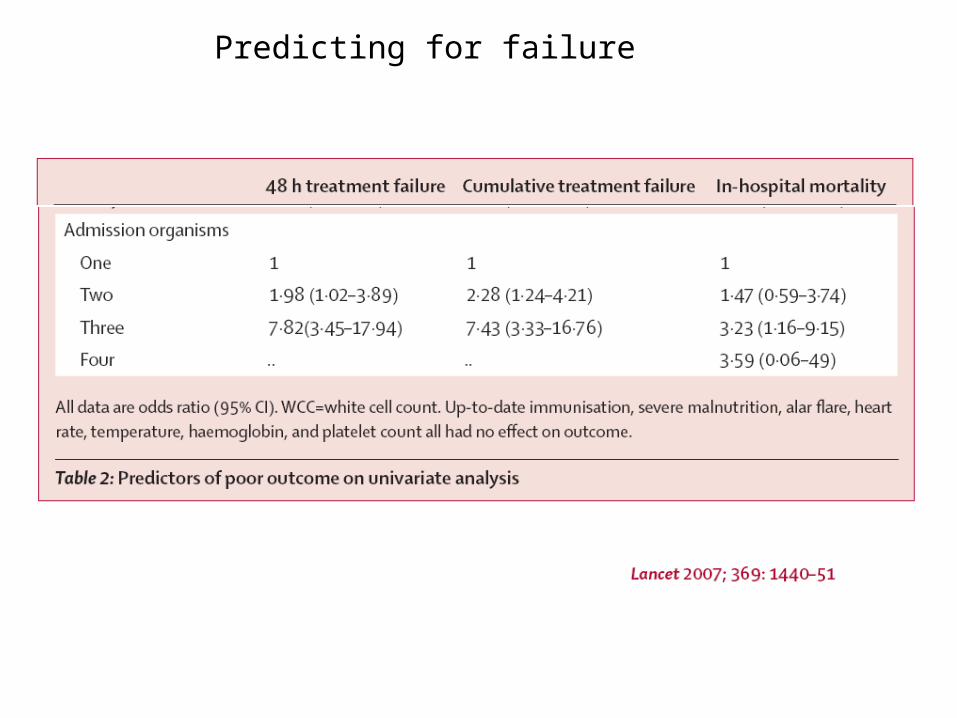
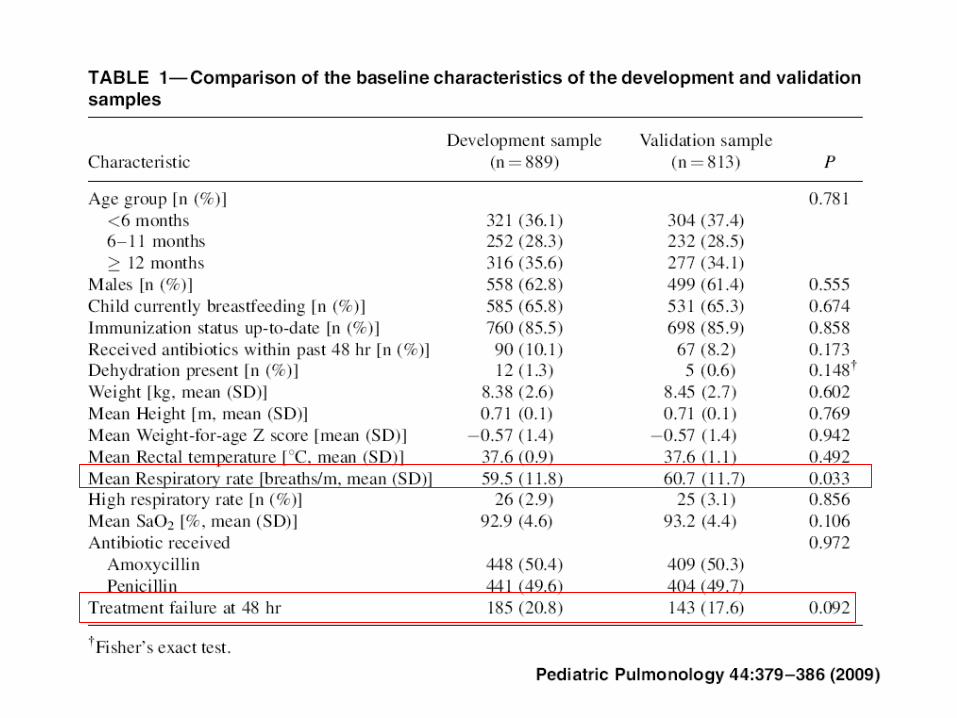
Predicting for failure
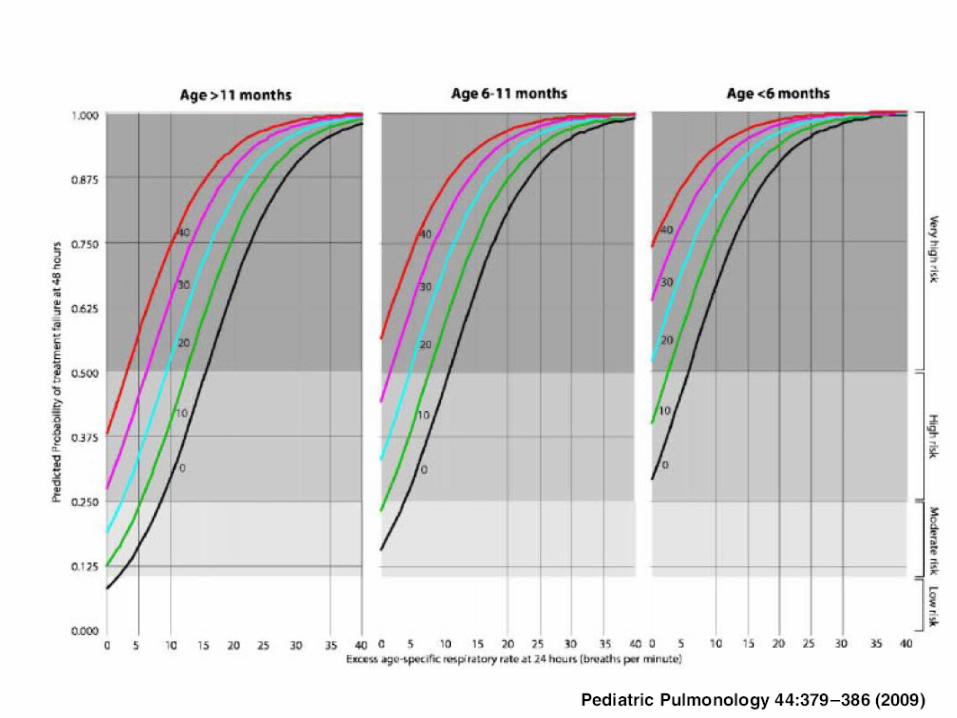
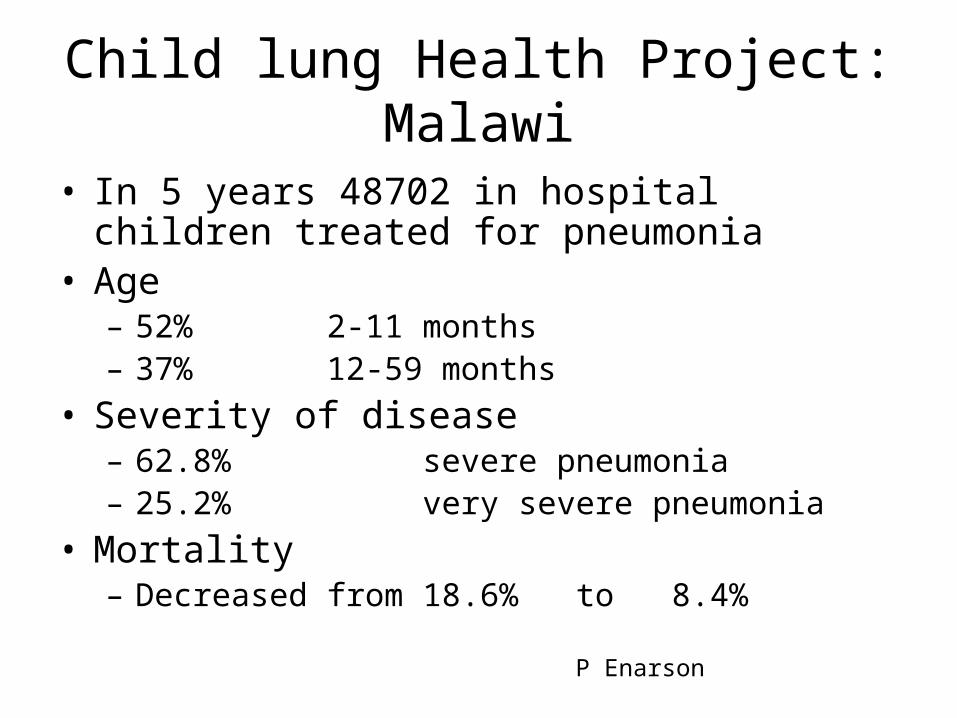
Child lung Health Project:Malawi
• In 5 years 48702 in hospital children treated for pneumonia
• Age– 52% 2-11 months– 37% 12-59 months
• Severity of disease– 62.8% severe pneumonia– 25.2% very severe pneumonia
• Mortality – Decreased from 18.6% to 8.4%
P Enarson